")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Evaluation of Quality of Prevention of Mother to Child Transmission of HIV Service Provision and Its Determinants: The Case of Health Facility Readiness and Mothers’ Perspectives
Authors Terefe B , Mekonnen BA , Tamir TT , Assimamaw NT , Limenih MA
Received 22 October 2023
Accepted for publication 29 December 2023
Published 6 January 2024 Volume 2024:17 Pages 93—110
DOI https://doi.org/10.2147/JMDH.S446035
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Bewuketu Terefe,1 Birhanu Abie Mekonnen,2 Tadesse Tarik Tamir,3 Nega Tezera Assimamaw,3 Miteku Andualem Limenih4
1Department of Community Health Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 2Department of Pediatrics and Child Health, School of Medicine, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 3Department of Pediatrics and Child Health Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia; 4Department of Epidemiology and Biostatistics, Institute of Public Health, College of Medicine and Health Sciences, University of Gondar, Gondar, Ethiopia
Correspondence: Bewuketu Terefe, Department of Community Health Nursing, School of Nursing, College of Medicine and Health Sciences, University of Gondar, Gondar, Amhara Region, Ethiopia, Post Office Box: 196, Tel +251918099504, Email [email protected]
Background: Prevention of Mother-To-Child Transmission of HIV (PMTCT) is a comprehensive intervention aimed at reducing vertical transmission. More than 90% of pediatric AIDS cases are caused by MTCT. However, the quality of care has lagged in terms of service integration, client satisfaction, and facility readiness, although improvements have been observed. Evidence on the quality of PMTCT services is required by clinicians, and policymakers. Therefore, this study aimed to evaluate the effectiveness of PMTCT services provided by public health facilities in Northwest Ethiopia.
Methods: This cross-sectional study was conducted at nine public health facilities in Gondar city between June 1 and July 17, 2022. A total of 334 mothers were participated. The Structure-Process-Outcome components were used to evaluate service quality. About 135 counseling sessions were observed. The SPSS 26 software was used for statistical analyses. To identify mothers’ satisfaction with the service, P-values < 0.25, and < 0.05 were considered in the binary and multiple logistic regression analyses to identify significant variables, respectively.
Results: The overall performance of the health facilities was 74.09% (72.19– 76.01 CI 95%). In 88.89% of cases, the output quality was higher and rated as good. However, the quality of the input and process services was 60.40% and 72.97%, respectively. Women’s satisfaction was 67.09%. Women aged 15– 24 years (AOR= 0.31; 95% CI:0.06, 0.79), formally educated (AOR=0.59; 95% CI:0.35, 0.67), > one hour of arrival (AOR=0.71; 95% CI:0.55, 0.93), > 30 minutes waiting time (AOR=0.23; 95% CI:0.11, 0.37), sufficient time for counseling (AOR=2.83; 95% CI:1.72, 3.97), and opening hours (AOR=4.27; 95% CI:2.09, 6.67) were factors associated with satisfaction in women.
Conclusion: The quality of PMTCT service provision and mothers’ satisfaction were low. Reducing waiting time, punctuality of service providers, adequate counselling, and availability of basic resources can boost mothers’ satisfaction.
Keywords: determinants, evaluation, health facility readiness, quality, satisfaction
Introduction
More than 90% of HIV infections in newborns are caused by vertical transmission, which is the HIV infection that occurs from an HIV-positive mother to her child during childbirth and remains an issue during the postnatal period until the child stops breastfeeding. Infants born to mothers with a positive HIV serostatus are known as exposed infants and may contract the virus through nursing, childbirth, or pregnancy.1–3 Africa is the most affected continent, accounting for over two-thirds of all new HIV infections globally, with 25.7 million individuals living with the virus in 2018.1,4 With an HIV prevalence of 0.96%, which varies from less than 0.1% in Ethiopia’s Somali region to 4.8% in the Gambella region, Ethiopia is one of 21 high-burden countries.4,5 However, the 2016 World Health Organization (WHO) report confirmed this; it estimated that Antiretroviral Therapy (ART) coverage for adults and children (0–14 years) was 59% and 35%, respectively.6 Hence, improving the quality of healthcare is vital to tackle the challenges among these segments of the population.
The quality of healthcare services plays a significant role in achieving the Universal Health Coverage (UHC) plan.7 Only in developing countries, around 5.7 to 8.4 million deaths, and 60% of the total deaths occur due to poor quality care in developing countries.7 Quality in the healthcare delivery system attracts and requires more attention from different stakeholders.8,9 To date, every individual has a great and indistinctive need for high-quality services everywhere they access what they need, regardless of the quality and dimensions of quality.10 The Institute of Medicine (IOM) defined the quality of healthcare more precisely after capturing the definition of quality by different scholars, institutions of health, and countries from different points of view: the degree to which health services for individuals and populations increase the likelihood of desired health outcomes and are consistent with current professional knowledge.11 Because it is assumed that equality and quality are related and should be addressed for every individual, quality and equity are defined in combination in Ethiopia.12,13 Quality in Ethiopia is defined as comprehensive care that is measurably safe, effective, patient-centered, uniformly delivered in a timely manner, affordable to all Ethiopians, and appropriately utilizes resources and services efficiently. Continuous exploration of quality will help us forecast the three core elements of quality, namely quality planning, quality improvement, and quality control.14
Numerous studies have been conducted regarding the quality of prevention of mother-to-child transmission of HIV. Sub-Saharan African (SSA) women experience a disproportionately high burden of HIV infection due to inadequate screening for Sexually Transmitted Diseases (STDs), inappropriate infant feeding practices, male partners’ non-participation in PMTCT, and a lack of knowledge regarding MTCT.15,16 Other challenges for the poor-quality service of PMTCT in SSA are limited human resources, poor monitoring leadership in health facilities, governance, infrastructure, poor working conditions, and service delivery systems.17–20 SSA needs to address structural and social barriers beyond the individual level to enhance PMTCT services.21 Capacity building of health providers for PMTCT, hepatitis B and C, Sexually Transmitted Infections (STIs), syphilis, providing information, support, and counselling on infant feeding methods, and other reproductive services are needed.22,23 A study conducted in Tanzania on health facilities’ readiness for quality PMTCT services indicated that one-third of pregnant women received all five components required for Provider-Initiated Testing and Counseling (PITC), which implies that increasing the availability of trained staff, diagnostic tools, and ARTs among health facilities is highly recommended.24
Several qualitative studies from Ethiopia stated that health system factors such as a lack of appropriate follow-up mechanisms, inadequate access to Antiretroviral drugs, trained humans, a high turnover rate, client unwillingness, and inadequate equipment could contribute to decreasing the quality of PMTCT services.25–27 Another qualitative study in northern Ethiopia showed about 33% of input, 25% of process, and output service quality.28 Furthermore, a mixed-method study showed that the overall quality of PMTCT services was low (47%).29
Despite existing evidence that attempts to address some of the factors that could contribute to low-quality PMTCT services, only a few have examined the level of facility and health provider readiness to enhance the provision of good-quality PMTCT services. It is crucial to evaluate how healthcare providers and facilities are committed to reducing MTCT of HIV infection. For this reason, not only the availability of services but also provider and facility readiness will promise clients a high quality of care.30,31 Therefore, a full understanding of the relationship between facility readiness and provision of high-quality PMTCT clients is crucial, as little is known about this relationship. Thus, the current study provides more information than existing evidence. Therefore, using the Donabedian paradigm, this study aimed to assess health facility readiness, satisfaction, and its associated factors among pregnant mothers in Gondar city public health facilities.
