")
Back to Journals » Nursing: Research and Reviews » Volume 13
Grip Strength Among Indian Nursing Students and Staff: A Cross-Sectional Study
Authors Sadan V, Seetharaman B , Jesudoss I, Esther A, Roberts LR
Received 2 April 2023
Accepted for publication 29 September 2023
Published 3 October 2023 Volume 2023:13 Pages 31—39
DOI https://doi.org/10.2147/NRR.S412809
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pariya Fazeli
Vathsala Sadan,1 Bala Seetharaman,2 Ilavarasi Jesudoss,2 Angelin Esther,1 Lisa R Roberts3
1Christian Medical College-Vellore, College of Nursing, Vellore, Tamil Nadu, India; 2Christian Medical College-Vellore, Nursing Service Dept, Vellore, Tamil Nadu, India; 3Loma Linda University, School of Nursing, Loma Linda, CA, USA
Correspondence: Lisa R Roberts, Loma Linda University School of Nursing, 11262 Campus St, Loma Linda, CA, 92350, USA, Tel +1 909 558 1000, Fax +1 909 558 0719, Email [email protected]
Purpose: The aim of the current study was to measure grip strength along with correlates, to inform recommendations to protect students entering the nursing workforce and increase career longevity, as well as health, among working nurses.
Participants and Methods: A convenience sample of nursing staff and students (18 to 59 years) at a large teaching hospital (N = 316) participated in a cross-sectional study. A brief survey included sociodemographic questions, the Perceived Stress Scale (PSS-4), and the Nordic Musculoskeletal Questionnaire (NMQ). Anthropometric measures included height, weight, waist circumference, and hand grip strength using a Jamar digital dynamometer.
Results: Only 22.5% of the participants met Indian normative grip strength parameters by age and gender, and on average had a normal body mass index (M = 22.31, SD 4.15). Grip strength was significantly associated with BMI and waist circumference, which explained 76% of the variance in grip strength.
Conclusion: This study provides a baseline measurement of grip strength among Indian nursing staff and students, and documents grip strength among young adults (18– 20 years of age) who were not included in published normative grip strength data among healthy Indian participants. Data from the current study demonstrates that very few participants met normative grip strength, thus indicating the need for strengthening. Variance in grip strength was largely explained by waist circumference, pointing to the importance of nutrition. Interventions are needed to improve physical performance of nursing duties and prevent on-the-job injuries.
Keywords: nurses, occupational health, musculoskeletal disorders, on-the-job injuries
Introduction
Globally, nurses are at risk for on the job (OTJ) injuries or musculoskeletal disorders (MSD), contributing to disability, and leaving the nursing workforce.1–4 Nurses who are not physically fit or do not lead an active lifestyle may be at increased risk.4,5 Additional factors contributing to OTJ injuries or MSD include fatigue, compressed shift schedules, variability of shifts, physical capacity, and upper body strength.6–9 Grip strength is an upper body strength measure indicating overall muscle strength, which also predicts musculoskeletal health, disease development and progression, disability and mortality, or healthy ageing.10–12
A review of normative data for grip strength across different countries reveals a common pattern throughout the course of life with an increase across childhood to a peak in early adult life, a relatively constant maintenance in midlife, and a decline from midlife on. Differences between grip strength peak and decline may have slight immediate effects on health but could also pose long-term consequences such as premature aging, disability and higher mortality.11 Average grip strength also varies geographically.13 A systematic review examining global variation in grip strength indicated clear differences in mean values between developed and developing regions, with lower grip strength in developing regions. Grip strength of healthy Indian adults to age and gender matched adults with similar physical activity levels in the USA, Europe, and Australia found significantly lower grip strength among Indian men and women.14 The authors indicated that differences in body size and composition likely explain the regional differences in normative grip strength. Factors affecting body size include early growth, nutrition and genetics.14 Body composition including greater waist circumference, may indicate central obesity, a characteristic for metabolic syndrome, and associated with back and joint pain, decreased performance on physical fitness tests, and weaker grip strength.15–17 In addition to body mass index (BMI) and body composition, factors that may affect grip strength include age, gender, hours worked, years in profession, consecutive shifts, stress, exercise habits, and physical demand of clinical work.9,11,14,18,19
India faces a shortage of over one million nurses,20 therefore, preserving the current workforce of nurses is essential, in addition to training more nurses to fulfill the needs of the Indian population. Studies in India have indicated that nurses are at risk; Singh et al found 75% of the nurses observed to be at increased risk for MSDs and OTJ injuries due to the physical nature of the work and rapid movements required,20 Anap et al indicated that back and extremity MSDs and OTJ injuries are common, with 89.1% of the nurses in their sample having experienced work-related musculoskeletal symptoms,21 Paul et al using the standardized Nordic questionnaire found that more than half of the nurses had musculoskeletal complaints, preventing many of them from being able to do their work,22 and Yasobant indicated that compared to other healthcare workers, nurses are at the highest risk for MSDs and OTJ injuries.23 These risks may result in nurses leaving the profession or shortening their career, yet awareness, ergonomic training, and preventive efforts to protect nurses in India are lacking.20–24
Considering the current global nursing shortage, as well as the critical shortage of nurses anticipated in India,20,25 preparing students for the physically demanding aspects of nursing may be advantageous. A study in Australia indicated that nursing students experienced musculoskeletal symptoms, and despite regular exercise, most of the students had poor to average fitness levels. Most of the students also had poor to fair grip strength.19
Measurement of grip strength may provide the opportunity for intervention needed to improve performance and prevent future OTJ injuries8,26 As grip strength is correlated with overall body strength and specifically upper extremity, grip strength measurement can serve as a needs assessment as well as efficacy of intervention.26 Recent determination of normative reference values of hand-grip strength among healthy individuals (ages 21–80 year-old men and women) in India may aid in interpreting grip-strength values for nursing students and staff, serving as a basis for comparison.27,28 The aim of the current study was to measure grip strength along with correlates, to inform recommendations to protect students entering the nursing workforce and increase career longevity, as well as health, among nurses already working.
