")
Back to Journals » Open Access Journal of Sports Medicine » Volume 15
Evaluation of Failed ACL Reconstruction: An Updated Review
Authors Kemler B, Coladonato C, Sonnier JH , Campbell MP , Darius D , Erickson BJ, Tjoumakaris FP, Freedman KB
Received 24 June 2023
Accepted for publication 23 March 2024
Published 2 April 2024 Volume 2024:15 Pages 29—39
DOI https://doi.org/10.2147/OAJSM.S427332
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Andreas Imhoff
Bryson Kemler,1 Carlo Coladonato,1 John Hayden Sonnier,1 Michael P Campbell,1 Danielle Darius,2 Brandon J Erickson,1 Fotios Paul Tjoumakaris,1 Kevin B Freedman1
1Department of Orthopaedic Surgery, Rothman Institute, Philadelphia, PA, USA; 2Department of Education, Drexel University College of Medicine, Philadelphia, PA, USA
Correspondence: Kevin B Freedman, Rothman Orthopaedics at Thomas Jefferson University, 825 Old Lancaster Road, Suite 200, Bryn Mawr, Philadelphia, PA, 19010, USA, Email [email protected]
Abstract: Failure rates among primary Anterior Cruciate Ligament Reconstruction (ACLR) range from 3.2% to 11.1%. Recently, there has been increased focus on surgical and anatomic considerations which predispose patients to failure, including excessive posterior tibial slope (PTS), unaddressed high-grade pivot shift, and improper tunnel placement. The purpose of this review was to provide a current summary and analysis of the literature regarding patient-related and technical factors surrounding revision ACLR, rehabilitation considerations, overall outcomes and return to sport (RTS) for patients who undergo revision ACLR. There is a convincingly higher re-tear and revision rate in patients who undergo ACLR with allograft than autograft, especially amongst the young, athletic population. Unrecognized Posterior Cruciate Ligament (PLC) injury is a common cause of ACLR failure and current literature suggests concurrent operative management of high-grade PLC injuries. Given the high rates of revision surgery in young active patients who return to pivoting sports, the authors recommend strong consideration of a combined ACLR + Anterolateral Ligament (ALL) or Lateral extra-articular tenodesis (LET) procedure in this population. Excessive PTS has been identified as an independent risk factor for ACL graft failure. Careful consideration of patient-specific factors such as age and activity level may influence the success of ACL reconstruction. Additional technical considerations including graft choice and fixation method, tunnel position, evaluation of concomitant posterolateral corner and high-grade pivot shift injuries, and the role of excessive posterior tibial slope may play a significant role in preventing failure.
Keywords: ACL, anterior cruciate ligament, anterior cruciate ligament reconstruction, failed ACL graft, posterior tibial slope, revision ACL reconstruction
Introduction
Anterior Cruciate Ligament Reconstruction (ACLR) tear rates have consistently increased over the past several years.1–4 Consequently, so too have the number of revision ACLR.5,6 Failure rates among primary ACLR range from 3.2% to 11.1% but have been reported to be as high as 34.2% when including high-risk cohorts such as young athletes.7,8 There are multiple factors which may lead to ACLR failure. Erickson et al published a review in 2017 outlining several of these including graft morphology, graft types, surgical technique, and timing of return to sport, all of which can affect outcomes in this patient population.9 Recently, there has been focus on surgical and anatomic considerations which predispose patients to failure, including excessive posterior tibial slope (PTS), unaddressed high grade pivot shift, and improper tunnel placement. As outcomes for revision ACLR are inferior compared to primary procedures,10–14 it is paramount to elucidate historical and contemporary reasons for failure. The purpose of this review is therefore to provide a current summary and analysis of the literature regarding patient-related and technical factors surrounding primary ACLR failure.
Methods
Review Process
A current concepts review was performed identifying 116 studies of interest pertaining to outcomes following primary ACLR with the most impactful articles shown in Table 1. PubMed, SCOPUS, and Cochrane databases were searched for any combination or variation of: “failed ACL reconstruction”, “rehabilitation considerations following ACL reconstruction”, and overall outcomes and return to sport (RTS) for patients who undergo revision ACLR. Studies were excluded if they were not in English, did not pertain to ACL reconstruction, were studies including animal subjects, or were done with cadaveric specimens.
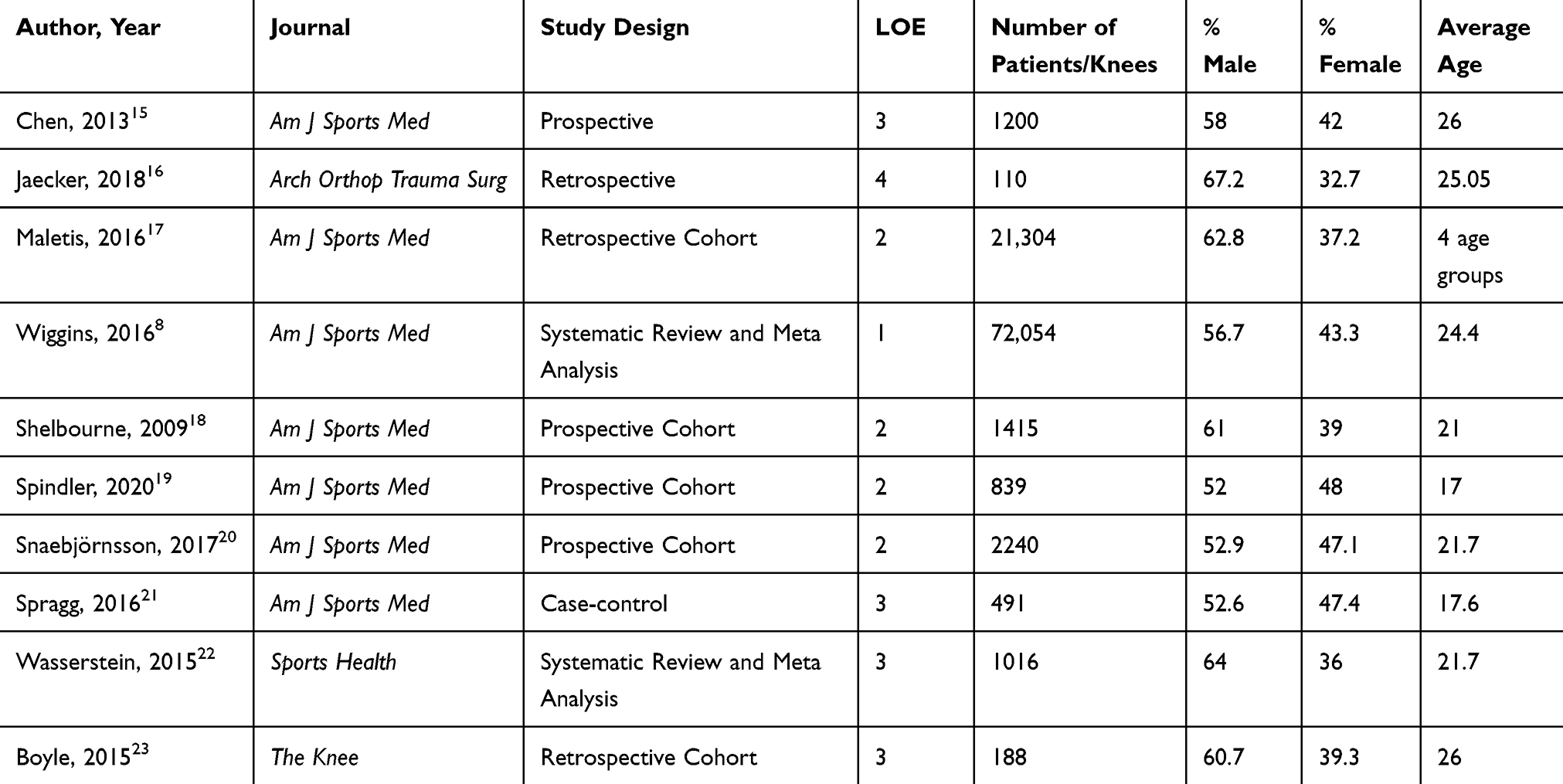 |
Table 1 Demographics of Included Studies |
Results
Traumatic vs Atraumatic Causes of Failure
The MARS cohort published their findings on mechanism of failure in single-revision ACLR from 2006 to 2011 and reported that a traumatic, noncontact injury to the ACL graft was the most common cause (55%) of re-rupture.15 Approximately 25% of patients in the cohort had a nontraumatic, gradual-onset recurrent injury, which contrasts with previously reported rates at high as 75%.24,25 Nontraumatic, gradual-onset recurrent injury was the most common cause (47%) of recurrent tear in patients who underwent multiple revisions, and the revising surgeon deemed technical error to be a contributing cause 58% of the time.15 The authors postulated femoral tunnel malposition was the main technical error contributing to failure, which is in agreement with current literature. Jaecker et al found in their cohort of 147 patients that non-anatomical femoral tunnel position was the most common cause of failure in patients deemed to fail due to technical error, followed by non-anatomical tibial tunnel position.16 A recent systematic review of 28 studies corroborated this, identifying technical error to contribute to 17% of failures, with femoral tunnel malposition being the leading cause.26
Patient Risk Factors for Re-Rupture
Several studies have analyzed patient-related risk factors on ACLR failure and have consistently found younger age to be the most significant factor.5,27–29 Maletis et al published data from the Kaiser Permanente ACL registry with mean follow-up of 2.2 years and divided patients into five cohorts based on age. The authors found that the youngest group (<21 yo) had the highest 5-year revision probability, and the risk of both ipsilateral and contralateral ACL injury decreases with age.17 Wiggins et al reported similar findings in their 2016 systematic review; overall, patients had a 15% second ACL reinjury rate (ipsilateral 7% and contralateral injury 8%), but patients younger than 25 years had a reinjury rate (ipsilateral + contralateral) of 21%. They found RTS to be a significant risk factor as well and concluded young athletes who RTS after ACLR have a 30 to 40 times greater risk of an ACL injury compared with uninjured adolescents.8 Considering the elevated incidence of recurrent injuries among younger athletes, patient age may actually serve as a surrogate marker for other predisposing elements. Greater risk-taking behaviors, sport-related factors such as aggressive play style and neuromuscular impairments have been theorized to contribute to these higher reinjury rates.30 Further, fear of reinjury has been reported as a major psychological barrier to rehabilitation progression following ACL injury, which may add to the risk profile of this population.31
