")
Back to Journals » Patient Preference and Adherence » Volume 18
Improving Medication Adherence Levels in Inflammatory Bowel Disease (IBD) Patients: A Narrative Evidence-Based Review
Authors Amiesimaka OI , Aluzaite K, Braund R, Schultz M
Received 9 October 2023
Accepted for publication 12 April 2024
Published 20 April 2024 Volume 2024:18 Pages 905—916
DOI https://doi.org/10.2147/PPA.S383304
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Johnny Chen
Obreniokibo Ibifubara Amiesimaka,1 Kristina Aluzaite,1 Rhiannon Braund,2 Michael Schultz1,3
1Gastroenterology Research Unit, Department of Medicine, Dunedin School of Medicine, University of Otago, Dunedin, New Zealand; 2New Zealand Pharmacovigilance Centre, University of Otago, Dunedin, New Zealand; 3Gastroenterology Unit, Dunedin Hospital, Te Whatu Ora/Health New Zealand, Dunedin, New Zealand
Correspondence: Michael Schultz, Gastroenterology Research Unit, Department of Medicine, Dunedin School of Medicine, University of Otago, PO Box 913, Dunedin, 9054, New Zealand, Tel +64 3 479 0999, Email [email protected]
Abstract: Inflammatory bowel disease (IBD) management is typified by a long-term medication regimen which can comprise multiple medications prescribed in different combinations, doses, frequencies, and with various administration routes. This complexity can make medication adherence (MA) – patients taking their medications per the prescription – for patients with IBD a challenge. The research corpus contains diverse interventions aimed at improving MA in patients with IBD. Therefore, to condense the evidenced strategies for ease of reference, this narrative evidence-based review broadly outlines the patient-level interventions reported. The interventions are grouped as educational, behavioural, cognitive-behavioural, and multicomponent. They, however, present mixed results as to their efficacy at improving MA, with those employing combined approaches being the most promising. This reflects the reality that MA is impacted by multiple factors encompassing those pertaining to the patient, disease, therapy, patients’ socioeconomic status, and health system. Hence, the most ideal interventions would likely be multifaceted patient-level interventions alongside policy/system-level strategies, to maximise the potential for successfully improving patients’ MA. These findings might have been impacted by the heterogeneity of the studies in terms of the method of MA assessment, duration of interventions, and more besides.
Keywords: Inflammatory Bowel Disease, IBD, interventions, medication adherence
Introduction
Inflammatory bowel disease (IBD) is a chronic gastroenterological disease with life-long medication therapy as a central disease management approach, alongside dietary and other interventions, such as surgery.1,2 Crohn’s disease (CD), ulcerative colitis (UC), and IBD unclassified (IBD-U) make up IBD. Underpinning IBD are interrelations between genetic susceptibility, environmental factors, and maladaptive immune system elements, causing the chronic, relapsing, and remitting gastrointestinal inflammation that typifies IBD.2 Patients with IBD might experience symptoms ranging from diarrhoea, often with bleeding, urgency/tenesmus, and constipation/loading to abdominal discomfort/pain, weight loss, fatigue, malnourishment, and others.2,3 Complications including strictures, fistulae, or abscesses may also arise.2,4
Various medications, jointly or alone, are used for IBD therapy depending on disease activity, therapy target, side effects, comorbidities, among others.5 Therapeutics used include: 5-aminosalicylic acid drugs (5-ASAs) (eg sulfasalazine, mesalamine); corticosteroids (eg budesonide); and immunomodulators (eg azathioprine).6,7 Further, biologic agents (eg infliximab and adalimumab, golimumab, vedolizumab, ustekinumab, etc.), and Janus kinase inhibitors (JAKi) (eg tofacitinib) might be used, alongside several others.5–9
For patients with IBD, taking their medications as prescribed (ie medication adherence (MA)10) is important for disease management as poor MA is linked with worse disease outcomes (such as flare-ups) and complications, in turn necessitating therapy escalation, as well as greater health costs, morbidity, disability, and mortality.9 Illustrating this, non-adherent IBD patients are reported as having significantly higher risk of relapse compared to adherent patients (RR, 2.9; 95% CI, 2.25–3.79; p=0.045).11 Similarly, adherent IBD patients are reported as having a greater likelihood of being in clinical remission than non-adherent patients (84% vs 43%; p<0.001).12
Moreover, the selection of medications available often differs across health systems/countries and can be limited by factors such as public funding restrictions.5 Therefore, besides MA being important for clinical IBD management, MA can be “extremely important” in settings where there are limited pharmaceuticals available, particularly for handling aggravated disease.5 The MA continuum consists of three stages: initiation (beginning the regimen), implementation (continuing the regimen by taking refills), and discontinuation (stopping the regimen); discontinuation is linked to persistence (the time from initiation until discontinuation).10,13 Non-adherence can occur at any point in the continuum; thus, MA patterns can differ between individuals or medicines taken by the same individual.
