")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Feasibility and Relevance of an Intervention with Systematic Screening as a Base for Individualized Rehabilitation in Breast Cancer Patients: A Pilot Trial of the ReScreen Randomized Controlled Trial
Authors Olsson IM , Malmström M, Rydén L , Olsson Möller U
Received 31 December 2021
Accepted for publication 14 March 2022
Published 10 May 2022 Volume 2022:15 Pages 1057—1068
DOI https://doi.org/10.2147/JMDH.S355055
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ing-Marie Olsson,1,2 Marlene Malmström,1,2 Lisa Rydén,2,3 Ulrika Olsson Möller1,4
1Department of Health Sciences, Lund University, Lund, Sweden; 2Skåne University Hospital, Malmö, Sweden; 3Department of Clinical Sciences Lund, Surgery, Lund University, Lund, Sweden; 4Department of Nursing and Integrated Health Sciences, Kristianstad University, Kristianstad, Sweden
Correspondence: Ing-Marie Olsson, Department of Health Sciences, Lund University, Box 157, Lund, 221 00, Sweden, Tel +46 701453530, Fax +46 40333674, Email [email protected]
Background: A substantial proportion of women with breast cancer (BC) experience a wide range of long-term persistent and troublesome side effects related to the disease and its treatment. The ReScreen randomized controlled trial is conducted aiming to evaluate the effect of early screening of distress followed by individualized rehabilitation after primary BC treatment.
Purpose: To examine recruitment, retention, distribution of distress, relevance of intervention and reported problems in a pilot trial of the ReScreen RCT.
Patients and methods: Based on international research, a cutoff of ≥ 7 on the Distress Thermometer was used to identify women in need of extended support. Those who reported high distress were randomized to intervention group (IG, n = 9) or control group (CG, n = 9), while women with low distress formed an observational group (OG, n = 67). Self-reported data was collected at baseline, 2 weeks and 3, 6, 9, and 12 months after start of treatment. The participants were recruited from a BC unit in Sweden. Descriptive statistics were used for analyses.
Results: Eighty-five patients consented to participate. The recruitment rate was 73%, answer frequency was 98%, 64%, 95%, and retention rate was 100%, 56%, 91% in the IG, CG and OG, respectively. Few systematic errors were identified. When exploring the distribution of distress, it was evident that the participants scoring ≥ 7 were fewer (21.2%) than reported in previous studies (34– 43%). The most commonly problems reported were in line with previous reports of symptoms, including fatigue and worry.
Conclusion: The satisfactory rates of inclusion and data collection and the few systematic errors indicate that the ReScreen study is feasible if well planned and executed. To identify patients in need of extended support, an adjustment of the cutoff in the main study is indicated. Based on self-reported problems, the intervention was found relevant in this context.
Keywords: breast cancer, distress, fatigue, feasibility, rehabilitation, screening
Introduction
Breast cancer (BC) is the most common cancer in women worldwide1 and rehabilitation is essential to ensure optimal recovery. Approximately 7600 women annually are newly diagnosed with BC in Sweden.2 Developments in BC diagnostics and treatment have resulted in decreased mortality,3,4 in Sweden, the 5-year and 10-year survival rates are 92% and 86%, respectively.5 The increasing number of survivors and the well-known fact that BC is associated with a wide range of persistent, disabling side effects, such as fatigue,6 depression,7 fear of recurrence,8 reduced quality of life,9 pain,10 and distress11 emphasize the need for rehabilitation interventions. It is also known that women with BC have a higher prevalence of psychological symptoms compared to the general population, 5 years after diagnosis,12 and that between 30% and 40% remain on sick leave 1 year after diagnosis.13,14 Altogether, this indicates that women are in need of comprehensive rehabilitation following BC treatment.
Cancer rehabilitation aims to prevent and reduce the physical, psychological, social and existential consequences of cancer and its treatment. Rehabilitation efforts should provide support and enable patients and their families to live as well as possible.15 Rehabilitation research has shown that a variety of different rehabilitation interventions can be effective for known BC-related complications, and that different interventions might be effective for the same problems, depending on how and when the intervention is provided.16 Previous research has predominantly focused on exercise,17,18 an important part of cancer rehabilitation. However, as the need for rehabilitation varies greatly between individuals and with the definition of cancer rehabilitation15 as a foundation, a comprehensive approach to rehabilitation is needed. Also, despite efforts, women report unmet needs.19–21
Recent research show the need for structures and models to identify individual needs and enable individualized rehabilitation.22,23 Efforts have been made, for example, a theoretical surveillance model was developed, aiming to facilitate early identification of BC-related physical impairments during the trajectory of medical management.24 Another model was a pilot study testing an individually tailored nurse-navigation intervention, focusing on both physical and psychological symptoms during the BC-trajectory, showing promising results concerning anxiety, depression and distress.25
The patients’ perceived level of distress is one important risk factor for unmet needs following BC treatment.20 Distress, in the cancer context, is a concept that captures the experience of cancer from multiple perspectives. It is defined as a multifactorial experience of a psychological, social, and/or spiritual nature that may interfere with the ability to cope with cancer, its physical symptoms, and treatment.26 About 34–43% of the women newly diagnosed with BC suffer from high distress27,28 and women newly diagnosed with BC who report high distress may be at risk of developing chronic distress.11 High distress in the initial phase of the BC cancer trajectory is a predictor of chronic distress 8 months later, and persistent high distress at 8 months after surgery has been shown to predict worse psychosocial outcomes as long as 6 years after treatment.29 Distress as a screening tool for rehabilitation needs in a BC context has been tested earlier with promising results.25,30 However, the level of distress may be culture specific and therefore need to be explored in various contexts.