Methods and Materials
Study Setting and Period
This institutional cross-sectional study was conducted in Gondar City’s public health facilities between June 1 and July 17, 2022. There were eight public health centers and one specialized compressive hospital in the city. The city is located 748 km northwest of Addis Ababa, the capital of Ethiopia. The Central Statistical Agency of Ethiopia’s (CSA) 2007 national census showed that Gondar has a total population of 207,044. All health facilities provide basic maternal and child health services, including the PMTCT. Moreover, the University of Gondar Comprehensive and Specialized Hospital is the only referral center for PMTCT/ART, as well as all maternal and child healthcare services, providing healthcare services to more than ten million people in the city and nearby catchments. This study was conducted in eight public health facilities and one comprehensive specialized hospital.
Source and Study Population
All public health facilities and pregnant mothers who had follow-up within these public health facilities in Gondar City were the source population to determine the quality of PMTCT services based on the status of health facility readiness and women’s satisfaction, respectively. Mothers who attended the Antenatal Care (ANC), and PMTCT services throughout the data collection period were included in this study.
Eligibility Criteria
This study included all pregnant women who visited health facilities and were provided PMTCT services. The study involved voluntary participation of health facilities, PMTCT counselors, and all pregnant women. Women who experienced severe pain and those who had less than six months of experience were excluded.
Sample Size Determination and Sampling Procedure
Sample Size for Mothers
The estimated sample size was determined based on the main outcome of the study (the overall quality of PMTCT services) and was powered by all other specific aims, including health facility readiness and women’s satisfaction. Among these, the maximum sample size and the number of health facilities were considered.
Therefore, the minimum number of participants required to estimate the proportion of quality of PMTCT services and women’s satisfaction was determined using the best available estimates from Assefa et al and computed by using a single population proportion formula with the following assumptions: the overall quality of PMCT was 74.7%.32 A response rate of 85% was expected in the study; therefore, a 15% non-response rate was achieved. As the study was conducted at a multicenter level, we need to increase the precision by using a larger possible sample size. Taking this into account, a margin of error of five percent was considered in the sample size calculation. Then the sample size was determined using the concept of a single population proportion formula by considering the assumptions  = critical value for normal distribution at a 95% confidence level, which equals 1.96 (z value at α = 0.05), estimated proportion (p = 74.7%), and absolute precision or margin of error 5% (d = 0.05) using the formula
= critical value for normal distribution at a 95% confidence level, which equals 1.96 (z value at α = 0.05), estimated proportion (p = 74.7%), and absolute precision or margin of error 5% (d = 0.05) using the formula  . Finally, considering the above assumptions, the minimum sample size was 334. However, we tried to calculate the minimum sample size to estimate the quality of PMTCT services based on the proportion of women’s satisfaction with PMTCT services, which is lower than the above sample size; we used a larger sample size to proceed further.
. Finally, considering the above assumptions, the minimum sample size was 334. However, we tried to calculate the minimum sample size to estimate the quality of PMTCT services based on the proportion of women’s satisfaction with PMTCT services, which is lower than the above sample size; we used a larger sample size to proceed further.
Each health facility’s sample size is distributed based on the total population it serves through PMTCT services. A systematic sampling strategy was used to gain access to clients at the ANC and PMTCT units, and proportional allocation was performed to select the study participants from each unit based on the existing maternal records. Facility readiness checkouts, record reviews, and existing interviews were conducted to address the objectives.
Data Collection Procedures and Measurement Tools
A structured and pre-tested questionnaire and a standardized facility readiness assessment checklist were used to collect all necessary information. An exit interview was conducted with the mothers after they received the service. The questionnaire was first prepared in English, translated into a local language, Amharic, and then translated back to English to maintain its consistency.
The list of resources, which evaluated the presence of health personnel, logistics and supplies, waiting areas, reporting forms and registers, PMTCT guidelines, and client education materials, was adapted from national PMTCT guidelines, UNAIDS and Family Health International (FHI) and literature. About 47 indicators were taken from the national guidelines and used to measure the input service quality.28,32–36 A facility inventory was done to make sure that the necessary tools, medicines, and supplies were available.
The process service quality comes in second. To evaluate process quality, 43 process-related indicators are articulated.26,28 A checklist was used for non-participant observation to determine whether the service followed best practices. Fifteen sessions at each facility were conducted during each round of data collection. Additional variables pertinent to the process are obtained from a documented review. About 13 criteria taken from national guidelines were used to evaluate the output quality.26,28,34,35 The confidentiality of patient records was safeguarded, and only authorized parties were contacted. Documents were secured and patient codes were applied.
Regarding mothers’ satisfaction, the correct answers were added to create the overall mother’s satisfaction score. To determine the total degree of satisfaction among the respondents, the responses were classified as “satisfied” or “not satisfied”. To find out how satisfied service users were with PMTCT users, about twelve questionnaires were used. The categories “neutral”, “dissatisfied”, and “very dissatisfied” were created by combining the terms “not satisfied” and “very dissatisfied”.
Observations
In order to evaluate healthcare professionals’ adherence to national PMTCT guidelines, non-participatory direct observations were undertaken. The size of the observation sample was established using the UNAIDS and Ethiopian National Guideline Tool for HIV testing and counseling suggestions.33,35,37 For direct observation, a total of 135 sessions were used. Counseling sessions were observed using a standardized check list from UNAIDS best Practice Collection tools, and facility surveys of all the chosen institutions were evaluated using a minimum requirement for PMTCT program package in accordance with the national PMTCT guideline.
Data Collectors
Two supervisors and three BSc midwives participated in the data gathering process. The supervisors have assumed the role of overseers in order to ensure consistency and reduce errors in data collection. The authors collected the resource inventor and provider-client interaction observations of the data. All supervisors and data collectors participated in two days of intense, uniform training to maintain the highest caliber of the study objectives.
