")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Experiences of Participation in a Multimodal Preventive Trial MIND-ADMINI Among Persons with Prodromal Alzheimer’s Disease: A Qualitative Study
Authors Akenine U, Thunborg C, Kivipelto M, Fallahpour M
Received 3 November 2021
Accepted for publication 10 December 2021
Published 29 January 2022 Volume 2022:15 Pages 219—234
DOI https://doi.org/10.2147/JMDH.S345607
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ulrika Akenine,1 Charlotta Thunborg,1,2 Miia Kivipelto,1– 4 Mandana Fallahpour1,5
1Department of Neurobiology, Care Sciences and Society, Division of Clinical Geriatrics, Karolinska Institutet, Stockholm, Sweden; 2School of Health, Care and Social Welfare, Department of Physiotherapy, Mälardalen University, Västerås, Sweden; 3Institute of Public Health and Clinical Nutrition, University of Eastern Finland, Kuopio, Finland; 4Stockholms Sjukhem, Research & Development Unit, Stockholm, Sweden; 5Department of Neurobiology, Care Sciences and Society, Division of Occupational Therapy, Karolinska Institutet, Stockholm, Sweden
Correspondence: Ulrika Akenine
Karolinska Institutet, Department of Neurobiology, Care Sciences and Society, Division of Clinical Geriatrics, Karolinska vägen 37A, QA32, SE-171 64, Solna, Stockholm, Sweden
Tel +46 70 667 99 67
Email [email protected]
Mandana Fallahpour
Karolinska Institutet, Department of Neurobiology, Care Sciences and Society, Division of Occupational Therapy, Alfred Nobels Allé 23, SE-141 83 Huddinge, Stockholm, Sweden
Tel +46 8 524 838 56
Email [email protected]
Introduction: Alzheimer’s disease (AD) is one of the world’s leading public health challenges. One-third of AD cases are attributable to modifiable vascular and lifestyle-related risk factors. The Multimodal Preventive Trial for Alzheimer’s Disease, MIND-ADMINI a 6-month multinational parallel-group randomized controlled trial (RCT), targeted persons with prodromal AD and built on the positive outcomes from the Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER) trial. The intervention consisted of four main components of (i) physical exercise training program, (ii) nutrition guidance, (iii) cognitive training, and (iv) social stimulation, as well as (iv) monitoring of metabolic/vascular risk factors.
Aim: The study aimed to explore and describe the experiences of participation in MIND-ADMINI among persons with prodromal AD.
Methods: This qualitative study was part of the larger MIND-ADMINI project. Eight participants were interviewed twice, before and after the intervention. The data was analyzed using qualitative content analysis.
Results: The results are presented as categories of (i) knowledge of AD and prevention, (ii) motives for study participation, (iii) experiences of the received information about the study, (iv) taking the decision to participate, (v) expectations on study participation, (vi) experiences of study participation and (vii) internal and external factors influencing study participation.
Conclusion: The MIND-ADMINI was well-tolerated by the participants. At the beginning of the study, the number of tasks and visits was perceived as burdensome but was later well-tolerated. The participant’ knowledge about AD and prevention increased during the trial. Their motives for participating in MIND-ADMINI were described as both altruistic and self-beneficial. Health benefits from the study components, access to specialized medical care were identified as benefits. Managing the intensive flow of information was described a major challenge. The participants’ needs for personalized support during the trial stress the importance of applying a person-centered approach providing the preventive trials.
Keywords: Alzheimer’s disease, multimodal prevention, participation, qualitative method
Introduction
Alzheimer’s disease (AD) is a progressive neurodegenerative disorder with cognitive dysfunctions (including deficits in short-term memory, executive and visuospatial dysfunction, and praxis), functional deficits and behavioral disturbances.1 AD is one of the world’s leading public health challenges.2 There is no curative treatment for AD, although a few symptomatic therapies (ie, cholinesterase inhibitors and memantine) are approved.3 Estimates show that a third of AD cases are attributable to modifiable vascular and lifestyle-related risk factors such as physical inactivity, smoking, obesity, low education, depression, diabetes mellitus and hypertension.4 Prevention of cognitive impairment has been identified as a global public health priority by the World Health Organization (WHO).2 Prevention has received increasing attention due to its focus on risk reduction through lifestyle management.5 Several randomized controlled trials (RCTs) targeting multiple risk factors simultaneously applying multimodal preventive interventions have been conducted among older adults in which results pointed to the promising direction.6–9 The 2-year Finnish Geriatric Intervention Study to Prevent Cognitive Impairment and Disability (FINGER) applied physical activity, dietary counseling, cognitive and social stimulation, and management of vascular and metabolic risk factors. It was the first study to demonstrate that simultaneously targeting multiple risk factors are effective for preventing neurocognitive disorders among older adults from the general population, who had an increased risk of dementia.6
Studies have shown that the first decline in cognitive performance may appear as early as 12 years before dementia, in measures of semantic memory and conceptual formation.10 The prodromal AD, defined as a pre-dementia stage, is characterized clinically as mild cognitive impairment (MCI).11 Persons with prodromal AD are mostly cognitively intact, with biomarker evidence of brain amyloid deposition representing a group at high risk for cognitive decline and dementia.12 This in turn means a particularly long and progressive prodromal phase of AD, without available treatment, making these patients an ideal population for trials aimed at delaying the emergence of the clinical syndromes of MCI and dementia.13,14
The Multimodal Preventive Trial for Alzheimer’s Disease (MIND-ADMINI) (ClinicalTrials.gov NCT03249688) built on the positive outcomes from the FINGER trial addressing multiple risk factors simultaneously to target persons with prodromal AD. More information about the development of MIND-ADMINI and protocol of the interventional program based on the modifiable risk factors is found elsewhere.15 The MIND-ADMINI was a 6-month multinational parallel-group randomized controlled trial (RCT). The intervention was a feasibility trial and consisted of the following four main components: (i) physical exercise training program, (ii) nutrition guidance, (iii) cognitive training, and (iv) social simulation, as well as (iv) monitoring of metabolic/vascular risk factors.The objectives for MIND-ADMINI, were to evaluate the feasibility of an adapted FINGER-based multimodal lifestyle intervention among individuals with prodromal AD. Primary outcomes were feasibility and safety and secondary outcomes were adherence to the interventions and lifestyle changes. Trials in general are becoming larger and increasingly complex, incorporating multimodal research designs, adaptive designs, and complicated assortments and randomization.16 Furthermore, individuals’ decisions regarding participation in trials may be influenced by different factors such as the received information facilitating or hindering their participation.17 A better understanding of the individuals’ motives for participating in AD research and their opinions of trial information and the consent process may lead to changes that facilitate recruitment in preventive trials and improve their satisfaction with the recruitment process.18 Previous research found altruism and hope for personal benefits as the most common motives for participating in research trials for persons with AD.19 On the other hand, participation in lifestyle prevention trials is demanding due to the required interest, efforts and engagement by the participants for the duration of the study. Understanding the participants’ experiences of the whole process is therefore essential in order to apply qualitative approaches used in this study.
