")
Back to Journals » Journal of Pain Research » Volume 17
Humoral Cytokine Levels in Patients with Herpes Zoster: A Meta-Analysis
Received 1 December 2023
Accepted for publication 26 February 2024
Published 5 March 2024 Volume 2024:17 Pages 887—902
DOI https://doi.org/10.2147/JPR.S449211
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Michael A Ueberall
Jiayu Yue,1,2 Ming Yao2
1The Second Affiliated Hospital & Yuying Children’s Hospital of Wenzhou Medical University/The Second School of Medicine, Wenzhou Medical University, Wenzhou City, Zhejiang, People’s Republic of China; 2Department of Anesthesiology and Pain Research Center, The First Hospital of Jiaxing or the Affiliated Hospital of Jiaxing University, Jiaxing City, Zhejiang, People’s Republic of China
Correspondence: Ming Yao, Email [email protected]
Background: The neurocutaneous disease caused by the reactivation of varicella-zoster virus (VZV) is called herpes zoster (HZ). The virus remains in the spinal cord back root after the chickenpox disappears. Diminished immune function can reactivate VZV, causing severe neuropathic pain that can last for months or even years, leading to postherpetic neuralgia (PHN), which severely affects the patient’s quality of life. Much literature compares various cytokine levels in the body fluids HZ and PHN patients; however, no studies comprehensively evaluate them.
Methods: The Cochrane Library, PubMed, Web of Science, and Medline were screened for studies on cytokine levels in body fluids of HZ and PHN patients in the English language. Healthy individuals were selected as the control group, and the standardized mean difference (SMD) between the case and control groups was imputed using a fixed-effects or random-effects model and expressed as a 95% confidence interval (CI). The Newcastle-Ottawa Scale (NOS) was used to assess article quality.
Results: This meta-analysis included 13 articles with 1373 participants. Compared with the control group, the HZ group had significantly higher levels of interleukin (IL)-4, IL-6, IL-10, Hcy, and C-reactive protein (CRP), whereas the levels of CD3+ T and CD4+ T lymphocytes were reduced. Additionally, PHN patients had significantly higher levels of IL-6 and IL-1β compared with the control group.
Conclusion: This meta-analysis provides compelling evidence that CRP, Hcy, IL-1β, IL-4, IL-6, IL-8, and IL-10 are associated with the genesis and development of HZ and PHN. These markers can be used to improve the diagnosis and treatment of these diseases.Furthermore, for making the results more convincing, it is necessary to harmonize sample acquisition techniques and analytical methods and also require larger, more rigorously designed studies with broader subgroups and sex/age-matched controls.
Keywords: herpes zoster, varicella-zoster virus, neurocutaneous disease, postherpetic neuralgia, biomarker
Introduction
Herpes zoster (HZ) is a disease characterized by skin blisters and nerve pain. When the immune system is compromised, latent varicella-zoster virus (VZV) reactivates in the back root ganglia of the spinal nerve. Age and immunosuppression are the main risk factors of HZ. Approximately one-third of people are at risk for HZ in their lifetime, and nearly half of people ≥ 85 years old develop HZ.1,2 Zoster-related pain can be classified into acute HZ neuralgia (AHN; within 1 month after the rash) or subacute (SHN; within 3 months after the rash) HZ neuralgia, and postherpetic neuralgia (PHN; more than three months after the rash).3 The main symptom of PHN is severe and persistent pain, mostly in HZ-infected areas such as the chest, abdomen, face, or neck. The pain can be described as a stabbing, burning, tingling, or electric shock sensation and is often unbearable in severity.4,5
The etiopathogenesis of HZ is not well known; however, several studies have indicated that it may be associated with immune system dysfunction,6 impaired oxidative status,7 and neuroinflammatory response.8 These factors can be determined using biomarkers, such as CRP, interleukins, lymphocytes, and antioxidant factors. Impaired immune function is closely related to the onset and progression of HZ.9 Lymphocytes crucially modulate viral infections, and their depletion is associated with viral reactivation.10 Oxidative stress and inflammation cause tissue damage, and redox regulation is involved in activating or inhibiting the inflammatory response during cellular stress.11 Pathogen invasion disrupts the body’s redox state, causing oxidative stress and promoting inflammation of skin cells, blood, and the central nervous system (CNS).12 However, the body’s natural antioxidants can counteract the damage caused by oxidative stress-related factors.13 Inflammation depletes antioxidants as they are consumed for the elimination of excess free radicals.14 C-reactive proteins (CRP) are biomarkers of systemic inflammation15 and modulate inflammation development and enhance the prevalence of chronic inflammatory and cardiovascular diseases.16 The relative stability of proinflammatory and anti-inflammatory cytokines contributes to the homeostasis of the inflammatory system, and their dysregulation can lead to PHN. Increased pro-inflammatory cytokine levels such as interleukin (IL)-6, IL-8, and tumor necrosis factor (TNF) have been associated with immune response in infants, elevated blood pressure, and target organ damage.17 Furthermore, anti-inflammatory factors such as IL-4 and IL-10 reduce the generation of pro-inflammatory factors and mitigate the inflammatory reaction.18
Currently, the treatment of HZ is based on medication and surgery, which mainly includes antiviral drugs, nutritive nerve drugs and painkillers, etc. Surgical treatments include nerve blocks, implantation of epidural analgesic pumps and radiofrequency ablation, etc. In recent years, many studies have suggested that the use of the HZ vaccine also has an impact on HZ. In recent years, the number of people vaccinated against shingles has also been expanding, but its effectiveness is still the subject of much controversy. In conclusion, the treatment and management of HZ remains a worldwide challenge.
Although some studies have emphasized the alterations in cytokine during HZ and PHN, the outcomes have varied, which may be because of the variations in patient characteristics, samples, or specific assays used. Therefore, a systematic approach to analyzing these studies is required. This meta-analysis aimed to provide a systematic and quantitative assessment of the existing data on cytokines in HZ and PHN.
Materials and Methods
This study adhered to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) checklist and the Cochrane Handbook for Systematic Reviews and Meta-Analyses19 and has been registered in PROSPERO (Registration number: CRD42023464039).
Data Sources and Search Strategy
Two investigators independently searched the Cochrane Library, PubMed, Web of Science, and MEDLINE databases. The search strategy included a combination of keywords and Medical Subject Headings (MeSH): herpes zoster OR shingles OR postherpetic neuralgia) AND (inflammation OR inflammations OR innate inflammatory response OR innate inflammatory responses OR cytokine OR biomarker OR chemokine) AND (cohort studies OR case-control studies OR comparative study OR risk factors OR cohort OR compared OR groups OR case-control OR multivariate).
Selection Criteria
Inclusion criteria: 1) Studies that assessed the cytokine levels in body fluids of HZ or PHN diagnosed patients, 2) were in English language, and 3) 5 or more cases were included.
Exclusion criteria: 1) Studies lacking valid data, 2) were performed on animals, 3) were meta-analyses, case reports, letters, reviews, meeting abstracts, and posters, 4) lacked full text, and 5) included controls with any other disease were excluded.
Data Extraction and Quality Assessment
Two authors screened the data independently according to a predetermined spreadsheet. The acquired data included study information (article title, year of publication, study design), participant characteristics (number of participants, age, proportion of females), sample characteristics (sample type and method of analysis), biomarkers measured, and the mean and standard deviation (SD) of the biomarkers examined.