Research suggest structures for cancer rehabilitation that include a comprehensive assessment of the patients life situation before start of treatment, with an ongoing surveillance during the cancer trajectory, facilitating individualized rehabilitation.31 This supports the relevance of early screening for distress at time of primary treatment to ensure individualized rehabilitation in the initial part of the cancer trajectory as well as repeated evaluations throughout the phase of illness to reduce the risk of long-term, BC-related problems. Lack of structures may result in suboptimal recovery, manifested as persistent treatment-related ailments, increased health consumption, long periods of sick leave, and insufficient use of available resources. The ReScreen randomized controlled trial (RCT) was designed to evaluate the effect of screening-based, individualized rehabilitation following primary BC treatment.32 Through pilot and feasibility studies, the likelihood of success of a main study and of valid inference from the research is enhanced.33 This study aimed to examine recruitment, retention, distribution of distress, relevance of the intervention, and reported problems in a pilot trial of the ReScreen study.
Methods
Design and Brief Description of the ReScreen Main Study
A study protocol of the ReScreen study has been published.32 To ensure transparency and quality, the pilot trial is reported according to the CONSORT extension for randomized feasibility and pilot trials.34
In brief, the ReScreen RCT32 was inspired by the UK Medical Research Council framework for developing and evaluating complex interventions35 and was designed as a three-armed trial. Women who agree to participate are screened for distress using the Distress Thermometer (DT),36 1–2 weeks following BC diagnosis. The DT is validated in different countries and cultures,37 and has good predictive validity in the context of oncology care in Sweden,38 and is a promising screening tool for identifying extended needs in a BC context.27,39 The DT includes a 0–10 visual analog scale, where 0 is equivalent to no distress, and 10 is the worst imaginable distress, and a 39-item problem list (PL) with the purpose of identifying problems in five categories: practical, family, emotional, spiritual/religious, and physical.36 The PL has been validated in a Swedish colon cancer context.40 Those who report high distress are randomized to either the intervention group (IG) or the control group (CG), while women with low distress form an observational group (OG). All groups (the IG, CG and OG) receive “care as usual.” In addition, the IG is monitored proactively by a research nurse (nurse navigator), for 1 year to facilitate evidence-based individualized rehabilitation supported by a decision support tool (DST), described in the study protocol,32 developed within this project to guide the research nurse. The DST focuses on areas of commonly reported problems by BC patients as well as health-related behaviours (physical activity, tobacco and alcohol consumption) and is based on research16 and national documents,15 and contains both general advice, and advice depending on identified individual needs. The dedicated research nurse will use the DST in conversation with the participant when structuring an individual rehabilitation plan, with explicit goals for the rehabilitation process. Evaluation and follow-up of the rehabilitation plan depends on the participant’s individual needs, but as a minimum at 2 weeks after start of treatment and once a month during the first 3 months.32 The primary outcome for the main study is distress.
Participants and Randomization
In Sweden, cancer rehabilitation is organized on various levels: 1) basic rehabilitation needs, 2) special rehabilitation needs, 3) advanced rehabilitation needs, and 4) very advanced rehabilitation needs. On the basic level, rehabilitation and information are provided by the contact nurse and a physician in a cancer unit, sometimes assisted by a social worker. Special rehabilitation needs could include counselling with social worker during crisis response. For patients with advanced rehabilitation needs a specialized multi-professional cancer rehabilitation team can be utilized.15 The patient will remain on the first level during the cancer trajectory, unless extended needs are identified.
Participants for this feasibility study were recruited between November 2018 and April 2019 at a BC unit at a university hospital in the south of Sweden. Inclusion criteria were 1) newly diagnosed primary BC; 2) age ≥18; 3) ability to communicate in Swedish; and 4) cognitive ability to participate. Exclusion criteria were 1) pregnancy; 2) psychological disease or drug abuse; 3) previously treated for BC (ie, relapse); and 4) endocrine therapy as only treatment.
All eligible women with newly diagnosed BC were consecutively invited to participate in the study. A contact nurse approached them about participation during a pre-planned visit to the outpatient clinic, approximately 1–2 weeks following the BC diagnosis. In line with Danish39 and Dutch27 studies on BC, a cutoff score of 7 was set to identify patients with moderate/high distress. Patients scoring ≥7 were randomized to the IG or CG. Patients scoring ≤6 were followed longitudinally for comparison (OG).32
Data Collection
Data were collected at baseline, and 2 weeks and 3, 6, 9, and 12 months after start of treatment. Clinical and treatment-related data was collected through the patients’ medical journal and was manually registered in an electronic case report form. Demographics and outcome data were collected via self-reported questionnaires containing validated instruments and single items focusing on physical, psychological, and behavioural aspects of rehabilitation.32 The questionnaires were sent to the patients by mail and returned in a pre-addressed, stamped envelope. Up to two reminders were sent. The questionnaires were scanned using a system with a control function for identifying missing data.
Feasibility Outcomes
Data Collection Rate and Frequency
“Recruitment rate” was defined as the number and percentage of participants who accepted to participate in the study out of all eligible patients. Reasons for non-participation were not systematically collected for ethical reasons. “Answer frequency” was defined as the number and percentage of patients returning the questionnaires at each given follow-up point for the sample as a whole and divided into subgroups (IG, CG, and OG). “Retention rate” was defined as the number and percentage of patients remaining in the study at each follow-up point for the sample as a whole, and divided into subgroups (IG, CG and OG).
