")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Hormonal Contraception Use and Depression Among Women in Saudi Arabia
Authors Albawardi I , Alqahtani AH , Aljamea DA, Aljaafari SA , Aldulijan FA, Almuhaidib SR , Elamin M , Al Qahtani NH
Received 17 April 2022
Accepted for publication 28 July 2022
Published 5 August 2022 Volume 2022:15 Pages 1677—1688
DOI https://doi.org/10.2147/JMDH.S371203
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Ibrahim Albawardi,1 Abdullah H Alqahtani,1 Dana A Aljamea,2 Sara A Aljaafari,2 Fajar A Aldulijan,2 Seereen R Almuhaidib,2 Mohamed Elamin,3 Nourah H Al Qahtani4
1Department of Psychiatry, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 2College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 3Department of Biochemistry, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia; 4Department of Obstetrics and Gynecology, College of Medicine, Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia
Correspondence: Ibrahim Albawardi, King Fahad University Hospital, Office 155, Building 200, Alburaq Street, Alkhobar, Saudi Arabia, Tel/Fax +966138966877. Ex.: 1554, Email [email protected]
Purpose: To estimate the prevalence of depression amongst hormonal and non-hormonal contraception users, and the risk factors associated with depression in the sample.
Patients and Methods: This is a community-based cross-sectional study conducted in the Kingdom of Saudi Arabia from October to November 2021, covering all regions of Saudi Arabia. All participants were women, living in Saudi Arabia, ≥ 21 years old and ≤ 45 years old, using a contraceptive method, and with no established history of depression.
Results: A total of 4853 out of 18,596 met our criteria and were included in this study. Among all sample groups, 29% had moderate to severe depression. Rates of depression and association studies’ results in women using hormonal were higher than those who use non-hormonal birth control methods. Psychiatric disorders, medical illnesses, substance use and depressogenic medication use were all associated with depression in both hormonal and non-hormonal contraception users.
Conclusion: The current study shows high prevalence of depression amongst hormonal contraceptive users compared to non-hormonal contraceptive users.
Keywords: hormonal contraception, non-hormonal contraception, depression, psychiatric disorders
Introduction
Contraception is a vital part of family planning that gives partners the choice of preventing conception, the ability to plan when they would like to start and stop having children and to determine the intervals between pregnancies. This may allow parents to dedicate time for other priorities and increase their chances of investing in their future children and thereby enhancing the quality of care provided for them. Besides personal and health reasons, contraception positively impacts the environment, economy, and education through controlling overpopulation in certain parts of the world. For these reasons, along with many others, contraception is enlisted under the United Nations Declaration of Human Rights. 1 Contraception is currently used by approximately 100 million women worldwide.2 Methods of birth control can be hormonal or non-hormonal. The non-hormonal methods include barriers (male and female condoms), mechanical (copper IntraUterine Device (IUD)), natural (fertility-awareness-based methods), and surgical methods (male or female sterilization). On the other hand, hormonal contraceptive methods include Oral Contraceptive Pills (OCPs), patches, hormonal IUD, implants, and injections. Combined estrogen-progesterone pills are the most commonly used contraceptive method both locally and globally.3–6
Periods where there are estrogen instability (e.g.: puberty, premestruation, postpartum) have increased risk of affective disorders. The interaction between gonadal steroidal hormones and the CNS neurotransmitters might have a rule in this risk. In the animal studies, estrogen increases the monoamines activity, the number of serotonergic receptors as well as the neurotransmitters’ transport and uptake.7
Unfortunately, none of the contraceptive methods are free of side-effects.8 Previous studies have shown that hormonal birth control methods were positively associated with subsequent mood disturbance, diagnosis of depression, use of antidepressants and even suicidal attempts. In fact, mood changes were considered one of the most important reasons for discontinuing hormonal contraception or opting for another method.9–12 On the other hand, results of two systematic reviews have denied the existence of a clear association between hormonal contraception and depression, or the potential for them to worsen symptoms of pre-diagnosed depression.13,14 Therefore, the answer of whether the two are positively associated remains vague and inconclusive.
