")
Back to Journals » Journal of Pain Research » Volume 17
Identifying Risk Factors for Cardiovascular Events Among Active-Duty Service Members and Veterans Prescribed Nonsteroidal Anti-Inflammatory Drugs (NSAIDs)
Authors Forbes WL, Petway J, Gressler LE, Thorfinnson H, Costantino RC, Atkinson TJ
Received 14 October 2023
Accepted for publication 1 March 2024
Published 15 March 2024 Volume 2024:17 Pages 1133—1144
DOI https://doi.org/10.2147/JPR.S440802
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Erica Wegrzyn
Whitney L Forbes,1 Justin Petway,2 Laura E Gressler,3 Hannah Thorfinnson,4 Ryan C Costantino,1,5 Timothy J Atkinson2,6
1Enterprise Intelligence and Data Solutions Program Management Office, Program Executive Office, Defense Healthcare Management Systems, Rosslyn, VA, USA; 2Department of Pharmacy, VA Tennessee Valley Healthcare System, Nashville, TN, USA; 3Division of Pharmaceutical Evaluation and Policy, College of Pharmacy, University of Arkansas for Medical Sciences, Little Rock, AR, USA; 4Department of Pharmacy, James A. Haley Veteran’s Hospital, Tampa, FL, USA; 5Department of Military and Emergency Medicine, Uniformed Services University of the Health Sciences, Bethesda, MD, USA; 6Pain Management, Opioid Safety, PDMP (PMOP) National Program Office, Department of Veterans Affairs, Washington, DC, USA
Correspondence: Timothy J Atkinson; Laura E Gressler, Email [email protected]; [email protected]
Background: Oral NSAIDs are widely used analgesic medications for the treatment of musculoskeletal and inflammatory conditions. NSAIDs are associated with adverse effects that arise from COX enzyme inhibition including cardiovascular events. The combined role of patient and prescription factors associated with NSAID use on cardiovascular risk is not well characterized.
Objective: The purpose of this study is to identify the risk factors with cardiovascular events among NSAID users.
Methods: This study is a retrospective, nested case–control study, within the DAVINCI database, among active-duty service members and veterans with at least one NSAID pharmacy claim between fiscal year (FY) 2015-FY2020. Inclusion criteria individuals ≥ 18 years of age received a prescription NSAID for ≥ 7-day supply and a duration ≥ 1 month overall. Cases experienced nonfatal myocardial infarction, nonfatal stroke, or new onset heart failure. Ten controls were selected per case. Risk factors were identified through logistic regression modeling.
Results: The risk factors with strongest association to the primary outcome included age starting at 45 up to 75 and older, the first 90 days of NSAID exposure, cerebrovascular disease, cardiomyopathy, and history of myocardial infarction. Cox-selectivity and dose did not appear to be clinically significant in their association with cardiovascular events.
Conclusion: The results of this study indicate that age, initial NSAID exposure, and comorbidities are more predictive than NSAID-specific factors such as COX-selectivity and dose. The results provide the framework for development of a risk score to improve prediction of NSAID-associated cardiovascular events.
Keywords: NSAID, cardiovascular, myocardial infarction, stroke, heart failure
Introduction
Oral nonsteroidal anti-inflammatory drugs (NSAIDs) have been the cornerstone of treatment for arthritis and inflammatory conditions for over a hundred years, making them one of the most utilized classes of medications worldwide.1 NSAIDs are associated with significant adverse effects characterized primarily by gastrointestinal (GI) ulceration/bleeding and cardiovascular events, including myocardial infarction and cerebrovascular disease.2 While the risk of GI ulceration/bleeding is well studied with mitigation and prevention strategies available, there remains a dearth of evidence to assess NSAID-related risk prior to a cardiovascular event and guide clinical recommendations for prevention and mitigation strategies.3–7 Studies evaluating NSAID-related cardiovascular risk have focused on COX selectivity, dose-dependent effects, and duration of NSAID therapy with variable and often conflicting results.8–13
Cardiovascular disease (CVD) remains a leading cause of morbidity and mortality worldwide, accounting for nearly 17.9 million deaths annually, representing 31% of all global deaths. CVD encompasses conditions such as myocardial infarction, stroke, and heart failure. Numerous studies have highlighted the prevalence of CVD and its associated risk factors.14 Well-established risk factors for cardiovascular disease include hypertension, dyslipidemia, smoking, obesity, diabetes mellitus, sedentary lifestyle, and family history of CVD.15 Several guidelines recommend avoidance of NSAIDs due to their potential adverse effects.16–19 However, NSAIDs remain first-line medications for many common pain conditions, making avoidance impractical without clear guidance regarding the magnitude of the risk factors most strongly associated with cardiovascular events.20–29 Furthermore, NSAIDs are critical non-opioid pharmacotherapy options serving as reasonable alternatives to opioid therapy for many chronic pain conditions in the midst of the opioid overdose crisis.30,31
This study is a collaboration between clinicians from the Veterans Health Administration (VHA) and the health science outcomes research group from the Department of Defense (DoD). This study aims to investigate the impact of demographics, comorbidities, and NSAID-specific risk factors on cardiovascular outcomes associated with NSAID use. Through this collaboration, we leverage the comprehensive databases of both the VA/DoD, which represents a more demographically diverse cohort and improves generalizability of outcomes. This study lays the groundwork for development of a risk index to improve predictability of cardiovascular events associated with NSAID use.
