")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Factors Associated with Self‐reported Oral Health Among Community-Dwelling Older Adults in a Rural Province of Thailand
Authors Chantaraboot Y, Sermsuti-anuwat N
Received 20 August 2022
Accepted for publication 15 September 2022
Published 21 September 2022 Volume 2022:15 Pages 2111—2119
DOI https://doi.org/10.2147/JMDH.S386993
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Yaowapa Chantaraboot,1,2 Nithimar Sermsuti-anuwat3
1Master of Science Program in Geriatric Dentistry and Special Patients Care (International Program), Faculty of Dentistry, Chulalongkorn University, Bangkok, Thailand; 2Department of Dentistry, Phon Thong Hospital, PhonThong, Roi Et, Thailand; 3Academic Affairs Division, Faculty of Dentistry, Chulalongkorn University, Bangkok, Thailand
Correspondence: Nithimar Sermsuti-anuwat, Email [email protected]
Background: Limited research has focused on self-reported oral health in older Thai individuals.
Objective: We explored the factors associated with self-reported oral health among older adults residing in rural Thailand.
Methods: This cross-sectional study included males and females aged ≥ 60 years living in Phon Thong district, Roi Et province, a rural area in northeast Thailand. This community-based study was conducted between May 2021 and December 2021. A trained interviewer administered a face-to-face interview questionnaire. Study data were analyzed using descriptive statistics, Pearson’s chi-squared test, and binary logistic regression.
Results: In total, 249 older individuals completed the interviews. Most study participants were aged ≥ 67 years (55.8%), with a mean age of 66.92 years. Pearson’s chi-squared test showed statistically significant associations between self-reported oral health and age (P = 0.035) and chewing ability (P = 0.005). The multivariate binary logistic regression analysis revealed significant associations between self-reported poor oral health and older age (AOR = 0.290, 95% CI: 0.091– 0.925) and chewing discomfort (AOR = 4.032, 95% CI:1.119– 14.56). We observed no significant associations between self-reported oral health and sex, toothbrushing frequency, and speaking ability.
Conclusion: Younger respondents with chewing discomfort were more likely to self-report poor oral health. In rural areas, nonprofessional health providers can use a single-item self-reported oral health question as a simple tool for evaluating oral health status in the elderly. Moreover, dental health education programs are needed to help older individuals improve their oral self-care, access dental services, and achieve appropriate oral function. Such programs are essential for promoting good oral health in this population, particularly among “younger” elders.
Keywords: geriatric dentistry, oral function, oral health, health promotion, self‐reported oral health
Introduction
In 2019, the United Nations reported on the Ageing of the World Population that approximately 16%―one in six individuals worldwide―will be ≥ 65 years of age by 2050. The number of people aged ≥ 80 years has rapidly increased from 143 million to 426 million.1 Similarly, Thailand is becoming an aging society, with more than 10% of the population being over 60 years of age.2 Older Thais are at a higher risk of age-related health problems,3 chronic diseases, and noncommunicable diseases, including poor oral health.4–7
According to a report from the 8th Thai National Health Survey in 2017, older Thai adults aged 60–70 years had an average of 18.6 residual teeth, which decreased to 10 among those aged 80–85 years. Older individuals encounter numerous oral hygiene challenges; for example, physical limitations impede plaque control efforts, and chronic diseases may result in a decline in overall well-being.5–7 Healthcare providers should encourage the development of strategies to maximize oral health and prevent complications. Such strategies, particularly those associated with oral health-related behaviors, may improve oral health among older adults.8
The global self-rating of oral health is a single-item measure of self-rating individual’s oral health.9 Self-reported oral health is widely used in combination with other clinical indicators.10 These ratings consider experience, cultural values, quality of life, satisfaction, and effectiveness of the health care system.11–20 Previous studies have suggested that self-reported oral health activities help patients recognize the importance of regular dental care and their overall oral health status.11 Moreover, self-reported oral health is associated with self-assessment of various oral functions such as chewing and speaking.11–14
A 2019 examination of dental records obtained from the Dental Department of Phon Thong Hospital, Phon Thong district, Roi Et province, indicated poor oral hygiene among several older individuals of the community. Unfortunately, only few older adults visited the hospital for dental care.21 Limited studies have focused on self-reported oral health of older Thai adults residing in rural communities.
Therefore, we aimed to explore the factors associated with self-reported oral health among older individuals in a rural province of Thailand.