Data Quality Control
To identify any flaws in the planning and structuring of the study instruments, pre-testing of the data collection tools was performed at the Debark hospital using 5% of the total sample size. Debark hospital is located in a nearby community whose residents have characteristics similar to those of Gondar city. After the pre-test, the tools were made clearer, easier to understand, and more effective in gathering the necessary data for the final study.
Analysis and Interpretation of Data
The EPI data program version 4.6 was used to initially code the data before further analysis. Descriptive frequencies, quality ratings, and the regression analyses across all facilities visited by clients were calculated using Statistical Package for the Social Sciences (SPSS) version 26.
Input Dimension
The availability of the people resources, materials, medications, equipment, and supplies required for the delivery of PMTCT services were evaluated using this input dimension.28,38
Process Dimension
This dimension was utilized to show how service providers followed the rules when providing PMTCT service in the maternal and child health department.28,39
Output Dimension
This dimension is used to assess patient satisfaction levels and the overall effectiveness of PMTCT services.39
Quality of the Service
The overall quality: this particular dimension was created by integrating the input, process, and output of three preset quality components.35,36,40
A five-point Likert scale (1-very dissatisfied, 2-dissatisfied, 3- neutral, 4-satisfied, and 5-very satisfied) was used to gauge the women’s degree of satisfaction. Customers who responded ”very satisfied” and ”satisfied” were classified as satisfied customers, while those who responded “neutral”, “dissatisfied”, and “very dissatisfied” were classified as unsatisfied customers. Finally, the satisfied, and dissatisfied answers were coded as 1 and 0, respectively.
Binary, and multiple logistic regressions were used to determine the independent factors that influence satisfaction. A p-value of less than or equal to 0.25 served as the cutoff point for selecting variables for the multiple logistic regression analysis entry in the binary logistic regression. Multiple logistic regression was used to identify independent determinants of maternal satisfaction in Gondar city public health facilities while controlling for confounders. A p-value of less than 0.05 and a 95% confidence interval were used to determine the statistical significance. A logistic regression was constructed using the tolerance, and Variance Inflation Factor (VIF) to investigate multicollinearity among the independent variables. The overall mean of VIF was 1.69. Furthermore, the Hosmer-Lemeshow test was used to assess the overall fitness of the final regression model.
Results
Sociodemographic Related Characteristics of the Study Participants
Interviews with 334 women resulted in a response rate 100%. The respondents’ ages ranged from 15 to 50 years, with a mean age of 29.33 years (± 5.97). Approximately 157 (47%) women achieved secondary or higher educational attainment. Two hundred and seventy-seven women (83%) were urban dwellers, and the others lived in the semi-urban area around the Gondar city administration. About 130 (39%) were housewives and 290 (87%) were married. Similarly, 264 (79%) of the mothers were Orthodox Christian. Moreover, 90 (27%) were primi (first-time) pregnant mothers. Regarding ethnicity, about 263 (79%) of them were belong to the Amhara ethnic group (Table 1).
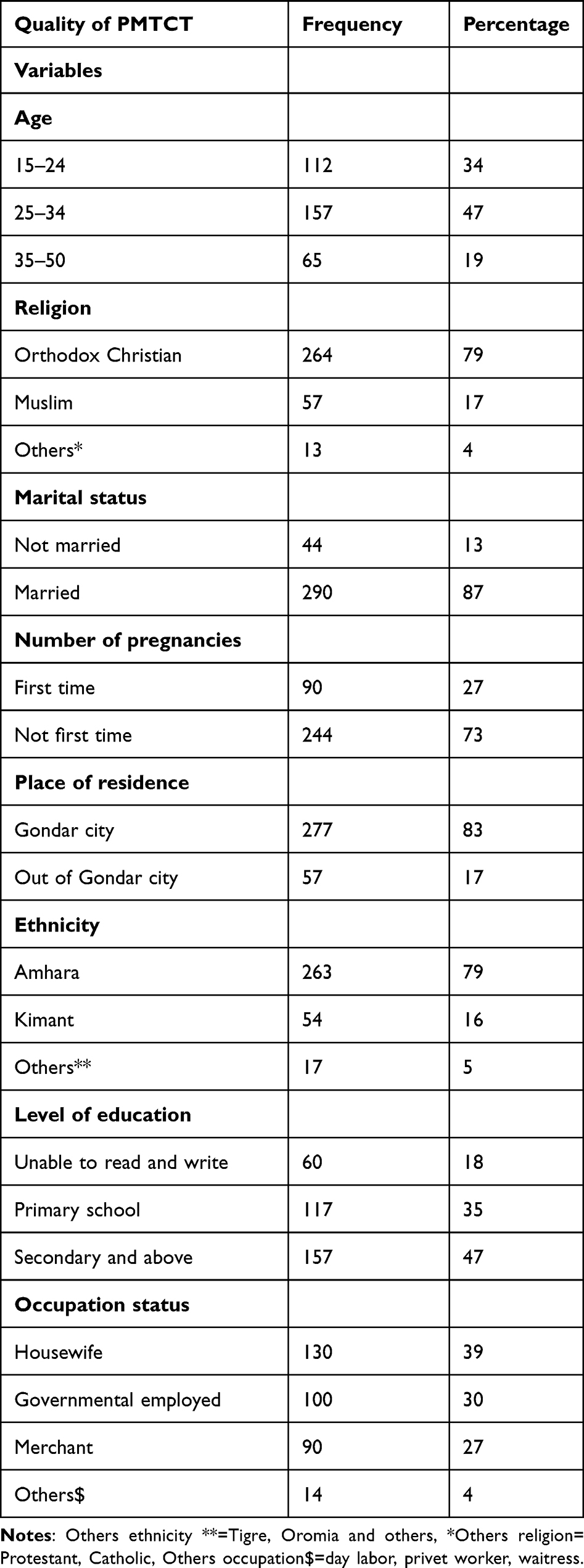 |
Table 1 Socio-Demographic Characteristics of Pregnant Mothers PMTCT Service Users in Gondar City Public Health Facilities, Northwest Ethiopia, 2022 (n=334) |
Level of Quality of PMTCT Services in MCH Units
The Donabedian input-process-output service quality evaluation paradigm was used to evaluate the study. Eight health centers and one hospital made up a total of nine facilities that offered PMTCT as part of the MNCH continuum of treatment in Gondar’s public health facilities. The integration of PMTCT with other maternal and child health service units was disintegrated and unsatisfactory according to national guidelines.
