")
Back to Journals » Nursing: Research and Reviews » Volume 13
Factors Associated with Male Involvement in Institutional Child Delivery Services of Their Partner in Southern Ethiopia
Authors Alemu M, Adhena G , Assefa N , Dessie Y
Received 29 June 2022
Accepted for publication 23 May 2023
Published 9 June 2023 Volume 2023:13 Pages 1—11
DOI https://doi.org/10.2147/NRR.S380433
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pariya Fazeli
Meseret Alemu,1 Girmay Adhena,2 Nega Assefa,3 Yadeta Dessie3
1Department of Reproductive Health, Lemmo District Health Office, Hossana, Southern Ethiopia; 2Department of Reproductive Health, International Medical Corps, Gambella, Ethiopia; 3School of Public Health, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia
Correspondence: Girmay Adhena, Email [email protected]
Background: Male partner involvement in reproductive health services is an important strategy to decrease maternal and child morbidity and mortality. Despite this, little attention is given to this issue around the globe, particularly in Africa, where male dominance is high. This study aimed to assess male partner involvement in institutional delivery services in Lemmo district, Southern Ethiopia.
Methods: A community-based cross-sectional study was conducted among 614 male participants. A multistage sampling technique was used to select study samples. A structured, pretested, and interviewer-administered questionnaire was used to collect the data. Male involvement in institutional delivery was measured using six yes or no items. The participants were asked if they communicated with relatives and health care providers, saved money, arrange transportation, decide to give birth at an institution, and arrange blood donation. Binary and multivariable logistic regression was used to identify associated factors. An adjusted odds ratio with 95% CI was used to show the strength and direction of the association. Variables with a p-value < 0.05 were considered statistically significant.
Results: A total of 251 (43.1%, 95% CI: (39.2, 46.9)) male partners were involved in the institutional delivery services of their partner. Primary educational level [AOR=2.2, 95% CI: (1.361, 3.532)], secondary and above educational level [AOR=2.4, 95% CI: (1.46, 4.01)], having good knowledge [AOR=3 (95% CI: (2, 4.49)], positive perception [AOR=3.66, 95% CI: (2.45, 5.46)], and discussing institutional delivery with their spouse [AOR=1.99, 95% CI: (1.3, 2.99)] were significantly associated factors.
Conclusion: More than two out of five male partners were involved in the institutional delivery services of their partner. Attending formal education, having good knowledge, positive perception, and discussing institutional delivery with a spouse were significantly associated factors. Strengthening male partner involvement in reproductive health services and enhancing the culture of reproductive inter-spousal communication through couple counseling and peer-to-peer group sessions at a facility and community level are important measures.
Keywords: male involvement, institutional delivery, Lemmo, Ethiopia
Introduction
Male involvement is defined as when a man is involved in activities such as attending antenatal care (ANC) visits, birth plans, encouraging exclusive breastfeeding, and immunization for their children.1 Male sharing responsibilities, participation in sexual and reproductive health (SRH), and promotion of gender equality have attracted considerable global attention since the International Conference on Population and Development (ICPD) in Cairo in 1994. Special shared responsibility, support, and their active taking part in fatherhood such as family planning, pregnancy, and maternal and child health services are among the important issues that had global attention during the conference.2,3
Males play a critical role in carrying gender equality and decision-making in most societies. So, full participation and partnership are needed in productive and reproductive life because pregnancy and childbirth are by tradition accepted as the domain of women and still masked in secret.2,4,5 Evidence showed that the three strategies for male involvement play a critical role in reproductive health services. The first strategy is men as clients, which encourages men to use SRH services, the second strategy is men as partners which engages couples to promote better couple relations for sexual, reproductive, and maternal health and the third strategy is men as agents of positive change which play crucial roles in catalyzing social change for the benefit of men, women, and child health.6,7
Male involvement can change health-seeking behavior for essential maternal and newborn health care (MNH), and home care practices for mothers and newborns. It also has a positive effect on couple relationship dynamics and contributes to enriching maternal and child mortality and morbidity.4 Most countries have no official policy on male involvement in reproductive health services.4,8 Male involvement during pregnancy, childbirth, and after birth helps to improve a woman’s and child’s health.9 Encouraging more help by the husband during childbirth can improve MNH because males are actively involved with accessibility, engagement, responsibility, and maintaining relationships.7,10
Globally, the maternal mortality ratio (MMR) due to preventable complications related to pregnancy and childbirth declined by 44% between 1990 and 2015. Of this, around 99% were from low-resource settings, with 66% from sub-Saharan Africa (SSA).9 In Ethiopia pregnancy-related MMR was 412 deaths per 100,000 live births.11 The neonatal mortality ratio (NMR) globally declined by 51% from 37 per 1000 live births to 18 between 1990 and 2017. Regionally, the NMR was the highest in SSA and South Asia, with an estimated 27 deaths per 1000 live births in 2017.9 In Ethiopia, NMR was 29 per 1000 live births.11 If women had interventions to address complications during pregnancy and newborn, they could be prevented and avoided.9,11,12
Pregnancy and childbirth are the most important issues of SRH that are affected by male partner involvement and their contribution is essential to improve maternal and child health services.2 Evidence in Ghana, Nepal, and Kenya showed that male partner involvement during childbirth was 44.5%, 47.9%, and 68% respectively.1,13 In studies in Ethiopia such as in Mekelle (60.4%) and Ambo (50.8%), male partners were involved during institutional delivery services.14,15
Limited knowledge about complications of childbirth and institutional delivery negatively affects the husband’s provision and involvement.16 Socio-cultural and health system-related factors are among the factors that affect male involvement in maternal health care services.17 Evidence showed that male partner involvement in institutional delivery is also affected by sociodemographic, health facility, knowledge, and perceptions-related factors.13,18
In Ethiopia, male partners are often the decision-makers about whether their partner can use reproductive services or not. Evidence about male involvement in institutional delivery services helps local policymakers and implementing partners to decrease maternal and child morbidity and mortality. Despite this, there is limited evidence on this issue in the study area. Thus, this study aimed to assess the prevalence of male partner involvement and associated factors in institutional child delivery services of their partner in Lemmo district, Southern Ethiopia.
