")
Back to Journals » International Journal of General Medicine » Volume 17
Genetic Polymorphisms of Endothelial Nitric Oxide Synthase Associated with Hypertension and Blood Homocysteine Levels
Authors Chaichanabut C, Sritara P, Sirivarasai J
Received 25 January 2024
Accepted for publication 9 April 2024
Published 20 April 2024 Volume 2024:17 Pages 1509—1519
DOI https://doi.org/10.2147/IJGM.S456519
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Yuriy Sirenko
Charinya Chaichanabut,1 Piyamitr Sritara,2 Jintana Sirivarasai3
1Master of Science Program in Nutrition, Faculty of Medicine Ramathibodi Hospital and Institute of Nutrition, Mahidol University, Bangkok, Thailand; 2Department of Medicine, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand; 3Nutrition Unit, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Jintana Sirivarasai, Nutrition Unit, Faculty of Medicine Ramathibodi Hospital, Mahidol University, Bangkok, 10400, Thailand, Tel +662-201-1483, Fax +662-201-2625, Email [email protected]
Purpose: Endothelial dysfunction is a key mechanism in the development of hypertension and is closely linked to impairment of endothelial nitric oxide synthase (eNOS) and hyperhomocysteinemia. Genetic polymorphisms of eNOS (rs1799983 and rs2070744) are strongly associated with the risk of hypertension in individuals of Asian ethnicities. This study aimed to investigate the relationship between these polymorphisms and the risk of hypertension associated with homocysteine levels.
Participants and Methods: For this cross-sectional study, we enrolled 370 Thai men aged 40– 60 years from the Electricity Generating Authority of Thailand cohort study for both variants genotyping by TaqMan allelic discrimination analysis. Clinical, anthropometric, and biochemical parameters were also analyzed.
Results: In the high blood pressure group (n = 267), systolic and diastolic blood pressure and triglyceride levels were higher in those with homocysteine levels ≥ 15 μmol/L than in those with homocysteine levels < 15 μmol/L (p < 0.05). Significant risk of hypertension was found in GG and GT of rs1799983 (G894T), and in TT and TC of rs2070744 (T-786C), with higher ORs in heterozygous genotypes (all p values < 0.05). Further evaluation of the interactions between SNPs and HCY revealed that individuals with the GT or TC genotype, together with hyperhomocysteinemia, had an increased risk of hypertension (all p< 0.05).
Conclusion: eNOS variants rs1799983 and rs2070744 may be risk factors for hypertension linked to hyperhomocysteinemia. These findings provide potentially useful healthcare strategies for the management of hypertension.
Keywords: endothelial nitric oxide synthase, polymorphisms, hypertension, hyperhomocysteinemia
Introduction
The global prevalence of hypertension has increased dramatically over the past two decades. The World Health Organization reported that in 2020, an estimated 1.28 billion adults aged 30–79 years worldwide had hypertension, two-thirds of whom were living in low- and middle-income countries.1 A cross-sectional study investigated the behavioral and metabolic risk factors for noncommunicable diseases based on an analysis of a survey conducted among 2311 adults (≥18 years). The results showed that the prevalence of metabolic risk factors, including age, smoking, alcohol consumption, and work status, was more pronounced in men and was related to high blood pressure, overweight and obesity, cholesterol level, and blood glucose level.2 In the Thailand National Health Security Office program, the prevalence of hypertension among men was found to be 37.8%, of which 23.9% of cases were uncontrolled.3 Established mechanisms associated with the development of hypertension include hyperhomocysteinemia (plasma concentration ≥ 15 µmol/L), which is recognized as a risk factor for cardiovascular diseases including the onset of hypertension.4 The proposed mechanisms involve homocysteine (HCY)-induced vascular damage, including increased smooth muscle cell proliferation, stimulated oxidation of the vascular endothelium, decreased vascular elasticity, and increased sodium reabsorption.5 The current study among patients with newly diagnosed primary hypertension reported an association between plasma total homocysteine levels and systolic blood pressure (SBP) (r = 0.696), diastolic blood pressure (DBP) (r=0.585), and age (r= 0.286).6 A cross-sectional study of 2615 Chinese people discovered that higher HCY levels were substantially linked to hypertension risk and influenced by interactions with age, obesity, dyslipidemia, and family history of the condition (all p < 0.05).7
Impairment of nitric oxide (NO) bioavailability can lead to endothelial dysfunction, which is a significant risk factor for hypertension. NO production is based on the function of endothelial NO synthase (eNOS or NOS3), which metabolizes l-arginine to NO. Decreased NO production promotes an imbalance in vascular homeostasis, leading to prothrombotic, proinflammatory, and less compliant blood vessel walls.8,9 Consequently, it is biologically plausible that functional eNOS polymorphisms may serve as potential biomarkers for susceptibility to hypertension. Several eNOS polymorphisms associated with hypertension have been identified. The eNOS single nucleotide polymorphism (SNP) rs1799983 (G894T) in exon 7 causes the replacement of glutamate by aspartate (Glu298Asp) and affects the structure and activity of eNOS, thereby decreasing NO availability. The production of basal NO in patients with high blood pressure patients was significantly lower than that in the healthy controls.10 Another SNP, rs2070744 (T-786C), indicates thymine-to-cytosine conversion in the 5′-flanking region of eNOS. This polymorphism is associated with the development of hypertension via the modulation of transcription, which influences translation efficiency, mRNA stability, and enzyme levels.10
A case-control study of hypertension in 154 participants (77 cases and 77 controls) revealed that the C allele of rs2070744 (T-786C) is associated with an increased risk of developing essential hypertension.11 A study of 2459 Han Chinese participants observed correlations between eNOS variants rs1799983 (G894T) and rs2070744 (T-786C) and the risk of essential hypertension.12 According to a meta-analysis of 63,258 participants, both variants were significantly related to the likelihood of developing hypertension. Analysis of the Asian subgroup indicated that both the T allele of rs1799983 (G894T) and the C allele of rs2070744 (T-786C) increased susceptibility to hypertension.13 Furthermore, the underlying molecular changes caused by hyperhomocysteinemia-mediated endothelial dysfunction involve the inhibition of nitric oxide (NO) production, directly interfering with the functions of eNOS, inactivating eNOS by upregulating caveolin-1, and decreasing the L-arginine transport systems for eNOS–NO synthesis by suppressing the cationic amino acid transporter family.14,15 Another significant cause of hypertension is HCY-induced oxidative stress, which results in an increase in the endogenous eNOS inhibitor asymmetric dimethylarginine (ADMA).16 A previous study found that eNOS G894T and 4a/b gene polymorphisms associated with total HCY levels have a substantial impact on blood pressure.17
Based on the various causes of endothelial dysfunction, there are limited data indicating the influence of eNOS polymorphisms and HCY on hypertension. Our findings deepen our understanding of hypertension and the complexity of its physiological regulation at the molecular level. Therefore, we aimed to investigate the association between two functional SNPs of eNOS, rs1799983 (G894T) and rs2070744 (T-786C), and their potential interaction with plasma HCY levels in the development of hypertension in men.
