")
Back to Journals » Open Access Journal of Sports Medicine » Volume 15
Impacts of the Early COVID-19 Pandemic on Depressive Symptoms and Mental Health Among Student-Athletes
Authors Ahmad CS, Hellwinkel JE , Ahmed R, Alexander FJ, Reynolds AW, Piasecki DP, Bottiglieri TS, Lynch TS, Popkin CA , Saltzman BM, Trofa DP
Received 10 January 2023
Accepted for publication 6 July 2023
Published 18 March 2024 Volume 2024:15 Pages 19—28
DOI https://doi.org/10.2147/OAJSM.S392977
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Andreas Imhoff
Christopher S Ahmad,1 Justin E Hellwinkel,1 Rifat Ahmed,1 Frank J Alexander,1 Alan W Reynolds,1 Dana P Piasecki,2,3 Thomas S Bottiglieri,1 T Sean Lynch,1 Charles A Popkin,1 Bryan M Saltzman,2,3 David P Trofa1
1Department of Orthopedic Surgery, Columbia University Irving Medical Center, New York, NY, 10032, USA; 2Sports Medicine Center, OrthoCarolina, Charlotte, NC, 28207, USA; 3Musculoskeletal Institute, Atrium Health, Charlotte, NC, 28207, USA
Correspondence: David P Trofa, Columbia University Irving Medical Center, 622 West 168 St, PH-11, New York, NY, 10032, Email [email protected]
Objective: Social distancing protocols due to the COVID-19 pandemic resulted in premature ending of athletic seasons and cancellation of upcoming seasons, placing significant stress on young athletes. Inability to play or forced early retirement has significant consequences on athlete’s mental health, as demonstrated by an extensive body of injury literature. We hypothesize that premature suspension and cancellation of athletic events due to the COVID-19 pandemic leads to higher incidence of depressive symptoms among high-school and collegiate athletes. Further, athletes who strongly derive their sense of self-worth centered around athletics would have higher rates of depressive symptoms.
Methods: High school and collegiate athletes were evaluated for depressive symptoms, emotional health and athletic identity measures through validated assessment instruments from May 2020 through July 2020. The Patient-Reported Outcomes Measurement Information System Depression Computer Adaptive Test (PROMIS-10 Depression CAT), Veterans RAND-12 (VR-12), which comprises both a physical and mental health component, and Athletic Identity Measurement Scale (AIMS) were utilized.
Results: Mental health assessments were completed by 515 athletes (52.4% male, 47.6% female; .84.5% collegiate, 15.5% high school). Female athletes scored significantly worse than males on VR-12 mental health assessments, as well as PROMIS-10 Depression scores; however, males scored significantly lower than females on VR-12 physical health assessments, irrespective of education level. Athletes who had strong associations with athletics as central to their personal identity exhibited worse psychologic impact on VR-12 mental health and PROMIS-10 Depression measures and female athletes in this cohort reported greater depressive symptoms than males.
Conclusion: Social distancing protocols due to the COVID-19 pandemic have limited athlete’s ability to participate in sports at the training and competition level. Higher rates of depressive symptoms in high school and college athletes have resulted among female athletes and those who identify strongly as an athlete.
Keywords: COVID-19, mental health, return to play, involuntary retirement, psychological impact, depression
Introduction
In early 2020, the World Health Organization (WHO) declared a public health emergency on behalf of the coronavirus disease 2019 (COVID-19) outbreak, leading to the systematic cessation of public, social, and sporting events.1 In an effort to promote social distancing, this concurrently stimulated a suspension of seasons and cancellation of competitions for many athletes, including those at the high school and collegiate levels. Many of these athletes rely on scholarships and their athletic performance to prolong careers and shape their personal identities as an athlete. Removal of an athlete’s social support network and normal training routine can be distressing, leading to stress related mood disorders including anxiety and depression.2 Athletes have unique risk factors for depression and other mental health issues compared with non-athletes that can be exacerbated by unforeseen factors such as a season ending injury.3 Country-wide lockdowns have similarly shown to impact training and negatively affect the mental health of athletes.4,5 Disruptions in training have also disrupted athlete’s sleep patterns and quality of sleep.6,7 Loss of a season of play secondary to injury can significantly impact athlete’s confidence in their ability to participate, as evidenced by athletes requiring surgery for a torn anterior cruciate ligament (ACL) who report lower psychological readiness upon clearance for return to sport.8 An extensive body of injury literature shows that inability to participate in sport and forced retirement due to injury can be psychologically devastating, leading to higher rates of depression, anxiety and substance abuse.9 These impacts can be long-lasting and shape the personal identity of these athletes afterward.10 Unplanned cancellation of sporting events due to the COVID-19 pandemic likely has similar psychological consequences, akin to a season-ending or career-ending injury. The lockdown has impacted training intensity of athletes across the world, with team athletes being the most affected.11 In the United States (US), the COVID-19 pandemic caused prompt cessation of athletic events in metropolitan regions in effort to mitigate viral spread.
This study aimed to evaluate the psychological impact of social distancing protocols on disruption of athletic activities at the high school and collegiate level in three Eastern US states due to the COVID-19 pandemic. We hypothesize that athletes missing a season of play will have higher depressive symptoms compared to the general population and those who strongly identify with athletics as central to their personal identity of self are predicted to have higher mental health disturbances compared to their peers.