Research has reported that as high as one-third of patients with IBD have poor MA to their medication regimens – 31.1% of patients with IBD in southern New Zealand, 32.8% in Italy, 36.2% in South Korea, 28.7% in Australia and the United Kingdom, and 12.1% and 13.3% of patients with CD and UC in the Netherlands, respectively.11,14–17 Furthermore, a one-year multi-centre study found that 28%, 48%, and 24% of Dutch IBD patients had low, medium, and high adherence per the self-reported Modified Morisky Adherence Scale-8 (MMAS-8), whilst 25% of the patients had pharmacy refill-derived, medication possession ratio (MPR) scores <80%, indicating “non-adherence”.18 This suggests that self-reported MA can differ from “objectively” calculated MA using health/medicine records. Further, non-adherence was significantly greater (p<0.01) among adalimumab users than among infliximab users.18 This might be because adalimumab is self-administered whereas infliximab is usually administered by a healthcare professional (HCP), highlighting that adherence to different medicines might differ based on mode of administration, with a further dimension of route of administration – oral (pills), subcutaneous, suppository, injection, etc. – also impacting adherence. Also noteworthy is the impact of the covid-19 pandemic on adherence of patients with IBD. An Italian study found significantly more non-adherent patients with IBD had had a previous covid-19 infection than had adherent patients (p<0.001).17 The authors also identified past covid-19 infection as a predictor of non-adherence (OR, 7.822; 95% CI, 3.385–18.07; p<0.001), with most patients (64.2%) having a worry concerning IBD and covid-19. A plurality (41.4%) of patients believed that having IBD made them more susceptible to covid-19, with significantly more adherent patients holding this belief than non-adherent patients (p=0.039).17 The authors also reported a dichotomy in patient satisfaction with IBD–covid-19 information received by different HCPs, with a majority being satisfied with information from their gastroenterologists but most being unsatisfied with information from their general practitioners. This suggests a need for HCPs in primary care to meet patients’ information needs as regards IBD and covid-19.17
Poor MA is not peculiar to IBD but has been reported across many diseases. MA levels average around 50% for long-term diseases in the developed world, and a wide range of MA levels have been reported based on disease, socioeconomic groups, geographical locations, and more besides.9,19–23 Around 200,000 deaths yearly are attributable to non-adherence in Europe,24 and non-adherence is also implicated in around 30–70% of medicine-related US hospitalisations.25 Estimates hold that poor MA costs EUR125 billion yearly in Europe and USD100–290 billion annually in the US.24,26–28 Estimating the monetary cost of non-adherence in IBD specifically, across different health systems, is a research field needing attention.
Patients with IBD have reported being motivated to practise good MA, which they view as an essential duty for preserving their health and wellbeing.29 Starting from accepting their IBD diagnosis, IBD patients take proactive steps to ensure they have their medicines to hand and take them as prescribed. However, MA in IBD can be complicated, with patients often taking numerous therapeutics with different dosing, administration routes, and storage conditions.29 MA typically involves patients getting to the prescriber, receiving a prescription, going to a pharmacy, obtaining the therapeutics, and finally taking the pharmaceuticals.30 Challenges/inequities in practice can occur at any point in this process, thus hampering MA at one/more stages.