Data Management Outcomes
To identify potential systematic errors, 1) all scanned questionnaires were manually verified and compared to the original data and 2) data were manually compared with the medical journal by two research team members, one of whom was not involved in the data management process.
Distribution of Distress
The distribution of distress was explored in several steps. Firstly, the mean value for distress was calculated in the total sample at each follow-up point. Secondly, the number and percentage of participants scoring ≥7 (cutoff) at baseline was calculated. Finally, alternative cutoffs were explored by calculating the number and percentage of patients scoring ≥4, 5, 6, or 8.
Adherence to Intervention Protocol and Frequently Reported Problems
To ensure adherence to the intervention, a review of the study documentation of the IG was conducted, focusing on 1) the number of contacts with the research nurse; 2) whether all patients had an established rehabilitation plan; 3) whether the rehabilitation goals stated by the patient were clearly documented; and 4) whether the goals were followed up by the research nurse.
To evaluate if the areas in the DST were consistent with the most common patient-reported problems, the PL was used to explore patient-reported problems in the total sample at each follow-up point. The PL was also used to investigate the number of reported problems per patient in the total sample.
Statistical Analyses
Descriptive statistics in terms of frequencies, mean, and standard deviation (SD) were used to evaluate outcome data using IBM SPSS Statistics for Windows, version 25.0 (IBM Corp., Armonk, NY, USA). Data on all participants were included in the analyses, except for data giving the number of problems, where only questionnaires with complete data on the PL at baseline were included.
Results
A total of 117 patients were found to be eligible and were invited to participate in the study. Eighty-five patients agreed to participate and signed informed consent, resulting in a recruitment rate of 73% (Figure 1). The mean age in the total sample was 62.8 years and the majority were married/cohabiting (n=57; 67.1%). Half of the participants had two children (n=43; 50.6%) and almost 86% were born in Sweden. About 9.5% were on sick leave at baseline. The majority reported having a good/very good financial situation (n=69; 82.1%) and almost half of the participants had a university degree (n=39; 45.9%). More than half of the participants used no or only small amounts of alcohol (n=49; 61.3%), and almost everyone was non-smoking (n=78; 94%). A large proportion of the participants stated that they had less than 30 minutes of exercise/week (n=40; 47.1%), but the majority reported other physical activity of more than 90 minutes/week (n=53; 62.4%) at baseline (Table 1).
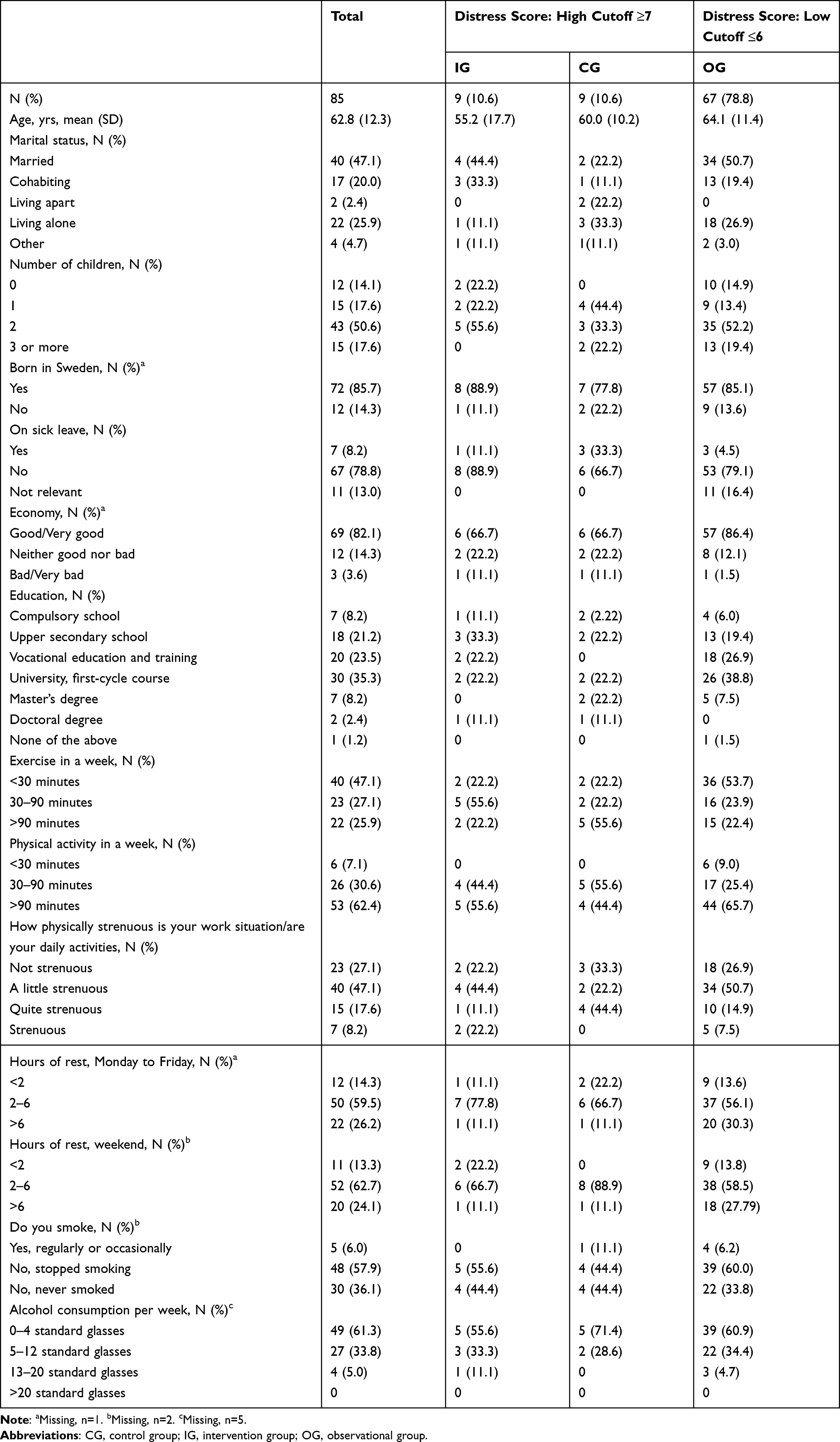 |
Table 1 Demographic Characteristics of the Participants |
 |
Figure 1 Flowchart of the recruitment process, randomization and answer frequency. |