Materials and Methods
After approval from the Institutional Review Board (IRB) at Columbia University Irving Medical Center, high school and colligate athlete under the care of the primary author’s home institution were recruited via Email to participate in this retrospective case series, and informed consent was obtained from each participant. The study period for data collection occurred from May 2020 through July 2020. Athletes surveyed resided in metropolitan regions of New York, New Jersey and North Carolina, and the majority participated in athletics at the collegiate level. Each completed validated assessment measures to evaluate athlete mental, physical and social health, and the effect of missing an athletic season. Study data and survey responses were collected and managed using REDcap (Research Electronic Data Capture) electronic data capture tools hosted at the primary author’s home institution. REDCap is a secure, web-based application designed to support data capture for research studies, providing 1) an intuitive interface for validated data entry; 2) audit trails for tracking data manipulation and export procedures; 3) automated export procedures for seamless data downloads to common statistical packages; and 4) procedures for importing data from external sources.12 A REDcap link containing the IRB approved Information Sheet to the study and the survey questionnaires was sent in an email. Minors were asked to provide the emails for their parents/legal guardians so that a copy of the information sheet can be sent to them. Participants were instructed to complete the surveys without others nearby, including teammates, or coaches. The study was compliant with the Declaration of Helsinki.
Instrumentation
A measure of health related to quality of life was obtained using the Veterans Rand 12-
Item Health Survey (VR-12) which provides a Physical Component Score (PCS) and Mental Component Score (MCS). In the 18–34-year-old age range, the national average from a nationwide representative sample for mental health score is 41.67 (SD ± 14.31) and physical health score is 40.76 (SD ± 12.98).13 The Patient-Reported Outcomes Measurement Information System (PROMIS®)-10 Depression measure was used to assess symptoms of depression on a 5-point Likert scale (Strong Agree/Agree/Neither Agree nor disagree/Disagree/Strong Disagree). Both measures are generic health-related quality of life measures utilized in varied populations. The Athletic Identity Measure Scale (AIMS) was utilized to assess a respondent’s exclusivity and kinship with the athletic role.14 Participants completed a 10-question survey regarding perception of themselves as athletes, self-worth identifying as an athlete and impact of poor sports performance on their emotional well-being. Scores were rated on a Likert scale from 1 (strongly disagree) to 7 (strongly agree) with an overall range of 10–70, with scores >50 being defined as more strongly related to identification as an athlete.15 AIMS has demonstrated construct validity and reliability in the student-athlete population.16 A basic demographic survey including questions about sport affiliation, training regimens, and access to sports-related equipment before and after COVID-19 restrictions was also obtained from participants.
Statistical Analysis
The data were all checked for incorrect entries, missingness and outliers. All variable distributions were assessed, and the appropriate corresponding statistical procedures were run. Statistical Software SPSS (Version 27.0, IBM Corp., Armonk, NY) was used for statistical analysis. Descriptive statistics were completed for all variables. Levene’s Test for Equality of Variance for Independent t-tests was used to determine if parametric or nonparametric analysis between variables was appropriate for sub-group analysis. One-Way Analysis of Variance (ANOVA) and a post-hoc tests were used to compare means of parametric variables. Multiple Kruskal Wallis test with post-hoc analysis was used for non-parametric comparisons between groups. Statistical significance was determined by a P value of <0.05.
Results
Demographics
A total of 762 athletes received the survey link and 515 athletes from 52 high schools and 17 colleges completed the surveys (52.4% male, 47.6% female) with an average age of 19.47 ± 1.95 (Table 1). High school and collegiate student athletes attended schools in New Jersey, New York, and North Carolina during the 2019–2020 and 2020–2021 academic years. Geographically, 67% of athletes resided in the Northeast, 16.9% in the South, 10.9% in the West, and 5.2% in the Midwest when COVID-19 restrictions were put in place throughout the month of March 2020. The majority of responses were from collegiate athletes (84.5% vs 15.5% high school), and the greatest number of responses were received from lacrosse (16.9%), soccer (13.4%) and track and field (11.3%) athletes. 85.0% reported participation in one sport only, and 15.0% were multisport athletes. When surveyed how the pandemic has affected their training, 85% of athletes reported training in some capacity during the pandemic, but 75.7% report training less overall and 53.6% were unable to participate in sport-specific drills. About 59.4% reported feelings of isolation as a result of inability to play sports and 47.4% feel unprepared to return to sport due to poor training. Consequently, 40.9% believe that they have a higher risk of injury when they return to play. About 98.8% of high-school athletes and 30.6% collegiate athletes reported ambitions of playing their primary sport at the collegiate or professional level, respectively, and 80.2% believe they should be allowed an extra year of eligibility due to the pandemic.
