")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Impact of an Educational Intervention on Oral Health Knowledge and Bacterial Plaque Control in Male Secondary School Students in a Peruvian Province: A Quasi-Experimental Study
Authors Lloclla-Sauñe S, Briceño-Vergel G, Ladera-Castañeda M, Huamaní-Echaccaya J, Romero-Velásquez L, Hernández-Huamaní E, Aroste-Andía R, Cervantes-Ganoza L, Cayo-Rojas C
Received 4 November 2023
Accepted for publication 9 January 2024
Published 16 January 2024 Volume 2024:17 Pages 205—217
DOI https://doi.org/10.2147/JMDH.S448217
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Shevaristh Lloclla-Sauñe,1 Gissela Briceño-Vergel,1 Marysela Ladera-Castañeda,2 José Huamaní-Echaccaya,1 Leysi Romero-Velásquez,1 Emily Hernández-Huamaní,1 Rosa Aroste-Andía,1 Luis Cervantes-Ganoza,3 César Cayo-Rojas1
1School of Stomatology, Universidad Privada San Juan Bautista, Ica, Peru; 2Faculty of Dentistry and Postgraduate School, Research Team “salud Pública – Salud Integral”, Universidad Nacional Federico Villarreal, Lima, Peru; 3Faculty of Stomatology, Universidad Inca Garcilaso de la Vega, Lima, Peru
Correspondence: César Cayo-Rojas, Address: School of Stomatology, Universidad Privada San Juan Bautista, Carretera Panamericana Sur Km. 300, La Angostura, Subtanjalla, Ica, Peru, Email [email protected]
Background: The purpose of this study was to evaluate the effect of an educational intervention on oral health knowledge and bacterial plaque control in male secondary school students in a Peruvian province.
Methods: This quasi-experimental study evaluated 294 male secondary school students in southern Peru. Oral health knowledge was measured with a validated 20-item questionnaire. Bacterial plaque was measured with the Simplified Oral Hygiene Index (OHI-S). This was rated as Excellent: 0, Good: 0.1– 1.2, Fair: 1.3– 3.0 and Poor: 3.1– 6.0, before receiving the educational intervention and after four weeks of receiving it. Variables such as age, area of residence, having health professionals as family members, educational level of mother and father, and living with parents were considered. A significance level of p< 0.05 was considered.
Results: The comparison between the level of oral health knowledge and the OHI-S, before and after 4 weeks of receiving the educational intervention, showed a significant improvement (p< 0.05) in all the categories of the variables studied. Likewise, before the educational intervention, there were significant differences in global knowledge about oral health among the categories of the following variables: age group (p=0.040), area of residence (p< 0.001), educational level (father) (p=0.011) and living with parents (p< 0.001). However, after four weeks of receiving the educational intervention, no significant differences were observed in all the variables studied (p> 0.05). Regarding the OHI-S, no significant differences were observed in any of the variables studied, both before (p> 0.05) and after four weeks (p> 0.05) of receiving the educational intervention.
Conclusion: After four weeks, the educational intervention significantly improved oral health knowledge and significantly reduced plaque bacterial plaque in male secondary school students in a Peruvian province, regardless of age, area of residence, having health professional family members, educational level of mother and father, and living with parents.
Keywords: educational intervention, bacterial plaque, level of knowledge, oral health, dentistry, secondary school students, Peru
Introduction
One of the most critical problems faced by several countries is the lack of knowledge regarding oral health care. This is reflected in the estimates published in the Global Burden of Disease study for the year 2019 that reported three and a half billion people affected by oral diseases, with dental caries being one of the most prevalent, since it has affected two thousand three hundred million inhabitants with permanent dentition and more than five hundred and thirty million children with primary dentition.1–5 In Peru, according to the last epidemiological study, the prevalence of dental caries was found to be 85.5% and 57.6% in the mixed and permanent dentition, respectively.6,7
Factors associated with oral diseases include continued high intake of free sugars, insufficient exposure to fluoride and poor plaque removal,3,8,9 the latter being the main etiological agent of periodontal diseases and dental caries.10 Bacterial plaque is a relevant factor for the development of gingival diseases because it behaves as a chemical-microbial agent with high aggressiveness for the oral mucosa, essentially due to the very high content of cocci, gram-positive and negative bacilli, fusobacteria, spirilla and spirochetes.11,12 It is therefore essential to control bacterial plaque and it should be included in all preventive and therapeutic procedures in order to prevent or mitigate oral diseases.13
Several studies have reported that these oral diseases can be avoided by implementing permanent education programs that focus especially on oral health self-care.13–15 Permanent oral health education programmes are those actions that are sustainable over time, which promote the development of knowledge and can lead to the adoption of behaviours to improve the oral health of schoolchildren. These programmes are delivered in health centres, hospitals and educational institutions as part of each country’s comprehensive school health policy.16 WHO has been promoting a school health initiative related to global health promotion through health education at all levels of government in each country.17
Oral health education comprises of deliberate teaching and learning activities intended to encourage voluntary actions that enhance the quality of life. It guides individuals to nurture and appreciate their oral structures through adopting appropriate habits to avoid risk situations.2 Moreover, it facilitates the acquisition of sustained and collective responsibility for addressing significant oral health issues.2,18
To date (September 2023), no study has been reported in which an educational intervention has been applied only in male schoolchildren, and this is of interest as some previous studies suggest that male sex is a risk factor for poor oral hygiene.19,20 In this sense, the virtual educational intervention could constitute an educational promotion strategy that contributes to improving the oral hygiene knowledge, attitudes and practices of schoolchildren in order to prevent oral diseases.16
Based on the above, the purpose of this study was to evaluate the effect of an educational intervention on oral health knowledge and bacterial plaque control in male secondary school students in a Peruvian province. The null hypothesis was that there are no significant differences when comparing oral health knowledge and bacterial plaque control in male secondary school students in a Peruvian province, before and after an educational intervention.