The Newcastle-Ottawa Scale was used to measure each study’s quality. Quality assessment criteria included: (1) selection of cases and controls: A. definition of cases; B. representativeness of these cases; C. selection of control systems; D. comparability of cases and controls; (2) comparability: comparability of cases and controls based on design or analysis; (3) exposure: A. determination of exposure status; B. same determination method for case and control groups; C. non-response rate. Table 1 indicates the evaluated results. The star allocation range for each parameter was from 0 (lowest) to 9 (highest). Studies with a score of ≥ 7 were considered high-quality studies, while others were classified as medium-quality.20
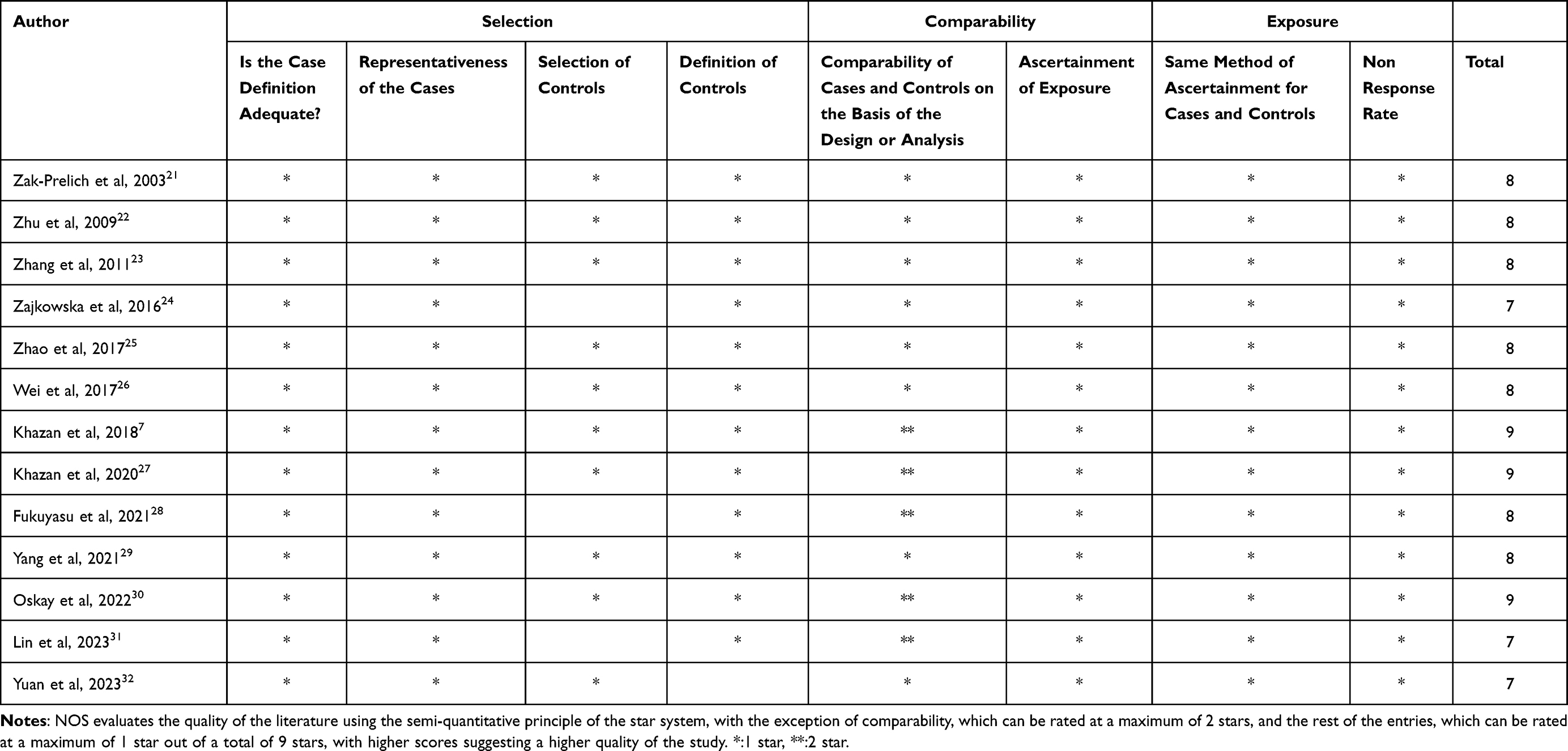 |
Table 1 Quality Assessments and Risk of Bias of Observational Studies |
Data Synthesis and Analysis
All data were converted to mean and standard deviation.33,34 All variables were analyzed with a standardized mean difference (SMD) and 95% confidence intervals (CI). Cochran’s Q test was performed to gauge heterogeneity, whereas to identify the degree of consistency, I² statistic was carried out: I² > 75% = high, > 50% = moderate, and < 25% = low inconsistency. Using a random-effects model, the size of the combined effect was estimated when heterogeneity was > 50%; otherwise, a fixed-effects model was used.35 A two-tailed p-value < 0.05 was considered statistically significant. A full assessment of publication bias was not performed because of the small number of studies in each comparison (< 10). All statistical analyses were performed using Review Manager 5.4.1.
Results
Literature Search
Figure 1 indicates the detailed search information. In total, 1720 documents were acquired from the Cochrane Library, PubMed, Web of Science, and Medline. All searchable articles were included in the EndNote database for searching. Finally, 13 studies that met the selection criteria were selected.
 |
Figure 1 PRISMA flow diagram. |
Study Characteristics
Table 2 lists basic information about the included studies. A total of 13 articles, which comprised 1373 contributors, were included in this study. All studies compared the levels of cytokines between HZ or PHN patients and control individuals. Of these 13 studies, 8 directly compared HZ patients with control groups, 1 categorized HZ patients into severe and mild groups based on clinical manifestations, 1 grouped HZ patients into groups with a duration of < 7 and > 7 days, 1 divided HZ patients into pre- and post-treatment groups, 2 directly compared PHN patients with control groups, and 1 categorized PHN patients into severe and mild groups based on pain scores.
