")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 15
High Prevalence of Hypovitaminosis D in Cutaneous and Systemic Lupus Erythematosus Patients and Its Associated Factors: A Cross-Sectional Study in Thailand
Authors Kanokrungsee S, Patcharapojanart C, Suchonwanit P , Chanprapaph K
Received 4 May 2022
Accepted for publication 29 July 2022
Published 17 August 2022 Volume 2022:15 Pages 1663—1671
DOI https://doi.org/10.2147/CCID.S373117
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jeffrey Weinberg
Silada Kanokrungsee, Chanikarn Patcharapojanart, Poonkiat Suchonwanit, Kumutnart Chanprapaph
Division of Dermatology, Department of Medicine, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand
Correspondence: Kumutnart Chanprapaph, Division of Dermatology, Department of Medicine, Faculty of Medicine, Ramathibodi Hospital, Mahidol University, 270 Rama IV Road, Bangkok, 10400, Thailand, Tel +66 626393659, Email [email protected]
Objective: To investigate the prevalence of low vitamin D levels in patients with cutaneous lupus erythematosus (CLE) and systemic lupus erythematosus (SLE) in Thailand and determine the influential factors associated with inadequate levels.
Methods: The medical records of patients diagnosed with SLE and/or CLE and evaluated for serum 25-OH vitamin D were retrospectively reviewed from January 2014 to January 2021. Vitamin D deficiency (< 20 ng/mL) and insufficiency (21– 29 ng/mL) were indicated, and predictors of hypovitaminosis D were identified by multiple linear regression analysis.
Results: In total, 414 patients with SLE and/or CLE were included in the study. Vitamin D deficiency was predominant in the CLE-only group (33.3%), followed by SLE without CLE (15.6%) and SLE with CLE (8%), p < 0.001. Likewise, vitamin D insufficiency was more prevalent in the CLE-only group (44.4%) compared to SLE with (35.8%) and without CLE (40%). Multivariate analysis showed that a higher SLEDAI-2K score and female sex had a negative association with vitamin D levels, while an intake of every 10,000 IU of vitamin D2 per week increased serum vitamin D levels by up to 2.37 ng/mL. Furthermore, forty-five percent of patients continued to have vitamin D depletion despite commencing the recommended doses of vitamin D replacement.
Conclusion: Approximately half of Thai patients with SLE and 80% of CLE had vitamin D inadequacy. Vitamin D replacement is a good predictor of high serum vitamin D levels, while lower serum levels were associated with higher disease severity. Therefore, serum vitamin D monitoring and supplementation are suggested for all lupus erythematosus cases, especially those with CLE.
Keywords: 25(OH) vitamin D, cutaneous lupus erythematosus, lupus, systemic lupus erythematosus, vitamin D status
Introduction
Systemic lupus erythematosus (SLE) and cutaneous lupus erythematosus (CLE) are autoimmune diseases with a complex interplay between genetic and environmental factors leading to loss of self-tolerance and impairment of antigen clearance. These antigens are phagocytosed by plasmacytoid dendritic cells (pDC) that release type-1 interferon (IFN). Type I IFN can stimulate Th17 cells and suppress regulatory cells (Tregs) function, thus leading to autoreactive T cell production. Moreover, IFN also promotes differentiation and production of B cell antibodies. Consequently, these processes lead to autoantibodies attacking self-antigens and result in tissue damage.1,2
Vitamin D is a steroid hormone that plays a crucial role in skeletal and calcium metabolism. The primary source of vitamin D in human is cholecalciferol (vitamin D3) derived from skin synthesis upon exposure to sunlight. Beyond bone and mineral homeostasis function, a potential immunomodulatory role of vitamin D has gained enormous attention as immune cells, including T and B cells, macrophage, and dendritic cells express vitamin D receptors (VDR). Vitamin D can suppress T cell proliferation and directly inhibit immunoglobulin production by B cells.3 Additionally, it can modulate the maturation state of dendritic cells leading to protective immunity and self-tolerance. Therefore, the link between vitamin D and autoimmune diseases has been established.