Methods
Study Design and Data Source
A retrospective case control leveraging the DAVINCI (Data Analysis and Visualization Initiative) data was used to identify the factors associated with cardiovascular events among patients who received an NSAID. DAVINCI is a collaborative effort between the Department of Defense (DoD) and the Veterans Health Administration (VHA) within the Department of Veterans Affairs (VA) in the US.32 The DAVINCI database integrates and analyzes various types of health data, including electronic health records (EHRs), administrative data, and clinical data from both the DoD and the VA using Observational Medical Outcomes Partnership (OMOP) common data models. More specifically, the clinical records include information regarding healthcare visits, conditions, dispensed drugs, and procedures in both the inpatient and outpatient settings. By combining these datasets, researchers and healthcare providers can gain a more comprehensive understanding of the health outcomes and healthcare utilization of military personnel, veterans, and their families, examine the long-term effects of military service, and evaluate the effectiveness of different interventions and treatments.
Study Cohort
Individuals with at least one NSAID pharmacy claim with a days’ supply greater than 7 days between October 1, 2016 and September 30, 2020 were identified in the DAVINCI national administrative healthcare database. The authors determined that requiring a days’ supply greater than 7 days effectively removed many short-term prescriptions from being associated with distant CV events while recognizing that previous studies indicated that CV risk may be significant within the first 30 days.6,11,33 NSAIDs were identified by national drug codes. Individuals under the age of 18, with missing sex, or missing race variables were excluded.
Matching and Index Date Assignment
The first occurrence of a cardiovascular event was the primary outcome of interest. A cardiovascular event included a non-fatal myocardial infarction, non-fatal stroke, and new onset of heart failure and was defined using the International Classification of Disease, 10th Revision, Clinical Modification (ICD10-CM) codes listed in Supplementary Table 1. All-cause mortality data was not included because it was not specific to cardiovascular disease and confounding could not be controlled. Cases were defined as individuals with at least one NSAID pharmacy claim with a days’ supply greater than 7 days during the study period and a subsequent claim for a cardiovascular event. The date of the first identified event for a cardiovascular event following a qualifying NSAID pharmacy prescription during the study period served as the index date. Controls were defined as individuals with at least one NSAID pharmacy claim with a days’ supply greater than 7 days during the study period and no subsequent claim for a cardiovascular event during the study period. For each case, 10 control patients were randomly assigned. The index date of the case was assigned to each of the 10 control patients it was matched to. To ensure that included individuals were regular users of TRICARE or VHA health services, individuals were required to have a recorded encounter in the 180 to 365 days prior to their identified or assigned index date.
Covariates
Baseline demographic variables were collected in the 180 days prior to the index date. These variables included age, sex, and race. Baseline comorbidity and prescription use measures were selected based on their known association with the receipt of an NSAID and/or the outcome. Comorbidity measures included diabetes,15 hypertension,15 dyslipidemia,15 history of myocardial infarctions,14 arthritis or spondylitis,34 peripheral artery disease,15 chronic kidney disease,14 atherothrombotic disease,14 history of tobacco use,15 cerebrovascular disease,15 coronary artery disease,15 cardiomyopathy,14 obstructive sleep apnea (OSA),14 liver dysfunction,14 and chronic obstructive pulmonary disease (COPD).14 Prescription use measures included the use of aspirin and other anticoagulants. NSAID-specific drug information included was active ingredient, selectivity9,10,35,36 (Cox 1, Cox 2, and non-selective), dosage10,13,33,35 (low/medium and high dose), and time since initial exposure6,13,33,35 (≤30, 31–90, 91–180, 181–365, 366–730, 731+, and no exposure) (see Supplementary Table 1 for ICD-10 codes used for all predefined risk factors).
Statistical Analyses
Descriptive and bivariate analyses were conducted using means, medians, interquartile range, and frequencies. Chi-squared tests were conducted for categorical variables, and t-tests were conducted for continuous variables to compare the characteristics among the identified cases and controls. Conditional multivariable logistic regression was used to calculate to explore the role of factors potentially associated with a cardiovascular event. All baseline demographic, comorbidity, prescription use, and NSAID-specific drug information covariates were included in the regression model. Odds ratios (ORs), 95% confidence intervals (CIs), and p-values were calculated to evaluate the presence and strength of the associations between the covariates and the primary composite outcome. Subgroup analyses evaluated the role of covariates on the risk of the individual conditions (non-fatal myocardial infarction, non-fatal stroke, and new onset heart failure) that make up the composite primary outcome. Additionally, the primary model was run combining active ingredient and dose as a factor in the model. A 5% significance level was used for all analyses. Model discrimination was assessed using the c-statistic, area under the curve (AUC), and receiver operating characteristic curve (ROC) measure.37 All analyses were conducted on a patient level. All statistical analyses were performed using R. This study followed the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) reporting guideline.38 This study was determined to be exempt by the Defense Health Agency Institutional Review Board.