It has been well-documented females are prone to higher risk of sustaining an ACL tear than males.32,33 Attempts have been made to link this to anatomical differences such as increased quadriceps angle and PTS in females, smaller notch width and ACL cross-sectional area, and hormonal contributions, however no conclusive correlation has been established.34–40 Interestingly, studies have consistently shown females to have similar or even slightly decreased rates of graft rupture and failure as males,17,33,41–43 however their rates of contralateral ACL injury are significantly greater following ACLR. Shelbourne et al published a 7.8% contralateral injury rate in female patients compared to a 4.3% ipsilateral reinjury rate (p > 0.001). This was in contrast to the study’s male population, in which there was no significant difference between the reinjury rate (4.1%) and contralateral injury rate (3.7%).18, indicating female-specific inherent risk factors which place them at higher risk for contralateral ACL rupture. Lindanger et al examined patients who returned to pivoting sports after ACLR and found 32% of females in the cohort sustained a contralateral tear compared to only 12% who required ipsilateral revision surgery. In their review, Erickson et al reported on the senior author’s (B.R.B.) 30-year outcome data and found a significantly higher percentage of female patients who went on to require contralateral ACLR than male patients (6.4% for female patients compared with 4.4% for male patients; p = 0.048). The contralateral procedure was performed at a mean of 34 months following the index ACLR in female patients, implying that the contralateral tear was not a compensatory phenomenon.9
Results
Tunnel Placement
Femoral tunnel malposition has consistently been cited as a significant factor in atraumatic ACLR failures.15,24–26 Biomechanical studies have confirmed the importance of femoral tunnel positioning on the force exerted on the ACL graft.44,45 Anterior tunnel placement causes the graft to stretch during knee flexion, which ultimately results in plastic deformation and eventual graft incompetence.46,47 Driscoll et al, in a cadaveric study of 6 specimens, found femoral tunnel placement in either the center of the bundles or the anteromedial portion of the ACL footprint resulted in similar anterior translation as the intact-ACL model in response to loading at 0⁰ to 60⁰. However, internal tibial rotation was greater in the anteromedial bundle tunnel model than the center tunnel model at all flexion angles, indicating improved rotatory stability without sacrificing anterior stability with femoral tunnel positioning in the center of the femoral footprint.45 Reliance on the native ACL footprint, however, assumes this anatomic location is ideal.48,49 Studies have reported substantial anatomic variability in location and size of ACL femoral and tibial footprints, with ranges from 83 mm2 to 197 mm2 and from 114 mm2to 229 mm2, respectively.50–52 In a study of 12 cadaveric specimens, Araujo et al assessed vertical tunnel placement on graft force. The authors found that at lower flexion angles (≤30⁰), tunnel positioning in the center of the femoral footprint resulted in similar in situ graft forces as the native ACL during both anterior tibial loading and simulated pivot shift loading, while in situ graft force with more vertical tunnel placement more closely resembled the native ACL at greater flexion angles (>45⁰).44 Transtibial drilling is particularly prone to excess tunnel verticality, although this may be counteracted through hyperflexion of the knee during drilling.53 Alternatively, contemporary surgical techniques utilize independent tibial and femoral drilling, with outside-in reamers, or straight and flexible reamers drilled inside-out through the anteromedial portal.54 Despite the importance of tunnel placement, agreement on ideal positioning amongst surgeons varies significantly.55
Graft Choice
Graft choice for primary ACLR has undergone continued debate. Hamstring tendon (HT) and bone-patellar tendon-bone (BPTB) autograft remain the two most utilized and studied grafts. As surgeon preference and experience factor heavily into graft choice, it is difficult to make an incontrovertible recommendation. A multicenter study consisting of 839 patients aged 14 to 22 years found autograft type to be 1 of the 3 most influential predictors of ACL graft revision at 6 years. Patients who underwent a hamstring autograft were found to have 2.1 times greater odds of requiring ACL graft revision compared to those who received a BPTB autograft (95% CI, 1.3–3.5; P = 0.004).19
A similar twofold higher failure rate after ACLR was seen with hamstring autograft compared to BPTB autograft in the Norwegian Cruciate Ligament Registry.56 In a meta-analysis comprised of fourteen randomized controlled trials, ten prospective comparative studies, and one national registry study, Samuelsen et al found a small but significant difference in graft rupture rate between patients who received BPTB autograft (212 out of 7560, 2.80%) and those who received HT autograft (1123 out of 39,510, 2.84%; p = 0.01). The authors observed overall low rates of failure in both groups and few differences between graft types in terms of knee laxity, and they concluded both remain viable options for primary ACLR. Graft-specific caveats must also be considered when deciding on graft choice. Rates of anterior kneeling pain in patients who underwent ACLR with autograft BPTB have been reported between 6.1% and 17.4% and may have a significant effect on patient outcome and satisfaction.57,58 The bone–bone interface, however, has been shown to fully incorporate histologically at 12 weeks in animal models, with the bone-tendon junction undergoing characteristic “ligamentization” over time.59,60 HT autograft relies on the soft tissue interface for healing, which may translate to substandard mechanical properties after transplantation.59
Autograft HT diameter has also been found to have an influence on revision risk following primary hamstring ACLR. Snaebjornsson et al found that for every increment of 0.5mm in graft diameter, the likelihood of patient requiring revision surgery after primary ACLR was 0.86x lower.20 Spragg et al found that ACLR patients with a 9 mm-diameter graft were 55% less likely to require revision than those with a 7 mm-diameter graft.21 Quadriceps tendon (QT) autograft has recently gained popularity, as it appears to have similar outcomes and less donor-site morbidity than BPTB.58 Shani et al reported cross-sectional area of the QT was almost double that of the BPTB (91mm2 vs 48 mm2, respectively), and found stiffness (466 N/mm vs 278 N/mm) and ultimate load to failure (2186 N vs 1581 N) were significantly greater for the QT graft compared with BPTB.61 Additionally, studies examining short- and mid-term outcomes found comparable failure and revision rates.62,63
