")
Back to Journals » Clinical Interventions in Aging » Volume 17
Falls Among Older Adults During the COVID-19 Pandemic: A Multicenter Cross-Sectional Study in Vietnam
Authors Nguyen HT , Nguyen CC, Le Hoang T
Received 16 July 2022
Accepted for publication 14 September 2022
Published 21 September 2022 Volume 2022:17 Pages 1393—1404
DOI https://doi.org/10.2147/CIA.S382649
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Nandu Goswami
Huan Thanh Nguyen, Chanh Cong Nguyen, Thien Le Hoang
Department of Geriatrics and Gerontology, University of Medicine and Pharmacy at Ho Chi Minh City, Ho Chi Minh city, Vietnam
Correspondence: Huan Thanh Nguyen, Department of Geriatrics and Gerontology, University of Medicine and Pharmacy at Ho Chi Minh City, 217 Hong Bang Street, Ward 11, District 5, Ho Chi Minh City, Vietnam, Tel +84-909097849, Email [email protected]
Purpose: We aimed to investigate the prevalence and factors associated with falls in older adult outpatients during the coronavirus disease (COVID-19) pandemic in Vietnam.
Patients and Methods: From February 2022 to June 2022, this cross-sectional study included 814 patients (aged ≥ 60 years; mean age 71.8 ± 7.3 years; women, 65.2%) attending three geriatric clinics for a comprehensive geriatric assessment. Self-reported fall events in the past 12 months and post-COVID-19 falls were assessed. Factors associated with falls were determined using logistic regression analysis.
Results: In total, 188 patients (23.1%) had falls (single fall, 75.5%; recurrent falls, 24.5%). The most frequent location, time, and circumstance of falls were the bedroom (43.1%), morning (54.3%), and dizziness (34.6%), respectively. Most patients experienced health issues after falls (bruise/grazes, 53.7%; fracture, 12.8%; immobility, 9.6%; hospital admission, 14.9%). In the adjusted model, factors associated with falls were being underweight (odds ratio [OR] 2.50, 95% confidence interval [CI] 1.37– 4.56, P = 0.003), limitations in instrumental activities of daily living (OR 2.03, 95% CI 1.05– 3.95, P = 0.036), poor sleep quality (OR 1.83, 95% CI 1.10– 3.05, P = 0.020), and fear of falling (OR 3.45, 95% CI 2.23– 5.33, P < 0.001). Among 357 COVID-19 infected patients, post-COVID-19 falls occurred in 35 patients (9.8%) and were associated with fear of falling (OR 3.14, 95% CI 1.18– 8.40, P = 0.023) and post-COVID-19 lower limb weakness (OR 2.55, 95% CI 1.07– 6.10, P = 0.035).
Conclusion: Our study found a substantial prevalence of falls among older outpatients during the COVID-19 pandemic in Vietnam. Management of factors associated with falls may be needed to reduce the burden of falls in the older population.
Keywords: falls, prevalence, Vietnam, COVID-19
Introduction
The coronavirus disease (COVID-19) pandemic has caused a major global communicable disease burden. Since the first COVID-19 cases were reported in January 2020,1 there have been four waves of the COVID-19 pandemic in Vietnam, a lower middle-income country in Southeast Asia.2 The Government of Vietnam has responded promptly and flexibly to achieve effective control of the pandemic through multiple policy tools and drastic measures, combined with launching the largest and fastest free vaccination campaign ever for the entire population of the country.3,4 According to the World Health Organization (WHO), in Vietnam, 10,749,324 confirmed COVID-19 cases with 43,088 deaths have been reported as of July 2022. Furthermore, a total of 228,484,003 COVID-19 vaccine doses have been administered, with 85,986,076 persons having received at least one dose and 78,872,470 persons being fully vaccinated.4
The COVID-19 pandemic has had a significant impact on the older population.5 Older individuals are more susceptible to COVID-19 and they are a vulnerable population group with a higher risk of complications and mortality as a result of age-related physiological alterations, immunosenescence, and comorbidities.6,7 In addition, the increased risk of virus infection, hospitalization, and associated fatal events has led to strict shelter-in-place lockdown restrictions in several countries, including Vietnam However, these measures can have adverse psychological effects on older adults due to the loss of social support, barriers to healthcare access, limited contact, and loneliness.8,9 Notably, as a result of social distancing and social isolation, older adults reported decreased time spent in physical activity and more sedentary behaviors,10 which may be associated with increased risk of disabilities and falls.11,12
Falls are commonly defined as inadvertently coming to rest on a lower level, excluding an intentional change in the position to rest on furniture, walls, or other objects.13 According to the WHO, falls are the world’s second leading cause of unintentional injury and mortality, and the frequency of falls increases with age.14 Cognitive impairment, reduced vision, neurologic changes, environmental hazards, and risky behaviors were considered common factors in the mechanisms that precipitate in falls in the older adults.15 This geriatric syndrome poses a considerable health issue in the older adult population with a variety of physical, psychological, and social consequences that require medical attention.13 In Vietnam, a previous study showed that falls occurred in 23.7% of outpatients aged ≥60 years.16 However, the patient enrollment for the previous study was conducted in 2018, before the COVID-19 pandemic. Therefore, the results of the previous study cannot reflect the impact of the pandemic on falls in older adults and the pattern of falls in COVID-19 infected older individuals. Furthermore, little is known about the burden of falls among older adults worldwide during the COVID-19 pandemic. Therefore, the present study aimed to determine the prevalence of all fall events among older outpatients during the COVID-19 pandemic in Vietnam as well as the prevalence of post-COVID-19 falls among COVID-19 infected older individuals. We also aimed to investigate the differences between the faller and non-faller groups and the COVID-19 infected and COVID-19 non-infected groups and identify the factors associated with all fall events and post-COVID-19 falls.