Methods
Study Design
This study had an analytical, prospective and longitudinal quasi-experimental design. It was carried out from July to September 2022 in the Secondary School for Male Students “San Luis Gonzaga de Ica” located in a southern Peruvian province (Ica, Peru).
Population and Selection of Participants
The population consisted of 356 students enrolled in the 1st year of secondary education at the “San Luis Gonzaga de Ica” educational institution, Ica, Peru in 2022. The sample size calculation was based on statistics obtained in a previous study where an educational intervention was applied in Peruvian adolescents and OHI-S and knowledge level were assessed before and after the intervention.21 In the statistical package Epidat 4.2 a paired mean comparison formula for the OHI-S score (considering the difference to be detected 0.77, SD1 = 0.37, SD2 = 0.76, 95% confidence level and a statistical power of 80%) and a paired proportion comparison formula for the level of knowledge (considering P1 = 21.3%, P2 = 11.5%, 95% confidence level and a statistical power of 80%); obtaining a minimum sample size of 12 and 226, respectively. As the calculated sample size was smaller than the 1st year secondary school student population, it was then decided to include the entire population according to the eligibility criteria, including 329 students and subsequently excluding 35 students, so the total number of participants was n = 294.
Inclusion criteria
- Students from the secondary school “San Luis Gonzaga de Ica” enrolled in first year of secondary school in 2022.
- Students whose parents gave their informed consent for the present study.
- Students who gave their informed assent voluntarily.
- Students with complete permanent incisor and molar teeth.
Exclusion criteria
- Students from the secondary school “San Luis Gonzaga de Ica” who did not complete the entire questionnaire (n = 23).
- Students who were undergoing orthodontic treatment (n = 8).
- Students who voluntarily withdrew while the study was being conducted (n = 4).
Variables
To evaluate the effect of the educational intervention, the level of oral health knowledge and the plaque index were considered as response variables. Age, area of residence, having health professionals as family members, educational level of mother, educational level of father and living with parents were considered as sociodemographic variables.
Instruments
A previously developed questionnaire with 20 closed-ended questions (Q1 - Q20) [supplementary materials] and multiple responses was validated to evaluate the general oral health knowledge of the students.22 The level of knowledge was defined according to the following score: poor (0–10 points), fair (11–13 points) and good (14–20 points). The cut-off points were set at 10.5 and 13.5 to determine the three levels of knowledge.23,24 These cut-off points were validated using Livingston’s K2 coefficient, yielding 0.784 and 0.786, respectively; these values were acceptable One point was awarded for each correct answer.
The content of the instrument was validated by three experts in dental research with an Aiken V equal to 0.93 (95% CI: 0.90–0.95), which is acceptable Regarding the reliability analysis of the questionnaire according to Cronbach’s alpha was (α) = 0.748 (95% CI: 0.704–0.788), so it was considered acceptable In addition, to assess the repeatability of the instrument, the questionnaire was administered at two different times to correlate the total scores over a lapse of 7 days to 30 students, altering the order of the questions to avoid recall bias, resulting in a Spearman’s coefficient (Rho) = 0.939 (95% CI: 0.871–0.971), which was acceptable This statistical test was performed because the scores were not normally distributed, according to the Shapiro Wilk test (p<0.05).
The method used to assess the level of oral hygiene was observation and the indicator used was Greene and Vermillion’s Simplified Oral Hygiene Index (OHI-S) comprising the simplified debris index (DI-S) and the simplified calculation index (CI-S).25 To assess oral hygiene status, a standardized data collection form was used which included the participant’s personal data, a table of 6 teeth with the vestibular and lingual sides as appropriate, as well as the coding criteria for assessing DI-S and CI-S with their respective scores, and a box for the final result.26,27 For the OHI-S, 6 teeth were evaluated and the vestibular surfaces of the upper right central incisor (tooth 1.1) and the lower left central incisor (tooth 3.1) were taken into account. If these teeth were missing, the left upper central incisor (tooth 2.1) or the right lower central incisor (tooth 4.1) was evaluated. In addition, for the posterior teeth, the vestibular surface of the upper right and left first molars (teeth 1.6 and 2.6, respectively) was examined, provided they were fully erupted, and in the absence of these teeth, the upper second molar (tooth 1.7 or 2.7) was evaluated. For the lower first molars (teeth 3.6 and 4.6) the lingual surfaces were taken into account and in case of absence of these teeth, teeth 3.7 or 4.7 were evaluated.26,27
The score for the DI-S was 0 (absence of detritus with extrinsic stain), 1 (presence of detritus covering no more than 1/3 of the tooth surface or absence of detritus plus presence of extrinsic stain), 2 (presence of detritus covering more than 1/3 but not more than 2/3 of the examined tooth surface), and 3 (presence of detritus covering more than 2/3 of the examined tooth surface). For the final DI-S score, the total vestibular score plus the total lingual score, divided by the number of teeth assessed, were considered.26,27
