")
Back to Journals » Risk Management and Healthcare Policy » Volume 17
Importance-Performance Analysis of Patient-Safety Nursing in the Operating Room: A Cross-Sectional Study
Received 7 December 2023
Accepted for publication 15 March 2024
Published 26 March 2024 Volume 2024:17 Pages 715—725
DOI https://doi.org/10.2147/RMHP.S450340
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Gulsum Kubra Kaya
Jieun Shin,1 Nam-Yi Kim2
1Department of Biomedical Informatics, College of Medicine, Konyang University, Daejeon, Republic of Korea; 2Department of Nursing, Konyang University, Daejeon, Republic of Korea
Correspondence: Nam-Yi Kim, Department of Nursing, Konyang University, Daejeon, 35365, Republic of Korea, Tel +82-42-600-8586, Fax +82-42-600-8555, Email [email protected]
Purpose: This study attempted to assess the perceived importance and performance of patient-safety nursing among operating room (OR) nurses and to identify the “concentrate here” level using importance-performance analysis (IPA). The goal was to identify the educational priorities of patient-safety nursing and to use it as foundational data to develop educational programs.
Methods: The IPA of patient-safety nursing (infection control, patient identification, specimen management, surgical coefficient, medical equipment and supplies, high-alert medicines, and damage prevention) was surveyed online for nurses in general hospitals in Korea, and the data of 47 participants were analyzed. Differences in the importance and performance of patient-safety nursing were analyzed using Wilcoxon signed rank test, and IPA was conducted to identify areas on which improvement efforts should be focused.
Results: Within the six areas of OR patient-safety nursing, notable differences in importance and performance were observed in infection control and surgical count areas. The IPA revealed specific items that require “concentrate here”, including handwashing, checking the cleanliness and sterility of medical equipment, and conducting 5-Rights checks before administering high-alert medications.
Conclusion: Regular training for OR nurses should encompass preoperative, intraoperative, and postoperative infection control, as well as appropriate surgical counts. In particular, training, monitoring, feedback, and intervention should be provided on hand hygiene, sterilization maintenance, and accurate administration of high-alert medications, which are items included in “concentrate here”.
Keywords: patient safety, perioperative, education, importance-performance analysis, nursing
Introduction
As an important healthcare issue worldwide, patient safety is defined as an event or situation that can cause unnecessary harm to patients.1 In particular, patient-safety incidents in operating rooms (ORs) require special attention, since they can cause fatal and irreversible conditions.2 There are various types of patient-safety incidents in ORs, namely wrong-site/patient surgery, postoperative residual foreign bodies, errors in surgical instrument reprocessing, pressure ulcers, fires, and hypothermia.3 Wrong-site surgery is reported to occur in 4.5 out of 10,000 cases,4 while postoperative residual foreign bodies are reported to occur in 1 out of 6975 cases.5 The Joint Commission on Accreditation of Health Organization (JCAHO) emphasizes the importance of teamwork, constant quality control, prompt communication, and information-sharing among healthcare professionals to ensure the safety of surgical patients.6 Moreover, although the Association of PeriOperation Registered Nurses (AORN) has recommended rapid streamlining and standardization of tasks to detect and correct errors that occur during surgery,7 patient-safety incidents nevertheless continue to occur in ORs. A systematic literature review of adverse events in hospitals reported that surgery-related incidents accounted for 39.6% of all incidents.8 In Korea, efforts are being made to improve the quality of patient safety through the evaluation of medical institutions. However, the number of patient safety incidents in ORs continues to rise by 2.3% per year.9 Therefore, patient-safety nursing in ORs is vital when it comes to preventing possible harm or incidents.
Nurses constitute the largest proportion of healthcare workers in the OR, with OR nurses acting as a conduit in the delivery of all medical services.10 Accordingly, OR nurses engage in patient safety nursing, delivering both direct and indirect nursing to patients. OR nurses are responsible for maintaining accurate records and smooth operation based on speed, expertise, and advanced technology.11,12 Patient safety is one of the most important responsibilities of OR nursing. They are responsible for accurately counting surgical instruments, preventing patient damage during all stages of the procedure, and accurately checking patients before surgery to ensure patient safety.12 They must also undertake additional activities to guarantee the safety of the surgical patients, such as accurate management of specimens collected during surgery, handling of instruments and equipment used in surgery, and infection control.13 Despite technological and intellectual advances, healthcare remains dependent on human intervention; thus, the perception and performance of nurses in ORs is crucial to ensuring patient safety, as they deliver direct and indirect care immediately next to the patient and contribute the most to patient safety. However, education and training on patient safety nursing in ORs are not systematically implemented in Korea; rather, they are partially conducted by hospitals. While it is accurate that patient safety nursing education programs should align with the unique characteristics of each hospital’s OR environment (structure, guidelines, composition of healthcare worker, etc.), there is a pressing need to establish a foundational education program for basic patient safety nursing in the OR. Therefore, it is necessary to first check the priority of the items for patient safety nursing in the OR. A number of preceding studies on OR patient-safety nursing have reported the influence of patient-safety culture.12,14,15 Other related factors included the experience of patient-safety incidents,16 the hospital safety system,13 and clinical experience.17 Although previous studies have suggested factors related to patient-safety nursing performance, it is necessary to categorize the key items of patient-safety nursing and specifically examine differences in perception and performance so as to formulate effective OR patient-safety nursing training. Importance-performance analysis (IPA) is an effective tool for identifying items that require additional training and priorities for training by visualizing the differences in importance and performance of each item in four quadrants on the x- and y-axes, allowing for easy visual comparison.18 By identifying the differences between how nurses perceive the importance of OR patient-safety nursing and how much they actually perform it, it will be possible to ascertain the areas that need concentration and reinforcement in OR patient-safety nursing training. Therefore, this study aimed to gather basic data for future educational data development by confirming the importance and performance of patient-safety nursing by OR nurses and using IPA to confirm the educational needs and priorities of patient-safety nursing in OR.
