")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 17
Four-Leaf Clover Shape Agglomerate Keratoacanthomas: A Case Report
Authors Yang D , Mao Y, Peng L, Huang S, Zhou L, Li C
Received 7 December 2023
Accepted for publication 16 April 2024
Published 24 April 2024 Volume 2024:17 Pages 921—924
DOI https://doi.org/10.2147/CCID.S453734
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Dingbin Yang,1,2 Yu Mao,3 Lu Peng,2 Shuqiong Huang,2 Lijun Zhou,2 Changqiang Li1
1Department of Dermatology, the Affiliated Hospital, Southwest Medical University, Luzhou, 646000, People’s Republic of China; 2Department of Dermatology, People’s Hospital of Leshan, Leshan, 614000, People’s Republic of China; 3Department of Pathology, People’s Hospital of Leshan, Leshan, 614000, People’s Republic of China
Correspondence: Changqiang Li, Department of Dermatology, the Affiliated Hospital, Southwest Medical University, Luzhou, 646000, People’s Republic of China, Email [email protected]
Abstract: Keratoacanthoma (KA) is a papule, plaque, or nodule in an exposed area, with a crater-like horn plug in the center. Multiple KAs are rare disorders, especially when the lesions are agglomerated together. Herein, we report a case of 65-year-old man who presented with four red nodules of different sizes on the right side of the chest. The lesions were clustered, with central keratotic cores, similar in appearance to a four-leaf clover. The nodules were completely removed by excisional surgery and the diagnosis of Agglomerate KAs was made based on clinical and pathological results. A 6-year follow-up found no recurrence.
Keywords: agglomerate keratoacanthomas, four-leaf clover
Introduction
Keratoacanthoma (KA) is a common cutaneous neoplasm, mainly seen in the middle-aged and elderly people. There is a current debate as to whether KA is a subtype of Squamous Cell Carcinomas (SCC) or a separate entity. KA occurs in chronic sun-exposed regions such as the face and head, growing rapidly, and tending to be self-healing. Skin lesions present as well demarcated volcano shaped nodules with a central keratin core, and usually present as a solitary lesion and less commonly in multiples. An unusual and infrequent instance of Agglomerate KAs, exhibiting a distinctive “Four-leaf clover shape” is presented in this report.
Case Report
The patient was a 65-year-old male who came to the Dermatology Department because of multiple red nodules on the right chest that had persisted for six months. Initially, a red nodule with central keratosis had appeared on the right chest with no pain or itching. The patient did not pay attention to it. Since it was first noticed, the lesion grew fast and three similar red nodules appeared around the primary nodule. The patient attempted to alleviate the lesions by applying ointment externally, however, the condition did not improve. There was no history of oral drugs, chemical insult to the skin, nor had there been any phototherapy in the past. And there was no family history of similar lesions.
Physical examination revealed the presence of four red nodules of different sizes, from 4 mm×3 mm to 10 mm×6 mm, were seen on the right chest, with a crater-like horn plug in the center. Four nodules were clustered together and looked like a “lucky four-leaf clover” (Figure 1). The lesions were completely removed by surgery, and the histopathological findings showed that the epidermal depression expanded like a volcanic crater filled with keratinocytes and keratin. Squamous epithelial nests infiltrated into the deep irregularly with smooth contours. The top of the deep epithelial nests had increased keratinized beads. The keratinocytes had rich cytoplasm and were eosinophilic. Some epithelial cells were atypical, accompanied by an obvious inflammatory reaction. The adjacent epidermis formed an exogenic protrusion, creating a lip-like contour (Figure 2). These elements are consistent with KA, so a final diagnosis of Agglomerate KAs was made based on clinical-pathological findings. We have conducted regular follow ups for the last six years and there has been no recurrence.