The score for the simplified calculus index (CI-S) was 0 (absence of calculus), 1 (presence of supragingival calculus covering no more than 1/3 of the examined surface), 2 (presence of supragingival calculus covering more than 1/3 but not more than 2/3 of the examined surface or small portions of subgingival calculus around the cervical portion), and 3 (presence of supragingival calculus covering more than 2/3 of the examined surface or small portions of subgingival calculus around the cervical portion), and 3 (presence of supragingival calculus covering more than 2/3 of the examined surface or a continuous band of supragingival calculus around the cervical region of the tooth). For the final CI-S score, the total vestibular score plus the total lingual score, divided by the number of teeth assessed, was considered.26,27
Finally, to obtain the OHI-S, the results of the DI-S and the CI-S were added, considering the following values for the clinical degree of oral hygiene: Excellent (0), Good (0.1–1.2), Fair (1.3–3.0) and Poor (3.1–6.0).26,27
The OHI-S was measured by a single investigator, but to avoid measurement bias, a pre-study calibration was performed with 30 participants using the intraclass correlation coefficient (ICC), both intra-examiner (ICC = 0.996; 95% CI: 0.992–0.998) and inter-examiner with a specialist (ICC = 0.995; 95% CI: 0.989–0.998), yielding acceptable values.26,27
Procedure
An initial face-to-face evaluation about oral health knowledge and OHI-S was conducted prior to the educational intervention, at a rate of one classroom per day. This was done in the tutoring hour of each of the 10 participating classrooms. Then, educational sessions (through the Zoom® platform) were conducted using the classroom projector in order to standardize the educational material, strategies and time used in each of the sessions. Thus, the educational session given by the main researcher (S.L.S.), was transmitted to the 10 classrooms in power point format. The 16 color slides, in parallel to the concise explanation of each slide, included four topics: oral cavity pathologies, oral health preventive treatments, oral hygiene habits and habits that influence oral health status.28–30 The educational sessions were held once a week for a month with a duration of 30 minutes.
The methodology used for the development of each of the educational sessions was the start phase, the transfer phase and the closing phase. The start phase consisted of motivating the student to awaken their interest in the subject, through the presentation of videos showing models of healthy and unhealthy behaviour and/or clinical cases of real situations centred on the main problem of each subject; in addition, previous knowledge on the subject was explored through open questions. The transfer phase lasted approximately 20 minutes and started with a brief overview of the topic, then the core contents were explained through attractive and dynamic images; and recommendations to improve oral health were shown. The final phase lasted approximately 5 minutes in which students were asked to demonstrate what they had learned through gamification tools and real time demonstrations of newly acquired skills according to the topic of each educational session in order to verify what they had learned and provide necessary corrections.5,31 Four weeks after the end of these cuatro educational sessions, a final evaluation about knowledge and OHI-S was carried out in a face-to-face manner.5,15,32,33
Statistical Analysis
Data analysis was performed with the Statistical Package for the Social Sciences (SPSS) version 28.0. Descriptive statistics were applied to calculate absolute and relative frequencies for qualitative variables, the mean and standard deviation for age, and the median and interquartile range for the score of ordinal variables. To compare students’ oral health knowledge and plaque index between two or more categories of the qualitative variables (before the educational intervention and four weeks after the intervention), the Mann Whitney U-test and the Kruskal Wallis test were used, respectively. In addition, the Wilcoxon signed-rank test was used for the comparison of related measures and the Mc Nemar Chi-square test was used for the comparison of the proportion of correct answers for each questionnaire item. In all statistical tests a significance level of p<0.05 was considered.
Bioethical Considerations
The present study respected the bioethical principles of the Declaration of Helsinki related to confidentiality, freedom, respect, and nonmaleficence.34 In addition, we had the approval of an Institutional Ethics Committee of the San Juan Bautista Private University with resolution No. 293–2022-CIEI-UPSJB on March 3, 2022. Finally, parents and students were asked for voluntary informed consent and assent, respectively.
Results
Factor Analysis of the Knowledge Level Instrument
For the structural validity of the dimensions, a principal component factor analysis was performed with Varimax rotation and Kaiser normalization, identifying four dimensions. The first dimension (D1) consisted of eight items (Q1 - Q8) related to the knowledge of the pathologies present in the oral cavity. The second dimension (D2) consisted of three items (Q9 - Q11) related to knowledge of preventive treatments on oral health. The third dimension (D3) consisted of three items (Q12 - Q14) related to oral hygiene habits. The fourth dimension (D4) consisted of six items (Q15 - Q20) related to habits that have an impact on oral health status. The item-total correlation determinant was equal to 0.042, the Kaiser-Meyer-Olkin (KMO) measure of adequacy was 0.824 and Bartlett’s test of sphericity was p<0.001, all resulting in acceptable values.35
Sociodemographic Characteristics
The mean age of the 294 participants was 12.5 ± 0.6 years. The 54.4% of participants were between 11 and 12 years of age and 79.3% resided in an urban area. The 45.9% did not have a health professional as family member. The 54.8% had a mother with a higher education. The 48.0% had a father with a higher level of education. Finally, the 55.1% of the participants lived with both parents [Table 1].