Materials and Methods
Research Design
This descriptive study attempted to identify the importance and performance of OR nurses in patient-safety nursing and to provide a basis for the development of future educational materials by identifying the need for training in OR patient-safety nursing through the use of IPA.
Participants and Data Collection
Participants were OR nurses. The inclusion criteria were nurses who 1) worked in the OR, 2) had more than 6 months of working experience, and 3) understood the purpose of the study and agreed to voluntary participate. The exclusion criteria were nurses who 1) did not currently work in the OR, 2) had less than 6 months of working experience, and 3) did not agree to participate in the study. Approval was obtained from the Institutional Review Board (IRB) of K University before the start of the study (IRB No.: KYH 2023-02-017). Regarding the number of subjects, the minimum required sample size was 44 based on an effect size of 0.5, a significance level of 0.05, and a power of 0.9 in a t-test using G*Power 3.1.9. The final number of subjects was determined to be 48 considering a 10% dropout rate.
Data were collected between June 1 and June 30, 2023, using an online questionnaire. Research participants were recruited by uploading recruitment notices and questionnaire links to online bulletin boards (at 2 general hospitals) freely available to nurses. The recruitment announcement outlined the purpose of the study, the inclusion and exclusion criteria, and ensured autonomy of participation by allowing the individuals who consented to proceed to the survey stage. A total of 48 participants completed the survey, but only the data of 47 participants were used in the final analysis owing to one participant not responding to the importance and performance questions.
Instruments
Patient-Safety Nursing
To measure the patient-safety nursing practices of OR nurses, three questions on high-risk drug management were revised and supplemented based on the International Patient Safety Goals (IPSGs) within the tools developed by Kim and Jeong.13 To enhance clarity, the word “drug” was modified to “high-alert medications”, and “two nurses” was specifically described as “scrub nurses and circulating nurses”. Seven subsections were created by adding high-alert medications as a sub-factor. To examine whether each item in the revised and supplemented tools was related to the characteristics to be measured, content validation was conducted with two PhDs in nursing, two nurses with more than 10 years of clinical experience in ORs, and two managers from the patient-safety department of a university hospital. All of the items were found to have a content validity index (CVI) of 0.8 or higher, making them suitable for use.
The tool used in this study consisted of 39 items categorized into seven subsections: infection control (six items), patient identification (five items), specimen management (five items), surgical counting (eight items), medical equipment and supplies (four items), high-alert medications (four items), and damage prevention (seven items). Each item in the survey was measured on a 5-point Likert scale, separating importance from performance. Importance was measured on a scale of 1 (not important at all) to 5 (very important), based on the degree of perceived importance of the item in OR patient-safety nursing. Performance was measured on a scale of 1 (never) to 5 (always) based on the extent to which the respondents performed OR patient-safety nursing. Cronbach’s α was 0.91 in the current study for both importance and performance.
Sociodemographic Characteristics of the Subjects
The sociodemographic characteristics of the subjects were examined in terms of sex, age, years of experience in the OR, number of times they had received training on surgical patient safety in the last three months, experience with patient-safety incidents, and experience with domestic medical center evaluation and accreditation. Considering the normality of the subjects by group, age, experience in the OR, and number of times they had received training, they were divided into two groups.
Data Analysis
The collected data were analyzed using SPSS 25.0 (SPSS; IBM, Armonk, NY, USA). The general characteristics of the participants were identified by frequency and percentage, while the differences in patient-safety nursing based on the general characteristics of the participants were analyzed using the Mann–Whitney U-test—a non-parametric method. Differences in the importance and performance of patient-safety nursing were analyzed using a Wilcoxon signed rank test, and IPA was performed for visualization. The centerline of the IPA matrix was divided into four levels—“Keep up the good work”, “Concentrate here”, “Possible overkill”, and “Low priority”—based on the mean of importance and performance.19
Results
General Characteristics of the Subjects
The subjects’ general characteristics included sex, age, experience in the OR, number of times they had received training on surgical patient safety, experience in medical center evaluation and accreditation, and experience in patient-safety incidents. Overall, 89.4% of the subjects were female, with a mean age of 36.60±8.80 years. The average number of years of experience in the OR was 13.48±10.18, with 42.6% having less than 10 years and 57.4% having more than 10 years. Regarding the number of times they received training on surgical patient safety, 61.7% had received one or fewer training sessions, and 38.3% had received two or more. Additionally, 85.1% had experience with medical center evaluation and accreditation, while 36.2% had experience with patient-safety incidents (Table 1).