Input Service Quality
Regarding input service quality, the study found that most healthcare facilities had clinical care supplies and medications for PMTCT service provision that must be maintained. All the healthcare facilities had health professionals who were trained to provide PMTCT in accordance with the national guidelines, but waiting and counselling rooms’ cleanliness, ventilation, availability of Dried Blood Spot (DBS) collection kits, and job aid Information, Education, and Communication (IEC) materials had scored almost no more than half. The lack of these items could seriously harm the quality of PMTCT and other maternal and child health services. Therefore, these findings must be highlighted. For the required input service quality, not more than half of the healthcare institutions had DBS test kits, medications for opportunistic infections, and trained service providers available. The overall input service quality was 60.40%, which was low compared to the other two dimensions. In this dimension, about three health facilities (33.34%) achieved the full expected criteria (Table 2).
 |
Table 2 Public Health Facilities Not Fulfilling 100% of Input Service Quality Performance Verification Indicators in Gondar City, Northern Ethiopia, 2022 (n=09) |
Process Service Quality
Process service quality, the second Donabedian dimension, was also evaluated in this study. Among the top indications that received outstanding scores were process indicators such as conducting physical examination, conducting physical history collection, and reviewing ARV treatment adherence for HIV-positive patients. Only 22.2% of the health facilities welcomed women when they arrived, which had an impact on poor service. Similar screenings for cervical cancer and psychological support only received a score of (44.45%), screenings for substance addiction only received a score of (33.34%), and the opening hours of health facilities were among the top indicators that had received poor scores and had an impact on the level of service. Service consultations revealed that excessive waiting times are another problem. It was discovered that the majority of healthcare institutions’ health service providers were seen as not adhering to service standards while providing service consultation. The overall process dimension score across all health facilities was 72.97%, indicating good performance (Table 3).
 |
Table 3 Public Health Facilities Not Fulfilling 90% of Process Service Quality Performance Verification Indicators in Gondar City, Northern Ethiopia, 2022 (n=09) |
Output Service Quality, and Client Satisfaction
This dimension has scored a higher quality level (88.89%) than the input and process service quality dimensions, which are judged to be very good achievements. In this dimension, about 5 health facilities (55.56%) fulfilled the required criteria, which is better than the other dimensions (Tables 4–6). Regarding the overall quality performance, the quality of health facilities’ performance was 74.09% based on the three quality components. The output quality was better and judged as good at 88.89%. However, input and process service quality revealed 60.40% and 72.97%, respectively, across health facilities.
 |
Table 4 Public Health Facilities Not Fulfilling 90% of Output Service Quality Performance Verification Indicators in Gondar City, Northern Ethiopia, 2022 (n=09) |
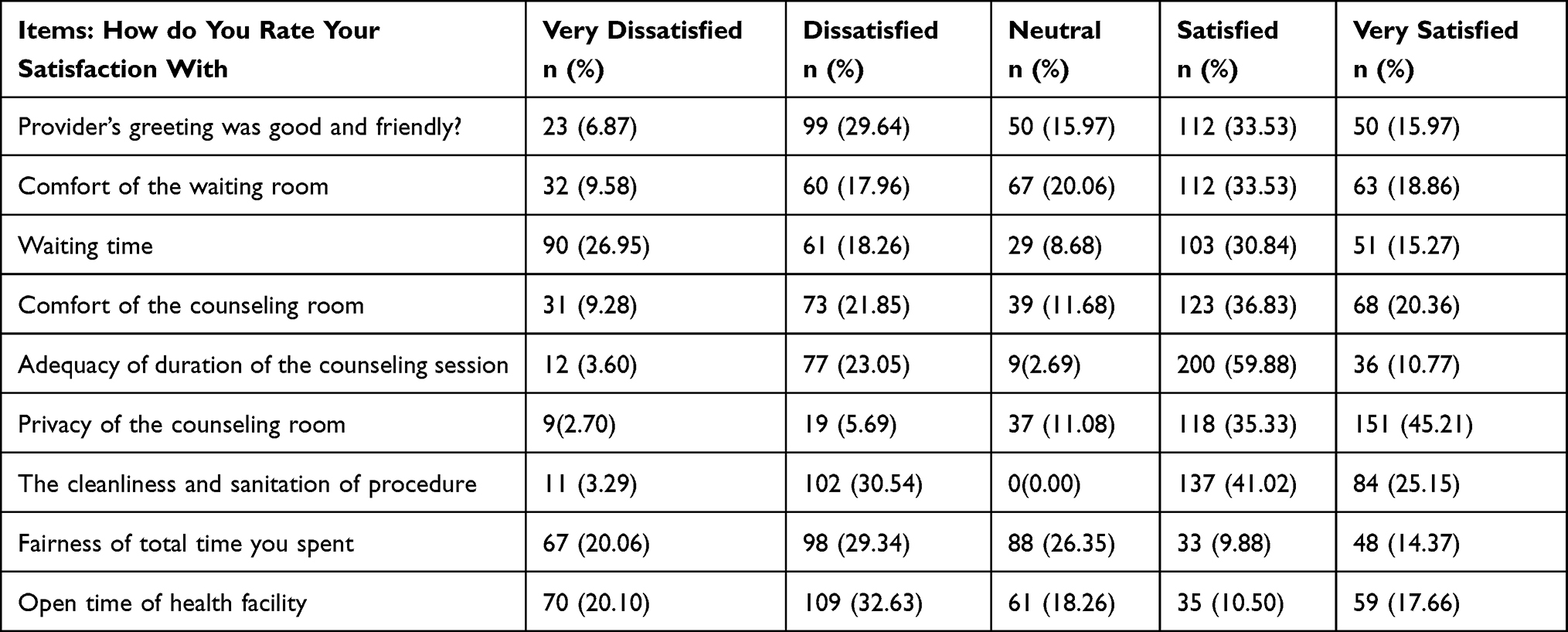 |
Table 5 Client Satisfaction with the Comfort and Privacy of Counseling Room, and Adequacy of Counseling Session; Quality of PMTCT Services in Public Health Facilities in Gondar City, Northwest, Ethiopia 2022 (n=334) |
 |
Table 6 Client Satisfaction by Counselor’s Characteristics and Availability of Services, Quality of PMTCT Services in Public Health Facilities in Gondar City, Northwest, Ethiopia 2022 (n=334) |
A total of 135 PMTCT service-related observations during the provider and client’s interaction were observed across all health facilities. To prevent the effect of Hawthorne, the first and the last three (six in total) observations were excluded from the analysis. The details are given in Table 7.
 |
Table 7 Direct Observation of HCT Quality of PMTCT Services in Public Health Facilities in Gondar City, Northwest, Ethiopia 2022 (n=135) |
Health Care Providers Adherence
To explore the adherence of health professionals from each health facilities about 135 sessions of PMTCT services was observed (Table 8).
 |
Table 8 Direct Observation Result of Adherence Support Session of PMTCT Services in Public Health Facilities in Gondar City, Northwest, Ethiopia 2022 (n=135) |
Factors Associated with Women’s Satisfaction in PMTCT Service in Gondar City Public Health Facilities
About eleven variables were included in the multivariable binary logistic regression analysis to find characteristics substantially linked with women’s satisfaction with PMTCT service in Gondar city after correcting for potential confounders during this study. Age, educational level, waiting time, sufficiency of counseling time, arrival time, and clinic opening hour were found to be substantially associated with women’s satisfaction with PMTCT in Gondar city after multivariable analysis.