Methods
Study Area and Period
The study was done in Lemmo district, which is located in the Hadiya zone, Southern Ethiopia. Hossana town is the administrative center of the district which is 232 kilometers away from Addis Ababa, the capital city of Ethiopia, and 194 kilometers away from Hawassa, the Southern Nation Nationalities regional state capital city. There were 35 Kebeles in the district (32 rural and 3 urban). The total estimated population of the district was 153,469, out of this 76,014 (49.5%) were males and 77,455 (50.5%) were females [Lemmo district plan and finance Bureau]. A total of 15,259 women were in the reproductive age group and the district has a total of 32,055 households. The study was conducted from March 7–30/2020.
Study Design
A community-based cross-sectional study was used in this study.
Population
All currently married males whose wives gave birth a year before the study period were the source population. Those men who are from the selected Keeble’s and selected households consisted of the study population. Males who were unable to communicate due to severe medical problems were excluded.
Sample Size Determination and Sampling Procedure
The sample size was calculated for the first objective using the single population proportion formula (n = (zα/2)2 p (1-p)/d2) where n is the desired sample size, z is the critical value at 95% confidence level (1.96), d is the margin of error (5%) and p (41.3%) is the prevalence of male involvement in institutional delivery from the previous study done in Mareka district.19 Using the formula and substituting the values, n= (1.96)2*0.413*0.587/(0.05)2=373, assuming a 10% non-response rate, and considering 1.5 design effect, 373*1.5+ (10%*559) resulted in 614. The sample size was also calculated for the associated factors using Epi-info software version 7, by considering power 80%, and 95% level of confidence, and it resulted in 386. Finally, the calculated sample sizes for the first objective (614) were higher than the sample size for the second objective (386). Thus, the final sample size used for this study was 614.
For the sampling procedure, a multistage sampling technique was used by considering the study participants to select from the Kebeles (smallest administrative unit). First, all Kebeles in the district were stratified into urban and rural areas. The district has 35 kebeles (32 rural and 3 urban). Then, one out of three urban and ten out of 32 rural Kebeles were selected by using a simple random sampling method. The number of women who gave birth within a year was obtained from the registry of the health post and health centers. The full address of the household for each kebele was seen from the registration book of the health office, kebele as well as the health extension workers. Allocation of proportion to the sample size was done to identify the required number of samples for each selected kebele. A systematic sampling method was employed to select the household from each kebele. Then the first household was selected from the house of the respective kebele using the lottery method, and the next household was selected using a systematic sampling technique. When more than one eligible respondent was found in the selected household, only one respondent was chosen by the lottery method. In cases where the eligible was not found in the selected household, a revisit has been arranged a minimum of three times, and if they were not present considered non-respondent.
Data Collection Procedure and Tool
A structured, pretested, and interviewer-administrated questionnaire adapted from different literature was used to collect the data.11,16 The questionnaire consisted of the socio-demographic, knowledge, perception, socio-cultural, and health facility-related characteristics. It was initially prepared in English and then translated into Hadiya and Amharic (local languages) by language experts (persons). Six healthcare providers who are fluent speakers of the local language collected the data. Two midwives (degree) supervised the data collection processes. Two days of intensive training was given to the data collectors and supervisors on how to collect, questionnaire, interview, ethical issue, and the purpose of the study to ensure the quality of the data collection process.
Operational Definition
Male involvement: This was measured by six yes or no questions with a total score of six points. The participants were asked if they communicated with relatives, saved money, arrange transportation, decide for their wife to deliver in a health institution, arrange blood donation, and discuss with the health care provider on institutional delivery. Those participants who scored three and above were categorized as involved and those who scored below three were categorized as not involved in institutional delivery services.11,16
Wealth index: This was measured by using 25 items consisting of domestic animals, durable assets, and household characteristics. The principal component analysis (PCA) was used to produce wealth quantiles to show and reveal the economic status of the household.11
Institutional delivery: A woman who gave birth at a health institution (health center, and hospital) and is attended by skilled health personnel.11
Discussion: This was measured by asking whether the respondents discussed with their partner about institutional delivery or not.
Male partner: A male whose wife gave birth within one year before the study period.