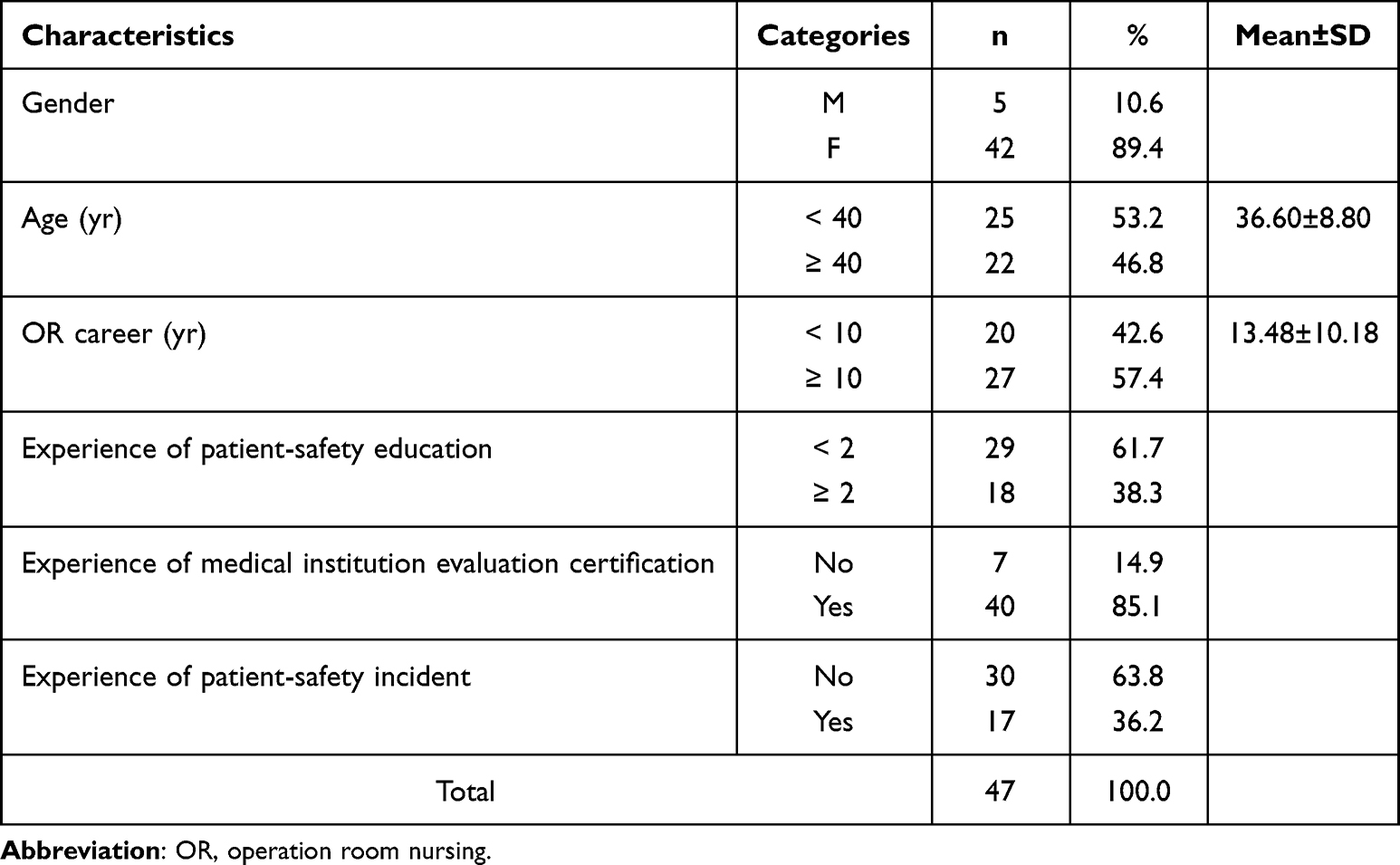 |
Table 1 General Characteristics of Participants (n=47) |
Differences in the Importance and Performance of or Patient-Safety Nursing
The median importance of OR patient-safety nursing was 4.85 (Mean±SD: 4.79±0.22), while the median performance was 4.82 (4.78±0.24); the difference between importance and performance was not statistically significant. When divided into seven sub-factors of OR patient-safety nursing, infection management (z=2.144, p=0.032) and surgical count (z=2.110, p=0.035) showed a statistically significant difference in importance and performance. Infection management recorded a median importance of 4.83 (4.68±0.36) and a median performance of 4.67 (4.54±0.46), which was lower than importance. Surgical count recorded a median importance of 4.88 (4.77±0.26) and a median performance of 5 (4.82±0.29), which was higher than importance (Table 2).