The World Health Organization (WHO) groups the many factors impacting MA into five: patient-related (eg beliefs, approaches, expectations, knowledge, etc.), disease-related (eg comorbidities, signs/symptoms, etc.), therapy-related (eg adverse effects, dose simplicity, etc.), socioeconomic (family structure, employment, education, age, race, etc.), and health system (healthcare costs, access, provider–patient relationship, etc.) factors.21 MA is also impacted by social-, policy-, and system-level factors which determine access to medicines. Barriers to medicine access have been classed as: structural barriers (eg accessing appointments, wait times, completing referrals, etc.); provider capacity to meet different patients’ needs (eg cultural safety/competency, knowledge and skills, etc.), and barriers to healthcare access (eg delayed access, costs, transport, etc.).30
The literature reports factors associated with non-adherence in patients with IBD including perceptions about medicine side effects, medication interactions, and response loss; anxiety/depression; dosing routine, etc.31,32 Others are having further health issues, prescription unaffordability, “not wanting to”, and failing to notice medicines had finished, besides medicines cost, refill inconvenience, medicine (physical) features, among others.16,32 Furthermore, patient education, on symptom prevention and IBD management, besides general information on IBD, understanding the value of MA, has been identified as essential to successful MA.33 More so, patients believing in the importance of medications (per the Beliefs about Medicines Questionnaire, BMQ) also independently predicts better MA.14 Based on the BMQ, 34%, 17%, 34%, and 15% of IBD patients’ (on thiopurines) views of the medications were designated as accepting, ambivalent, indifferent, or sceptical.34 Therapy discontinuation was least among accepting patients (22%), compared to the ambivalent (37%; p<0.01), indifferent (35%; p=0.02), or sceptical (54%; p<0.01).34 Uncertainties about the importance of maintenance therapy, medicine efficacy, and effects of non-adherence also impact MA behaviours.32 These highlight the need for MA initiatives that help patients understand the importance of the medications and allay any fears, eg about medicine side effects/dependency. Being male has been significantly associated with better adherence to IBD therapeutics than being female.35,36 Conversely, lower age at the point of diagnosis15 and being ≤30 years has been significantly linked with non-adherence (OR, 5.88; 95% CI, 1.51–22.94; p=0.011) as are limited knowledge of prescribed medicines (OR, 5.61; 95% CI, 1.60–19.67; p=0.038) and greater durations between outpatient clinic visits (OR, 30.31; 95% CI, 3.06–300.17; p=0.004).11 In turn, non-adherence increases the risk of disease relapse (RR, 2.9; 95% CI, 2.25–3.79; p=0.045). Medicines knowledge – on side effects (p=0.015), names (p=0.015), and dosages (p=0.011) – has also been found to be significantly better in patients who are adherent versus in non-adherent patients.11 Patients’ knowledge of IBD and the regimen, their beliefs, MA behaviours, the HCP–patient relationship, mental health comorbidities (eg depression), and the regimen/medicines access factors could all be targets for MA improvement.37 The aforementioned factors could inform the identification of patients who might be at risk of poor adherence by HCPs.
Recognising the importance of MA in IBD, studies have explored interventions for improving MA in patients with IBD, and these are broadly categorised as educational, behavioural, cognitive-behavioural, and multicomponent.38,39 Greenley et al39 conducted an evidence-based review of the MA promotion literature. In the decade since, further research has been published on MA promotion strategies which might reflect newer innovations and developments. Therefore, the purpose of this non-systematic, narrative, evidence-based review is to underline the more recent interventions for improving MA in patients with IBD, using the aforementioned categories, in the literature. This could guide further research and the implementation of MA interventions targeted at IBD patients especially.
MA Interventions in IBD
Reviewed Studies
This review focuses on original research, using high-quality study designs, published in English between 2013 and 2023, in any country, featuring only patient-level interventions of any type and targeting all age groups. Being a narrative review, select studies identified by a literature search of Google Scholar, the University of Otago Library, Scopus, Web of Science, and PubMed, besides the Google search engine, are presented to broadly outline the intervention landscape for promoting MA. The 19 studies included in this review are outlined in Table 1 below.