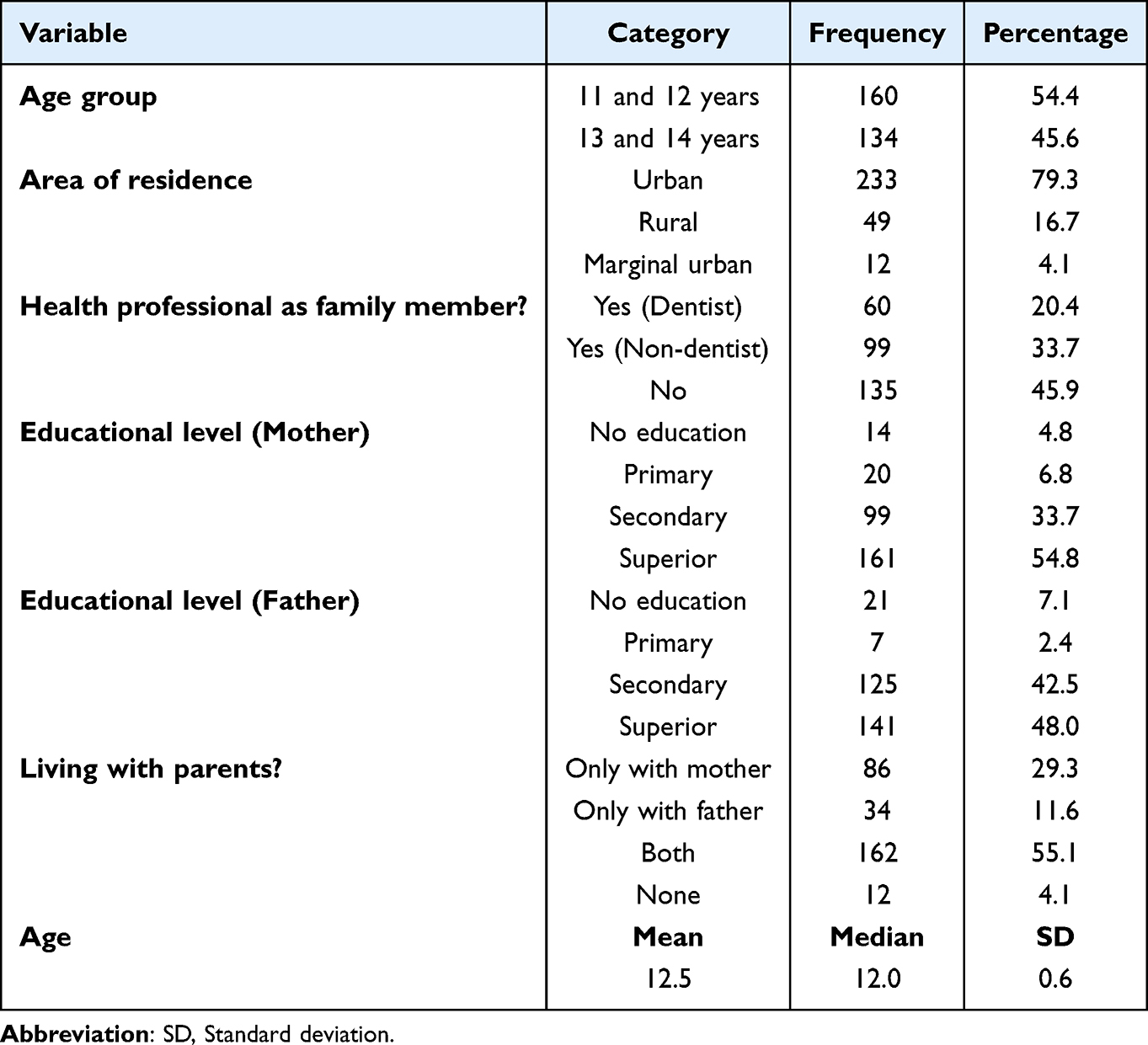 |
Table 1 Sociodemographic Characteristics of Male Students Belonging to an Educational Institution in a Peruvian Province |
Changes in Oral Health Knowledge and Bacterial Plaque Control
When comparing the correct answers regarding oral health knowledge before and after 4 weeks of receiving educational intervention, it was observed that there was a significant improvement in knowledge (p<0.05) in all questions except Q15 (Which of the following foods do you think are harmful to teeth?), since the proportion of correct answers in both evaluations did not show significant differences (p=0.189) [Table 2].
 |
Table 2 Comparison of Correct Answers About Oral Health Knowledge Before and After 4 Weeks of Receiving Educational Intervention |
When comparing the level of total oral health knowledge, a significant improvement was observed in all categories of age group (p<0.001), area of residence (p<0.05), having a health professional as a family member (p<0.001), educational level of the mother (p<0.05) and father (p<0.05), and living or not with parents (p<0.05) [Table 3]. Likewise, before the educational intervention, when comparing oral health knowledge among the categories of each variable, there were significant differences in the age group (p=0.040), area of residence (p<0.001), educational level of the father (p=0.011) and living or not with parents (p<0.001). However, after 4 weeks of receiving the last educational intervention, the students did not present significant differences among the categories of all the variables considered in the study (p>0.05) [Table 3].
 |
Table 3 Comparison of Oral Health Knowledge Before and After 4 Weeks of Receiving Educational Intervention According to Sociodemographic Variables |
When comparing the IHOS of the students, a significant reduction could be observed in all categories of age group (p<0.001), area of residence (p<0.05), having a health professional as family member (p<0.001), educational level of the mother (p<0.05) and father (p<0.05), and living or not with parents (p<0.05) [Table 4]. On the other hand, both before and after 4 weeks of receiving the last educational intervention, no significant differences were observed between the categories of any variable (p>0.05) [Table 4].
 |
Table 4 Comparison of OHI-S Before and After 4 Weeks of Receiving Educational Intervention According to Sociodemographic Variables |
Discussion
Oral cavity diseases, like other pathologies, have biological, psychosocial and emotional effects.36 Oral diseases are chronic and progressive in nature, and the most prevalent are dental caries, periodontal disease, and oral cancer. These diseases constitute a major burden on families and health systems in many countries, affecting the quality of life in all age groups by causing pain, discomfort, disfigurement, and even death.8,14 Adolescence is a period in which the main variations in development occur, establishing attitudes that will form an important part of general and oral health care.8,37 It is necessary at this stage to acquire sufficient knowledge and correct oral hygiene practices since these habits will be present during the growth process and will have a profound impact throughout their individual development.8,38 Therefore, the purpose of this study was to evaluate the effect of an educational intervention on oral health knowledge and bacterial plaque control in male secondary school students in a Peruvian province. Based on the results, the null hypothesis was rejected.