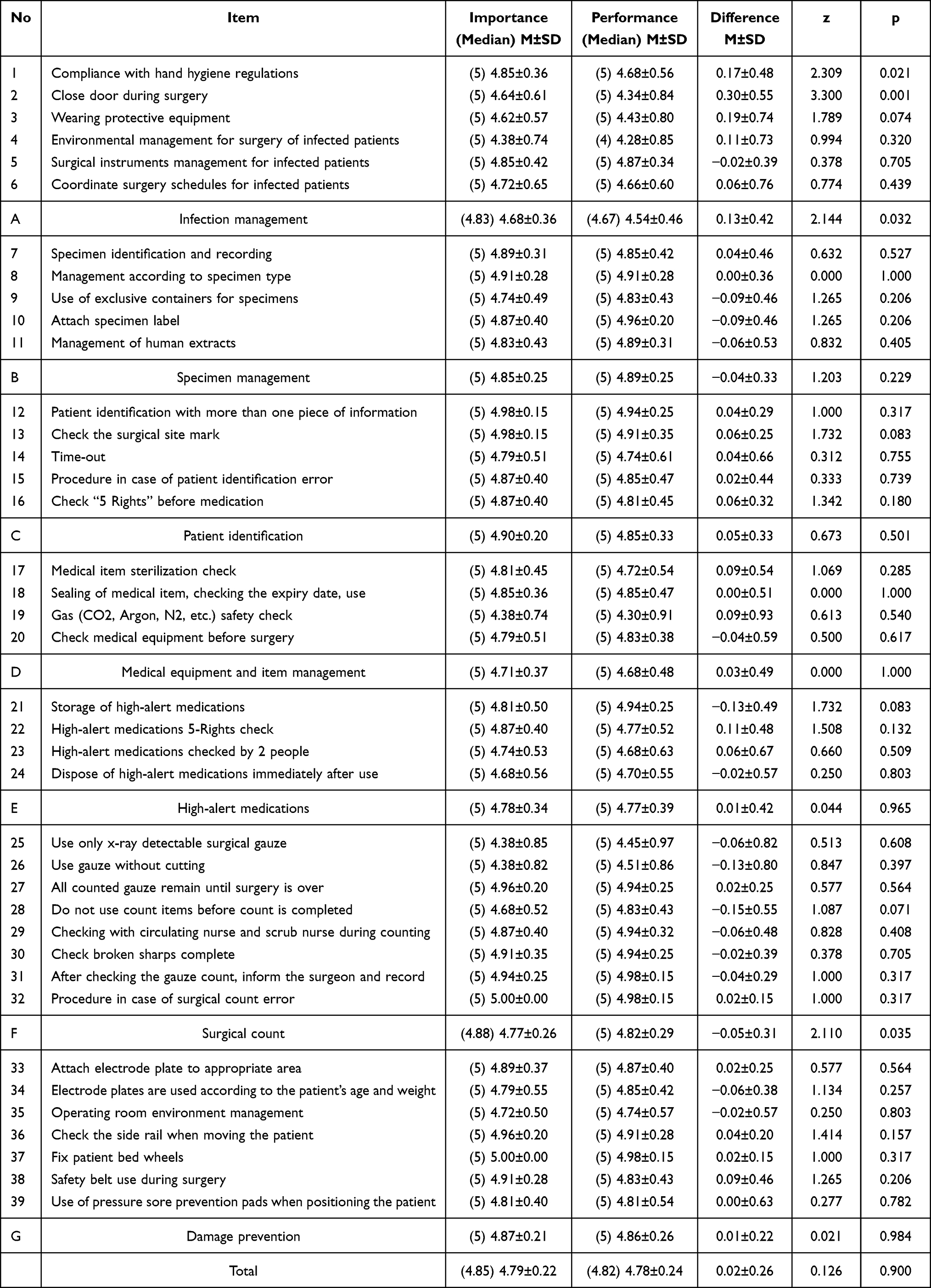 |
Table 2 Importance-Performance Comparison |
The Importance and Performance of or Patient-Safety Nursing by General Characteristics
When analyzing the differences in importance and performance according to general characteristics, only some importance results exhibited differences. The importance of OR patient-safety nursing showed a statistically significant difference in training experience (z=−2.322, p=0.020), with a median of 4.82 (4.74±0.23) for those with two or more training experiences compared to 4.85 (4.87±0.17) for those with one or fewer training experiences. There were no differences between the groups in terms of sex, age, years of experience in the OR, medical center evaluation and accreditation experience, or experience with patient-safety incidents (Table 3).
 |
Table 3 Differences in Importance and Performance According to General Characteristics (n=47) |
The Needs for Training in or Patient-Safety Nursing Based on the IPA
For the IPA, a two-dimensional matrix with importance as the x-axis and performance as the y-axis was drawn, and the points where the scores of importance and performance of OR patient-safety nursing met were placed in four quadrants, centered on the mean of 4.79 for importance and 4.78 for performance. Items with a score of 4.79 or higher were considered to be of high perceived importance, and items scoring 4.79 or lower were considered of low perceived importance. Regarding performance, items with a score of 4.78 or higher were considered to be of high perceived performance, and those scoring 4.78 or lower were considered of low perceived performance (Figure 1). Based on the IPA analysis, the areas on which to focus improvement efforts (“Concentrate here”) that showed high importance but low performance were “I follow the hospital’s hand hygiene protocol (Item 1)” in the infection control area, “I check the cleanliness and sterility of medical equipment before use (Item 17)” in the supplies management area, and “I check the 5 Rights before administering high-alert medications to surgical patients (Item 22)” in the high-alert medications area (Figure 2).