Materials and Methods
Study Design, Participants and Data Collection
This was a cross-sectional study of Thai male participants (N=370) aged 40–60 years who were recruited from the Electricity Generating Authority of Thailand (EGAT) cohort study in 2018 (the EGAT study began in 1985 and resurveys participants every 5 years). The details of this cohort study have been described.18 We extracted information from original datasets (in 2018) related to demographics, body composition/clinical measurement, laboratory tests, and questionnaires contained in the EGAT database with specific high-risk group of age 40–60 years. In addition, the participants underwent physical examination and blood collection for biochemical analysis, and answered questionnaires on demographic data and lifestyle factors. Participants with the following conditions were excluded from the study: metabolic syndrome with medical treatment; secondary hypertension; cancer; metabolic disease (ie, thyroid, osteoarthritis, or immune disease) with pharmacological treatment; and chronic liver and kidney diseases. The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the Faculty of Medicine Ramathibodi Hospital, Mahidol University (COA.MURA 2021/230 and 2023/98). At the time of recruitment, informed consent was obtained from each participant.
Anthropometric and Biochemical Measurements
Participants visited the research site between 7:00 AM and 10:00 AM, after an overnight fast. Venous blood samples were collected for DNA extraction and biochemical analysis, as follows: fasting blood glucose (FBS), glycosylated hemoglobin A1C (HbA1C), total cholesterol, triglycerides, high-density lipoprotein cholesterol (HDL-C), low-density lipoprotein cholesterol (LDL-C), uric acid, creatinine, and blood urea nitrogen. These parameters were measured using an automated method (Roche COBAS, Mannheim, Germany). Plasma HCY concentrations were determined using direct electrochemiluminescence immunoassay (Abbott Laboratories, Abbott Park, IL, USA). This analysis is based on the reaction of dithiothreitol to reduce bound or dimerized homocysteine (oxidized form) to free homocysteine. Subsequently, free homocysteine is converted to S-adenosyl homocysteine. S-adenosyl homocysteine then contests with acridinium-labeled S-adenosyl cysteine for a particle-bound monoclonal antibody.19 During the same visit, anthropometric and blood measurements were obtained by trained research staff. Body mass index (BMI) was calculated using the standard formula of body weight (in kilograms) divided by the square of height (in meters). SBP and DBP were measured on the right arm in a semi-flexed position at heart level, with the participants in a supine position and after 10 min of rest. In adults, SBP >120 mmHg and DBP > 80 mmHg were considered indicative of high blood pressure.20
Genetic Analysis
To discriminate between the eNOS G894T (rs1799983) G and T and eNOS −786T/C (rs2070744) T and C alleles, TaqMan Pre-Designed SNP Genotyping Assays (Applied Biosystems, USA) were used, including primers and fluorescently labeled (FAM and VIC) MGB probes, in accordance with the procedures recommended by the manufacturer. Fifteen microliters of the reaction mixture (Master Mix, Primer-probe Assay, H2O) and 5 µL of DNA were added to the multiwell plates for each sample. The analysis was performed by RT-PCR (LC480; Roche, Basel, Switzerland). The PCR procedure for both SNPS was as follows: denaturation at 95° °C for 600s, amplification (40 cycles) consisting of denaturation at 95° °C for 15s, annealing at 60° °C for 60s, and cooling at 40° °C for 30s.
Statistical Analysis
Statistical analyses were performed using the SPSS statistical software version 25 (IBM, Inc., Armonk, NY, USA). The sample size in this cross-sectional study was calculated based on the prevalence of hypertension cases ~33.42% in males aged 45–59 years from the National Health Examination Survey Office, Health System Research Institute (2014).21 The minimum number of participants was 340. All continuous variables were tested for normality using the Kolmogorov–Smirnov test. For data with a normal distribution, the baseline characteristics for each group were reported as means, and standard deviations as well as for non-normal variables were presented as median(IQR). Categorical variables are presented as numbers or frequencies (%) and were compared using the chi-squared test. Differences between groups were analyzed using independent t-tests and analysis of variance. Statistical significance was set at p < 0.05. The SNPStats web tool (www.snpstats.net/start.htm) was used to evaluate the association between the two eNOS SNPs and the susceptibility to hypertension. The overall genetic data were also analyzed, including allelic and genotypic frequencies, to estimate the Hardy-Weinberg equilibrium, inheritance mode (co-dominant, dominant, overdominant, and recessive), linkage disequilibrium (LD), association of eNOS SNP haplotypes with the risk of hypertension, and interaction with plasma HCY. Hyperhomocysteinemia was defined as a plasma HCY level ≥ 15 μmol/L. The OR (odds ratio) for each genotype or both genotypes with respect to the reference genotype was adjusted for BMI, WC, WHR, TG, and LDL-C.
