")
Back to Journals » Journal of Blood Medicine » Volume 15
HIF2-α Expression in CML Patients Receiving Hydroxyurea Prior to Imatinib That Achieved Major Molecular Response (MMR) versus in Those Not Achieving MMR
Authors Rinaldi I , Mauludi R, Jusman SW, Sinto R, Harimurti K
Received 18 August 2023
Accepted for publication 18 January 2024
Published 13 February 2024 Volume 2024:15 Pages 61—67
DOI https://doi.org/10.2147/JBM.S436015
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Martin H Bluth
Ikhwan Rinaldi,1,2 Radinal Mauludi,2 Sri Widia Jusman,3 Robert Sinto,4 Kuntjoro Harimurti5,6
1Division of Hematology and Medical Oncology, Department of Internal Medicine, Cipto Mangunkusumo National General Hospital, Faculty of Medicine, Universitas Indonesia, Jakarta, Indonesia; 2Department of Internal Medicine, Cipto Mangunkusumo National General Hospital, Faculty of Medicine, Universitas Indonesia, Jakarta, Indonesia; 3Department of Biochemistry and Molecular Biology, Faculty of Medicine, Universitas Indonesia, Jakarta, Indonesia; 4Division of Tropical and Infectious Diseases, Department of Internal Medicine, Cipto Mangunkusumo National General hospital, Faculty of Medicine, Universitas Indonesia, Jakarta, Indonesia; 5Clinical Epidemiology Unit, Department of Internal Medicine, Faculty of Medicine Universitas Indonesia - Cipto Mangunkusumo National General Hospital, Jakarta, Indonesia; 6Division of Geriatrics, Department of Internal Medicine, Cipto Mangunkusumo National General Hospital, Faculty of Medicine, Universitas Indonesia, Jakarta, Indonesia
Correspondence: Ikhwan Rinaldi, Email [email protected]
Introduction: Currently, Imatinib (IM) which is a Tyrosine Kinase Inhibitor (TKI), is the main treatment for patients with chronic myeloid leukemia (CML). Major molecular response (MMR) is used as therapeutic response. Resistance to IM may be caused by hypoxia which is regulated by hypoxia inducible factor (HIF) 2-α. The role of HIF2-α is currently not researched extensively. This study aimed to analyse the differences in HIF-2α expression between chronic phase CML patients that achieved MMR and those that did not achieve MMR.
Methods: This study used a cross-sectional method which analysed secondary data from whole blood samples in chronic phase CML patients aged 18– 60 years that received hydroxyurea (HU) before IM, aged 18– 60 years, received IM therapy for more than 12 months, and were willing to participate in the study. The exclusion criteria for this study were patients who were receiving IM at a dose of more than 400 mg/day. HIF-2α protein expression was examined using the enzyme-linked immunosorbent assay (ELISA) method. Differences between HIF-2α protein expression in groups that achieved MMR versus not achieving MMR was analysed using the Mann–Whitney test.
Results: A total of 79 subjects were obtained. The median HIF-2α was 90.56 pg/mg protein (3.01– 4628.74). There was no statistically significant difference in expression of HIF-2α in the group that reached MMR and did not reach MMR, namely 123.45 pg/mg protein and 89.25 pg/mg protein respectively (p 0.718).
Conclusion: This study found no statistically significant difference between HIF-2α expression level and MMR achievement of chronic phase CML patients who received HU before IM therapy.