There is more conclusive evidence to guide surgeons when deciding between autograft and allograft in ACLR. Several studies have found higher re-tear and revision rates in patients who undergo ACLR with allograft than autograft, especially amongst the young, athletic population. Wasserstein et al found that the combined failure rate for allografts was 25%, while the failure rate for autografts stood at 9.6%, with a mean patient age of 21.7 years.22 In patients younger than 18 years, Ellis et al found a 15x higher risk of re-tear in patients who received a BPTB allograft compared with those who received BPTB autograft.64 The risk of re-injury extends to older patients as well, but the difference is not as profound. Kraeutler et al’s meta-analysis of 5182 patients (average age = 27.6 years for autograft and 32.3 years for allograft) found a three-fold higher risk of re-rupture in those patients receiving BPTB allograft compared to autograft ACLR (12.7% vs 4.3%).65 While the exact reasoning behind this data is unknown, it is hypothesized allograft patients may feel better in the early months after ACLR and return to athletics sooner, increasing the risk of graft failure.29 Additionally, time to biologic incorporation of autograft tissue is dissimilar to allograft; Shino et al performed biopsies of ACL allografts and found that full graft maturity was not obtained until 18 months postoperatively in a canine model.66 Further, allograft tends to tear at different locations than autograft, which typically fails at the femoral insertion.67
Inadequate Graft Fixation
It is important to consider ACLR graft fixation techniques as several are currently in use, and load to failure and graft slippage vary amongst the different techniques.68 Tibial fixation is most commonly achieved with an interference screw, as it has been found to have satisfactory biomechanical properties to withstand the forces placed on the graft during the rehabilitation period.69 Femoral fixation is more variable and often depends on surgeon preference. For aperture fixation and especially for BTB grafts, an interference screw is most often utilized; however, it comes with the known complication of widening of the femoral tunnel, reportedly between 3% and 45%.70–74 Of note, the upper limit of 45% tunnel widening was in patients who underwent ACLR using single-bundle hamstring tendon with bioabsorbable screw fixation.73 Screw divergence with loss of femoral bone-plug fixation and screw migration are also documented causes of failure.75–79 Suspensory fixation is more commonly utilized for soft tissue grafts and has biomechanically superior results with soft-tissue graft slippage compared to aperture fixation.80 Suspensory fixation is accomplished with either fixed-loop or adjustable-loop devices; the adjustable-loop device can pull the graft to the top of the femoral tunnel to decrease the distance between the graft and its fixation, however biomechanical studies suggest these constructs can loosen after deployment.81,82 To counteract this, re-tensioning and knot tying over the device have been proposed after initial fixation of the graft and cycling of the knee.82–84 Choi et al evaluated 117 patients (67 patients with fixed-loop cortical femoral fixation compared to 50 with adjustable-loop cortical femoral fixation) and found no difference in arthrometer-measured knee laxity or functional outcome.85 Similarly, a recent large retrospective cohort series found no significant difference in postoperative knee stability or graft failure rates between adjustable- and fixed-loop cortical suspension in patients undergoing ACLR (10% vs 11%, p = 0.71).23 Despite the seemingly adequate stability achieved with suspensory fixation, however, it has been shown to result in larger degrees of tunnel widening compared with interference screws fixation, which is an important caveat to consider when evaluating a patient for revision ACLR.86
Missed Posterolateral Corner Injury
The posterolateral corner (PLC) of the knee consists of three major stabilizers: the fibular collateral ligament (FCL), the popliteus tendon (PLT), and the popliteofibular ligament (PFL).87,88 Unrecognized PLC injury has been increasingly recognized as a cause of ACLR failure.87 Biomechanically, force exerted on the ACL graft is significantly higher in the presence of an FCL injury than with an intact PLC.89 Clinically, conservative management of Fanelli type B PLC injuries has been shown to lead to poor outcomes as compared to Fanelli type A PLC injuries in patients who underwent ACLR.90 This suggests concurrent operative management of higher-grade PLC injuries to be necessary to achieve optimal outcomes.
High-Grade Pivot Shift
The ACL functions as the primary restraint to anterior tibial translation (ATT) but also is an important stabilizer to internal rotation.91,92 Studies have shown patients who experience persistent rotatory instability in the setting of a reconstructed ACL have worse outcomes, as well as higher rates of graft failure and revision surgery.93–95 In addition to the ACL, the IT band and anterolateral ligament (ALL) are lateral structures which function as adjunct stabilizers to anterolateral rotatory laxity.96–98 Cadaveric studies have shown LET in conjunction with ACLR improved rotatory laxity control, and this correlates with decreased pivot shift on exam.99–104 A recent multicenter randomized control trial found young, active patients (age 14–25) presenting with ACL rupture and high-grade rotatory laxity who underwent HT ACLR + LET had a clinical failure rate of 25% and a graft rupture rate of 4% compared to 40% and 11%, respectively, who underwent ACLR alone. Furthermore, ACL-deficient knees with a high-grade pivot shift have an increased risk of persistent instability with resultant medial meniscal tears and lateral compartment chondral damage. For these high-risk patients, early intervention is of the utmost importance.93,95,104 Given the high rates of revision surgery in young patients who return to pivoting sports, the authors recommend consideration of a combined ACLR + LET procedure in this population.30,105
Excessive Posterior Tibial Slope
Excessive PTS has been identified as an independent risk factor for ACL graft failure. Tibial slope has a strong, linear relationship to the level of force exerted on the ACL graft in an axially loaded knee; as slope increases, the force on the graft also increases.106 Christensen et al demonstrated a magnitude–response relationship, with an escalating risk for graft failure with increasing posterior slope.107 Winkler et al found that multiple ACL graft failures were associated with steeper medial posterior tibial slope, and the authors recommended strong consideration of posterior tibial slope in the re-revision setting. Biomechanical studies have shown that slope-reducing osteotomy significantly decreases anterior tibial translation in ACL deficient knees, and in the same study, ACL graft-forces decreased by 33.1% under a 400N axial load after a slope-reducing osteotomy compared to isolated reconstruction.108–110 Akoto et al published a case series of twenty patients with ACLR failure and found PTS >12⁰ was associated with increased shear forces on the ACL graft and resulted in a failure rate 11x higher than patients with PTS <12⁰.111 Song et al examined a case series of 18 patients who underwent slope-reducing osteotomy with combined primary ACLR for excessively steep PTS (range, 17⁰-18⁰) with a mean follow-up of 33.2 months. At final follow-up, they found mean medial and lateral tibial subluxation was significantly decreased with all patients returning to preinjury level.112 While posterior tibial slope is gaining increased awareness as an independent risk factor for ACLR failure, a slope-reducing osteotomy represents a much more complex and morbid procedure, and at this point should only be considered in the revision or re-revision setting.