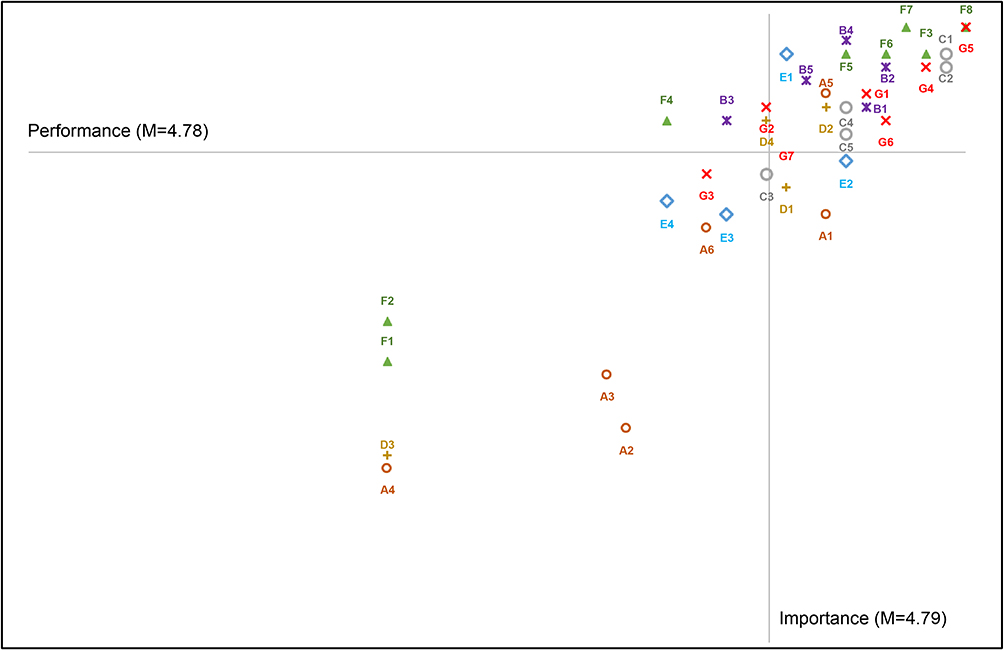 |
Figure 1 Importance-performance analysis of patient-safety nursing. Notes: A: infection management; B: specimen management; C: patient identification; D: medical equipment and item management; E: high-alert medications; F: surgical count; G: damage prevention. |
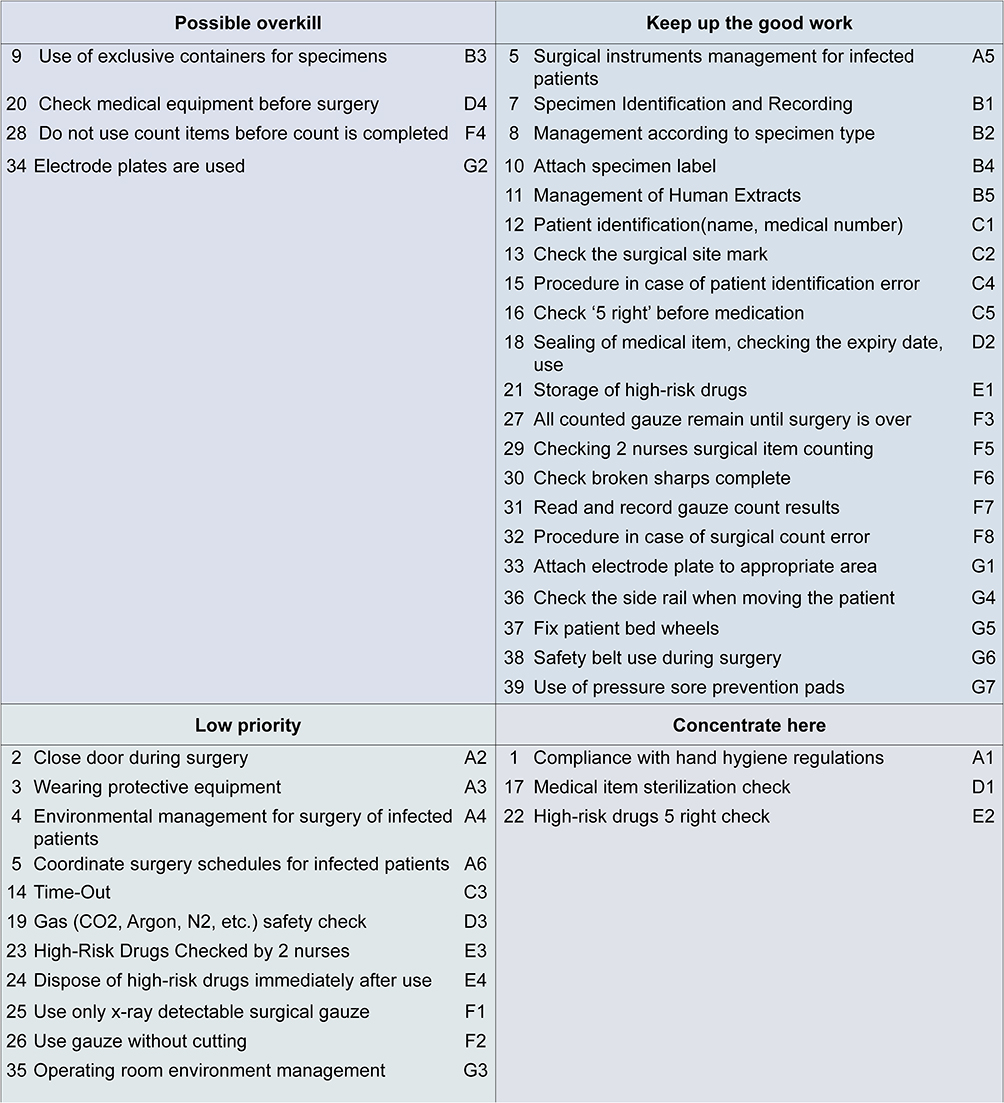 |
Figure 2 Patient-safety nursing matrix. Notes: A: infection management; B: specimen management; C: patient identification; D: medical equipment and item management; E: high-alert medications; F: surgical count; G: damage prevention. |
Discussion
This study identified the importance and performance of patient-safety nursing among OR nurses and determined the need for training in OR patient-safety nursing using IPA. The study’s significance is that the importance and performance of patient-safety nursing, as perceived by OR nurses, were compared and analyzed to identify areas for intensive improvement.