Materials and Methods
Research Design
We conducted this study using a cross-sectional survey design with anthropometric measures and convenience sampling.
Setting and Sample
At a large teaching hospital and university, staff nurses and nursing students were invited to participate. Data collection stations were set up on site and staff/students present were recruited using convenience sampling technique and participants self-selected to participate. Convenience sampling is efficient and effective in settings with participants readily available,29 such as in a school or hospital. Inclusion criteria were being a staff nurse (performing bedside patient care), faculty with dual appointment (College of Nursing and clinical post), or enrolled as a nursing student. Exclusion criteria consisted of being physically unable to perform the grip strength test (eg due to existing hand injury, anomaly, or recent hand/wrist surgery). Participants immediately completed a short survey and anthropometric measures. The data collection period lasted June 29 through July 5, 2022. A priori sample size calculation was based on pilot data, where the proportion of nurses meeting Indian grip strength norms was 35.1%. Using the formula 4PQ/d2 keeping the precision at 6, the calculation is 35.1×64.9 x 4/36 = 253.
Data Collection
Using a paper survey, responses to sociodemographic questions and validated scales were collected and measurements documented on the same form. No identifiable information was collected and because anthropometric measures were documented on the participants’ surveys, no mechanism to link data was required. Sociodemographic questions included age, gender, indication of staff or student role, work hours, length on the job, and self-reported leisure and physical activity. Validated scales included the Perceived Stress Scale 4-item version (PSS-4), and the Nordic Musculoskeletal Questionnaire (NMQ).
Leisure activity was assessed by self-report with a dichotomous (yes/no) question regarding a regular practice of meditation/relaxation, and if yes, followed by an open-ended question regarding the type of meditation/relaxation activities practiced, and how many times per week. Physical activity was assessed with questions regarding the typical number of days per week exercise was performed, length of time spent exercising per week, type of exercise (eg cardio, stretching), and self-rated exercise intensity (low, medium, high).
The PSS-4 has been used in many settings, including India, and measures the degree to which one perceived one’s life situations as stressful in the last month. Responses range from 0 = never to 4 = very often. Items are summed, with higher scores indicating higher levels of perceived stress.30–32 The PSS-4 had an acceptable level of internal consistency in the current study (Cronbach’s alpha = 0.74).
The NMQ is used to evaluate location and severity of self-rated musculoskeletal symptoms during the past week to 12 months. Items are summed, with higher scores indicating greater musculoskeletal symptoms. NMQ items ask about problems in the neck, shoulders, elbows, wrists/hands, upper and lower back, hips/thighs, knees, and ankles/feet; the effect of problems on leisure and work activities; and whether or not healthcare was sought.33 The NMQ has been shown test-retest reliability and validity when compared to clinical history,34 has previously been used and found reliable in India,35 and is commonly used among nurses.36–38
Anthropometric measures included height, weight, waist circumference, using the same stadiometer, digital scale, and tape measure for all participants. Waist circumference of 85cm for men and 80cm for women, and a BMI of 23 kg/m2 were used as the normal cutoff values for Asian Indian Adults.39 Dominant hand grip strength was measured three times and averaged for each participant, using a Jamar digital dynamometer. A standard protocol was followed for grip strength measurement, which included having participants seated in a chair without armrests, dynamometer held in the dominant hand, with the elbow flexed at a right angle, forearm rotation 0° with the wrist in a neutral position.40
Statistical Analysis
Data analysis was completed using IBM SPSS Statistics version 27. Descriptive analyses were conducted using frequencies for nominal variables (student or staff status, gender, exercise intensity, routine practice of meditation/relaxation, orthopedic problem reported) or mean and standard deviation for continuous variables (hours worked per week, number of years working, age, BMI, waist circumference, hours of exercise per week, frequency of meditation/relaxation practice, perceived stress scale, total number of musculoskeletal symptoms, and grip strength), followed by Chi square or t-tests respectively to determine statistically significant differences between subgroups (students vs staff). Grip strength data was compared to Indian normative reference ranges and were separated into below vs meeting or exceeding normative values for age groups with published reference values. (For younger aged participants averages are reported, establishing a baseline, as the published reference values are for ages 21 years and older.) Pearson’s correlations indicating significant bi-variable associations between the continuous independent variables and grip strength (outcome variable) informed model building for multivariate analysis.