Knowledge: This was measured by six yes or no knowledge-related items. Participants were asked did they know about institutional delivery, health problems during labor and delivery, health complications for the mother-child during delivery, the importance of institutional delivery for the mother and child, and knowledge about the birth preparedness plan. Those participants who scored three and above were considered as having good knowledge and those who scored below three were categorized as having poor knowledge.20,21
Perception: This was measured when participants were asked to reflect on their opinion on ten items concerning institutional delivery using a Likert scale with a score ranging from 1= strongly disagree to 5= strongly agree. We used reverse scoring for the item “women do not go to a health facility for the delivery service because the health workers do not treat them respectfully including you”. Using the mean score as the cut-off point, above or equal to 3 was categorized as a positive perception and below 3 was categorized as having a negative perception of institutional delivery.19,20
Data Quality Assurance
To assure the quality of data, a structured, pre-tested, and interviewer administrative questionnaire was used. A pretest was done on 5% (31) of the study samples in Omoshora, which was out of the selected kebeles. The questionnaire was translated into the local language and back translated to the English language by language experts (person) to ensure its consistency. Close follow-up was done by supervisors and principal investigators throughout the data collection period. Two days of training were given for data collectors and supervisors and regular follow-up was done to check the collected data for its completeness, accuracy, and consistency throughout the data collection period.
Data Analysis
The data were checked, coded, and entered using Epi-Data 3.1 version software and then exported into SPSS version 24 for analysis. The wealth index was constructed using principal component analysis (PCA) by considering locally available household assets to assess the economic status of the household. The outcome variable was recoded to dichotomous outcomes whether they are involved or not. Those who were involved were coded as 1 and not involved were coded as “0”. Univariate analysis such as sample frequency, a measure of central tendency, and a measure of variability was used to describe the characteristics of participants. Bivariable regression analysis was done to see the association between the independent variable with the outcome variable. Independent variables with a p-value of <0.25 were considered a candidate for the multi-variable analysis to control confounding factors. Multi-collinearity was checked to see the linear correlation among the independent variables. The Hosmer-Lemeshow test was done to check the model goodness of fit. The adjusted odds ratio with 95% CI was estimated to show the strength and direction of the association. Finally, a variable with a p-value <0.05 in the final model (multivariable regression analysis) was considered statically significant.
Ethical Consideration
Ethical clearance was secured from Haramaya University, College of Health and medical science Institutional Health Research Ethics Review Committee (IHRERC). The official letter was written to the Hadiya zone health department and the Lemmo district health office before the data collection period began. The study purpose, procedure, possible risks, and benefits of the study were explained for each participant and written consent was obtained from each participant.
Results
Background Characteristics of Participants