 |
Figure 1 Four red nodules of different sizes, from 4 mm×3 mm to 10 mm×6 mm, were seen on the right chest, with a crater-like horn plug in the center. Lesions were clustered together and looked like a “lucky four-leaf clover”. |
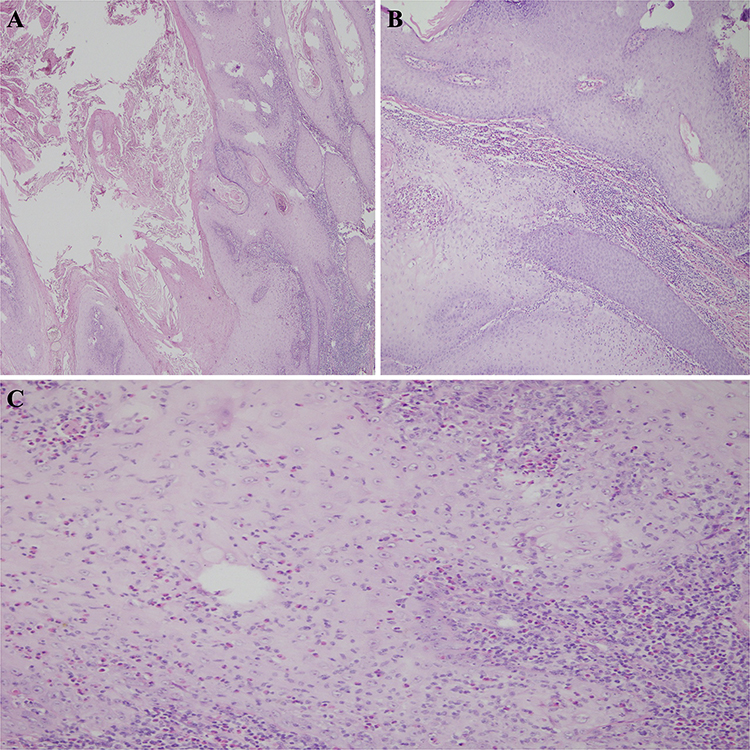 |
Figure 2 Histopathological Findings. (A) The epidermal depression expanded like a volcanic crater filled with keratinocytes and keratin (HE×40). (B) Squamous epithelial nests infiltrated into the deep irregularly with smooth contours. The top of the deep epithelial nests had increased keratinized beads. The keratinocytes had rich cytoplasm and were eosinophilic (HE×100). (C) A large number of inflammatory cells infiltrated the superficial dermis. Some epithelial cells were atypical. The adjacent epidermis formed an exogenic protrusion, creating a lip-like contour (HE×200). |
Discussion
KA is a rapidly growing epithelial tumor of the skin with a spontaneous involution. Lesions often occur in ultraviolet (UV) irradiation areas, but also perianal, perineum, and under the nails.1 In 2001 Ackerman and Choonhakam attempted to separate KAs into two categories, follicular and non-follicular, based on distinct clinical and histologic features they found at different anatomic locations.2 A KA typically goes through three stages of clinical development, hyperplasia, maturity, and regression, which usually takes four to nine months. In our case the lesions increased rapidly for about six months.
The etiology remains unknown and may be associated with myelodysplastic syndrome, immunosuppression, the use of medications, or red tattoos. Gualdi Giulio reported a 84-year old male patient who had a large number of KAs after clavicular surgery that might have been related to Koebnerization.3 Zhu reported a female patient with myelodysplastic syndrome who developed multiple nodules in her right ear and on her eyebrow during a three-drug chemotherapy treatment with decitabine, aclarubicin, and azacytidine.4 In 2008 Goldenberg presented the first case of multiple KAs after a colored tattoo.5 Since then, an increasing number of similar cases have been reported. Interestingly, most tattoo cases appear to be associated with red tattoo pigment.6 In our case the patient had none of the above factors, however, he is a farmer and may have experienced long-term exposure to UV light during outdoor farming activities.
KA is generally divided into two categories, either single type or multiple types based on clinical presentation. Multiple types have been described in several typical clinical forms, including the Agglomerate type, Ferguson-Smith type, Witten-Zak type, and Generalized Eruptive Keratoacanthoma (GEKA) of Grzybowski.7 The Ferguson-Smith type is the most commonly described multiple KAs.8 Agglomerate KA is a fusion of several individual KAs, while other types of Multiple KA exist in isolation.9 In our case, four nodules are arranged together, which is a typical Agglomerate type. Due to the limited number of clinical reports on Agglomerate KA there is a heightened risk of misdiagnosis, often mistaken for Verrucous Carcinoma or SCC.