Results
We identified 237,852 patients with a claim of a cardiovascular event (myocardial infarction, non-fatal cerebrovascular accident, or new heart failure) during the study period. During the study period, 231,967 patients had a pharmacy claim for an NSAID and encounter data for at least 6 months prior to the cardiovascular event (index date). Among those who received an NSAID prescription from VA/DoD during the study period, 2,319,670 patients without cardiovascular events who met selection criteria (see Figure 1) were assigned as controls.
 |
Figure 1 Consort diagram. |
Descriptive Analysis
Median age of cases was 69 and controls 49. As shown in Table 2, cases were more likely than controls to be older, black or other than white race, or male sex.
 |
Table 1 Diagnostic Codes for Cardiovascular Events and Predefined Risk Factors |
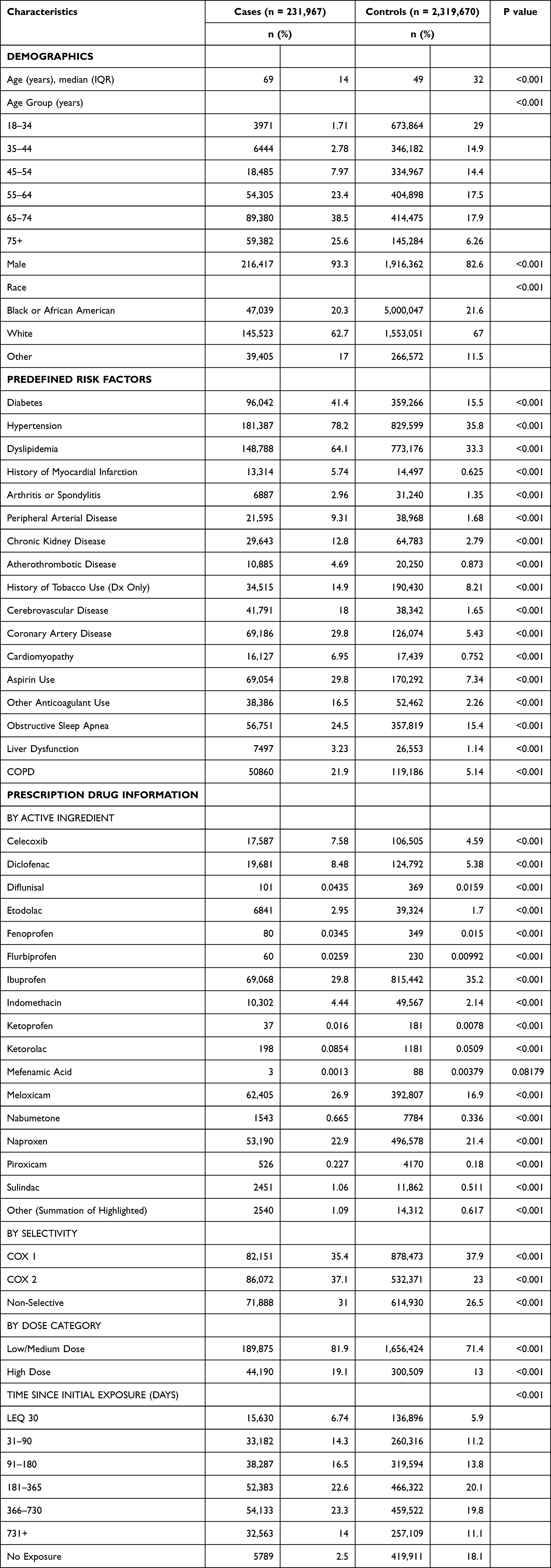 |
Table 2 Baseline Demographics & Predefined Risk Factors |
Compared with controls, patients with cardiovascular events were more likely to have high disease burdens. As shown in Table 1, cases had significantly higher frequency of diagnosed conditions including diabetes, hypertension, dyslipidemia, arthritis, peripheral artery disease, chronic kidney disease, atherothrombotic disease, history of tobacco use, coronary artery disease, cardiomyopathy, obstructive sleep apnea, chronic obstructive pulmonary disease (COPD), and liver dysfunction. In addition to disease comorbidity, cases also reported higher frequency of previous cardiovascular events specifically history of myocardial infarction and cerebrovascular accident.