Results
Baseline Characteristics of the Study Population
This study included 370 Thai men from the EGAT cohort study. Participants were assigned to either the normal blood pressure group (103 participants) or the high blood pressure group (267 participants) based on their blood pressure levels. The mean age of the study population was 57.68 ± 1.39 years, and there were no significant differences in age between the normal blood pressure and high blood pressure groups (57.63 ± 1.37 and 57.70 ± 1.49 years, respectively). The high blood pressure group had significantly higher BMI, waist circumference, waist-to-hip ratio, SBP, DBP, triglyceride level, and LDL-C level than the normal blood pressure group (p < 0.05). However, HCY levels in both groups were high compared to the normal reference levels (5.00–15.00 µmol/L). There were no significant differences in smoking, alcohol consumption, or family history between the two groups (Table 1).
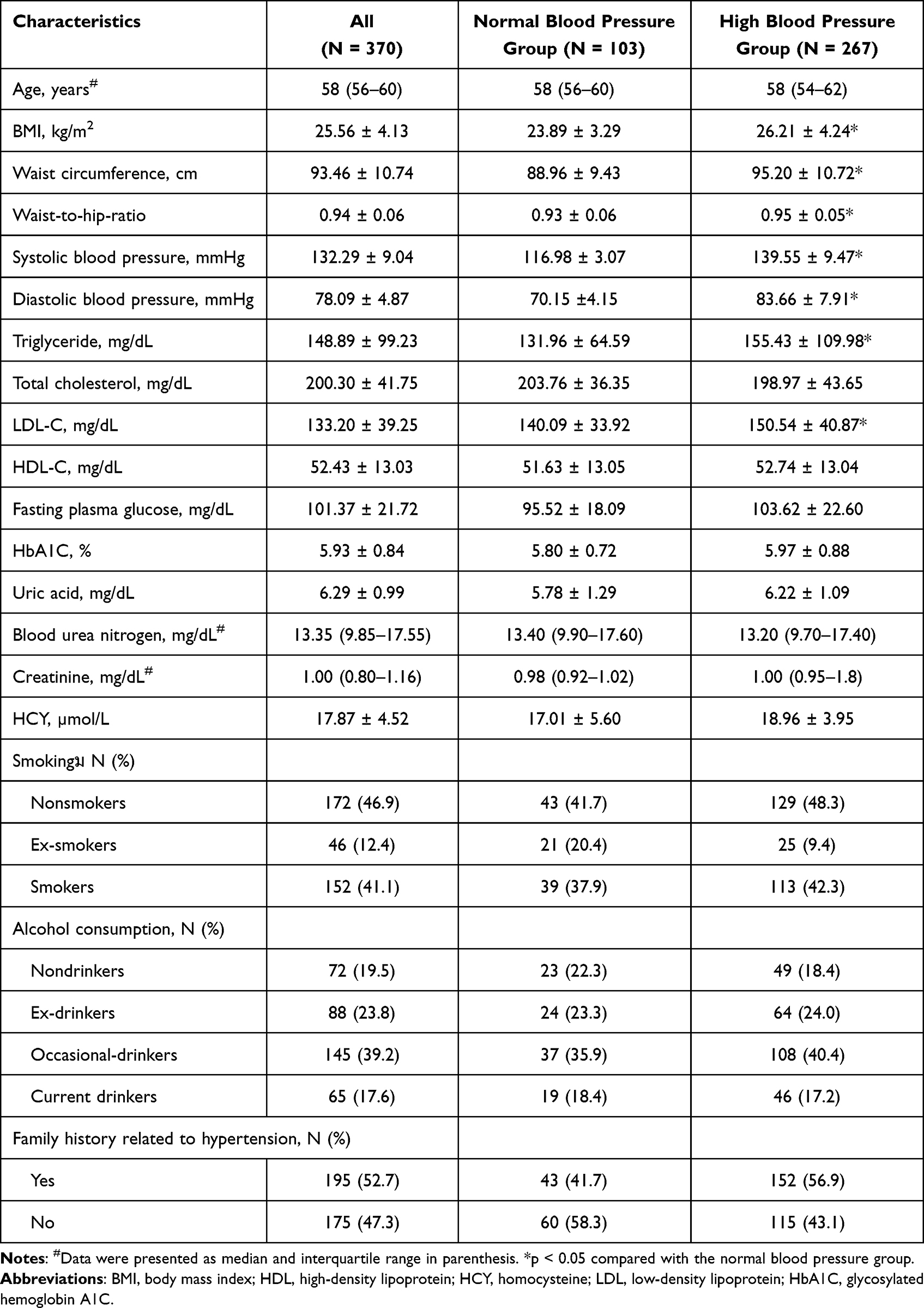 |
Table 1 Characteristics, Biochemical Parameters, and Lifestyle Factors of the Study Population |
Additionally, in the high blood pressure group, those with HCY ≥15 µmol/L had significantly higher SBP (145.57 ± 15.72 vs 138.47 ± 13.62 mmHg), DBP (82.65 ± 9.49 vs 78.16 ± 9.76 mmHg) and triglyceride levels (161.91 ± 119.52 vs 131.50 ± 57.78 mg/dL) than those with plasma HCY < 15 µmol/L (p < 0.05) (Table 2).