Out of 614 expected participants, 583 of them were interviewed making a response rate of 95%. Near to half, 265 (45.5%) of the respondents were aged between 26 and 35. The mean age of the respondents was 35.6 (SD±8) years old. The majority of the participants, 576 (98.8%) were monogamous in their relationship status. About 479 (82.2%) participants were protestant in their religion and 474 (81.3%) were Hadiya in their ethnicity. The majority, 477 (81.8%) of the participants were a farmer in their employment status and 534 (91.6%) participants were rural dwellers. Two hundred forty-nine (42.7%) participants attended primary school. More than one-third of 224 (38.4%) participants had low economic status (Table 1).
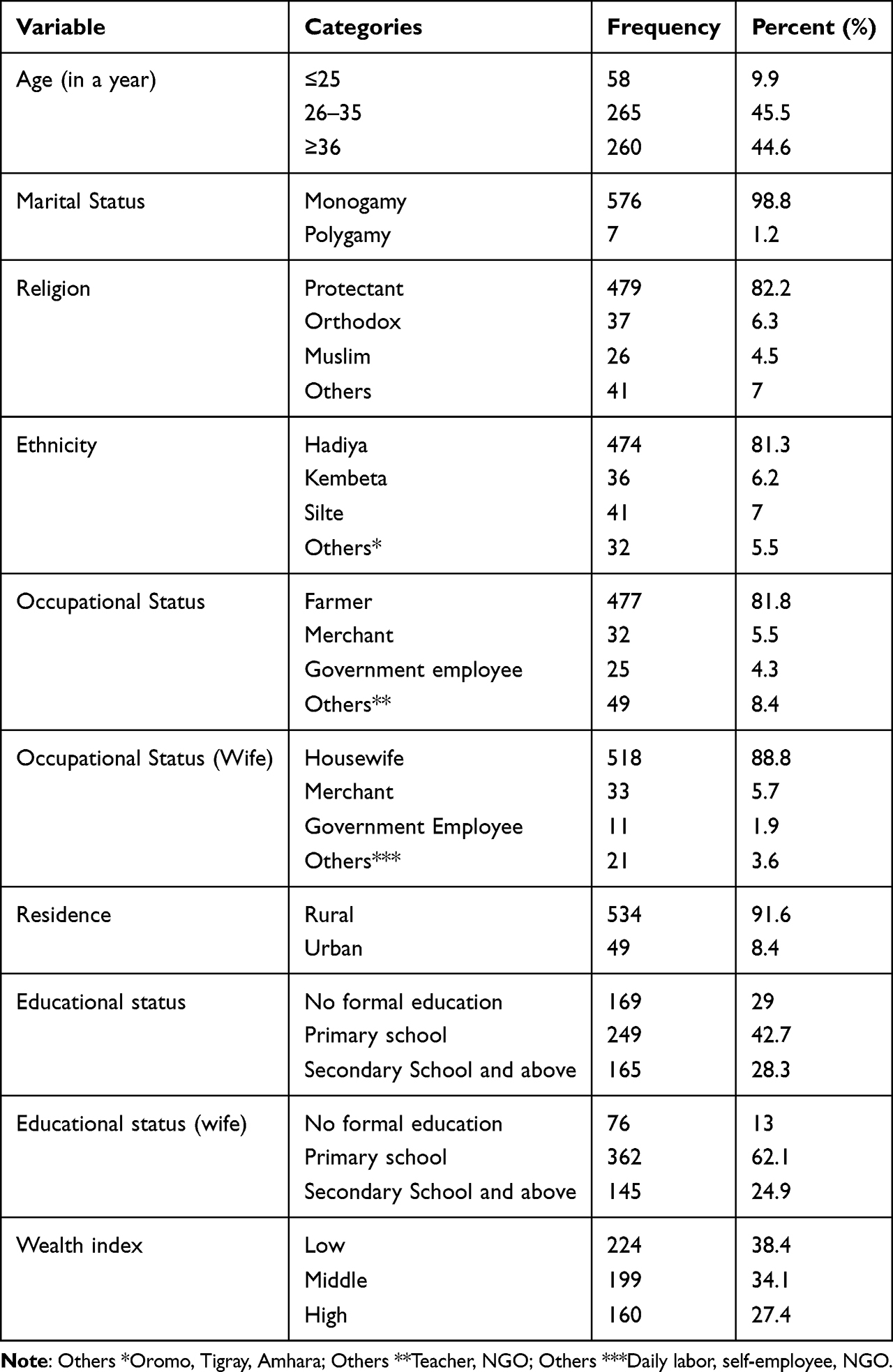 |
Table 1 Background Characteristics of Participants and Their Intimate Partners in Lemmo District, Southern Ethiopia, 2020 (N=583) |
Male Partner Involvement in Institutional Delivery
Among a total of 583 participants, 251 (43.1%, 95% CI: (39.2, 46.9)) of them were involved in the institutional delivery services of their spouses. More than one-third, 202 (34.6%) of participants had discussed with a health care provider about the delivery of their partners, 439 (75.3%) communicated with their relatives, 422 (72.4%) of the participants saved money for delivery expenses, 242 (41.5%) had arranged transportation during delivery, 19 (3.1%) arranged blood for donation and 221 (37.9%) participants decided and agreed to deliver their spouse in the health institution (Figure 1).
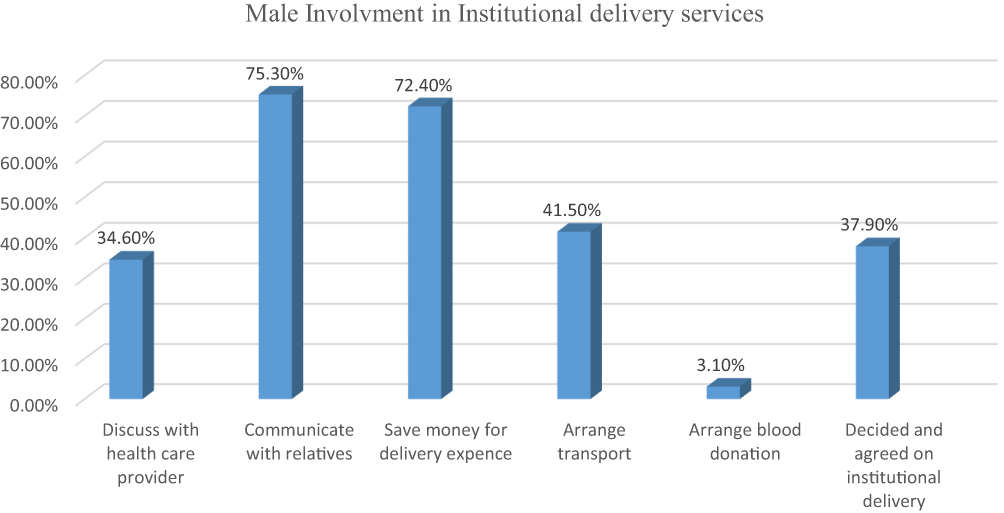 |
Figure 1 Male involvement in specific institutional delivery services in Lemmo district, Southern Ethiopia, 2020 (N= 583). |
Perception and Knowledge of Male Partners Towards Institutional Delivery
Among the total participants, 364 (62.4%) of them had good knowledge and 219 (37.4%) had poor knowledge about institutional delivery service. Out of this, 397 (68.09%) heard information about intuitional delivery, 382 (65.5%) know about the health problems that may happen during delivery, 444 (76.2%) have knowledge on the complication to child during birth, 241 (41.3%) know about birth preparedness plan, 478 (82%) and 203 (34.8%) know the importance of institutional delivery to the mother and child respectively. Regarding the perception of participants towards institutional delivery services, 351 (55.1%) had a positive perception and 262 (44.9%) had a negative perception. Out of this number, 338 (58%) either agreed or strongly agreed that pregnant women are risky for delivery-related complications, 317 (54.4%) either agreed or strongly agreed that delivery complication can be severe for mother, 340 (58.3%) either agreed or strongly agreed that delivery complication may be dangerous for a newborn, 328 (56.2%) either agreed or strongly agreed that attended by a skilled delivery attendant may be beneficial for the mother, 320 (54.8%) either agreed or strongly agreed that attended by a skilled delivery attendant may be beneficial for the newborn, 267 (45.8%) either agreed or strongly agreed that giving birth in a health facility is more important than home delivery, 214 (36.7%) either agreed or strongly agreed that discussion with the spouse is important to reduce delivery related risks, 319 (54.7%) either agreed or strongly agreed not to feel that communities consider you dominated by your wife if you follow your partner while accompanying her to a health facility for delivery service, and 245 (42%) either agreed or strongly agreed that women are not going to the institution due to the health care provider not treating the spouse and partner respectfully (Table 2).