A total of 425 forms were sent out during the 1-year follow-up, of which 392 were returned, resulting in an answer frequency of 92% (Figure 1). The answer frequency decreased over time from 85 questionnaires at baseline to 81 (95%) at 2 weeks, 79 (93%) at 3 months, 81 (95%) at 6 months, 76 (89%) at 9 months, and 75 (88%) at 12 months. Divided into the groups IG, CG, and OG, 44 out of 45 (98%) forms were sent back in the IG, while 29 out of 45 (64%) and 319 out of 335 (95%) were sent back for the CG and the OG, respectively. The retention rate for the total sample was 99% at 2 weeks (n=78), 98% at 3 months (n=75), 95% at 6 months (n=76), 93% at 9 months (n=72), and 88% at 12 months (n=72). The retention rate at 12 months was 100% in the IG (n=9), 56% in the CG (n=9), and 91% in the OG (n=67).
Data Management
Three systematic errors were identified. Two were related to the scanning procedure, namely 1) the scanning system in some cases interpreted handwritten numbers inaccurately, resulting in incorrectly recorded patient identification number; and 2) the system did not interpret commas; for example, 78.9 kg was interpreted as 789 kg. 3) The third error was related to the timing of data extraction from the medical record as the treatment regime could change during the process, for example, when a patient declined recommended adjuvant treatment after visiting the oncologist.
Distribution of Distress
The mean value for distress in the total sample (n=85) was 3.99 (SD 2.67) at baseline declining to 2.78 (SD 2.40) at 12 months (Figure 2).
 |
Figure 2 Mean distress scores and standard deviation (whiskers) at the pilot trials data collection points. |
With the cutoff set at ≥7, 18 participants (21.2%) were identified as having high distress at baseline and were randomized to either the IG (n=9) or the CG (n=9). Exploring distribution of distress at baseline using different cutoffs showed that 49 participants (56.9%) scored 4 or higher, 38 (44.2%) scored ≥5, 29 (33.7%) scored ≥6, and nine (10.4%) scored ≥8.
Adherence to Intervention
Of the nine participants in the IG, eight accepted to take part in the intervention. The eight participants had at least the minimum amount of planned contact (one occasion per month during the first 3 months). All of the participants had a rehabilitation plan documented in the medical journal, with clearly stated and followed-up rehabilitation goals. Advice concerning, for example, physical activity or sleep was documented, followed up, and evaluated.
Frequently Reported Problems
The most frequently patient-reported problems in the total sample (n=85) were in the emotional and physical domains of the PL. Five problems were among the most frequently reported problems at all time points (Figure 3): Almost 68% of the participants reported “Worry” as a problem at baseline, decreasing to 38.5% at 3 months, and increasing to 48% at 12 months. “Fatigue” increased from 32.5% at baseline to 67.5% at 3 months, but decreased to 44% at 12 months. “Sleep”, “Sadness” and “Memory/concentration” remained stable over time (Figure 3). The most common problems were consistent with the areas in the DST.
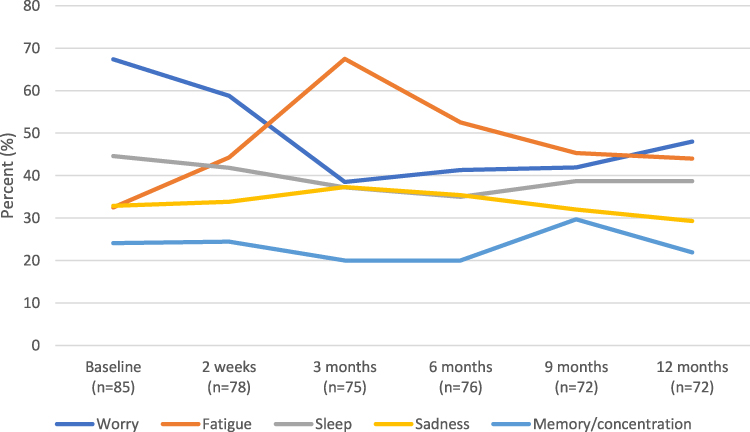 |
Figure 3 The most common problems in percentage (%) reported at the pilot trials data collection points. |
Some problems were more frequently reported at different follow-up points. “Nervousness” and “Fear” were frequently reported in the beginning of the trajectory (baseline) (41% and 38.6%, respectively) and at 2 weeks (38.6% and 28.7%); “Dry skin/itchy” was reported by 44.7% at 3 months. “Getting around” was reported by 30% at 9 months. “Pain” was more frequently reported at 2 weeks (26.9%) compared to baseline, but was most frequently reported at 9 months (29.7%).