Ethical Considerations
The Institutional Review Boards of both institutions, Christian Medical College-Vellore, and Loma Linda University, of the respective affiliated authors approved the study, and it was conducted in accordance with the Declaration of Helsinki. Recruited individuals were provided with study information and all questions answered. Consent was obtained from study participants prior to data collection. After completion of the survey participants approached research team members for anthropometric measurements, including grip strength measurement, of their own accord.
Results
The total sample (N = 312) consisted of 148 students (47.4%) and 164 staff (52.6%). Both groups were primarily composed of female participants, (96.6% and 95.7% respectively). The participants ranged in age from 18 to 59 years (M = 23.61, SD = 5.77). Overall, the average BMI was below 23 with a range of 14.2 to 38.8. Waist circumference averaged < 80 cm, with a range of 58.0 to 117.0 cm. While only 127 participants (40.7%) reported regular exercise, these participants averaged over three hours of exercise per week with 45 (35.4%) reporting low-intensity, 80 (63%) medium-intensity, and 2 (1.6%) high-intensity. Only 70 (22.4%) reported practicing meditation or relaxation during leisure time, and those who did reported doing so an average of 4.58 (SD = 2.70) times per week. There were significant differences between students and staff in terms of age, waist circumference, and total number of musculoskeletal symptoms reported, which were all higher among staff nurses (see Table 1). Of note, mean grip strength did not significantly differ between students and staff.
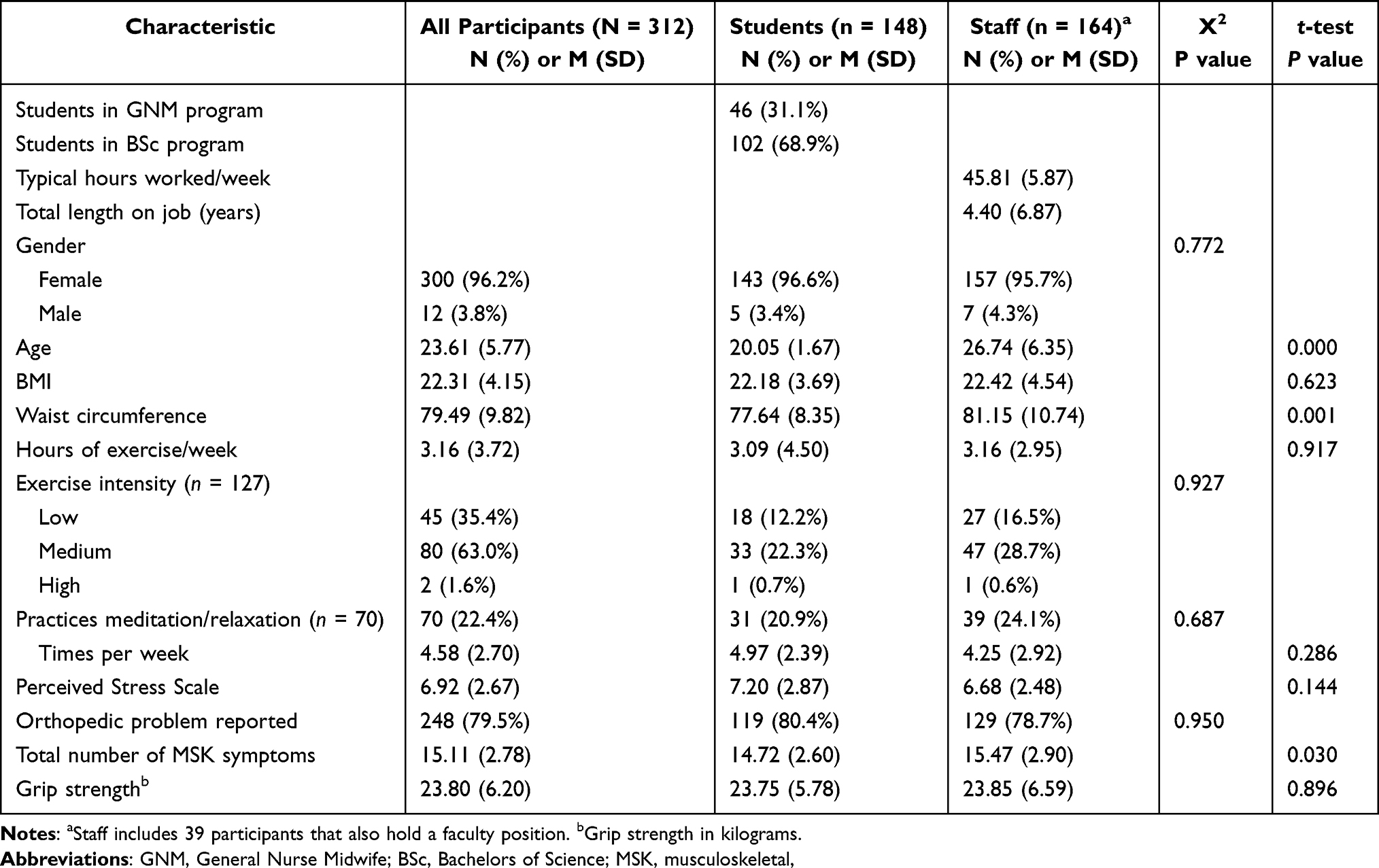 |
Table 1 Characteristics of Participants |
The mean grip strength for male participants 18–20 years of age was 36.68 kg (SD = 6.33), with a range of 27.81 to 45.45 kg. The mean grip strength for female participants 18–20 years of age was 23.11 kg (SD = 5.62), with a range of 6.76 to 38.15 kg.