Several epidemiologic studies, including one meta-analysis, have shown that low vitamin D level increases the risk and severity of SLE.4–6 Patients with SLE are at extremely high risk of vitamin D deficiency owing to several factors. VDR polymorphisms, which can moderate vitamin D levels, were found to be a genetic risk of SLE development in some populations.7,8 The use of glucocorticoids, limited sunlight exposure and application of photoprotective measures could lead to low vitamin D levels in lupus erythematosus (LE) patients. Likewise, published data showed that patients with CLE have higher prevalence of vitamin D inadequacy levels than control subjects.9,10 Moreover, treating vitamin D insufficiency is associated with improved CLE disease severity.9 Two prior studies from Thailand demonstrated that approximately 60–70% SLE patient experienced with vitamin D inadequacy.11,12 Nevertheless, data on the vitamin D status in CLE patients are sparse and there is no information on the Thai populations. In addition, a comparison of vitamin D levels in SLE and CLE patients is lacking. We aimed to investigate the prevalence of vitamin D status in SLE and CLE patients in Thailand and also to identify the influential factors associated with low serum vitamin D levels .
Methods
Study Design and Participants
This cross-sectional, analytic, retrospective study was conducted in a university-based hospital (Ramathibodi Hospital, Mahidol University, Bangkok, Thailand) between June 2019 and January 2021. The study protocol was approved by the Mahidol University Institutional Review Board for Ethics in Human Research (protocol number MURA2019/534), in accordance with Declaration of Helsinki. Medical records of all patients with SLE or CLE who were evaluated for serum 25-hydroxy vitamin D (25(OH)D) at the dermatology and/or rheumatology outpatient clinics from January 2014 to January 2021 were retrospectively reviewed. The data were collected cross-sectionally, where a single time point of serum 25(OH)D level for each individual was assessed. The informed consent was omitted based on the retrospective design of the study and the analysis used anonymous clinical data.
All patients older than 18 years of age who fulfilled the 2012 Systemic Lupus International Collaborating Clinics (SLICC) criteria and/or the 2019 European Alliance of Associations for Rheumatology/American College of Rheumatology (EULAR/ACR) classification criteria for SLE or have been previously and/or currently diagnosed with CLE with specific cutaneous manifestations were recruited. Subjects with CLE were further divided into acute CLE (ACLE), subacute CLE (SCLE), or chronic CLE (CCLE) based on clinical and/or histopathological findings. Other coexisting autoimmune diseases, gut malabsorption, impaired kidney or liver function, parathyroid disease, history of thyroid surgery, and incomplete medical records were excluded.
Demographic data of lupus patients including age, genders, onset, and duration of the disease, weight, and height including calculated body mass index (BMI), underlying diseases, Systemic lupus international collaborating clinics/American College of Rheumatology Damage Index (SLICC/ACR-DI) were collected from medical records. Systemic Lupus Erythematosus Disease Activity Index 2000 (SLEDAI-2K) score for indicating the disease severity, laboratory results (eg, creatinine, urinalysis, liver function test, serum 25(OH)D), systemic therapy (ie, systemic corticosteroids, antimalarials, and immunosuppressants including azathioprine, mycophenolate mofetil, methotrexate, cyclosporin, and cyclophosphamide) and vitamin D intake and calcium supplements during the previous 3 months before vitamin D measurement, were recorded and filled in protocol record form. All prescribed medications were given according to the guidelines for the management of SLE and CLE.13 The flow chart of the study is shown in Figure 1.
 |
Figure 1 The flow of patients included in the study. Abbreviations: CLE, cutaneous lupus erythematosus; CKD, chronic kidney disease; ESRD, end stage renal disease; SLE, systemic lupus erythematosus. |
Classifying Disease Activity Index and Damage Severity Score for SLE
To determine the severity of SLE patients, the SLEDAI-2K score was used to describe disease activity. The scores ranged between 0 and 105 which is evaluated from nine system involvements and disease activity, with higher scores indicating higher disease severity. Only SLEDAI-2K scores at the time of serum sampling were recorded. SLICC/ACR-DI is used to access accumulated damage since the onset of the disease in SLE patients. The index reflects irreversible damage in the various systems. The score is collected if the patient has had an item for at least 6 months and occurred after the onset of SLE.
Proteinuria and Lupus Nephritis
Proteinuria in the study was defined as more than 0.5 g per day by 24-hour urine or equivalent spot urine protein-to-creatinine ratio following the 2019 EULAR/ACR classification criteria. The presence of lupus nephritis (LN) in this study was defined as patients who were previously diagnosed with biopsy-proven LN.