 |
Table 2 Comparison Between Clinical and Biochemical Parameters Among Two Groups Based on Homocysteine Levels |
Association of eNOS Variants rs1799983 (G894T) and rs2070744 (T-786C) with the Risk of Hypertension and Plasma HCY Levels
In all study groups, the genotypic frequencies of eNOS rs1799983 (G894T) were 67.3% for GG, 28.4% for GT, and 4.3% for TT. Regarding eNOS rs2070744 (T-786C), the genotypic frequencies were 79.7%, 19.5%, and 0.8% for TT, TC, and CC, respectively. The minor allele frequencies of eNOS rs1799983 (G894T) and rs2070744 (T-786C) were 0.18 and 0.10, respectively. The distributions of both variants were consistent with the Hardy-Weinberg equilibrium (χ2= 1.31 and 0.38 for rs1799983 and rs2070744, respectively; all p > 0.05).
Both variants were significantly associated with a high BP (Table 3). Additionally, we further examined the role of each variant in the risk of hypertension using a genetic model of inheritance (codominant, dominant, recessive, overdominant, and log-additive) and unconditional logistic regression analysis (Table 4). Odds ratios (ORs) were adjusted for BMI, WC, WHR, and TG and LDL-C levels. Analysis of the results showed significant associations between the TT genotype in rs1799983 and increased risk of hypertension under the codominant (OR = 15.97, 95% confidence interval [CI] = 2.03–125.92, P = 0.0001), dominant (OR = 5.05, 95% CI = 2.89–8.81, P = 0.0001), recessive (OR = 10.87, 95% CI = 1.39–85.12, P = 0.0019), overdominant (OR = 4.01, 95% CI = 2.37–7.08, P = 0.0001) and log-additive (OR = 4.38, 95% CI = 2.61–7.36, P = 0.001) models. For rs2070744, there were statistical relationships between the TC genotype and susceptibility to hypertension in the codominant (OR = 2.16, 95% CI = 1.19–3.90, P = 0.0095), dominant (TC-CC; OR = 2.26, 95% CI = 1.25–4.07, P = 0.0048), overdominant (OR = 2.13, 95% CI = 1.18–3.85, P = 0.0098) and log-additive (OR = 2.27, 95% CI = 1.28–4.03, P = 0.0033) models.
 |
Table 3 Analysis of the Associations Between eNOS Genotypes and Blood Pressure |
 |
Table 4 Association of ENOS Polymorphisms with the Risk of Hypertension (≥ 130/80 mmHg) by Inheritance Mode (Odd Ratios Were Adjusted for BMI, WC, WHR, TG and LDL-C) |
Interactions between SNPs, the risk of hypertension, and hyperhomocysteinemia are shown in Table 5. The findings also indicated influence of the GT genotype in rs1799983 (G894T) and the TC genotype in rs2070744 (T-786C) on the risk of hypertension among individuals with plasma HCY < 15 µmol/L, with ORs of 4.75 (95% CI = 1.69–13.36) and 3.23 (95% CI = 1.15–9.05), respectively (all P<0.05). For hyperhomocysteinemia, significant risk of hypertension was found in GG and GT of rs1799983 (G894T), and in TT and TC of rs2070744 (T-786C), with higher ORs in heterozygous genotypes (OR = 10.58, 95% CI = 4.76–23.51 for GT and OR = 4.88, 95% CI = 2.18–10.93 for TC, all P<0.05).
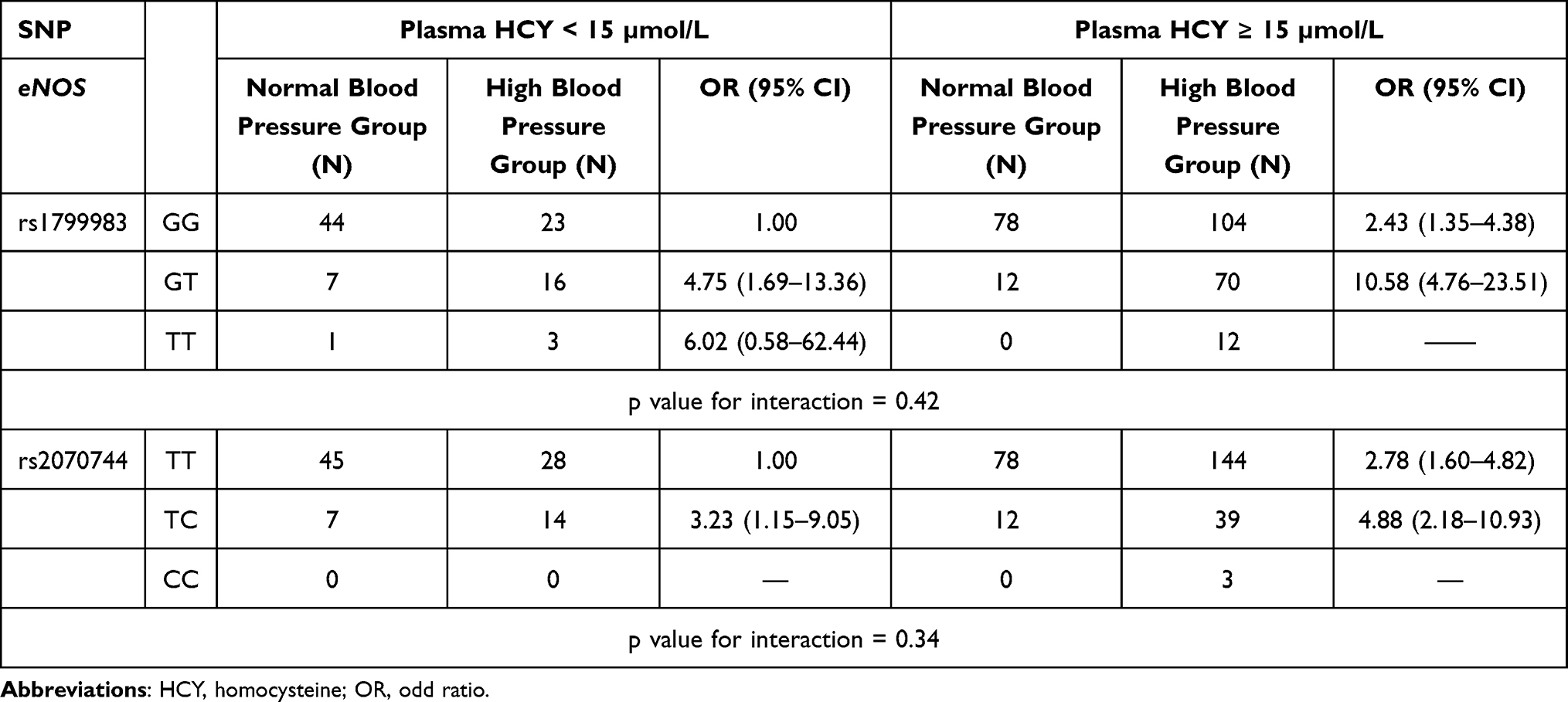 |
Table 5 Interaction Analysis of ENOS Polymorphisms with the Risk of Hypertension in Relation to Hyperhomocysteinemia (Odd Ratios Were Adjusted for BMI, WC, WHR, TG and LDL-C) |
Based on the results obtained using SNPStats, allelic associations calculated with D’ = 0.57 and R2 = 0.24 indicated that both SNPs were in LD. Of the four eNOS constructed from the two SNPs, TT, GC, and TC were significantly associated with an increased risk of hypertension in the logistic regression model adjusted for BMI. Among individuals with hyperhomocysteinemia, the TC haplotype conferred the highest risk of hypertension (OR = 16.35, 95% CI = 3.73–71.65).
Discussion