The odds of satisfaction in PMTCT among women aged 15–24 years were reduced by 69% (AOR = 0.31, 95% CI: 0.06–0.79) compared to women aged 35–50 years. When compared to women who were unable to read and write, the odds of satisfaction in PMTCT for pregnant women who have an educational status of secondary and above were reduced by 41% (AOR = 0.59, 95% CI: 0.35, 0.67). Moreover, regarding time of arrival, when compared to women who arrived within an hour and more before the service being commenced, the odds of PMTCT dissatisfaction were reduced by 29% for women who arrived within 30 minutes (AOR = 0.71, 955 CI: 0.55, 0.93). The odds of satisfaction in PMTCT among women having more than 30 minutes of waiting time were reduced by 77% (AOR = 0.23; 95% CI: 0.11, 0.37), taking women having waiting times of less than 30 minutes as a reference. In addition, the odds of satisfaction in PMTCT among women who had adequate counseling were 2.83 times higher (AOR = 2.83; 95% CI: 1.72; 3.97) compared to women who had inadequate counseling time. Furthermore, for women who had convenient opening hours at the clinic, the odds of satisfaction in PMTCT were 4.27 times higher (AOR = 4.27, 95% CI: 2.09, 6.67) compared to women who had no convenient opening hours (Table 9). In addition, the odds of satisfaction in PMTCT among women who had adequate counseling were 2.83 times higher (AOR = 2.83; 95% CI: 1.72; 3.97) compared to women who had inadequate counseling time. Furthermore, for women who had convenient opening hours at the clinic, the odds of satisfaction in PMTCT were 4.27 times higher (AOR = 4.27, 95% CI: 2.09, 6.67) compared to women who had no convenient opening hours (Table 9).
 |
Table 9 Binary and Multiple Logistic Regression Analysis of Associated Variables with Overall Satisfaction of Pregnant Women Attending in Gondar City Public Health Facilities Northwest Ethiopia 2022 |
Discussion
This cross-sectional study reports the quality of PMTCT services and determinants of women’s satisfaction with PMTCT services among 334 women at ANC and PMTCT units in Gondar city public health facilities.
The evaluation was carried out in accordance with the Donabedian model’s three quality criteria and in accordance with Ethiopia’s national standards for PMTCT service provision.33,35,41,42 Accordingly, considering the overall Donabedian input-process and output service dimensions across all health institutions, the study’s findings indicated that the overall level of service quality for PMTCT was determined to be good (74.09%). It’s crucial to remember that the three quality components are interconnected, and each one’s impact can be seen in the other two.43 Based on data from the national aim set for 2020, this finding was far from being the case.44
Our study showed that about 214 (67.08%, 95% CI: 64.97, 69.31) of pregnant women were satisfied with the PMTCT services offered by the health facilities in Gondar city. This finding is lower than the previous studies in Ethiopia: Adama town, Hadiya zone, Dire Dawa, and Addis Ababa, with satisfaction of 74.7%,32 80%,26 82.2%45 and 89.8%,46 respectively. The study period could be a possible reason for this discrepancy in level of satisfaction with PMTCT services. The more recent the study, the more women expect to get better PMTCT services due to increased awareness about quality services, and this may cause women to be less satisfied with routine services. On the other side, this disparity could be significantly attributed to the study’s techniques and selection of participants.
In this study, women’s age, educational status, waiting time, adequate counseling time, time of arrival, and opening hours of health facilities were the factors significantly associated with women’s satisfaction with PMTCT services in the multiple logistic regression analysis.
This study showed that the odds of satisfaction with PMTCT service among women aged 15–24 years were 69% lower than those of women aged 35–50 years. This could be associated with young women having low ANC and ART utilization coverage. Hence, it is implied that there is a higher risk of MTCT and low awareness of the benefits of PMTCT service among these segment of the population.47 Studies have shown that younger women are often less satisfied with the attitude of healthcare workers, waiting time, and the cost of services compared to older women.48 Additionally, maternal age has been found to impact satisfaction at each stage of pregnancy, childbirth, and the postpartum period.49 Furthermore, factors such as the provision of care, clinical characteristics, and the overall experience of care can influence women’s satisfaction with maternal health services.50,51 It is also important to consider the prevalence of mistreatment or discrimination during pregnancy and delivery, as these experiences can contribute to lower satisfaction among younger women. Therefore, policymakers should focus on improving the attitude of healthcare workers, reducing waiting times, addressing the cost of services, and ensuring that all women receive respectful and high-quality care to enhance the satisfaction of younger women with maternal and child health services.
Furthermore, the odds of satisfaction with PMTCT services among women who attended secondary education and above were lower than by 41% compared to women who attended no formal education. Previous studies have reported the same conclusion.45,52 It may be a plausible reason that educated women were better aware of PMTCT-related information or that those with higher levels of education were not as satisfied as those with lower levels of education due to higher service expectations.53 Additionally, educated women might mistakenly believe that they are more knowledgeable and less vulnerable to infection, which would prevent them from actively participating in counseling sessions.45
Our study demonstrated that women who arrived more than an hour earlier had 2.13 times higher odds of being satisfied with the PMTCT services than those who arrived within a half-hour. This could probably because the mother who came early did not receive the health service treatment, she sought at two o’clock after her arrival, so her chances of being satisfied with the service were slim. These studies54 show that the long waiting time of mothers at the PMTCT unit leads to lower levels of service satisfaction.
The waiting time for ANC and PMTCT counseling services was a significant factor in women’s satisfaction with PMTCT services. Women who were waiting longer than half an hour had lower odds of being satisfied with PMTCT services compared to women who waited for less than half an hour. Similar findings were reported in previous studies.45,55–58 Spending additional time to obtain PMTCT services could easily result in dissatisfaction because it may result in an additional loss of income related to timing. It could also be associated with the presence of other urgent problems that the clients need to attend to. Moreover, other contributing factors could have an effect on low client satisfaction, like the fact that the clinics may not settle as clients obtain PMTCT services in an effort to reduce waiting times.59 Short waiting times in antenatal clinics have been found to be more acceptable to pregnant women, making maternal health services more efficient and preventing dissatisfaction.60 Additionally, a study conducted in Ethiopia found that wait time was significantly associated with maternal satisfaction with childbirth services.61 Therefore, policymakers should consider reducing waiting times in health facilities to improve maternal satisfaction with maternal and child health services.