Vitamin D Measurement and the Definition of Vitamin D Status
Total serum 25(OH)D was performed by an electrochemiluminescence immunoassay analyzer (DiaSorin-LIAISON® XL (DiaSorin S.p.A, Vercelli, Italy). Vitamin D deficiency was defined as serum 25(OH)D level ≤ 20 nanograms (ng)/milliliter (mL), vitamin D insufficiency was 21–29 ng/mL, and vitamin D sufficiency was 30 ng/mL or higher based on the US Endocrine Society criteria.14
Statistical Analysis
All statistical analysis was performed using STATA/MP version 16 (STATA Corp, College Station, TX). For continuous variables, normally distributed variables were summarized using the mean and SD, while the median and interquartile ranges were used for non-normally distributed variables. Univariate comparisons between categorical variables were performed using the Chi-square test or Fisher's exact test. We performed three independent groups comparison (SLE without CLE, SLE with CLE, and CLE-only). We used ANOVA to compare the difference among normally distributed variables. Meanwhile, non-normally distributed variables were analyzed by Kruskal–Wallis tests.
Multivariate analyses were performed by multiple linear regression models to identify independent factors of serum 25(OH)D level which allows adjustment for potential confounding factors (ie, age, gender, BMI, disease duration, lupus subgroup, SLEDAI-2K score, presence of LN, prednisolone dose, hydroxychloroquine (HCQ) intake, immunosuppressants administration, calcium, and vitamin D supplement). A p-value less than 0.05 was considered statistically significant.
Results
Baseline Demographics Among SLE and/or CLE Patients
Supplementary Table displays patients’ demographics in SLE and/or CLE patients. A total of 414 patients with SLE and/or CLE were included and further divided into 3 subgroups, SLE without CLE (n = 225, 54.3%), SLE with CLE (n = 162, 39.1%), and CLE alone (n = 27, 6.5%). The mean age of the patients was older in the CLE group as compared to SLE without CLE and SLE with CLE, 51.9 (20.4), 46.2 (14.6), and 42.4 (13.4)-year-old, respectively, p=0.002. Females were predominant in all groups, the female-to-male ratio was 13:1 and 17.1 in SLE without and with CLE, and the ratio decreased significantly in CLE patients to 2.8:1, p=0.001. Compared to CLE cases, both SLE without and with CLE experienced longer median disease duration 12 (6.5–18), 13.0 (8–18), and 1.5 (0–3.5) years, p<0.001. With regard to the CLE subtype, discoid lupus erythematosus was the most common cutaneous manifestation in patients with SLE with CLE, and CLE alone, accounting for 67.9% and 63%, respectively. SLEDAI-2K score and SLICC/ACR-DI were not significantly different between SLE with and without CLE. The percentage of LN was slightly higher in SLE without CLE (42.4%) compared to SLE with CLE (33.1%) but without statistical significance.
Regarding current treatment, a higher percentage of patients commencing oral prednisolone was found in SLE with and without CLE, as compared to CLE alone (69.2% and 63.2% vs 7.7%, p<0.001). A similar trend was demonstrated for the immunosuppressants used, p<0.001. The number of patients who received HCQ was similar among all subgroups. Only one-fourth of CLE patients received vitamin D supplements, whereas over three-fourths of SLE with and without cutaneous involvement received a 20,000 IU weekly dose of vitamin D2 formulation . Calcium supplement was taken in only one patient in the CLE group, while roughly 80% of SLE patients had calcium intake (p<0.001) with a median dose of 1200 mg/day.
Prevalence of Vitamin D Insufficiency/Deficiency and Serum Vitamin D Levels
The overall prevalence of vitamin D deficiency and insufficiency in this study was 13.8% and 38.7%, respectively (Table 1). Approximately half of the patients (47.6%) had sufficient vitamin D levels. Vitamin D deficiency was predominant in the CLE-only group (33.3%), followed by SLE without CLE (15.6%) and SLE with CLE (8.0%), p<0.001. Likewise, vitamin D insufficiency was also more commonly observed in the CLE-only group (44.4%) compared to SLE with (35.8%) and without (40%) CLE. Only 22.2% of patients with skin limited disease were categorized as having vitamin D sufficiency status, while 56.2% and 44.4% of SLE with and without CLE cases had sufficient vitamin D. Correspondingly, the lowest mean serum 25(OH)D level was found in the CLE-alone group followed by SLE without and with cutaneous involvement, respectively (23.1, 30.7 and 33.1 ng/mL, p<0.001).