The mean performance of OR nurses in patient-safety nursing was 4.78, which was higher than the 4.15 and 4.30 reported by studies concerning hospital nurses.20,21 The importance of patient-safety nursing in the OR has been repeatedly emphasized, because patient safety incidents can cause fatal and irreversible conditions for patients. Patient-safety incidents in the OR have led to medical disputes and have been publicized,22,23 while surgery-related patient-safety incidents are designated critical events that require mandatory reporting in the Korean Patient Safety Incident Report.24 Therefore, it is reasonable to assume that the level of importance and performance of patient-safety nursing, as perceived by OR nurses, is higher than that perceived by general nurses.
Based on general characteristics, the perceived importance of OR patient-safety nursing varied according to training experience. The group with more training in OR patient-safety nursing had a higher level of perceived importance, confirming the importance of consistent training. Previous studies have shown that training affects nurses’ knowledge, awareness, and performance.25 However, in terms of performance, while the group with more training scored higher, there was no statistically significant difference, unlike in preceding studies. It is necessary to expand the number of subjects and repeat the study in the future, since the number of subjects in this study differs from that in previous studies.
The sub-factors that showed differences in the importance and performance of patient-safety nursing in the OR were infection control and surgical count. Among the sub-factors of patient-safety nursing in this study, infection control was also the one with the lowest level of performance, suggesting that interventions are needed. Infection control in the OR includes the application of surgical asepsis to surgical patients, ensuring that the OR environment (maintaining positive pressure) does not cause infection, and ensuring that surgery on a patient who already has an infectious disease does not cause transmission of the disease to other surgical patients. While many factors contribute to postoperative infections, including length of surgery, patient condition, surgical asepsis by healthcare providers, and antibiotic use,26 infection prevention activities by OR nurses throughout the surgical procedure are key factors. Examples include surgical hand washing, ensuring that sterile gowns are not contaminated after donning, sterilization of the surgical site, management of sterile supplies, disinfection of the OR environment, sterilization of surgical tools, and management of intraoperative surgical team changeover.27 Notably, training for OR nurses in infection control specific to pre-, intra-, and postoperative procedures should be regularly provided. Surgical count is a crucial procedure aimed at preventing retained surgical items, which can lead to complications such as infection and pain, reoperation and, in severe cases, can be fatal.28 The main causes of retained surgical items include omission of the preoperative count, error in recording the surgical count, neglect of safety protocols, and communication errors.28 As digital systems (microchips, etc.) for surgical counts are also being developed, efforts must be made to implement surgical count guidelines suitable for each hospital.
The results of the IPA of OR patient-safety nursing identified the following areas for improvement efforts: handwashing before administering high-alert medications, checking cleanliness and aseptic conditions, and checking 5-Right. Direct comparison is challenging owing to limited studies exploring the educational needs of OR nurses using the analysis of patient safety nursing importance-performance. However, a survey of 3000 OR nurses worldwide, who had joined AORN, identified the top 10 patient safety issues (accurate patient identification, surgical item count, medication error, instrument reprocessing disinfection, and bedsores, etc).3 Most of the “concentrate here” items identified in this study were found to be consistent.
Because pathogens can be transmitted through direct or indirect contact, surgical teams must practice good hand hygiene before surgery to avoid inadvertently touching door handles, surgical patient carts, computer keyboards, or other equipment in the OR, and transferring microbial contaminants from those items to the patient. All surgical teams should use alcohol-based hand sanitizers before donning non-sterile gloves and complete hand hygiene procedures by removing gloves and using alcohol-based hand sanitizers or traditional hand washing when patient contact has ended.29,30 Hand hygiene reduces the risk of transmission of endogenous organisms from patients and exogenous organisms from other patients, healthcare teams, and the OR environment.31 Surgical hand washing is also important because there is a risk of transmitting microorganisms that can cause infection through the sterile gloves of surgical team members. Before and after surgery, the surgical team members must complete a surgical hand scrub with a brush using running water, antibacterial scrubbing agents, and a non-abrasive sponge for at least 3–5 minutes.27 Subsequently, brushless handwashing is recommended, since it reduces microscopic cuts in the dermis, causes excessive shedding of skin cells, and removes pathogens from the skin surface.32
Medical equipment and sterilized supplies must be checked before use, and their packaging and expiration dates verified. All surgeries involve the use of medical devices or surgical tools in contact with sterile tissues or mucous membranes.33 Therefore, if surgical equipment or tools are not properly disinfected or sterilized, they can cause infections in patients through contaminated instruments. Additionally, unsealed or expired supplies and tools should be considered contaminated and should not be used during surgery.
High-alert medications used in patients undergoing surgery include sedatives/hypnotics (eg, midazolam), induction agents (eg, propofol), neuromuscular blocking agents (eg, rocuronium), inhaled anesthetic agents (eg, sevoflurane), and opioids (eg, fentanyl and morphine).34 It has been reported that medication errors involving high-alert medications are particularly common in the OR,35 and can result in hypertension, ventricular arrhythmias, pulmonary edema, and cardiac arrest.33 Therefore, to minimize risk for surgical patients, the access, storage, administration, and monitoring of high-alert medications must be strictly controlled. Such medications need to be stored separately in a restricted area, and warning labels must be attached to the bottles for visibility.33 Efforts should also be made to reduce the risk of medication errors by having at least two healthcare providers make a 5-Right check before administering medications.