VA/DoD prescription data indicated a higher percentage of cases receiving aspirin and anticoagulants compared to controls. COX-2 and non-selective NSAIDs were prescribed more often in cases, but COX-1 selective NSAIDs were prescribed more often in controls driven by ibuprofen which was prescribed more frequently in controls. All other individual NSAIDs were prescribed more frequently in cases including celecoxib, diclofenac, etodolac, indomethacin, meloxicam, naproxen, piroxicam, sulindac, and several others with low prescription counts for both cases and controls. NSAIDs were prescribed more frequently across low/medium and high doses tracked.
Multivariable Analysis
The logistic regression model for the dichotomous outcome of NSAID-related composite cardiovascular event or myocardial infarction, nonfatal cerebrovascular accident, and new heart failure resulted in multiple, independent, statistically significant associations. History of heart failure was removed from the composite outcome as there were only 10 cases of prior heart failure despite the large sample size. The final model yielded a c-statistic of 0.88. As shown in Table 2, significant demographic predictors of NSAID-related cardiovascular events included all ages starting at 35–44 (OR = 2.59; CI 2.49–2.70), 45–54 (OR = 5.69; CI 5.49–5.89), 55–64 (OR = 9.72; CI 9.39–10.05), 65–74 (OR = 12.35; CI 11.94–12.79), and 75 and above (OR = 20.04; CI 19.35–20.77), black and racial groups other than white. Concomitant health conditions that were most strongly associated with the occurrence of NSAID-related cardiovascular events were cerebrovascular disease (OR = 5.04; CI 4.95–5.13), cardiomyopathy (OR = 2.70; CI 2.63–2.78), and history of myocardial infarction (OR 2.07; CI 2.01–2.13). Other comorbidities that were statistically significant in their association with the primary outcome included coronary artery disease, COPD, hypertension, atherothrombotic disease, chronic kidney disease, hepatic dysfunction, history of tobacco use, diabetes, peripheral arterial disease, and obstructive sleep apnea (see Table 3).
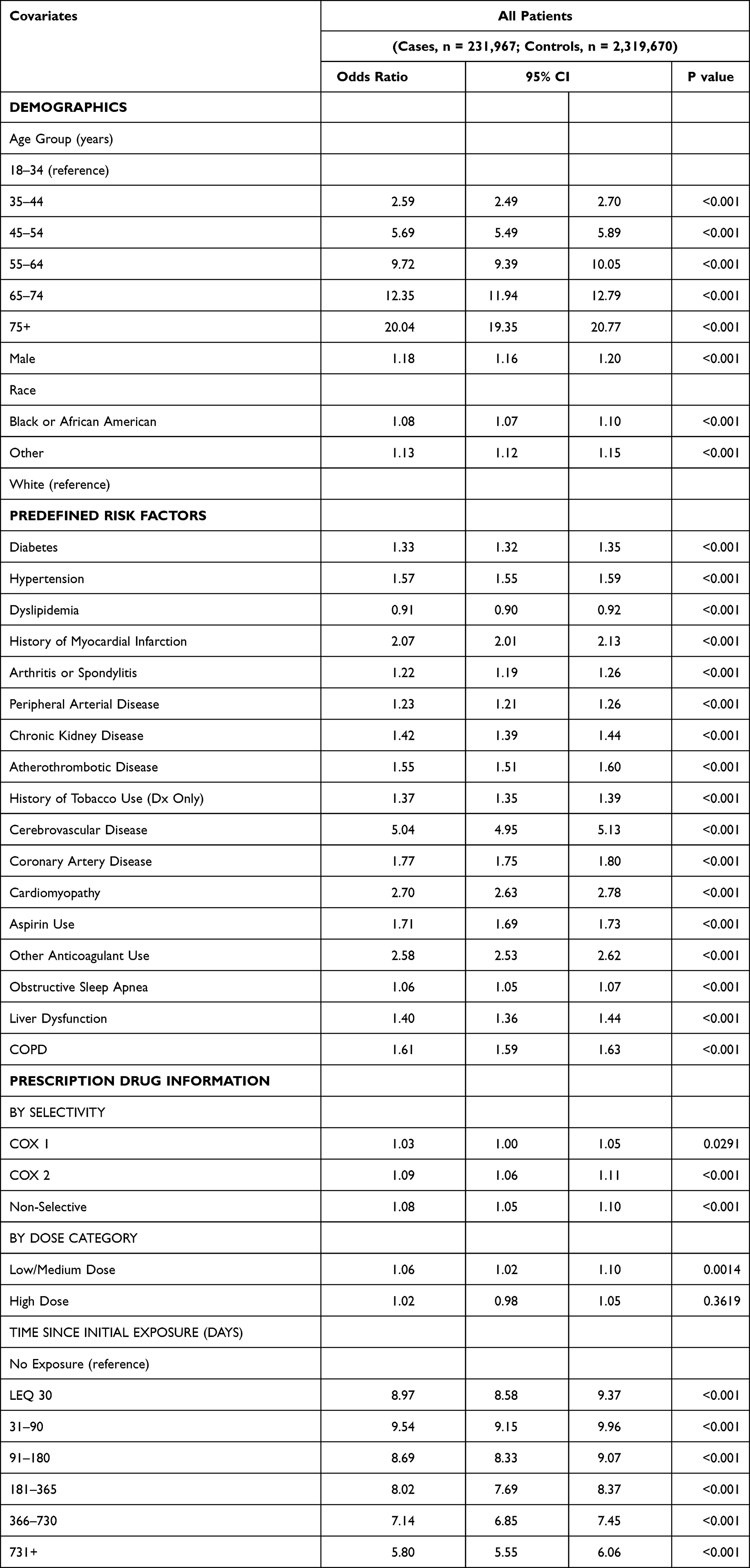 |
Table 3 Primary Outcome: Composite Cardiovascular Events |
Prescriptions for anticoagulants (OR = 2.58; CI 2.53–2.62) and aspirin (OR = 1.71; CI 1.69–1.73) significantly increased risk of NSAID-related CV events. As shown in Table 2, COX-1 selectivity (OR = 1.03; CI 1.00–1.05), and high dose NSAID use (OR = 1.02; CI 0.98–1.05) were not statistically significant but COX-2 (OR = 1.09; CI 1.06–1.11), non-selective (OR = 1.08; CI 1.05–1.10), and low/medium dose (OR = 1.06; CI 1.02–1.10) were statistically significant but with minimal impact on effect size. Time since initial exposure to NSAIDs is significant across all time intervals but appears to be high initially (OR = 8.97; CI 8.58–9.37) and peaks between 30 and 90 days (OR = 9.54; CI 9.15–9.96) before slowly tapering off the longer they are exposed to NSAIDs. Full regression results, including secondary outcomes and factors that were not statistically significant in relation to the outcome in the logistic regression model, are provided in the Supplementary Table 2–5.
Discussion
Our study reaffirms the association between NSAID use and an increased risk of cardiovascular events producing a robust multivariable model that characterized the risk of NSAID-related myocardial infarction, nonfatal stroke, and new heart failure in a composite outcome of cardiovascular events. Age, NSAID exposure within the past 90 days, and history of myocardial infarction or cerebrovascular disease were the factors most strongly associated with a cardiovascular event in the NSAID-exposed cohort of predominantly US Veterans and active-duty military personnel.