Although oral hygiene indices that require assessment of all tooth surfaces should be preferred, partial indices can be used as an alternative, the most suitable being those that assess 6 teeth, for example the IHO-S. This index is indicated in epidemiological studies and educational programmes, as it is easy to use and the examination can be performed without delay.39 In contrast, although the Turesky-Gilmore-Glickman index is considered one of the best indices for plaque assessment in clinical studies, its application in daily clinical practice is considered impractical.39 Therefore, the decision was taken in this research to use the IHO-S to assess the oral hygiene level of secondary school children, as it tested an educational intervention in which a quick and practical measurement by a single operator was needed, even more so when at the time of the present study there were certain restrictions on access to the population due to the Covid-19 pandemic.
The results obtained showed that when comparing the correct answers on oral health knowledge before receiving the educational intervention and after 4 weeks of the same, there was a significant improvement in the students’ oral health knowledge. These results were consistent with those obtained by Movaseghi et al, Subedi et al and Haque et al14–16 who reported significant improvement of knowledge in adolescents from Iran, Nepal and Bangladesh respectively on the same topic. This reinforces the idea that educational intervention is an important tool to motivate adolescents to improve knowledge regarding oral health related topics.38,40 It should be noted that there was a significant improvement in knowledge in all questions except Q15 (Which of the following foods do you think are harmful to teeth?) as the proportion of correct answers in both assessments did not present significant differences. Perhaps it was because the respondents already knew that foods such as chocolate or candy are harmful to their teeth as they had received this information many times through parents, teachers and health professionals.41,42 Perhaps during the time that the educational intervention lasted, this knowledge was reinforced and helped the participants to improve their healthy habits as evidenced by the OHI-S.37
Before the educational intervention, there were differences in the categories of some variables with respect to knowledge. With respect to OHI-S there were no significant differences. This showed that in some cases knowledge was bad while practices were not so bad. This is probably due to the fact that the older age of the schoolchildren and the area of residence (urban) gave them greater access to information on this topic, helping them to create awareness of good hygiene habits. Likewise, according to the results obtained, it may be that the presence of both parents or the greater academic preparation of the same allowed the students to be inculcated with good oral hygiene habits. In spite of the differences obtained on oral health knowledge, it was observed that at the end of the 4 weeks of receiving the educational intervention, the gaps in knowledge about this topic were closed in all the study variables to the point of not observing significant differences in their conceptual and procedural learning, which supports the idea that the educational intervention contributes to the acquisition of knowledge that motivates the modification of healthy behaviors and practices.14,43
On the other hand, when comparing the OHI-S before and after 4 weeks of receiving the educational intervention, a significant reduction was observed in all the categories of the study variables. These results were similar to those reported by Subedi et al and Movaseghi et al14,15 who found a significant reduction in the levels of bacterial plaque after an educational intervention in schoolchildren, showing that this type of intervention has a positive effect on the oral hygiene of students by reducing bacterial plaque as students improve their oral health knowledge.44,45
In this research, the educational intervention was chosen to be carried out with male secondary school students because some studies reported that they have poor oral hygiene attitudes and practices, and that they make fewer visits to the dentist,19,42,43,46,47 which is why they are more exposed to developing oral diseases.47 Likewise, Rajabzadeh et al, Rajeh and Woelber,48–50 reported that females scored higher mean scores in relation to oral hygiene practices than males, according to them this could be because females had better self-care attitudes and better willingness to make more frequent visits to the dentist.48–50 In addition, it has been reported that women are more concerned about their general health in order to improve their appearance and self-esteem.47,48,51 In that sense, it was considered necessary to address specific strategies to decrease these inequalities between women and men.47
Maintaining the tooth surface free of bacterial plaque is the cornerstone of the prevention of more prevalent oral diseases such as dental caries and periodontal disease.45 The continuous and regular interruption of plaque formation as well as oral health literacy, awareness creation and the establishment of healthy habits at an early age play a fundamental role in the reduction and control of these pathologies, so the present educational intervention is an essential strategy to fulfill this purpose.16,43
The present study had some limitations such as carrying out the educational intervention in 4 weeks (short term), which did not allow the long-term results to be evaluated. In addition, attitudes and other healthy oral health practices, such as proper nutrition, frequency of brushing, use of fluoride toothpaste and use of mouthwashes, were not assessed. Another limitation of this study was that it was conducted at the height of the pandemic when the government decreed compulsory social isolation,52 so only one public school authorized the study. However, this was one of the schools with the largest student population in the province of Ica. On the other hand, it should be noted that this research may have been influenced by the Hawthorne effect, as the schoolchildren, being aware that they are part of a study, may have made more effort to acquire good practices by changing their behaviour. Therefore, it is not certain that the desired effects or behaviours will be maintained in the long term.53 Finally, although this study worked with a larger number of adolescent male students from the province of Ica than the minimum sample size required, it must be recognized that the results of this study are not applicable to adolescent female students from that province, nor are these results extrapolable to adolescent students from the whole country, and it is therefore suggested that similar studies be developed that include different Peruvian regions.