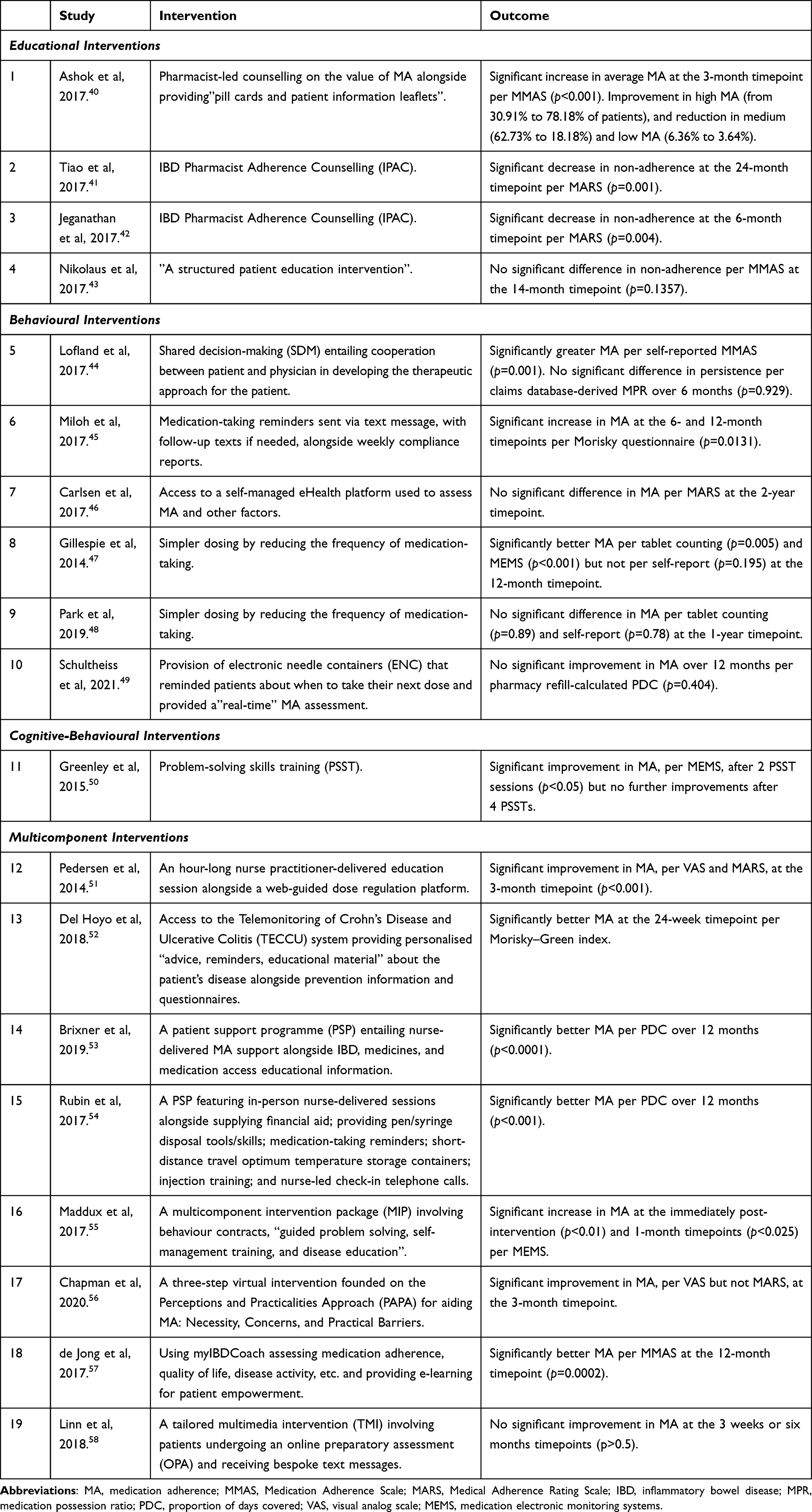 |
Table 1 Data Extraction Table Outlining the Studies Reviewed |
MA Assessment – a Synopsis
To contextualise the interventions, a look at the techniques applied in assessing MA is instructive. These can be grouped across different dimensions namely direct (eg blood/urine tests for medicines) versus indirect methods (all non-test methods), or objective versus subjective methods.20,25 Subjective methods involve the patient/healthcare professional (self-)assessing (via interviews, questionnaires, etc.) the patient’s MA behaviours, whilst objective methods involve using observational/monitoring approaches (eg calculating MA from medication dispensing/claims records, using medication electronic monitoring systems (MEMS) etc.) to assess MA. Objective methods focus more on providing “accurate” evaluations of medication-taking, whilst subjective measures make room for assessment of nuanced reasons for non-adherence.27 Using objective methods especially, MA can be calculated via measures described as medication possession ratio (MPR) or proportion of days covered (PDC), and daily polypharmacy possession ratio (DPPR), amongst others.9,20,36,59 It is noteworthy that different methods assess different components of MA (eg assessing dispensing records investigates whether patients are collecting dispensings at the pharmacy, whilst pill counts assess how many pills patients appear to have actually taken etc.). Similarly, different measures calculate MA in different ways (eg MPR and PDC calculate MA to single-medication regimens, whilst DPPR is optimised for multidrug regimens). Moreover, when patients estimate their MA, their perceptions can differ materially from results obtained using standardised tools; for instance, one-third of New Zealand IBD patients over-/under-estimated their MA when compared to their MA measured with a validated MA questionnaire, ProMAS.16 Therefore, each method/measure has its areas of strength and weakness, which must be considered when making comparisons. This heterogeneity in MA assessment approaches makes comparison of studies quite challenging as the MA methods, measures, and parameters (eg patient groups, medications, duration of the period under review, etc.) used can vary widely.
Educational Interventions
Comprehensive education of patients on the broad spectrum of topics pertaining to IBD has been applied as an important MA promotion intervention.60 Educational interventions can be delivered in-person, online, or via telephone etc., and by a diverse range of personnel including HCPs, trained educators, and others. Educational interventions could cover aetiology, diagnosis, therapeutics (drugs/surgery), action pathways of therapeutics, dosing regimen, medication side effects, and nutrition, among other facets of IBD therapy.38