Consistent with published findings on cardiovascular risk, we found certain demographic characteristics, and comorbid conditions were factors associated with NSAID-related cardiovascular events. Demographic variables previously identified as risk factors and confirmed in the present study, which include black and other non-white racial groups.14 Comorbidities previously identified as risk factors and confirmed in the present study, included history of myocardial infarction, cerebrovascular disease, coronary artery disease, and atherothrombotic disease.4,6,8,9
Cardiovascular disease increases with age and comorbidities.39,40 However, there is a paucity of research evaluating the cardiovascular risk of an aging population using NSAIDs for common pain conditions. The odds ratio for experiencing a cardiovascular event doubles starting at 45 years-old and increases steadily each decade until at 75 years-old and beyond the risk has nearly quadrupled. This underpins the urgent need for clinicians to consider age not just as a chronological measure but as a marker of the cumulative effect of various physiological changes and disease states that predispose older individuals to cardiovascular risks and who may have attenuated compensatory mechanisms to deal with the cardiovascular strain NSAIDs may impose. In clinical decision-making, this calls for a paradigm shift from a one-size-fits-all to a more age-attuned prescription model. Practitioners should also be mindful of the comorbidities that significantly elevate cardiovascular risk when NSAIDs are used, as identified in the study. This suggests that medical practitioners should employ a conservative approach when initiating NSAID therapy in the elderly, perhaps opting for the lowest effective doses and considering alternative pain management strategies where feasible. In addition, these data support the need for regular cardiovascular monitoring of patients on NSAIDs, particularly in the early stages of treatment.
In our study, we have identified several critical aspects that both align with and diverge from the current body of literature on the cardiovascular risks associated with NSAID use. Previously published studies evaluating NSAID-related cardiovascular risk focused on three aspects of NSAIDs including COX-1 vs COX-2 selectivity,4,6,9,10,12,13,33–36,41,42 dose-dependent risks,4,6,9,11–13,33,41 and length of NSAID exposure.6,11,13,33,35 The present study confirms previously published reports on increased risk with early exposure to NSAIDs with the highest risk being the first 90 days of treatment after which the risk gradually diminishes but remains significantly higher than most other risk factors reviewed. In contrast to previous studies that were highly focused on evaluating the impact of COX selectivity on cardiovascular risk, the present study characterizes these effects as minor even when statistically significant. This raises questions about clinical significance when compared against other risk factors evaluated and potentially explains the heterogeneity of previously published results with inconsistent conclusions about the risk of individual NSAIDs. The dose-dependent risks of NSAIDs remain unclear as the low/moderate and high dose categories for each NSAID were not statistically significant for most outcomes despite the large cohort. The low/moderate dose category was significant for the primary outcome but not MI or non-fatal stroke and the odds ratio 1.03 is not clinically significant compared to other risk factors. These findings offer a comprehensive blend of reinforcement of established data and fresh insights, contributing to a more nuanced understanding of NSAID-related cardiovascular events.