 |
Table 1 Serum Vitamin D Levels and Vitamin D Status in SLE with and without CLE, and CLE-Only Patients |
Independent Factors Associated with Vitamin D Levels
In the multivariate regression analysis model, we found three factors independently associated with vitamin D levels, as shown in Table 2. First, male gender had higher vitamin D levels than female (ß = 9.17 ng/mL, 95% CI 3.18, 15.16, p=0.003). Second, higher SLEDAI-2K score was correlated with lower serum vitamin D levels (ß = −0.88, 95% CI −1.58, −0.18, p=0.014). Lastly, vitamin D replacement therapy had a significant association with high serum vitamin D levels. Specifically, an intake of every 10,000 IU per week of vitamin D2 elevated serum vitamin D levels to 2.37 ng/mL (95% CI 1.11, 3.62, p<0.001). However, no significant correlation was found among other variables, namely the presence of LN, systemic treatments (prednisolone, immunosuppressants, and HCQ intake), and calcium supplementation.
 |
Table 2 Regression Coefficient Between Variables and Serum Vitamin D Levels |
Vitamin D Status in Patients with and without Vitamin D Supplementation
Three hundred and thirteen of 408 (76.7%) patients received vitamin D supplementation. Only 25.9% of CLE-only cases were on vitamin D replacement. Conversely, the majority of SLE patients received vitamin D supplements (84.6% and 76.5% of SLE patients with and without CLE, respectively, Table 3). However, 45.1% of all patients still experienced vitamin D insufficiency/deficiency despite supplementation. CLE-only patients with vitamin D supplementation also showed the lowest serum vitamin D levels and the lowest proportion of sufficient vitamin D compared to SLE patients, p<0.002 and p=0.026, respectively. Nevertheless, there was no difference between the vitamin D status among LE subgroups in patients without supplementation, p=0.463. Moreover, patients who received prednisolone or immunosuppressants were more likely prescribed with vitamin D supplement (68.6% vs 31.4% for those with prednisolone intake, p<0.001, and 60.6% vs 39.4% for those commencing immunosuppressive therapy, p<0.001).
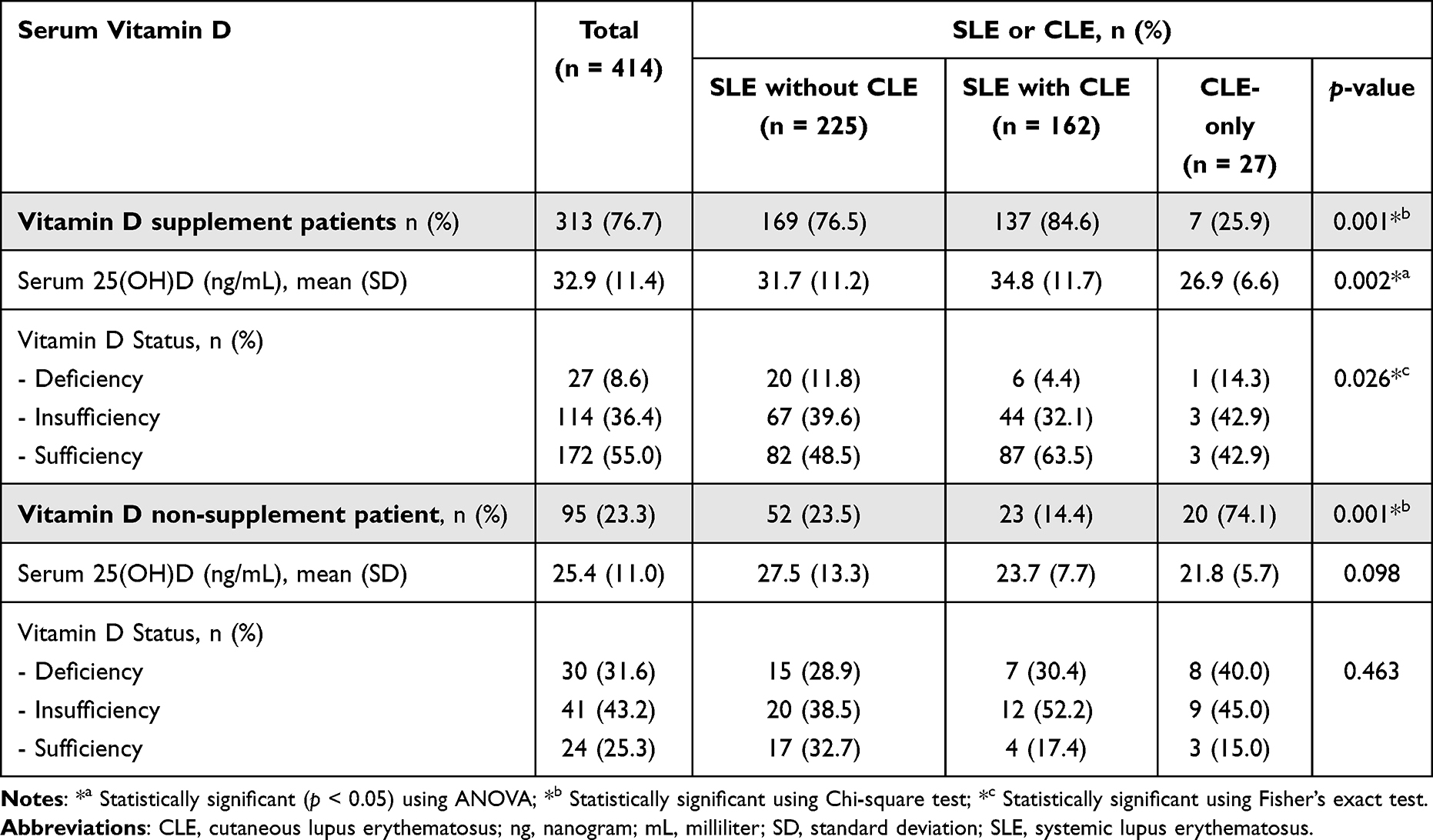 |
Table 3 Serum Vitamin D Levels and Vitamin D Status in Supplemented and Non-Supplemented Patients |
Discussion
The high prevalence of hypovitaminosis D in patients with SLE has been observed worldwide. While aberrant innate immune systems along with T and B cells activation contribute to inflammatory cytokines release and autoantibody production in lupus, vitamin D is interconnected as an immune modulator that dampens the inflammatory reaction. To date, this is the first study to compare the vitamin D status between SLE with and without CLE, and CLE-only patients. We revealed a high prevalence of vitamin D insufficiency/deficiency in all LE subgroups, and approximately half of SLE with and without CLE had inadequate serum vitamin D levels.