Based on this information, “handwashing before administering high-alert medications”, “checking cleanliness and aseptic conditions”, and “checking 5-Right” should be prioritized in the OR patient-safety nursing program. In addition, infection control should be given top priority among the seven subsections of OR patient-safety nursing. According to the Theory of Planned Behavior, an individual’s behavior is influenced by their attitude toward the behavior itself, subjective norms, and perceived behavioral control. Given the great importance of patient-safety nursing among OR nurses, attitudes toward the behavior appear to be positive. Therefore, subjective norms (the pressure to perform a particular behavior) and perceived behavioral control (how much control an individual has over their behavior) should be strengthened to increase the performance of patient-safety nursing in the OR. It is necessary to monitor the performance of patient-safety nursing, evaluate the results, and provide feedback or improve systems (such as increasing personnel and creating checklists) and environments (such as facility structures and supplies) to remove barriers to patient-safety nursing.13 In particular, based on the results of this study, training and interventions should focus on areas where improvement efforts can be concentrated.
Limitations and Suggestions
First, this study collected data from OR nurses; however, as the number of samples was small and OR nurses were recruited from two general hospitals, there is a potential for significant bias (ceiling effects, etc.) in the research results. Therefore, care should be taken in generalizing the research results. Second, the items related to OR patient-safety nursing may vary by medical institution, but this study collected data from only two hospitals. Therefore, it is necessary to categorize and research different hospitals, and develop training programs and interventions tailored to each hospital based on the results.
This study aimed to explore the importance and performance of patient-safety nursing education needs (priority) among OR nurses using IPA. In particular, the importance and performance of OR patient-safety nursing perceived by OR nurses were compared and analyzed to identify areas in need of intensive improvement. As a result of the analysis, “hand washing before administration of high-alert medications”, “checking cleanliness and aseptic condition”, and “checking 5-Right” were found to be “Concentrate here” aspects. Because patient-safety incidents in OR can be fatal, education to improve OR nurses’ performance on “Concentrate here” items should be prioritized, and monitoring, feedback, and intervention should be provided. To this end, health and medical policies related to patient safety in ORs (eg, implementing patient safety education as essential education for medical personnel, strengthening monitoring in ORs, reflecting patient safety indicators in medical institution evaluation) should be prioritized. Hospitals should first establish an OR patient-safety nursing education program, emphasizing the importance of patient-safety nursing. Adequate resources, including surgical goods and manpower necessary to improve performance, should be provided. Nursing managers should encourage nurses to internalize and independently prioritize patient-safety nursing by continuously monitoring and feedback, particularly focusing on the “Concentrate here” aspects.
Data Sharing Statement
Data cannot be shared publicly because of restrictions by the Konyang University Institutional Review Board. Data are available from the Konyang University Institutional Data Access/Ethics Committee for researchers who meet the criteria for access to confidential data. Data requests can be addressed to the Konyang University Institutional Review Board (82-42-600-8466, [email protected]).
Ethics Approval and Informed Consent
This study submitted a research plan to the Konyang University IRB. This study was approved for review (IRB No.: KYU 2023-02-017).
Acknowledgments
We would like to thank everyone who took part in the survey.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by the National Research Foundation of Korea (NRF) grant funded by the Korea government (MSIT) (No. 2022R1F1A106359712). The funding agency had no role in any of the stages from study design to submission of the paper for publication.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Larizgoitia I, Bouesseau MC, Kelley E. WHO efforts to promote reporting of adverse events and global learning. J Public Health Res. 2013;2(3):e29. doi:10.4081/jphr.2013.e29
2. Wong DA, Herndon JH, Canale ST, et al. Medical errors in orthopaedics: results of an AAOS member survey. J Bone Joint Surg Am. 2009;91(3):547–557. doi:10.2106/JBJS.G.01439
3. Steelman VM, Graling PR, Perkhounkova Y. Priority patient safety issues identified by perioperative nurses. AORN J. 2013;97(4):402–418. doi:10.1016/j.aorn.2012.06.016
4. Hempel S, Maggard-Gibbons M, Nguyen DK, et al. Wrong-site surgery, retained surgical items, and surgical fires: a systematic review of surgical never events. JAMA Surg. 2015;150(8):796–805. doi:10.1001/jamasurg.2015.0301
5. Stawicki SP, Moffatt-Bruce SD, Ahmed HM, et al. Retained surgical items: a problem yet to be solved. J Am Coll Surg. 2013;216(1):15–22. doi:10.1016/j.jamcollsurg.2012.08.026
6. Ludwick S. Surgical Safety: Addressing the JCAHO Goals for Reducing Wrong-Site, Wrong-Patient, Wrong-Procedure Events. AHRQ Publication No. 05-0021-3. Rockville, MD: Agency for Healthcare Research and Quality; 2011.
7. Association of Perioperative Registered Nurses. AORN guidance statement: safe medication practices in perioperative settings across the life span. AORN J. 2006;84(2):276–283. doi:10.1016/s0001-2092(06)60495-x
8. De Vries EN, Ramrattan MA, Smorenburg SM, Gouma DJ, Boermeester MA. The incidence and nature of in-hospital adverse events: a systematic review. Qual Saf Health Care. 2008;17(3):216–223. doi:10.1136/qshc.2007.023622
9. Ministry of Health and Welfare, Korea Institute for Healthcare Accreditation. Korean patient safety incident report 2022. Seoul: Korea Institute for Healthcare Accreditation; 2023. Available from: https://www.kops.or.kr/portal/board/statAnlrpt/boardList.do.