The large dataset resulted in meaningful comparisons of each secondary outcome with most predefined risk factors achieving statistically significant results. Myocardial infarction is the most studied NSAID-related cardiovascular outcome.4,6,8,11,13,33,35,39 In the present study, the comorbidities serving as predefined risk factors most strongly associated with a myocardial infarction were history of myocardial infarction, coronary artery disease, and cardiomyopathy. Stroke is often evaluated as a vascular event or hemorrhagic stroke; however, non-fatal stroke was chosen in the present study due to NSAIDs dual mechanism potentially resulting in both hemorrhagic and thromboembolic events.4,6,8,40 For non-fatal stroke, the comorbidities that were the strongest risk factors were cerebrovascular disease, atherothrombotic disease, and hypertension. New heart failure is the least studied of the secondary outcomes, but the current study confirms previous published reports on NSAID-related risks.4,36 All secondary outcomes were influenced by age, but heart failure was the most influenced at every age group evaluated. The comorbidities with the strongest association to new heart failure were cardiomyopathy, coronary artery disease, and chronic obstructive pulmonary disease (COPD) (see Supplementary Tables S2-S5). Our findings corroborate the literature’s emphasis on the role of comorbid conditions, such as hypertension, diabetes, and atherothrombotic disease, in amplifying cardiovascular risks in NSAID users. This underscores the importance of considering underlying health conditions in prescribing practices.
The use of aspirin and anticoagulants were among the highest odds ratios for predefined risk factors for both primary and secondary outcomes. Due to their ability to minimize risk of thromboembolic events, it is unlikely that their mechanism contributed to events other than non-fatal stroke. However, patients with significant underlying risk or previous cardiovascular events may be on these agents for secondary prevention, which may explain their strong association with future cardiovascular events.
Limitations
Our study provides critical insights into NSAID-related cardiovascular risks but also presents several limitations related to potential confounders and biases. Administrative data inherently carry risks of coding errors, misclassification, missing data or incomplete data, which could influence the accuracy of comorbidity profiles and medication adherence. The absence of detailed patient lifestyle behaviors, genetic predispositions, and socioeconomic factors from the database introduces potentially unknown confounding variables that are challenging to control. The over-the-counter (OTC) medication coverage is self-reported within VHA and DoD, and it is possible that patients obtained and utilized NSAIDs from unreported sources. Although the large dataset allowed for meaningful comparisons, the study was limited to a specific population of US Veterans and active-duty military personnel, which may affect the generalizability to other populations. These factors underscore the importance of a cautious approach when applying our findings to clinical practice and policy-making, especially in demographically diverse settings outside of the VA/DoD population.
Conclusion
The results of our study both reinforce and expand the existing body of knowledge regarding NSAID use and cardiovascular risk. It emphasizes the inherent risks of these medications and the exacerbating role of comorbidities and concomitant medication use. Our research offers new insights into the impact of specific demographic factors and the relative influence of NSAID-specific risk factors including age starting at 45 up to 75 and older, NSAID exposure within the past 90 days, cerebrovascular disease, cardiomyopathy, and history of myocardial infarction are the factors most strongly associated with NSAID-related cardiovascular events. Cox-selectivity and dose did not appear to be clinically significant in their association with cardiovascular events. These findings underscore the critical importance of a personalized approach in prescribing NSAIDs, taking into account patient-specific factors such as age, race, and detailed comorbidity profiles to optimize cardiovascular safety among patients requiring NSAID therapy. These results also facilitate the creation of a risk index designed to predict cardiovascular events related to NSAID use and should be utilized in a prospective trial to validate results.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ugurlucan M, M Caglar I, N Turhan Caglar F, et al. Aspirin: from a Historical Perspective. Recent Patents Cardiovascular Drug Discovery. 2012;7:71–76. doi:10.2174/157489012799362377
2. Sun SX, Lee KY, Bertram CT, et al. Withdrawal of COX-2 selective inhibitors rofecoxib and valdecoxib: impact on NSAID and gastroprotective drug prescribing and utilization. Curr Med Res Opin. 2007;23(8):1859–1866. doi:10.1185/030079907X210561