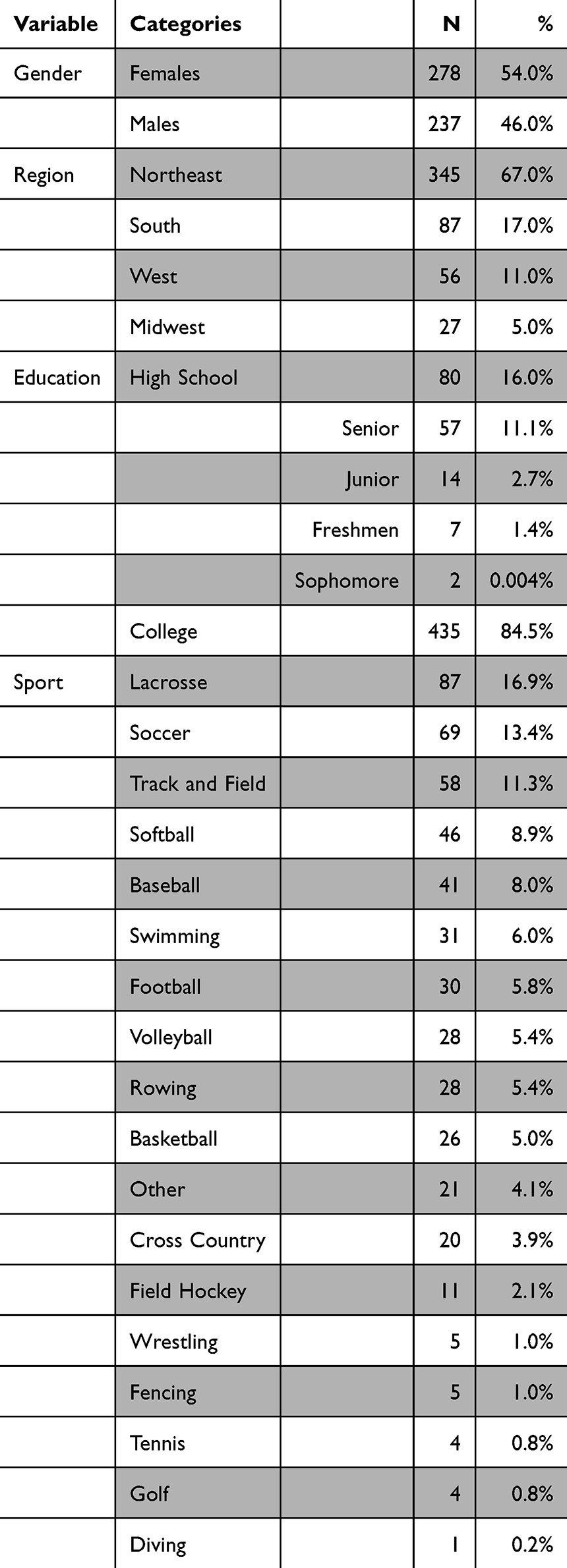 |
Table 1 Demographics of Respondents Including Gender, Region of Residence, Level of Education and Type of Primary Sport Played by Athletes |
VR-12 and PROMIS-10 Depression Scores
VR-12 scores revealed an average mental health score of 46.48 (±7.93) and physical health score of 41.67 (±7.41) which are similar to the national average.13 PROMIS-10 Depression index resulted in overall score of 51.163 (±9.29) for all athletes. When stratified by education level, no differences were noted between collegiate and high-school athletes on the VR-12 mental or physical health scores (46.23 vs 48.03, p = 0.098, 41.65 vs 41.81, p = 0.879, respectively). High-school athletes performed significantly worse on the PROMIS-10 Depression index (51.72 vs 48.15, p = 0.002). Female athletes scored significantly worse than their male counterparts on VR-12 mental health assessments, as well as PROMIS-10 Depression scores (45.63 vs 47.44, p = 0.016 and 53.65 vs 48.25, p < 0.001, respectively), however, males scored significantly lower than females on VR-12 physical health assessments (40.65 vs 42.58, p = 0.006) (Figure 1).
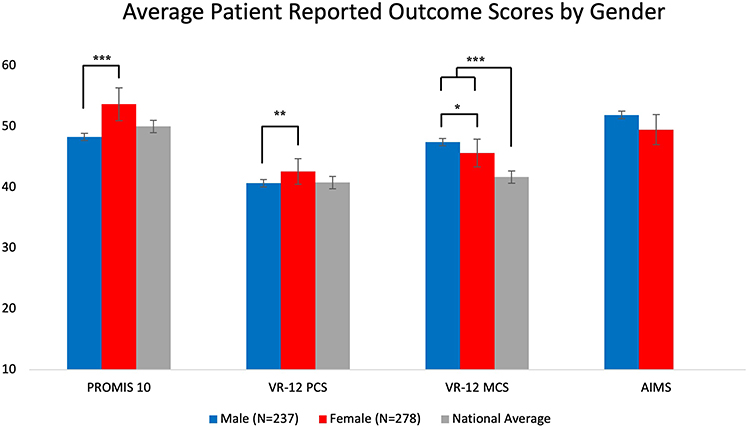 |
Figure 1 Female athletes scored significantly worse than their male counterparts on PROMIS Depression scores (53.65 vs 48.25, p<0.001), however males scored significantly lower than females on VR-12 physical health assessments (40.65 vs 42.58, p=0.006). Female athletes scored significantly lower than male athletes on VR-12 mental health assessments (p=0.016) however both male (47.44) and female (45.63) athletes scored significantly higher than the national average (p<0.001). *p<0.05, **p<0.01, ***p<0.001. |
Responses Stratified by Athletic Identity
About 56.7% of respondents scored ≥50 on the AIMS scale, indicating a strong sense of identity as being an athlete, which comprised 10.1% of high school and 46.6% of collegiate athletes. High-identifying athletes scored significantly worse on VR-12 mental health (45.77 vs 47.43, p = 0.029) and PROMIS-10 Depression (52.146 vs 49.88, p = 0.006) measures but not on VR-12 physical health scores compared to those who did not strongly identify with athletics (Figure 2). Highly identifying female athletes scored significantly higher on PROMIS-10 Depression scores when compared to high identifying male athletes, indicating higher levels of depressive symptoms (54.96 vs 49.22, p < 0.001). More high-identifying athletes reported significantly greater feelings of anger (57.32%), depression (55.79%), difficulty with concentration (55.13%), and feelings of isolation (53.69%) due to their inability to participate in sports (p < 0.001). High identifying athletes also feel more unprepared to return to sports due to their lack of individualized or team training more than lower identifying ones (61.43% vs 51.55%, p = 0.034).