HCY is an established risk factor for hypertension and its associated complications. In this study, HCY levels were high compared to the normal reference levels, and hyperhomocysteinemia significantly exacerbated the increases in SBP and DBP in the high blood pressure group. These findings highlight the involvement of HCY in the regulation of BP. Similar results were found in a cross-sectional study of patients diagnosed with primary hypertension, which showed positive correlations between increased plasma total HCY levels and SBP, DBP, and age.6 A previous study revealed that among patients with hyperhomocysteinemia, increased plasma HCY was positively correlated with plasma asymmetric dimethylarginine but negatively correlated with plasma NO (all p < 0.001).22 These findings indicate dysregulation of the NOS pathway and the development of hypertension caused by HCY. Additionally, we found that participants with hypertension and hyperhomocysteinemia had higher TG levels than those with plasma HCY levels < 15 µmol/L, which is comparable to a study in a Chinese population.23 In multivariable logistic-regression analysis, participants with hyperhomocysteinemia had risk of dyslipidemia, namely, low HDL-C and hypertriglyceridemia, with significantly adjusted ORs of 1.406 (95% CI = 1.143–1.728) and 1.293 (95% CI = 1.096–1.524), respectively.24 The underlying mechanism of these associations may involve: 1) HCY-induced expression of sterol regulatory element-binding proteins, which subsequently increase the intracellular accumulation of total cholesterol and triglycerides; and 2) HCY-mediated oxidative stress of the endoplasmic reticulum and prolonged expression of misfolded proteins, causing increased hepatic biosynthesis and uptake of cholesterol and triglycerides.24
eNOS plays an important role in the molecular mechanisms that regulate NO signaling. Frequently occurring SNPs in the promoter (˗786T/C of rs2070744) and exon 7 (G894T and Glu298Asp of rs1799983) of eNOS are the most well-studied functionally associated variants.20 Several studies have found that eNOS polymorphic variations change the rate of eNOS transcription and/or processing, thereby impairing its enzymatic activity and prompting extensive investigation into their relevance in many diseases, including hypertension.25 In the present study, we found significant associations between eNOS rs1799983 and rs2070744 and the risk of hypertension. The allele frequencies of these SNPs among the Thai population in this study (0.18 for rs1799983 and 0.10 for rs2070744) were similar to MAFs of 0.13 and 0.10 for the two SNPs in Chinese26 and Korean27 populations, but were lower than those in Europeans (0.25 for rs1799983 and 0.37 for rs2070744).28 In a previous study in Chinese men, those with the rs1799983 genotype had significantly higher SBP and DBP than those with the wild-type genotype (161.8 ± 20.2 vs 154.3 ± 8.1 mmHg, p = 0.013 and 102.8 ± 9.6 vs 99.5 ± 7.8 mmHg, p = 0.02, respectively).29 Additionally, analysis of covariance in male subjects with high blood pressure revealed combined effects of this SNP, alcohol consumption, and smoking on SBP and DBP (p = 0.034 and p = 0.043, respectively).29
In this study, strong associations with the risk of hypertension were found for TT variants of rs1799983 in the codominant, dominant, recessive, overdominant, and log-additive models and for TC-TT variants of rs2070744 in the codominant, dominant, overdominant, and log-additive models (Table 4). Although the human eNOS gene is highly polymorphic, the previously reported effects of these variants on susceptibility to hypertension have been inconsistent. A genetic study among Han Chinese did not identify significant associations between eNOS polymorphisms (T-786C, intron4b/a, and G894T) and EH in three genetic models using single-locus analyses.30 For T-786C, there was no association between variant genotypes and risk of hypertension (OR = 1.12, 95% CI = 0.97–1.29, p = 0.137). However, ORs in subgroup analyses by ethnicity only suggested positivity for hypertension in white individuals with the 2786C allele and 2786CC genotype.31 Alter-native explanations for the effects of eNOS variants on hypertension involve changes in the protein sequence and structure, causing enzyme dysfunction in the Glu298Asp (G894T) variant, and a 50% decrease in transcription of eNOS in the T-786→C promoter substitution variant. Overall, these changes in eNOS polymorphisms result in decreased NO production and vasoreactivity.32