The number of reported problems at baseline ranged from 0 to 27. Having three problems were most frequently reported (n=15; 20.5%). Fifty-five participants (75.3%) reported having no problems to 5 problems, 14 (19.2%) reported 6–12 problems and 4 (5.5%) reported 19 problems or more.
Discussion
This feasibility study examined the data collection and data management process of a pilot trial of the ReScreen RCT. The study also explored the distribution of distress for comparison with international studies and assessed the relevance of the intervention. The results show that the processes are working well, with satisfactory recruitment rates, answer frequency, and retention rates. Few systematic errors were identified, and they were easily corrected. The results also showed that fewer women in this sample scored ≥7 at baseline compared to international studies. After adjustment of the cutoff, the result facilitates the decision to move on to the full-scale study.
Recruitment to RCTs is known to be difficult and the recruitment rate can affect the results.41 Previous studies highlight the importance of organization, training, and support to facilitate recruitment to RCTs.42 The recruitment rate of 73% in this study is in line with earlier studies in a similar context,30 which indicates well-functioning procedures for recruitment. In the initiation of this study, several preparatory meetings were held with the contact nurses at the outpatient clinic recruiting potential patients. The meetings aimed to enhance compliance, by clarifying inclusion and exclusion criteria and emphasizing the importance of inclusion. It is known that the way recruiters communicate about a trial is important for recruitment, as is a person-centered approach.43 Therefore, the meetings discussed how the study was to be presented to the patients, in order to facilitate recruitment. A dedicated research nurse was available on a daily basis to support recruiters whenever they had questions about recruitment or the study. In other studies, the importance of support44,45 and the presence of research staff45 for recruitment has been highlighted as an important factor to enhance recruitment.
The comprehensive support to the recruiting contact nurses may also be a possible explanation for the high answer frequency and retention rate. Research on retention has highlighted the importance of good strategies within the trial plan, and also the importance of a good relationship with the participants.46 Since the recruitment situation was the only occasion when the participants in the CG and OG formally received information and had time to ask questions about the study this situation became very important, which was emphasized at the preparatory meetings. In this study, 93% of the questionnaires were returned. The recruitment procedure, together with the procedures for data collection that included pre-addressed, stamped envelopes and up to two remainders, contributed to the answer frequency and facilitated retention, which indicates good strategies and well-functioning procedures.
The lower answer frequency in the CG compared to the OG probably relates to the fact that the participants who were randomized to the CG were more stressed by their situation than those in the OG, as they reported ≥7 on the DT. The answer frequency was also lower in the CG compared to the IG group, which can be related to the fact that they did not receive the enhanced support as did those who were randomized to the IG. The IG was followed continuously by the dedicated contact nurse, and the good outcome of the individualized rehabilitation support in this group reflects a good relationship and the participants’ satisfaction with the support, both of which were described as important in previous research.46 In this study, the low number of participants in the IG and CG groups prevents any definitive conclusions, but the outcome of the pilot trial is important to take into account in the main study.
The cutoff of 7 was initially set in line with Danish28 and Dutch27 studies using the DT in a similar context, where 43% and 34%, respectively, scored ≥7 on the DT, indicating moderate/high distress for women with newly diagnosed BC. In this study, 21.2% of the women scored ≥7 on the DT, a lower percentage than expected. International research shows a mean distress score of 5.428 and 5.547 for women newly diagnosed with BC, compared to 3.99 in this study. It is evident that women in this Swedish context had a lower distress score than women in other BC contexts, and the reason for this is unknown. When exploring different cutoffs and lowering the cutoff to 5 or 6, the same frequency (34% and 44%, respectively) as in other studies27,28 was seen. This indicates that a lower cutoff is feasible in this context, which will lead to an increased number of participants in the IG and CG. To enable evaluation of the optimal cutoff in a Swedish context, the cutoff will be reviewed in the main study.
To ensure the relevance of the DST, the most common patient-reported problems in this study were compared with earlier research. The most reported problems in this sample are known problems in patients with BC, such as worry,28 fatigue,6 sleep and concentration problems48 and sadness.28 Over time, some problems fluctuated while others remained stable. Previous research has shown that some patients with BC have increased levels of distress and associated problems in the re-entry to the survivorship phase.11 This study showed a marked increase in worry at 12 months, in agreement with a longitudinal study exploring anxiety, indicating that almost 30% of participants were suffering from persistent or newly developed anxiety at 12 months after surgery.49 For the majority of the patients in the Swedish BC care context, the treatment phase is completed at 12 months and no more physical follow-ups are planned. This is a likely cause of their increased perceived distress, which indicates that they may benefit from increased support at this stage. However, this needs to be explored in future studies.
Long-term follow-up studies report that fatigue, and cognitive and sleep problems can lower the quality of life for BC patients for as long as 5 years after diagnosis,21 and high distress during the first year after diagnosis can predict worse psychosocial outcomes 6 years later.29 This knowledge clarifies the need for early identification and long-term support and rehabilitation to avoid persistent treatment-related ailments. Together with the finding in this study showing a wide range of reported problems, the pathway for BC patients seems to be complex, with different problems appearing at different time points during the trajectory. Women with BC report unmet needs,8,19 indicating that even if some problems are reported more frequently on a group level, the need for a complex intervention is evident, with the possibility to identify needs and act upon them individually, where the patients’ preferences are combined with evidence-based interventions. The individualized approach is also important considering the known fact that one problem can have different origins and that different interventions can be effective depending on individual preferences.16 This feasibility study shows that the reported problems are in line with earlier research, indicating that the RCT is feasible and relevant.