The field of AD prevention research is constantly developing. Although there are many similarities among dementia prevention trials, there are differences in study design, interventions, and target groups. Therefore, it is important to investigate participants’ experiences to apply this knowledge in the further development of the evaluation and design of future trials. The overall aim of the study was to explore and describe the experiences of participation in the Multimodal preventive trial for Alzheimer’s disease (MIND-ADMINI) among persons with prodromal AD.
Method
Design and Participants
This qualitative study was part of the larger MIND-ADMINI project. MIND-ADMINI was a 6-month multinational in Sweden, Finland, Germany and France, randomized controlled trial with three parallel arms: (i) a multimodal lifestyle/vascular intervention, (ii) a multimodal lifestyle/vascular intervention + medical food, and (iii) a control. The intervention components are presented in Table 1.
 |
Table 1 Descriptions of the Intervention Components in MIND-ADMINI |
Inclusion and exclusion criteria for the MIND-ADMINI are described in a previous publication describing the intervention protocol.15 In Sweden, the participants were invited to participate in a 6-months extension of the study. Participants in the Swedish MIND-ADMINI trial site, who were allocated in the intervention groups, were invited to participate in this interview study if they were (i) interested in participation and share their experiences, (ii) able to speak in Swedish, and (iii) gave their written informed consent. All the participants who took part in two first parallel arms of intervention trial received the information about the interview study both oral and written by the second author (CT). Those participants who fulfilled the inclusion criteria and accepted the invitation were recruited in the study. Among the eligible participants a purposive sample was selected to include a representative sample of participants taking part in both parallel arms of interventions as well as having a variety of demographic characteristics to include different variations of the experiences among the participants.
Eight persons gave their written informed consent and participated in present study. The participants informed consent included publication of anonymized responses. Table 2 presents the demographic characteristics of the participants.
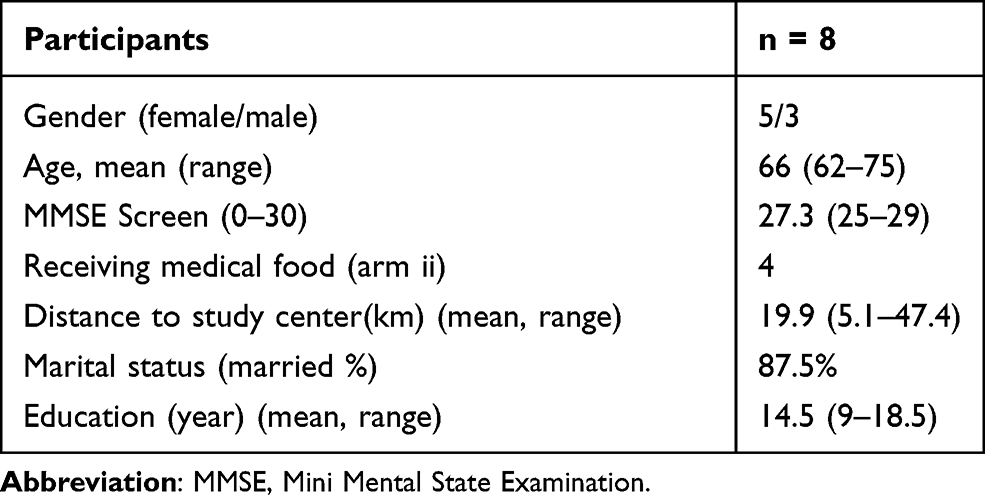 |
Table 2 Demographic Characteristics of the Participants in the Study |
Ethical Approval
The MIND-ADMINI and this sub-study received ethical approval from the Regional Ethical Review Board (Regionala Etikprövningsnämnden) in Stockholm, Sweden (Registration number: 2016/2605-31/1). All participants signed a separate consent form for the interview study in accordance with the Declaration of Helsinki (World Medical Association of Helsinki, 2013).
Data Collection
The MIND-ADMINI trial was conducted between October 2017 and December 2019. During November to December 2017 and April to June 2018, semi-structured, individually face-to-face interviews with eight participants were conducted twice, before and after the intervention. The participants were interviewed by the same interviewer (UA and CT) on both occasions. An interview guide was created based on the guidelines for qualitative interviews,20 that corresponded to the aims of the study. The topic areas are presented in Table 3. The participants were specifically asked questions regarding their experiences of participating in the intervention program, the information they received during the study, their motives and expectations. Semi-structured questions allowed the participants to freely reflect on the topics discussed.21 All interviews were audio-recorded and transcribed verbatim. During the interview, notes were taken by the interviewer. The interviews took between 30 to 120 minutes. Interviews were conducted in close connection to a MIND-AD trial activity in a university hospital facility in Stockholm.
 |
Table 3 Topic Areas of Questions in the Interviews |
Data Analysis
Qualitative content analysis was used, inspired by Granheim and Lundman,22,23 to systematically transform the large amount of data into the key results. The initial step was to read and re-read the interviews to get a sense of the whole (UA and CT). The transcriptions were color-coded, and notes were written in the margins. By continually comparing specific incidents in the data, concepts were identified, and codes were generated. The work included identifying meaning units, condensing, abstraction, and labeling codes in an inductive process. Conceptual codes were then grouped into major categories. During the analysis process, there were frequent meetings with discussions within the research team until an agreement was reached.
Results
The results of the study are presented in terms of a dynamic process, as demonstrated in Figure 1. The results are presented as categories of (i) knowledge of AD and prevention, (ii) motives for study participation, (iii) experiences of the received information about the study, (iv) taking the decision to participate, (v) expectations on study participation, (vi) experiences of study participation and (vii) internal and external factors influencing study participation. The study in the description of the results refers to the MIND-ADMINI prevention trial. As it is presented in the figure, participants’ knowledge about AD and prevention, their motives to take part in the prevention trial, and their experiences of the received information regarding the prevention trial has led them to take the decision to participate in the prevention trial and formulate their expectations. However, a number of internal and external factors influenced their participation in the study. The participants’ experiences of their participation in the prevention trial are described in the last part of this process.
 |
Figure 1 Dynamic process of participation in the MIND-ADMINI prevention trial. |
Knowledge About Alzheimer’s Disease and Prevention
The participants described that they had limited knowledge about AD and prevention before they started the study. They could give superficial descriptions of AD symptoms and treatment in general.
Before the study, I just knew that when someone gets AD, they forget things; that was the knowledge I had (participant 1, first interview).
Participants who had previous experiences of AD or other types of dementia in the family, related their knowledge almost entirely to these experiences. They described their feelings of fear of the disease and the consequences of the symptoms, which made them express reluctance to learn more about their own diagnosis.
What can I say, it’s just tragic with Alzheimer’s [Disease] if I am told I have it, I’m almost suicidal to avoid suffering (participant 4, second interview).
Several participants described that they, in the period after receiving their diagnosis, did not want to know more about the disease and therefore did not search for information and avoided the information provided by their caregivers. After 6 months of participation in the trial, participants experienced that their knowledge about the disease had increased. They also described how they had gained knowledge and insight about how to live with the diagnosis of prodromal AD during their participation in the study. The participants did not experience that their life in general changed immediately after receiving the diagnosis. Rather, they described that there were possibilities to take actions to affect their overall health and well-being and to delay symptoms.