10. Lm MY, Sung YH, Jung JH. Relationship among types of nursing organizational culture, self-leadership and burnout as perceived by perioperative nurses. J Korean Acad Nurs Adm. 2017;23(2):170–180. doi:10.11111/jkana.2017.23.2.170
11. Lim EJ, Lee YJ. Comparison of operating room nurses and general ward nurses on communicative competence and interpersonal relationship ability within the medical team. J Korean Acad Nurs Adm. 2014;20(3):313–321. doi:10.11111/jkana.2014.20.3.313
12. Peñataro‐Pintado E, Rodríguez E, Castillo J, Martín‐Ferreres ML, De Juan MÁ, Díaz Agea JL. Perioperative nurses’ experiences in relation to surgical patient safety: a qualitative study. Nurs Inq. 2021;28(2):e12390. doi:10.1111/nin.12390
13. Kim NY, Jeong SY. Perioperative patient safety management activities: a modified theory of planned behavior. PLoS One. 2021;16(6):e0252648. doi:10.1371/journal.pone.0252648
14. Kwon KN, Hwang SY. Impact of perception of patient safety culture and safety control on patient safety management activities among perioperative nurses in University hospitals. J Korean Acad Nurs Adm. 2022;28(3):285–296. doi:10.11111/jkana.2022.28.3.285
15. Kim MR, Kwon MS. The effects of operating room nurses’ perceptions of organizational health, safety climate, and the nursing working environment on engagement in patient safety management activities. Korean J Occup Health Nurs. 2019;28(4):197–207.
16. Kwon EY, Park KY. Influencing factors on patient safety awareness, satisfaction with organizational communication, and patient safety management activities of operating room nurses in small and medium-sized hospitals. Health Soc Res. 2019;39(1):428–452.
17. Kim A, Lee H. Influences of teamwork and job burnout on patient safety management activities among operating room nurses. J Korean Acad Nurs Adm. 2022;28(5):605–615. doi:10.11111/jkana.2022.28.5.605
18. fvgnSiniscalchi JM, Beale EK, Fortuna A. Using importance‐performance analysis to evaluate training. Perf Improv. 2008;47(10):30–35. doi:10.1002/pfi.20037
19. Martilla JA, James JC. Importance-performance analysis. J Mark. 1977;41(1):77–79. doi:10.1177/002224297704100112
20. Kim NY. Novice and advanced beginner nurses’ patient safety management activities: mediating effects of informal learning. J Korean Acad Nurs Adm. 2020;26(5):542–549. doi:10.11111/jkana.2020.26.5.542
21. Kim JS, Kim JS. Association of job crafting and perception of patient safety culture with patient safety management activities among hospital nurses. J Korean Acad Nurs Adm. 2022;28(4):382–392. doi:10.11111/jkana.2022.28.4.382
22. Hernández-Herrero M, Cayón-De Las Cuevas J. Litigation in cardiology and cardiovascular surgery: a cross-sectional observational study of liability in the Spanish public healthcare system. Span J Leg Med. 2022;48(4):136–143. doi:10.1016/j.remle.2022.10.001
23. Sarmiento S, Wen C, Cheah MA, Lee S, Rosson GD. Malpractice litigation in plastic surgery: can we identify patterns? Aesthet Surg J. 2020;40(6):NP394–NP401. doi:10.1093/asj/sjz258
24. Shin J, Lee JH, Kim NY. Analysis of factors related to domestic patient safety incidents using decision tree technique. Risk Manag Healthcare Policy. 2023;16:1467–1476. doi:10.2147/RMHP.S421167
25. Cant RP, Cooper SJ, Lam LL. Hospital nurses’ simulation-based education regarding patient safety: a scoping review. Clin Simul Nurs. 2020;44:19–34. doi:10.1016/j.ecns.2019.11.006
26. Sattar F, Sattar Z, Zaman M, Akbar S. Frequency of post-operative surgical site infections in a tertiary care hospital in Abbottabad, Pakistan. Cureus. 2019;11(3):e4243. doi:10.7759/cureus.4243
27. Bashaw MA, Keister KJ. Perioperative strategies for surgical site infection prevention. AORN J. 2019;109(1):68–78. doi:10.1002/aorn.12451
28. Stawicki SP, Cook CH, Anderson HL, et al. Natural history of retained surgical items supports the need for team training, early recognition, and prompt retrieval. Am J Surg. 2014;208(1):65–72. doi:10.1016/j.amjsurg.2013.09.029
29. Spruce L. Back to basics: hand hygiene and surgical hand antisepsis. AORN J. 2013;98(5):
30. Goldberg JL. Guideline implementation: hand hygiene. AORN J. 2017;105(2):203–212. doi:10.1016/j.aorn.2016.12.010
31. Hughes RG, editor. Patient Safety and Quality: An Evidence-Based Handbook for Nurses. AHRQ Publication No. 08-0043. Rockville, MD: Agency for Healthcare Research and Quality; 2008.
32. Liu LQ, Mehigan S. The effects of surgical hand scrubbing protocols on skin integrity and surgical site infection rates: a systematic review. AORN J. 2016;103(5):468–482. doi:10.1016/j.aorn.2016.03.003
33. Rutala WA, Weber DJ. Disinfection and sterilization: an overview. Am J Infect Control. 2013;41(5):S2–S5. doi:10.1016/j.ajic.2012.11.005
34. Golembiewski J, Wheeler PJ. High-alert medications in the perioperative setting. J PeriAnesthesia Nurs. 2007;22(6):435–437. doi:10.1016/j.jopan.2007.09.002
35. Manias E, Williams A, Liew D, Rixon S, Braaf S, Finch S. Effects of patient-, environment- and medication-related factors on high-alert medication incidents. Int J Qual Health Care. 2014;26(3):308–320. doi:10.1093/intqhc/mzu037
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.