Materials and Methods
Study Design, Period, and Setting
This cross-sectional study was conducted between May 2021 and December 2021, at health-promoting community hospitals in Phon Thong district, Roi Et province, Thailand.
Study Subjects, Inclusion and Exclusion Criteria
The survey was conducted among community-dwelling older individuals living in Phon Thong district. The participants were invited by health providers from Phon Thong Health District Networks that work on health promotion for the community. We included healthy males and females aged ≥ 60 years. We excluded individuals with disabilities and severe chronic diseases, those unable to communicate in the Thai language, and those who were unwilling to participate.
Sample Size and Sampling Technique
The sample size assumed a two-sided test with a significance level of 0.05 and a power of 80%. We estimated that healthy older adults represented 79.3% of the total older population in Phon Thong district.21 The total number of participants required for the study was 249. Consecutive sampling was performed until we attained the target sample size.
Ethical Consideration
The study protocol and consent form were approved in accordance with the Declaration of Helsinki by the Ethics Review Committee of Chulalongkorn University, Faculty of Dentistry (HREC-DCU 2021–023). All participants provided written informed consent before participating in the study.
Study Variables
The independent variables of this study included participants’ background characteristics (age, sex, marital status, educational level, monthly income, dental health insurance, and history of systemic diseases); oral health-related behaviors (frequency and duration of toothbrushing, frequency of dental visits, smoking, alcohol consumption); and self-assessed oral functions (chewing and speaking abilities). The dependent variable was the participants’ self-reported oral health.
Data Measurements
The questionnaire was adapted from the standard oral health questionnaire for older adults by the Thailand Oral Health National Survey 2017.4 The Modified Oral Health Questionnaire comprises four parts. Part 1 consists of seven questions on the following variables: age (years), sex (male/female), marital status (married/other), education level (≤ primary education/> primary education), monthly income (< 15,000 Thai Baht/≥ 15,000 Thai Baht [$425]), having dental health insurance (Yes/No), and history of systemic disease (Yes/No). Part 2 consists of six oral health-related behavioral questions on the following variables: tooth brushing frequency (< twice daily/≥ twice daily), tooth brushing duration (< 2 min/≥ 2 min), regular dental visits (yes/no), smoking (yes/no), and alcohol consumption (yes/no). Part 3 consists of two oral function questions associated with chewing and speaking abilities: “How would you rate your chewing ability?” and “How would you rate your speaking ability?” Both questions were evaluated on a three-point scale; participants responded “comfortable”, “fair”, or “uncomfortable.” For the purpose of categorization during analysis, oral functions were self-categorized as “comfortable/fair” = “comfort” and “uncomfortable” = “discomfort.” Part 4 consists of a single-item self-reported oral health: “How would you rate your dental health?” This was assessed on a three-point scale (“good”, “fair”, or “poor”). For the purpose of categorization during analysis, self-reported oral health was categorized as “good/fair” = “good” and “poor” = “poor”.
Questionnaire Validity and Reliability
The item-objective congruence (IOC) index was analyzed for content validity of each questionnaire. The IOC involves separate item ratings according to their relevance to each objective. The IOC of the Modified Oral Health Questionnaire was 0.89, indicating an acceptable validity.
A pilot test was used to assess the reliability of the Modified Oral Health Questionnaire. This pilot study protocol was approved in accordance with the Declaration of Helsinki by the Research Ethics Review Committee of the Roi Et Province Health Office, Rot Et, Thailand (COE 0842563). In total, 30 individuals aged ≥ 60 years in Selaphum district (a nearby neighborhood) were included in the pilot study. A Cronbach’s alpha coefficient of 0.76 was obtained, indicating that the test had good reliability.
Reducing Bias During Interviews
The researchers trained an interviewer to conduct the interview survey over a 3-hour training program. During this training, questionnaire content and basic interview techniques―such as reading the questions as written with a suitable and gentle vocal tone and an appropriate explanation―were clarified. The interviewer had never met the participants before this study.
Data Analysis
All quantitative data were analyzed using SPSS software (version 28; SPSS Inc., IBM Company, Chicago, IL, USA). A statistically significant level (alpha) of 0.05 and a 95% confidence interval (CI) were used for the analysis. A P value of < 0.05 was considered statistically significant. Descriptive statistics included means, standard deviations, frequencies, and percentages. Pearson’s chi-squared test for homogeneity to compare the proportions of categorical variables. Variables with P values of < 0.25 were included in logistic regression analyses. The “enter” method of the binary logistic regression analysis was used. Bivariate analyses among self-reported oral health and sociodemographic characteristics, oral health-related behavior, and self‐assessment of oral functions were performed; independent variables with P values of <0.25 were included in the multivariate logistic regression analysis.