Moreover, providing adequate counseling was significantly associated with women’s satisfaction in PMTCT services.26,46,58 The odds of satisfaction with PMTCT services among women who had adequate counseling were nearly three times higher compared to women who had inadequate counseling time. This may be due to the fact that women who get adequate counseling become more aware of the benefits of PMTCT service utilization and are more satisfied with the services. Several studies have indicated that counseling can significantly improve mothers’ satisfaction with overall maternal functioning.62,63 Prenatal counseling has been identified as a major determinant of satisfaction, as it is critical for a woman’s understanding of her health condition and her overall satisfaction with maternal health care.64 Additionally, individual counseling by healthcare providers during pregnancy has been linked to positive attitudes toward childbirth and informed decision-making, which can contribute to higher satisfaction among mothers.65 Therefore, providing adequate counseling, tailored to the individual needs of women, can play a crucial role in enhancing maternal satisfaction with maternal and child health services.
In addition to counseling time, the opening hours of the health facility were significantly associated with women’s satisfaction in PMTCT.54 For women who had no convenient opening hours at the clinic, the odds of satisfaction with PMTCT were 4.27 times lower as compared to women who had convenient opening hours. Other similar findings were reported from England.66 This could be because the health facilities with convenient opening hours of the PMTCT unit provide timely service for the women, and this could make women more satisfied with the PMTCT they get. Due to the fact that facility-based research yields more favorable patient answers, there may be a social desirability bias. This could lead to a “halo effect” that is only temporary and causes patients to feel satisfied more right away than they do afterwards.
Conclusions
This study indicates the quality of PMTCT service provision was low compared to the national guideline expectation by using the Donabedian structure-process-outcome quality dimensions. More than two-thirds of women were satisfied with PMTCT services in public health facilities in Gondar city. The satisfaction level in this study was also low in comparison to previous studies in other parts of Ethiopia. The women’s age, educational status, waiting time, counseling time adequacy, time of arrival, and opening hours of health facilities should be taken into consideration during the provision of PMTCT services in public health facilities to better satisfy women’s needs for the services. Recognizing the diversity among women accessing PMTCT services, healthcare providers, and facilities can adopt a more individualized and patient-centered approach. This involves considering the women’s age and educational status to provide information and counseling that is appropriate, comprehensible, and culturally sensitive to their specific needs and circumstances, work on optimizing their processes to minimize waiting times for women seeking PMTCT services, allocating sufficient time for counseling sessions, extending their opening hours to accommodate women who may face challenges accessing services during regular working hours, implementing efficient appointment systems, and continuous quality improvement. Furthermore, focusing on the availability of resources (counseling room cleanliness, ventilation, illumination), HIV/AIDS-related inputs, training, and other referral systems, and integrating the PMTCT service with other maternal and child health service units, is mandatory. Continuous training in gender-sensitive and client-centered care is imperative for healthcare personnel to guarantee they possess the skills and information required to effectively manage the distinct requirements of women who avail PMTCT treatments. Topics such cultural competency, effective communication, and the significance of taking socioeconomic determinants of health into account should all be included in this training.
Data Sharing Statement
Most data and materials are included in the manuscript. Additional data can be accessed from the correspondence author with a reasonable request.
Ethical Approval and Consent to Participate
The School of Nursing’s ethical review committee provided ethical review on behalf of the University of Gondar College of Medicine and Health Sciences with Reg. No. SoN/CHNU/72/06/22. The healthcare facilities were addressed in a formal letter of collaboration. The participants in the study also gave their written informed consent agreement after being fully informed about the study objective. Because of the nature or noninvasive of the research, only written informed consent was collected from each participant after they had received services from the department’s maternity and child health services to find out how they felt about the services. The written informed consent form was ordered by the IRB ethical letter. Participants were informed that any information they provided would remain confidential and that their names would not be mentioned. Participants’ identity and privacy were protected, and confidentiality was ensured by removing their names from the informed consent form. Moreover, based on the IRB ethical letter order, participants under 18 years of age were approved to provide informed consent on their own behalf. All the methods and materials in this study have been regulated based on the Declaration of Helsinki.
Author Contributions
The research’s conception, study design, execution, data collection, analysis, and interpretation, as well as its drafting, revision, and critical review, were all completed by the authors. They also decided which journal the article should be submitted to. Every author is also aware of every version of the article. In addition, the authors committed to accepting accountability and responsibility for the article’s content. The authors chose the journal to submit the work to and approved the final draft of the manuscript.
Funding
This study was not supported financially by anyone.
Disclosure
The authors declare that they have no competing interests.
References
1. World Health Organization. Global Health Sector Strategy on HIV 2016–2021. Towards Ending AIDS. World Health Organization; 2016.
2. Ababa A Competency Based National Comprehensive PMTCT/MNCH Training Participant’s Manual. 2017.
3. Trivedi S, Kariya P, Shah V, Mody S, Patel P, Desai K. Does maternal HIV status affect infant growth?: a hospital based follow up study. National J Med Res. 2012;2(04):512–517.
4. Ethiopia FMo H National consolidated guidelines for comprehensive HIV prevention, care and treatment. Federal Ministry of Health Addis Ababa, Ethiopia; 2018.
5. Farhoudi B, Ghalekhani N, Afsar Kazerooni P, et al. Cascade of care in people living with HIV in Iran in 2019; how far to reach UNAIDS/WHO targets. AIDS Care. 2022;34(5):590–596. doi:10.1080/09540121.2021.1944603
6. UNAIDS W. Global AIDS Monitoring. Geneva: UNAIDS; 2017.
7. World Health Organization. Fact Sheets on Quality Health Services. World Health Organization; 2020.
8. Albritton E, Edmunds M, Thomas V, et al. Engaging Stakeholders to Improve the Quality of Children’s Health Care. Agency Healthcare Res Qual. 2014;1:1.
9. Cottrell E, Whitlock E, Kato E, et al. Defining the benefits of stakeholder engagement in systematic reviews. Comparat Effect Res. 2014;1:13–19.
10. Halbesleben JR, Whitman MV. Evaluating survey quality in health services research: a decision framework for assessing nonresponse bias. Health Serv Res. 2013;48(3):913–930. doi:10.1111/1475-6773.12002
11. Plsek P. Institute of Medicine. Crossing the Quality Chasm: A New Health System for the 21st Century. Washington, DC: National Academies Pr; 2001.
12. Hagaman AK, Singh K, Abate M, et al. The impacts of quality improvement on maternal and newborn health: preliminary findings from a health system integrated intervention in four Ethiopian regions. BMC Health Serv Res. 2020;20(1):1–12. doi:10.1186/s12913-020-05391-3
13. Health EFMo. HEALTH & HEALTH-RELATED I N D I C A T O R S; 2020/2021. Available from: https://www.moh.gov.et/site/sites/default/files/2021-10/Health%20and%20health%20related%20indicators%20_2013%20EFY.pdf.