Keywords: CML, leukemia, imatinib, resistance, chronic myeloid leukemia, IM
Introduction
Chronic myeloid leukemia (CML) is a myeloproliferative disorder characterized by the excessive proliferation of myeloid cells at various stages of differentiation.1 The disorder is characterized by a specific genetic alteration, a reciprocal translocation of chromosomes 9 and 22, which results in the formation of the Philadelphia chromosome.1 This translocation leads to the fusion of the Breakpoint Cluster Region-Abelson murine Leukemia (BCR-ABL) gene, which plays a crucial role in the development and progression of CML.1
The effectiveness of CML therapy is evaluated by determining the level of therapeutic response, which is measured by major molecular response (MMR).1,2 Other measurement of therapeutic response include complete hematologic response and complete cytogenetic response.3 However, MMR is proven to be superior as outcome measurement, especially for predicting long-term relapse.4
Failure to achieve a therapeutic response can be caused by resistance to therapy.2 The mechanisms of resistance can be either BCR-ABL dependent, caused by genetic mutations in the BCR-ABL gene itself, or BCR-ABL independent, which can be caused by various factors, including increased production of reactive oxygen species (ROS).5–7 ROS play a significant role in maintaining genome integrity as they can damage DNA through direct or indirect processes. Research has also shown that ROS formation can occur as a result of hydroxyurea (HU) treatment before imatinib (IM) therapy.6,7
Hypoxia-inducible factor (HIF) plays a role in regulating oxygen homeostasis and is involved in the pathogenesis of various diseases, including leukemia. There are three isoforms of HIF protein: HIF-1α, HIF-2α, and HIF-3α.8–10 HIF-1α is the most widely studied and is expressed in nearly all cell types. HIF-2α is expressed in a limited number of cell types, such as vascular endothelial cells, type 2 pneumocytes, renal interstitial cells, liver parenchyma, and myeloid cells. HIF-3α is currently less well-researched compared to the other isoforms.8,11
Increased expression of HIF has been reported in a majority of cases of acute myeloid leukemia (AML), acute lymphoblastic leukemia (ALL), and CML.12 In an in vitro study of HIF-2α expression in AML cases, it was found that there was an increase in HIF-2α protein expression which was associated with accelerated disease progression and poor response to therapy.13 HIF-2α acts as a transcription factor and plays a role in cell proliferation. If the expression of HIF-2α increases, it is believed that the proliferation of CML cells will also increase.14
There are currently no studies that specifically examine the relationship between HIF-2α expression and treatment response in chronic phase CML. Therefore, this study aims to investigate the association between HIF-2α expression and response to therapy, as measured by an MMR in CML patients.
Method
This study was a cross-sectional study with a total sample of 118 blood samples (leukocyte protein isolates) saved from previous research subjects with the research title “Longer Hydroxyurea Administration Prior to Imatinib Mesylate is Risk Factor for Unsuccessful Major Molecular Response in Chronic-Phase Chronic Myeloid Leukemia: Possibility of P-Glycoprotein Role”.15
This study recruited samples from chronic phase CML patients who received HU before IM at Hematology and Medical Oncology polyclinic at Cipto Mangunkusumo National General Hospital from January 2015 to June 2016. Procedures of BCR-ABL/ABL ratio is described and measured in previous studies.14 Examination of HIF-2α expression was carried out by the enzyme-linked immunosorbent assay (ELISA) method.
In this study, MMR was measured after at least 12 months of IM therapy. Attainment of MMR was determined based on the most recent patient measurement, with a cutoff of BCR-ABL <0.1% defining MMR achievement.
Inclusion and Exclusion Criteria
The inclusion criteria for this study were chronic phase CML patients who received HU before IM aged 18–60 years, had received IM therapy for more than 12 months, and were willing to participate in the study. The exclusion criteria for this study were patients who were receiving IM at a dose of more than 400 mg/day.
Statistical Analysis
Data analysis was performed using the Statistical Package for the Social Sciences (SPSS) version 26 (IBM Corp., released 2019. IBM SPSS Statistics for Windows, version 20.0, Armonk, NY: IBM Corp.). Descriptive analysis of categorical data is presented as proportions (percentages). Continuous variables with a normal distribution are presented as means (average) with standard deviations (SD), while continuous variables with non-normal distribution are presented as medians and first and third quartile values except for HIF-2α and BCR-ABL ratio which use range. The Student’s t-test was used to compare continuous variables with normal distribution, while the Mann–Whitney test was used for continuous variables with non-normal distribution. Correlation test used Spearman correlation analysis.