Several studies reported a high prevalence of suboptimal vitamin D (25(OH)D < 30 ng/mL) in SLE patients ranging from 62.2% to 96% from United States,15 Canada,15,16 European countries,15,17 China,18,19 Hong Kong,20 Malaysia,21 Mexico,22 and Egypt.23 The current study showed that approximately half of Thai SLE patients had inadequate vitamin D, which was lower than previously described in other reports (58% and 73.1%).11,12 The lower prevalence of hypovitaminosis D in Thai SLE patients compared to other areas around the world could be because of the geographic location and latitudes, as Thailand is a country with abundant sunshine, a high UV index, and minimal year-round daily variation in sunlight, the main source of vitamin D. However, other studies from Korea24 and Brazil25 reported lower frequencies of vitamin D insufficiency, 16.6% and 37.7%, respectively. Hence, many other potential factors related to serum vitamin D concentration could be explored.
The highest frequency of vitamin D inadequacy in our study was found in patients with the skin-limited disease, where over three-fourth had serum 25(OH)D below 30 ng/mL. Previous studies from European countries have reported the prevalence of vitamin D insufficient/deficient ranging from 65% to 97% in patients with CLE.10,26–28 Again, the higher latitudes and lower levels of year-round sunlight may contribute to a higher prevalence of suboptimal vitamin D among those countries. Nevertheless, we found that the prevalence of vitamin D inadequacy in CLE-only Thai patients remained high. Our recent publication demonstrated that SLE patients with cutaneous involvement appear to perform better photoprotective practice than those without. A valid explanation is that patients with cutaneous lesions have had direct exposure to sunlight, exacerbating their cutaneous disease, which raises the motivation for them to implement a more rigorous photoprotection measure.29 A study conducted in Singapore also demonstrated serum 25(OH)D less than 20 ng/mL (deficiency) in 51% of CLE patients, which is slightly more than our study (33.3%).30 The reason why Singaporeans had higher vitamin D deficiency may contribute to the genetic factors and variety of ethnicity, where the majority were Malay and Indian with darker skin types, and the higher melanin content may have resulted in limited vitamin D biosynthesis.
Comparing vitamin D supplemented and non-supplemented patients, only 25% of cases with limited CLE received vitamin D treatment, while 80% of SLE patients were on supplementation. Vitamin D replacement has been recommended to those commencing long-term systemic glucocorticoids; therefore, the majority of our SLE patient with internal organ involvement had vitamin D supplementation. Given the relatively benign nature of CLE, the importance of vitamin D supplementation has been under concern. Our data demonstrated that CLE patients are at the highest risk of vitamin D inadequacy and possess the lowest chance of restoring vitamin D. Cutillas-Marco et al9 have shown that vitamin D replacement in CLE patients can significantly decrease the disease severity compared to those without treatment. Accordingly, while physicians should adequately address photoprotective behavior and reinforce proper implementation, vitamin D replacement therapy may be equally as important to prevent disease exacerbation in patients with LE.