Patients and Methods
Study Design, Participants, and Data Collection
From February 2022 to June 2022, this cross-sectional study was conducted in outpatients aged ≥60 years at the geriatric clinics of three hospitals (Gia Dinh People’s hospital, Cho Ray hospital, and University Medical Center, Ho Chi Minh City, Vietnam). Patients with acute illness or serious mental condition were excluded. The study was carried out in accordance with the ethical principles stated in the Declaration of Helsinki. All the participants provided written informed consent. This study was approved by the Ethics Committee of the University of Medicine and Pharmacy at Ho Chi Minh City, Vietnam (reference number: 683/HĐĐĐ-ĐHYD). Data collection was performed during the clinic visit. Patients were physically examined and then instructed to complete a structured questionnaire after a careful explanation and personal interview with trained geriatricians. The caregivers were asked to ensure the correct reporting context. The demographic characteristics and comorbidities were obtained from interviews and electronic medical records. On an average, it took 30–40 min to complete an interview.
Assessment of Falls
Participants self-reported information on falls in the past 12 months, including the number of falls (one or more falls), location of falls (living room, bedroom, bathroom, staircase, kitchen, hallway/corridor, outside home, and others), circumstances of falls (dizziness, loss of balance, slippery surface, tripping, riding a bike/motorbike, and others), and health issues after falls (bruise/grazes, fracture, immobility, and hospital admission). Time of falls was divided into four hour categories: 5:00 am–12:00 pm, 12:00 pm–5:00 pm, 5:00 pm–11:00 pm, and 11:00 pm–5:00 am.
Independent Variables
The multimorbidity and polypharmacy data were collected from the current electronic medical records. Polypharmacy was defined as taking five or more medications. Multimorbidity was defined as the presence of two or more chronic diseases. Educational levels included pre-senior high school, senior high school, and tertiary education. Marital status was divided into three groups: married, widowed, and single/divorced. Alcohol consumption in the past 12 months was self-reported and classified as alcohol intake and non-alcohol intake. Decreased outdoor recreation (eg shopping, walking, fishing) was determined if the older adults reported spending less time outdoors than before the pandemic. Body mass index (BMI) was calculated by dividing the body weight (kg) with the square of the body height (m2). Bodyweight and height were measured following a standardized protocol using identical equipment. BMI was stratified as per the WHO’s guidelines for the Asia-Pacific region and defined as underweight (<18.5 kg/m2), normal weight (18.5–22.9 kg/m2), overweight (23.0–24.9 kg/m2), and obese (≥25 kg/m2).17
Functional status was self-reported using the Katz activities of daily living (ADLs) and Lawton instrumental ADLs indices. The ADLs include six tasks: bathing, dressing, toileting, transferring, continence, and feeding. The instrumental ADLs include eight tasks: using the telephone, preparing food, shopping, housekeeping, doing laundry, using transportation, handling medications, and handling finances.18,19 Older adults were coded as having limitations in ADLs or instrumental ADLs if they were unable to complete one or more tasks by themselves. Fear of falling was assessed by the Falls Efficacy Scale-International (FES-I) with 16 questions related to functional tasks and social aspects of falls. A total score of >23 indicates fear of falling.20 Frailty was screened by the Program of Research to Integrate Services for the Maintenance of Autonomy 7 (PRISMA-7) questionnaire with seven dichotomous questions, each scoring 0 or 1 point. A total score of ≥3 was considered indicative of frailty.21 Depressive disorder was evaluated using the 15-item geriatric depression scale (GDS). A total score of ≥5 was considered to indicate depression.22 Sleep quality was assessed by the Pittsburgh sleep quality index (PSQI). A total score of ≥5 indicates poor sleep quality.23
COVID-19 infected participants self-reported post-COVID-19 medical conditions, including fatigue, attention disorder, headache, hair loss, dyspnea, lower limb weakness, and decreased physical activity (compared to those before the COVID-19 infection). Time from COVID-19 infection to study enrolment was divided into <3 months and ≥3 months.
Sample Size Calculation
Sample size was calculated using a single population proportion formula: n = Z21- α/2*(p*[1-p]/d2), with n = required sample size, Z1- α/2 = 1.96 (with α = 0.05 and 95% confidence interval), p = prevalence of falls in older adults, and d = precision (assumed as 0.03). A previous study showed that falls occurred in 23.7% of older outpatients in Vietnam.16 Therefore, the required sample size for this study was a minimum of 810 participants with an allowable margin of error of 5%.
Statistical Analyses
All the collected data were analyzed using IBM SPSS Statistics, version 25 (IBM Corp., Armonk, N.Y., USA). Categorical variables were described as frequencies and percentages (%). Continuous variables were expressed as means and standard deviations. To perform between-group comparisons of baseline characteristics, all the participants were divided into the faller group and the non-faller group or the COVID-19 infected group and the COVID-19 non-infected group. Comparisons between two groups were conducted using the chi-square test or Fisher’s exact test for categorical variables and Student’s t-test for continuous variables. Univariate logistic regression was performed on the potential factors associated with falls. Variables with P values <0.2 in the univariate analysis were selected for multivariate logistic regression. All variables were examined for interaction and multicollinearity. Odds ratio (OR) was calculated with 95% confidence interval (95% CI). Statistical significance was defined as a two-tailed value of P <0.05.