Ethics
This study was ethically approved by the ethics committee of the Faculty of Medicine, University of Indonesia – Cipto Mangunkusumo Hospital with protocol number 2-0-8-0964. This study follows the guidelines from the Declaration of Helsinki. As this is a study using previously obtained blood samples from previous study, no informed consent was required based on evaluation by the ethics committee.
Result
From a total of 118 samples, 85 samples were found that met the inclusion criteria. Out of the 33 samples that were not eligible for inclusion, 2 were from patients in the accelerated phase, 10 were from patients over 60 years of age, 8 were from patients who had received IM therapy for less than 12 months, and 13 were from patients who had not been evaluated for an MMR. However, in total, only 79 samples were available for analysis, as the other 6 samples did not have sufficient blood volume for analysis.
The characteristics of the study subjects are shown in Table 1. The mean age of the CML patients in the study was 41.51 years. The median blast percentage of the patients in this study was 0% (0–1%), which is in accordance with definition of chronic phase CML from European Society of Medical Oncology.2
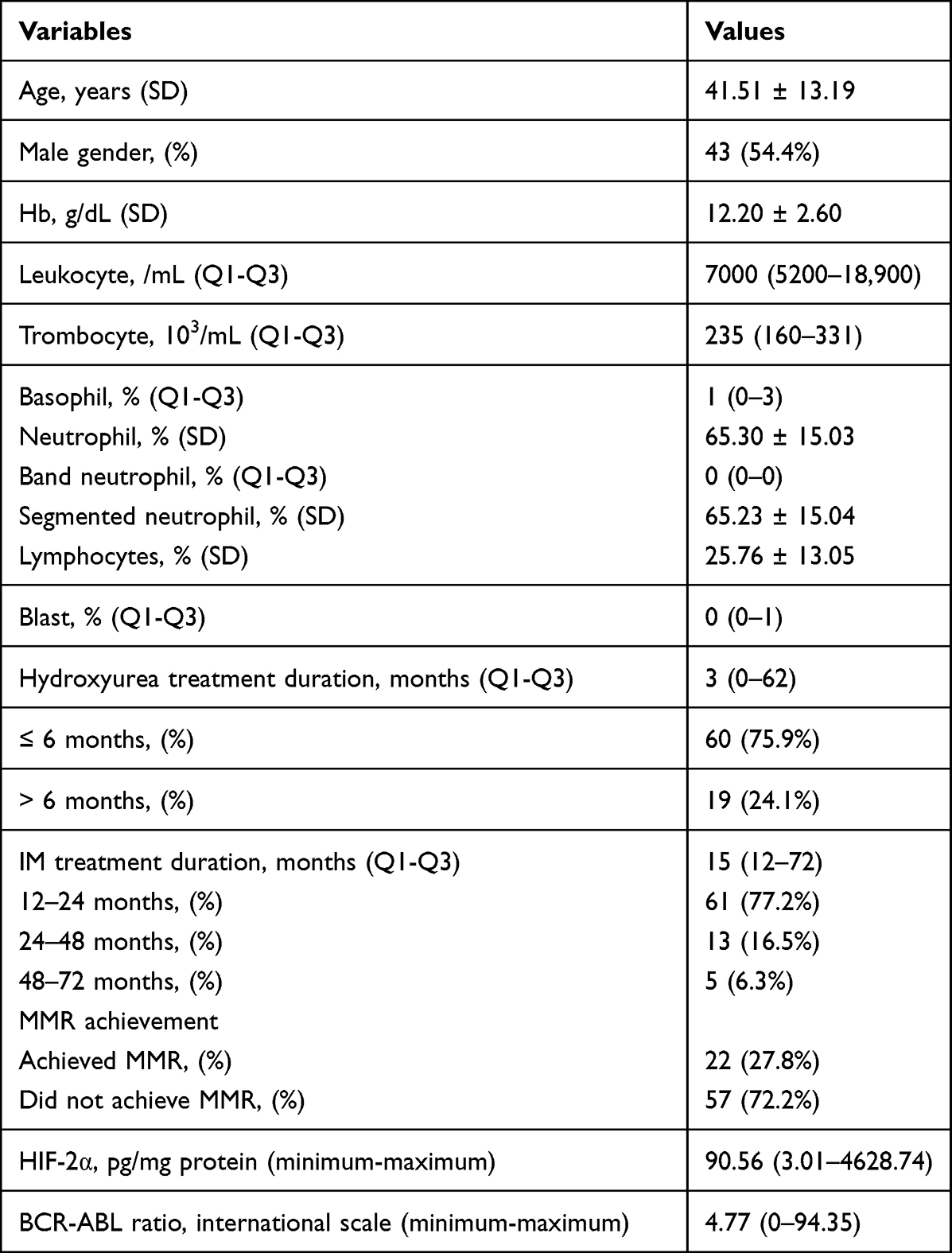 |
Table 1 Basic Characteristics of Research Subjects (N = 79) |
Of the total patients, 22 patients (27.8%) achieved an MMR. The median leukocyte count among our patients was 7000 mg/dL (5200–18,900). Median HIF-2α is 90.56 pg/mg protein (range: 3.01–4628.74) and the median BCR-ABL ratio was 4.77 (range: 0–94.35).