In non-supplemented patients, the proportion of vitamin D insufficiency/deficiency has increased to 70–85%, which is in line with the literature.15–23,31,32 The presence of low vitamin D levels in SLE patients contributes to a higher risk of hypertension, hyperlipidaemia, fatigue, and lower bone mineral density. It has also been associated with high disease severity17,18,25 and disease flare.33,34 A study by Abou-Raya et al35 demonstrated that SLE patients who were restored with 2000 IU daily vitamin D3 supplement had significant reduction in proinflammatory cytokines after 12 months. Additionally, previous data have shown that vitamin D supplementation is being considered to improve fatigue symptoms and diseases severity in SLE and CLE patients.9,36–39 To correct vitamin D deficiency, 400–1000 IU/day of oral vitamin D3 or 800–1000 IU/day of vitamin D2 is recommended. Oral vitamin D3 replacement is generally more effective than vitamin D2. Based on our data, approximately 45% of patients with CLE/SLE still encountered vitamin D insufficiency or deficiency despite commencing the recommended dose of vitamin D supplementation. Additionally, an intake of every 10,000 IU of vitamin D2 per week could elevate serum vitamin D levels up to 2.37 ng/mL. Therefore, it is important not only to monitor serum 25-hydroxy vitamin D at baseline but also after vitamin D replacement to achieve the optimum supplementary dose.
Many influential factors determining lower serum vitamin D levels in SLE patients have been established including ethnicity,21 photoprotective measures,17,25 glucocorticoid doses,11 cumulative glucocorticoids,16 serum creatinine levels,11,16 renal disease,12,21,26 inadequate vitamin D supplement17,18 and HCQ used.17 Among these factors, we found that gender, disease severity, and vitamin D supplement dosage were correlated with serum 25(OH) levels. Women have lower serum vitamin D levels than men, perhaps because women may implement better photoprotection to maintain desirable white skin, as this appears to be an attractive trend in Thailand.40 The inverse correlation between SLEDAI-2K score and serum vitamin D levels was shown in our report. Several researchers determining the effect of vitamin D on the progression and disease severity favored the immunomodulatory role of vitamin D.17,18,22,24,25,37 This relationship may be due to the inhibitory effect of vitamin D on potentiating the innate immune response, as well as downregulating Th1 response and inflammatory cytokines production such as IL-2 and IFN.3 However, whether low vitamin D levels are a consequence of LE or have a pathogenic role relating to the disease activity remains unclear and requires further investigation.
This study is subjected to several limitations. We did not collect certain variables affecting vitamin D levels, such as sun exposure, sunscreen use, and the serum levels of parathyroid hormone, calcium, and phosphorus. Additionally, as this is a retrospective study, incomplete data may exist. Lastly, the data was assessed at a single timepoint, which does not allow us to establish a causal relationship between lupus disease activity and vitamin D levels.
Conclusion
The prevalence of vitamin D inadequacy was 50% and 80% in Thai patients with SLE and CLE, respectively. Despite vitamin D supplementation, the occurrence of inadequate vitamin D remained high. Vitamin D replacement is a good predictor of high serum vitamin D levels in a dose-dependent manner, and lower serum levels were associated with higher disease severity. While vitamin D is accountable for immune protective activity against lupus, it is unclear whether low vitamin D levels are a consequence of LE or have a causative role. Nevertheless, serum vitamin D monitoring and supplementation are recommended to all patients with SLE and CLE. Further studies are warranted to identify the role of vitamin D in lupus and the optimum vitamin D supplemental dose for these particular patients.
Data Sharing Statement
Data are available from the corresponding author upon reasonable request.
Acknowledgments
The study was supported by the Division of Dermatology and the Clinical Research Unit, all from the Faculty of Medicine, Ramathibodi Hospital, Mahidol University, Bangkok, Thailand.
Funding
There is no funding support for this study.
Disclosure
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
1. Nguyen MH, Bryant K, O’Neill SG. Vitamin D in SLE: a role in pathogenesis and fatigue? A review of the literature. Lupus. 2018;27:2003–2011.
2. Ronnblom L, Leonard D. Interferon pathway in SLE: one key to unlocking the mystery of the disease. Lupus Sci Med. 2019;6:e000270.