14. Ethiopian Federal Democratic Republic, Ministry of Health. Ethiopian National Health Care Quality Strategy: Transforming the Quality of Health Care in Ethiopia, 2016-2020. Available from: http://repository.iifphc.org/handle/123456789/737.
15. Magadi MA. Understanding the gender disparity in HIV infection across countries in sub‐Saharan Africa: evidence from the Demographic and Health Surveys. Sociol Health Illness. 2011;33(4):522–539. doi:10.1111/j.1467-9566.2010.01304.x
16. Yah CS, Tambo E. Why is mother to child transmission (MTCT) of HIV a continual threat to new-borns in sub-Saharan Africa (SSA). J Infect Public Health. 2019;12(2):213–223. doi:10.1016/j.jiph.2018.10.008
17. Goga AE, Dinh T-H, Essajee S, et al. What will it take for the Global Plan priority countries in Sub-Saharan Africa to eliminate mother-to-child transmission of HIV? BMC Infect Dis. 2019;19(1):1–13. doi:10.1186/s12879-019-4393-5
18. Goga A, Singh Y, Jackson D, et al. How are countries in sub-Saharan African monitoring the impact of programmes to prevent vertical transmission of HIV? BMJ. 2019;364:2.
19. Mutabazi JC, Zarowsky C, Trottier H. The impact of programs for prevention of mother-to-child transmission of HIV on health care services and systems in sub-Saharan Africa-A review. Public Health Rev. 2017;38(1):1–27. doi:10.1186/s40985-017-0072-5
20. Teshome GS, Modiba LM. Strategies to Eliminate Mother-to-Child Transmission of HIV in Addis Ababa, Ethiopia (Qualitative Study). HIV/AIDS Res Palliative Cares. 2020;12:821. doi:10.2147/HIV.S277461
21. Hampanda K. Vertical transmission of HIV in Sub-Saharan Africa: applying theoretical frameworks to understand social barriers to PMTCT. Int Scholarly Res Notices. 2013;2013:3.
22. World Health Organization. WHO Validation for the Elimination of Mother-to-Child Transmission of HIV and/or Syphilis Geneva. World Health Organization; 2020.
23. UNODC U INPUD, UNAIDS UNICEF, WHO. Addressing the specific needs of women who use drugs - prevention of mother-to-child transmission of HIV, Hepatitis B and C and Syphilis; 2021.
24. Bintabara D, Lilungulu A, Jumanne S, Nassoro MM, Mpondo BC. Does facility readiness promote high-quality of provider-initiated HIV testing and counseling to pregnant women? A national survey for improving policy of prevention of mother-to-child transmission of HIV in Tanzania. AIDS Res Ther. 2021;18(1):1–11. doi:10.1186/s12981-021-00362-y
25. Adedimeji A, Abboud N, Merdekios B, Shiferaw M. A qualitative study of barriers to effectiveness of interventions to prevent mother-to-child transmission of HIV in Arba Minch, Ethiopia. Int J Popul Res. 2012;2012:1–7. doi:10.1155/2012/532154
26. Bachore B, Tafese F, Gebissa F, Mekango D. Quality of prevention of mother to child transmission (PMTCT) of HIV services in public hospitals of Hadiya Zone, Southern Ethiopia. Health Syst Policy Res. 2018;5(2):73. doi:10.21767/2254-9137.100092
27. Terefe B, Kebede A, Amare Muche G. Process evaluation of prevention of mother-to-child transmission of HIV service at Gondar City administration governmental health facilities, Northwest Ethiopia: a mixed approach case study evaluation design. HIV/AIDS-Res Palliative Care. 2021;Volume 13:1127–1147. doi:10.2147/HIV.S340103
28. Ajemu KF, Desta A. Level of quality of option B+ PMTCT service provision in public health facilities in Mekelle zone, northern Ethiopia: cross-sectional study. BMC Health Serv Res. 2020;20(1):1–10. doi:10.1186/s12913-020-05429-6
29. Goshiye D, Sebsebie G, Gedamu S. Quality of prevention of mother-to-child Transmis-sion of HIV service at South Wollo Zone Governmental Hospitals, Amhara Region, Ethiopia, 2018. Int J Pediatr Res. 2019;5:057.
30. Dussault G, Dubois C-A. Human resources for health policies: a critical component in health policies. Hum Res Health. 2003;1(1):1–16. doi:10.1186/1478-4491-1-1
31. Bintabara D, Nakamura K, Seino K. Determinants of facility readiness for integration of family planning with HIV testing and counseling services: evidence from the Tanzania service provision assessment survey, 2014–2015. BMC Health Serv Res. 2017;17(1):1–11. doi:10.1186/s12913-017-2809-8
32. Asefa A, Mitike G. Prevention of mother-to-child transmission (PMTCT) of HIV services in Adama town, Ethiopia: clients’ satisfaction and challenges experienced by service providers. BMC Pregnancy Childbirth. 2014;14(1):1–7. doi:10.1186/1471-2393-14-57
33. UNAIDS W. Technical Guidance Note for Global Fund HIV Proposals Prevention of Mother-to-Child Transmission of HIV. WHO/UNAIDS Global-Plan-Elimination-HIV-Children; 2011.
34. Abeba A. Federal HIV/AIDS Prevention and Control Office. Federal Ministry of Health; 2007.
35. Ethiopia F. National Consolidated Guidelines for Comprehensive HIV Prevention, Care and Treatment. Addis Ababa: Fmoh; 2018:1–238.
36. Baggaley R. Tools for Evaluating HIV Voluntary Counselling and Testing. UNAIDS; 2000.
37. HEALTH FDROEMO. NATIONAL COMPREHENSIVE AND INTEGRATED PREVENTION OF MOTHER-TO-CHILD TRANSMISSION OF HIV GUIDELINE; 2017. Available from: https://platform.who.int/docs/default-source/mca-documents/policy-documents/guideline/ETH-RH-43-04-GUIDELINE-2017-eng-PMTCT-HIV-National-Guideline.pdf.
38. Abaynew Y. Quality of prevention of mother to child transmission (PMTCT) services in Dessie referral hospital, Dessie city administration, Ethiopia: client perspective. Neonatal Pediatric Med. 2016;3:123.
39. Bayou NB. Quality of PMTCT services in gebretsadiq shawo memorial hospital, Kafa Zone, South West Ethiopia: a descriptive study. Open Access Lib J. 2015;2(05):1.