HIF-2 Alpha Expression and MMR Outcome
No statistically significant difference in median HIF-2α expression was observed based on the Mann–Whitney test between subjects who achieved MMR and those who did not (p-value: 0.718) (Figure 1). The median HIF-2α expression was 123.45 pg/mg protein (range: 3.01–4628.74 pg/mg protein) in subjects who achieved an MMR, while it was 89.25 pg/mg protein (range: 3.01–2755.7 pg/mg protein) in subjects who did not attain an MMR.
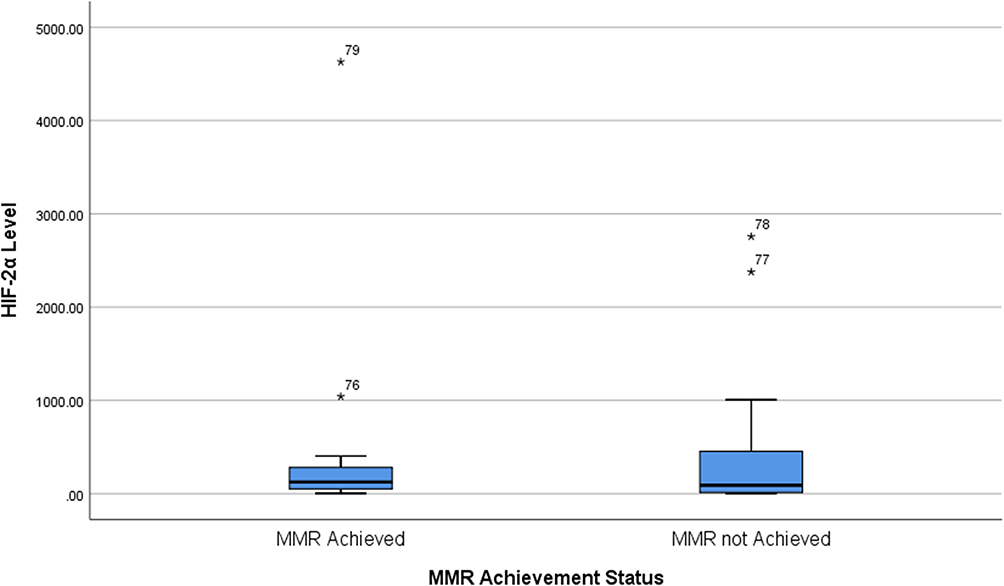 |
Figure 1 HIF-2α Level based on MMR status. |
Further analysis is conducted that exclude patients receiving HU <2 months. A total of 44 patients receiving HU ≥2 months is available for analysis. Mann–Whitney test also showed no statistically significant difference in HIF-2α between the 2 groups (p: 0.235).
Correlation Between HIF-2α and BCR-ABL Ratio
Correlation analysis between HIF-2α and BCR-ABL ratio was conducted using Spearman correlation test. The correlation test showed weak negative correlation between the 2 variables but this is not statistically significant (correlation coefficient: −0.165; p value: 0.146).