One prospective intervention follow-up study employed pharmacist-led counselling on the value of MA coupled with the provision of “pill cards and patient information leaflets” to 110 Indian hospital patients with IBD.40 A comparison of pre- and three-month post-intervention results using the Morisky Medication Adherence Scale (MMAS-8) and Crohn’s and Colitis Knowledge Assessment Questionnaire (CCKNOW) showed that high adherence increased from 30.91% to 78.18% of patients, while medium adherence dropped from 62.73% to 18.18%, just as low adherence fell from 6.36% of patients to 3.64% of them. Likewise, the average (CCKNOW) score rose from 8.15 to 11.65. Both the average adherence and knowledge scores significantly increased (p<0.001).40 This intervention shows the usefulness of education interventions and underscores the role pharmacists play in the MA processes and provides an example that could be replicated relatively easily. However, care should be taken to ensure that adding such duties to pharmacists does not put excessive pressure on their time and resources.
Furthermore, IBD Pharmacist Adherence Counselling (IPAC) entailing a lone counselling session, personalised, based on the patient’s circumstances, was applied in a prospective multi-centre study in Australia.41 Ab initio, using the Medical Adherence Rating Scale (MARS), 100 Australian participants were delineated based on adherence (64 patients; MARS, ≥17) and non-adherence (36 patients; MARS ≤16). The non-adherent patients received the IPAC intervention, whilst the adherent group did not. After 24 months, whereas non-adherence stayed the same, with no statistically significant change, in the control group (p=0.38), the rates of non-adherence in the intervention group reduced significantly from 100% to 44.4% (p=0.001).41 Assessment using the BMQ also revealed that baseline non-adherent patients saw a significant rise in medication “acceptance”, ie high medication necessity and low concerns, after 12 months (p=0.031).41
Similarly, an intervention study, with Australian participants, employed IPAC provided by a trained pharmacist to non-adherent patients with IBD (MARS ≤16) aged 12–25 years old.42 The study found a significant reduction in non-adherence by 60% (p=0.004), per the MARS, 240 days on average post-intervention.