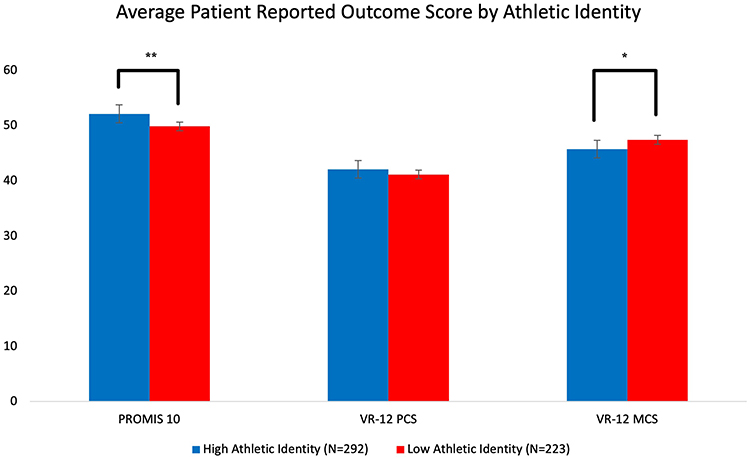 |
Figure 2 High-identifying athletes scored significantly worse on VR-12 mental health (45.77 vs 47.43 p=0.029) and PROMIS Depression (52.15 vs 49.88, p=0.006) measures, but matched on VR-12 physical health scores compared to those who did not strongly identify with athletics (42.07 vs 41.15, p=0.062). *p<0.05, **p<0.01. |
Discussion
Mental health among late adolescents has become a growing concern in recent years and a major focus among high-school and collegiate athletes.3,17 Participation in athletics helps build interpersonal relationships and self-confidence and has demonstrated to be beneficial against the development of stress-related mood disorders, including anxiety, depression, and suicide.18 Additionally, athletes who compete at high levels often build a strong sense of self-worth around athletics, which largely forms their identity. The psychological insult to athletes after lockdown has shown vary based on level of competition, and higher-level athletes may be more protected from psychological injury compared to lower-level athletes.4 Despite the numerous positive mental health benefits of sports participation, the prevalence of anxiety and depressive symptoms among current and former elite athletes is estimated to be 15%–34%.3,9
The COVID-19 pandemic uniquely affected an entire population of healthy high school and collegiate athletes on a scale never seen before, providing researchers with the rare opportunity to study the impact of losing competitive seasons and/or early retirement for many athletes. Further, our results show that 53.6% of athletes report inability to participate in any sport-specific training, resulting in decreased overall training load across all sports. This level of sport-specific training is mildly higher than a recent multinational study of 12,000 athletes which reported only 30–40% of all athletes were able to maintain the same type of sport-specific training.5 Our differences are likely due to a smaller sample size. Although many athletes were unable to participate in sport-specific exercises, modifications to home programs and communication with coaches and athletic trainers during lockdown have been demonstrated as a method to maintain fitness during these types of restrictions.4,19 These modified training regimens are also associated with injuries, primarily to the knees and ankles, likely due to lack of proper equipment and training surface. One study of >600 athletes reported injuries in 18% of all individuals.4 Athletes surveyed in our study participated in a wide variety of individual-level and team-level competitions, and it is likely these environments have some influence on participants' responses. However, these differences are difficult to interpret since the majority of high school and collegiate athletes who participate in individual-level competition (Ie, track and field or swimming) belong to a team associated with their educational institution. This particular study did not aim to analyze differences due to absence of competition versus absence of team interaction (Supplementary Figure 1 and Supplementary Table 1). Inability to participate in sports due to injury has significant psychologic implications for athletes that persist many years later.20,21 Kilic et al prospectively observed professional rugby players over a 12-month period and found those who sustained an injury resulting in losing 28 days of play, had 1.5 odds of developing anxiety or depressive symptoms.22 A separate longitudinal study by these authors demonstrated injury of professional soccer players resulted in a prevalence of mental health disorder symptoms that was 1.8–7 times higher than healthy players.23 Padaki et al evaluated a cohort of student-athletes who sustained anterior cruciate ligament injuries and observed post-traumatic stress disorder symptoms, including avoidance, intrusion and hyperarousal, in 75–87.5% of participants after injury.15 Female athletes were noted to be more affected than male athletes in this study. These data are consistent with previous results by Appaneal et al demonstrating that female athletes tend to develop greater rates of depressive symptoms than males in the acute phase after severe athletic injury.24 We observed overall VR-12 MCS and PCS scores among our respondents were similar to the national average. However, further stratification revealed female athletes scored worse on MCS and PROMIS-10 depression assessments than their male counterparts, indicating greater levels of depressive symptoms, irrespective of education level. Recent studies reveal increased incidence of depressive symptoms on PROMIS-10 Depression scores in athletes after a season-ending injury.25 It is not yet known how long-lasting this condition persists, however the responsiveness of the PROMIS10 Depression tool provides opportunity for monitoring recovery in these athletes. Poor performance on the PROMIS-10 Depression tool after ACL injury has shown to improve to normal population levels after ACL reconstruction.26