Further evaluation of the interactions between SNPs and HCY (Table 5) revealed that individuals with the GT or TC genotype, together with hyperhomocysteinemia, had an increased risk of hypertension. We hypothesized that the mechanism underlying this interaction might be linked to decreased NO bioavailability due to abnormal functioning of eNOS and exposure of endothelial cells to HCY, causing increased superoxide anion (O2-.) via the uncoupling of eNOS and formation of S-nitrosohomocysteine.33
Haplotype analysis undertaken for more accurate risk prediction revealed that haplotype 894T/-786C, which had moderate LD, was associated with an increased risk of high blood pressure in our Thai study population (Table 6), especially among those with hyperhomocysteinemia. Data supporting the effect of these polymorphisms on impaired enzyme function and hyperhomocysteinemia-induced endothelial dysfunction in association with NO inhibition in the development of hypertension are possible. A previous study genotyped two polymorphisms of eNOS in 105 high-blood pressure patients and identified 786C894G as the risk haplotype for metabolic syndrome susceptibility (p = 0.011).34 However, a case-control study investigating rs1799983, a VNTR in intron 4, and rs2070744 in essential hypertension found only significant ORs for the risk of hypertension in the haplotype of rs1799983 with intron 4 VNTR.35 These discrepancies may be due to differences in the sample size, age, hypertension criteria, other metabolic diseases, study design, lifestyle factors, and ethnic differences within the distribution of eNOS genetic variants.
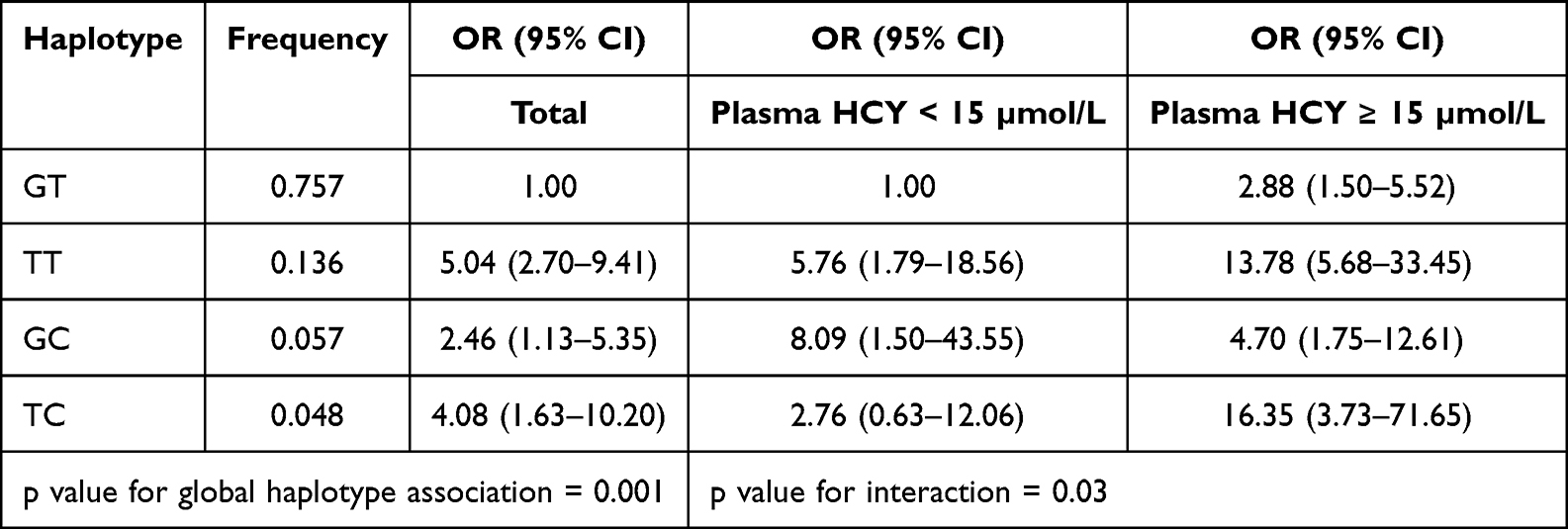 |
Table 6 Haplotype Analysis of ENOS Polymorphism and Risk of Hypertension (Odd Ratios Were Adjusted for BMI, WC, WHR, TG and LDL-C) |
In this study, we provided evidence that eNOS polymorphisms and their interaction with hyperhomocysteinemia are involved in the development of endothelial dysfunction through mechanisms of the NO pathway. The potential pathways might be the functional impairment of eNOS by polymorphism, together with other possible causes such as inhibition of this enzyme by HCY-induced ADMA level16 or interactions between eNOS genotype and decreased serum folate, leading to elevated HCY level.36 Recent advances exemplifying the physiological role of NOS and the mechanisms of dysfunctional and dysregulated NOS in cardiovascular disease have been proposed as therapeutic targets in cardiovascular disease.37 Overall, the associations between these studies and our study can provide an important strategy in the therapeutic approach for hypertension related to improved NOS activity and nutritional supplementation with folate and vitamin B12 to reduce the risk of hyperhomocysteinemia. However, this study has several limitations. The small sample size for subgroup genetic analysis may have reduced the power of the study to predict the risk of hypertension. Cross-sectional studies limit to establish cause-and-effect relationships. Biomarkers related to NO levels and oxidative stress (such as malondialdehyde and protein carbonyl) were not measured in our study. Further studies using these biomarkers will provide supportive evidence for hypertension-related HCY and endothelial dysfunction. In addition, as is the case for Thai populations, it may not be generalized for SNPs specifically in hypertension in specific geographic, racial, and ethnic populations, including the identification of persons at risk for developing hypertension.