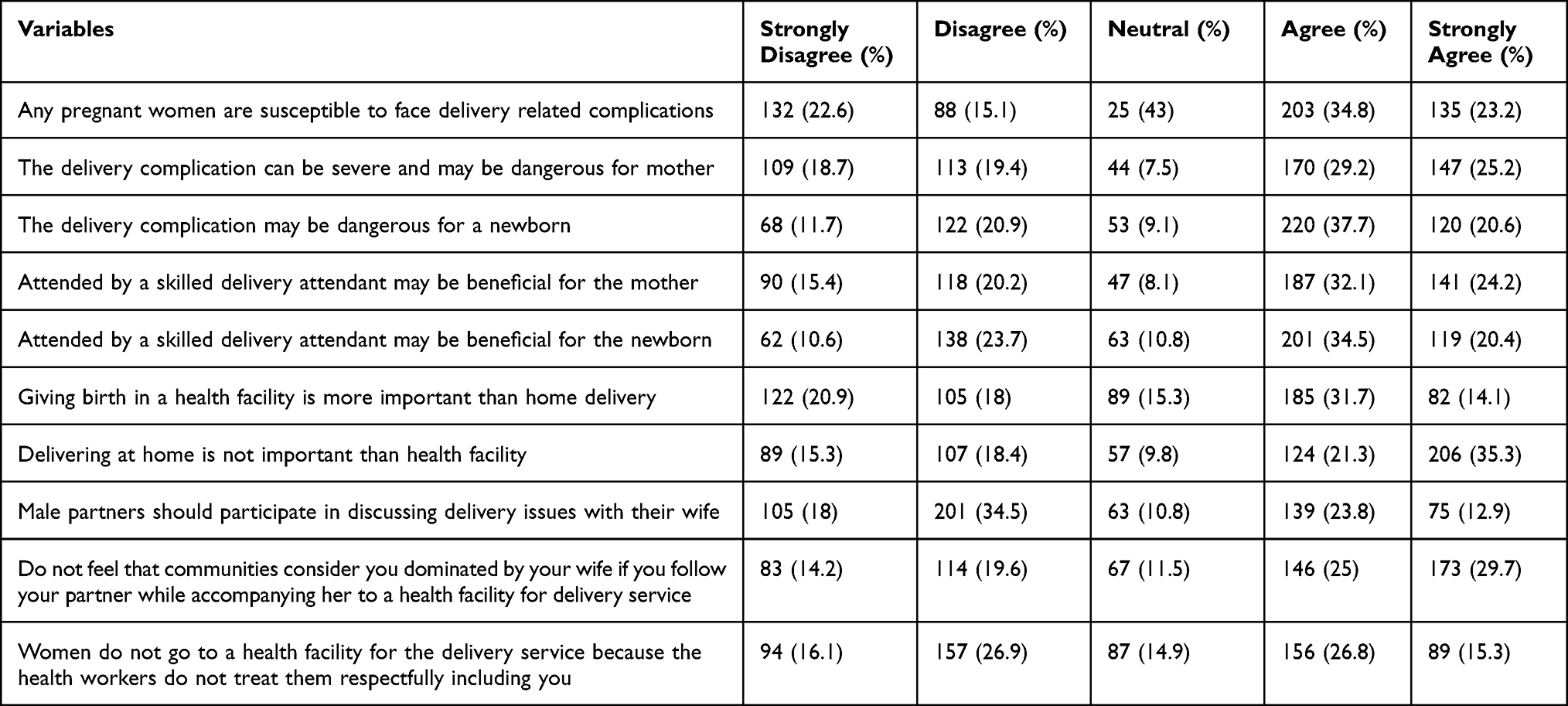 |
Table 2 Perception of Male Partner Towards Institutional Delivery Service in Lemmo District, Southern Ethiopia 2020 (N=583) |
Factors Associated with Male Partner Involvement in Institutional Delivery
In the binary logistic regression, age, educational status, residence, educational status of spouse, economic status of the household, knowledge, perception, birthplace of a child, and discussion with a spouse about institutional delivery services were associated factors with male involvement. Those whose age 25 years-old and below are 65% less involved in institutional delivery compared to those whose age is above 25 years old. Urban dwellers were 1.55 times more involved in institutional delivery compared to rural dwellers. Participants who attend primary school and secondary and above were 1.5 and 2.3 times more involved in institutional delivery respectively. Those who have middle- and high-income status were 1.3 and 1.4 times respectively more involved than those who have low-income status. Those who have good knowledge about institutional delivery were 2.48 times more involved than those who have poor knowledge. Participants who have positive attitude towards institutional delivery were 3.12 times more involved compares to those who have negative attitude. Those who discussed about institutional delivery with their partner were 2.64 times more involved compared to those who did not discuss with their partner.
In the final model (multivariable analysis) attending primary school and above, having good knowledge, having a discussion with the spouse, and having a positive perception towards institutional delivery services were significantly associated with male involvement. Those who attended primary school and secondary and above educational level were 2.1 and 2.4 times more likely to involve in institutional delivery services of their partner than those who did not attend formal education. Respondents who have good knowledge about institutional delivery were three times more likely involved compared to those who have poor knowledge. Those participants who have positive perceptions towards institutional delivery were 3.67 times more involved in the institutional delivery of their partner compared to those who have a negative perception. Those who discussed delivery-related information with their spouse were 1.99 times more involved in the institutional delivery of their spouse than those who did not discuss it with their partner (Table 3).