The treatment of KA includes surgery, systemic treatments, and topical treatments. For a single type of solitary KA, a surgical excision with a safety margin is the gold standard treatment.10 For those with multiple or large lesions, the most commonly treatment involves medical therapy. Medical treatments include acitretin and systemic chemotherapies such as methotrexate (MTX) or 5-fluorouracil (5-FU). Elston reported that a patient with a huge facial KA was treated with oral MTX in doses similar to those given for psoriasis, and the lesion subsided.11 To avoid systemic toxicities, other methods like intralesional therapy, photodynamic therapy, cryotherapy, and topical creams are sometimes better alternatives. Intralesional administration of MTX, 5-FU, or Interferon alpha (INF-α) appear to be the most effective alternatives to surgical excision and systemic drug therapy.10 Zhu presented a case in which the skin lesions of a KA patient resolved after eight weeks of treatment with 5% imiquimod cream.4 Additionally, Pham reported the successful treatment of a patient with multiple KAs associated with Ferguson-Smith syndrome using cetuximab and cisplatin.12 The four lesions in our case clumped together and were completely removed after just a one-time operation.
Interestingly, to our knowledge this is the first four-leaf clover shape KAs that have been reported. After a 6-year follow-up no progression or recurrence was observed.
Conclusion
This report highlights a rare case of Agglomerate KAs. Dermatologists should be mindful of this unusual cutaneous manifestation.
Ethical Concerns
Written informed consent was obtained from the patient for the publication of the case details including the images. Institutional approval was not required for publishing these case details.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Paulson N, Gibson J, Glusac E. Perianal and perineal keratoacanthoma: two cases demonstrating histologic similarity to subungual keratoacanthoma. J Cutan Pathol. 2019;46(10):794–797. doi:10.1111/cup.13518
2. Choonhakarn C, Ackerman AB. Keratoacanthomas: a new classification based on morphologic findings and on anatomic site. Dermatopathol Pract Concept. 2001;7(1):7–16.
3. Gualdi G, Frasci F, Amerio P. Post-surgical eruptive keratoacanthoma: koebner is not enough. Int J Dermatol. 2022;61(6):766–768. doi:10.1111/ijd.15768
4. Zhu P, Wang Y. Multiple keratoacanthomas in a patient with myelodysplastic syndrome. Lancet Haematol. 2021;8(1):e94. doi:10.1016/S2352-3026(20)30363-X
5. Goldenberg G, Patel S, Patel MJ, et al. Eruptive squamous cell carcinomas, keratoacanthoma type, arising in a multicolor tattoo. J Cutan Pathol. 2008;35(1):62–64. doi:10.1111/j.1600-0560.2007.00764.x
6. Kluger N, Koljonen V. Tattoos, inks, and cancer. Lancet Oncol. 2012;13(4):e161–168. doi:10.1016/S1470-2045(11)70340-0
7. Kato N, Ito K, Kimura K, et al. Ferguson Smith type multiple keratoacanthomas and a keratoacanthoma centrifugum marginatum in a woman from Japan. J Am Acad Dermatol. 2003;49(4):741–746. doi:10.1067/S0190-9622(03)00454-7
8. Feldman RJ, Maize JC. Multiple keratoacanthomas in a young woman: report of a case emphasizing medical management and a review of the spectrum of multiple keratoacanthomas. Int J Dermatol. 2007;46(1):77–79. doi:10.1111/j.1365-4632.2006.02948.x
9. Schwartz RA. Keratoacanthoma. J Am Acad Dermatol. 1994;30(1):1–22. doi:10.1016/S0190-9622(94)70001-X
10. Kiss N, Avci P, Bánvölgyi A, et al. Intralesional therapy for the treatment of keratoacanthoma. Dermatol Ther. 2019;32(3):e12872. doi:10.1111/dth.12872
11. Elston DM. Medical therapy for keratoacanthomas. J Am Acad Dermatol. 2020;83(5):1544–1545. doi:10.1016/j.jaad.2020.06.1011
12. Pham F, Buiret G, Bonnet-Dupeyron MN, et al. Multiple and aggressive keratoacanthomas associated with Ferguson-Smith syndrome, successfully treated by cetuximab and cisplatin. Eur J Dermatol. 2021;31(2):271–272. doi:10.1684/ejd.2021.4025
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.