Discussion
The mean age of the study population was 41.51 years, with the youngest participant being 19 years old and the oldest being 60 years old.15,16 However, this mean age is lower when compared to the mean age of CML patients in Western countries, which tend to be higher. Research in the United States reported a median age of 66 years for CML patients. Studies in European countries such as France reported a median age of 56 years, while in Germany, it was reported as 57 years, in Sweden it was 60 years, and in the UK it was 59 years.17–21 This difference in age may be attributed to racial and environmental factors.
In a review article that collected data from various registries in several countries in Asia such as China, India, the Philippines, Hong Kong, Singapore, Taiwan, South Korea and Thailand, the median age range was 36–55 years.22 This was also in accordance with a study conducted by Mendizabal et al, who studied the relationship between geography and income and the age of patients when diagnosed with CML where the lowest median was in Asia and Africa, namely 47 years and the highest in the Oceania region, namely 72 years.23 Thus, there may be an interaction between geographic factors and age. From this study, other hypotheses that need to be considered such as genetic mutations triggered by environmental exposures also emerged.
All subjects in this study had received IM mesylate therapy for at least 12 months. The median leukocyte level in this study was below 10,000/mL, namely 7000 (5200–18,900)/mL, with 42.4% (n: 31) subjects having levels leukocytes above 10,000/mL. Only 11 subjects still had blasts and the number of blasts above 5% was only observed in 1 subject. The median basophils in this study were 0.00 (0.0–3.0) % with a percentage of basophils above 20% observed only in 1 subject with a basophil level of 47%.
Several studies have shown that hypoxia inducible factors (HIFs) may play a significant role in CML progression by promoting stem cell survival, angiogenesis, and resistance to therapy.24 A study by King Pan et al demonstrated that hypoxia-inducible factor 1 α (HIF1-α) is expressed in bone marrow of CML patients.25 Interestingly, the Authors also demonstrated that HIF1-α is only partially suppressed by IM therapy. Thus, the Authors recommend anti-BCR-ABL1 and anti-HIF1- α to eliminate CML stem cells. Furthermore, a study by Hen Chen et al showed lack of colony formation in cells with HIF-1α knockdown.14 In small cell lung cancer cells, IM may suppress angiogenesis.26
HIF-2α as a transcription factor increases the activity of the transcription factor c-Myc and the expression of cyclin D, both of which are required to maintain stem cells in an undifferentiated state.27 HIF-2α is known to cause AML leukemia cells to survive the apoptotic process induced by endoplasmic reticulum stress.28
A study conducted by Forristal et al, showed that there was an increase in HIF-2α expression in AML cells compared to normal cells, and this increase in expression was associated with increased proliferation of leukemia cells, accelerated disease progression, and increased resistance to apoptosis.13 Knockdown of HIF-2α in myeloid leukemia cell lines leads to decreased cell proliferation in vitro, slowing disease progression and prolonging survival.13
In this study, we did not find significant difference between HIF-2α expression level and MMR achievements in chronic phase CML patients. According to Deynoux et al there is conflicting data on the role of HIFs in leukemias.12 Indeed, it is still not determined whether HIFs are oncogenes or tumor suppressors.
It is possible that HIF-2α may have no role in MMR at all in chronic phase CML but in blast phase CML instead. As proliferation of CML cells in chronic phase is relatively lower than in blast phase CML, which resembles AML, HIF-2α expression may not be different between groups that achieved and not achieved MMR. As described above, HIF-2α expression increase was associated with proliferation in AML.13 It is also possible that IM treatment in both groups irrespective of MMR achievement may suppress HIF-2α expression and thus, causing no difference in HIF-2α levels. As a result, further studies are needed to elucidate the role of HIF2-α in CML and cancer in general. We also recommend further studies that assess HIF-2α expression in CML with blast phase and to compare HIF-2α expression between chronic phase and blast phase of CML. However, this may be difficult as patients with blast phase CML is very rare.
Study Limitations
Limitations of this study include variable months of measurement for MMR above 12 months and variable duration of HU treatment prior to IM.