3. Conaghan P. A turbulent decade for NSAIDs: update on current concepts of classification, epidemiology, comparative efficacy, and toxicity. Rheumatol Int. 2012;32:1491–1502. doi:10.1007/s00296-011-2263-6
4. Bhala N, Emberson J, Merhi A, et al.; Coxib and traditional NSAID Trialists’ (CNT) Collaboration. Vascular and upper gastrointestinal effects of non-steroidal anti-inflammatory drugs: meta-analyses of individual participant data from randomized trials. Lancet. 2013;382(9894):769–779. doi:10.1016/s0140-6736(13)60900-9
5. Yuan YH, Wang C, Yuan Y, et al. Meta-analysis: incidence of endoscopic gastric and duodenal ulcers in placebo arms of randomized placebo-controlled NSAID trials. Aliment Pharmacol Ther. 2009;30:197–209. doi:10.1111/j.1365-2036.2009.04038.x
6. Ray W, Varas-Lorenzo C, Chung C, et al. Cardiovascular Risks of Nonsteroidal Anti-inflammatory Drugs in Patients After Hospitalization for Serious Coronary Heart Disease. Cir Cardiovasc Qual Outcomes. 2009;2:155–163. doi:10.1161/CIRCOUTCOMES.108.805689
7. Ho KY, Cardosa M, Chaiamnuay S, et al. Practice Advisory on the Appropriate Use of NSAIDs in Primary Care. J Pain Res. 2020;13:1925–1939. doi:10.2147/JPR.S247781
8. Trelle S, Reichenbach S, Wandel S, et al. Cardiovascular safety of non-steroidal anti-inflammatory drugs: network meta-analysis. BMJ. 2011;342:c7086. doi:10.1136/bmj.c7086
9. Kearney P, Baigent C, Godwin J, et al. Do selective cyclo-oxygenase-2 inhibitors and traditional non-steroidal anti-inflammatory drugs increase the risk of atherothrombosis? Meta-analysis of randomized trials. BMJ. 2006;332:1302–1305. doi:10.1136/bmj.332.7553.1302
10. Gunter B, Butler K, Wallace R, et al. Non-steroidal anti-inflammatory drug-induced cardiovascular adverse events: a meta-analysis. J Clin Pharm Ther. 2017;42:27–38. doi:10.1111/jcpt.12484
11. Bally M, Dendukuri N, Rich B, et al. Risk of acute myocardial infarction with NSAIDs in real world use: bayesian meta-analysis of individual patient data. BMJ. 2017:
12. Martin Arias L, Gonazalez A, Fadrique R, et al. Cardiovascular Risk of Nonsteroidal Anti-inflammatory Drugs and Classical and Selective Cyclooxygenase-2 Inhibitors: a Meta-analysis of Observational Studies. J Clin Pharmacol. 2019;59(1):55–73. doi:10.1002/jcph.1302
13. Garcia Rodgriguez L, Tacconelli S, Patrignani P. Role of dose potency in the prediction of risk of myocardial infarction associated with nonsteroidal anti-inflammatory drugs in the general population. J Am Coll Cardiol. 2008;52(20):1628–1636. doi:10.1016/j.jacc.2008.08.041
14. Benjamin E, Muntner P, Alonso A, et al. Heart Disease and Stroke Statistics-2019 Update: a Report From the American Heart Association. Circulation. 2019;139(10):e56–e528. doi:10.1161/CIR.0000000000000659
15. D’Agostino R, Vasan R, Pencina M, et al. General Cardiovascular Risk Profile for Use in Primary Care: the Framingham Heart Study. Circulation. 2008;117(6):743–753. doi:10.1161/CIRCULATIONAHA.107.699579
16. Yancy CW, Jessup M, Bozkurt B, et al. 2013 ACCF/AHA guideline for the management of heart failure: a report of the American College of Cardiology Foundation/American Heart Association Task Force on Practice Guidelines. J Am Coll Cardiol. 2013;62(16):e147–239. doi:10.1016/j.jacc.2013.05.019
17. Page RL, O’Bryant CL, Cheng D, et al. Drugs That May Cause or Exacerbate Heart Failure: a Scientific Statement From the American Heart Association. Circulation. 2016;134(6):e32–69. doi:10.1161/CIR.0000000000000426
18. Whelton PK, Carey RM, Aronow WS, et al. 2017 Guideline for the Prevention, Detection, Evaluation, and Management of High Blood Pressure in Adults: executive Summary: a Report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. Hypertension. 2018;71(6):1269–1324. doi:10.1161/HYP.0000000000000066
19. Stevens PE, Levin A. Evaluation and management of chronic kidney disease: synopsis of the kidney disease: improving global outcomes 2012 clinical practice guideline. Ann Intern Med. 2013;158(11):825–830. doi:10.7326/0003-4819-158-11-201306040-00007
20. V.A./DoD Clinical Practice Guideline for the Non-Surgical Management of Hip & Knee Osteoarthritis. Available from: https://www.healthquality.va.gov/guidelines/CD/OA/VADoDOACPG.pdf.
21. Bannuru RR, Osani MC, Vaysbrot EE, et al. OARSI guidelines for the non-surgical management of knee, Hip, and polyarticular osteoarthritis. Osteoarthritis Cartilage. 2019;27:1578–1589. doi:10.1016/j.joca.2019.06.011
22. Kolasinski SL, Neogi T, Hochberg M, et al. 2019 American College of Rheumatology/Arthritis Foundation Guideline for the Management of Osteoarthritis of the Hand, Hip, and Knee. Arthritis Care Res. 2020;72(2):149–162. doi:10.1002/acr.24131
23. VA/DoD Clinical Practice Guideline for the Diagnosis and Treatment of Low Back Pain. Available from: https://www.healthquality.va.gov/guidelines/pain/lbp/.