Results
Prevalence of Falls and Baseline Characteristics of Participants
Of the 821 patients assessed for eligibility, 7 patients were excluded due to acute illness (5 patients) and serious mental condition (2 patients). Supplementary Figure S1 shows the flow diagram for the study participants. Among the 814 patients included in this study, there were 188 reported falls (23.1%). Table 1 summarizes the baseline characteristics of the participants by falls. The faller group was significantly older, had female predominance, lower BMI, higher rates of using psychotropic drugs, polypharmacy, multimorbidity, decreased outdoor recreation time, limitations in ADLs and instrumental ADLs, depression, frailty, poor sleep quality, and fear of falling than the non-faller group. Hypertension, stroke, and osteoarthritis were more frequently reported in the faller group. Of the 357 COVID-19 infected patients, total fall events and post-COVID-19 falls were reported in 84 (23.5%) and 35 patients (9.8%), respectively. Table 2 summarizes the baseline characteristics of the patients by COVID-19 infection. There was no significant difference in the rate of total falls between the COVID-19 infected and non-infected groups.
 |
Table 1 Baseline Characteristics of Participants According to Falls |
 |
Table 2 Baseline Characteristics of Participants According to COVID-19 Infection |
The COVID-19 infected patients were assigned to a post-COVID-19 faller or post-Covid-19 non-faller group. Table 3 compares the characteristics of the post-COVID-19 conditions between the two groups. The rate of COVID-19 related hospitalization was significantly higher in the post-COVID-19 faller than in the post-Covid-19 non-faller group. Post-COVID-19 conditions were more significantly prevalent in the post-COVID-19 faller group than in the post-Covid-19 non-faller group. The three most common post-COVID-19 conditions were fatigue, lower limb weakness, and decreased physical activity. Compared to the post-Covid-19 non-faller group, the post-COVID-19 faller group exhibited significantly higher rates of attention disorder, lower limb weakness, and decreased physical activity.
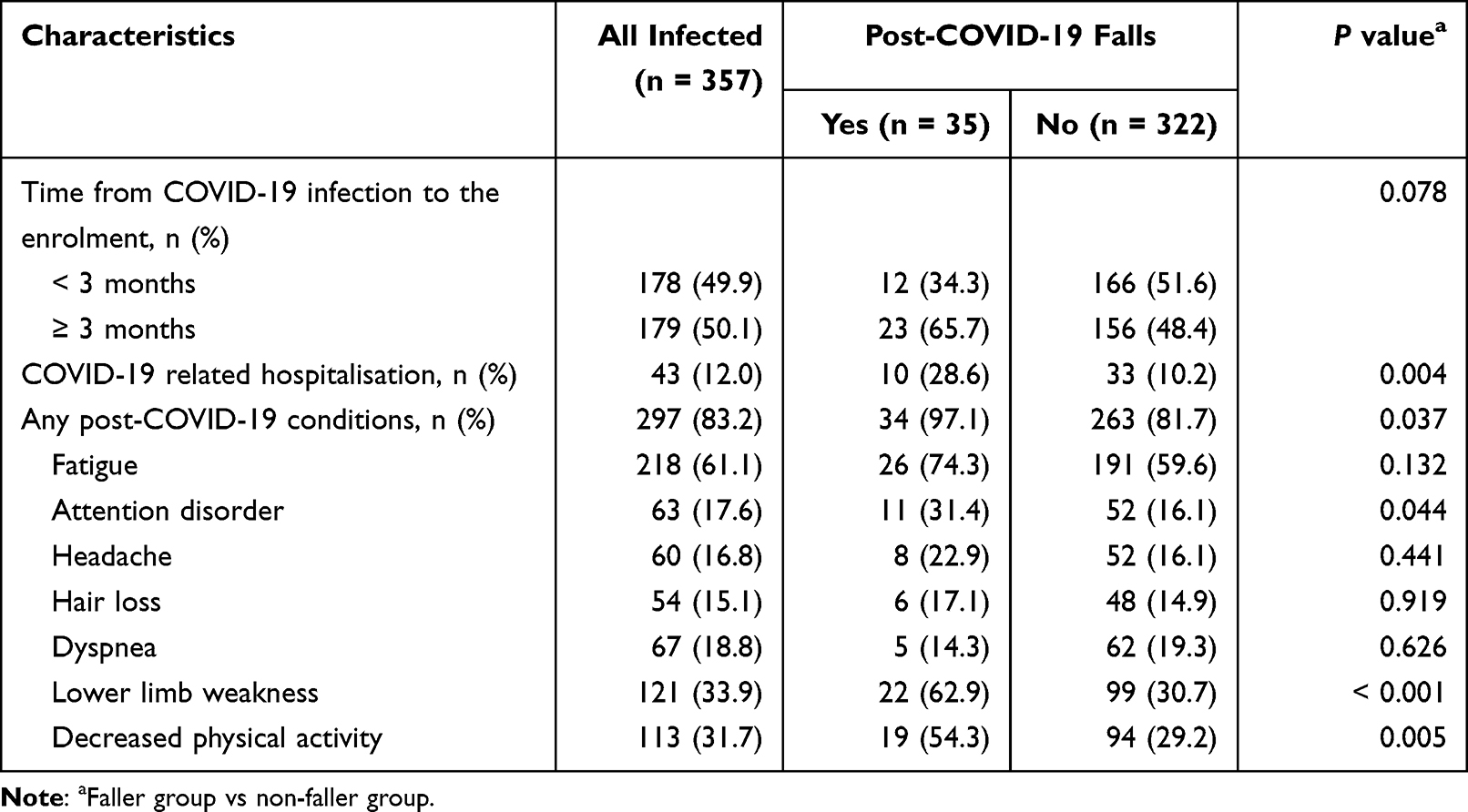 |
Table 3 Characteristics of Post-COVID-19 Conditions According to Post-COVID-19 Falls |
Characteristics of Falls
The characteristics of falls by history of COVID-19 infection are shown in Table 4. Among 188 fallers, a single fall was three times greater than recurrent falls. In our study, no participant reported falling in the living room or kitchen. The most frequently reported site of falls was the bedroom. The most frequent circumstances associated with falls were dizziness and a slippery surface. Approximately two-thirds of fallers experienced at least one health issue after the fall, and the most frequent was bruise/grazes. While the majority of total fall events occurred in the morning, most of the post-COVID-19 falls occurred in the bedtime.