Grip strength data for participants over the age of 21 were divided as below vs meeting or exceeding normative reference by age group and gender,27 with those in the latter group designated as having normal grip strength. In total, only 71 (22.5%) of the participants were found to have normal grip strength. On average, the few male participants (3.8% of total sample) exceeded normative values by age group, whereas female participants, on average, were below normative values in every age group (see Table 2).
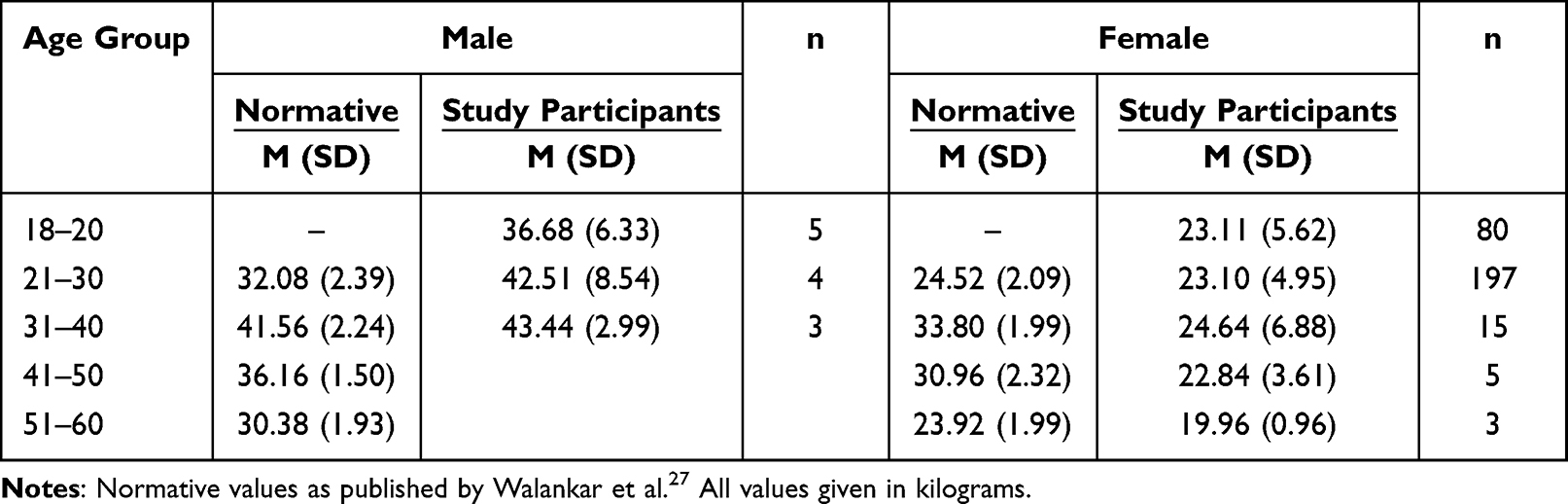 |
Table 2 Normative Hand Grip Strength for Healthy Adults in India and Grip Strength of Study Participants |
Correlations
While mean grip strength did not significantly differ between staff and students, these groups were statistically different in terms of age, waist circumference, and total number of musculoskeletal symptoms reported, therefore, we conducted Pearson’s correlations on these variables to see if they needed to be controlled for in multivariate analysis. Age was significantly positively correlated with waist circumference (r = 0.278, p < 0.001). However, age was not significantly associated with the number of musculoskeletal symptoms (r = −0.048, p < 0.395).
Grip strength was significantly positively associated with BMI (r = 0.266, p < 0.001) and waist circumference (r = 0.274, p < 0.001) using Pearson’s correlations. Age, relaxation/mediation habits, exercise habits, length of time on the job, average number of hours worked per week, perceived stress, and musculoskeletal symptoms were not significantly associated with grip strength (see Table 3).