24. Qaseem A, Wilt TJ, McLean RM, et al. Noninvasive treatments for acute, subacute, and chronic low back pain: a clinical practice guideline from the American College of Physicians. Ann Intern Med. 2017;166(7):514–530. doi:10.7326/M16-2367
25. Stochkendahl MJ, Kjaer P, Hartvigsen J, et al. National clinical guidelines for non-surgical treatment of patients with recent onset low back pain or lumbar radiculopathy. Eur Spine J. 2018;27(1):60–75. doi:10.1007/s00586-017-5099-2
26. Traeger AC, Buchbinder R, Elshaug A, et al. Care for low back pain: can health systems deliver? Bull World Health Organ. 2019;97:423–433. doi:10.2471/BLT.18.226050
27. FitzGerald JD, Dalbeth N, Mikuls T, et al. 2020 American College of Rheumatology Guideline for the Management of Gout. Arthritis Care Res. 2020;72(6):744–760. doi:10.1002/acr.24180
28. Becker CM, Bokor A, Hekinheimo O, et al. ESHRE guideline: endometriosis. Human Reproduction Open. 2022;2022(2):1–26. doi:10.1093/hropen/hoac009
29. Singh JA, Guyatt G, Ogdie A, et al. 2018 American College of Rheumatology/National Psoriasis Foundation Guideline for the Treatment of Psoriatic Arthritis. Arthritis Rheumatol. 2019;71(1):5–32. doi:10.1002/art.40726
30. VA/DoD Clinical Practice Guideline Use of Opioids in the Management of Chronic Pain. Available from: https://www.healthquality.va.gov/guidelines/pain/cot/.
31. Dowell D, Ragan KR, Jones CM, et al. CDC Clinical Practice Guideline for Prescribing Opioids for Pain – United States, 2022. MMWR Recomm RepI. 2022;71(No. RR–3):1–95. doi:10.15585/mmwr.rr7103a1
32. DuVall SL, Matheny ME, Ibragimov IR, et al. A Tale of Two Databases: the DoD and V.A.VA Infrastructure for Clinical Intelligence (DaVINCI). Stud Health Technol Inform. 2019;264:1660–1661. doi:10.3233/SHTI190584
33. Varas-Lorenzo C, Riera-Guardia N, Calingaert B, et al. Stroke risk and NSAIDs: a systematic review of observational studies. Pharmacoepidemiol Drug Saf. 2011;20:1225–1236. doi:10.1002/pds.2227
34. Wang H, Bail J, He B, et al. Osteoarthritis and the risk of cardiovascular disease: a meta-analysis of observational studies. Sci Rep. 2016;22(6):39672. doi:10.1038/srep39672
35. Helin-Salmivaara A, Virtanen A, Vesalainen R, et al. NSAID use and the risk of hospitalization for first myocardial infarction in the general population: a nationwide case-control study from Finland. Eur Heart J. 2006;27(14):1657–1663. doi:10.1093/eurheartj/ehl053
36. Ungprasert P, Srivali N, Thongprayoon C. Nonsteroidal Anti-inflammatory Drugs and Risk of Incident Heart Failure: a Systematic Review and Meta-analysis of Observational Studies. Clin Cardiol. 2016;39(2):111–118. doi:10.1002/clc.22502
37. Cook NR. Use and misuse of the receiver operating characteristic curve in risk prediction. Circulation. 2007;115(7):928–935. doi:10.1161/CIRCULATIONAHA.106.672402
38. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The strengthening the reporting of observational studies in epidemiology (STROBE) statement: guidelines for reporting observational studies. Int j Surg. 2014;12(12):1495–1499. doi:10.1016/j.ijsu.2014.07.013
39. Rodgers J, Jones J, Bolleddu S, et al. Cardiovascular Risks Associated with Gender and Aging. Int J Med. 2019;6(2):19. doi:10.3390/jcdd6020019
40. Yazdanyar A, Newman A. The Burden of Cardiovascular Disease in the Elderly: morbidity, Mortality, and Costs. Clin Geriatr Med. 2009;24(4):563–577. doi:10.1016/j.cger.2009.07.007
41. Nissen S, Yeomans N, Solomon D, et al. Cardiovascular Safety of Celecoxib, Naproxen, or Ibuprofen for Arthritis. New Eng J Med. 2017;376(14):1390. doi:10.1056/NEJMoa1611593
42. Ungprasert P, Matteson E, Thongprayoon C. Nonaspirin Nonsteroidal Anti-Inflammatory Drugs and Risk of Hemorrhagic Stroke: a Systematic Review and Meta-Analysis of Observational Studies. Stroke. 2016;47:356–364. doi:10.1161/STROKEAHA.115.011678
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.