Conclusion
This study found no statistically significant difference between HIF-2α expression and MMR in chronic phase CML patients who received HU before IM therapy. Further large-scale studies should be conducted to explore the role HIF-2 alpha in CML and leukemia.
Acknowledgment
The authors would like to thank Kevin Winston MD, MRes for his help in manuscript revision, data analysis, and proofreading.
Funding
This study received funding from “Direktorat Riset dan Pengembangan Universitas Indonesia (DRP UI)” in the year 2020 with grant number NKB-4709/UN2.RST/HKP.05.00/2020.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jabbour E, Kantarjian H. Chronic myeloid leukemia: 2020 update on diagnosis, therapy and monitoring. Am J Hematol. 2020;95(6):691–709. doi:10.1002/ajh.25792
2. Hochhaus A, Saussele S, Rosti G, et al. Chronic myeloid leukaemia: ESMO Clinical Practice Guidelines for diagnosis, treatment and follow-up†. Ann Oncol. 2017;28:iv41–iv51. doi:10.1093/annonc/mdx219
3. Cortes J, Quintás-Cardama A, Kantarjian HM. Monitoring molecular response in chronic myeloid leukemia. Cancer. 2011;117(6):1113–1122. doi:10.1002/cncr.25527
4. Galinsky I, Buchanan S. Guide to Interpreting disease responses in chronic myeloid leukemia. J Adv Pract Oncol. 2012;3(4):225–236. doi:10.6004/jadpro.2012.3.4.3
5. Alves R, Gonçalves AC, Rutella S, et al. Resistance to tyrosine kinase inhibitors in chronic myeloid leukemia-from molecular mechanisms to clinical relevance. Cancers. 2021;13(19):4820. doi:10.3390/cancers13194820
6. Antoszewska-Smith J, Pawlowska E, Blasiak J. Reactive oxygen species in BCR-ABL1-expressing cells - relevance to chronic myeloid leukemia. Acta Biochim Pol. 2017;64(1):1–10. doi:10.18388/abp.2016_1396
7. Głowacki S, Synowiec E, Szwed M, Toma M, Skorski T, Śliwiński T. Relationship between oxidative stress and imatinib resistance in model chronic myeloid leukemia cells. Biomolecules. 2021;11(4):610. doi:10.3390/biom11040610
8. Kumar H, Choi D-K. Hypoxia inducible factor pathway and physiological adaptation: a cell survival pathway? Mediators Inflamm. 2015;2015:584758. doi:10.1155/2015/584758
9. Gao Q, Ren Z, Jiao S, et al. HIF-3α-induced miR-630 expression promotes cancer hallmarks in cervical cancer cells by forming a positive feedback loop. J Immunol Res. 2022;2022:5262963. doi:10.1155/2022/5262963
10. Jun JC, Rathore A, Younas H, Gilkes D, Polotsky VY. Hypoxia-Inducible Factors and Cancer. Curr Sleep Med Rep. 2017;3(1):1–10. doi:10.1007/s40675-017-0062-7
11. Loboda A, Jozkowicz A, Dulak J. HIF-1 and HIF-2 transcription factors--similar but not identical. Mol Cells. 2010;29(5):435–442. doi:10.1007/s10059-010-0067-2
12. Deynoux M, Sunter N, Hérault O, Mazurier F. Hypoxia and hypoxia-inducible factors in leukemias. Front Oncol. 2016;6:41. doi:10.3389/fonc.2016.00041
13. Forristal CE, Brown AL, Helwani FM, et al. Hypoxia inducible factor (HIF)-2α accelerates disease progression in mouse models of leukemia and lymphoma but is not a poor prognosis factor in human AML. Leukemia. 2015;29(10):2075–2085. doi:10.1038/leu.2015.102
14. Chen H, Shen Y, Gong F, Jiang Y, Zhang R. HIF-α promotes chronic myelogenous leukemia cell proliferation by upregulating p21 expression. Cell Biochem Biophys. 2015;72(1):179–183. doi:10.1007/s12013-014-0434-2