Rehabilitation
In the literature, two main rehabilitation approaches are commonly discussed: a conservative method, which typically targets a return to sports within 9 to 12 months post-reconstruction, and an accelerated approach, which aims to enable patients to resume sports activities within 6 months.113,114 Unfortunately, the literature lacks a clear definition of the ideal timeframe for resuming sports activities following ACL reconstruction (ACLR), largely due to the significant influence of patient-specific factors on determining successful return-to-play (RTP). Further literature should seek to more clearly elucidate the role that various physiological and, importantly, psychological factors play in the RTP process.115
Discussion
The rates of Anterior Cruciate Ligament Reconstruction (ACLR) tear rates, along with the number of ACLR revisions performed, have been consistently increasing in recent years. Failure rates among primary ACLR range from 3.2% to 11.1%, and in young athletes, rates as high as 34.2% have been reported.7,8 Given the rise in revisions and established inferior outcomes following a revision ACLR, the purpose of this review was to analyze recent literature regarding patient related and technical factors surrounding revision ACLR and subsequent outcomes to provide the latest evidence-based data on the topic.
There are various mechanisms in which re-rupture occurs after ACLR, with the most common (55%) being a traumatic, noncontact injury to the graft.15 In several studies, younger age was consistently reported as the most significant patient-related factor leading to rupture. While it also has been well documented that females are prone to higher risk of sustaining an ACL tears than males, there has yet to be a conclusive anatomical reason for this.32,33 Furthermore, there are no differences in rates of graft rupture between males and females following ACLR.17,33,41–43
Due to the biomechanical force exerted on the ACL graft, femoral tunnel positioning is an important surgical consideration regarding rupture. However, there has yet to be a consensus or statistical evidence on optimal tunnel placement and the decision is largely made on surgeon preference. More concrete data on graft choice for primary ALCR has been shown, with the odds of revision being 2.1 times higher for patients receiving a hamstring autograft instead of a bone-patellar-bone autograft.19 Further, a comparative study by Biz et al demonstrated no statistical difference in clinical outcomes between patients undergoing ACLR with BTB allograft or hamstring tendon autograft after 2 years.116 Still, failure rates have been shown to be significantly higher in patients who undergo allograft compared to autograft.19,56 Moreover, considering the evidence in the literature, both options remain viable, and their trade-offs should be considered in order to meet the specific needs of the patient.
ACLR graft fixation techniques are an important intraoperative consideration. Tibial fixation is most commonly achieved with an interference screw while femoral fixation is more variable. While the biomechanical properties have been shown to be satisfactory, there are sparse data for subsequent revision when comparing fixation techniques.44,45 Unrecognized posterolateral corner injury is another intraoperative factor that has been increasingly linked to revision surgery in recent years.
Patients who experience persistent rotatory instability in the setting of a reconstructed ACL have worse outcomes and higher rates of both graft failure and revision surgery.93–95 Patients returning to pivoting sports should be considered for a combined ACLR + LET procedure for this population. Another patient-related factor for ACLR revision is excessive posterior tibial slope. Tibial slope has a strong, linear relationship to the level of force exerted onto an ACL graft in an axially loaded knee, making excessive posterior tibial slope an independent risk factor for ACL graft failure.106 However, a slope reducing osteotomy is not currently suggested for primary cases.
Finally, optimal patient rehabilitation is crucial to preventing ACLR revision. Unfortunately, patient-specific factors and the large variety of activities being performed by patients has made it difficult to determine an ideal timeline for returning to sport after ACLR. This topic remains poorly defined in the literature.
Conclusion
Careful consideration of patient-specific factors such as age and activity level may influence the success of ACL reconstruction. Additional technical considerations including graft choice and fixation method, tunnel position, evaluation of concomitant posterolateral corner and high-grade pivot shift injuries, and the role of excessive posterior tibial slope may play a significant role in preventing failure.
Disclosure
Dr Brandon J Erickson reports personal fees from Arthrex, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Gans I, Retzky JS, Jones LC, Tanaka MJ. Epidemiology of recurrent Anterior Cruciate Ligament injuries in National Collegiate Athletic Association sports: the injury surveillance program, 2004–2014. Orthop J Sports Med. 2018;6(6):232596711877782. doi:10.1177/2325967118777823
2. Lyman S, Koulouvaris P, Sherman S, Do H, Mandl LA, Marx RG. Epidemiology of Anterior Cruciate Ligament Reconstruction: trends, readmissions, and subsequent knee surgery. J Bone Jt Surg-Am Vol. 2009;91(10):2321–2328. doi:10.2106/JBJS.H.00539
3. Mall NA, Chalmers PN, Moric M, et al. Incidence and trends of Anterior Cruciate Ligament Reconstruction in the United States. Am J Sports Med. 2014;42(10):2363–2370. doi:10.1177/0363546514542796
4. Southam BR, Colosimo AJ, Grawe B. Underappreciated factors to consider in revision Anterior Cruciate Ligament Reconstruction: a current concepts review. Orthop J Sports Med. 2018;6(1):232596711775168. doi:10.1177/2325967117751689
5. Sanders TL, Pareek A, Hewett TE, et al. Long-term rate of graft failure after ACL reconstruction: a geographic population cohort analysis. Knee Surg Sports Traumatol Arthrosc. 2017;25(1):222–228. doi:10.1007/s00167-016-4275-y
6. Liukkonen RJ, Ponkilainen VT, Reito A. Revision rates after primary ACL Reconstruction performed between 1969 and 2018: a systematic review and meta regression analysis. Orthop J Sports Med. 2022;10(8):23259671221110190. doi:10.1177/23259671221110191
7. Magnussen RA, Meschbach NT, Kaeding CC, Wright RW, Spindler KP. ACL graft and contralateral ACL tear risk within ten years following reconstruction: a systematic review. JBJS Rev. 2015;3(1). doi:10.2106/JBJS.RVW.N.00052
8. Wiggins AJ, Grandhi RK, Schneider DK, Stanfield D, Webster KE, Myer GD. Risk of secondary injury in younger athletes after Anterior Cruciate Ligament Reconstruction: a systematic review and meta-analysis. Am J Sports Med. 2016;44(7):1861–1876. doi:10.1177/0363546515621554
9. Erickson BJ, Cvetanovich GL, Frank RM, Riff AJ, Bach BR. Revision ACL Reconstruction: a critical analysis review. JBJS Rev. 2017;5(6):e1. doi:10.2106/JBJS.RVW.16.00094