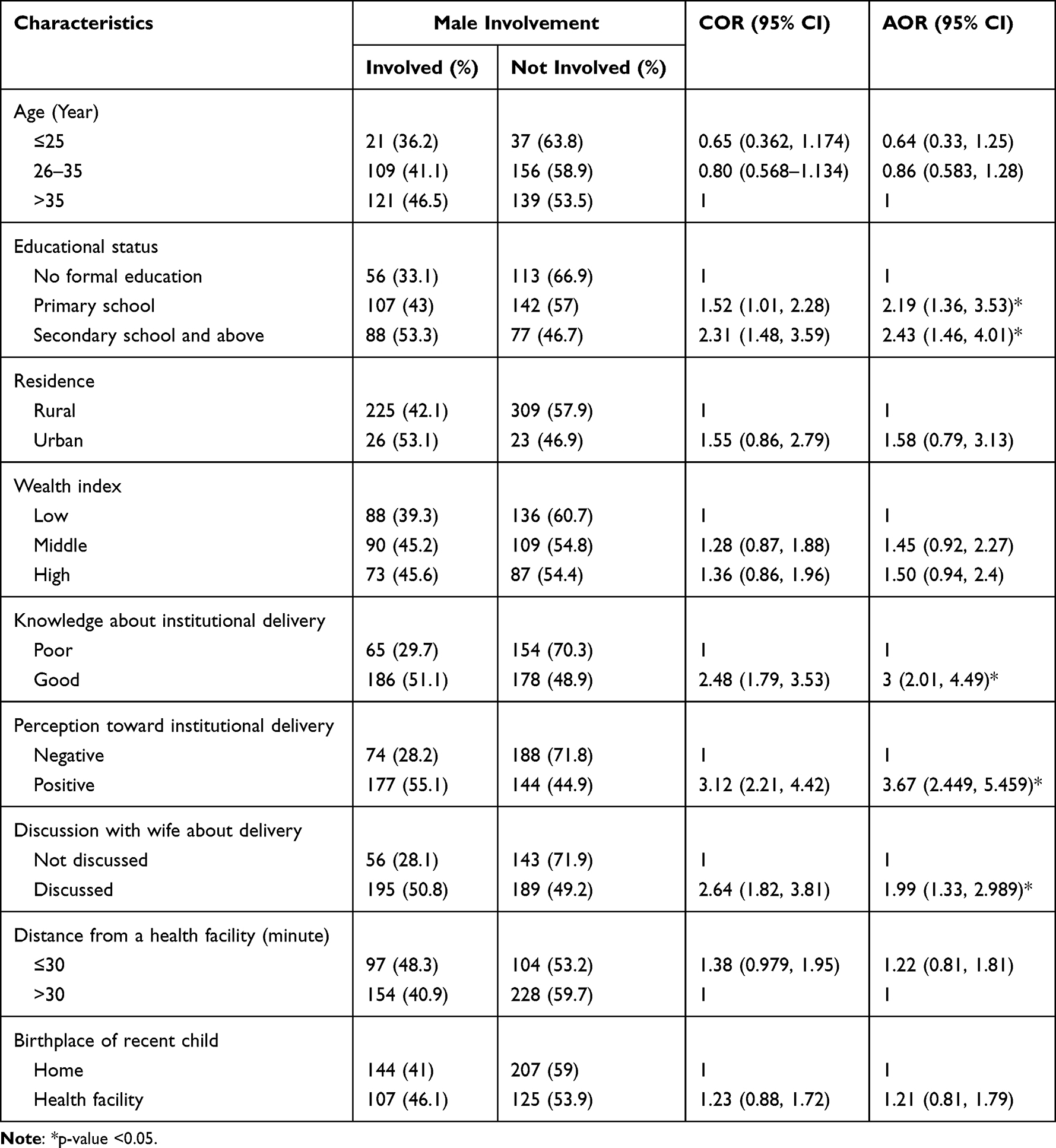 |
Table 3 Factors Independently Associated with Male Involvement in Institutional Delivery in Lemmo District, Southern Ethiopia, 2020 (N= 583) |
Discussion
Overall, 251 (43.1% (95% CI: (39.2, 46.9))) male partners were involved in the institutional delivery services of their partners. Educational level with primary school and above, having good knowledge, having a positive perception, and discussing institutional delivery services with their spouse were significantly associated factors with male partner involvement.
The finding of this study (43.1%) is in line with the study done in Mareka district (41.3%), Ambo (41.9%), Mombasa County (Kenya) (40.6%), inner-city communities in Ghana (44%), and central region of Ghana (44.5%).14,16–19 However, it is higher than from studies done in the Lemo district (38.2%), Tanzania (12%), and Northern Nigeria (32.1%).21–23 The difference might be due to the variation in the duration of the study, sample size, sampling method, and socio-culture of study subjects. For example, the study subjects of study in Tanzania were rural residents who might have less access to information and health facility compared to those urban residents. But this study includes both rural and urban dwellers which could be the reason for the difference in the magnitude of male involvement.
The finding is less than from studies done in Mekele (60%), Wolaita-Sodo (55%), Bangladesh (50%), and Myanmar (69.7%).15,24–26 The possible reason for the difference might be due to the study setting, and the socioeconomic level of the study subjects. For example, the participants in Ambo, Wolaita Sodo, and Mekele were urban residents which may have had better access to information and knowledge about institutional delivery services in addition to access to the health facility which may increase their involvement. But, the majority of the participants in this study were rural residents which might have a lack of information in addition to the distance and access to transportation may also become an obstacle for decreasing their involvement compared to the other studies. The other discrepancy may be also due to the duration of the study. For example, a study in Myanmar also included those who gave birth two years before the study period but this study includes only one year before the study period.