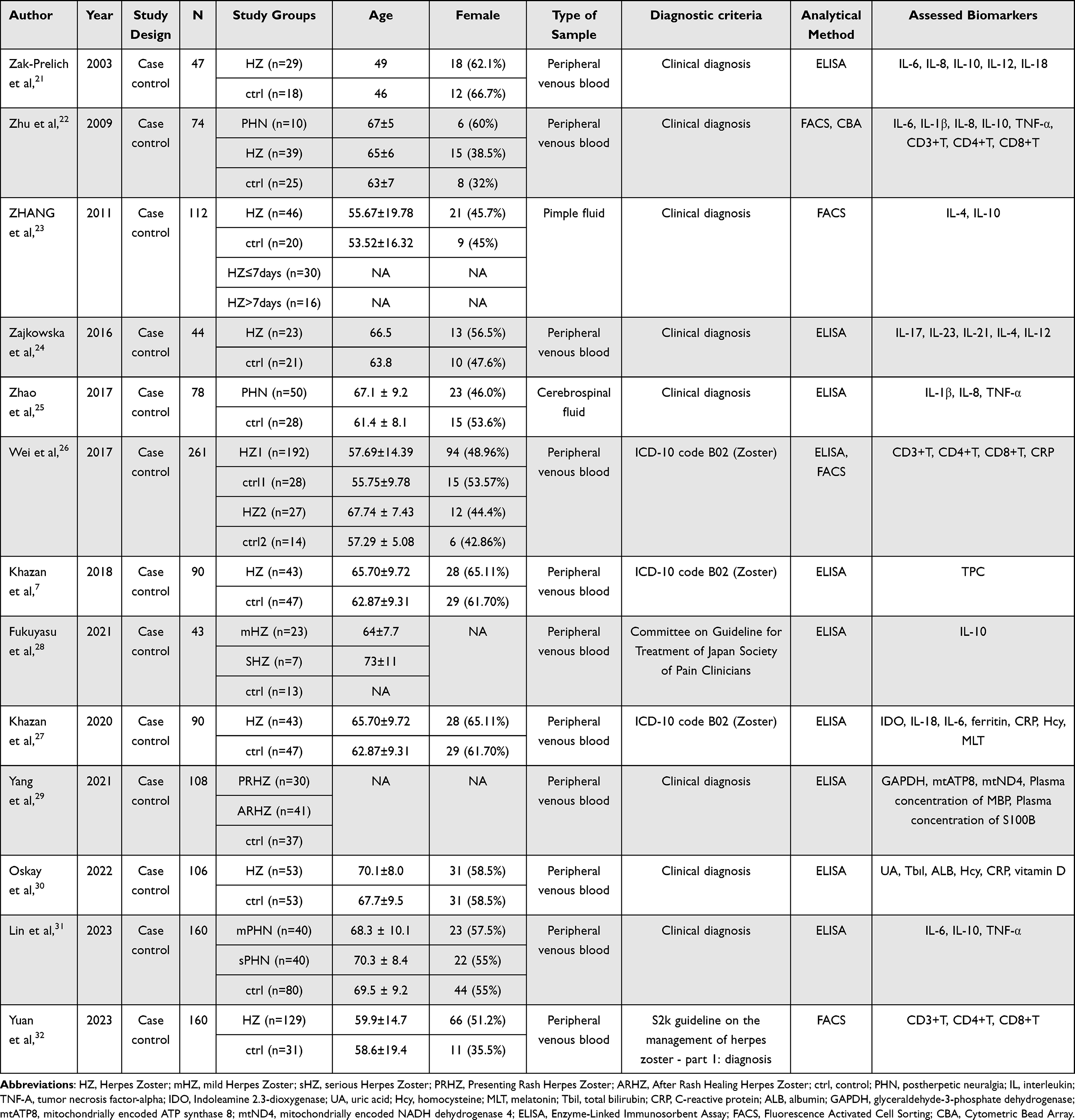 |
Table 2 Basic Information About the Included Studies |
Each study’s levels of cytokines were assessed. The samples included peripheral venous blood, blister fluid, and cerebrospinal fluid, and the detection methods used were ELISA (Enzyme-Linked Immunosorbent Assay), FACS (Fluorescence-Activated Cell Sorting), and CBA (Cytometric Bead Array).
Quality Assessments and Risk of Bias
The quality scores of the included studies ranged from 7 to 9, reflecting the robustness of the different research approaches. Three studies, two by Marjan Khazan et al7,27 and one by Tuba Oskay et al,30 scored the highest with 9 points, indicating that they had good quality methods and low risk of bias. Seven studies had a high-quality score of 8, indicating representative cases, appropriate selection and definition of controls, good comparability between cases and controls, and sound and reliable study methodology and data analysis. Three other remaining studies scored 7 because of the minor flaws in the selection of controls or comparability based on design or analyses (Table 2).
Comparison of Cytokine Levels in Patients with HZ
CRP
Sufficient data was acquired from 4 comparative groups comprising 457 participants, which indicated a significant difference in CRP levels between the HZ group and the control group. The CRP levels in HZ patients were significantly higher than in the control group (SMD = 4.48; 95% CI: 1.38 to 7.59; p = 0.005; Figure 2A). Furthermore, there was significant heterogeneity within the groups (I² = 99%; p < 0.00001), which was resolved after excluding the studies by Wei et al,26 and Oskay et al.30 However, the effect size remained significant (SMD = 1.52, 95% CI: 1.12 to 1.92, p < 0.00001).
 |
Figure 2 Forest plot of differences in each cytokine between HZ patients and controls. (A) CRP; (B) IL-4; (C) IL-6; (D) IL-8; (E) IL-10; (F) IL-12; (G) IL-18; (H) CD3+T cell; (I) CD4+T cell; (J) CD8+T cell; (K) Hcy. |
IL-4
The IL-4 levels were also extracted from four control groups, totaling 196 individuals. The pooled effect sizes showed that IL-4 levels significantly differed between the HZ group and the control group (SMD = 5.28; 95% CI: 3.01 to 7.55; p < 0.00001; Figure 2B). The subgroup was highly heterogeneous (I² = 93%; p < 0.00001), and the sensitivity analysis could not resolve the heterogeneity.
IL-6
A total of 201 samples were included in the three comparison, and the fixed-effects model revealed a significant difference in IL-6 levels between the HZ and other groups, with HZ patients indicating higher IL-6 levels (SMD = 0.92; 95% CI: 0.63 to 1.22; p < 0.00001; Figure 2C). The combined data were homogeneous (I² = 0%; p = 0.38).
IL-8
Two studies with 111 participants reported IL-8 levels, and no significant differences were observed in IL-8 levels between HZ patients and controls (SMD = 1.10; 95% CI: −0.10 to 2.31; p = 0.07; Figure 2D). Moreover, high levels of heterogeneity were detected (I² = 88%; p = 0.004), and sensitivity analysis could not resolve this heterogeneity.
IL-10
A study of 319 individuals comprising seven comparisons and random-effects meta-analysis indicated significant differences in IL-10 levels between the case and control groups. The HZ patients had significantly higher IL-10 levels than healthy individuals (SMD = 1.10; 95% CI: 0.64 to 1.56; p < 0.00001; Figure 2E). To resolve high heterogeneity (I² = 70%; p = 0.003), the study by Zak Prelich et al21 was excluded (heterogeneity after removal I² = 31%; p = 0.20), and the effect size remained significant (SMD = 1.24; 95% CI: 0.90 to 1.58; p < 0.00001).
IL-12
Random effects modeling in two studies showed no significant difference in IL-12 levels between HZ patients and controls (SMD = 0.50; 95% CI: −0.11 to 2.31; p = 0.11; Figure 2F). Furthermore, moderate levels of heterogeneity were detected (I² = 51%; p = 0.16), which was not resolved by the sensitivity analysis.
IL-18
Two studies comprising 111 individuals assessed IL-18 levels, and the results indicated no significant difference in IL-18 levels between the two groups (SMD = 0.58; 95% CI: −0.59 to 1.75; p = 0.33; Figure 2G). Additionally, a high degree of heterogeneity was found (I2 = 90%; p = 0.002) but could not be resolved by sensitivity analysis.
CD3+T Cells
Data were extracted from three comparisons with a sample size of 444 cases. The random effects model indicated no significant differences in the levels of CD3+ T cells between HZ patients and controls. (SMD = −3.16; 95% CI: −7.59 to 0.37; p = 0.08; Figure 2H). However, this result had high heterogeneity (I² = 99%; p < 0.00001), which was resolved by excluding the study by Wei et al.26 After resolving the heterogeneity, the CD3+T cell concentration was found to be lower in the HZ patients than in the controls (SMD = −0.78; 95% CI: −1.47 to −0.08; p = 0.03).