Involuntary retirement or career termination from sports is a unique life transition that can be a difficult adjustment for athletes who have not psychologically prepared for this change.21 It has been associated with feelings of hostility and incompetence, low self-esteem, substance abuse, and depressive symptoms both immediately and many years after discontinuation of sport.27–29 The long-term psychological effect of unexpected career termination due to injury in not completely understood at this time. Kerr et al noted former collegiate athletes who sustained career-ending injuries scored significantly worse on VR-12 PCS, but not MCS measurements, 14 years after injury compared to voluntary retirement.30 They did not find differences between male and female athletes, suggesting some degree of recovery of mental health symptoms in female athletes over time. Our study demonstrated lower PCS scores in male athletes compared to female athletes, suggesting greater loss of perceived quality of life due to inability to participate in sports. In larger international cohorts, loss of social interaction with friends and family showed lower satisfaction in quality of life as well.31
Athlete Identity
One of the more devastating aspects of mental health for athletes who can no longer participate in sport is loss of identity as an athlete. The demanding rigors and time commitment of a student-athlete schedule is akin to holding two full-time jobs for some students. The significant time commitment and personal investment in athletics influences the personal and social identity of these athletes. Athletic identity (AI) is most commonly defined as “the degree to which an individual identifies with the athletic role”.14 Identity is comprised of personal, social, and affective components that develop as athletes engage their sport. AI can be a powerful construct to empower athletes to shape self-image and redefine it as demonstrated by paraathletes. The development of the AIMS scoring instrument by Brewer et al helped to characterize the importance of athletics as central to one’s identity as an athlete.14 Participation in sports confers a stronger AI compared to nonparticipants and it has been demonstrated that elite athletes more strongly identify as athletes compared to recreational and nonathletes. Additionally, elite and recreational athletes derive a greater amount of self-worth from their identity as an athlete compared to nonathletes, thus participation at any level can shape one’s identity.32 Importantly, during the late teenage age and early 20’s is the point of development when peer influence and social identity are strongly built, which are the primary years evaluated by our study throughout high school and college-level play.33 Student-athletes have unique psychosocial stressors compared to non-athletes due to the close relationship between athletics with their scholarly activity. Mental health and physical health are closely linked, and the student-athlete population must balance their academic pursuits with athletic pursuits, which can adversely affect stress-management strategies.34–36 Loss of athletic identity is a significant psychological stressor that most commonly occurs after injury or retirement. Park et al evaluated factors impacting athlete transition out of sport and identified 19 significant variables, including athletic identity at the time of retirement and voluntariness of retirement.37 Athletes with stronger AI and those who retired involuntarily due to unexpected circumstances had greater difficulty transitioning careers and had greater development of depressive symptoms after retirement.20 Strong athletic identities can predict anxiety in the post-retirement phase of an athlete’s career, even when retirement is planned.38 Our study revealed athletes who more strongly identified with athletics reported significantly greater feelings of anger, depression, difficulty with concentration and isolation, and also scored worse on VR-12 and PROMIS-10 Depression measures, most notably among female athletes with strong AI. The psychological impact of unexpected inability to play due to COVID-19 has many of the same features as a career-ending injury or forced retirement from sport. Those athletes who strongly identify with athletics carry a greater psychological burden than their peers and may require additional support in their return to play or transition to other careers.