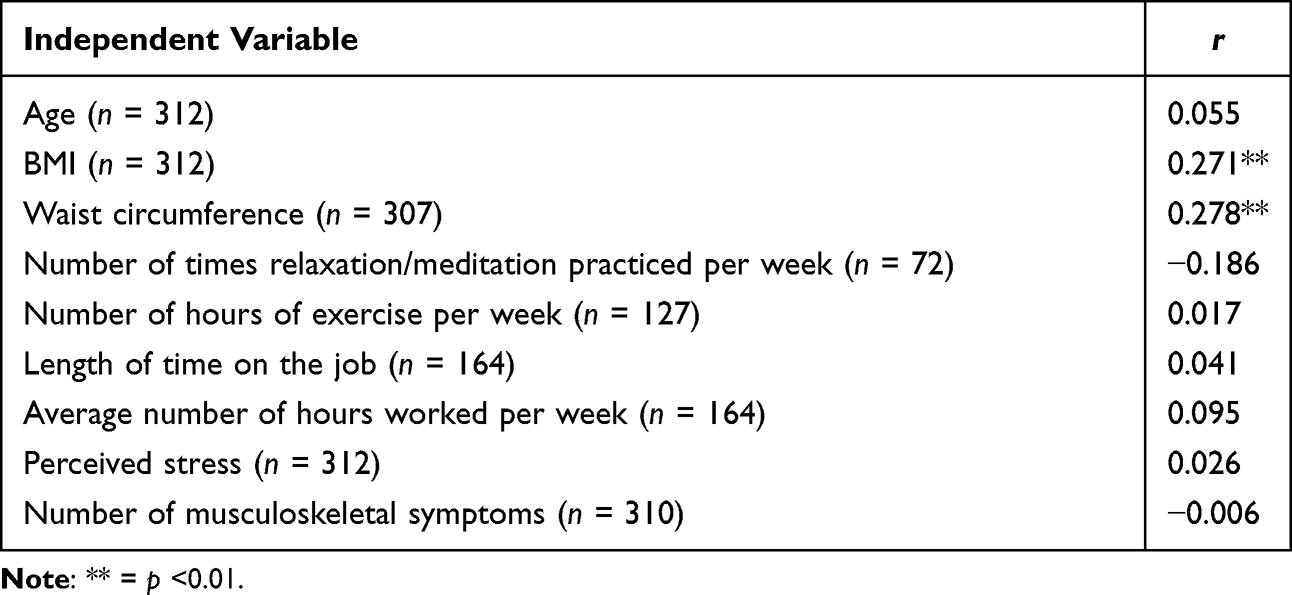 |
Table 3 Bivariate Correlations of Independent Variables with Grip Strength, (2-Tailed) |
Analysis of Predictors of Grip Strength
Initial multiple linear regression analysis included control variables (age, number of musculoskeletal symptoms) and significant bivariates of grip strength (BMI and waist circumference). The control variables were not significant in the model, therefore, only BMI and waist circumference (significant correlates of grip strength) were included in the final model, which explained 76% of the variance in grip strength. Only waist circumference remained significant in the model; as waist circumference increased, grip strength increased. See Table 4 for details.
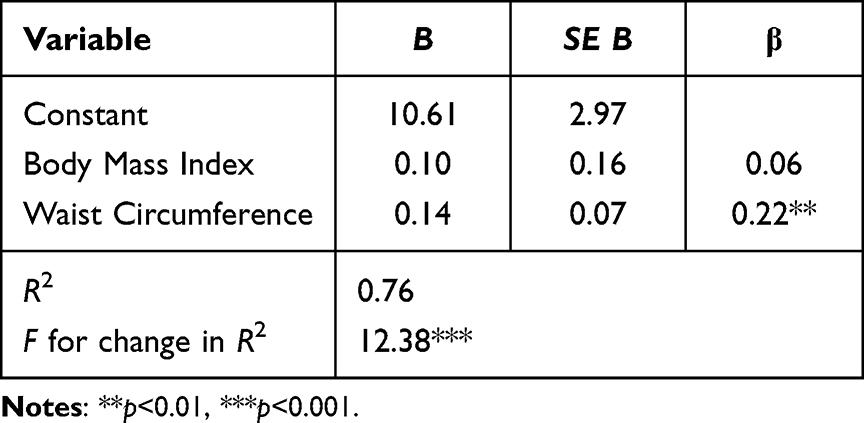 |
Table 4 Summary of Regression Analyses for Variables Predicting Grip Strength |
Discussion
In this study, we measured grip strength among working staff nurses and nursing students at a large teaching hospital and college of nursing in South India. Typical of the nursing profession, the sample was predominantly female participants, within the age range of the nursing workforce in India41 (ages 18–59 years).
Less than half of the participants reported engaging in a regular exercise routine, and those who did exercise routinely reported low to medium intensity for an average of three hours per week. Less than a quarter of the participants reported regular meditation or relaxation during leisure time. This pattern of physical activity/inactivity and leisure activity/inactivity is not inconsistent with findings from a recent systematic review among South-Asian adults.42 Of note, in the current study, grip strength was not significantly associated with exercise habits or meditation/relaxation habits, however, low participation in these activities may have contributed to less than a quarter of the participants meeting or exceeding normative grip strength.8,9,18 This study adds to the literature, providing data for healthy male and female participants 18–20 years of age. Participants over 21 years of age were compared with normative data published by Walankar et al in 201627 for a healthy Indian population, and less than a quarter of the participants were found to meet the normative values for their corresponding age and gender. On average, the small number of male participants in the 21–30 and 31–40 age groups exceeded the normative values. However, female participants were, on average, below the normative values in every age group. Grip strength is expected to be greater for males compared to females,14,27 but the disparity in the percentage of male and female participants meeting or exceeding normative values is troubling. The gender difference in meeting respective normative values may reflect differences in early growth and nutrition.14 While it is important to adjust normative values for grip strength to body size,43 it is dismaying that the female participants in this study did not meet the normative grip values of their peers (healthy Indian women).27 Little variation in physical size among Indian ethnic groups would be expected.44 Therefore, we may presume our participants have similar body size and composition to Walankar et al’s sample of healthy Indian subjects, though BMI and waist circumference were not discussed. Nonetheless, male grip strength is greater than female grip strength, among our participants and the published normative grip strength values,27 therefore, given the looming shortage of over one million nurses in India,20 and the physically demanding nature of nursing,1–4 it may behoove the Indian Nursing Council and educational institutions to consider policies that would encourage greater entry and participation of males in the nursing profession.