10. Wright RW, Gill CS, Chen L, et al. Outcome of Revision Anterior Cruciate Ligament Reconstruction: a systematic review. J Bone Jt Surg. 2012;94(6):531–536. doi:10.2106/JBJS.K.00733
11. Grassi A, Kim C, Muccioli GMM, Zaffagnini S, Amendola A. What is the mid-term failure rate of revision ACL reconstruction? A systematic review. Clin Orthop. 2017;475(10):2484–2499. doi:10.1007/s11999-017-5379-5
12. Yan X, Yang X, Feng J, Liu B, Hu Y. Does Revision Anterior Cruciate Ligament (ACL) reconstruction provide similar clinical outcomes to primary ACL Reconstruction? A systematic review and meta‐analysis. Orthop Surg. 2020;12(6):1534–1546. doi:10.1111/os.12638
13. Wright R, Spindler K, Huston L, et al. Revision ACL reconstruction outcomes: MOON cohort. J Knee Surg. 2011;24(04):289–294. doi:10.1055/s-0031-1292650
14. Wright RW, Huston LJ, Haas AK, et al.; MARS Group. Association between graft choice and 6-year outcomes of Revision Anterior Cruciate Ligament Reconstruction in the mars cohort. Am J Sports Med. 2021;49(10):2589–2598. doi:10.1177/03635465211027170
15. Chen JL, Allen CR, Stephens TE, et al. Differences in mechanisms of failure, intraoperative findings, and surgical characteristics between single- and multiple-revision ACL reconstructions: a Mars cohort study. Am J Sports Med. 2013;41(7):1571–1578. doi:10.1177/0363546513487980
16. Jaecker V, Zapf T, Naendrup JH, Kanakamedala AC, Pfeiffer T, Shafizadeh S. Differences between traumatic and non-traumatic causes of ACL revision surgery. Arch Orthop Trauma Surg. 2018;138(9):1265–1272. doi:10.1007/s00402-018-2954-5
17. Maletis GB, Chen J, Inacio MCS, Funahashi TT. Age-related risk factors for Revision Anterior Cruciate Ligament Reconstruction: a cohort study of 21,304 patients from the Kaiser Permanente Anterior Cruciate Ligament Registry. Am J Sports Med. 2016;44(2):331–336. doi:10.1177/0363546515614813
18. Shelbourne KD, Gray T, Haro M. Incidence of subsequent injury to either knee within 5 years after Anterior Cruciate Ligament Reconstruction with patellar tendon autograft. Am J Sports Med. 2009;37(2):246–251. doi:10.1177/0363546508325665
19. Spindler KP, Huston LJ, Zajichek A, et al.; MOON Knee Group. Anterior Cruciate Ligament Reconstruction in high school and college-aged athletes: does autograft choice influence anterior cruciate ligament revision rates? Am J Sports Med. 2020;48(2):298–309. doi:10.1177/0363546519892991
20. Snaebjörnsson T, Hamrin Senorski E, Ayeni OR, et al. Graft diameter as a predictor for revision Anterior Cruciate Ligament Reconstruction and KOOS and EQ-5D values: a cohort study from the Swedish National Knee Ligament Register based on 2240 patients. Am J Sports Med. 2017;45(9):2092–2097. doi:10.1177/0363546517704177
21. Spragg L, Chen J, Mirzayan R, Love R, Maletis G. The effect of autologous hamstring graft diameter on the likelihood for revision of Anterior Cruciate Ligament Reconstruction. Am J Sports Med. 2016;44(6):1475–1481. doi:10.1177/0363546516634011
22. Wasserstein D, Sheth U, Cabrera A, Spindler KP. A systematic review of failed Anterior Cruciate Ligament Reconstruction with autograft compared with allograft in young patients. Sports Health. 2015;7(3):207–216. doi:10.1177/1941738115579030
23. Boyle MJ, Vovos TJ, Walker CG, Stabile KJ, Roth JM, Garrett WE. Does adjustable-loop femoral cortical suspension loosen after anterior cruciate ligament reconstruction? A retrospective comparative study. The Knee. 2015;22(4):304–308. doi:10.1016/j.knee.2015.04.016
24. Diamantopoulos AP, Lorbach O, Paessler HH. Anterior Cruciate Ligament Revision Reconstruction: results in 107 Patients. Am J Sports Med. 2008;36(5):851–860. doi:10.1177/0363546507312381
25. Wang B, Lee KT. Results of revision anterior cruciate ligament reconstruction using a transportal technique. Acta Orthop Belg. 2015;81(4):752–758.
26. Vermeijden HD, Yang XA, van der List JP, DiFelice GS, Rademakers MV, Kerkhoffs GMMJ. Trauma and femoral tunnel position are the most common failure modes of anterior cruciate ligament reconstruction: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2020;28(11):3666–3675. doi:10.1007/s00167-020-06160-9
27. Maletis GB, Inacio MCS, Funahashi TT. Risk factors associated with revision and contralateral Anterior Cruciate Ligament Reconstructions in the Kaiser Permanente ACLR Registry. Am J Sports Med. 2015;43(3):641–647. doi:10.1177/0363546514561745
28. Rugg CM, Pitcher AA, Allen C, Pandya NK. Revision ACL reconstruction in adolescent patients. Orthop J Sports Med. 2020;8(9):232596712095333. doi:10.1177/2325967120953337
29. Borchers JR, Pedroza A, Kaeding C. Activity level and graft type as risk factors for Anterior Cruciate Ligament graft failure: a case-control study. Am J Sports Med. 2009;37(12):2362–2367. doi:10.1177/0363546509340633
30. Webster KE, Feller JA. Exploring the high reinjury rate in younger patients undergoing Anterior Cruciate Ligament Reconstruction. Am J Sports Med. 2016;44(11):2827–2832. doi:10.1177/0363546516651845
31. Truong LK, Mosewich AD, Holt CJ, Le CY, Miciak M, Whittaker JL. Psychological, social and contextual factors across recovery stages following a sport-related knee injury: a scoping review. Br J Sports Med. 2020;54(19):1149–1156. doi:10.1136/bjsports-2019-101206
32. Sutton KM, Bullock JM. Anterior cruciate ligament rupture: differences between males and females. J Am Acad Orthop Surg. 2013;21(1):41–50. doi:10.5435/JAAOS-21-01-41
33. Salmon L, Russell V, Musgrove T, Pinczewski L, Refshauge K. Incidence and risk factors for graft rupture and contralateral rupture after Anterior Cruciate Ligament Reconstruction. Arthrosc J Arthrosc Relat Surg. 2005;21(8):948–957. doi:10.1016/j.arthro.2005.04.110
34. Wordeman SC, Paterno MV, Quatman CE, Bates NA, Hewett TE. Arthrometric curve-shape variables to assess anterior cruciate ligament deficiency. Clin Biomech. 2012;27(8):830–836. doi:10.1016/j.clinbiomech.2012.04.011
35. Schneider A, Arias C, Bankhead C, Gaillard R, Lustig S, Servien E. Greater medial tibial slope is associated with increased anterior tibial translation in females with an ACL-deficient knee. Knee Surg Sports Traumatol Arthrosc. 2020;28(6):1901–1908. doi:10.1007/s00167-019-05643-8
36. Endo Y, Takemura M, Monma M, Mutsuzaki H, Mizukami M. Difference in sex and the effect of a dominant lower extremity in the posterior tibial slope angle in healthy Japanese subjects. Asia-Pac J Sports Med Arthrosc Rehabil Technol. 2021;23:8–12. doi:10.1016/j.asmart.2020.09.002
37. Shen L, Jin ZG, Dong QR, Li LB. Anatomical risk factors of Anterior Cruciate Ligament injury. Chin Med J. 2018;131(24):2960–2967. doi:10.4103/0366-6999.247207
38. Anderson AF, Dome DC, Gautam S, Awh MH, Rennirt GW. Correlation of anthropometric measurements, strength, anterior cruciate ligament size, and intercondylar notch characteristics to sex differences in anterior cruciate ligament tear rates. Am J Sports Med. 2001;29(1):58–66. doi:10.1177/03635465010290011501
39. Slauterbeck JR, Fuzie SF, Smith MP, et al. The menstrual cycle, sex hormones, and Anterior Cruciate Ligament Injury. J Athl Train. 2002;37(3):275–278.