 |
Table 4 Characteristics of Falls According to COVID-19 Infection |
Factors Associated with Falls
Logistic regression analyses were performed to identify the potential factors associated with falls in the study population (Table 5) and post-COVID-19 falls in the COVID-19 infected patients (Table 6). In the adjusted model, four factors that increased the odds of falls were being underweight, limitations in instrumental ADLs, poor sleep quality, and fear of falling. Among COVID-19 infected patients, besides fear of falling, the other post-COVID-19 condition associated with post-COVID-19 falls was lower limb weakness.
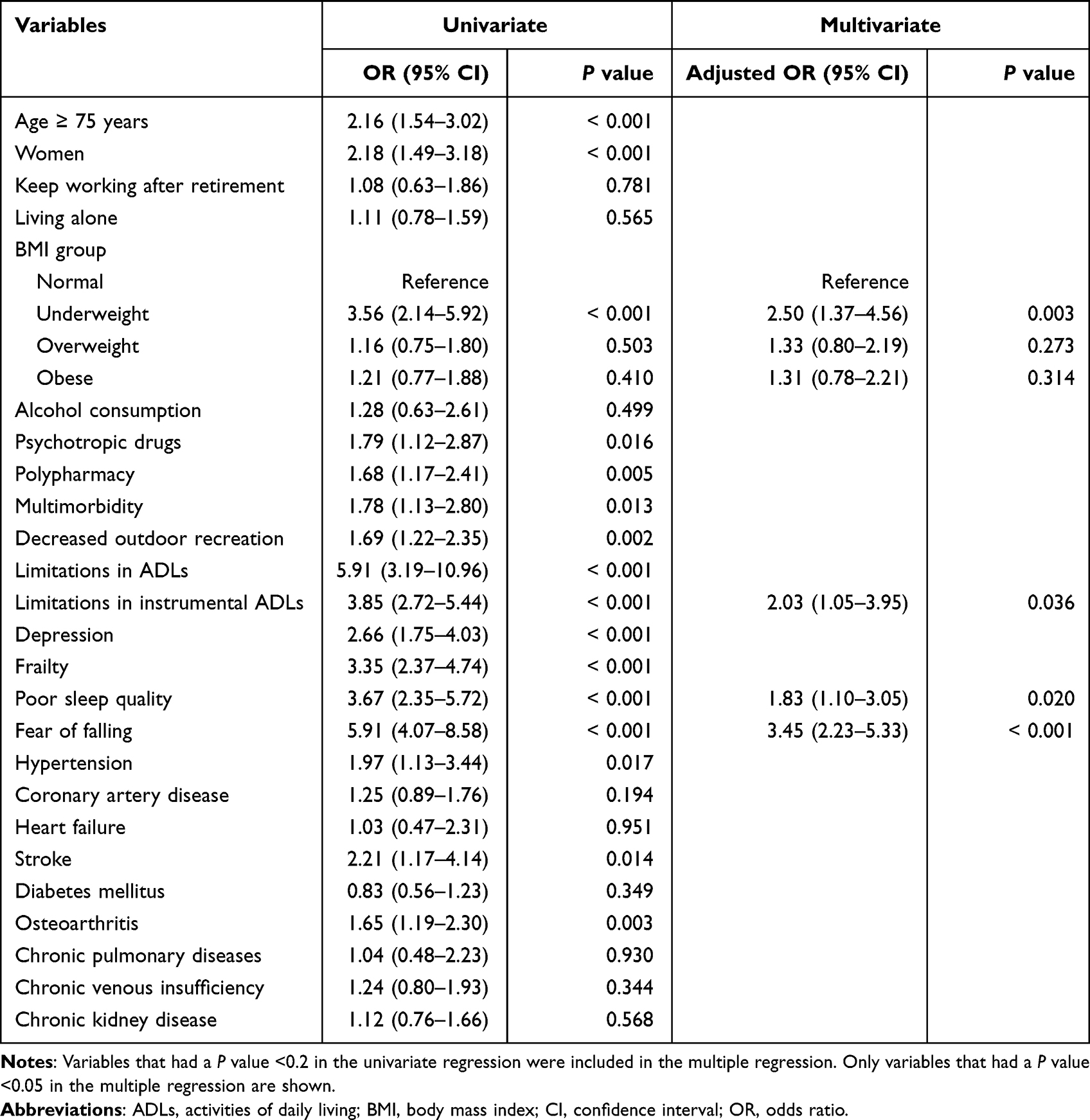 |
Table 5 Factors Associated with Falls (n = 814) |
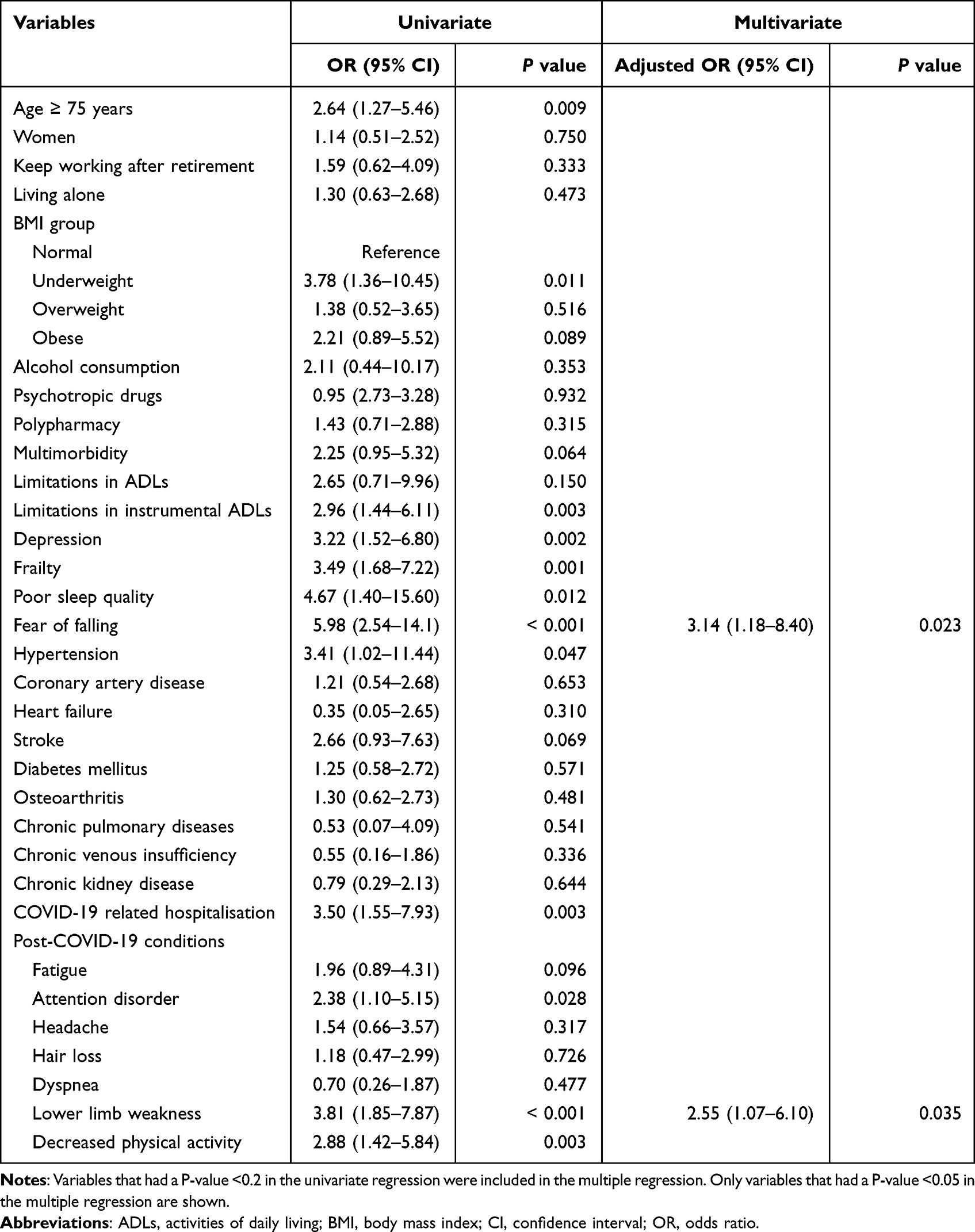 |
Table 6 Factors Associated with Post-COVID-19 Falls (n = 357) |
Discussion
Older adults worldwide have been negatively affected during the global spread of COVID-19.5,6 While many COVID-19 related consequences have been studied, there is a lack of published studies showing the burden of falls among the older population during the pandemic. A previous study predicted that the COVID-19 pandemic may lead to an increase in fall events as a consequence of less physical activity in older adults during the pandemic.24 This hypothesis is consistent with the findings in the older population in developed countries where one-third of American older adults reported a decrease in the daily time spent on their feet after the start of the COVID-19 pandemic, with falls occurring more frequently in these individuals.12 In Vietnam, the third wave of the COVID-19 was the most serious outbreak, which started in January 2021 due to the alpha variant, followed by the fast-spreading fourth wave due to the delta variant from April 2021.2 Supplementary Figure S2 shows the four waves of the COVID-19 pandemic in Vietnam. Our study found that 23.1% of older adults visiting geriatric clinics experienced falls in the community during the two severe COVID-19 outbreaks. Since the prevalence of falls among Vietnamese geriatric outpatients before the pandemic was 23.7%,16 our results suggest that there was no trend of increasing falls in this population during the pandemic.