15. Rinaldi I, Reksodiputro AH, Jusman SW, et al. Longer hydroxyurea administration prior to imatinib mesylate is risk factor for unsuccessful major molecular response in chronic-phase chronic myeloid leukemia: possibility of P-glycoprotein role. Asian Pac J Cancer Prev APJCP. 2019;20(12):3689–3695. doi:10.31557/APJCP.2019.20.12.3689
16. Saussele S, Richter J, Guilhot J, et al. Discontinuation of tyrosine kinase inhibitor therapy in chronic myeloid leukaemia (EURO-SKI): a prespecified interim analysis of a prospective, multicentre, non-randomised, trial. Lancet Oncol. 2018;19(6):747–757. doi:10.1016/S1470-2045(18)30192-X
17. Hoffmann VS, Baccarani M, Hasford J, et al. The EUTOS population-based registry: incidence and clinical characteristics of 2904 CML patients in 20 European Countries. Leukemia. 2015;29(6):1336–1343. doi:10.1038/leu.2015.73
18. Höglund M, Sandin F, Hellström K, et al. Tyrosine kinase inhibitor usage, treatment outcome, and prognostic scores in CML: report from the population-based Swedish CML registry. Blood. 2013;122(7):1284–1292. doi:10.1182/blood-2013-04-495598
19. Smith AG, Painter D, Howell DA, et al. Determinants of survival in patients with chronic myeloid leukaemia treated in the new era of oral therapy: findings from a UK population-based patient cohort. BMJ Open. 2014;4(1):e004266. doi:10.1136/bmjopen-2013-004266
20. Chen Y, Wang H, Kantarjian H, Cortes J. Trends in chronic myeloid leukemia incidence and survival in the United States from 1975 to 2009. Leuk Lymphoma. 2013;54(7):1411–1417. doi:10.3109/10428194.2012.745525
21. Corm S, Micol J, Leroyer A, et al. Kinetic of chronic myeloid leukaemia (CML) prevalence in Northern France since the introduction of imatinib. J Clin Oncol. 2008;26(15_suppl):7088. doi:10.1200/jco.2008.26.15_suppl.7088
22. Au WY, Caguioa PB, Chuah C, et al. Chronic myeloid leukemia in Asia. Int J Hematol. 2009;89(1):14–23. doi:10.1007/s12185-008-0230-0
23. Mendizabal AM, Younes N, Levine PH. Geographic and income variations in age at diagnosis and incidence of chronic myeloid leukemia. Int J Hematol. 2016;103(1):70–78. doi:10.1007/s12185-015-1893-y
24. Qiu G, Xu X, Liu Q. Targeting HIF-2α for the Treatment of CML by affecting LSCs metabolism and the vascular microenvironment. Blood. 2022;140(Supplement 1):5926–5927. doi:10.1182/blood-2022-168304
25. Ng KP, Manjeri A, Lee KL, et al. Physiologic hypoxia promotes maintenance of CML stem cells despite effective BCR-ABL1 inhibition. Blood. 2014;123(21):3316–3326. doi:10.1182/blood-2013-07-511907
26. Litz J, Krystal GW. Imatinib inhibits c-Kit-induced hypoxia-inducible factor-1alpha activity and vascular endothelial growth factor expression in small cell lung cancer cells. Mol Cancer Ther. 2006;5(6):1415–1422. doi:10.1158/1535-7163.MCT-05-0503
27. Gordan JD, Bertovrt JA, Hu CJ, Diehl JA, Simon MC. HIF-2α promotes hypoxic cell proliferation by enhancing c-Myc transcriptional activity. Cancer Cell. 2007;11(4):335–347. doi:10.1016/j.ccr.2007.02.006
28. Rouault-Pierre K, Lopez-Onieva L, Foster K, et al. HIF-2α protects human hematopoietic stem/progenitors and acute myeloid leukemic cells from apoptosis induced by endoplasmic reticulum stress. Cell Stem Cell. 2013;13(5):549–563. doi:10.1016/j.stem.2013.08.011
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.