… my knowledge has changed in a way. Alzheimer’s [Disease], the word itself has been like a red curtain. If you get it, life is over. But I think, it goes slowly, and I feel that even if some parts get worse, I know what the cause is. But it is not like I am panicking, so I do not feel like going to dig myself down (participant 6, second interview).
Several participants described the time from first experiencing symptoms to finally receiving the diagnosis as stressful. During this time period, they were in contact with several different healthcare providers such as general practitioners, psychiatrists, and neurologists before getting referred to the memory clinic. Their descriptions showed that they received other diagnoses, such as depression and burnout syndrome, prior to getting diagnosed with prodromal AD. Finally, receiving their diagnosis was described as a relief for some participants and as a shock for others. Interestingly, several participants were uncertain and showed hesitance when describing their own diagnosis and were unable to name that.
Because Alzheimer’s disease is quite common. I think [with hesitation] it is Alzheimer’s disease I have. I guess that’s it [AD] (participant 6, second interview).
Participants’ knowledge of prevention was not specifically related to AD or dementia. It was but rather a general knowledge about maintaining a healthy lifestyle which was expressed as their interest even before they participated in the study. Their limited knowledge on the possibility of dementia prevention was connected to the knowledge about the cause of dementia and the high attribution of genetic factors.
I do not know how much the genetics has to do with it all, but maybe that prevention is enough to delay the disease (participant 3, first interview).
After 6 months of participation in the study, the knowledge on prevention had increased. The increased level of knowledge also reflected how the participants perceived stigma in the beginning and at the end of the study, and how it might have influenced their participation. In the beginning of the study, the participants described feelings of fear and shame, while at the end of the study, they connected their increased level of knowledge with a higher sense of self-esteem and a decreased experience of stigma.
Yes, I have to say that I have, since I started, learned that there are so much that affects, exercise and diet, for example. Yes, you could … but I never thought that far. But I have got a little tougher somehow. Damn pity, I am alive anyway. That’s how I feel (participant 6, second interview).
Participants described it as shameful, to some extent, to become old and to lose the ability to perform different tasks. Some participants also described that they were trying to hide the fact that they had cognitive problems. One participant had not informed her family and children about her problems or what kind of trial she was participating in.
It’s a little shameful to grow old and not be able, and you can feel a little ashamed when you are not capable of doing things. Or, you know you are sick, but you’re trying to hide it (participant 3, first interview).
The experience of possible stigma or stigmatic situations was sometimes expressed through a denial of such expected situations. This became evident in participants’ descriptions of participating in the social groups during different components of the interventions.
No, I do not see the others in the group as someone who does not remember what my name is or what we have talked about. You get into something, yes but we talked about it last time, you do not remember it, that reasoning never happens, I see them as any friends. Not that we are a group of disabled people in any way. Absolutely not (participant 1, second interview).
Motives for Study Participation
The participants described a complex and multifaced picture of their motives for participating in the study. Two participants stated only one main motive for participating in the trial. It was either pure altruistic motives or hope for personal benefits. Six participants described a combination of both.
The participants described that being able to contribute to the scientific knowledge of AD and prevention and thereby helping others in the same situation was a strong motive for them to participate, and for one participant, it was their only reason. The participants strongly expressed the importance of being acknowledged as a person with an important task in the research. The participants described this motive as essential to actively participate in this study and to take responsibility for their contribution as a significant member in the intervention study.
I think that maybe I can be involved and contribute with something. I can leave something behind. That is the only reason I am in the study (participant 6, first interview).
Personal experiences of having persons with AD in the family strongly influenced their motives. They described that having such personal experiences might result in great fear for the disease and its consequences, especially the burden it would bring to children and relatives. Even if they hoped that the intervention would slow down their disease, the main goal for them to participate in the study was to minimize the burden for their families.
I hope, I really hope that you will be able to figure out how to avoid or prevent [development of AD] if you are in the risk group. At least that is why I’m here. Because it might lead to something better for others. I hope my kids will not get it (participant 6, first interview).
To be included in such a prevention trial was described as an opportunity. When the healthcare system has little to offer, participation in the trial was regarded as a possibility to act and to do something that could help to influence their situation.
I’m going to continue with this because I think it’s good and that I’m going out and not just sitting at home and just letting Alzheimer’s [disease] take over. I want to do this because I feel better (participant 8, second interview).
Access to specialized medical healthcare professionals at the memory clinic was described as another reason for participation in the prevention trial. Persons diagnosed with prodromal AD are often recruited as research participants soon after having received their diagnosis. They described that in a turbulent situation after receiving the diagnosis, being involved in the study allowed them to ask their questions from the specialized healthcare professionals that was experienced as safe and trustworthy. Not participating in the study and only being referred to a general practitioner might lead them to a loss of contact with the specialized healthcare clinic, which was perceived as threatening.
It was to be able to stay at the memory clinic, to have that support, I should start taking a stronger patch, have access to knowledge that a general practitioner does not have. To be able to go to someone and ask what should I do now? Just to have a support (participant 8, first interview).
After 6 months of participating in the study, new motives for participation were identified. Taking part in the social groups, socializing between interventions components, and supporting each other when needed became increasingly important for the participants. The participants’ descriptions demonstrate that the scheduled activities planned as intervention components had brought new content and meaning to their everyday lives.
Experiences of the Received Information About the Study
This category is presented as two subcategories focusing on participants’ experiences of the received information regarding the MIND-ADMINI prevention trial.
Understanding of the MIND-AD MINI Prevention Trial
During the initial phase of the study, the participants received oral and written information about the study aim and the contents of the trial. The written information in the informed consent form, was perceived as hard to understand by the participants and did not help them to fully comprehend the extent of engagement that was demanded. Several participants expressed that they did not have a clear understanding of the number of interventions and study visits that were required.
The information then, in the beginning, was that it would be a group with some members, that it would be about training memory, diet, and physical training. You did not know in what way, but it is just as well that you do not know everything from the beginning (participant 1, first interview).
Although the participants could not recall all the contents of the study at the time of the interview, all of them perceived that they had received good information at the time for informed consent. The positive reflections on receiving information at this time refers to interactions with the study physician and the study team, as well as feelings of being taken care of, being listened to and being important, and that they built a trusting relationship with the study team.
I understood that it would be to train the brain and train the body and it felt healthy in some ways (participant 8, first interview).
When participants were asked to describe the trial, only a few weeks after giving their informed consent, they were able to give a basic overview of the study aim and the intervention components. No one mentioned all five intervention components, and no one mentioned the medical food arm. The physical training component was highlighted as the most important component by the participants. However, after 6 months the descriptions of the trial showed substantial variation in the level of understanding of the study where several participants failed to describe the study aim.
I understand that this is some form of research. You asked? Yes, the purpose of the study is to try to help others and find out why it is this way. I guess you might want to develop medicine but I’m not sure if it works, but, because it must have been tested on humans or animals, so I hope you get something, but that’s probably why I’m here (participant 5, second interview).
When the participants were asked questions regarding their understanding of the benefits of the trial, they described their personal benefits as direct health benefits. They also described the study as important for society with regard to the economic and social burdens of AD. Moreover, they perceived that this research would provide knowledge that has benefits for the care of older adults.