CD4+T Cell
The pooled results of samples from the three control groups showed that the CD4+ T cell levels in the HZ group were not comparable to the control group (SMD = −3.43; 95% CI: −7.30 to 0.43; p = 0.08; Figure 2I). However, this result had high heterogeneity (I2 = 99%, p < 0.00001), which was addressed by excluding Wei et al.26 The CD4+ T cell concentration in the HZ group was significantly reduced compared to the control group after resolving the heterogeneity (SMD = −0.62, 95% CI: −0.93 to −0.03, p = 0.0001).
CD8+T Cell
A study of three control groups revealed no significant differences in CD8+ cell levels in body fluids between patients and healthy individuals (SMD = −3.26; 95% CI: −7.31 to 0.79; p = 0.11; Figure 2J). However, this result had a high degree of heterogeneity, which could not be resolved (I² = 99%; p < 0.00001).
HCY
Fixed-effects modeling obtained from 196 samples showed that Hcy concentrations were significantly higher in the HZ patients than the control group (SMD = 1.43; 95% CI: 1.11 to 1.74; p < 0.00001; Figure 2K), and the merged data are homogeneous (I² = 0%; p = 0.51).
Comparison of Cytokine Levels in Patients with PHN
IL-1β
IL-1β levels were extracted from two control groups, including 113 participants. The fixed-effects modeling revealed substantially higher IL-1β concentrations in the PHN group than the control group (SMD = 0.50; 95% CI: 0.10 to 0.90; p = 0.01; Figure 3A), and the heterogeneity was almost non-existent (I² = 0%; p = 0.65).
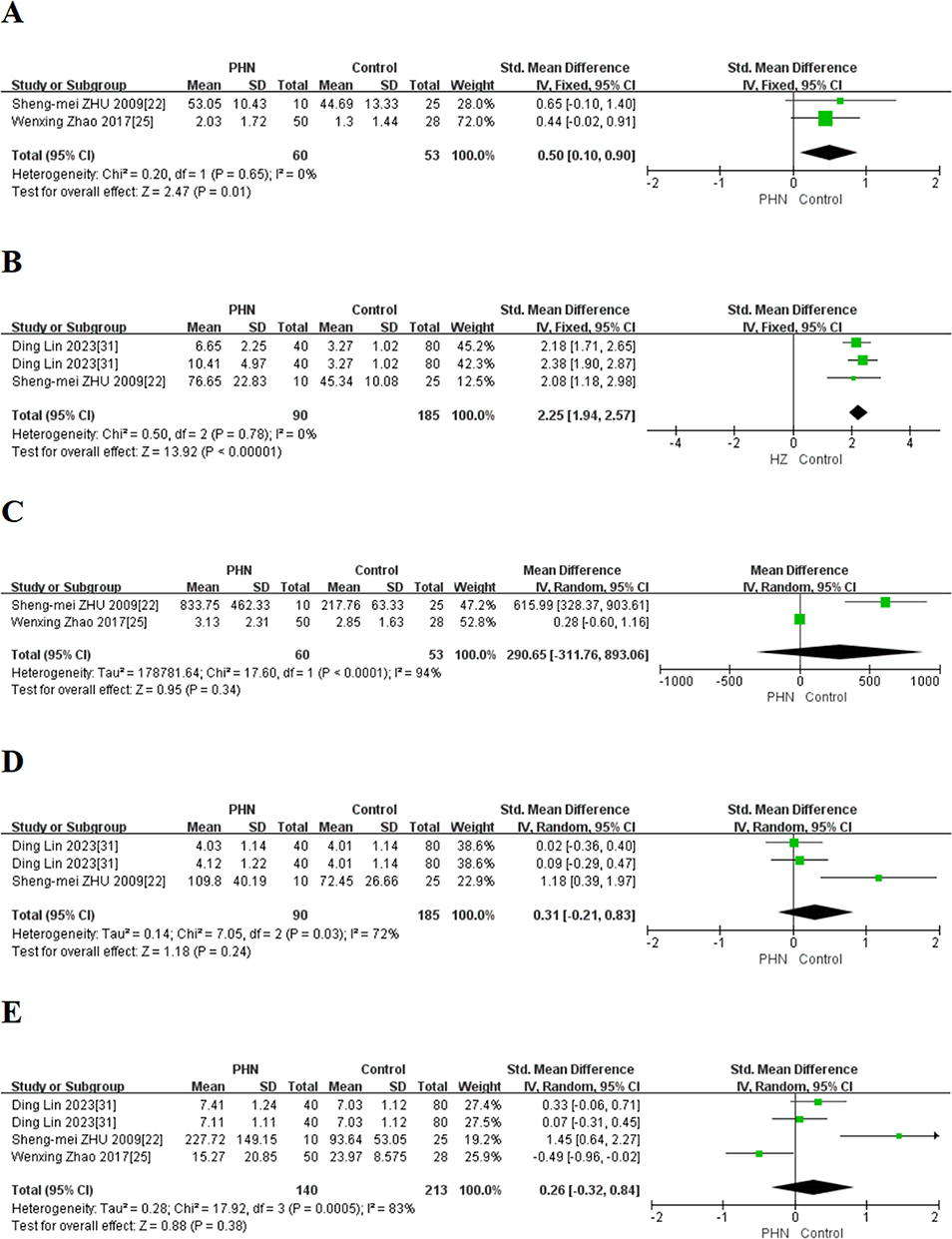 |
Figure 3 Forest plot of differences in each cytokine between PHN patients and controls. (A) IL-1β; (B) IL-6; (C) IL-8; (D) IL-10; (E) TNF-α. |
IL-6
A fixed-effects meta-analysis of 3 contrasting groups comprising 275 participants showed that IL-6 concentrations were significantly higher in the PHN group compared to the control group (SMD = 2.25; 95% CI: 1.94 to 2.57; p < 0.00001; Figure 3B). The combined data were homogeneous (I² = 0%; p = 0.78).
IL-8
Two comparisons, including 113 participants, performed a random-effects meta-analysis to assess the levels of IL-8 levels and revealed that its levels in body fluids were the same in both groups (SMD = 290.65; 95% CI: −311.76 to 893.06; p = 0.34; Figure 3C). However, the high heterogeneity could not be resolved by sensitivity analysis (I² = 94%; p < 0.0001).
IL-10
A three-group comparison of 275 samples provided data indicating that the PHN group had the same IL-10 concentration as the control group (SMD = 0.31; 95% CI: −0.21 to 0.83; p = 0.24; Figure 3D). The heterogeneity for this result was moderate (I2 = 72%; p = 0.03) and could not be resolved through sensitivity analysis.
TNF-α
From 4 sets of comparisons, the levels of TNF-α in the body fluids obtained from 113 participants were assessed, which showed that TNF-α levels were similar between PHN patients and healthy individuals (SMD = 0.26; 95% CI: −0.32 to 0.84; p = 0.38; Figure 3E). The heterogeneity for this result was high (I2 = 83%; p = 0.0005) and could not be resolved by sensitivity analysis.