Conclusion
In this study, we demonstrated an association between genetic polymorphisms in exon 7 and the promoter region of eNOS, together with high plasma HCY levels, with a causal role in hypertension through a key vascular mechanism of endothelial dysfunction. This information on genetic susceptibility is valuable for vulnerable individuals and can be applied in the development of molecular etiological strategies to prevent and treat hypertension.
Acknowledgments
This research was funded by the Thailand Research Fund (Grant Number 485/2563). We would like to express our thanks to all the Electricity Generating Authority of Thailand study participants, as well as the research staff at the Research and Innovation Center, Faculty of Medicine Ramathibodi Hospital, Mahidol University.
Disclosure
The authors report no conflicts of interest in this work.
References
1. World Health Organization. Hypertension; 2021. Available from: https://www.who.int/news-room/fact-sheets/detail/hypertension.
2. Majić A, Arsenović D, Čvokić DD. Behavioral and metabolic risk factors for noncommunicable diseases among population in the Republic of Srpska (Bosnia and Herzegovina). Healthcare. 2023;11(4):483. doi:10.3390/healthcare11040483
3. Sakboonyarat B, Rangsin R, Kantiwong A, et al. Prevalence and associated factors of uncontrolled hypertension among high blood pressure patients: a nation-wide survey in Thailand. BMC Res Notes. 2019;12(1):380. doi:10.1186/s13104-019-4417-7
4. Maron BA, Loscalzo J. The treatment of hyperhomocysteinemia. Annu Rev Med. 2009;60(1):39–54. doi:10.1146/annurev.med.60.041807.123308
5. Tinelli C, Di Pino A, Ficulle E, et al. Hyperhomocysteinemia as a risk factor and potential nutraceutical target for certain pathologies. Front Nutr. 2019;6:49. doi:10.3389/fnut.2019.00049
6. Tran SK, Ngo TH, Nguyen PH, et al. Hyperhomocysteinemia in patients with newly diagnosed primary hypertension in Can Tho City, Vietnam. Healthcare. 2023;11(2):234. doi:10.3390/healthcare11020234
7. Yang B, Fan S, Zhi X, et al. Interactions of homocysteine and conventional predisposing factors on hypertension in Chinese adults. J Clin Hypertens. 2017;19(11):1162–1170. doi:10.1111/jch.13075
8. Cyr AR, Huckaby LV, Shiva SS, et al. Nitric Oxide and Endothelial Dysfunction. Crit Care Clin. 2020;36(2):307–321. doi:10.1016/j.ccc.2019.12.009
9. Hermann M, Flammer A, Lüscher TF. Nitric oxide in hypertension. J Clin Hypertens. 2006;8(12 Suppl 4):17–29. doi:10.1111/j.1524-6175.2006.06032.x
10. Shankarishan P, Borah PK, Ahmed G, et al. Endothelial nitric oxide synthase gene polymorphisms and the risk of hypertension in an Indian population. Biomed Res Int. 2014;2014:793040. doi:10.1155/2014/793040
11. Midoun AA, Kiando SR, Treard C, et al. Genetic association study between T-786C NOS3 polymorphism and essential hypertension in an Algerian population of the Oran city. Diabetes Metab Syndr. 2019;13(2):1317–1320. doi:10.1016/j.dsx.2019.02.024
12. Niu WQ, Qi Y, Zhang LT, et al. Endothelial nitric oxide synthase genetic variation and essential hypertension risk in Han Chinese: the Fangshan study. J Hum Hypertens. 2009;23(2):136–139. doi:10.1038/jhh.2008.111
13. Xie X, Shi X, Xun X, et al. Endothelial nitric oxide synthase gene single nucleotide polymorphisms and the risk of hypertension: a meta-analysis involving 63,258 subjects. Clin Exp Hypertens. 2017;39(2):175–182. doi:10.1080/10641963.2016.1235177
14. Skeete J, DiPette DJ. Relationship between homocysteine and hypertension: new data add to the debate. J Clin Hypertens. 2017;19(11):1171–1172. doi:10.1111/jch.13073
15. Chen Z, Oliveira SDS, Zimnicka AM, et al. Reciprocal regulation of eNOS and caveolin-1 functions in endothelial cells. Mol Biol Cell. 2018;29(10):1190–1202. doi:10.1091/mbc.E17-01-0049
16. Stühlinger MC, Stanger O. Asymmetric dimethyl-L-arginine (ADMA): a possible link between homocyst(e)ine and endothelial dysfunction. Curr Drug Metab. 2005;6(1):3–14. doi:10.2174/1389200052997393
17. Rodríguez Esparragón FJ, Rodríguez Pérez JC, Macías Reyes A, et al. Arterial blood pressure variations: homocysteine and nitric oxide synthase gene polymorphisms (NOS3). Nefrologia. 2006;26(5):559–563.