Strengths and Limitations
According to the CONSORT statement,34 a feasibility study aims to investigate if and how a future trial should be performed. The final sample was deemed adequate for assuring evaluation of procedures, and relevance of the intervention. The large number of participants in this pilot trial is a strength and validates the results. A limitation is the exclusion of certain groups of women with BC, such as those with relapse and those unable to communicate in Swedish. Since people with language difficulties, such as migrated women, are often excluded from research, future studies are needed to explore the BC care trajectory also in these women.
Conclusion
The satisfactory recruitment rate, answer frequency, and retention rate, together with few systematic errors, show that the data collection and management in the ReScreen randomized controlled trial is feasible, with well-functioning procedures. The answer frequency and retention rate in the control group were lower than in the intervention group and observational group. This will be monitored actively in the main study. The difference in distribution of distress in this sample compared with international studies, leading to few participants in IG and CG, indicates a need to adjust the cutoff to identify patients in need of extended support in the main ReScreen randomized controlled trial and to explore the optimal cut-off in this context. Perceived problems reported by the participants are in line with previous studies and show the relevance of the planned complex intervention.
Abbreviations
BC, breast cancer; CG, control group; DST, decision support tool; DT, distress thermometer; IG, intervention group; OG, observation group; PL, problem list; RCT, randomized controlled trial; SD, standard deviation.
Data Sharing Statement
In accordance with the national ethical regulations, and the ethical approval of this study, only the members of the research group who are involved in the study will have access to data. This means that we are not allowed to share the raw data from this study.
Ethics Approval and Informed Consent
The ReScreen study was approved by the Regional Ethical Review Board in Lund, Sweden (Dnr 2015/505, amendments 2018/924, 2020-04664), and registered with Clinicaltrials.gov (NCT03434717). The study complies with the Declaration of Helsinki.50 The potential participants received oral and written information about the study and were assured that they could decline participation or withdraw from the study without this affecting their present or future care. Written informed consent was obtained from all patients willing to participate.
Acknowledgments
Firstly, we would like to express our gratitude to all patients who accepted inclusion and participated in the study. We would like to thank research nurse Helena Erixon for delivering the intervention to the IG. We would also like to thank both Helena Erixon and administrator Eva Wahlström for all their efforts in collecting data. Finally, we want to thank the contact nurses at the BC unit who recruited participants to the study.
Author Contributions
MM and LR designed the study. MM and UOM were responsible for acquisition of data. IMO was responsible for analysis and interpretation of data. IMO wrote the initial draft of the manuscript and MM, LR and UOM made substantial contributions to the interpretation of data and the revision of the manuscript. All authors have agreed on the journal to which the manuscript was submitted. All authors have approved the submitted version and agree to take responsibility and to be accountable for the contents of the article.
Funding
The ReScreen study has received external funding through governmental funding of clinical research within the Swedish National Health Service, and the Swedish Breast Cancer Association, the Percy Falk Foundation, the LMK Foundation for Interdisciplinary Scientific Research, and the Cancer and Allergy Foundation. The funding bodies had no role in the design of this study and will not have any role in its execution, analysis interpretation of the data, or decision to submit results. Open access funding was provided by Lund University.
Disclosure
The authors declare no competing interests in this work.
References
1. Sung H, Ferlay J, Siegel RL, et al. Global cancer statistics 2020: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin. 2021;71(3):209–249. doi:10.3322/caac.21660
2. National board of Health and Wellfare. Stockholm: statistics on newly detected cancer cases 2020 (In Swedish: Statistik om nyupptäckta cancerfall 2020). Available from: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/statistik/2021-12-7700.pdf.
3. Miller KD, Siegel RL, Lin CC, et al. Cancer treatment and survivorship statistics, 2016. CA Cancer J Clin. 2016;66(4):271–289. doi:10.3322/caac.21349
4. Carioli G, Malvezzi M, Rodriguez T, Bertuccio P, Negri E, La Vecchia C. Trends and predictions to 2020 in breast cancer mortality in Europe. Breast. 2017;36:89–95. doi:10.1016/j.breast.2017.06.003
5. National Board of Health and Welfare. Stockholm: cancer in numbers 2018 (in Swedish: Statistik om cancer 2018). Available from: https://www.socialstyrelsen.se/globalassets/sharepoint-dokument/artikelkatalog/statistik/2018-6-10.pdf.