To assess the relationship between depression and contraception, it is vital to take depression risk factors into consideration. Some of the risk factors are female sex, financial or social stressors, chronic or serious diseases, family history and substance use.15
Materials and Methods
This is a community-based cross-sectional study conducted in the Kingdom of Saudi Arabia from October to November 2021. It is a comprehensive study covering all regions of Saudi Arabia.
Study Subjects, Inclusion and Exclusion Criteria
We included all the Saudi women to assess the prevalence of contraception use. Then we applied the inclusion criteria to assess the relationship between hormonal and non-hormonal contraception use and depression. All women who met our inclusion criteria were included (living in Saudi Arabia, ≥21 years old and ≤45 years old, currently using a contraceptive method whether hormonal or non-hormonal). Women who are using non-hormonal contraceptive methods were included in this study for comparison purposes. Excluded participants were those who were <21 or >45 years old, and those with an established history of depression. History of depression and being <21 or >45 years old can act as confounders mixing the pathophysiology of having higher risk of depression because of already having disturbed hormonal levels such as in depression, adolescence age, or menopausal age, and exogenous hormonal use.16,17 Also we excluded those who combined using hormonal and nonhormonal methods to keep the results more accurate.
Sample Size and Sampling Technique
According to the Saudi General Authority for Statistics, our study’s population equals 6,776,111 (21–45 years old women residing in Saudi Arabia).18 Epi info version 7 was used to estimate the sample size of this study with a confidence level of 95%, and 3% margin of error, with a P-value set at 0.05. The estimated sample size was 1067 participants.
Ethical Consideration
Online consent was obtained from participants before participating in this study. Participants had the choice to opt-out after starting to fill the survey. Ethical approval (IRB-UGS-2021-01-370) was obtained in October 2021 from the Institutional Review Board (IRB) office of Imam Abdulrahman Bin Faisal University, Dammam, Saudi Arabia.
Data Collection and Materials Used
An online survey was randomly sent to the participants through QuestionPro. The survey is an expert-approved checklist based on available literature consisting of 7 parts: demographic data, obstetric and gynecological history (including use of contraception, reason and duration of use, type of contraception), psychiatric history, past medical history, depressogenic medication use, social history (including alcohol, smoking, and illicit use), and Patient Health Questionnaire-9 (PHQ9) which is a tool used for screening for depression.
Patient Health Questionnaire-9 (PHQ9): It is a well-known self-administered screening and provisional diagnostic tool for depression. The original version was in English. However, as our study population is Arabic, the translated version was used in this study. Cronbach’s alpha was used in another study conducted in Saudi Arabia to test the internal reliability of the Arabic version of PHQ-9 and it was found to be 0.857. Validity of the questionnaire was also measured when it was first translated into Arabic in 2002 and it was valid in the Saudi Population.19
PHQ 9 consists of 9 questions, each question has 4 choices to choose from regarding the frequency of the presence of symptoms (“Not at all”, “Several days”, “More than half of the days” and “Nearly every day”). Total score of 0–4 indicates normal or no depression (none-minimal depression), score between 5 and 9 indicates mild depression, 10 and 14 indicates moderate depression, 15 and 19 indicates moderately severe depression and 20 or more indicates severe depression.
During data analysis, we found that the question that assesses the sleep in the PHQ-9 questionnaire was missed in the survey. To overcome this accidental mistake, we calculated the mean of the results of the available questions then multiply it by 9. This came after we calculated the reliability of the 8 questions and found that the Cronbach’s Alpha was 0.87.
Statistical Analysis
Data analysis was carried out using SPSS version 25, and all data were analyzed anonymously. All quantitative (categorical) variables were summarized as frequencies and percentages using Frequency Analysis Test.