18. Vathesatogkit P, Woodward M, Tanomsup S, et al. Cohort profile: the electricity generating authority of Thailand study. Int J Epidemiol. 2012;41(2):359–365. doi:10.1093/ije/dyq218
19. Abbott, Abbott Architect System. Homocysteine; 2008. Available from: http://www.ilexmedical.com/files/PDF/Homocysteine_ARC.pdf.
20. Whelton PK, Carey RM, Aronow WS, et al. 2017 ACC/AHA/AAPA/ABC/ACPM/ AGS/APhA/ASH/ASPC/NMA/PCNA guideline for the prevention, detection, evaluation, and management of high blood pressure in adults: executive summary: a report of the American college of cardiology/American heart association task force on clinical practice guidelines. Hypertension. 2018;71(6):1269–1324. doi:10.1161/HYP.0000000000000066
21. The National Health Examination Survey Office, Health System Research Institute; 2014. Available from: https://www.hiso.or.th/hiso/picture/reportHealth/report/report9.pdf.
22. Holven KB, Haugstad TS, Holm T, et al. Folic acid treatment reduces elevated plasma levels of asymmetric dimethylarginine in hyperhomocysteinaemic subjects. Br J Nutr. 2003;89(3):359–363. doi:10.1079/BJN2002779
23. Momin M, Jia J, Fan F, et al. Relationship between plasma homocysteine level and lipid profiles in a community-based Chinese population. Lipids Health Dis. 2017;16(1):54. doi:10.1186/s12944-017-0441-6
24. Werstuck GH, Lentz SR, Dayal S, et al. Homocysteine-induced endoplasmic reticulum stress causes dysregulation of the cholesterol and triglyceride biosynthetic pathways. J Clin Invest. 2001;107(10):1263–1273. doi:10.1172/JCI11596
25. Vecoli C. Endothelial nitric oxide synthase gene polymorphisms in cardiovascular disease. In: Litwack G, editor. Vitamins & Hormones. 96: Academic Press; 2014:387–406.
26. Zhao GL, Li QJ, Lu HY. Association between NOS3 genetic variants and coronary artery disease in the Han population. Genet Mol Res. 2016;15(2):1–4.
27. Heidari MM, Khatami M, Tahamtan Y. Molecular analysis of rs2070744 and rs1799983 polymorphisms of NOS3 gene in Iranian patients with multiple sclerosis. Basic Clin Neurosci. 2017;8(4):279–284. doi:10.18869/nirp.bcn.8.4.279
28. Zmijewski P, Cieszczyk P, Ahmetov II, et al. The NOS3 G894T (rs1799983) and −786T/C (rs2070744) polymorphisms are associated with elite swimmer status. Biol Sport. 2018;35(4):313–319. doi:10.5114/biolsport.2018.76528
29. Hong Z, Pan L, Ma Z, et al. Combined effects of cigarette smoking, alcohol drinking and eNOS Glu298Asp polymorphism on blood pressure in Chinese male high blood pressure subjects. Tob Induc Dis. 2019;17:59. doi:10.18332/tid/110678
30. Zhao Q, Su SY, Chen SF, et al. Association study of the endothelial nitric oxide synthase gene polymorphisms with essential hypertension in northern Han Chinese. Chin Med J. 2006;119(13):1065–1071. doi:10.1097/00029330-200607010-00002
31. Niu W, Qi Y, Reitsma PH. An updated meta-analysis of endothelial nitric oxide synthase gene: three well-characterized polymorphisms with hypertension. PLoS One. 2011;6(9):e24266. doi:10.1371/journal.pone.0024266
32. Rossi GP, Taddei S, Virdis A, et al. The T-786C and Glu298Asp polymorphisms of the endothelial nitric oxide gene affect the forearm blood flow responses of Caucasian high blood pressure patients. J Am Coll Cardiol. 2003;41(6):938–945. doi:10.1016/S0735-1097(02)03011-5
33. Cheng Z, Yang X, Wang H. Hyperhomocysteinemia and endothelial dysfunction. Curr Hypertens Rev. 2009;5(2):158–165. doi:10.2174/157340209788166940
34. Fernandez ML, Ruiz R, Gonzalez MA, et al. Association of NOS3 gene with metabolic syndrome in high blood pressure patients. Thromb Haemost. 2004;92(2):413–418. doi:10.1160/TH04-02-0103
35. Gamil S, Erdmann J, Abdalrahman IB, et al. Association of NOS3 gene polymorphisms with essential hypertension in Sudanese patients: a case control study. BMC Med Genet. 2017;18(1):128. doi:10.1186/s12881-017-0491-7
36. Brown KS, Kluijtmans LA, Young IS, et al. Genetic evidence that nitric oxide modulates homocysteine: the NOS3 894TT genotype is a risk factor for hyperhomocystenemia. Arterioscler Thromb Vasc Biol. 2003;23(6):1014–1020. doi:10.1161/01.ATV.0000071348.70527.F4
37. Roy R, Wilcox J, Webb AJ, O’Gallagher K. Dysfunctional and dysregulated nitric oxide synthases in cardiovascular disease: mechanisms and therapeutic potential. Int J Mol Sci. 2023;24(20):15200. doi:10.3390/ijms242015200
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.