3. Dall’Ara F, Cutolo M, Andreoli L, et al. Vitamin D and systemic lupus erythematous: a review of immunological and clinical aspects. Clin Exp Rheumatol. 2018;36:153–162.
4. Guan SY, Cai HY, Wang P, et al. Association between circulating 25-hydroxyvitamin D and systemic lupus erythematosus: a systematic review and meta-analysis. Int J Rheum Dis. 2019;22:1803–1813.
5. Colotta F, Jansson B, Bonelli F. Modulation of inflammatory and immune responses by vitamin D. J Autoimmun. 2017;85:78–97.
6. Yap KS, Northcott M, Hoi AB, et al. Association of low vitamin D with high disease activity in an Australian systemic lupus erythematosus cohort. Lupus Sci Med. 2015;2:e000064.
7. Bae SC, Lee YH. Association between Vitamin D level and/or deficiency, and systemic lupus erythematosus: a meta-analysis. Cell Mol Biol (Noisy-le-Grand). 2018;64:7–13.
8. Ruiz-Ballesteros AI, Meza-Meza MR, Vizmanos-Lamotte B, et al. Association of Vitamin D Metabolism Gene Polymorphisms with Autoimmunity: evidence in Population Genetic Studies. Int J Mol Sci. 2020;21:9626.
9. Cutillas-Marco E, Marquina-Vila A, Grant WB, et al. Vitamin D and cutaneous lupus erythematosus: effect of vitamin D replacement on disease severity. Lupus. 2014;23:615–623.
10. Cutillas-Marco E, Morales-Suarez-Varela M, Marquina-Vila A, et al. Serum 25-hydroxyvitamin D levels in patients with cutaneous lupus erythematosus in a Mediterranean region. Lupus. 2010;19:810–814.
11. Chaiamnuay S, Chailurkit LO, Narongroeknawin P, et al. Current daily glucocorticoid use and serum creatinine levels are associated with lower 25(OH) vitamin D levels in Thai patients with systemic lupus erythematosus. J Clin Rheumatol. 2013;19:121–125.
12. Sumethkul K, Boonyaratavej S, Kitumnuaypong T, et al. The predictive factors of low serum 25-hydroxyvitamin D and vitamin D deficiency in patients with systemic lupus erythematosus. Rheumatol Int. 2013;33:1461–1467.
13. Fanouriakis A, Kostopoulou M, Alunno A, et al. update of the EULAR recommendations for the management of systemic lupus erythematosus. Ann Rheum Dis. 2019;(78):736–745.
14. Holick MF, Binkley NC, Bischoff-Ferrari HA, et al. Evaluation, treatment, and prevention of vitamin D deficiency: an Endocrine Society clinical practice guideline. J Clin Endocrinol Metab. 2011;96:1911–1930.
15. Lertratanakul A, Wu P, Dyer A, et al. 25-hydroxyvitamin D and cardiovascular disease in patients with systemic lupus erythematosus: data from a large international inception cohort. Arthritis Care Res. 2014;66:1167–1176.
16. Toloza SM, Cole DE, Gladman DD, et al. Vitamin D insufficiency in a large female SLE cohort. Lupus. 2010;19:13–19.
17. Ruiz-Irastorza G, Egurbide MV, Olivares N, et al. Vitamin D deficiency in systemic lupus erythematosus: prevalence, predictors and clinical consequences. Rheumatology. 2008;47:920–923.
18. Gao CC, Liu SY, Wu ZZ, et al. Severe vitamin D deficiency increases the risk for moderate to severe disease activity in Chinese patients with SLE. Lupus. 2016;25:1224–1229.
19. Zheng ZH, Gao CC, Wu ZZ, et al. High prevalence of hypovitaminosis D of patients with autoimmune rheumatic diseases in China. Am J Clin Exp Immunol. 2016;5:48–54.
20. Mok CC, Birmingham DJ, Ho LY, et al. Vitamin D deficiency as marker for disease activity and damage in systemic lupus erythematosus: a comparison with anti-dsDNA and anti-C1q. Lupus. 2012;21:36–42.
21. Ong SG, Ding HJ. Vitamin D status in a monocentric cohort of systemic lupus erythematosus (SLE) patients and correlations with clinical and immunological profile. Med J Malaysia. 2019;74:492–498.
22. Garcia-Carrasco M, Mendoza-Pinto C, Etchegaray-Morales I, et al. Vitamin D insufficiency and deficiency in Mexican patients with systemic lupus erythematosus: prevalence and relationship with disease activity. Reumatol Clin. 2017;13:97–101.