In the current study, mean grip strength did not significantly differ between working staff nurses and nursing students. This result is seemingly in contrast to literature suggesting that hours worked, years in profession, consecutive/rotating shifts, and the stress and physical demand of clinical work negatively influenced grip strength.8,9,18 BMI and waist circumference were positively associated with grip strength, and explained 76% of the variance in grip strength. However, only waist circumference remained a significant predictor of grip strength in the regression model. Similarly, a previous study among 1005 healthy Indian adults found only a weak correlation between grip strength and BMI.28
On average, our participants had a BMI below 23, meeting the criteria for normal weight according to the revised consensus guidelines for Asian Indians, which categorizes overweight as a BMI of 23.0 to 24.9, and a BMI of ≥ 25.0 as obesity.45 Participant’s waist circumference on average was less than 80 cm. However, there were significant differences between staff and students on age, as with greater age (staff), BMI was slightly higher and waist circumference was significantly greater, indicating a trend toward central obesity. The low BMI among students, along with a significantly smaller waist circumference, again may reflect early growth and nutrition,14 while the increased girth of staff may reflect more availability of nutritious food as they are now earning an income,46 and improved nutrition would also align with the positive association noted between waist circumference and grip strength.
Several strengths and limitations should be considered in understanding the results of the current study. The participants were not a nationally representative sample of Indian nurses and nursing students. While the sample size was small, it exceeded the a priori minimum sample required for analyses. Participants were recruited from one institution, as a convenience sample, in a medium-sized city in South India, and may not have been representative of nurses everywhere in India. The small number of participants 18–20 years old limits the generalizability of average grip strength as normative parameters, but nevertheless adds to the literature for this age group. The small number of male participants compared to female participants was representative of the institution where data were collected and of the nursing profession in general, but again, may not be representative of the entire Indian nursing workforce. Nonetheless, participants were from both rural and urban backgrounds, and included a varied ethnic composition because students hailing from across India study at this particular institution of national renowned. Self-report bias or inconsistencies may have obscured variations in exercise and relaxation activities, stress, and musculoskeletal symptoms, introducing the potential for a confounding influence on grip strength that was not detected. All grip strength measurements were taken using a Jamar hand dynamometer, which is a valid and reliable tool for measuring grip strength.47 One dynamometer was used for all measurements, using a standard protocol, and all measurements were taken by the same member of the research team, thus increasing reliability.
Despite these limitations, with so few participants (< 25%) meeting or exceeding Indian normative grip strength parameters, the need for interventional response is demonstrated. Interventions could include strategies to increase awareness, ergonomic training, exercise programs designed to increase nurses’ overall strength and fitness, as well as other safety measures such as implementing a patient lift team or equipment, which have been effective in efforts to prevent and limit nurse injuries, improve occupational health and reduce organizational costs resulting from injuries.22–24,38,48 Given the critical shortage of nurses globally, and in India, the need for intervention is compelling. We need to protect students entering the nursing workforce, and increase the career longevity, as well as health, of nurses already working.
Conclusion
This study presents the first measurement of grip strength among nursing staff and students in India, to the best of our knowledge, and adds to the literature by reporting grip strength for healthy Indian males and females 18 to 20 years of age. The average hand grip strength measurements for female nursing staff and students age 21–59 years were lower than the published Indian normative values by age. The importance of this baseline measurement is the demonstrated need for strengthening among female nurses, which are the vast majority in nursing. Variance in grip strength was largely explained by waist circumference, pointing to the importance of nutrition. Understanding the need provides an opportunity to develop informed interventions to improve physical performance of nursing duties and prevent future OTJ injuries. Preserving career longevity and attracting more males to the profession are essential strategies to help mitigate the anticipated critical shortage of nurses in India.
Acknowledgments
The authors thank the nursing department supervisors, and College of Nursing deans and faculty who facilitated the participation of staff nurses and nursing students.
Funding
Loma Linda University intramural funding, grant # 239401-1000707.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lee SJ, Lee JH, Gershon RR. Musculoskeletal symptoms in nurses in the early implementation phase of California’s safe patient handling legislation. Res Nurs Health. 2015;38(3):183–193. doi:10.1002/nur.21657
2. Younan L, Clinton M, Fares S, Jardali FE, Samaha H. The relationship between work‐related musculoskeletal disorders, chronic occupational fatigue, and work organization: a multi‐hospital cross‐sectional study. J Adv Nurs. 2019;1–11. doi:10.1111/jan.13952
3. Thinkhamrop W, Sawaengdee K, Tangcharoensathien V, et al. Burden of musculoskeletal disorders among registered nurses: evidence from the Thai nurse cohort study. BMC Nurs. 2017;16(1):68. doi:10.1186/s12912-017-0263-x
4. Richardson A, McNoe B, Derrett S, Harcombe H. Interventions to prevent and reduce the impact of musculoskeletal injuries among nurses: a systematic review. Int J Nurs Stud. 2018;8(1):87–109.