We assume that at least two factors are related to the steady prevalence of falls in Vietnam. First, in our study, although the fallers had less outdoor recreation time than the non-fallers, this was not a significant factor associated with falls. This may be explained by the habits of older adults as reported in the Longitudinal Study of Ageing and Health in Vietnam, in which only one-third of older adults performed physical activities and most of the daily activities were indoors.25 For this reason, decreased outdoor recreation, such as walking outside or shopping may not influence the likelihood of falls in Vietnamese older adults, since they indulge in more indoor exercises, such as gardening or walking around their houses. However, further studies are needed to clarify the impact of the different types and levels of indoor physical activities on falls among older adults during the COVID-19 pandemic. Second, unlike families in developed countries, the majority of families in Vietnam have many generations living together and the older adults are cared for by their offspring and relatives. During social distancing, the younger members also stayed at home and likely gave more assistance and care to the older ones. In agreement with this notion, our study found that no older adults had falls in the gathering places of the house, such as the living room or kitchen.
Our study highlights the bedroom as a high-risk area for falls, while dizziness was the most commonly reported circumstance preceding falls in older adults during the COVID-19 pandemic. These findings are in contrast to those of a previous study performed in Vietnam before the pandemic that revealed that the bathroom was the most unsafe location carrying a risk of falls, due to circumstances such as a slippery surface.16 The differences may reflect the impact of the COVID-19 pandemic on both extrinsic and intrinsic factors related to falls in older adults. While staying at home during social distancing may have given the family members more time for home-modification interventions that make the house safer, the pandemic was a barrier to physical activity in older adults for maintaining their well-being.12 This may explain the notable rate of falls related to physical conditions, such as dizziness and loss of balance, among older adults in our study. Furthermore, while the older adults may receive more care from family members in the gathering places, they may have less support in their bedroom, leading to more than half of the participants in our study experiencing falls in this location. Importantly, among the falls that occurred in the bedroom, the most frequent time of occurrence was waking-up time in the morning and the most frequent circumstances associated with falls were dizziness and loss of balance (Supplementary Table S1). Taken together, our findings suggest that the COVID-19 pandemic may not have increased the prevalence of falls but may have changed the patterns of falls in the older population. Suitable strategies for fall prevention may be required specifically in the bedroom and in the morning as they are the most frequent place and time of falls, respectively, in addition to balance training referral for older adults during COVID-19 related social distancing.
Several personal and environmental factors associated with falls in older adults have been identified.16,26,27 Some of these factors can be controlled, which may reduce the risk of having a fall.28–30 Our study identified being underweight, limitations in instrumental ADLs, poor sleep quality, and fear of falling as factors associated with falls in older adults during the COVID-19 pandemic. The evidence on the relationship between the BMI categories and risk of falls is conflicting in the published literature, which may be related to the different cutpoints of BMI.31–33 In our study, consistent with two previous studies, underweight was defined as BMI <18.5 kg/m2,32,33 and it was shown that older adults experiencing falls were more likely to be underweight than older individuals without falls. The mechanism of a lower BMI preceding falls is not fully understood but is likely to be related to sarcopenia in older adults with decreased BMI.34 Besides BMI, we found limitations in instrumental ADLs as an important geriatric factor associated with falls. It may be explained by the fact that a functional decline can negatively impact skeletal muscle integrity resulting in an increased risk of falls.35 Previous studies have yielded consistent results with regard to a link between inadequate sleep and greater risk of falling in older adults.36,37 Poor sleep quality can lead to impaired daytime functioning, poor cognitive performance, and balance disorders, thereby resulting in falls in older adults.38,39 Although fear of falling was considered as a predictor of falling,40 the cause-consequence relationship between them is likely bidirectional because fall events can also lead to fear of falling.41 In clinical practice, geriatricians who attend to older adults with fear of falling should evaluate them for falls and vice versa.
To our knowledge, this is the first study to demonstrate that post-COVID-19 falls were associated with post-COVID-19 lower limb weakness. A decrease in muscle strength was reported as an initial and common symptom in COVID-19 infected individuals.42 Although the mechanism of muscular involvement in COVID-19 remains unclear, it might be indirectly related to the adverse effects of the inflammatory process induced by COVID-19 in the musculoskeletal tissue.43 Since a previous meta-analysis has demonstrated that decreased lower-limb muscle strength is a factor associated with an increased risk of falls in older adults,44 post-COVID-19 lower limb weakness should be assessed and managed in COVID-19 infected older adults.
Our study has several limitations. First, there was a lack of information on the symptoms in the acute phase of the COVID-19 illness, as well as symptom severity and COVID-19 vaccination status. Second, we only assessed some post-COVID-19 conditions; thus, the impact of other symptoms on falls could not be identified. Third, since lower limb weakness was self-reported and no assessment was completed with a dynamometer, the cut-off values of muscle strength related to falls could not be determined. Fourth, due to cultural issues, the results of our study may not reflect the total burden of falls in other countries. Finally, due to the cross-sectional nature of the study design, we could not evaluate the causal relationship between falls and the associated factors.
Conclusions
This is the first study to determine the prevalence of falls among older adults during the COVID-19 pandemic in Vietnam. We found no trend of increasing falls in this population, but the pattern of falls may have changed during the pandemic. In COVID-19 infected older individuals, post-COVID-19 lower limb weakness was associated with falls and should be a consideration for screening.