It is society as such and me, of course. I feel like the main character in a movie (participant 1, first interview).
Trust in Different Levels
The participants described a superficial and limited understanding of the information provided by the informed consent form, and after 6 months, their understanding of the study aim and content had further decreased. They described that feelings of trust were a factor that made them perceive themselves as well-informed and strongly influenced their willingness to participate in research. The participants expressed their trust in different levels: Trust in the health care system, research systems, university, and even previous research results and in the study team. The feeling of trust was strongly connected to the credibility of the university and hospital as well as the participants’ previous experiences of receiving regular clinical care and previous knowledge and experiences of research.
This study has been done in Finland as well and there is so much knowledge from it. Professor K. (name), I wrote her name online and have read everything she has written (participant 4, first interview).
Furthermore, the participants described their trust in the research team. They also trusted that the data they helped to generate through their participation in the MIND-ADMINI would be well administered and substantially contribute to the scientific knowledge about AD.
I really trust the doctors in the hospital (participant 2, first interview).
The participants’ descriptions point to the need for developing trust with the research team over time. In particular, the trust that the research team members were skilled in their area of expertise and that they had a broad knowledge in the research topic as well as in the clinical field of dementia. Moreover, they should be trained not only to deliver the components of the interventions in the study but also to provide the support that the participants needed in relation to their diagnosis on an individual level.
… You should share that information with everyone. It is so important that everyone who works here really knows and has all the knowledge about previous studies and what advice you can give (participant 4, first interview).
The initial three mentioned categories describe what happens before the participants entered the study and how these categories influence the participants’ participation in the trial. The five following categories represent the period when the participants were included in the trial, from when they took the decision to participate, formulated their expectations and described their experiences after 6 months of participating in the trial. The internal and external factors describe a number of conditions that became either facilitators or barriers to influence the participants’ decisions to participate, their expectations, and their experiences of participation in the trial (Figure 1).
Taking the Decision to Participate in the Study
The decision to participate in the trial was described as easy to take. The participants made the decision by themselves or after a discussion with their family or study partner. They perceived themselves as being well-informed and having trust in the physician that delivered the information. The decision was made undoubtedly. In this study, no participants expressed their regrets regarding their decision to participate in the MIND-ADMINI Trial.
I felt from my side that this was not so much to think about, but it was just to say yes, a privilege to be part of something like this, that you were chosen (participant 1, first interview).
Expectations for Study Participation
The participants’ descriptions of their previous knowledge, motives to participate in the clinical trial, and the information that they received about the trial, shaped their expectations of participating in the study. During the initial phases of the study, the participants experienced a lack of information, and the fact that they did not know what was going to happen caused irritation and worries. Although the participants initially received a limited amount of information during the screening and inclusion period, due to randomization procedures in the protocol, the overall acceptance of the situation was good. None of the participants reflected on the possibility of being assigned to a specific arm in the study protocol. The participants did not have any specific expectations due to their limited knowledge about what was going to happen in the study and their expressed difficulties grasping the full extent of all components of the study. However, the participants expressed a sense of acceptance, optimism, and excitement about their participation.
When you get to be part of a project like this, then you have to follow the rules of the game, so to speak, otherwise it is useless both for myself and for you (participant 1, first interview).
While the participants strongly emphasized that the research in MIND-ADMINI was important and that their own contribution was essential for research success, they expressed more doubt about the expected personal benefits of the interventions on their own disease progression. They acknowledged that lifestyle changes were suitable for prevention purposes but that it was too late for them to benefit on a personal level due to the expected progression of the disease. In the beginning of the study, the participants carefully expressed some hopes about the positive effects of the interventions. After six months, these feelings of belief in the interventions were more strongly expressed with increased hope for positive effects and the possibility to delay the symptoms of the disease.
Just because I think it’s good [the interventions] when you have Alzheimer’s [disease], partly this with good food and then the flow of blood in body and brain and stuff like that. I think it’s good, that it might delay a little (participant 3, second interview).
No, I do not think the study can give me anything, for me it is too late, somehow. I do not think you can turn anything around; it will only get worse. I’m set on it anyway. It is mainly for the sake of others. For me, it’s too late (participant 6, first interview).
Experiences of Study Participation
The participants’ experiences of participation in the MIND-ADMINI are presented regarding a) study organization and logistics, and according to the following five domains representing the intervention components of the study: b) physical exercise training program, c) nutritional guidance, d) cognitive training e) social stimulation, and f) management of metabolic and vascular risk factors.
Study Organization and Logistics
In the beginning of the study, the participants described that they found the logistics of planning and organizing all different visits and tasks in the study to be challenging. This included communication with the study team and receiving large amounts of information. The number of tasks in the study, in terms of frequency of tasks and level of challenges, was perceived as borderline to what they were able to cope with. The example of tasks included multiple screening visits, baseline testing, and introduction sessions to present the interventions. The participants perceived that twice a week was a well-tolerated number of visits during the intervention period. More frequent visits were perceived as too demanding with no time for recovery and with too significant an impact on everyday life. Participants described fatigue during these initial weeks of the trial.
Yes, it’s starting to feel overwhelming, I’m getting tired. I get so tired; I do not understand. So, for me, two things are enough (participant 5, first interview).
In the end of the study, the number of tasks was not perceived as too many or too demanding despite the additional test visits and extra scheduled appointments. The participants repeatedly referred to their cognitive difficulties when describing how they managed the logistics of planning and receiving information. Difficulties with remembering oral information seemed to be a major problem for all participants. Keeping track of delivered written information, planning for study-related visits at the clinic, and estimating how time-consuming certain tasks would also create problems. Not being able to manage these tasks in an efficient way or having to put considerable effort into them created stress and feelings of insecurity. Difficulties with orientation often exacerbated that distress.
I try to keep track of everything, how much is this? I have not been able, and that is what I think has been the hardest part, that there is no order (participant 6, first interview).
The participants used different types of strategies to create order and keep track of information and tasks. These strategies included different solutions for sorting papers and getting reminders. Such strategies worked well for most participants but were easily disturbed, and a phone call about a rescheduled appointment was enough to induce feelings of self-doubt and worries.
I have a folder where I put the stuff, but I have to understand that I have received this note now, so I put a cross over it. For me, writing things down is very important (participant 8, first interview).
The participants emphasized the importance of the means of delivery of information. They specifically highlighted the need to receive written information. The information delivered by phone was perceived as especially challenging to remember. Furthermore, they preferred for the information to be organized and structured. For example, the information about nutrition should be gathered in a folder to make it easier to access after a meeting, and information about logistic matters should be delivered separately. Written information also made it easier for the participants to recall and inform their study partners about events in the study.
Then my husband comes and asks what did she (the nurse on the phone) say then? I do not know, then I really do not know. And now I think he understands it, but he has not understood it and he has become so annoyed with me! I can hang up and then the (information) is gone. So written information is necessary because I understand exactly what you are saying, but then I can mix it all up, it is hard to explain, but I cannot remember it (participant 5, first interview).
Participants in the prevention trial described that they received support from their study-partners, the person that was closely involved in the study together with the participant (eg, spouse, family member, or close relative). However, they also perceived problems with required visits during workdays since the majority of the study partners worked full-time.