Results
Sociodemographic Characteristics of the Participants
Table 1 presents the distribution of related variables of 249 participants aged 60–74 years, with a mean age of 66.92 years. For categorical variables, most participants were female (77.5%), aged ≥ 67 years (55.8%), married (72.7%), had educational level of ≤ primary education (88.4%), had monthly income of < 15,000 Thai Baht (96.4%), and had dental health insurance (96.8%). Most participants reported a history of systemic diseases (69.1%). Regarding oral health-related behaviors, most of them reported the frequency of toothbrushing of ≥twice daily (87.6%), with toothbrushing duration of ≥ 2 min (83.5%), and irregular dental visits (96.4%) over the past 12 months. In addition, > 90.0% of participants denied habitual smoking or alcohol consumption. Regarding self-reported oral function, 45.8% of participants reported feeling comfortable chewing and 94.4% reported feeling comfortable speaking. Despite this, only 17.3% of participants self-reported good oral health.
 |
Table 1 Participants’ General Characteristics (N = 249) |
Factors Associated with Self-Reported Oral Health
As shown in Table 2, Pearson’s chi-squared test revealed statistically significant associations between self-reported oral health and age (P = 0.035) and chewing ability (P = 0.005). No statistically significant differences were observed between self-reported oral health and sex, marital status, educational level, monthly income, dental health insurance, history of systemic disease, frequency and duration of toothbrushing, frequency of dental visits, smoking, alcohol consumption, and speaking ability. Independent variables with P values of < 0.25 in chi-squared test were included in the binary logistic regression analyses (Table 3).
 |  | 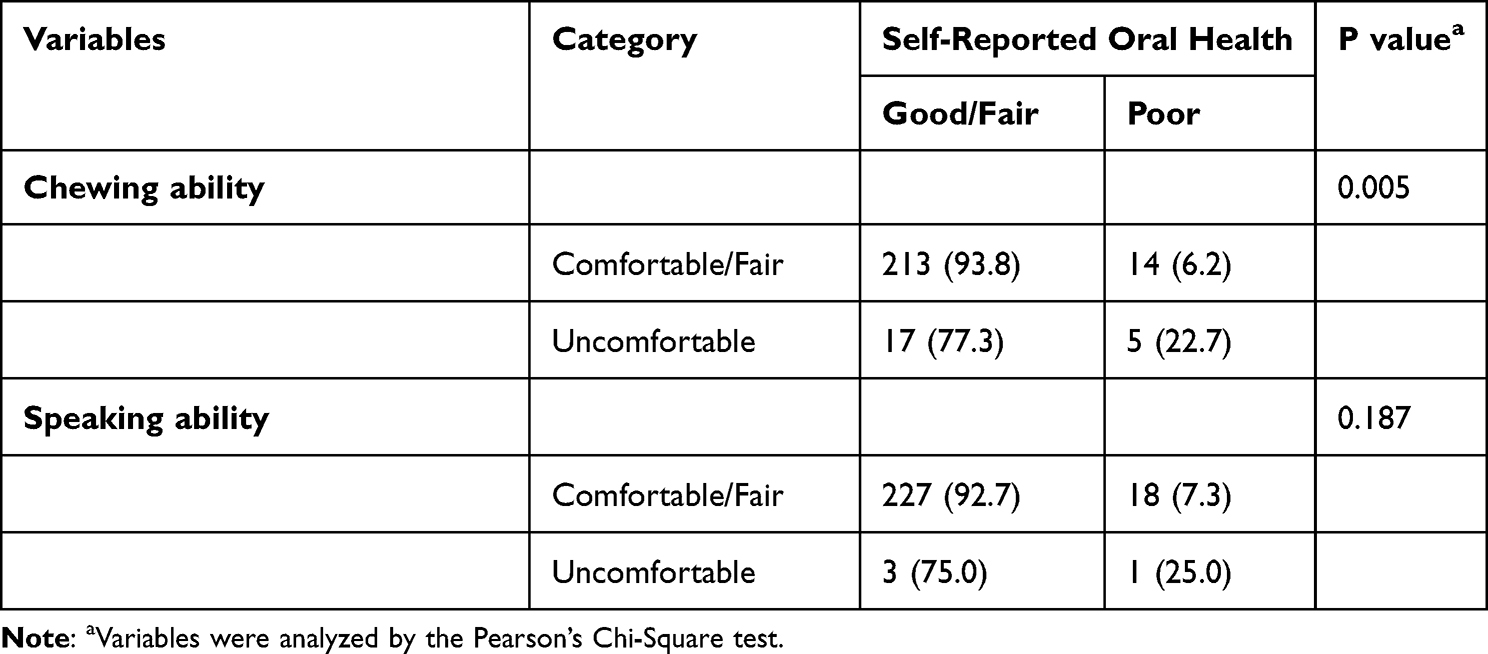 |
Table 2 Factors Associated with Self-Reported Oral Health (N = 249) |
 |
Table 3 Simple Bivariate and Multivariate Binary Logistic Regression Analyses of Self-Reported Oral Health of the Study Participants (N = 249) |
Factors Associated with Self-Reported Poor Oral Health
The unadjusted model indicated a P value of < 0.25 between self-reported poor oral health and age (P = 0.044), sex (P = 0.126), toothbrushing frequency (P = 0.245), chewing ability (P = 0.010), and speaking ability (P = 0.224). In the multivariate model, significant associations were observed between self-reported poor oral health and older age (AOR = 0.290, 95% CI: 0.091–0.925) and chewing discomfort (AOR = 4.032, 95% CI: 1.119–14.56). We observed no significant associations between self-reported oral health and sex, toothbrushing frequency, and speaking ability (Table 3).
Discussion
This study reflects the importance of self-reported oral health in community-dwelling older Thais. Younger participants who expressed chewing discomfort were more likely to self-report poor oral health. In particular, younger participants (≤ 67 years) were 3.45 times (1/0.29) more likely to self-report poor oral health than older participants (> 67 years). This might be because all study participants were considered “healthy” older individuals (60–74 years). Participants who were relatively “Younger” tended to be concerned about their oral health as they were in the early stages of “old age”, whereas those