Differences between the two groups (women who were using hormonal contraceptive methods and women who were using non-hormonal contraceptive methods) were tested using two-way crosstab tests. The association between variables was tested using Pearson’s Chi-square Test. P value of <0.05 was considered statistically significant.
Study Variables
The independent variable in this study was the use of a hormonal contraceptive method. The dependent variable was depression, and the controlled variables were participant’s age, past medical history, past psychiatric history, and substance use.
Results
Demographic Characteristics
Out of the participants that answered the survey (n = 18,596), we excluded those who did not use contraception, and those who have been diagnosed with depression. Four thousand eight hundred and fifty-three out of 18,596 met our criteria and were included in this study. Our study participants were almost evenly distributed between the different regions of Saudi Arabia and the majority were aged between 21 and 35 years old. Most of the women were married (87.4%), Saudi (93.6%), and received college education (73%). Approximately half of the participants were unemployed (51%) and had a monthly family income of 5000–15,000 Saudi Riyals (SR) (54.5%) (Table 1). Regarding the obstetric part of the questionnaire, 29.2% of the participants had more than 3 children, 57.9% had given birth in the past 12 months, and 68.1% had a negative history of abortion (Table 2).
 |
Table 1 Demographic Characteristics of the Study Sample (N= 4853) |
 |
Table 2 Obstetric Data of the Sample (N= 4853) |
The Prevalence, Types, and Duration of Contraception Use
The overall prevalence of contraception use was 30.1% of those who answered the survey. Amongst the sample, 66.5% (n = 3228) reported hormonal contraception use, whilst 33.5% (n = 1625) reported using non-hormonal methods (Figure 1). Among hormonal methods, 26.4% and 25.6% of the women reported using combined estrogen and progesterone and progestin only pills, respectively, making OCPs the most used method. As for non-hormonal methods, Copper IUD ranked highest in percentage (14.2%) (Table 3). Furthermore, it was found that 57.6% (n = 2795) of the participants had been using contraception for more than 12 months, 23.8% (n = 1154) had been using it for 3–12 months, and 18.6% (n = 904) for less than 3 months.
 |
Table 3 Breakdown of the Specific Types of Hormonal and Non-Hormonal Contraception Methods Used (N= 4853) |
 |
Figure 1 Types of contraception. |
No significant differences were observed regarding the demographic data between the two groups (Table 4).
 |
Table 4 Comparative Study Between Hormonal and Non-Hormonal Contraception in Relation to Different Demographic Factors and Obstetric History [N (%)] |
The Prevalence of Depression and Its Risk Factors
The majority of the screening results for depression were none-minimal and mild depression, with prevalence rates of 43.1% (n = 2091) and 27.9% (n = 1353), respectively. Moderate depression was shown in 15.8%, moderately severe in 9.2%, and severe in 4% of the women (Figure 2). In our sample, the prevalence of depression risk factors was as the following: 18.2% (n = 881) of the participants were previously diagnosed with psychiatric disorders, 15.9% (n = 774) were previously diagnosed with physical illnesses, 7.2% (n = 404), had history of substance use, and 25.7% (1247) were using depressogenic medications. It was also found that more than one year of contraceptive use was positively associated with none-minimal and mild degrees of depression (P value = 0.00) (Table 5).