It is important to identify athletes most affected in order to supply proper resources for them. Unfortunately, many high school and collegiate athletes experience a variety of barriers to seeking care for mental health conditions including associated stigma, cultural acceptance, peer influence, fear of retaliation, and gender discrimination.39,40 The stigma of mental health disorders often prevents athletes from seeking help, which prolongs and worsens their condition. An effort should be made to identify those athletes with signs and symptoms of depression and engage them in treatment early. An athlete’s direct support system has a critical role in identifying athletes at risk and helping them get access to the help they need. These include coaches, trainers, teammates, family members, physicians and other sports medicine specialists. In the setting of a global pandemic, it is possible the conversation surrounding stigma may shift due to widespread impact on all athletes. Access to mental health specialists will undoubtedly be beneficial during this transition phase. Psychotherapy, in conjunction with other treatment modalities, can be a very powerful instrument for these athletes.41 A multimodal approach is commonly used to engage a support system and help the athlete return to play or transition to the next phase of their career. Individualized therapies help maximize benefit of treatment in particular subsets of athletes. For example, differing psychologic effects between male and female athletes were found in our study and prior work has suggested male and female athletes psychologically recover differently after injury.42 Unique cohorts like elite athletes also benefit from individualized psychotherapy treatment strategies for mental health conditions. Recently, the International Olympic Committee generated a consensus group to optimize treatment strategies for addressing mental health in this population.43
Transition to Next Phase of Career
Transition to the next phase of career is a critical component in the recovery process for athletes who have been unable to play due to the COVID-19 pandemic. Athletes who return to sport will benefit from proper physical and psychological support prior to beginning play. Li et al demonstrated that collegiate athletes who report preseason anxiety or depressive symptoms have a 2.3 times increased risk of sustaining an injury in the subsequent season.44 Our study suggests that female athletes and those with high athletic identities may be at increased risk based on performance of mental health measures. Studies of international competition and Olympic-level athletes report lower levels of perceived stress in female athletes compared to male athletes.45 This discrepancy is an area for future studies to help determine what factors may protect one population or create vulnerability for the other. Further, approximately 40% of the athletes in our survey indicated fear of injury upon return to play. One strategy that can be helpful in the recovery process is engagement of athletes’ support system and use of positive language as they return to play. Emphasis on positive language and goal setting can provide benefit for athletes to refine their self-image and confidence after injury.46 Psychologic readiness to return to play and impact of therapeutic interventions can be difficult to quantify, particularly in the setting of recovering from a global pandemic. Validated measures that are responsive to therapeutic intervention, such as the PROMIS-10 Depression scale, are useful instruments to help monitor players' rehabilitation progress to guide return to play protocols.47
Retirement from sport is a major life event for many athletes and is associated with psychologic distress. Retirement planning and anticipation of life away from sports helps athletes’ transition to the next phase of their careers and find new value in their sense of self.10,28,48 Conversely, involuntary retirement is associated with significant psychologic disturbances, including anxiety, depression, substance abuse and eating disorders, which can last for many years later.9 Loss of identity is thought to be a substantial contributor to this transition. Athletes with a single strong identity as an athlete are at risk for not coping well with involuntary retirement from sport.10 The COVID-19 pandemic forced involuntary retirement upon a large number of athletes throughout the world. Eighty-five percent of athletes in our study identified as single-sport athletes and 56.7% highly identified as athletes on the AIMS assessment. These individuals should be recognized and provided with adequate support to aide in transition away from sport. Schools, coaches, family, and an athlete’s social circle can assist with connecting at-risk athletes with mental health counselors, career advisors and life coaches among others to improve their long-term metal health.
Strengths
The primary strengths of our study were the use of three separate instruments to evaluate depression, mental health and sense of individual identity. We collected data from many participants across a wide age range in our target demographic who participate in variety of sports. We were able to obtain data from athletes whose season was prematurely terminated and from others who were unable to play an entire season due to the pandemic. We were also able to capture data from athletes who would continue playing their sport and from athletes who would be forced into involuntary retirement due to the pandemic.
Limitations
Our study focused primarily on high school and collegiate athletes cared for by the author’s institution, the majority of which reside within the Northeast. It is likely that different regions throughout the country and recreational athletes may respond differently to these measures. The primary limitation of this study includes the use of self-reported data through surveys, which has the potential to introduce response and recall bias. It is possible that athletes surveyed after a longer period in lockdown would respond differently to the survey and the instruments utilized to assess mental and physical well-being may reveal more information about these athletes over time. Furthermore, since the collection of these data, there have been additional psychometric testing instruments that have been validated for use with the athlete population, which will be useful for future studies. Due to social stigma associated with mental health in athletes, participants have the potential to answer dishonestly or may have poor understanding of their own mental health. Similarly, our study is also vulnerable to social desirability bias, and for respondents to answer in a way, they believe their teammates would. Athletes were asked to complete surveys alone and responses remained anonymous to reduce these sources of bias.
Conclusion
The COVID-19 pandemic limited athletic participation in competitive and recreational sports at high school and collegiate levels. Higher rates of depressive symptoms in high school and college athletes have resulted among female athletes and those who identify strongly as an athlete.
Disclosure
Dr T Sean Lynch reports personal fees from Smith and Nephew, outside the submitted work; Dr Charles A Popkin reports Research Support from Arthrex and Research Support and Educational Activities from Gotham Surgical, during the conduct of the study. None of the authors have conflicts of interest related to the data presented in this manuscript.