I have had good support from my husband, he thinks it is good for me that I have things to do, that I leave the house (participant 6, second interview).
To receive feedback information on individual performance in the different intervention components was regarded as a sensitive topic by the participants. Some participants eagerly demanded feedback on their results to motivate them to perform better. However, they were scared of receiving feedback representing negative results as confirmation of the progression of their disease.
I don’t know if I want any feedback information on my results. I guess that you hope that the disease has not progressed. If I get it in writing, then I will know that I am getting worse (participant 3, second interview).
Participants experienced that it was important for them to receive information that was easy to understand and delivered in a way that was helpful for them to remember and to keep order. Furthermore, well-planned visits (number of visits and easy access to study center) could facilitate their participation in the study. Long-distance to study-center, costs for traveling and parking, perceived lack of information were described as barriers for participation. Participants experienced it very time consuming to take part in the study, which was described as the most disadvantage.
Physical Exercise Training Program
The physical exercise training component, which consisted of having visits to the gym twice a week, was perceived as the most important component by the participants which demanded a great deal of effort. Participants’ overall positive experiences mainly refer to the skilled and engaged coach who led the physical exercise training as a group activity. The ability to engage and stimulate the participants with personalized and varied exercises helped the participants persist in participating in this component even if they experienced resistance. Even if the training sometimes was experienced as very demanding, tiresome, and sometimes even painful, the intervention was highly appreciated by the participants. They experienced that they gained mainly from the training on a personal level and after 6 months they perceived themselves as stronger and at a better health.
When I started here, I was in a very poor condition, I had not trained for a very long time (participant 7, second interview).
The participants identified that a skilled and engaged coach to deliver the physical exercise training component was the most important facilitator for this component. They also experienced that training together in small groups enabled them to encourage each other. Other facilitators included well-planned logistics, such as good communications between all involved in the study (study team and participants), and combined study visits with other intervention components, such as the cognitive training. Physical pain, limited time for recovery, and fear of facing possible stigmatic situations were described as examples of barriers to participation in this component.
Nutritional Guidance
In the nutritional intervention component, the participants mostly perceived their diet as already healthy in the beginning of the study. They did not expect any need for change in their diet. They found even the intervention unnecessary and not providing them with any new knowledge helping them to adapt to a healthier diet. However, previously in the study, the participants had identified areas needing potential improvements, such as eating too much sugar or high alcohol intake in their personal diet. After 6 months, they showed an increased awareness of how their diet could affect health. They also reported several changes that they had implemented in their everyday diets.
I got to learn a lot about diet, but I have had some knowledge about it anyway. But now you think about it more. To eat the right things, lots of nuts, fruits, and fish and not [not to eat], remove butter and stuff like that, butter that is so good (participant 1, second interview).
Some participants experienced that the food diary increased their awareness about what they ate:
When I write in the diary, I eat fewer sweets (participant 7, first interview).
The participants reported a higher intake of vegetables, fish, and nuts. After 6 months, they also felt convinced that this was an important part of a healthy lifestyle and that they were planning on continuing with a healthier diet after the end of the study. Several participants described the support from spouses as vital to make the changes. Information provided during group sessions was more difficult to comprehend and remember than information provided in individual sessions where the information was more individualized. The need for written information was crucial for the participants to be able to assimilate the information.
I do not remember anything of what we talked about at the group meetings (participant 7, second interview).
The delivery of written information and having support from study partners were described as facilitators of participation in this component. Not being able to take part in the visits that happened in daytime schedules, loss of income for study-partners was described as barriers of participation in this intervention component.
Cognitive Training
The cognitive training intervention conducted by a computer program was perceived as complicated and hard to understand. Although most participants experienced the training as being challenging, they perceived the hinders differently. Some were not emotionally affected and described the training as fun and entertaining. Others found it hard to face failures in the training program and felt shortcomings to personal expectations about their ability when cognitive problems became evident. Some participants could not distinguish whether it was a training session or an assessment.
The cognitive training is very difficult. I am bad at it and find it difficult. It will be difficult to do (participant 2, first interview).
Most participants did not take the opportunity to do the training at home since they did not have a computer or found it challenging to use a computer. Other reasons for not conducting the training at home were related to their difficulties in finding the motivation to both initiate and complete the task.
Conversely, the skilled and knowledgeable coach to guide the participants and provide support and a quiet and tranquil environment to help the participants focus on the tasks without disturbance were described as facilitators of participation in this intervention component. The participants experienced that the training was challenging, which revealed their cognitive difficulties, and they reported it as a barrier to their participation in this intervention component.
Social Stimulation
In the beginning of the 6-month intervention period, the participants perceived the small groups in intervention components positively. Their interactions were described as joyful with jokes and small talks but also as supportive and with an element of competition. Early in the study, participants engaged in conversations about their common situation, which created affinity and a sense of safety. Some participants reflected on the stigmatic situations that might or might not occur. After 6 months, the results indicated that the importance of the social groups had increased for the participants and that they were even perceived as the main benefit of participating in the trial for several participants. The participants perceived the social groups as a strong motive for the participation in the trial extension at 6 to 12 months. The small groups also created a trustful environment helping to reduce the participants’ feelings of stigma.
I also like the connection with those who are in the group, that we have the same disease. We talk openly about it, and compare a little bit with each other, and we can laugh at it and get serious about it and yes, it’s great that we are a group with exactly the same thing (participant 3, second interview).
Well-composed groups, providing time and locations for social interactions between interventions, were described as facilitators of social stimulations. Stigmatic situations may constitute barriers.
Management of Metabolic and Vascular Risk Factors
This study component was least discussed by the participants, although they referred to visits with the physicians and nurses, expressing the feelings of being looked after and having medical check-ups. No participants mentioned or reflected on this intervention component concerning the control or management of specific cardiovascular risk factors. Overall, the participants were satisfied with the received services during the process.
There are meetings with the nurse and check-ups at the doctor. And you get to know a lot about the disease and how to live with it. It is very interesting. Everything is very good I think (participant 7, first interview).
Internal and External Factors Influencing Study Participation
The participants described internal and external factors as conditions influencing their participation in the trial as facilitators or barriers for participation (see Table 4). Participants gave examples of several such factors with broad variations. Internal factors were referred to as conditions directly connected to the individual, while external factors represented conditions in the context and surrounding society.