Data Sharing Statement
The dataset used and analyzed in the current study is available from the corresponding author on reasonable request.
Acknowledgments
We thank the patients for their participation in our study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Phan LT, Nguyen TV, Luong QC, et al. Importation and human-to-human transmission of a novel coronavirus in Vietnam. N Engl J Med. 2020;382(9):872–874. doi:10.1056/NEJMc2001272
2. Minh LHN, Khoi Quan N, Le TN, Khanh PNQ, Huy NT. COVID-19 timeline of Vietnam: important milestones through four waves of the pandemic and lesson learned. Front Public Health. 2021;9:709067. doi:10.3389/fpubh.2021.709067
3. Le TT, Vodden K, Wu J, Atiwesh G. Policy responses to the COVID-19 pandemic in Vietnam. Int J Environ Res Public Health. 2021;18(2):559. doi:10.3390/ijerph18020559
4. The World Health Organization [homepage on the Internet]. WHO Coronavirus (COVID-19) Dashboard: Viet Nam Situation. Available from: https://covid19.who.int/region/wpro/country/vn.
5. Lebrasseur A, Fortin-Bedard N, Lettre J, et al. Impact of the COVID-19 pandemic on older adults: rapid review. JMIR Aging. 2021;4(2):e26474. doi:10.2196/26474
6. Singhal S, Kumar P, Singh S, Saha S, Dey AB. Clinical features and outcomes of COVID-19 in older adults: a systematic review and meta-analysis. BMC Geriatr. 2021;21(1):321. doi:10.1186/s12877-021-02261-3
7. Nikolich-Zugich J, Knox KS, Rios CT, Natt B, Bhattacharya D, Fain MJ. SARS-CoV-2 and COVID-19 in older adults: what we may expect regarding pathogenesis, immune responses, and outcomes. Geroscience. 2020;42(2):505–514. doi:10.1007/s11357-020-00186-0
8. Le XTT, Dang AK, Toweh J, et al. Evaluating the psychological impacts related to COVID-19 of Vietnamese people under the first nationwide partial lockdown in Vietnam. Front Psychiatry. 2020;11:824. doi:10.3389/fpsyt.2020.00824
9. Do BN, Nguyen PA, Pham KM, et al. Determinants of health literacy and its associations with health-related behaviors, depression among the older people with and without suspected COVID-19 symptoms: a Multi-Institutional Study. Front Public Health. 2020;8:581746. doi:10.3389/fpubh.2020.581746
10. Yamada M, Kimura Y, Ishiyama D, et al. Effect of the COVID-19 epidemic on physical activity in community-dwelling older adults in Japan: a cross-sectional online survey. J Nutr Health Aging. 2020;24(9):948–950. doi:10.1007/s12603-020-1501-6
11. Klenk J, Kerse N, Rapp K, et al. Physical activity and different concepts of fall risk estimation in older people–results of the ActiFE-Ulm study. PLoS One. 2015;10(6):e0129098. doi:10.1371/journal.pone.0129098
12. Hoffman GJ, Malani PN, Solway E, Kirch M, Singer DC, Kullgren JT. Changes in activity levels, physical functioning, and fall risk during the COVID-19 pandemic. J Am Geriatr Soc. 2022;70(1):49–59. doi:10.1111/jgs.17477
13. The World Health Organization. WHO global report on falls prevention in older age; 2007.
14. The World Health Organization. Step Safely: Strategies for Preventing and Managing Falls Across the Life-Course. Geneva: World Health Organization; 2021. Licence: CC BY-NC-SA 3.0 IGO
15. Fuller GF. Falls in the elderly. Am Fam Physician. 2000;61(7):2159–2168, 2173–2154.
16. Ha VT, Nguyen TN, Nguyen TX, et al. Prevalence and factors associated with falls among older outpatients. Int J Environ Res Public Health. 2021;18(8):4041. doi:10.3390/ijerph18084041
17. Consultation WHOE. Appropriate body-mass index for Asian populations and its implications for policy and intervention strategies. Lancet. 2004;363(9403):157–163. doi:10.1016/S0140-6736(03)15268-3
18. Shelkey M, Wallace M. Katz index of independence in activities of daily living. J Gerontol Nurs. 1999;25(3):8–9. doi:10.3928/0098-9134-19990301-05
19. Graf C. The Lawton instrumental activities of daily living scale. Am J Nurs. 2008;108(4):52–62; quiz 62–53. doi:10.1097/01.NAJ.0000314810.46029.74
20. Hauer K, Yardley L, Beyer N, et al. Validation of the falls efficacy scale and falls efficacy scale international in geriatric patients with and without cognitive impairment: results of self-report and interview-based questionnaires. Gerontology. 2010;56(2):190–199. doi:10.1159/000236027
21. Hebert R, Durand PJ, Dubuc N, Tourigny A, Group P. PRISMA: a new model of integrated service delivery for the frail older people in Canada. Int J Integr Care. 2003;3:e08. doi:10.5334/ijic.73
22. Lyness JM, Noel TK, Cox C, King DA, Conwell Y, Caine ED. Screening for depression in elderly primary care patients. A comparison of the center for epidemiologic studies-depression scale and the geriatric depression scale. Arch Intern Med. 1997;157(4):449–454. doi:10.1001/archinte.1997.00440250107012
23. Smyth C. The Pittsburgh Sleep Quality Index (PSQI). J Gerontol Nurs. 1999;25(12):10–11.
24. De La Camara MA, Jimenez-Fuente A, Pardos AI. Falls in older adults: the new pandemic in the post COVID-19 era? Med Hypotheses. 2020;145:110321.