Results of Individual Studies
Xin Yang et al29 found that during the occurrence of HZ and after its cure, the HZ group had significantly higher levels of GAPDH, mtATP8, mtND4, and plasma concentration of MBP and S100B compared to the control group. Furthermore, according to Marjan Khazan et al,7,27 compared to controls, the HZ group had significantly higher levels of IDO and ferritin and lower levels of MLT and TPC. These differences were statistically significant. Zajkowska et al24 also found that HZ patients had higher levels of IL-17, IL-21, and IL-23 compared to healthy individuals.Additionally, Tuba Oskay et al30 indicated that the HZ group had significantly lower levels of UA, Tbil, and albumin than the control group. These differences were also statistically significant.
Discussion
The reactivation of the primary VZV infection causes shingles. After the original infection, the virus may remain latent in the dorsal root or cranial ganglia, and its reactivation causes characteristic nerve pain and blister-like rash.36 Several underlying mechanisms, including immune suppression, pro-inflammatory and anti-inflammatory factors dysregulation, and imbalanced oxidative stress and antioxidant levels, have been associated with VZV reinfection. Assessing the patient’s cytokines alterations can provide preliminary insights into the pathogenesis of HZ. Different assays and sample types often affect cytokine expression, leading to inconsistent results. Meta-analysis integrates information, removes the effects of confounding factors, and provides reliable outcomes. Furthermore, different stages and disease severity can alter cytokine levels differently. Therefore, this investigation analyzed all the subgroups.
Neuroinflammation is a complex biological process that has an essential role in various neurological conditions and increases the secretion of various inflammatory mediators.37 Here, HZ patients indicated significantly higher CRP, IL-4, IL-6, and IL-10 levels than controls. IL-6 is an early tissue damage marker associated with chronic inflammatory and immune-mediated diseases.38,39 Moreover, it is essentially associated with abnormal pain perception and hyperalgesia following peripheral nerve injury in rodents.40 Furthermore, enhanced IL-6 transcription and expression are observed on the surface of herpes viruses infected newborn skin.41 However, the pathological role of IL-6 in virus-induced inflammatory diseases remains unknown. IL-10 inhibits macrophage-specific immune function, potentiates immune induction, inhibits inflammatory cytokine release from macrophages, and diminishes the expression of adhesion molecules, thus playing an essential role in immune-mediated processes in humans. The source of IL-10 in HZ patients is still unclear, and regulatory T cells have been suspected as one of its sources.42 Furthermore, studies suggest that IL-10 gene polymorphisms may be associated with susceptibility to HZ.43 IL-4 is produced by Th2, eosinophils, and mast cells and has a wide range of biological effects. Excessive IL-4 production is associated with inflammation and autoimmune disorders.44 Under inflammatory conditions, acute-phase proteins are stimulated and produced by pro-inflammatory cytokines such as IL-6. CRP is an important acute-phase protein marker and is significantly elevated, especially in infectious and inflammatory diseases. The elevated levels of pro-inflammatory cytokines accompanied by an increase in anti-inflammatory cytokines and CRP stimulation by pro-inflammatory cytokines might explain the observed results.45,46
Elevated levels of Hcy may act as a potential factor that enhances oxidative stress and alters inflammatory status, causing endothelial dysfunction and promoting chronic inflammation development.47–49 Additionally, Hcy is not only a pro-inflammatory factor but also an anti-inflammatory factor. Furthermore, its high levels are closely associated with vitamin B12 and folate deficiencies, which are major cofactors in Hcy metabolism and are influenced by dietary intake.50 The elevated Hcy levels in HZ patients may result from oxidative stress, inflammatory reactions, and deficiency in folate, vitamin B12, or both.
Studies have shown that in the pathogenesis of HZ, the body’s defense primarily relies on cellular immune responses, and the function of T lymphocyte subsets is crucial for maintaining normal immune function.32 The literature has confirmed the presence of cellular immune abnormalities in HZ patients, particularly specific cellular immune suppression. The number of specific T cells against VZV gradually decreases as the age increases.51,52 CD3+ T cells are markers of mature T cells in peripheral blood, while CD4+ T cells help activate B and cytotoxic T cells and induce their antibody production to activate macrophages. Studies have shown that a significant decrease in CD3+T and CD4+T cells in peripheral blood leads to severe impairment of autoimmune function,53 consistent with the results of this study.
Complications occur in 5–30% of people with HZ, and PHN is the most common of these complications. PHN is defined as pain that persists for > 3 months after HZ onset and is usually accompanied by sensory deficits and sensory irregularities that can be disabling or even fatal as the disease progresses.54 PHN pathogenesis is complex and may result from a combination of factors such as nerve injury, immune activation, and genetic predisposition, all of which may cause chronic pain onset and persistence. VZV predominantly infects sensory nerve fibers, leading to inflammation and neuronal impairment. This damage sensitizes the nerves, promoting the transmission of painful signals, even after the virus has been removed from the body.55–57 Immune activation also produces inflammatory molecules that injure nerve cells and cause persistent pain. Furthermore, chronic inflammation alters how the CNS processes pain signals; in the case of HZ lesions, the pain persists even after the lesions have healed.57–59 In addition, genetic factors are also critically associated with pathogenesis, and several researches have indicated specific genetic variants associated with an elevated risk of PHN, suggesting a genetic predisposition to the condition.60–62
When cells are damaged, infected, or invaded, and inflammation occurs, monocytes, macrophages, and other non-immune cells, such as fibroblasts and endothelial cells, release a cytokine called interleukin-1 beta (IL-1β). Recent literature has revealed that injured dorsal root ganglion (DRG) neurons also express IL-1β.63 Its expression increases in peripheral nerves after compression injury and in the CNS microglia and astrocytes after trauma.64,65 Furthermore, IL-1β promotes the production of neuropeptide substance P and prostaglandin E2 (PGE2) in many neurons and glial cells.63,66 It can also inhibit glutamate clearance between synapses by glial cells.67 Additionally, an in-vivo study suggested that IL-1β is involved in neurodevelopment.68 In conclusion, the onset and progression of PHN may be closely associated with IL-1β, as evidenced by this meta-analysis.
This investigation also suggests distinct discrepancies in IL-6 levels between PHN patients and healthy individuals. Previous studies have found increased IL-6 and its receptor expression in spinal cord tissue following peripheral nerve injury. An animal study showed that injection of IL-6 into normal rats inhibited their response to thermal and mechanical stimuli. Even with the preserved pain response to mechanical stimuli, IL-6 injection could suppress pain response to heat stimuli. Thus, IL-6 is an important factor in persistent pain caused by peripheral and CNS injuries.69,70
The above studies suggest these cytokines may be used for HZ and PHN diagnosis and prognosis. Although there is substantial heterogeneity among the included research, sensitivity analyses can effectively verify the results. The main sources of heterogeneity are classification criteria, sample type, analytical techniques, and possible individual differences in the included research. For the classification criteria, among the 13 included articles, Atsuko Fukuyasu et al28 followed the criteria of the Committee on Guideline for Treatment of Japan Society of Pain Clinicians,71 Li Wei et al26 and Marjan Khazan et al7 used the ICD-10 code B02 (Zoster) criteria, and Yanrong Yuan et al32 used the S2k guideline on the management of HZ-part 1: diagnosis.72 Patients were clinically diagnosed in the remaining 9 articles without specifying which diagnostic criteria were used. Previously, it has been indicated that different types and levels of cytokines are found in different body fluids.73 In this literature, one study23 used blister fluid as a sample, and another25 used cerebrospinal fluid. Since different analysis techniques can result in different cytokine levels,74 ELISA for quantitative analysis of large samples, FACS for multi-parameter analysis and cell sorting at the single-cell level, and CBA for quantitative analysis of multiple cytokines or markers were used in the included studies.