References
1. Golberstein E, Wen H, Miller BF. Coronavirus Disease 2019 (COVID-19) and mental health for children and adolescents. JAMA Pediatr. 2020;174:819. doi:10.1001/jamapediatrics.2020.1456
2. Toresdahl BG, Asif IM. Coronavirus Disease 2019 (COVID-19): considerations for the competitive athlete. Sports Health. 2020;12(3):221–224. doi:10.1177/1941738120918876
3. Wolanin A, Gross M, Hong E. Depression in athletes: prevalence and risk factors. Curr Sports Med Rep. 2015;14(1):56–60. doi:10.1249/JSR.0000000000000123
4. Washif JA, Kok LY, James C, et al. Athlete level, sport-type, and gender influences on training, mental health, and sleep during the early COVID-19 lockdown in Malaysia. Front Physiol. 2022;13:1093965. doi:10.3389/fphys.2022.1093965
5. Washif JA, Farooq A, Krug I, et al. Training during the COVID-19 lockdown: knowledge, beliefs, and practices of 12,526 athletes from 142 countries and six continents. Sports Med. 2022;52(4):933–948. doi:10.1007/s40279-021-01573-z
6. Romdhani M, Rae DE, Nedelec M, et al. COVID-19 lockdowns: a worldwide survey of circadian rhythms and sleep quality in 3911 athletes from 49 countries, with data-driven recommendations. Sports Med. 2022;52(6):1433–1448. doi:10.1007/s40279-021-01601-y
7. Romdhani M, Fullagar HHK, Vitale JA, et al. Lockdown duration and training intensity affect sleep behavior in an international sample of 1454 elite athletes. Front Physiol. 2022;13:904778. doi:10.3389/fphys.2022.904778
8. McPherson AL, Feller JA, Hewett TE, Webster KE. Smaller change in psychological readiness to return to sport is associated with second anterior cruciate ligament injury among younger patients. Am J Sports Med. 2019;47(5):1209–1215. doi:10.1177/0363546519825499
9. Gouttebarge V, Castaldelli-Maia JM, Gorczynski P, et al. Occurrence of mental health symptoms and disorders in current and former elite athletes: a systematic review and meta-analysis. Br J Sports Med. 2019;53(11):700–706. doi:10.1136/bjsports-2019-100671
10. Stambulova N, Alfermann D, Statler T, Côté J. ISSP Position stand: career development and transitions of athletes. Int J Sport Exercise Psychol. 2009;7(4):395–412. doi:10.1080/1612197X.2009.9671916
11. Washif JA, Sandbakk O, Seiler S, et al. COVID-19 lockdown: a global study investigating the effect of athletes’ sport classification and sex on training practices. Int J Sports Physiol Perform. 2022;17(8):1242–1256. doi:10.1123/ijspp.2021-0543
12. Harris PA, Taylor R, Thielke R, Payne J, Gonzalez N, Conde JG. Research electronic data capture (REDCap)--a metadata-driven methodology and workflow process for providing translational research informatics support. J Biomed Inform. 2009;42(2):377–381. doi:10.1016/j.jbi.2008.08.010
13. Selim AJ, Rogers W, Fleishman JA, et al. Updated U.S. population standard for the veterans RAND 12-item health survey (VR-12). Qual Life Res. 2009;18(1):43–52. doi:10.1007/s11136-008-9418-2
14. Brewer BW, Van Raalte JL, Linder DE. Athletic identity: Hercules’ muscles or achilles heel? Int J Sport Psychol. 1993;24(2):237–254.
15. Padaki AS, Noticewala MS, Levine WN, Ahmad CS, Popkin MK, Popkin CA. Prevalence of Posttraumatic Stress Disorder symptoms among young athletes after anterior cruciate ligament rupture. Orthop J Sports Med. 2018;6(7):2325967118787159. doi:10.1177/2325967118787159
16. Mitchell T, Rongen F, Perry J, Littlewood M, Till K. Validation of the athletic identity measurement scale in youth academy soccer players. J Athlete Development and Experience. 2021;3(3):4. doi:10.25035/jade.03.03.04
17. Wolanin A, Hong E, Marks D, Panchoo K, Gross M. Prevalence of clinically elevated depressive symptoms in college athletes and differences by gender and sport. Br J Sports Med. 2016;50(3):167–171. doi:10.1136/bjsports-2015-095756
18. Rao AL, Asif IM, Drezner JA, Toresdahl BG, Harmon KG. Suicide in national collegiate athletic association (NCAA) athletes: a 9-year analysis of the NCAA resolutions database. Sports Health. 2015;7(5):452–457. doi:10.1177/1941738115587675
19. Washif JA, Mujika I, DeLang MD, et al. Training practices of football players during the early COVID-19 lockdown worldwide. Int J Sports Physiol Perform. 2023;18(1):37–46. doi:10.1123/ijspp.2022-0186
20. Sanders G, Stevinson C. Associations between retirement reasons, chronic pain, athletic identity, and depressive symptoms among former professional footballers. Eur J Sport Sci. 2017;17(10):1311–1318. doi:10.1080/17461391.2017.1371795
21. Young JA, Pearce AJ, Kane R, Pain M. Leaving the professional tennis circuit: exploratory study of experiences and reactions from elite female athletes. Br J Sports Med. 2006;40(5):477–482. doi:10.1136/bjsm.2005.023341
22. Kilic O, Hopley P, Kerkhoffs G, et al. Impact of concussion and severe musculoskeletal injuries on the onset of mental health symptoms in male professional rugby players: a 12-month study. BMJ Open Sport Exerc Med. 2019;5(1):e000693. doi:10.1136/bmjsem-2019-000693
23. Kilic O, Aoki H, Goedhart E, et al. Severe musculoskeletal time-loss injuries and symptoms of common mental disorders in professional soccer: a longitudinal analysis of 12-month follow-up data. Knee Surg Sports Traumatol Arthrosc. 2018;26(3):946–954. doi:10.1007/s00167-017-4644-1
24. Appaneal RN, Levine BR, Perna FM, Roh JL. Measuring postinjury depression among male and female competitive athletes. J Sport Exerc Psychol. 2009;31(1):60–76. doi:10.1123/jsep.31.1.60