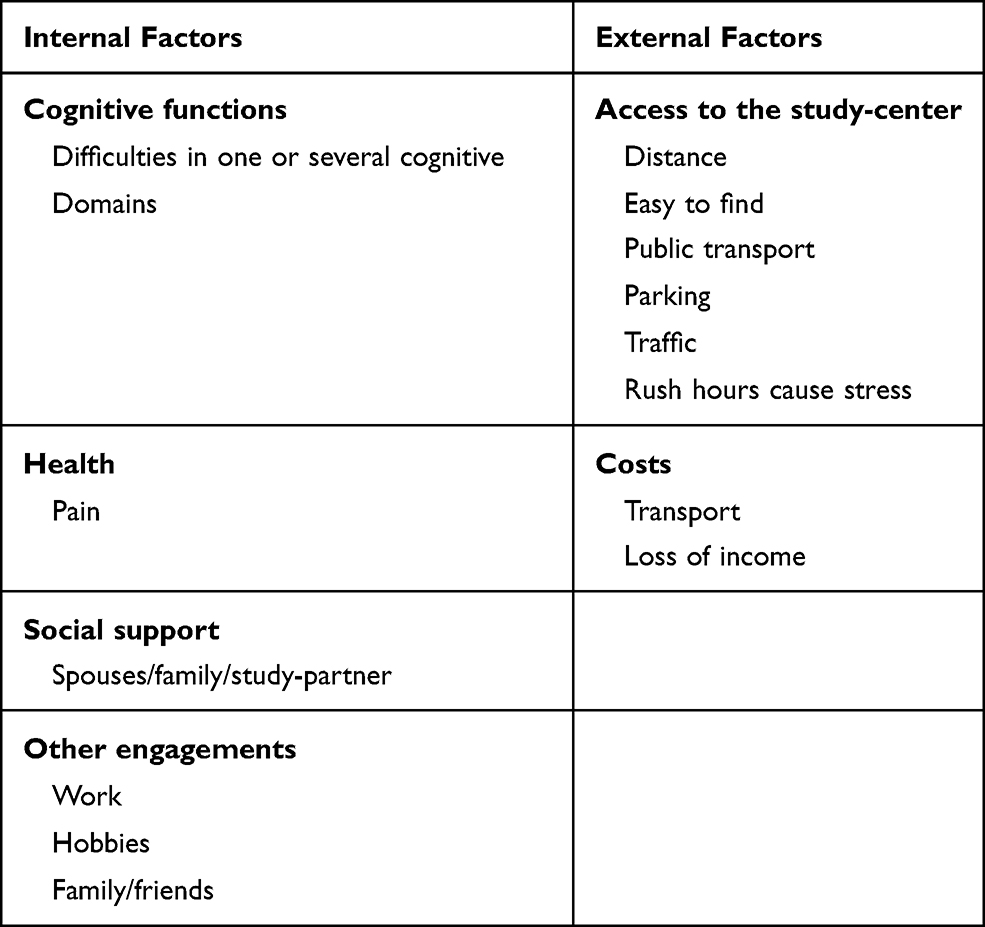 |
Table 4 Summary of Internal and External Factors Influencing Study Participation |
Discussion
This qualitative study explored experiences of participation in the MIND-ADMINI prevention trial where a multimodal adapted FINGER6 intervention protocol was evaluated for safety and feasibility for persons with prodromal AD. To participate in a pharmacological AD preventive clinical trial has been described as demanding, often due to the high burden for the participants with frequent visits and invasive measurements or interventions.24,25 To participate in a multimodal preventive trial for Alzheimer’s disease, such as MIND-ADMINI, may also be demanding. This is due mainly to the high burden of frequent visits over a more extended period of time. The results of this study indicate that MIND-ADMINI was well-tolerated by the participants. The participants described the high burden and tiredness they experienced due to their participation in the study, which is in line with previous research.24 However, these experiences were mostly concentrated at the beginning of the study. One possible explanation for these findings might be participants’ decreased level of cognitive functions leading them to experience the described challenges with managing new situations and receiving large amounts of information. However, over the period of time participating in the intervention program and getting familiar with the tasks and the new routine, the interventions and the related procedures were no longer experienced as new, challenging and highly burden. Furthermore, these findings indicate that the experiences vary during a lengthy and complex study.
Although the public knowledge about AD and dementia has increased, especially among higher-educated trial participants,26 the participants in this study described their knowledge about AD and prevention as superficial in the beginning of the study. In line with previous research,27,28 they referred to genetic factors as having a major impact on the disease and described limited belief in preventive actions. Interestingly this perception changed, and after 6 months of participating in the prevention trial, the participants described stronger beliefs and a more optimistic view of the possibility to delay the disease with preventive actions. The participants experienced increased knowledge about AD and reflected on how they had overcome the initial ‛shock’ of receiving a diagnosis and learning how to live with the diagnose in a better way, after 6 months of participation in the study.
The participants’ need, and search for information has been described in several studies as a motive to participate in clinical trials.29–31 In the present study, the participants also revealed resistance to seeking information and avoiding reading about AD or dementia-related information provided by their physicians. This may be related to the time of the recruitment to the study, soon after receiving the diagnosis of prodromal AD. To receive a diagnosis of AD is life-changing,32 and to receive the diagnosis of MCI is also described with strong emotional reactions and experiences of stigma.33 The participants in this study discussed their own diagnoses with several uncertainties and with many questions. In this situation, it may be hard to know what information to seek. The need for study-centers with AD trials to also provide non-study-related support to their participants has been suggested by Bardach et al.31
Motives for study participation were both altruistic and self-beneficial. Health benefits, access to specialized care were common motives for participation. In this study and several others,26,31,32 altruism and willingness to help research have been reported as one of the most important motives for the participants to take part in the clinical trials. Researchers should acknowledge this effort, with feedback to the participants on the value that their participation represents.
Before the participants made their decision to participate in the trial, they received a large amount of information about the study. The written informed consent information was perceived as hard to understand, and this interview study shows that the participants had difficulties to recall and speak about the aim and content of the study. Despite this, the participants perceived themselves as well-informed. They described that feelings of trust contributed to the feeling of being safe, which was important when receiving the information and deciding to participate in the trial. This is aligned with previous research indicating that trust is often connected to the reputation of the university or hospital,31 and that a trustful relationship with the researcher and the study team, which acknowledges the participants’ efforts in the trial, encourages further participation.34
When participants entered the trial, they described the decision as easy to take, and their expectations were shaped from their previous knowledge, motives, and the received information. The decision was generally discussed with the family, but the participants stressed that the decision was their own. Most studies that include participants with dementia require a study partner to sign the informed consent and to conduct several important tasks in the study, such as support the participant with practical tasks in the trial and to provide the researcher with knowledge and information on the participants’ status and well-being. Previous research showed that the perceived burden on the study partners varies from no extra burden to high extra burden due to the study-partner demands.35,36 The requirement of a study partner in the MIND-ADMINI trial entailed some extra burdens as the majority of the study partners were still working, and practical or economic factors prevented them from participating in daytime activities. Furthermore, this could be discussed from an ethical point of view, where the participants in future trials targeting persons with prodromal AD who are still fully autonomous and do not have dementia could be non-eligible if they have not revealed their diagnoses and therefore could not present a study-partner. This needs to be discussed, and study-partners experiences from trials targeting prodromal AD should be further investigated.
Internal and external factors influenced the participants’ participation as possible facilitators and barriers to their study participation. Internal factors, such as health issues and cognitive difficulties, led to different support needs of support. Other engagements in the participants’ lives may have to be reduced in favor of participation in the time-consuming trial. External factors, such as finding a parking space or access to public transportation to the study center, were experienced as important for participation in a trial at the study centers.37,38 With a more personalized approach to identify specific needs of support, study-centers could more easily optimize the resources to ensure the participants’ satisfaction.