However, a randomised, prospective clinical trial involving 126 German UC patients receiving an educational intervention alongside standard care and 122 others receiving just standard care, as controls, found no significant improvement in MA to mesalamine between the two cohorts.43 The educational intervention was administered by a doctor or nurse, and MA was self-reported using the MMAS.
Although encouraging, these results were derived under trial settings; hence, the effectiveness of these interventions in the real world, with different patient groups, in different locations etc., needs consideration.
Behavioural Interventions
MA improvement interventions could also be behavioural with a focus on driving, prompting, and incentivising good MA behaviours. This could involve using audio-visual reminders, pill boxes, streamlined dosing, MA monitoring with feedback provision to patients, among others.38
Medication adherence to biological agents has been reported to be significantly more likely in patients with IBD, as well as psoriatic arthritis or rheumatoid arthritis, who participated in shared decision-making (SDM) than those who did otherwise.44 SDM entails cooperation between patient and physician in developing the therapeutic approach for managing the patient’s condition. In this study, patients were delineated based on whether or not they partook in SDM with their health provider. Those who did not had worse persistence than those who engaged in SDM (p=0.029), although there was no significant difference in MA per the claims database-derived medication possession ratio (MPR), “objectively” assessing MA implementation. However, patients’ self-reported MA, per the self-reported MMAS, was significantly greater for those who partook in SDM than for others who did not (p=0.001).44 Further results showed the non-SDM cohort were significantly more likely to forget to take their medication, prematurely discontinue the biologics regimen upon feeling better, and be less cautious about adherence. Moreover, IBD patients who were part of SDM incurred significantly lower total medical costs (USD9404) than those who did not (USD25,071) (p=0.003).44
Likewise, in a randomised controlled trial (RCT) with paediatric patients with IBD (≥8 years), 21 patients were randomised to the intervention and 30 others served as controls.45 Two-way medication-taking reminders were sent via text message to the intervention cohort; another text message was sent to the paediatric patients’ carers if the patients did not confirm having taken their medications. Moreover, patients/carers/HCPs all received reports on compliance every week. MA, per Morisky questionnaire, for the intervention group significantly improved at both the 6- and 12-month timepoints compared to baseline (p=0.0131), whereas there was no significant improvement in MA for the control group (p=0.1687).45
However, a 2-year Danish RCT of 56 child/adolescent patients with IBD (aged 10–17 years) provided the 27 patients in the intervention group with access to an eHealth platform to which the 26 controls did not have access.46 The eHealth platform was self-managed and used to assess MA alongside disease activity, school attendance, and others. The results showed no significant difference in the MA levels of patients in the intervention versus the control groups, per the MARS and a visual analog scale (VAS).46 Nonetheless, the intervention was not totally without benefit as the intervention group had fewer school absences due to IBD reasons (1.6 vs 16.5 – eHealth vs controls; p<0.002) as well as fewer total outpatient health facility events (3.26 vs 7.31 – eHealth vs controls; p<0.0001).
For UC patients, a sub-study of a UK multi-centre randomised trial found that reducing the frequency of medication-taking was associated with improved MA.47 Fifty-eight participants were assigned to two mesalazine dosing regimens: 28 took three 800 mg tablets at once every day, while the other 30 took one 800 mg tablet three times a day, both for a 12-month duration. MA was measured using: self-report (ie asking patients to estimate their adherence), tablet counting, and MEMS (medicine containers which electronically record when they are opened presumably for medication-taking). Although no statistically significant difference was found between the two groups based on self-report (p=0.195), the once-a-day group had significantly better MA than the triple-dosing group based on both tablet counting (98.9% vs 94.2%; p=0.005) and MEMS (96.6% vs 54.9%; p<0.001).47 These results indicate that simpler dosing regimens could improve MA for UC patients, although the authors note that the MEMS device might not have been easy to carry around which might have impacted the results for the thrice daily group and that a validated self-report survey tool might have been better than just asking the patients for their perceived MA.