 |
Table 5 The Association Between Depression and Duration of Contraceptive Use |
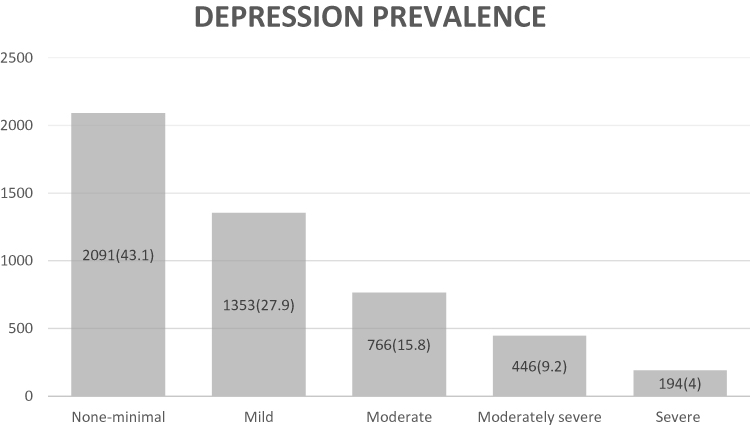 |
Figure 2 Depression provenance. |
The Association Between Depression and Contraception Use
Rates of depression were higher in women using hormonal contraceptive methods compared to non-hormonal birth control methods. The rate of moderate to severe depression was 30.6% in the hormonal contraception group in comparison to 25.8% in the group using non-hormonal contraceptives (Figure 3). When we recategorized the depression scores to two groups, one group who has none-minimal to mild depression and the other group who has moderate to severe depression aiming to assess the Odd ratio, we found the hormonal group having 1.267 times higher risk to develop moderate to severe depression compared to non-hormonal contraceptive methods’ users (P value: 0.00) (Table 6).
 |
Table 6 The Association Between Depression and Contraception Methods [N (%)] |
 |
Figure 3 Types of contraception and depression. |
Furthermore, the association between depression in women using hormonal contraceptive methods and the specified risk factors has been studied to determine the presence of a relationship. Psychiatric disorders, medical illnesses, substance use and depressogenic medications use were all positively associated with depression in both hormonal and non-hormonal contraception users, OR: 3.3, 1.9, 1.59 and 2.27 respectively (P value: 0.00).
Discussion
Contraceptive methods are widely used by women during their reproductive age. The relation between depression and hormonal contraceptive use remains a matter of debate. In light of this, a number of studies were done to examine the association between the two. However, inconsistency in the results of these studies was observed, which may be attributed to variations in the settings of these studies such as socio-demographic data, methods, and sample size. This study was conducted to highlight the prevalence of hormonal contraception use and its association with depression among women in the Kingdom of Saudi Arabia.
According to our data, 4853 of the respondents were using contraceptive methods and 66.5% of them were on hormonal contraceptives while only 33.5% were using non-hormonal contraceptive methods. Regarding the depression prevalence amongst our sample, we observed that the majority of the respondents were exhibiting none-minimal to mild depression accounting to 43.1% and 27.9%, respectively. Fortunately, this rate of depression does not need psychiatric attention or further intervention. However, moderate, moderately severe, and severe depression rates were present in our sample and were found to be 15.8%, 9.2%, and 4% among participants, respectively. In addition, we studied the prevalence of certain risk factors among our sample to assess their relation to depression. Among all risk factors, depressogenic medication’s use was found in 25.7% followed by previous psychiatric disorders (18.2%), previous physical illness (15.9%), and substance use history (7.2%). Moreover, as we expected, rates of depression were observed to be higher among hormonal contraceptive group compared to non-hormonal contraceptive group. Further, rates of moderate to severe depression among hormonal contraceptive group were 30.6% in contrast to 25.8% in non-hormonal group. The positive relationship between the previously mentioned risk factors and depression was noticed among hormonal contraceptive group.
Depression is one of the most disabling conditions worldwide.20 Women have double the risk of developing depression compared to men.21 Approximately 17 out of 100 women will experience major depression during their lifetime, with a peak during reproductive years.22 In our study, we observed that women on hormonal contraceptive methods were at increased risk of moderate to severe depression compared to those using non-hormonal contraceptive methods.