In general, the participants experienced their study participation positively. The intervention components implied different challenges for the participants. Cognitive deficits were often described as a reason for experienced difficulties. This was especially evident when the participants described their capability to handle the logistics matters. They stressed the need to receive written information that was easy to understand. Clear and concise study information is also a crucial factor in the recruitment of participants to AD trials.39 The physical exercise training component was perceived as the most important and beneficial for health. In the cognitive training intervention, the participants experienced various degrees of resistance, where some participants found it hard to be confronted with their difficulties. In computer-based cognitive training studies, adherence to the intervention has been challenging.40 In the nutritional component, the participants described an increased awareness about their diet after 6 months, even though they did not experience any need to change their habits in the beginning of the study. In line with previous studies, cognitive difficulties affected the ability to retain information from the intervention and make decisions according to recommended guidelines.41 Being part of a small group that regularly met in the study center and performed the interventions together became increasingly important to the participants. Skilled and engaged coaches and staff were reported as the most important element to support the participants during the trial.
Strength and Limitations
The present study aimed to explore and describe participants’ experiences of participation in the intervention program. In line with the qualitative methodology and epistemology of the design,22,23 the study results are not intended to be generalised to the whole population of persons with prodromal AD, but rather to reflect on the results from a person-centered approach and individuals’ perspective in further development of intervention program. Although MIND-ADMINI is an international RCT, this sub-study was conducted in only one of the four participating countries. The results of this study must therefore be interpreted within other countries’ health care systems and cultural settings. It is a strength that this study is exploring the experiences of participants taking part in a prevention trial. Many similar studies have been investigating non-participant’s attitudes about hypothetical research situations.42,43
Despite the small number of participants, the interviews were conducted twice, which gave a more nuanced picture of the whole process of study participation and provided deep and rich data. This interview study included participants from MIND-ADMINI, and consequently, the participants reflected the inclusion criteria for the RCT. The participants were highly educated, and fluent Swedish speaking which could be representative for participants in the clinical trial but probably less representative for a general population. However, the sample reflects a variety of demographic characteristics (age, gender, marital status and education), providing the opportunity for a more heterogeneous sample to capture different experiences among the participants and rich data. In two recent studies,44,45 both specialized nurses in preventive care and persons at-risk of CVD and dementia discussed the possibility to increase motivation by highlighting the fact that managing CVD risk factors might reduce the risk for dementia. However, in present study the participants did not seem to be aware of the importance of the “management of metabolic and vascular risk factors” as an intervention in the study. One reflection could also be that the participants were not asked more specifically about this intervention in relation to the other interventions, and further exploration of the area could be a topic for future explorations. Another area that was not discussed by the participants in the interviews was the randomization into different arms in the protocol. Even if the participants were informed of the administration of the medical food in one of the study arms before randomization in the trial, they did not sufficiently describe how this intervention was experienced in detail. One possible reflection might be experiencing difficulties in understanding or remembering the received information in this area due to its complexity in the informed consent which was also expressed by some participants. The participants also found it hard to distinguish the medical food from the general nutrition component of the study which made it hard for them to express any specific expectations or experiences related to the medical food. Future studies are needed to further explore this dimension.
Conclusion
The results of this study indicate that the multimodal lifestyle intervention applied in the MIND-ADMINI was well-tolerated by the participants with prodromal AD. The participants’ knowledge about AD and prevention increased during the trial, and their motives for participating in MIND-ADMINI were described as both altruistic and self-beneficial in nature. To help and contribute to research was regarded as important and should be more acknowledged by researchers in future trials. Health benefits from the study components, access to specialized medical care, and experienced staff in the study team were found as perceived benefits. To handle the intensive flow of information was a major challenge for the participants. The physical exercise training component was regarded as the most important and appreciated intervention. The number of tasks and visits at the study center was perceived as burdensome at the beginning of the study but was later well-tolerated. Although the MIND-ADMINI protocol includes personalized intervention components, this study shows a need for applying a person-centered approach in the conduction of the study, acknowledging the variation in needs that persons with prodromal AD might experience in the different categories presented in the results. Finally, applying a person-centered approach could be beneficial for recruitment, avoiding potential barriers, and increasing participants’ satisfaction in future trials.
Acknowledgments
We want to thank all participants in this study for their willingness and active participation in sharing their experiences with us. We also thank Sofie Gaber for the language edition.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Disclosure
Miia Kivipelto reports Advisory boards: Combinostics, Swedish Care International, Roche, Biogen Board of Governors member: Alzheimer’s Drug Discovery Foundation Guidelines development group: WHO Governance Committee member: Global Council on Brain Health Grant support: Academy of Finland, Swedish Research Council, Social Insurance Institution of Finland, Ministry of Education and Culture of Finland, Alzheimer’s Research and Prevention Foundation, EU 7th framework, AXA Research Foundation, CIMED, JPND, IMI, EiT-Health, Wallenberg Clinical grant, Stiftelse Stockholms Sjukhem, FORTE, KI-Janssen Strategic Collaboration, Imperial College ITMAT, Gates Ventures/ADDI, Alzheimer’s Drug Discovery Foundation, Part the Cloud. No other conflict of interest in this study is reported by the authors.
References
1. Apostolova LG. Alzheimer Disease. Continuum (Minneap Minn). 2016;22(2Dementia):419–434.
2. World Health Organization. Dementia: A Public Health Priority. Geneva, Switzerland: World Health Organization; 2012. Retrieved from: https://www.who.int/publications/i/item/dementia-a-public-health-priority.
3. Gauthier S, Albert M, Fox N, et al. Why has therapy development for dementia failed in the last two decades? Alzheimer’sdementia. 2016;12(1):60–64.
4. Barnes DE, Yaffe K. The projected effect of risk factor reduction on Alzheimer’s disease prevalence. Lancet Neurol. 2011;10:819–828.
5. Livingston G, Sommerlad A, Orgeta V, et al. Dementia prevention, intervention, and care. Lancet. 2017;390(10113):2673–2734.
6. Ngandu T, Lehtisalo J, Solomon A, et al. A 2 year multidomain intervention of diet, exercise, cognitive training, and vascular risk monitoring versus control to prevent cognitive decline in at-risk elderly people (FINGER): a randomised controlled trial. Lancet. 2015;385(9984):2255–2263.
7. Andrieu S, Guyonnet S, Coley N, et al. Effect of long-term omega 3 polyunsaturated fatty acid supplementation with or without multidomain intervention on cognitive function in elderly adults with memory complaints (MAPT): a randomised, placebo-controlled trial. Lancet Neurol. 2017;16(5):377–389.
8. Chhetri JK, de Souto Barreto P, Cantet C, et al. Effects of a 3-Year multi-domain intervention with or without omega-3 supplementation on cognitive functions in older subjects with increased CAIDE dementia scores. J Alzheimers Dis. 2018;64(1):71–78.
9. Moll van Charante EP, Richard E, Eurelings LS, et al. Effectiveness of a 6-year multidomain vascular care intervention to prevent dementia (preDIVA): a cluster-randomised controlled trial. Lancet. 2016;388(10046):797–805.
10. Amieva H, Le Goff M, Millet X, et al. Prodromal Alzheimer’s disease: successive emergence of the clinical symptoms. Ann Neurol. 2008;64(5):492–498.
11. Dubois B, Feldman HH, Jacova C, et al. Advancing research diagnostic criteria for Alzheimer’s disease: the IWG-2 criteria. Lancet Neurol. 2014;13(6):614–629.