This meta-analysis showed no significant differences in IL-8, IL-12, IL-18, and CD8+ T cell levels between the HZ and healthy cohort or that of IL-8, IL-10, and TNF-α between the PHN and healthy cohort.
The study by Wenxing Zhao et al25 used cerebrospinal fluid rather than peripheral venous blood as samples, which may explain the inconsistency in the results of TNF-α and IL-8 with other studies. ShenMei Zhu et al22 used different analytical methods, which may be the reason for the higher heterogeneity and inability to resolve it through sensitivity analysis in the comparison of IL-8 and CD8+ T cells in the HZ group. The data from the study of Zak Prelich et al21 had a large standard deviation for IL-8, IL-10, IL-12, and IL-18, indicating significant individual differences in the included study samples, which may have resulted in insignificant differences in these cytokines between the HZ and controls groups. Therefore, the data of these studies should be interpreted carefully. Among the reported studies, Ding Lin et al31 found no significant difference in IL-10 levels between PHN and control groups, which is inconsistent with the studies of ShenMei Zhu et al22 and Wei Chen et al75 and the reason for the difference may be due to the use of different analytical methods. Yanrong Yuan et al32 reported that CD8+ T cells did not show a remarkable difference between the two groups, which may be because 129 patients were included in the case group while only 31 patients were included in the control group, causing an insufficient statistical test.
Furthermore, the study by Zak Prelich et al21 included younger subjects, with an average age of 49 years in the case group and 46 in the control group. The literature reported by Xin Yang29 did not specify the age of the included cases, and the same samples were used in the two Khazan et al articles;7,27 no independent validation was performed, which might have caused biased results. In one study,28 the queue size involved was relatively small, with 30 patients in the case group and only 7 in the control group. This would affect the credibility of the obtained cytokine levels and cause an inability to conduct statistical tests. The included researchers did not group diseases for most studies, which we believe is flawed.
Limitation
1) There was a significant degree of heterogeneity in some of the included studies, and while sensitivity analyses can address this in some cases, the impact of heterogeneity on the reliability and utility of the results must be carefully assessed and considered. 2) The comprehensive analysis of publication bias was impossible because of the relatively small number of studies included in each comparison. Although tools such as funnel plots or Egger regression tests are commonly used to assess publication bias in such cases, these tests are often considered unreliable or insignificant for < 10 studies. Therefore, there is a possibility of publication bias in this meta-analysis. 3) Due to insufficient relevant data, the association between the above cytokines and disease severity or subgroup analyses was performed. 4) Non-English and other gray literature were excluded.
Conclusions
This meta-analysis provides compelling evidence that CRP, Hcy, IL-1β, IL-4, IL-6, IL-8, and IL-10 are associated with the genesis and development of HZ and PHN. These markers can be used to improve the diagnosis and treatment of these diseases.Furthermore, for making the results more convincing, it is necessary to harmonize sample acquisition techniques and analytical methods and also require larger, more rigorously designed studies with broader subgroups and sex/age-matched controls.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mbinta JF, Wang AX, Nguyen BP, et al. Herpes zoster vaccine effectiveness against herpes zoster and postherpetic neuralgia in New Zealand: a retrospective cohort study. Lancet Reg Health West Pac. 2023;31:100601. doi:10.1016/j.lanwpc.2022.100601
2. Irigoyen-Mansilla VM, Gil-Prieto R, Gea-Izquierdo E, et al. Hospitalization burden related to herpes zoster infection during the COVID-19 pandemic in Spain (2020-2021). Hum Vaccin Immunother. 2023;19(2):2256047. doi:10.1080/21645515.2023.2256047
3. Liu L, Zhang W-J, Xu S-X, et al. Propensity score matching comparing short-term nerve electrical stimulation to pulsed radiofrequency for herpes zoster-associated pain: a retrospective study. Front Mol Neurosci. 2022;15:1069058. doi:10.3389/fnmol.2022.1069058
4. Wen SY, Chao OY, Catherine KA, et al. Impact of type 1 versus type 2 diabetes on developing herpes zoster and post-herpetic neuralgia: a population-based cohort study. Acta Derm Venereol. 2023;103:adv9400. doi:10.2340/actadv.v103.9400
5. Pei J, Tian Y, Ye W, et al. A novel recombinant ORF7-siRNA delivered by flexible nano-liposomes inhibits varicella zoster virus infection. Cell Biosci. 2023;13(1):167. doi:10.1186/s13578-023-01108-1
6. de Oliveira Gomes J, Gagliardi AM, Andriolo BN, et al. Vaccines for preventing herpes zoster in older adults. Cochrane Database Syst Rev. 2023;10(10):Cd008858. doi:10.1002/14651858.CD008858.pub5
7. Khazan M, Hedayati M, Robati RM, et al. Impaired oxidative status as a potential predictor in clinical manifestations of herpes zoster. J Med Virol. 2018;90(10):1604–1610. doi:10.1002/jmv.25204
8. Thomsen MM, Tyrberg T, Skaalum K, et al. Genetic variants and immune responses in a cohort of patients with varicella zoster virus encephalitis. J Infect Dis. 2021;224(12):2122–2132. doi:10.1093/infdis/jiab254
9. Boeren M, Meysman P, Laukens K, et al. T cell immunity in HSV-1- and VZV-infected neural ganglia. Trends Microbiol. 2023;31(1):51–61. doi:10.1016/j.tim.2022.07.008
10. Jin W, Fang M, Sayin I, et al. Differential CD4+ T-Cell cytokine and cytotoxic responses between reactivation and latent phases of herpes zoster infection. Pathog Immun. 2022;7(2):171–188. doi:10.20411/pai.v7i2.560
11. Dery KJ, Wong Z, Wei M, et al. Mechanistic insights into alternative gene splicing in oxidative stress and tissue injury. Antioxid Redox Signal. 2023. doi:10.1089/ars.2023.0437
12. Dobrzyńska M, Moniuszko-Malinowska A, Skrzydlewska E. Metabolic response to CNS infection with flaviviruses. J Neuroinflammation. 2023;20(1):218. doi:10.1186/s12974-023-02898-4
13. Yang X, Liu X, Nie Y, et al. Oxidative stress and ROS-mediated cellular events in RSV infection: potential protective roles of antioxidants. Virol J. 2023;20(1):224. doi:10.1186/s12985-023-02194-w
14. Vatner SF, Zhang J, Oydanich M, et al. Healthful aging mediated by inhibition of oxidative stress. Ageing Res Rev. 2020;64:101194. doi:10.1016/j.arr.2020.101194
15. Hage FG. C-reactive protein and hypertension. J Hum Hypertens. 2014;28(7):410–415. doi:10.1038/jhh.2013.111
16. Yao Z, Zhang Y, Wu H. Regulation of C-reactive protein conformation in inflammation. Inflamm Res. 2019;68(10):815–823. doi:10.1007/s00011-019-01269-1
17. Pioli MR, de Faria AP. Pro-inflammatory cytokines and resistant hypertension: potential for novel treatments? Curr Hypertens Rep. 2019;21(12):95. doi:10.1007/s11906-019-1003-2
18. Sapartini G, Wong GWK, Indrati AR, et al. The association between vitamin d, interleukin-4, and interleukin-10 levels and CD23+ expression with bronchial asthma in stunted children. Biomedicines. 2023;11(9):2542. doi:10.3390/biomedicines11092542
19. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:n71. doi:10.1136/bmj.n71
20. Wells G, Shea B, O’Connell D, et al. The Newcastle-Ottawa Scale (NOS) for Assessing the Quality of Nonrandomised Studies in Meta-Analyses. Liverpool, UK: University of Liverpool; 2011.