In the contrary, several studies have highlighted the effect of OCPs in stabilizing mood swings in premenstrual dysphoric disorders.22 A scientific review by McEwen was done to highlight the effect of estrogen on the brain and its influence in modulating the pathways implicated in the pathogenesis of mood disorders. This review showed that estrogen receptors are present in different brain neurons including cell nuclei, in addition to non-nuclear sites such as mitochondria, dendrites, glial cells, and neuronal synapses. These receptors are located in several central nervous system regions including hypothalamus, hippocampus, amygdala, and the brain stem. Through these receptors, estrogen modulates the neural plasticity as well as signaling pathways such as neurotransmitters and neuromodulators systems including serotonergic, dopaminergic, glutamatergic, noradrenergic, and opioidergic systems. All of which can exert an influence on mood and overall well-being;22 however, no definitive answer has been obtained.
Rates of depression were higher in women using hormonal contraceptive methods in comparison to non-hormonal birth control methods in the present study. The rate of moderate to severe depression was 30.6% in the hormonal contraception group compared to 25.8% in the group using non-hormonal contraceptives. Furthermore, hormonal group has 1.267 times higher risk to develop moderate to severe depression compared to non-hormonal contraceptive methods’ users. These results were higher than the rates of depression amongst Saudi population, which were 20%, 6.2% and 3.2% for moderate, moderately severe and severe depression, respectively.23 This could be explained by the increased levels of monoamine oxidase following external progestins intake, leading to serotonin degradation and thus occurrence of depression.24 Moreover, clinical studies showed that changes of estrogen levels in women with depression risk factors could trigger depressive episodes.25
Three review studies done in 2018, 2020, and 2021 have established that there was no clear association between hormonal contraceptive methods and depression.2,13,26 Interestingly, an observational study published in 2013 on 6654 young women showed that hormonal methods can, in fact, reduce the levels of depressive symptoms.20
On the other hand, other studies have suggested that the development of depressive disorders can be a side effect of hormonal contraceptive methods use.4,9,12 A nation-wide cohort prospective analysis including over a million Danish women that were followed up for a mean of 6.4 years concluded that the use of hormonal contraceptive methods was associated with the development of clinical depression and use of antidepressants.9 However, some argued that the study did not include the outcome of non-hormonal contraceptive methods.27 In addition, although the study had addressed the demographic and clinical factors, the results could be due to unrecognized patient-related factors.27
Local studies have also shown some limitations. A cross-sectional study was done in Jazan province, Saudi Arabia, in 2017 and concluded that 43.3% of hormonal birth control methods users suffered from depressive disorder. This had indicated high depression rates in hormonal contraceptive methods users, with the highest rate being mild depression with 21.6%, and the least rates being severe and extreme depression with 7.5% and 3.1%, respectively.12 However, this study did not exclude women who had a previous history of depression or antidepressants use.
Another cross-sectional study conducted in Jeddah, 2016, concluded that mood swings and depression were the most common adverse effects of contraceptive methods reported with a percentage of 34.6%.4 However, it was not clarified whether the latter percentage only included women who were using hormonal methods or not. Moreover, this study did not mention which questionnaire has been used for depression screening. In addition, there was no comparison of hormonal vs non-hormonal birth control methods and their associated depressive disorder percentages.
In the current study, there is a high prevalence of depressive disorders risk factors reported by our participants. These are previous diagnosis with psychiatric disorders (18.2%), previous diagnosis with physical illnesses (15.9%), history of substance use (7.2%), and depressogenic medications use (25.7%). This is consistent with the study conducted in Jazan in 2017, in which physical illness, history of depression, and smoking were all significantly associated with depression in addition to some risk factors that have not been studied here such as social support and relationship with the husband.11 The previous paper and another national Danish study have studied the relationship between socio-demographic data and depression development in women using hormonal contraception. They found that adolescence, minimal social support, presence of living problems in the past two months, an uncomfortable marital status, and contraceptive type were associated with increased risk of depression development.9,12 However, in our study, we only considered the previously mentioned risk factors as they have been approved in the literature as risk factors for depression in our area.