40. Fisseha G, Berhane Y, Worku A, Terefe W. Quality of the delivery services in health facilities in Northern Ethiopia. BMC Health Serv Res. 2017;17(1):1–7. doi:10.1186/s12913-017-2125-3
41. Federal H. AIDS Preventi on and Control Office Federal Ministry of Health. In: Guidelines for Prevention of Mother-to-Child Transmission of HIV in Ethiopia. Addis Ababa: Federal Ministry of Health; 2007.
42. Federal H. AIDS prevention and control office federal ministry of health. In: Guidelines for Management of Opportunistic Infections and Antiretroviral Treatment in Adolescents and Adults in Ethiopia 2007. Federal Ministry of Health; 2017.
43. Donabedian A. The quality of care: how can it be assessed? JAMA. 1988;260(12):1743–1748. doi:10.1001/jama.1988.03410120089033
44. FMOH E. Health Sector Transformation Plan (HSTP): 2015/16-− 2019/20. Addis Ababa. 2015.
45. Abayneh K, Mengistie B, Oljira L, Tiruye G. Clients’ satisfaction with services for prevention of mother-to-child transmission of HIV in public health facilities in Diredawa City, Eastern Ethiopia. HIV/AIDS Res Palliative Care. 2020;Volume 12:611–620. doi:10.2147/HIV.S264854
46. Ismail H, Ali A. Pregnant women’s satisfaction and comprehension level of information given during HIV Counseling and Testing for PMTCT in public health facilities in Addis Ababa. Ethiop J Health Dev. 2011;25(2):126–134.
47. Burrage AB, Mushavi A, Shiraishi RW, et al. Mother-to-child transmission of HIV in adolescents and young women: findings from a national prospective cohort survey, Zimbabwe, 2013–2014. J Adolesc Health. 2020;66(4):455–463. doi:10.1016/j.jadohealth.2019.10.023
48. Emelumadu OF, Onyeonoro UU, Ukegbu AU, Ezeama NN, Ifeadike CO, Okezie OK. Perception of quality of maternal healthcare services among women utilising antenatal services in selected primary health facilities in Anambra State, Southeast Nigeria. Niger Med J. 2014;55(2):148. doi:10.4103/0300-1652.129653
49. Molina-García L, Hidalgo-Ruiz M, Gálvez-Toro A, Aguilar-Puerta SC, Delgado-Rodríguez M, Martínez-Galiano JM. The Age at Which a Woman Becomes a Mother and Her Satisfaction with the Process of Pregnancy. In: Childbirth and the Puerperium. Healthcare. MDPI; 2020.
50. Lazzerini M, Mariani I, Semenzato C, Valente EP. Association between maternal satisfaction and other indicators of quality of care at childbirth: a cross-sectional study based on the WHO standards. BMJ open. 2020;10(9):e037063. doi:10.1136/bmjopen-2020-037063
51. Sehngelia L, Pavlova M, Groot W. Women’s satisfaction with maternal care services in Georgia. Health Policy Open. 2021;2:100028. doi:10.1016/j.hpopen.2020.100028
52. Lyatuu M, Msamanga G, Kalinga A. Clients’ satisfaction with services for prevention of mother-to-child transmission of HIV in Dodoma Rural district. East Af J Public Health. 2008;5(3):174–179. doi:10.4314/eajph.v5i3.38999
53. Ashipa T, Ighedosa S. Assessment of clients’ satisfaction with the PMTCT counselling service in Benin city, Edo state, Nigeria. J Med Biomed Res. 2013;12(2):150–165.
54. Eshetie G, Feleke A, Genetu M. Patient satisfaction and associated factors among outpatient health service users at primary hospitals of North Gondar, Northwest Ethiopia, 2016. Adv Public Health. 2020;2020:1–8. doi:10.1155/2020/6102938
55. Augustino T Evaluation of clients’ satisfaction with waiting time and privacy for PMTCT services in Kinondoni Municipal Council. 2015.
56. Mezemir R, Getachew D, Gebreslassie M. Patients’ satisfaction and its determinants in outpatient Department of Deberebirhan Referral Hospital, north Shoa, Ethiopia. Int J Econ Manag Sci. 2014;3(191):2. doi:10.4172/2162-6359.1000191
57. Anand D, Kaushal S, Gupta S. A study on status of client satisfaction in patients attending government health facilities in Agra District. Indian J Commu Health. 2012;24(3):209–214.
58. Alarcon-Ruiz CA, Heredia P, Taype-Rondan A. Association of waiting and consultation time with patient satisfaction: secondary-data analysis of a national survey in Peruvian ambulatory care facilities. BMC Health Serv Res. 2019;19(1):1–9. doi:10.1186/s12913-019-4288-6
59. Sam M, Manu E, Anaman-Torgbor J, Tarkang EE Client satisfaction with quality of prevention of mother-to-child transmission (PMTCT) of HIV services in the oti region of Ghana: a facility-based cross-sectional study. 2021.
60. Abdus-Salam R, Adeniyi A, Bello F. Antenatal clinic waiting time, patient satisfaction, and preference for staggered appointment–a cross-sectional study. J Patient Exper. 2021;8:23743735211060802. doi:10.1177/23743735211060802
61. Tadele M, Bikila D, Fite RO, Obsa MS. Maternal satisfaction towards childbirth service in public health facilities at Adama town, Ethiopia. Reproductive Health. 2020;17(1):1–8. doi:10.1186/s12978-020-00911-0
62. Esmkhani M, Ahmadi L, Maleki A. The effect of client needs counseling on the postpartum quality of life of women. J Perinatal Educ. 2020;29(2):95–102. doi:10.1891/J-PE-D-18-00044
63. Chamgurdani FK, Barkin JL, Esmaeilpour K, Malakouti J, Buoli M, Mirghafourvand M. The effect of counseling with a skills training approach on maternal functioning: a randomized controlled clinical trial. BMC Women’s Health. 2020;20(1):1–10. doi:10.1186/s12905-020-00914-w
64. Srivastava A, Avan BI, Rajbangshi P, Bhattacharyya S. Determinants of women’s satisfaction with maternal health care: a review of literature from developing countries. BMC Pregnancy Childbirth. 2015;15(1):1–12. doi:10.1186/s12884-015-0525-0
65. Andaroon N, Kordi M, Kimiaee SA, Esmaeili H. The effect of individual counseling on attitudes and decisional conflict in the choice of delivery among nulliparous women. J Educ Health Promot. 2020;9. doi:10.4103/jehp.jehp_472_18
66. Cowling TE, Majeed A, Harris MJ. Importance of accessibility and opening hours to overall patient experience of general practice: analysis of repeated cross-sectional data from a national patient survey. Br J Gen Pract. 2018;68(672):e469–e77. doi:10.3399/bjgp18X697673
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.