21. Zak-Prelich M, Mckenzie RC, Sysa-Jedrzejowska A, et al. Local immune responses and systemic cytokine responses in zoster: relationship to the development of postherpetic neuralgia. Clin Exp Immunol. 2003;131(2):318–323. doi:10.1046/j.1365-2249.2003.02061.x
22. Zhu SM, Liu Y-M, An E-D, et al. Influence of systemic immune and cytokine responses during the acute phase of zoster on the development of postherpetic neuralgia. J Zhejiang Univ Sci B. 2009;10(8):625–630. doi:10.1631/jzus.B0920049
23. Zhang M, Wu N, Yang L, et al. Study on the T-helper cell 1/2 cytokine profile in blister fluid of patients with herpes zoster and its clinical significance. J Dermatol. 2011;38(12):1158–1162. doi:10.1111/j.1346-8138.2011.01289.x
24. Zajkowska A, Garkowski A, Świerzbińska R, et al. Evaluation of chosen cytokine levels among patients with herpes zoster as ability to provide immune response. PLoS One. 2016;11(3):e0150301. doi:10.1371/journal.pone.0150301
25. Zhao W, Wang Y, Fang Q, et al. Changes in neurotrophic and inflammatory factors in the cerebrospinal fluid of patients with postherpetic neuralgia. Neurosci Lett. 2017;637:108–113. doi:10.1016/j.neulet.2016.11.041
26. Wei L, Zhao J, Wu W, et al. Decreased absolute numbers of CD3(+) T cells and CD8(+) T cells during aging in herpes zoster patients. Sci Rep. 2017;7(1):15039. doi:10.1038/s41598-017-15390-w
27. Khazan M, Nasiri S, Riahi SM, et al. Measurement of melatonin, indole-dioxygenase, IL-6, IL-18, ferritin, CRP, and total homocysteine levels during herpes zoster. J Med Virol. 2020;92(8):1253–1259. doi:10.1002/jmv.25484
28. Fukuyasu A, Kamata M, Sy Hau C, et al. Serum interleukin-10 level increases in patients with severe signs or symptoms of herpes zoster and predicts the duration of neuralgia. J Dermatol. 2021;48(4):511–518. doi:10.1111/1346-8138.15818
29. Yang X, Shen Y, Ding Z, et al. Circulating level of myelin basic protein predicts postherpetic neuralgia: a prospective study. Clin J Pain. 2021;37(6):429–436. doi:10.1097/AJP.0000000000000937
30. Oskay T, Keskin C, Özen M. Antioxidant and inflammatory biomarkers in herpes zoster. J Med Virol. 2022;94(8):3924–3929. doi:10.1002/jmv.27781
31. Lin D, Zhong C, Jiang Q, et al. Serum interleukin-6 levels are increased in post-herpetic neuralgia: a single-center retrospective study. An Bras Dermatol. 2023;98(2):202–207. doi:10.1016/j.abd.2022.03.007
32. Yuan Y, Zhang Y, Wang J, et al. Immune changes and their relationship with prognosis in patients with varicella-zoster virus encephalitis/meningitis. Am J Transl Res. 2023;15(2):1421–1429.
33. Wan X, Wang W, Liu J, et al. Estimating the sample mean and standard deviation from the sample size, median, range and/or interquartile range. BMC Med Res Methodol. 2014;14:135. doi:10.1186/1471-2288-14-135
34. McGrath S, Zhao X, Steele R, et al. Estimating the sample mean and standard deviation from commonly reported quantiles in meta-analysis. Stat Methods Med Res. 2020;29(9):2520–2537. doi:10.1177/0962280219889080
35. Higgins JP, Thompson SG, Deeks JJ, et al. Measuring inconsistency in meta-analyses. BMJ. 2003;327(7414):557–560. doi:10.1136/bmj.327.7414.557
36. Le P, Rothberg M. Herpes zoster infection. BMJ. 2019;364:k5095. doi:10.1136/bmj.k5095
37. Stöberl N, Maguire E, Salis E, et al. Human iPSC-derived glia models for the study of neuroinflammation. J Neuroinflammation. 2023;20(1):231. doi:10.1186/s12974-023-02919-2
38. Tanaka T, Narazaki M, Kishimoto T. IL-6 in inflammation, immunity, and disease. Cold Spring Harb Perspect Biol. 2014;6(10):a016295. doi:10.1101/cshperspect.a016295
39. Yoshida Y, Tanaka T. Interleukin 6 and rheumatoid arthritis. Biomed Res Int. 2014;2014:698313. doi:10.1155/2014/698313
40. Arruda JL, Sweitzer S, Rutkowski MD, et al. Intrathecal anti-IL-6 antibody and IgG attenuates peripheral nerve injury-induced mechanical allodynia in the rat: possible immune modulation in neuropathic pain 11 Published on the world wide web on 28 August 2000. Brain Res. 2000;879(1–2):216–225. doi:10.1016/S0006-8993(00)02807-9
41. Jarosinski KW, Carpenter JE, Buckingham EM, et al. Cellular stress response to varicella-zoster virus infection of human skin includes highly elevated interleukin-6 expression. Open Forum Infect Dis. 2018;5(6):ofy118. doi:10.1093/ofid/ofy118
42. Xing Q, Hu D, Shi F, et al. Role of regulatory T cells in patients with acute herpes zoster and relationship to postherpetic neuralgia. Arch Dermatol Res. 2013;305(8):715–722. doi:10.1007/s00403-013-1367-0
43. Cho JW, Shin DH, Lee KS. Polymorphism of the IL-10 gene is associated with susceptibility to herpes zoster in Korea. J Dermatol Sci. 2007;45(3):213–215. doi:10.1016/j.jdermsci.2006.11.004
44. Akdis M, Burgler S, Crameri R, et al. Interleukins, from 1 to 37, and interferon-γ: receptors, functions, and roles in diseases. J Allergy Clin Immunol. 2011;127(3):701–21. doi:10.1016/j.jaci.2010.11.050
45. Gruys E, Toussaint MJM, Niewold TA, et al. Acute phase reaction and acute phase proteins. J Zhejiang Univ Sci B. 2005;6(11):1045–1056. doi:10.1631/jzus.2005.B1045
46. Sproston NR, Ashworth JJ. Role of C-reactive protein at sites of inflammation and infection. Front Immunol. 2018;9:754. doi:10.3389/fimmu.2018.00754
47. Pushpakumar S, Kundu S, Sen U. Endothelial dysfunction: the link between homocysteine and hydrogen sulfide. Curr Med Chem. 2014;21(32):3662–3672. doi:10.2174/0929867321666140706142335
48. Sharma M, Tiwari M, Tiwari RK. Hyperhomocysteinemia: impact on neurodegenerative diseases. Basic Clin Pharmacol Toxicol. 2015;117(5):287–296. doi:10.1111/bcpt.12424
49. Zahedi AS, Daneshpour MS, Akbarzadeh M, et al. Association of baseline and changes in adiponectin, homocysteine, high-sensitivity C-reactive protein, interleukin-6, and interleukin-10 levels and metabolic syndrome incidence: Tehran lipid and glucose study. Heliyon. 2023;9(9):e19911. doi:10.1016/j.heliyon.2023.e19911