5. De La Motte SJ, Gribbin TC, Lisman P, Murphy K, Deuster PA. Systematic Review of the Association Between Physical Fitness and Musculoskeletal Injury Risk: part 2-Muscular Endurance and Muscular Strength. J Strength Conditioning Res. 2017;31(11):3218–3234. doi:10.1519/JSC.0000000000002174
6. Thompson BJ. Does work-induced fatigue accumulate across three compressed 12 hour shifts in hospital nurses and aides? Article. PLoS One. 2019;14(2):1–15. doi:10.1371/journal.pone.0211715
7. Thompson BJ, Stock MS, Banuelas VK. Effects of accumulating work shifts on performance-based fatigue using multiple strength measurements in day and night shift nurses and aides. Hum Factors. 2017;59(3):346–356. doi:10.1177/0018720816677814
8. Merchaoui I, Bouzgarrou L, Mnasri A, et al. Influence of shift work on the physical work capacity of Tunisian nurses: a cross-sectional study in two university hospitals. Pan African Medical Journal. 2017;26(1):1–10. doi:10.11604/pamj.2017.26.1.9891
9. Merchaoui I, Bouzgarrou L, Amri C, et al. Determinants of Grip Strength in Tunisian Nurses: a Bicentric Study. Recent Pat Inflamm Allergy Drug Discov. 2016;10(1):54–60. doi:10.2174/1872213X10666160607125547
10. Hahn P, Spies C, Unglaub F, Muhldorfer-Fodor M. Grip strength measurement: significance and boundaries. Orthopade. 2018;47(3):191–197. doi:10.1007/s00132-017-3487-2
11. Carney C, Benzeval M. Social patterning in grip strength and in its association with age; a cross sectional analysis using the UK Household Longitudinal Study (UKHLS). BMC Public Health. 2018;18(1):385. doi:10.1186/s12889-018-5316-x
12. Wang YC, Bohannon RW, Li X, Sindhu B, Kapellusch J. Hand-Grip Strength: normative Reference Values and Equations for Individuals 18 to 85 Years of Age Residing in the United States. J Orthop Sports Phys Ther. 2018;48(9):685–693. doi:10.2519/jospt.2018.7851
13. Leong DP, Teo KK, Rangarajan S, et al. Prognostic value of grip strength: findings from the Prospective Urban Rural Epidemiology (PURE) study. Lancet. 2015;386(9990):266–273. doi:10.1016/S0140-6736(14)62000-6
14. Dodds RM, Syddall HE, Cooper R, Kuh D, Cooper C, Sayer AA. Global variation in grip strength: a systematic review and meta-analysis of normative data. Age Ageing. 2016;45(2):209–216. doi:10.1093/ageing/afv192
15. Darsini D, Hamidah H, Notobroto HB, Cahyono EA. Health risks associated with high waist circumference: a systematic review. J Public Health Res. 2020;9(2):56.
16. Merchant RA, Chan YH, Lim JY, Morley JE. Prevalence of metabolic syndrome and association with grip strength in older adults: findings from the HOPE study. Diabetes Metab Syndrome Obesity. 2020;2677–2686. doi:10.2147/DMSO.S260544
17. Lockie RG, Ruvalcaba TR, Stierli M, Dulla JM, Dawes JJ, Orr RM. Waist circumference and waist-to-Hip ratio in law enforcement agency recruits: relationship to performance in physical fitness tests. J Strength Conditioning Res. 2020;34(6):1666–1675. doi:10.1519/JSC.0000000000002825
18. Sakzewski L, Naser-ud-Din S. Work-related musculoskeletal disorders in Australian dentists and orthodontists: risk assessment and prevention. Work. 2015;52(3):559–579. doi:10.3233/WOR-152122
19. Pugh JD, Cormack K, Gelder L, Williams AM, Twigg DE, Blazevich AJ. Exercise, fitness and musculoskeletal health of undergraduate nursing students: a cross‐sectional study. J Adv Nurs. 2019;75(10):2110–2121. doi:10.1111/jan.13990
20. Singh L. Prevalence of MSDs among nurses: a study in Indian health care industry. Ergon Int J. 2018;2(3):5965.
21. Anap DB, Iyer C, Rao K. Work related musculoskeletal disorders among hospital nurses in rural Maharashtra, India: a multi centre survey. Int J Res Med Sci. 2013;1(2):101–107. doi:10.5455/2320-6012.ijrms20130513
22. Paul A. A Pilot Study on Awareness of Ergonomics and Prevalence of Musculoskeletal Injuries among Nursing Professionals. Int J Nursing Educ. 2012;4(1):4.
23. Yasobant S, Rajkumar P. Health of the healthcare professionals: a risk assessment study on work-related musculoskeletal disorders in a tertiary hospital, Chennai, India. Int J Med Public Health. 2015;5(2):189–195. doi:10.4103/2230-8598.153836
24. Koshy N, Sriraman S, Kamat YD. Patient handling in India—Evidence from a pilot study. J Family Med Primary Care. 2020;9(3):1397–1402. doi:10.4103/jfmpc.jfmpc_1173_19
25. World Health Organization. Global strategy on human resources for health: workforce 2030. WHO. 2016;61.
26. Richards L, Palmiter-Thomas P. A Critical Review of Tools, Methods, and Clinical Utility for Grip Strength Measurement. Critical Rev Phys Rehabilitation Med. 1996;29(1–4):87–109. doi:10.1615/CritRevPhysRehabilMed.v8.i1-2.50
27. Walankar P, Verma C, Mehta A. Study of hand grip strength in Indian population. Int J Health Sci Res. 2016;6(11):162–166.