25. Challa S, Holliday M, Bartolomei K, Bartolomei J. Assessing elite athletes using PROMIS tools: the STEALTH project (student athlete health assessment). Orthop J Sports Med. 2020;8(7 suppl6):2325967120S2325900399. doi:10.1177/2325967120S00399
26. Kuhns B, Reuter J, Rouse L, et al. The effect of depression on patient reported outcomes measurement and information system computer adaptive test (PROMIS-CAT) scores and return-to-sport following ACL reconstruction. Orthop J Sports Med. 2020;8(7 suppl6):2325967120S2325900460. doi:10.1177/2325967120S00460
27. Erpič S C, Wylleman P, Zupančič M. The effect of athletic and non-athletic factors on the sports career termination process. Psychol Sport Exercise. 2004;5(1):45–59. doi:10.1016/S1469-0292(02)00046-8
28. Esopenko C, Coury JR, Pieroth EM, Noble JM, Trofa DP, Bottiglieri TS. The psychological burden of retirement from sport. Curr Sports Med Rep. 2020;19(10):430–437. doi:10.1249/JSR.0000000000000761
29. Wippert P-M, Wippert J. The effects of involuntary athletic career termination on psychological distress. J Clinic Sport Psychol. 2010;4(2):133–149. doi:10.1123/jcsp.4.2.133
30. Kerr ZY, DeFreese JD, Marshall SW. Current physical and mental health of former collegiate athletes. Orthop J Sports Med. 2014;2(8):2325967114544107. doi:10.1177/2325967114544107
31. Ammar A, Chtourou H, Boukhris O, et al. COVID-19 home confinement negatively impacts social participation and life satisfaction: a worldwide multicenter study. Int J Environ Res Public Health. 2020;17(17):6237. doi:10.3390/ijerph17176237
32. Lamont-Mills A, Christensen SA. Athletic identity and its relationship to sport participation levels. J Sci Med Sport. 2006;9(6):472–478. doi:10.1016/j.jsams.2006.04.004
33. Warriner K, Lavallee D. The retirement experiences of elite female gymnasts: self identity and the physical self. J Appl Sport Psychol. 2008;20(3):301–317. doi:10.1080/10413200801998564
34. Grubic N, Jain S, Mihajlovic V, Thornton JS, Johri AM. Competing against COVID-19: have we forgotten about student-athletes’ mental health? Br J Sports Med. 2021;55(17):950–951. doi:10.1136/bjsports-2021-104218
35. Matsushita K, Grubic N. Bridging the gap: considerations for the design of effective and tailored student mental health supports. Can J Psychiatry. 2023;68(2):130–131. doi:10.1177/07067437221125303
36. Grubic N, Badovinac S, Johri AM. Student mental health in the midst of the COVID-19 pandemic: a call for further research and immediate solutions. Int J Soc Psychiatry. 2020;66(5):517–518. doi:10.1177/0020764020925108
37. Park S, Lavallee D, Tod D. Athletes’ career transition out of sport: a systematic review. Int Rev Sport Exercise Psychol. 2013;6(1):22–53. doi:10.1080/1750984X.2012.687053
38. Giannone ZA, Haney CJ, Kealy D, Ogrodniczuk JS. Athletic identity and psychiatric symptoms following retirement from varsity sports. Int J Soc Psychiatry. 2017;63(7):598–601. doi:10.1177/0020764017724184
39. Castaldelli-Maia JM, Gallinaro J, Falcão RS, et al. Mental health symptoms and disorders in elite athletes: a systematic review on cultural influencers and barriers to athletes seeking treatment. Br J Sports Med. 2019;53(11):707–721. doi:10.1136/bjsports-2019-100710
40. Gulliver A, Griffiths KM, Christensen H. Barriers and facilitators to mental health help-seeking for young elite athletes: a qualitative study. BMC Psychiatry. 2012;12(1):157. doi:10.1186/1471-244X-12-157
41. Stillman MA, Glick ID, McDuff D, et al. Psychotherapy for mental health symptoms and disorders in elite athletes: a narrative review. Br J Sports Med. 2019;53(12):767. doi:10.1136/bjsports-2019-100654
42. Lisee CM, DiSanti JS, Chan M, et al. Gender differences in psychological responses to recovery after anterior cruciate ligament reconstruction before return to sport. Journal of Athletic Training. 2020;55(10):1098–1105. doi:10.4085/1062-6050-558.19
43. Reardon CL, Hainline B, Aron CM, et al. Mental health in elite athletes: international Olympic committee consensus statement. Br J Sports Med. 2019;53(11):667–699. doi:10.1136/bjsports-2019-100715
44. Li H, Moreland JJ, Peek-Asa C, Yang J. Preseason anxiety and depressive symptoms and prospective injury risk in collegiate athletes. Am J Sports Med. 2017;45(9):2148–2155. doi:10.1177/0363546517702847
45. Washif JA, Ammar A, Trabelsi K, et al. Regression analysis of perceived stress among elite athletes from changes in diet, routine and well-being: effects of the COVID-19 lockdown and “bubble” training camps. Int J Environ Res Public Health. 2021;19(1):402. doi:10.3390/ijerph19010402
46. D’Astous E, Podlog L, Burns R, Newton M, Fawver B. Perceived competence, achievement goals, and return-to-sport outcomes: a mediation analysis. Int J Environ Res Public Health. 2020;17(9):2980. doi:10.3390/ijerph17092980
47. Fisk F, Franovic S, Tramer JS, et al. PROMIS CAT forms demonstrate responsiveness in patients following arthroscopic rotator cuff repair across numerous health domains. J Shoulder Elbow Surg. 2019;28(12):2427–2432. doi:10.1016/j.jse.2019.04.055
48. Lally P. Identity and athletic retirement: a prospective study. Psychol Sport Exercise. 2007;8(1):85–99. doi:10.1016/j.psychsport.2006.03.003
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.