who were relatively older may have been more accepting of health declines, including oral health, according to their Buddhist culture in rural Thailand. This finding was consistent with that of an earlier Korean study that found younger participants were more likely to self-report worse oral health.14 Nevertheless, the findings of our study are discrepant with those of some previous studies. A Portuguese study found that older individuals (≥ 85 years) were more likely to have a lower self-perception of oral health than others.15 Other studies conducted in Japan,11 Bolivia,12 Brazil,16 Sri Lanka,17 and Norway18 found no association between age and self-reported oral health.
This study did not report a significant association between self-reported oral health and sex. This finding is consistent with that of earlier studies in Japan,11 Brazil,16 Sri Lanka,17 and Norway.18 However, previous studies by Ugarte et al11 and Nogueira et al19 reported a contrasting finding that females had significantly better self-perceived oral health than males.
Self-reported oral health is a comprehensive measure representing an individual’s overall experience within functional contexts.11–14 We found that participants who reported chewing discomfort were 4.032 times more likely to self-report poor oral health. Other studies have supported this finding; poor chewing ability was significantly associated with poor self-reported oral health in studies conducted in Japan,11 Bolivia,12 Australia13, and Korea.14 A single-item self-reported question can be used as an effective oral health screening tool in rural areas with limited access to healthcare practitioners and resources.10,20
Limitation of the Study
This cross-sectional study could not determine cause-effect relationships and focused on a single community; thus, our results may not be generalizable to other populations. Despite these limitations, we expect that our results can be useful for educational and preventive healthcare programs to prevent oral diseases among older Thais.
Conclusions
Younger participants who reported chewing discomfort were more likely to self-report poor oral health. In rural areas, nonprofessional health providers can use a single-item self-reported questionnaire as a simple tool for evaluating oral health status in older adults. Moreover, dental health education programs are needed to help older individuals improve their oral self-care, access dental services, and achieve appropriate oral function. Such programs are essential for promoting good oral health in this population, particularly among “younger” elders.
Abbreviations
AOR, adjusted odds ratio; CI, confidence interval; IOC, item-objective congruence index.
Data Sharing Statement
Study data are available from the authors upon reasonable request to the corresponding author.
Acknowledgment
The authors thank all participants and contributing people who helped facilitate this research.
Disclosure
The authors have no financial or nonfinancial competing interests concerning this study.
References
1. United Nations Department of Economic and Social Affairs Population Division. World population ageing 2019: highlights. Available from: https://www.un.org/en/development/desa/population/publications/pdf/ageing/WorldPopulationAgeing2019-Highlights.pdf.