40. Dienst M, Schneider G, Altmeyer K, et al. Correlation of intercondylar notch cross sections to the ACL size: a high resolution MR tomographic in vivo analysis. Arch Orthop Trauma Surg. 2007;127(4):253–260. doi:10.1007/s00402-006-0177-7
41. Kaeding CC, Pedroza AD, Reinke EK, Huston LJ, Spindler KP; MOON Consortium. Risk factors and predictors of subsequent ACL injury in either knee after ACL Reconstruction: prospective analysis of 2488 primary ACL reconstructions from the MOON cohort. Am J Sports Med. 2015;43(7):1583–1590. doi:10.1177/0363546515578836
42. Mitchell JJ, Cinque ME, Dornan GJ, et al. Primary versus revision Anterior Cruciate Ligament Reconstruction: patient demographics, radiographic findings, and associated lesions. Arthrosc J Arthrosc Relat Surg. 2018;34(3):695–703. doi:10.1016/j.arthro.2017.08.305
43. Schlumberger M, Schuster P, Schulz M, et al. Traumatic graft rupture after primary and revision anterior cruciate ligament reconstruction: retrospective analysis of incidence and risk factors in 2915 cases. Knee Surg Sports Traumatol Arthrosc. 2017;25(5):1535–1541. doi:10.1007/s00167-015-3699-0
44. Araujo PH, Asai S, Pinto M, et al. ACL graft position affects in situ graft force following ACL Reconstruction. J Bone Jt Surg. 2015;97(21):1767–1773. doi:10.2106/JBJS.N.00539
45. Driscoll MD, Isabell GP, Conditt MA, et al. Comparison of 2 femoral tunnel locations in anatomic single-bundle Anterior Cruciate Ligament Reconstruction: a biomechanical study. Arthrosc J Arthrosc Relat Surg. 2012;28(10):1481–1489. doi:10.1016/j.arthro.2012.03.019
46. Trojani C, Sbihi A, Djian P, et al. Causes for failure of ACL reconstruction and influence of meniscectomies after revision. Knee Surg Sports Traumatol Arthrosc. 2011;19(2):196–201. doi:10.1007/s00167-010-1201-6
47. Marrale J, Morrissey MC, Haddad FS. A literature review of autograft and allograft anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2007;15(6):690–704. doi:10.1007/s00167-006-0236-1
48. Kopf S, Musahl V, Tashman S, Szczodry M, Shen W, Fu FH. A systematic review of the femoral origin and tibial insertion morphology of the ACL. Knee Surg Sports Traumatol Arthrosc off J ESSKA. 2009;17(3):213–219. doi:10.1007/s00167-008-0709-5
49. Cho HJ, Kim TK, Kang SB, Do MU, Chang CB. Variations in sagittal locations of anterior cruciate ligament tibial footprints and their association with radiographic landmarks: a human cadaveric study. BMC Musculoskelet Disord. 2017;18(1):448. doi:10.1186/s12891-017-1822-8
50. Siebold R, Ellert T, Metz S, Metz J. Femoral insertions of the anteromedial and posterolateral bundles of the anterior cruciate ligament: morphometry and arthroscopic orientation models for double-bundle bone tunnel placement--a cadaver study. Arthrosc J Arthrosc Relat Surg off Publ Arthrosc Assoc N Am Int Arthrosc Assoc. 2008;24(5):585–592. doi:10.1016/j.arthro.2007.12.008
51. Ferretti M, Ekdahl M, Shen W, Fu FH. Osseous landmarks of the femoral attachment of the anterior cruciate ligament: an anatomic study. Arthrosc J Arthrosc Relat Surg off Publ Arthrosc Assoc N Am Int Arthrosc Assoc. 2007;23(11):1218–1225. doi:10.1016/j.arthro.2007.09.008
52. Luites JWH, Wymenga AB, Blankevoort L, Kooloos JGM. Description of the attachment geometry of the anteromedial and posterolateral bundles of the ACL from arthroscopic perspective for anatomical tunnel placement. Knee Surg Sports Traumatol Arthrosc off J ESSKA. 2007;15(12):1422–1431. doi:10.1007/s00167-007-0402-0
53. Bedi A, Raphael B, Maderazo A, Pavlov H, Williams RJ. Transtibial versus anteromedial portal drilling for Anterior Cruciate Ligament Reconstruction: a cadaveric study of femoral tunnel length and obliquity. Arthrosc J Arthrosc Relat Surg. 2010;26(3):342–350. doi:10.1016/j.arthro.2009.12.006
54. Steiner ME, Smart LR. Flexible instruments outperform rigid instruments to place anatomic Anterior Cruciate Ligament femoral tunnels without hyperflexion. Arthrosc J Arthrosc Relat Surg. 2012;28(6):835–843. doi:10.1016/j.arthro.2011.11.029
55. McConkey MO, Amendola A, Ramme AJ, et al. Arthroscopic agreement among surgeons on anterior cruciate ligament tunnel placement. Am J Sports Med. 2012;40(12):2737–2746. doi:10.1177/0363546512461740
56. Persson A, Fjeldsgaard K, Gjertsen JE, et al. Increased risk of revision with hamstring tendon grafts compared with patellar tendon grafts after Anterior Cruciate Ligament Reconstruction: a study of 12,643 patients from the Norwegian Cruciate Ligament Registry, 2004–2012. Am J Sports Med. 2014;42(2):285–291. doi:10.1177/0363546513511419
57. Freedman KB, D’Amato MJ, Nedeff DD, Kaz A, Bach BR. Arthroscopic Anterior Cruciate Ligament Reconstruction: a meta analysis comparing patellar tendon and hamstring tendon autografts. Am J Sports Med. 2003;31(1):2–11. doi:10.1177/03635465030310011501
58. Mouarbes D, Menetrey J, Marot V, Courtot L, Berard E, Cavaignac E. Anterior Cruciate Ligament Reconstruction: a systematic review and meta-analysis of outcomes for quadriceps tendon autograft versus bone–patellar tendon–bone and hamstring-tendon autografts. Am J Sports Med. 2019;47(14):3531–3540. doi:10.1177/0363546518825340
59. Yoshiya S, Nagano M, Kurosaka M, Muratsu H, Mizuno K. Graft healing in the bone tunnel in Anterior Cruciate Ligament Reconstruction. Clin Orthop Relat Res. 2000;376:278.