12. Donohue MC, Sperling RA, Salmon DP, et al. The preclinical Alzheimer cognitive composite: measuring amyloid-related decline. JAMA Neurol. 2014;71(8):961–970.
13. Sperling RA, Jack CR
14. Aisen PS, Andrieu S, Sampaio C, et al. Report of the task force on designing clinical trials in early (predementia) AD. Neurology. 2011;76(3):280–286.
15. Sindi S, Thunborg C, Rosenberg A, et al. Multimodal preventive trial for Alzheimer’s Disease: MIND-ADMINI Pilot Trial Study Design and Progress. J Prev Alzheimer’s Dis. 2022:1-10.
16. Vellas B, Pesce A, Robert PH, et al. AMPA workshop on challenges faced by investigators conducting Alzheimer’s disease clinical trials. Alzheimer’sdementia. 2011;7(4):e109–117.
17. Dellson P, Nilsson K, Jernström H, Carlsson C. Patients’ reasoning regarding the decision to participate in clinical cancer trials: an interview study. Trials. 2018;19(1):528.
18. Grill JD, Galvin JE. Facilitating Alzheimer disease research recruitment. Alzheimer Dis Assoc Disord. 2014;28(1):1–8.
19. Grill JD, Karlawish J, Elashoff D, Vickrey BG. Risk disclosure and preclinical Alzheimer’s disease clinical trial enrollment. Alzheimer’s Dementia. 2013;9(3):356–359.e351.
20. Kvale S. Interviews: An Introduction to Qualitative Research Interviewing. Lund: Studentlitteratur; 2007.
21. Whiting LS. Semi-structured interviews: guidance for novice researchers. Nurs Stand. 2008;22(23):35–40.
22. Graneheim UH, Lundman B. Qualitative content analysis in nursing research: concepts, procedures and measures to achieve trustworthiness. Nurse Educ Today. 2004;24(2):105–112.
23. Graneheim UH, Lindgren BM, Lundman B. Methodological challenges in qualitative content analysis: a discussion paper. Nurse Educ Today. 2017;56:29–34.
24. Nuno MM, Gillen DL, Dosanjh KK, et al. Attitudes toward clinical trials across the Alzheimer’s disease spectrum. Alzheimers Res Ther. 2017;9(1):81.
25. Solomon A, Akenine U, Andreasen N, et al. Practical lessons from amyloid immunotherapy trials in Alzheimer disease. Curr Alzheimer Res. 2012;9(10):1126–1134.
26. Cahill S, Pierce M, Werner P, Darley A, Bobersky A. A systematic review of the public’s knowledge and understanding of Alzheimer’s disease and dementia. Alzheimer Dis Assoc Disord. 2015;29(3):255–275.
27. Kim S, Sargent-Cox KA, Anstey KJ. A qualitative study of older and middle-aged adults’ perception and attitudes towards dementia and dementia risk reduction. J Adv Nurs. 2015;71(7):1694–1703.
28. Glynn RW, Shelley E, Lawlor BA. Public knowledge and understanding of dementia-evidence from a national survey in Ireland. Age Ageing. 2017;46(5):865–869.
29. Coley N, Rosenberg A, van Middelaar T, et al. Older Adults’ reasons for participating in an eHealth prevention trial: a cross-country, mixed-methods comparison. J Am Med Dir Assoc. 2019;20(7):843–849.
30. Rosenberg A, Coley N, Soulier A, et al. Experiences of dementia and attitude towards prevention: a qualitative study among older adults participating in a prevention trial. BMC Geriatr. 2020;20(1):99.
31. Bardach SH, Parsons K, Gibson A, Jicha GA. “From victimhood to warriors”: super-researchers’ insights into Alzheimer’s disease clinical trial participation motivations. The Gerontologist. 2020;60(4):693–703.
32. Robinson L, Gemski A, Abley C, et al. The transition to dementia–individual and family experiences of receiving a diagnosis: a review. Int Psychogeriatrics. 2011;23(7):1026–1043.
33. Morris JL, Hu L, Hunsaker A, Liptak A, Seaman JB, Lingler JH. Patients’ and Family members’ subjective experiences of a diagnostic evaluation of mild cognitive impairment. J Patient Exp. 2020;7(1):124–131.
34. Hedman R, Hellström I, Ternestedt BM, Hansebo G, Norberg A. Sense of self in Alzheimer’s research participants. Clin Nurs Res. 2018;27(2):191–212.
35. Black BS, Taylor H, Rabins PV, Karlawish J. Researchers’ perspectives on the role of study partners in dementia research. Int Psychogeriatrics. 2014;26(10):1649–1657.
36. Black BS, Taylor HA, Rabins PV, Karlawish J. Study partners perform essential tasks in dementia research and can experience burdens and benefits in this role. Dementia (London, England). 2016;17(4):494.
37. Bardach SH, Holmes SD, Jicha GA. Motivators for Alzheimer’s disease clinical trial participation. Aging Clin Exp Res. 2018;30(2):209–212.
38. Grill JD, Kwon J, Teylan MA, et al. Retention of Alzheimer disease research participants. Alzheimer Dis Assoc Disord. 2019;33(4):299–306.
39. Clement C, Selman LE, Kehoe PG, Howden B, Lane JA, Horwood J. Challenges to and Facilitators of Recruitment to an Alzheimer’s Disease Clinical Trial: a Qualitative Interview Study. J Alzheimer’s Dis. 2019;69(4):1067–1075.
40. Turunen M, Hokkanen L, Bäckman L, et al. Computer-based cognitive training for older adults: determinants of adherence. PLoS One. 2019;14(7):e0219541.
41. McGrattan AM, McEvoy CT, Vijayakumar A, et al. A mixed methods pilot randomised controlled trial to develop and evaluate the feasibility of a Mediterranean diet and lifestyle education intervention ‘THINK-MED’ among people with cognitive impairment. Pilot Feasibility Stud. 2021;7(1):3.
42. Milne R, Bunnik E, Tromp K, et al. Ethical issues in the development of readiness cohorts in Alzheimer’s disease research. j Prev Alzheimer’s Dis. 2017;4(2):125–131.
43. Milne R, Diaz A, Badger S, Bunnik E, Fauria K, Wells K. At, with and beyond risk: expectations of living with the possibility of future dementia. Sociol Health Illn. 2018;40(6):969–987.
44. Akenine U, Barbera M, Beishuizen CR, et al. Attitudes of at-risk older adults about prevention of cardiovascular disease and dementia using eHealth: a qualitative study in a European context. BMJ Open. 2020;10(8):e037050.
45. Beishuizen CR, Akenine U, Barbera M, et al. Integrating nurses’ experiences with supporting behaviour change for cardiovascular prevention into a self-management internet platform in Finland and the Netherlands: a qualitative study. BMJ Open. 2019;9(6):e023480.
 © 2022 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.
© 2022 The Author(s). This work is published by Dove Medical Press Limited, and licensed under a Creative Commons Attribution License.
The full terms of the License are available at http://creativecommons.org/licenses/by/4.0/.
The license permits unrestricted use, distribution, and reproduction in any medium, provided the original author and source are credited.