2. National Statistical Office. Number of the elderly from survey of the older persons; 2017. Thai.
3. Woodham NS, Taneepanichskul S, Somrongthong R, et al. Effectiveness of a multidisciplinary approach intervention to improve blood pressure control among elderly hypertensive patients in rural Thailand: a quasi-experimental study. J Multidiscip Healthc. 2020;13:571–580. doi:10.2147/jmdh.s254286
4. Ministry of Public Health. National oral health survey of Thailand 2017; 2018. Available from: http://www.dent.chula.ac.th/upload/news/791/file_1_5834.pdf.
5. Piyakhunakorn P, Sermsuti-Anuwat N. The associations between oral health literacy and oral health-related behaviours among community-dwelling older people in Thailand. Glob J Health Sci. 2021;13(3):1. doi:10.5539/gjhs.v13n3p1
6. Piyakhunakorn P, Sermsuti-Anuwat N. The relationship between periodontitis and oral health literacy among the older people in Thailand. Glob J Health Sci. 2021;13(6):103. doi:10.5539/gjhs.v13n6p103
7. Sermsuti-Anuwat N, Piyakhunakorn P. Association between oral health literacy and number of remaining teeth among the Thai elderly: a cross-sectional study. Clin Cosmet Investig Dent. 2021;13:113–119. doi:10.2147/ccide.s306110
8. Razak PA, Richard KMJ, Thankachan RP, et al. Geriatric oral health: a review article. J Int Oral Health. 2014;6(6):110–116.
9. Locker D, Wexler E, Jokovic A. What do older adults’ global self-ratings of oral health measure? J Public Health Dent. 2007;65(3):146–152. doi:10.1111/j.1752-7325.2005.tb02804.x
10. Lundbeck HJ, Smith MB, Thomson WM. Clinical validity of self‐rated oral health among New Zealand nursing home residents. Gerodontology. 2020;37(3):253–257. doi:10.1111/ger.12458
11. Ugarte Cabo JL, Fukuda H, Abe Y, et al. Self-perceived oral health of the elderly in a rural area, Japan. Acta Med Nagasaki. 2006;51:89–94.
12. Ugarte J, Abe Y, Fukuda H, et al. Self-perceived oral health status and influencing factors of the elderly residents of a peri-urban area of La Paz, Bolivia. Int Dent J. 2007;57(1):19–26. doi:10.1111/j.1875-595x.2007.tb00114.x
13. Wright FAC, Law GG, Milledge KL, et al. Chewing function, general health and the dentition of older Australian men: the concord health and ageing in men project. Community Dent Oral Epidemiol. 2019;47(2):134–141. doi:10.1111/cdoe.12435
14. Moon JH, Heo SJ, Jung JH. Factors influencing self-rated oral health in elderly people residing in the community: results from the Korea community health survey, 2016. Osong Public Health Res Perspect. 2020;11(4):245–250. doi:10.24171/j.phrp.2020.11.4.14
15. Carvalho C, Manso AC, Escoval A, et al. Self-perception of oral health in older adults from an urban population in Lisbon, Portugal. Rev Saude Publica. 2016;50. doi:10.1590/s1518-8787.2016050006311
16. Martins AB, Dos Santos CM, Hilgert JB, et al. Resilience and self-perceived oral health: a hierarchical approach. J Am Geriatr Soc. 2011;59(4):725–731. doi:10.1111/j.1532-5415.2011.03350.x
17. Ekanayke L, Perera I. Factors associated with perceived oral health status in older individuals. Int Dent J. 2005;55(1):31–37. doi:10.1111/j.1875-595x.2005.tb00029.x
18. Dahl KE, Calogiuri G, Jönsson B. Perceived oral health and its association with symptoms of psychological distress, oral status and socio-demographic characteristics among elderly in Norway. BMC Oral Health. 2018;18(1). doi:10.1186/s12903-018-0556-9
19. Nogueira CMR, Falcão LMN, Nuto SDAS, et al. Self-perceived oral health among the elderly: a household-based study. Rev Bras Geriatr Gerontol. 2017;20(1):7–19. doi:10.1590/1981-22562017020.160070
20. Balasubramanian M, Keuskamp D, Amarasena N, et al. Predictors for oral and general health outcomes and quality of life among older people attending general practice clinics in South Australia. Gerodontology. 2021;38(4):395–403. doi:10.1111/ger.12534
21. Department of dentistry, Pone Thong district hospital. Dental report; 2019. Thai.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.