23. Abaza NM, El-Mallah RM, Shaaban A, et al. Vitamin D Deficiency in Egyptian Systemic Lupus Erythematosus Patients: how Prevalent and Does It Impact Disease Activity? Integr Med Insights. 2016;11:27–33.
24. Kim HA, Sung JM, Jeon JY, et al. Vitamin D may not be a good marker of disease activity in Korean patients with systemic lupus erythematosus. Rheumatol Int. 2011;31:1189–1194.
25. Souto M, Coelho A, Guo C, et al. Vitamin D insufficiency in Brazilian patients with SLE: prevalence, associated factors, and relationship with activity. Lupus. 2011;20:1019–1026.
26. Cusack C, Danby C, Fallon JC, et al. Photoprotective behaviour and sunscreen use: impact on vitamin D levels in cutaneous lupus erythematosus. Photodermatol Photoimmunol Photomed. 2008;24:260–267.
27. Renne J, Werfel T, Wittmann M. High frequency of vitamin D deficiency among patients with cutaneous lupus erythematosus [corrected]. Br J Dermatol. 2008;159:485–486.
28. Heine G, Lahl A, Muller C, et al. Vitamin D deficiency in patients with cutaneous lupus erythematosus is prevalent throughout the year. Br J Dermatol. 2010;163:863–865.
29. Chanprapaph K, Ploydaeng M, Pakornphadungsit K, et al. The behavior, attitude, and knowledge towards photoprotection in patients with cutaneous/systemic lupus erythematosus: a comparative study with 526 patients and healthy controls. Photochem Photobiol Sci. 2020;19:1201–1210.
30. Gronhagen CM, Tang MB, Tan VW, et al. Vitamin D levels in 87 Asian patients with cutaneous lupus erythematosus: a case-control study. Clin Exp Dermatol. 2016;41:723–729.
31. Wu PW, Rhew EY, Dyer AR, et al. 25-hydroxyvitamin D and cardiovascular risk factors in women with systemic lupus erythematosus. Arthritis Rheum. 2009;61:1387–1395.
32. Yeap SS, Othman AZ, Zain AA, et al. Vitamin D levels: its relationship to bone mineral density response and disease activity in premenopausal Malaysian systemic lupus erythematosus patients on corticosteroids. Int J Rheum Dis. 2012;15:17–24.
33. Birmingham DJ, Hebert LA, Song H, et al. Evidence that abnormally large seasonal declines in vitamin D status may trigger SLE flare in non-African Americans. Lupus. 2012;21:855–864.
34. Bonakdar ZS, Jahanshahifar L, Jahanshahifar F, et al. Vitamin D deficiency and its association with disease activity in new cases of systemic lupus erythematosus. Lupus. 2011;20:1155–1160.
35. Abou-Raya A, Abou-Raya S, Helmii M. The effect of vitamin D supplementation on inflammatory and hemostatic markers and disease activity in patients with systemic lupus erythematosus: a randomized placebo-controlled trial. J Rheumatol. 2013;40:265–272.
36. Aranow C, Kamen DL, Dall’Era M, et al. Randomized, Double-Blind, Placebo-Controlled Trial of the Effect of Vitamin D3 on the Interferon Signature in Patients With Systemic Lupus Erythematosus. Arthritis Rheumatol. 2015;67:1848–1857.
37. Munoz-Ortego J, Torrente-Segarra V, Prieto-Alhambra D, et al. Prevalence and predictors of vitamin D deficiency in non-supplemented women with systemic lupus erythematosus in the Mediterranean region: a cohort study. Scand J Rheumatol. 2012;41:472–475.
38. Terrier B, Derian N, Schoindre Y, et al. Restoration of regulatory and effector T cell balance and B cell homeostasis in systemic lupus erythematosus patients through vitamin D supplementation. Arthritis Res Ther. 2012;14:R221.
39. Lima GL, Paupitz J, Aikawa NE, et al. Vitamin D Supplementation in Adolescents and Young Adults With Juvenile Systemic Lupus Erythematosus for Improvement in Disease Activity and Fatigue Scores: a Randomized, Double-Blind, Placebo-Controlled Trial. Arthritis Care Res. 2016;68:91–98.
40. Rajatanavin N, Kanokrungsee S, Aekplakorn W. Vitamin D status in Thai dermatologists and working-age Thai population. J Dermatol. 2019;46:206–212.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.