Based on the results obtained, it is recommended that oral health education interventions be included in the school health plan of each institution so that students acquire healthy habits at an early age that are sustainable throughout their lives.14,15,45 On the other hand, it is recommended that schools be accompanied not only by a psychologist or doctor on a permanent basis, but also by a dentist who periodically evaluates the level of oral hygiene of schoolchildren. It is necessary for parents to monitor the oral hygiene of their adolescent children, as poor oral health practices have been reported at this stage.8 In addition, it is recommended to train and raise awareness among parents and their children to promote the development of oral health self-care skills. Finally, longitudinal studies are recommended to evaluate the effectiveness of different educational techniques on oral hygiene knowledge, attitudes and practices in school children together with their parents or guardians.
Conclusion
After four weeks, the educational intervention on topics related to pathologies present in the oral cavity, preventive oral health treatments, oral hygiene habits and habits that have an impact on oral health status, significantly improved oral health knowledge and significantly reduced bacterial plaque in male secondary school students in a Peruvian province, regardless of age, area of residence, having a health professional as family member (dentist or not), educational level of the mother or father, and living or not with parents. Oral health literacy, awareness and reinforcement of healthy habits in early adolescence are recommended, as they play a key role in the prevention of dental caries and periodontal disease.
Data Sharing Statement
The datasets used and/or analysed during the current study available from the corresponding author on reasonable request.
Ethic Approval and Consent to Participate
The present study respected the bioethical principles for medical research on human beings of the Declaration of Helsinki, related to confidentiality, freedom, respect and non-maleficence. It was also approved by the Institutional Research Ethics Committee of the Universidad Privada San Juan Bautista with resolution No. 293-2022-CIEI-UPSJB dated March 3, 2022. Finally, parents and students were asked for voluntary informed consent and assent, respectively.
Acknowledgments
We thank the team of the ”Salud Pública Estomatológica” research line of the School of Stomatology of the Universidad Privada San Juan Bautista, Peru, for their constant support in the preparation of this manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research received no external funding.
Disclosure
The authors declare that they have no conflicts of interest with the development and publication of this research.
References
1. Wen PYF, Chen MX, Zhong YJ, Dong QQ, Wong HM. Global burden and inequality of dental caries, 1990 to 2019. J Dent Res. 2022;101(4):392–399. doi:10.1177/00220345211056247
2. Bolaños SN. Educación para la conservación de la salud bucal. Rev Odont Mex. 2020;24(4):228–232.
3. World Health Organization. Oral health. 2023. Available from: https://www.who.int/es/news-room/fact-sheets/detail/oral-health.
4. Gaspar-Dámaso N, Ladera-Castañeda M, Córdova-Limaylla N, et al. Sociodemographic factors associated with the level of knowledge of early postpartum women about oral health prevention in infants aged 0 to 2 years old: a cross-sectional study under a multivariable analysis. J Environ Res Public Health. 2023;20(3):1–14. doi:10.3390/ijerph20031881
5. Ladera-Castañeda M, Córdova-Limaylla NE, Briceño-Vergel G, Rosas-Díaz JC, Cervantes-Ganoza LA, Cayo-Rojas CF. Impact of puppet theater on oral health knowledge and oral hygiene in preschoolers from a Peruvian educational institution: a quasi-experimental study. J Int Soc Prevent Communit Dent. 2022;12(1):28–37. doi:10.4103/jispcd.JISPCD_212_21
6. A CB, Vergel GB, Cáceres CP, Perazzo MF, Vieira-Andrade RG, Cury JA. Fluoride content in children’s dentifrices marketed in Lima, Peru Braz. Oral Res. 2019;33:1–9. doi:10.1590/1807-3107bor-2019.vol33.0051
7. Ministerio de Salud (Perú). Guía técnica: guía de práctica clínica para la prevención, diagnóstico y tratamiento de la caries dental en niñas y niños. 2017. Available from: http://bvs.minsa.gob.pe/local/MINSA/4195.pdf.
8. Allen-Revoredo C, Ladera-Castañeda MI, Córdova-Limaylla NE, Briceño-Vergel G, Cervantes-Ganoza LA, Cayo-Rojas C. Knowledge, attitudes, and practices on oral health prevention associated with sociodemographic factors of adolescent students from a Peruvian-Swiss educational institution. J Int Oral Health. 2022;14(5):475–486. doi:10.4103/jioh.jioh_120_22
9. World Health Organization. Highlights oral health neglect affecting nearly half of the world’s population. 2022. Available From: https://www.who.int/es/news/item/18-11-2022-who-highlights-oral-health-neglect-affecting-nearly-half-of-The-world-s-population.
10. Sarduy L, E GM. Biofilm: a new conception of dentobacterial plaque. Medicentro Electrónica. 2016;20(3):167–175.
11. Clerehugh V, Tugnait A. Diagnosis and management of periodontal diseases in children and adolescents. J Periodontol. 2001;26(1):146–168. doi:10.1034/j.1600-0757.2001.2260108.x
12. Gita JB, Chandrasekaran SC, Darshani DD, Gnanamani A. Gram-positive anaerobes in periodontal pathogenesis: new kids on the block? - A mini review. J Bacteriol Mycol Open Acces. 2016;3(1):196. doi:10.15406/jbmoa.2016.03.00052
13. Avalos J, Huillca N, Picasso M, Omori E, Gallardo A. Level of knowledge on oral health related to quality of oral hygiene in schoolchildren of a Peruvian population. Kiru. 2015;12(1):61–65.