Several limitations were notable in our study despite the fact that a wide range of confounders were controlled. As our study was an observational one, residual confounders such as use of depressogenic medications were not excluded from the study sample which might affect the results. Furthermore, our data were self-reported by using an online questionnaire which can lead to recall bias and misunderstanding of some questions. In addition, there was no breakdown of the different hormonal methods associated with depression as well as missing one question of the PHQ-9 survey which might affect the results of the study. Finally, our data lacked information on pill formulation, doses and compliance with medications. We recommend prospective cohort studies that address depression association with different hormonal contraception types, doses, formulations and compliance which enable researchers to follow up the participants from the earliest stage and reduce any possible confounder. The generalizability of the results is applicable only for women who have not been diagnosed with depression, as our questions were targeting women with no history of depression.
Conclusion
Our study provides insight about the association between depression and hormonal contraceptive methods. We conclude that hormonal contraceptive methods increase the risk of moderate to severe depression by 1.267 times compared to non-hormonal methods. Furthermore, we noticed a positive association between depression and risk factors mentioned earlier in this study. Due to the importance of this topic and its controversy, we recommend further studies to be directed in this field. In addition, since we noticed high prevalence of depression risk factors in our study, we emphasize on the importance of screening females prior to the prescription of hormonal contraceptives.
Abbreviations
IUD, intrauterine device; OCPs, oral contraceptive pills; IRB, Institutional Review Board; PHQ9, Patient Health Questionnaire-9; SR, Saudi Riyals; N, number.
Acknowledgments
The efforts of our data collectors are greatly appreciated. Many thanks to Dr Ahmad N. AlHadi et al for the provision of the translated PHQ-9 upon request.
Disclosure
Our study complies with the Declaration of Helsinki and the authors report no conflicts of interest in this work.
References
1. New Zealand family planning [homepage on the internet]. Benefits of contraception use - family planning; 2013. Available from: https://www.familyplanning.org.nz/news/2013/benefits-of-contraception-use.
2. Fruzzetti F, Fidecicchi T. Hormonal contraception and depression: updated evidence and implications in clinical practice. Clin Drug Investig. 2020;40(12):1097–1106. doi:10.1007/s40261-020-00966-8
3. Cooper DB, Patel P, Mahdy H. Oral contraceptive pills. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2022.
4. Alhusain F, Alkaabba F, Alhassan N, et al. Patterns and knowledge of contraceptive methods use among women living in Jeddah, Saudi Arabia. Saudi J Health Sci. 2018;7(2):121–126. doi:10.4103/sjhs.sjhs_8_18
5. Abdel-Salam DM, Albahlol IA, Almusayyab RB, et al. Prevalence, correlates, and barriers of contraceptive use among women attending primary health centers in Aljouf Region, Saudi Arabia. Int J Environ Res Public Health. 2020;17(10):3552. doi:10.3390/ijerph17103552
6. Elgharabawy R, Ahmed A, Alsuhaibani R. Awareness, Prevalence and determinants of birth control methods use among women in Saudi Arabia. Int Arch Med. 2015;8(245):e34.
7. Halbreich U, Kahn LS. Role of estrogen in the aetiology and treatment of mood disorders. CNS Drugs. 2001;15(10):797–817. [PubMed: 11602005]. doi:10.2165/00023210-200115100-00005
8. Ehsanpour S, Aghaii A, Kheirabadi GR. The association of contraceptive methods and depression. Iran J Nurs Midwifery Res. 2012;17(3):234–238.