6. Abrahams HJG, Gielissen MFM, Schmits IC, Verhagen C, Rovers MM, Knoop H. Risk factors, prevalence, and course of severe fatigue after breast cancer treatment: a meta-analysis involving 12,327 breast cancer survivors. Ann Oncol. 2016;27(6):965–974. doi:10.1093/annonc/mdw099
7. Pilevarzadeh M, Amirshahi M, Afsargharehbagh R, Rafiemanesh H, Hashemi SM, Balouchi A. Global prevalence of depression among breast cancer patients: a systematic review and meta-analysis. Breast Cancer Res Treat. 2019;176(3):519–533. doi:10.1007/s10549-019-05271-3
8. Ellegaard MB, Grau C, Zachariae R, Bonde Jensen A. Fear of cancer recurrence and unmet needs among breast cancer survivors in the first five years. A cross-sectional study. Acta Oncol. 2017;56(2):314–320. doi:10.1080/0284186x.2016.1268714
9. Jones SM, LaCroix AZ, Li W, et al. Depression and quality of life before and after breast cancer diagnosis in older women from the Women’s Health Initiative. J Cancer Survivorship. 2015;9(4):620–629. doi:10.1007/s11764-015-0438-y
10. Cooney MA, Culleton-Quinn E, Stokes E. Current knowledge of pain after breast cancer treatment: a systematic review. Pain Manage Nurs. 2013;14(2):110–123. doi:10.1016/j.pmn.2010.09.002
11. Henselmans I, Helgeson VS, Seltman H, de Vries J, Sanderman R, Ranchor AV. Identification and prediction of distress trajectories in the first year after a breast cancer diagnosis. Health Psychol. 2010;29(2):160–168. doi:10.1037/a0017806
12. Maass S, Boerman LM, Verhaak PFM, Du J, de Bock GH, Berendsen AJ. Long-term psychological distress in breast cancer survivors and their matched controls: a cross-sectional study. Maturitas. 2019;130:6–12. doi:10.1016/j.maturitas.2019.09.003
13. Sjövall K, Attner B, Englund M, et al. Sickness absence among cancer patients in the pre-diagnostic and the post-diagnostic phases of five common forms of cancer. Support Care Cancer. 2012;20(4):741–747. doi:10.1007/s00520-011-1142-8
14. Sun Y, Shigaki CL, Armer JM. Return to work among breast cancer survivors: a literature review. Support Care Cancer. 2017;25(3):709–718. doi:10.1007/s00520-016-3446-1
15. Regional Cancer Centres in Sweden (RCC). Swedish national guidelines for cancer rehabilitation; 2021. Available from: https://cancercentrum.se/globalassets/vara-uppdrag/rehabilitering-palliativ-vard/vardprogram/nationellt-vardprogram-cancerrehabilitering.pdf.
16. Olsson Möller U, Beck I, Rydén L, Malmström M. A comprehensive approach to rehabilitation interventions following breast cancer treatment - a systematic review of systematic reviews. BMC Cancer. 2019;19(1):472. doi:10.1186/s12885-019-5648-7
17. Wiggenraad F, Bolam KA, Mijwel S, van der Wall E, Wengström Y, Altena R. Long-term favorable effects of physical exercise on burdensome symptoms in the optitrain breast cancer randomized controlled trial. Integr Cancer Ther. 2020;19:1534735420905003. doi:10.1177/1534735420905003
18. Demmelmaier I, Brooke HL, Henriksson A, et al. Does exercise intensity matter for fatigue during (neo-)adjuvant cancer treatment? The Phys-Can randomized clinical trial. Scand J Med Sci Sports. 2021;31(5):1144–1159. doi:10.1111/sms.13930
19. von Heymann-horan AB, Dalton SO, Dziekanska A, et al. Unmet needs of women with breast cancer during and after primary treatment: a prospective study in Denmark. Acta Oncol. 2013;52(2):382–390. doi:10.3109/0284186X.2012.746468
20. Lo-Fo-Wong DNN, de Haes H, Aaronson NK, et al. Risk factors of unmet needs among women with breast cancer in the post-treatment phase. Psychooncology. 2020;29(3):539–549. doi:10.1002/pon.5299
21. Schmidt ME, Wiskemann J, Steindorf K. Quality of life, problems, and needs of disease-free breast cancer survivors 5 years after diagnosis. Qual Life Res. 2018;27(8):2077–2086. doi:10.1007/s11136-018-1866-8
22. Olsson Möller U, Olsson IM, Sjövall K, Beck I, Rydén L, Malmström M. Barriers and facilitators for individualized rehabilitation during breast cancer treatment - a focus group study exploring health care professionals’ experiences. BMC Health Serv Res. 2020;20(1):252. doi:10.1186/s12913-020-05107-7
23. Brick R, Lyons KD, Bender C, et al. Factors influencing utilization of cancer rehabilitation services among older breast cancer survivors in the USA: a qualitative study. Support Care Cancer. 2022;30(3):2397–2405. doi:10.1007/s00520-021-06678-9
24. Stout NL, Binkley JM, Schmitz KH, et al. A prospective surveillance model for rehabilitation for women with breast cancer. Cancer. 2012;118(8 Suppl):2191–2200. doi:10.1002/cncr.27476
25. Mertz BG, Dunn-Henriksen AK, Kroman N, et al. The effects of individually tailored nurse navigation for patients with newly diagnosed breast cancer: a randomized pilot study. Acta Oncol. 2017;56(12):1682–1689. doi:10.1080/0284186X.2017.1358462
26. Riba MB, Donovan KA, Andersen B, et al. Distress management, version 3.2019, NCCN clinical practice guidelines in oncology. J Natl Compr Canc Netw. 2019;17(10):1229–1249. doi:10.6004/jnccn.2019.0048