14. Movaseghi Ardekani F, Ghaderi F, Kaveh MH, Nazari M, Khoramaki Z. The Effect of an Educational Intervention on oral health literacy, knowledge, and behavior in Iranian adolescents: a theory-based randomized controlled trial. Biomed Res Int. 2022;2022:1–10. doi:10.1155/2022/5421799
15. Subedi K, Shrestha A, Bhagat T, Baral D. Effectiveness of oral health education intervention among 12–15-year-old school children in dharan, Nepal: a randomized controlled trial. BMC Oral Health. 2021;21(1):1–11. doi:10.1186/s12903-021-01877-6
16. Haque SE, Rahman M, Itsuko K, et al. Effect of a school-based oral health education in preventing untreated dental caries and increasing knowledge, attitude, and practices among adolescents in Bangladesh. BMC Oral Health. 2016;16(1):1–10. doi:10.1186/s12903-016-0202-3
17. Organización Mundial de la Salud. Directrices de la OMS sobre los servicios de salud escolar. 2021. Available from: https://iris.paho.org/bitstream/handle/10665.2/56726/9789275325865_spa.pdf?sequence=1&isAllowed=y.
18. Al-Qahtani SM, Razak PA, Khan SD. Knowledge and practice of preventive measures for oral health care among male intermediate schoolchildren in Abha, Saudi Arabia. Int J Environ Res Public Health. 2020;17(3):1–11. doi:10.3390/ijerph17030703
19. Abe M, Mitani A, Hoshi K, Yanagimoto S. Large gender gap in oral hygiene behavior and its impact on gingival health in late adolescence. Int J Environ Res Public Health. 2020;17(12):1–8. doi:10.3390/ijerph17124394
20. Zhang M, Lan J, Zhang T, Sun W, Liu P, Wang Z. Oral health and caries/gingivitis-associated factors of adolescents aged 12–15 in Shandong province, China: a cross-sectional oral health survey. BMC Oral Health. 2021;21(1):1–8. doi:10.1186/s12903-021-01640-x
21. Rufasto-Goche K, Saavedra-Alvarado B. Aplicación de un programa educativo en salud oral en adolescentes de una institución educativa peruana. Rev Estomatol Herediana. 2012;22(2):82–90.doi:10.20453/reh.v22i2.130
22. Hurtado Centeno JJ Efecto de una estrategia educativa en el nivel de conocimiento sobre salud oral en odontología en los pacientes de la posta Santiago Apóstol, Comas 2017 [Master Thesis]. Lima: Universidad Cesar Vallejo; 2019. Available from: https://repositorio.ucv.edu.pe/bitstream/handle/20.500.12692/31833/Hurtado_CJJ.pdf?sequence=1&isAllowed=y.
23. Cayo-Rojas CF, Soto-Castro L, Castro-Mena M, et al. Level of knowledge about metalloproteinases in dental students close to graduate from three universities in Peruvian capital city. Eur J Dent Educ. 2022;26(4):692–699. doi:10.1111/eje.12748
24. Cayo-Rojas CF, Medrano-Colmenares SM, Escurra-Estrada CI, Ladera-Castañeda MI, Agramonte-Rosell RC, Cervantes-Ganoza LA. Epidemiological, preventive and healthcare knowledge about COVID-19, in dental students from three Peruvian universities. Rev Cuba De Educ Med Super. 2021;20(2):1–16. doi:10.3390/ijerph20021020
25. Gandhi JM, Gurunathan D, Doraikannan S, Balasubramaniam A. Oral health status for primary dentition - A pilot study. J Indian Soc Pedod Prev Dent. 2021;39(4):369–372. doi:10.4103/jisppd.jisppd_155_21
26. Baishya B, Satpathy A, Nayak R, Mohanty R. Oral hygiene status, oral hygiene practices and periodontal health of brick kiln workers of Odisha. J Indian Soc Periodontol. 2019;23(2):163–167. doi:10.4103/jisp.jisp_383_18
27. Mora K, Calle D, Sacoto F. Simplified oral hygiene index in schoolchildren of 6 years of age, ecuador, 2016. Odontología Vital. 2020;2(33):73–78.
28. Ministerio de Salud. Módulo de promoción de la salud bucal: higiene oral. 2013. Available from: https://www.gob.pe/institucion/minsa/informes-publicaciones/321210-modulo-de-promocion-de-la-salud-bucal-higiene-oral.
29. Haleem A, Siddiqui MI, Khan AA. School-based strategies for oral health education of adolescents- A cluster randomized controlled trial. BMC Oral Health. 2012;12(1):1–12. doi:10.1186/1472-6831-12-54
30. Da’aj S, Al-Bayati S, Al-Karawi A, Hameed A. Oral health education (OHE) program on adolescents before and after teacher’s training in Diyala city: a comparative clinical study Egypt. J Hosp Med. 2023;90(1):1120–1125.
31. Sanaeinasab H, Saffari M, Taghavi H, et al. An educational intervention using the health belief model for improvement of oral health behavior in grade-schoolers: a randomized controlled trial. BMC Oral Health. 2022;22(1):1–11. doi:10.1186/s12903-022-02132-2
32. Robaina B, Rubio M, García F. Oral health knowledge and tooth brushing quality before and after an educational intervention in children aged 9 and 10. Av. Odontoestomatol. 2012;28(1):17–23.