28. Mullerpatan RP, Karnik G, John R. Grip and pinch strength: normative data for healthy Indian adults. Hand Therapy. 2013;18(1):11–16. doi:10.1177/1758998313479874
29. Simkus J Convenience sampling: definition, method and examples. Simply Psychology; 2023. https://www.simplypsychology.org/convenience-sampling.html.
30. Cohen S, Kamarck T, Mermelstein R. Perceived Stress Scale. Measuring Stress: A Guide for Health and Social Scientists. New York: Oxford University Press; 1994.
31. Warttig SL, Forshaw MJ, South J, White AK. New, normative, English-sample data for the short form perceived stress scale (PSS-4). J Health Psychol. 2013;18(12):1617–1628. doi:10.1177/1359105313508346
32. Pangtey R, Basu S, Meena GS, Banerjee B. Perceived stress and its epidemiological and behavioral correlates in an Urban Area of Delhi, India: a community-based cross-sectional study. Indian J Psychol Med. 2020;42(1):80–86. doi:10.4103/IJPSYM.IJPSYM_528_18
33. Crawford JO. The Nordic musculoskeletal questionnaire. Occup Med (Chic Ill). 2007;57(4):300–301. doi:10.1093/occmed/kqm036
34. Kuorinka I, Jonsson B, Kilbom A, et al. Standardised Nordic questionnaires for the analysis of musculoskeletal symptoms. Appl Ergon. 1987;18(3):233–237. doi:10.1016/0003-6870(87)90010-X
35. Gupta G, Bhavana R, Rishikesh R. Reliability and validity of Hindi version of Nordic musculoskeletal questionnaire. EC Orthop. 2018;9(8):533–538.
36. Fang Y, Li S, Zhang Y, Zhang P, Wu H, Wang D. Test-retest reliability of Nordic Musculoskeletal Questionnaire in nurses. Zhonghua Lao dong wei sheng zhi ye bing za zhi= Zhonghua laodong weisheng zhiyebing zazhi=. Chine j Industrial Hygiene Occupational Dis. 2013;31(10):753–758.
37. Amin NA, Nordin RB, Noah R, Oxley J, Fatt QK. Work related musculoskeletal disorders in female nursing personnel: prevalence and impact. Int J Collaborative Res Internal Med Public Health. 2016;8(3):294–315.
38. Trinkoff AM, Brady B, Nielsen K. Workplace prevention and musculoskeletal injuries in nurses. JONA. 2003;33(3):153–158. doi:10.1097/00005110-200303000-00006
39. Snehalatha C, Viswanathan V, Ramachandran A. Cutoff values for normal anthropometric variables in Asian Indian adults. Diabetes Care. 2003;26(5):1380–1384. doi:10.2337/diacare.26.5.1380
40. Singh AK, Meena ML, Chaudhary H, Dangayach GS. A comparative assessment of static muscular strength among female operative’s working in different handicraft occupations in India. Health Care Women Int. 2019;40(4):459–478. doi:10.1080/07399332.2018.1484468
41. Karan A, Negandhi H, Hussain S, et al. Size, composition and distribution of health workforce in India: why, and where to invest? Hum Resour Health. 2021;19(1):1–14. doi:10.1186/s12960-021-00575-2
42. Ranasinghe CD, Ranasinghe P, Jayawardena R, Misra A. Physical activity patterns among South-Asian adults: a systematic review. Int J Beha Nutrition Phys Activity. 2013;10:1–11. doi:10.1186/1479-5868-10-116
43. Abdalla PP, Bohn L, Dos Santos AP, et al. Adjusting Grip Strength to Body Size: analyses From 6 Countries. J Am Med Dir Assoc. 2022;23:
44. Lam NW, Goh HT, Kamaruzzaman SB, Chin A-V, Poi PJH, Tan MP. Normative data for hand grip strength and key pinch strength, stratified by age and gender for a multiethnic Asian population. Singapore Med J. 2016;57(10):578–584. doi:10.11622/smedj.2015164
45. Aziz N, Kallur SD, Nirmalan PK. Implications of the revised consensus body mass indices for Asian Indians on clinical obstetric practice. J Clin Diagnostic Res. 2014;8(5):1–3. doi:10.7860/JCDR/2014/8062.4212
46. Mayen A-L, Marques-Vidal P, Paccaud F, Bovet P, Stringhini S. Socioeconomic determinants of dietary patterns in low-and middle-income countries: a systematic review. Am J Clin Nutr. 2014;100(6):1520–1531. doi:10.3945/ajcn.114.089029
47. Peolsson A. Intra- and intertester reliability and reference values for hand strength. J Rehabil Med. 2001;33:36–41. doi:10.1080/165019701300006524
48. Rogers B, Buckheit K, Ostendorf J. Ergonomics and nursing in hospital environments. Workplace Health Saf. 2013;61(10):429–439. doi:10.1177/216507991306101003
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.