50. Shemirani F, Titcomb TJ, Saxby SM, et al. Association of serum homocysteine, folate, and vitamin B(12) and mood following the Swank and Wahls elimination dietary interventions in relapsing-remitting multiple sclerosis: secondary analysis of the WAVES trial. Mult Scler Relat Disord. 2023;75:104743. doi:10.1016/j.msard.2023.104743
51. Vukmanovic-Stejic M, Sandhu D, Seidel JA, et al. The characterization of varicella zoster virus-specific T cells in skin and blood during aging. J Invest Dermatol. 2015;135(7):1752–1762. doi:10.1038/jid.2015.63
52. Ku CC, Besser J, Abendroth A, et al. Varicella-Zoster virus pathogenesis and immunobiology: new concepts emerging from investigations with the SCIDhu mouse model. J Virol. 2005;79(5):2651–2658. doi:10.1128/JVI.79.5.2651-2658.2005
53. Jiménez M, Fernández‐Naval C, Navarro V, et al. Kinetics of cellular and humoral immunogenicity and effectiveness of SARS-CoV −2 booster vaccination in hematologic neoplasms. Am J Hematol. 2023;98(8):1204–1213. doi:10.1002/ajh.26951
54. Liang X, Fan Y. Bidirectional two-sample Mendelian randomization analysis reveals a causal effect of interleukin-18 levels on postherpetic neuralgia risk. Front Immunol. 2023;14:1183378. doi:10.3389/fimmu.2023.1183378
55. Gershon AA, Gershon MD, Breuer J, et al. Advances in the understanding of the pathogenesis and epidemiology of herpes zoster. J Clin Virol. 2010;48(Suppl 1):S2–7. doi:10.1016/S1386-6532(10)70002-0
56. Forstenpointner J, Rice ASC, Finnerup NB, et al. Up-date on clinical management of postherpetic neuralgia and mechanism-based treatment: new options in therapy. J Infect Dis. 2018;218(suppl_2):S120–s126. doi:10.1093/infdis/jiy381
57. Li H, Li X, Wang J, et al. Pain-related reorganization in the primary somatosensory cortex of patients with postherpetic neuralgia. Hum Brain Mapp. 2022;43(17):5167–5179. doi:10.1002/hbm.25992
58. Fan X, Ren H, Bu C, et al. Alterations in local activity and functional connectivity in patients with postherpetic neuralgia after short-term spinal cord stimulation. Front Mol Neurosci. 2022;15:938280. doi:10.3389/fnmol.2022.938280
59. Peng Q, Guo X, Luo Y, et al. Dynamic Immune Landscape and VZV-Specific T cell responses in patients with herpes zoster and postherpetic neuralgia. Front Immunol. 2022;13:887892. doi:10.3389/fimmu.2022.887892
60. Anosike UG, Ouko I, Mwaura AW, et al. Phenotypes and genotypes in postherpetic neuralgia drug therapy: a narrative mini-review. Clin J Pain. 2022;38(8):536–540. doi:10.1097/AJP.0000000000001045
61. Nishizawa D, Iseki M, Arita H, et al. Genome-wide association study identifies candidate loci associated with chronic pain and postherpetic neuralgia. Mol Pain. 2021;17:1744806921999924. doi:10.1177/1744806921999924
62. Xing X, Bai Y, Sun K, et al. Identification of candidate genes associated with postherpetic neuralgia susceptibility. Pain Physician. 2020;23(3):E281–e288.
63. Tiwari V, Hemalatha S. Sida cordifolia L. attenuates behavioral hypersensitivity by interfering with KIF17-NR2B signaling in rat model of neuropathic pain. J Ethnopharmacol. 2023;319(Pt 1):117085. doi:10.1016/j.jep.2023.117085
64. Sheu ML, Pan L-Y, Yang C-N, et al. Neuronal death caused by HMGB1-evoked via inflammasomes from thrombin-activated microglia cells. Int J Mol Sci. 2023;24(16):12664. doi:10.3390/ijms241612664
65. Koop MA, Sleijser-Koehorst MLS, Hooijmans CR, et al. The potential protective effects of pre-injury exercise on neuroimmune responses following experimentally-induced traumatic neuropathy: a systematic review with meta-analysis. Front Immunol. 2023;14:1215566. doi:10.3389/fimmu.2023.1215566
66. Wan S, Chen Q, Xiang Y, et al. Interleukin-1 increases cyclooxygenase-2 expression and prostaglandin E2 production in human granulosa-lutein cell via nuclear factor kappa B/P65 and extracellular signal-regulated kinase 1/2 signaling pathways. Mol Cell Endocrinol. 2023;566–567:111891. doi:10.1016/j.mce.2023.111891
67. Laughlin TM, Bethea JR, Yezierski RP, et al. Cytokine involvement in dynorphin-induced allodynia. Pain. 2000;84(2–3):159–167. doi:10.1016/S0304-3959(99)00195-5
68. Liao Z, Zhu Q, Huang H. Involvement of IL-1β-mediated necroptosis in neurodevelopment impairment after neonatal sepsis in rats. Int J Mol Sci. 2023;24(19):14693. doi:10.3390/ijms241914693
69. Xu X, Liu Z, Liu H, et al. The effects of galanin on neuropathic pain in streptozotocin-induced diabetic rats. Eur J Pharmacol. 2012;680(1–3):28–33. doi:10.1016/j.ejphar.2012.01.011
70. Yang XM, He RG. 牛痘疫苗致炎兔皮提取物治疗老年带状疱疹后遗神经痛及对血清IL-6的影响 [Effect of extracts from rabbit skin inflamed by vaccinia virus in the management of postherpetic neuralgia and on serum interleukin-6 level in aged patients]. Nan Fang Yi Ke Da Xue Xue Bao. 2007;27(12):1941–1943. Chinese.
71. Committee for the Development of Pain Clinic Treatment Guidelines, Japan Pain Clinic Society. Treatment CoGf. J Jpn Soc Pain Clin. 2010;17:S55–S134.
72. Werner RN, Nikkels AF, Marinović B, et al. European consensus-based (S2k) Guideline on the Management of Herpes Zoster – guided by the European Dermatology Forum (EDF) in cooperation with the European Academy of Dermatology and Venereology (EADV), Part 1: diagnosis. J Eur Acad Dermatol Venereol. 2017;31(1):9–19. doi:10.1111/jdv.13995
73. Liu C, Chu D, Kalantar‐Zadeh K, et al. Cytokines: from clinical significance to quantification. Adv Sci. 2021;8(15):e2004433. doi:10.1002/advs.202004433
74. De Preter V. Metabolomics in the clinical diagnosis of inflammatory bowel disease. Dig Dis. 2015;33(1):2–10. doi:10.1159/000437033
75. Chen W, Zhu L, Shen -L-L, et al. T lymphocyte subsets profile and toll-like receptors responses in patients with herpes zoster. J Pain Res. 2023;16:1581–1594. doi:10.2147/JPR.S405157
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.