60. Claes S, Verdonk P, Forsyth R, Bellemans J. The “Ligamentization” process in Anterior Cruciate Ligament Reconstruction: what happens to the human graft? A systematic review of the literature. Am J Sports Med. 2011;39(11):2476–2483. doi:10.1177/0363546511402662
61. Shani RH, Umpierez E, Nasert M, Hiza EA, Xerogeanes J. Biomechanical Comparison of Quadriceps and Patellar Tendon Grafts in Anterior Cruciate Ligament Reconstruction. Arthrosc J Arthrosc Relat Surg. 2016;32(1):71–75. doi:10.1016/j.arthro.2015.06.051
62. Dai W, Leng X, Wang J, Cheng J, Hu X, Ao Y. Quadriceps tendon autograft versus bone–patellar tendon–bone and hamstring tendon autografts for Anterior Cruciate Ligament Reconstruction: a systematic review and meta-analysis. Am J Sports Med. 2021;036354652110302. doi:10.1177/03635465211030259
63. Perez JR, Emerson CP, Barrera CM, et al. Patient-reported knee outcome scores with soft tissue quadriceps tendon autograft are similar to bone–patellar tendon–bone autograft at minimum 2-year follow-up: a retrospective single-center cohort study in primary Anterior Cruciate Ligament Reconstruction surgery. Orthop J Sports Med. 2019;7(12):232596711989006. doi:10.1177/2325967119890063
64. Ellis HB, Matheny LM, Briggs KK, Pennock AT, Steadman JR. Outcomes and revision rate after bone–patellar tendon–bone allograft versus autograft Anterior Cruciate Ligament Reconstruction in patients aged 18 years or younger with closed physes. Arthrosc J Arthrosc Relat Surg. 2012;28(12):1819–1825. doi:10.1016/j.arthro.2012.06.016
65. Kraeutler MJ, Bravman JT, McCarty EC. Bone–patellar tendon–bone autograft versus allograft in outcomes of Anterior Cruciate Ligament Reconstruction: a meta-analysis of 5182 patients. Am J Sports Med. 2013;41(10):2439–2448. doi:10.1177/0363546513484127
66. Shino K, Kawasaki T, Hirose H, Gotoh I, Inoue M, Ono K. Replacement of the anterior cruciate ligament by an allogeneic tendon graft. An experimental study in the dog. J Bone Joint Surg Br. 1984;66(5):672–681. doi:10.1302/0301-620X.66B5.6501359
67. Magnussen RA, Taylor DC, Toth AP, Garrett WE. ACL graft failure location differs between allografts and autografts. Sports Med Arthrosc Rehabil Ther Technol. 2012;4(1):22. doi:10.1186/1758-2555-4-22
68. Monaco E, Labianca L, Speranza A, et al. Biomechanical evaluation of different anterior cruciate ligament fixation techniques for hamstring graft. J Orthop Sci. 2010;15(1):125–131. doi:10.1007/s00776-009-1417-9
69. Fabbriciani C, Mulas PD, Ziranu F, Deriu L, Zarelli D, Milano G. Mechanical analysis of fixation methods for anterior cruciate ligament reconstruction with hamstring tendon graft. An experimental study in sheep knees. The Knee. 2005;12(2):135–138. doi:10.1016/j.knee.2004.05.001
70. Webster KE, Feller JA, Hameister KA. Bone tunnel enlargement following anterior cruciate ligament reconstruction: a randomised comparison of hamstring and patellar tendon grafts with 2-year follow-up. Knee Surg Sports Traumatol Arthrosc. 2001;9(2):86–91. doi:10.1007/s001670100191
71. Höher J, Möller HD, Fu FH. Bone tunnel enlargement after anterior cruciate ligament reconstruction: fact or fiction? Knee Surg Sports Traumatol Arthrosc. 1998;6(4):231–240. doi:10.1007/s001670050105
72. Clatworthy MG, Annear P, Bulow JU, Bartlett RJ. Tunnel widening in anterior cruciate ligament reconstruction: a prospective evaluation of hamstring and patella tendon grafts. Knee Surg Sports Traumatol Arthrosc. 1999;7(3):138–145. doi:10.1007/s001670050138
73. Järvelä T, Moisala AS, Paakkala T, Paakkala A. Tunnel enlargement after double-bundle Anterior Cruciate Ligament Reconstruction: a prospective, randomized study. Arthrosc J Arthrosc Relat Surg. 2008;24(12):1349–1357. doi:10.1016/j.arthro.2008.07.018
74. Iorio R, Vadalà A, Argento G, Di Sanzo V, Ferretti A. Bone tunnel enlargement after ACL reconstruction using autologous hamstring tendons: a CT study. Int Orthop. 2007;31(1):49–55. doi:10.1007/s00264-006-0118-7
75. Schroeder FJ. Reduction of femoral interference screw divergence during endoscopic Anterior Cruciate Ligament Reconstruction. Arthrosc J Arthrosc Relat Surg. 1999;15(1):41–48. doi:10.1053/ar.1999.v15.015004
76. Dworsky BD, Jewell BF, Bach BR. Interference screw divergence in endoscopic anterior cruciate ligament reconstruction. Arthrosc J Arthrosc Relat Surg. 1996;12(1):45–49. doi:10.1016/S0749-8063(96)90218-2
77. Baums MH, Zelle BA, Schultz W, Ernstberger T, Klinger HM. Intraarticular migration of a broken biodegradable interference screw after anterior cruciate ligament reconstruction. Knee Surg Sports Traumatol Arthrosc. 2006;14(9):865–868. doi:10.1007/s00167-006-0049-2
78. Krappel FA, Bauer E, Harland U. The migration of a BioScrew® as a differential diagnosis of knee pain, locking after ACL reconstruction: a report of two cases. Arch Orthop Trauma Surg. 2006;126(9):615–620. doi:10.1007/s00402-006-0101-1
79. Appelt A, Baier M. Recurrent locking of knee joint caused by intraarticular migration of bioabsorbable tibial interference screw after arthroscopic ACL reconstruction. Knee Surg Sports Traumatol Arthrosc. 2007;15(4):378–380. doi:10.1007/s00167-006-0220-9
80. Ahmad CS, Gardner TR, Groh M, Arnouk J, Levine WN. Mechanical properties of soft tissue femoral fixation devices for Anterior Cruciate Ligament Reconstruction. Am J Sports Med. 2004;32(3):635–640. doi:10.1177/0363546503261714
81. Chang MJ, Bae TS, Moon YW, Ahn JH, Wang JH. A comparative biomechanical study of femoral cortical suspension devices for soft-tissue Anterior Cruciate Ligament Reconstruction: adjustable-length loop versus fixed-length loop. Arthrosc J Arthrosc Relat Surg. 2018;34(2):566–572. doi:10.1016/j.arthro.2017.08.294
82. Petre BM, Smith SD, Jansson KS, et al. Femoral cortical suspension devices for soft tissue Anterior Cruciate Ligament Reconstruction: a comparative biomechanical study. Am J Sports Med. 2013;41(2):416–422. doi:10.1177/0363546512469875
83. Monaco E, Bachmaier S, Fabbri M, Lanzetti RM, Wijdicks CA, Ferretti A. Intraoperative workflow for all-inside Anterior Cruciate Ligament Reconstruction: an in vitro biomechanical evaluation of preconditioning and knot tying. Arthrosc J Arthrosc Relat Surg. 2018;34(2):538–545. doi:10.1016/j.arthro.2017.08.283
84. Noonan BC, Dines JS, Allen AA, Altchek DW, Bedi A. Biomechanical evaluation of an adjustable loop suspensory Anterior Cruciate Ligament Reconstruction Fixation Device: the value of retensioning and knot tying. Arthrosc J Arthrosc Relat Surg. 2016;32(10):2050–2059. doi:10.1016/j.arthro.2016.02.010
85. Choi NH, Yang BS, Victoroff BN. Clinical and radiological outcomes after hamstring Anterior Cruciate Ligament Reconstructions: comparison between fixed-loop and adjustable-loop cortical suspension devices. Am J Sports Med. 2017;45(4):826–831. doi:10.1177/0363546516674183
86. Noyes FR, Barber SD, Simon R. High tibial osteotomy and ligament reconstruction in varus angulated, anterior cruciate ligament-deficient knees. A two- to seven-year follow-up study. Am J Sports Med. 1993;21(1):2–12. doi:10.1177/036354659302100102
87. Vinson EN, Major NM, Helms CA. The posterolateral corner of the knee. Am J Roentgenol. 2008;190(2):449–458. doi:10.2214/AJR.07.2051
88. Dean RS, LaPrade RF. ACL and posterolateral corner injuries. Curr Rev Musculoskelet Med. 2020;13(1):123–132. doi:10.1007/s12178-019-09581-3
89. LaPrade RF, Resig S, Wentorf F, Lewis JL. The effects of grade iii posterolateral knee complex injuries on Anterior Cruciate Ligament Graft Force. Am J Sports Med. 1999;27(4):469–475. doi:10.1177/03635465990270041101
90. Dhillon M, Akkina N, Prabhakar S, Bali K. Evaluation of outcomes in conservatively managed concomitant Type A and B posterolateral corner injuries in ACL deficient patients undergoing ACL reconstruction. The Knee. 2012;19(6):769–772. doi:10.1016/j.knee.2012.02.004
91. Chhabra A, Starman JS, Ferretti M, Vidal AF, Zantop T, Fu FH. Anatomic, radiographic, biomechanical, and kinematic evaluation of the Anterior Cruciate Ligament and its two functional bundles. J Bone Jt Surg. 2006;88(suppl_4):2–10. doi:10.2106/JBJS.F.00616
92. Smith BA, Livesay GA, Woo SL. Biology and biomechanics of the anterior cruciate ligament. Clin Sports Med. 1993;12(4):637–670.