This study tried to assess factors associated with male involvement in the institutional delivery services of their spouses. Participants who attended primary school and, secondary school and above were 2.2 and 2.43 times more likely involved in institutional delivery services respectively compared to those who did not attend formal education. This is consistent with studies done in Nepal, Kenya, Ambo, Mareka, Myanmar, and Bangladesh.1,13,16,19,26,27 The possible reason might be due to those who attended primary school and above may have more knowledge and exposure to institutional delivery than those who did not attend formal education. Besides, an educated partner may not tend to hold on to the traditional belief, which greatly impairs inter-spousal communication, and they may positively influence health-seeking behavior to make the necessary decisions.
Participants who have good knowledge about institutional delivery services were three times more likely to be involved in institutional delivery services than those who have poor knowledge. This is consistent with the study done in Buska (Kenya), Mekelle, Ambo, Mombasa (Kenya), Maraka, and Wolaita-Sodo.1,13,15–17,19,24 The possible reason for this might be due to those who have good knowledge about institutional delivery services may have a better understanding and exposure to the consequences of home delivery on the health of mother and child compared to those who have poor knowledge.
Participants who have positive perception towards institutional delivery services were 3.7 times more involved compared to those who have negative attitude. This is supported by the findings done in Busia (Kenya), Mombasa county (Kenya), Mareka district, and Myanmar.13,17,19,26 The possible reason might be due to those who have a positive perception might have a better understanding of the importance of institutional delivery and the seriousness of the complications of home delivery. Whereas those male partners who have negative perceptions may pose a challenge to being involved in institutional delivery service. Those who have negative attitudes may not themselves be involved but they may also not allow their spouse to attend their antenatal care and other health services.
Participants who discussed with their spouses the delivery-related issues were two times more likely involved in institutional delivery service than those who did not discuss them with their partners. This is consistent with studies done in Nepal, Wolaita-Sodo, and Tiyo district (Oromiya region).10,24,28 The possible reason might be due to those who discussed delivery-related issues may have good experience in deciding about delivery and health care. This may also improve inter-spousal communication and increase their agreement which enhances institutional delivery service utilization.
In the multivariable model, age, residence, household wealth index, and distance from the health facility were not significantly associated with male involvement in institutional delivery service. This is contradicted by studies conducted in different areas.1,18,27,28 The possible reason for this might be due to nowadays health extension workers with the health development army and health care providers in collaboration with different non-governmental organization (NGO) are working on maternal and child health in institutional delivery services and danger signs during labor and childbirth by creating awareness about the importance of male involvements for all males at the community level.
Limitation
The knowledge question is not really an objective knowledge question, its perceived knowledge, a true knowledge measure would have items in which participant may indicate a correct answer. Discussion with spouse was also measured using a single item which needs further investigations. The authors recommend longitudinal study to investigate further on the knowledge, and discussion towards male involvement in institutional delivery.
Conclusions
Overall, more than two out of five partners were involved in the institutional delivery service of their spouses. Attending primary school and above, having good knowledge, positive perception, and discussing institutional delivery services with their spouse were significantly associated factors. Strengthening male partner involvement in Reproductive Health services and enhancing the culture of reproductive inter-spousal communication through couple counseling and peer-to-peer group sessions at a facility and community level are important measures.
Abbreviations
ANC, Antenatal care; MNH, Maternal and newborn health; MMR, Maternal mortality ratio; NMR, Neonatal mortality ratio; RH, Reproductive health; SRH, Sexual and reproductive health; WHO, World Health Organization.
Ethical Approval
The study was conducted following the declaration of Helsinki on human subjects. Ethical clearance was secured from Haramaya University Institutional Health Research Ethics Review Committee (IHRERC) and official permission was obtained from the Lemmo district health office and municipal. After the purpose, benefit and risk were briefed, informed consent was obtained from the study participants.
Acknowledgments
We would like to appreciate Haramaya University. Our heartfelt thanks also extend to the staff of Lemmo district, supervisors, data collectors, and the study participants for their willingness and cooperation in the data collection process.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflicts of interest.
References
1. Bhatta DN. Involvement of males in antenatal care, birth preparedness, exclusive breastfeeding and immunizations for children in Kathmandu, Nepal. BMC Pregnancy Childbirth. 2013;13(1):1. doi:10.1186/1471-2393-13-14
2. United Nations (UN). United Nations Population Information Network (POPIN) UN Population Division, Department of Economic and Social Affairs, with Support from the UN Population Fund (UNFPA): A/CONF.171/13: Report of the ICPD (94/10/18) (385k). United Nations (UN); 1994.
3. United Nations (UN). United Nations Report of the Fourth World Conference on Women. Beijing: United Nations (UN); 1995.
4. World Health Organization (WHO). Making Pregnancy Safer: The Critical Role of the Skilled Attendant a Joint Statement by WHO, ICM, and FIGO. Geneva: World Health Organization (WHO); 2004.
5. United Nations Population Fund (UNFPA). Engaging men and boys: a brief summary of UNFPA experience and lessons learned; 2013. Available from: https://www.unfpa.org/resources/engaging-men-and-boys-brief-summary-unfpa-experience-and-lessons-learned.