33. Alvarez P, De la Hoz L, Martinez F. Educational intervention on oral health in preschool children. Edumecentro. 2022;14:1–15.
34. World Medical Association. World medical association declaration of helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
35. Cayo-Rojas CF, Córdova-Limaylla NE, Briceño-Vergel G, et al. Psychometric evidence of a perception scale about covid-19 vaccination process in Peruvian dentists: a preliminary validation. BMC Health Serv Res. 2022;22(1):1–13. doi:10.1186/s12913-022-08677-w
36. Geethapriya PR, Asokan S. Comparison of oral health status and knowledge on oral health in two age groups of schoolchildren: a cross-sectional study. J Clin Pediatr Dent. 2017;10(4):340–345. doi:10.5005/jp-journals-10005-1462
37. Penoni DC, Moura MF, da Costa Florenzano LG, Dos Santos MM, Carlos JC. The impact of oral hygiene instruction on plaque control in orthodontic patients: a cross-sectional study. Brazilian Dent Sci. 2022;25(4):1–7. doi:10.4322/bds.2022.e3557
38. Dadipoor S, Akbarizadeh F, Ghaffari M, Alipour A, Safari-Moradabadi A. Educational Intervention of improve student’s oral health: a systematic review and meta-analysis school-based. Iran J Public Health. 2023;52(3):500–514. doi:10.18502/ijph.v52i3.12133
39. Delia G, Floris W, Marini L, et al. Methods for evaluating the effectiveness of home oral hygiene measures-a narrative review of dental biofilm indices. J Dent. 2023;11(7):1–24. doi:10.3390/dj11070172
40. Gurav KM, Shetty V, Vinay V, Bhor K, Jain C, Divekar P. Effectiveness of oral health educational methods among school children aged 5–16 years in improving their oral health status: a meta-analysis. Int J Clin Pediatr Dent. 2022;15(3):338–349. doi:10.5005/jp-journals-10005-2395
41. Savage JS, Adams EL, Rollins BY, Bleser JA, Marini ME. Teaching families to manage intake of candy in the home: results from a feasibility study using multiphase optimization strategy (MOST). Obes Sci Pract. 2020;6(6):649–659. doi:10.1002/osp4.44
42. Samaddar A, Shrikrishna SB, Moza A, Shenoy R. Association of parental food choice motives, attitudes, and sugar exposure in the diet with early childhood caries: case-control study. J Indian Soc Pedod Prev Dent. 2021;39(2):171–177. doi:10.4103/jisppd.jisppd_104_21
43. Ramírez K, Mercado J, Cumpa R, Padilla-Cáceres T, Sucari W. Educational intervention on the knowledge level of oral health in primary school teachers in a rural area of Puno. Peru Revista Innova Edu. 2022;4(4):125–134. doi:10.35622/j.rie.2022.04.009
44. Cabrera MF, Pillacela JF, Lafebre MF, Reinoso JC, Ramón JE. Impact of an educational intervention on oral health in children aged 8 to 11 years N.a. J Adv Res Rev. 2022;14(2):510–514. doi:10.30574/wjarr.2022.14.2.0459
45. Reddy MP, Lakshmi SV, Kulkarni S, Doshi D, Reddy BS, Shaheen SS. Impact of oral health education on plaque scores with and without periodic reinforcement among 12-year-old school children. J Indian Assoc Public Health Dent. 2016;14(2):116–120. doi:10.4103/2319-5932.183806
46. Lipsky MS, Su S, Crespo CJ, Hung M. Men and oral health: a review of sex and gender differences. Am J Mens Health. 2021;15(3):1–8. doi:10.1177/15579883211016361
47. Su S, Lipsky MS, Licari FW, Hung M. Comparing oral health behaviours of men and women in the United States. J Dent. 2022;122:1–8. doi:10.1016/j.jdent.2022.104157
48. Rajabzadeh M, Hajian-Tilaki K, Ghasempour M. Assessment of knowledge, attitude and practice of medical and dental students about maintaining and disinfecting toothbrushes. Int J Dent Hyg. 2023;21(2):350–356. doi:10.1111/idh.12667
49. Rajeh MT. Gender differences in oral health knowledge and practices among adults in Jeddah, Saudi Arabia. Clin Cosmet Investig Dent. 2022;14:235–244. doi:10.2147/CCIDE.S379171
50. Woelber JP, Bienas H, Fabry G, et al. Oral hygiene-related self-efficacy as a predictor of oral hygiene behaviour: a prospective cohort study. J ClinPeriodontol. 2015;42(2):142–149. doi:10.1111/jcpe.12348
51. Kumar H, Behura SS, Ramachandra S, Nishat R, Dash KC, Mohiddin G. Oral health knowledge, attitude, and practices among dental and medical students in eastern India - A comparative study. J Int Soc Prev Community Dent. 2017;7(1):58–63. doi:10.4103/jispcd.JISPCD_30_17v
52. Santome-Pariona J, Briceño-Vergel G, Córdova-Limaylla N, et al. Factors associated with the level of knowledge about biosafety against covid-19 in Peruvian dental students: a cross-sectional study under a multivariable regression model. Int J Environ Res Public Health. 2023;20(11):1–14. doi:10.3390/ijerph20115938
53. McCambridge J, Witton J, Dr E. Systematic review of the hawthorne effect: new concepts are needed to study research participation effects. J Clin Epidemiol. 2014;67(3):267–277. doi:10.1016/j.jclinepi.2013.08.015
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.