93. Ayeni OR, Chahal M, Tran MN, Sprague S. Pivot shift as an outcome measure for ACL reconstruction: a systematic review. Knee Surg Sports Traumatol Arthrosc. 2012;20(4):767–777. doi:10.1007/s00167-011-1860-y
94. Mohtadi NG, Chan DS, Dainty KN, Whelan DB. Patellar tendon versus hamstring tendon autograft for anterior cruciate ligament rupture in adults. Cochrane Database Syst Rev. 2011. doi:10.1002/14651858.CD005960.pub2
95. Prodromos CC, Joyce BT, Shi K, Keller BL. A meta-analysis of stability after Anterior Cruciate Ligament Reconstruction as a function of hamstring versus patellar tendon graft and fixation type. Arthrosc J Arthrosc Relat Surg. 2005;21(10):
96. Herbst E, Albers M, Burnham JM, et al. The anterolateral complex of the knee: a pictorial essay. Knee Surg Sports Traumatol Arthrosc. 2017;25(4):1009–1014. doi:10.1007/s00167-017-4449-2
97. Kittl C, El-Daou H, Athwal KK, et al. The role of the anterolateral structures and the ACL in controlling laxity of the intact and ACL-deficient knee. Am J Sports Med. 2016;44(2):345–354. doi:10.1177/0363546515614312
98. Vincent JP, Magnussen RA, Gezmez F, et al. The anterolateral ligament of the human knee: an anatomic and histologic study. Knee Surg Sports Traumatol Arthrosc. 2012;20(1):147–152. doi:10.1007/s00167-011-1580-3
99. Geeslin AG, Moatshe G, Chahla J, et al. Anterolateral knee extra-articular stabilizers: a robotic study comparing anterolateral ligament reconstruction and modified Lemaire lateral extra-articular tenodesis. Am J Sports Med. 2018;46(3):607–616. doi:10.1177/0363546517745268
100. Inderhaug E, Stephen JM, Williams A, Amis AA. Anterolateral tenodesis or anterolateral ligament complex reconstruction: effect of flexion angle at graft fixation when combined with ACL reconstruction. Am J Sports Med. 2017;45(13):3089–3097. doi:10.1177/0363546517724422
101. Inderhaug E, Stephen JM, Williams A, Amis AA. Biomechanical comparison of anterolateral procedures combined with Anterior Cruciate Ligament Reconstruction. Am J Sports Med. 2017;45(2):347–354. doi:10.1177/0363546516681555
102. Devitt BM, Bell SW, Ardern CL, et al. The role of lateral extra-articular tenodesis in primary Anterior Cruciate Ligament Reconstruction: a systematic review with meta-analysis and best-evidence synthesis. Orthop J Sports Med. 2017;5(10):232596711773176. doi:10.1177/2325967117731767
103. Getgood AMJ, Bryant DM, Litchfield R, et al. Lateral extra-articular tenodesis reduces failure of hamstring tendon autograft Anterior Cruciate Ligament Reconstruction: 2-year outcomes from the STABILITY Study randomized clinical trial. Am J Sports Med. 2020;48(2):285–297. doi:10.1177/0363546519896333
104. Song GY, Hong L, Zhang H, Zhang J, Li Y, Feng H. Clinical outcomes of combined lateral extra-articular tenodesis and intra-articular Anterior Cruciate Ligament Reconstruction in addressing high-grade pivot-shift phenomenon. Arthrosc J Arthrosc Relat Surg. 2016;32(5):898–905. doi:10.1016/j.arthro.2015.08.038
105. Webster KE, Feller JA, Leigh WB, Richmond AK. Younger patients are at increased risk for graft rupture and contralateral injury after Anterior Cruciate Ligament Reconstruction. Am J Sports Med. 2014;42(3):641–647. doi:10.1177/0363546513517540
106. Bernhardson AS, Aman ZS, Dornan GJ, et al. Tibial slope and its effect on force in Anterior Cruciate Ligament grafts: anterior cruciate ligament force increases linearly as posterior tibial slope increases. Am J Sports Med. 2019;47(2):296–302. doi:10.1177/0363546518820302
107. Christensen JJ, Krych AJ, Engasser WM, Vanhees MK, Collins MS, Dahm DL. Lateral tibial posterior slope is increased in patients with early graft failure after Anterior Cruciate Ligament Reconstruction. Am J Sports Med. 2015;43(10):2510–2514. doi:10.1177/0363546515597664
108. Imhoff FB, Mehl J, Comer BJ, et al. Slope-reducing tibial osteotomy decreases ACL-graft forces and anterior tibial translation under axial load. Knee Surg Sports Traumatol Arthrosc. 2019;27(10):3381–3389. doi:10.1007/s00167-019-05360-2
109. Imhoff FB, Comer B, Obopilwe E, Beitzel K, Arciero RA, Mehl JT. Effect of slope and varus correction high tibial osteotomy in the ACL-deficient and ACL-reconstructed knee on kinematics and ACL graft force: a biomechanical analysis. Am J Sports Med. 2021;49(2):410–416. doi:10.1177/0363546520976147
110. Winkler PW, Wagala NN, Hughes JD, Lesniak BP, Musahl V. A high tibial slope, allograft use, and poor patient-reported outcome scores are associated with multiple ACL graft failures. Knee Surg Sports Traumatol Arthrosc. 2021. doi:10.1007/s00167-021-06460-8
111. Akoto R, Alm L, Drenck TC, Frings J, Krause M, Frosch KH. Slope-correction osteotomy with lateral extra-articular tenodesis and revision Anterior Cruciate Ligament Reconstruction is highly effective in treating high-grade anterior knee laxity. Am J Sports Med. 2020;48(14):3478–3485. doi:10.1177/0363546520966327
112. Yang SG, Kun NQ, Zheng T, Jun ZZ, Feng H, Zhang H. Slope-reducing tibial osteotomy combined with primary Anterior Cruciate Ligament Reconstruction produces improved knee stability in patients with steep posterior tibial slope, excessive anterior tibial subluxation in extension, and chronic meniscal posterior horn tears. Am J Sports Med. 2020;48(14):3486–3494. doi:10.1177/0363546520963083
113. Waldron K, Brown M, Calderon A, Feldman M. Anterior cruciate ligament rehabilitation and return to sport: how fast is too fast? Arthrosc Sports Med Rehabil. 2022;4(1):e175–e179. doi:10.1016/j.asmr.2021.10.027
114. Silva F, Ribeiro F, Oliveira J. Effect of an accelerated ACL rehabilitation protocol on knee proprioception and muscle strength after anterior cruciate ligament reconstruction. Arch Exerc Health Dis. 2012;3:139–144. doi:10.5628/aehd.v3i1-2.113
115. Ellman MB, Sherman SL, Forsythe B, LaPrade RF, Cole BJ, Bach BR. Return to play following Anterior Cruciate Ligament Reconstruction:. J Am Acad Orthop Surg. 2015;23(5):283–296. doi:10.5435/JAAOS-D-13-00183
116. Biz C, Cigolotti A, Zonta F, Belluzzi E, Ruggieri P. ACL reconstruction using a bone patellar tendon bone (BPTB) allograft or a hamstring tendon autograft (GST): a single-center comparative study. Acta Biomed. 2019;90(12–S):109–117. doi:10.23750/abm.v90i12-S.8973
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.