27. Ploos van Amstel FK, Tol J, Sessink KH, van der Graaf WTA, Prins JB, Ottevanger PB. A specific distress cutoff score shortly after breast cancer diagnosis. Cancer Nurs. 2017;40(3):E35–E40. doi:10.1097/NCC.0000000000000380
28. Mertz BG, Bistrup PE, Johansen C, et al. Psychological distress among women with newly diagnosed breast cancer. Eur J Oncol Nurs. 2012;16(4):439–443. doi:10.1016/j.ejon.2011.10.001
29. Lam WW, Shing YT, Bonanno GA, Mancini AD, Fielding R. Distress trajectories at the first year diagnosis of breast cancer in relation to 6 years survivorship. Psychooncology. 2012;21(1):90–99. doi:10.1002/pon.1876
30. Ploos van Amstel FK, Peters M, Donders R, et al. Does a regular nurse-led distress screening and discussion improve quality of life of breast cancer patients treated with curative intent? A randomized controlled trial. Psychooncology. 2020;29(4):719–728. doi:10.1002/pon.5324
31. Alfano CM, Pergolotti M. Next-generation cancer rehabilitation: a giant step forward for patient care. Rehabil Nurs. 2018;43(4):186–194. doi:10.1097/rnj.0000000000000174
32. Olsson Möller U, Rydén L, Malmström M. Systematic screening as a tool for individualized rehabilitation following primary breast cancer treatment: study protocol for the ReScreen randomized controlled trial. BMC Cancer. 2020;20(1):484. doi:10.1186/s12885-020-06815-3
33. Thabane L, Ma J, Chu R, et al. A tutorial on pilot studies: the what, why and how. BMC Med Res Methodol. 2010;10:1. doi:10.1186/1471-2288-10-1
34. Eldridge SM, Chan CL, Campbell MJ, et al. CONSORT 2010 statement: extension to randomised pilot and feasibility trials. Pilot Feasibil Stud. 2016;2:64. doi:10.1186/s40814-016-0105-8
35. Craig P, Dieppe P, Macintyre S, Michie S, Nazareth I, Petticrew M. Developing and evaluating complex interventions: the new Medical Research Council guidance. BMJ. 2008;337:a1655. doi:10.1136/bmj.a1655
36. Holland JC, Andersen B, Breitbart WS, et al. Distress management. J Natl Compr Canc Netw. 2013;11(2):190–209. doi:10.6004/jnccn.2013.0027
37. Donovan KA, Grassi L, McGinty HL, Jacobsen PB. Validation of the distress thermometer worldwide: state of the science. Psychooncology. 2014;23(3):241–250. doi:10.1002/pon.3430
38. Thalén-Lindström A, Larsson G, Hellbom M, Glimelius B, Johansson B. Validation of the distress thermometer in a Swedish population of oncology patients; accuracy of changes during six months. Eur J Oncol Nurs. 2013;17(5):625–631. doi:10.1016/j.ejon.2012.12.005
39. Bidstrup PE, Mertz BG, Dalton SO, et al. Accuracy of the Danish version of the ‘distress thermometer’. Psychooncology. 2012;21(4):436–443. doi:10.1002/pon.1917
40. Sarenmalm EK, Nasic S, Håkanson C, et al. Swedish version of the distress thermometer: validity evidence in patients with colorectal cancer. J Natl Compr Canc Netw. 2018;16(8):959–966. doi:10.6004/jnccn.2018.7027
41. Treweek S, Pitkethly M, Cook J, et al. Strategies to improve recruitment to randomised trials. Cochrane Database Syst Rev. 2018;2(2):Mr000013. doi:10.1002/14651858.MR000013.pub6
42. Donovan JL, Paramasivan S, de Salis I, Toerien M. Clear obstacles and hidden challenges: understanding recruiter perspectives in six pragmatic randomised controlled trials. Trials. 2014;15:5. doi:10.1186/1745-6215-15-5
43. Houghton C, Dowling M, Meskell P, et al. Factors that impact on recruitment to randomised trials in health care: a qualitative evidence synthesis. Cochrane Database Syst Rev. 2020;10(10):Mr000045. doi:10.1002/14651858.MR000045.pub2
44. Elliott D, Husbands S, Hamdy FC, Holmberg L, Donovan JL. Understanding and improving recruitment to randomised controlled trials: qualitative research approaches. Eur Urol. 2017;72(5):789–798. doi:10.1016/j.eururo.2017.04.036
45. Aspden T, Armstrong M, Serfaty M. Views of healthcare professionals on recruiting to a psychosocial randomised controlled trial: a qualitative study. BMC Health Serv Res. 2021;21(1):837. doi:10.1186/s12913-021-06817-2
46. Daykin A, Clement C, Gamble C, et al. ‘Recruitment, recruitment, recruitment’ - the need for more focus on retention: a qualitative study of five trials. Trials. 2018;19(1):76. doi:10.1186/s13063-018-2467-0
47. Jørgensen L, Laursen BS, Garne JP, Sherman KA, Søgaard M. Prevalence and predictors of distress in women taking part in surgical continuity of care for breast cancer: a cohort study. Eur J Oncol Nurs. 2016;22:30–36. doi:10.1016/j.ejon.2016.01.004
48. Lo-Fo-Wong DN, de Haes HC, Aaronson NK, et al. Predictors of enduring clinical distress in women with breast cancer. Breast Cancer Res Treat. 2016;158(3):563–572. doi:10.1007/s10549-016-3896-7
49. Kim J, Cho J, Lee SK, et al. Surgical impact on anxiety of patients with breast cancer: 12-month follow-up prospective longitudinal study. Ann Surg Treat Res. 2020;98(5):215–223. doi:10.4174/astr.2020.98.5.215
50. World Medical Association. World Medical Association Declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.