25. Vu NCT, Dang MT, Chei LT, Saito CL, editors. Ageing and Health in Viet Nam. Jakarta, Indonesia: Economic Research Institute for ASEAN and East Asia (ERIA); 2020.
26. Bueno-Cavanillas A, Padilla-Ruiz F, Jimenez-Moleon JJ, Peinado-Alonso CA, Galvez-Vargas R. Risk factors in falls among the elderly according to extrinsic and intrinsic precipitating causes. Eur J Epidemiol. 2000;16(9):849–859. doi:10.1023/A:1007636531965
27. Ambrose AF, Paul G, Hausdorff JM. Risk factors for falls among older adults: a review of the literature. Maturitas. 2013;75(1):51–61. doi:10.1016/j.maturitas.2013.02.009
28. Karlsson MK, Vonschewelov T, Karlsson C, Coster M, Rosengen BE. Prevention of falls in the elderly: a review. Scand J Public Health. 2013;41(5):442–454. doi:10.1177/1403494813483215
29. Balzer K, Bremer M, Schramm S, Luhmann D, Raspe H. Falls prevention for the elderly. GMS Health Technol Assess. 2012;8:Doc01. doi:10.3205/hta000099
30. Guirguis-Blake JM, Michael YL, Perdue LA, Coppola EL, Beil TL. Interventions to prevent falls in older adults: updated evidence report and systematic review for the US preventive services task force. JAMA. 2018;319(16):1705–1716. doi:10.1001/jama.2017.21962
31. Deandrea S, Lucenteforte E, Bravi F, Foschi R, La Vecchia C, Negri E. Risk factors for falls in community-dwelling older people: a systematic review and meta-analysis. Epidemiology. 2010;21(5):658–668. doi:10.1097/EDE.0b013e3181e89905
32. Kim SY, Kim MS, Sim S, Park B, Choi HG. Association between obesity and falls among Korean adults: a population-based cross-sectional study. Medicine. 2016;95(12):e3130. doi:10.1097/MD.0000000000003130
33. Ogliari G, Ryg J, Andersen-Ranberg K, Scheel-Hincke LL, Masud T. Association between body mass index and falls in community-dwelling men and women: a prospective, multinational study in the Survey of Health, Ageing and Retirement in Europe (SHARE). Eur Geriatr Med. 2021;12(4):837–849. doi:10.1007/s41999-021-00485-5
34. Linge J, Heymsfield SB, Dahlqvist Leinhard O. On the definition of sarcopenia in the presence of aging and obesity-initial results from UK biobank. J Gerontol a Biol Sci Med Sci. 2020;75(7):1309–1316. doi:10.1093/gerona/glz229
35. Nagarkar A, Kulkarni S. Association between daily activities and fall in older adults: an analysis of longitudinal ageing study in India (2017–18). BMC Geriatr. 2022;22(1):203. doi:10.1186/s12877-022-02879-x
36. Takada S, Yamamoto Y, Shimizu S, et al. Association between subjective sleep quality and future risk of falls in older people: results from LOHAS. J Gerontol a Biol Sci Med Sci. 2018;73(9):1205–1211. doi:10.1093/gerona/glx123
37. Lee S, Chung JH, Kim JH. Association between sleep quality and falls: a nationwide population-based study from South Korea. Int J Gen Med. 2021;14:7423–7433. doi:10.2147/IJGM.S331103
38. Mirelman A, Herman T, Brozgol M, et al. Executive function and falls in older adults: new findings from a five-year prospective study link fall risk to cognition. PLoS One. 2012;7(6):e40297. doi:10.1371/journal.pone.0040297
39. Hsu CL, Nagamatsu LS, Davis JC, Liu-Ambrose T. Examining the relationship between specific cognitive processes and falls risk in older adults: a systematic review. Osteoporos Int. 2012;23(10):2409–2424. doi:10.1007/s00198-012-1992-z
40. Young WR, Mark Williams A. How fear of falling can increase fall-risk in older adults: applying psychological theory to practical observations. Gait Posture. 2015;41(1):7–12. doi:10.1016/j.gaitpost.2014.09.006
41. Murphy SL, Dubin JA, Gill TM. The development of fear of falling among community-living older women: predisposing factors and subsequent fall events. J Gerontol a Biol Sci Med Sci. 2003;58(10):M943–947. doi:10.1093/gerona/58.10.M943
42. Baj J, Karakula-Juchnowicz H, Teresinski G, et al. COVID-19: specific and non-specific clinical manifestations and symptoms: the current state of knowledge. J Clin Med. 2020;9(6):1753. doi:10.3390/jcm9061753
43. Dos Santos PK, Sigoli E, Braganca LJG, Cornachione AS. The musculoskeletal involvement after mild to moderate COVID-19 infection. Front Physiol. 2022;13:813924. doi:10.3389/fphys.2022.813924
44. Moreland JD, Richardson JA, Goldsmith CH, Clase CM. Muscle weakness and falls in older adults: a systematic review and meta-analysis. J Am Geriatr Soc. 2004;52(7):1121–1129. doi:10.1111/j.1532-5415.2004.52310.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.