6. Davis J, Luchters S, Holmes W. Men and Maternal and Newborn Health: Benefits, Harms, Challenges and Potential Strategies for Engaging Men, Compass: Women’s and Children’s Health Knowledge Hub. Melbourne, Australia: Women’s And Children’s Health Knowledge Hub; 2013:1–28.
7. Comrie-Thomson L, Mariam T, Frances A, et al. Challenging gender inequity through male involvement in maternal and newborn health: a critical assessment of an emerging evidence base. Cult Health Sex. 2015;17:177–S189. doi:10.1080/13691058.2015.1053412
8. Tokhi M, Liz C, Jessica D, et al. Involving men to improve maternal and newborn health: a systematic review of the effectiveness of interventions. PLoS One. 2018;13(1):1–16. doi:10.1371/journal.pone.0191620
9. World Health Organization. WHO Recommendations on Health Promotion Interventions for Maternal and Newborn Health. Geneva, Switzerland: World Health Organization; 2015.
10. Thapa D, Niehof A. Women s autonomy and husbands’ involvement in maternal care in Nepal Social Science & Medicine Women’s autonomy and husbands’ involvement in maternal health care in Nepal. Soc Sci Med. 2013;93:1–10. doi:10.1016/j.socscimed.2013.06.003
11. Central Statistical Agency (CSA) [Ethiopia] and ICF. Ethiopia Demographic and Health Survey 2016: Key Indicators Report. Addis Ababa, Ethiopia, and Rockville, Maryland, USA: CSA and ICF; 2016.
12. United Nations International Children’s Emergency Fund (UNICEF). Monitoring the situation of children and women, neonatal mortality. 2018.
13. Nanjala M, Wamalwa D. Determinants of male partner involvement in promoting deliveries by skilled attendants in Busia, Kenya. Glob J Health Sci. 2012;4(2):60–67. doi:10.5539/gjhs.v4n2p60
14. Atuahene MD, Acquah SA, Atuahene NF, et al. Inclusion of men in maternal and safe motherhood services in inner-city communities in Ghana: evidence from a descriptive cross-sectional survey. BMC Pregnancy Childbirth. 2017;17(1):1–10. doi:10.1186/s12884-017-1590-3
15. Haftom G. Determinant factors of male involvement in birth preparedness and complication readiness at Mekelle Town; a community-based study. Sci J Public Health. 2015;3(2):175–180. doi:10.11648/j.sjph.20150302.14
16. Demissie DB. Involvement of male in antenatal care, birth preparedness and complication readiness and associated factors in Ambo Town. J Health Med Nurs. 2016;27(2):14–23. doi:10.11604/pamj.2014.19.349.5090
17. Onchong’a JM, Were T, Osero JOS. Knowledge, perception and level of male partner involvement in the choice of the delivery site among couples at Coast Level Five Hospital, Mombasa county, Kenya. Afr J Reprod Health. 2016;20(1):71–79. doi:10.1109/10.477697
18. Craymah JP, Oppong RK, Tuoyire DA. Male involvement in maternal health care at Anomabo, Central Region, Ghana. Int J Reprod Med Matern. 2017. doi:10.1155/2017/2929013
19. Zerihun T, Tizta T, Misra A. Male involvement on skilled delivery care utilization in Mareka Woreda, Southern Ethiopia: a community-based cross-sectional study. Sci J Public Health. 2015;3(5):699–706. doi:10.11648/j.sjph.20150305.26
20. Mitchell GT. Male involvement in maternal health decision-making in Nkwanta South District, Ghana. Univ Ghana. 2012;1(2):25.
21. Katiso NA, Adinew Y. Male partners’ involvement in institutional delivery in rural Ethiopia. J Womens Health Care. 2014;4(3):3–6. doi:10.4172/2167-0420.1000239
22. August F, Pembe AB, Mpembeni R, et al. Men’s knowledge of obstetric danger signs, birth preparedness and complication readiness in Rural Tanzania. PLoS One. 2015;10(5):1–12. doi:10.1371/journal.pone.0125978
23. Iliyasu Z, Abubakar IS, Galadanci IS, Aliyu MH. Birth preparedness, complication readiness and fathers’ participation in maternity care in a northern Nigerian community. Afr J Reprod Health. 2010;14(1):21–32. doi:10.4314/ajrh.v14i1.55773
24. Tadesse M, Boltena TA, Asamoah OB. Husbands’ participation in birth preparedness and complication readiness and associated factors in Wolaita Sodo town, Southern Ethiopia. Afri J Prim Health Care Fam Med. 2018;10(1):1–8. doi:10.4102/phcfm.v10i1.1471
25. Rahman AE, Perkins J, Islam S, et al. Knowledge and involvement of husbands in maternal and newborn health in rural Bangladesh. BMC Pregnancy Childbirth. 2018;18(247):1–12. doi:10.1186/s12884-018-1882-2
26. Wai KM, Shibanuma A, Oo NN, Fillman TJ, Saw YM. Are husbands involving in their spouses’ utilization of maternal care services ? A cross-sectional study in Yangon, Myanmar. PLoS One. 2015;10(12):e0144135. doi:10.1371/journal.pone.0144135
27. Bishwajit G, Tang S, Yaya S, et al. Factors associated with male involvement in reproductive care in Bangladesh. BMC Public Health. 2017;17(3). doi:10.1186/s12889-016-3915-y
28. Lingerhi W, Abebaye B, Ali I, et al. Magnitude and factors that affect males’ involvement in deciding partners’ place of delivery in Tiyo District of Oromia Region. Ethiop J Health Dev. 2014;28(1):6–13.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.