9. Skovlund CW, Mørch LS, Kessing LV, Lidegaard Ø. Association of hormonal contraception with depression. JAMA Psychiatry. 2016;73(11):1154–1162. doi:10.1001/jamapsychiatry.2016.2387
10. Skovlund CW, Mørch LS, Kessing LV, Lange T, Lidegaard Ø. Association of hormonal contraception with suicide attempts and suicides. Am J Psychiatry. 2018;175(4):336–342. doi:10.1176/appi.ajp.2017.17060616
11. Hughes LD, Majekodunmi O. Hormonal contraception and suicide: a new dimension of risk. Br J Gen Pract. 2018;68(676):512–513. doi:10.3399/bjgp18X699473
12. Alfaifi M, Najmi AH, Swadi KH, Almushtawi AA, Jaddoh SA. Prevalence of contraceptive use and its association with depression among women in the Jazan province of Saudi Arabia. J Family Med Prim Care. 2021;10(7):2503–2511. doi:10.4103/jfmpc.jfmpc_1308_20
13. Worly BL, Gur TL, Schaffir J. The relationship between progestin hormonal contraception and depression: a systematic review. Contraception. 2018;97(6):478–489. doi:10.1016/j.contraception.2018.01.010
14. Pagano HP, Zapata LB, Berry-Bibee EN, Nanda K, Curtis KM. Safety of hormonal contraception and intrauterine devices among women with depressive and bipolar disorders: a systematic review. Contraception. 2016;94(6):641–649. doi:10.1016/j.contraception.2016.06.012
15. Razzak HA, Harbi A, Ahli S. Depression: prevalence and associated risk factors in the United Arab Emirates. Oman Med J. 2019;34(4):274–282. doi:10.5001/omj.2019.56
16. Kulkarni J. Perimenopausal depression - an under-recognised entity. Aust Prescr. 2018;41(6):183–185. doi:10.18773/austprescr.2018.060
17. Johnson D, Dupuis G, Piche J, Clayborne Z, Colman I. Adult mental health outcomes of adolescent depression: a systematic review. Depress Anxiety. 2018;35(8):700–716. doi:10.1002/da.22777
18. General Authority for Statistics [homepage in the Internet]. Population estimate; 2021. Available from: https://www.stats.gov.sa/en/43.
19. AlHadi AN, AlAteeq DA, Al-Sharif E, et al. An Arabic translation, reliability, and validation of patient health questionnaire in a Saudi sample. Ann Gen Psychiatry. 2017;16:32. doi:10.1186/s12991-017-0155-1
20. Keyes KM, Cheslack-Postava K, Westhoff C, et al. Association of hormonal contraceptive use with reduced levels of depressive symptoms: a national study of sexually active women in the United States. Am J Epidemiol. 2013;178(9):1378–1388. doi:10.1093/aje/kwt188
21. Kuehner C. Why is depression more common among women than among men? Lancet Psychiatry. 2017;4(2):146–158. doi:10.1016/S2215-0366(16)30263-2
22. McEwen BS, Akama KT, Spencer-Segal JL, Milner TA, Waters EM. Estrogen effects on the brain: actions beyond the hypothalamus via novel mechanisms. Behav Neurosci. 2012;126(1):4–16. doi:10.1037/a0026708
23. Alyami HS, Naser AY, Dahmash EZ, Alyami MH, Alyami MS. Depression and anxiety during the COVID-19 pandemic in Saudi Arabia: a cross-sectional study. Int J Clin Pract. 2021;75(7):e14244. doi:10.1111/ijcp.14244
24. Klaiber EL, Broverman DM, Vogel W, Peterson LG, Snyder MB. Individual differences in changes in mood and platelet monoamine oxidase (MAO) activity during hormonal replacement therapy in menopausal women. Psychoneuroendocrinology. 1996;21(7):575–592. PMID: 9044441. doi:10.1016/s0306-4530(96)00023-6
25. Payne JL. The role of estrogen in mood disorders in women. Int Rev Psychiatry. 2003;15(3):280–290. PMID: 15276966. doi:10.1080/0954026031000136893
26. Buggio L, Barbara G, Facchin F, Ghezzi L, Dridi D, Vercellini P. The influence of hormonal contraception on depression and female sexuality: a narrative review of the literature. Gynecol Endocrinol. 2022;38(3):193–201. doi:10.1080/09513590.2021.2016693
27. Chesney E. Hormonal contraception and its association with depression. JAMA Psychiatry. 2017;74(3):302. doi:10.1001/jamapsychiatry.2016.3703
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.