Conversely, a South Korean prospective, multi-centre, randomised trial found no significant difference in MA between 90 patients with UC who took mesalazine tablets once a day (2.4 g once daily) compared to 90 others who took divided doses (either 0.8 g thrice daily or 1.2 g twice daily).48 This was the result when MA was measured both via tablet counting and self-reported daily drug diaries at all timepoints (three, six, nine, and twelve months). However, the once-a-day group reported significantly greater satisfaction with their regimen than the divided dose group (p<0.001).48
Likewise, employing MA technological aids such as MEMS, which record the time and date of events when medicine containers are opened,20,25 was found not to have improved MA in IBD. A multi-centre 12-month observational study, set in the Netherlands,49 found no significant improvement in the MA (per the pharmacy refill-calculated, “objective” proportion of days covered (PDC)) of the intervention group of 69 IBD patients who had been provided with electronic needle containers (ENC) to use in adalimumab administration compared to the 97 controls who did not receive ENCs. The ENCs reminded patients about when to take their next dose and provided them with a “real-time” assessment of their MA.
The mixed results on behavioural interventions highlight the opportunities for MA improvement that exist but underscore the need for research to identify the most appropriate strategies to adopt, which might differ based on the MA methods/measures used, the target population, and context.
Cognitive-Behavioural Interventions
Related to behavioural interventions, cognitive behavioural therapy (CBT) can also be used for improving patients’ MA. Skills-building, for instance, in helping patients overcome pessimistic thoughts that can hinder patients’ belief in medications is a CBT approach.38 Approaches adopted across diseases include motivational interviewing, problem-solving skills training, habit-formation training, and others.60
An RCT involving paediatric patients with IBD (11–18 years old) featured problem-solving skills training (PSST) as the intervention.50 Clinical psychology doctoral candidates delivered the PSST by telephone to the intervention group. However, only the 16–18-year-olds recorded a significant improvement in MA, measured using medication electronic monitoring systems (MEMS) packages, after 2 PSST sessions (p<0.05).50 There was no further improvement in MA after 4 PSST sessions were completed.
This presents tenuous evidence of CBT efficacy in improving MA specifically in IBD but underlines the need for further research as several studies using CBT, for other diseases, have found significant improvements in patients' MA.60
Multicomponent Interventions
Recognising that multiple factors impact MA behaviours of patients with IBD, multicomponent approaches incorporating different types of interventions have been used across studies. These aim to maximise the likelihood of successfully improving patients’ MA by addressing a range of factors which might be hampering their MA.
A Danish prospective open-label study involving 95 patients with mild-to-moderate UC51 employed an hour-long nurse practitioner-delivered education session (on “UC knowledge, mesalazine therapy, instructions on use of the self-managed web-based application”) alongside a web-guided mesalazine dose regulation platform. After 3-month follow-up, the patients’ MA to the mesalazine regimen had significantly improved both per a visual analog scale (VAS) scale and the MARS.51
Likewise, an RCT, conducted with 63 Spanish patients with IBD, found that patients who received remote web-based monitoring via a Telemonitoring of Crohn’s Disease and Ulcerative Colitis (TECCU) platform saw a significant improvement in their MA, as did patients who received only nurse-led telephone support and the controls who only received face-to-face standard care.52 However, the patients receiving the TECCU intervention recorded a significantly larger improvement in MA (ie greater decrease in Morisky–Green score) than the controls (OR, 0.0001; 95% CI, 1.02e-10 to 0.517). The TECCU system provided personalised “advice, reminders, educational material” about the patient’s disease alongside prevention information and questionnaires.52 Further, the patients’ survey responses helped guide the medical care team who modified the medication regimen as needed.
A longitudinal retrospective study, set in the US, involved adults who received adalimumab, including CD and UC patients.53 The 12-month PDC was calculated, using claims records, from index registration date in a patient support programme (PSP) entailing nurse-delivered MA support alongside IBD, medicines, and medication access educational information, for the 1134 patients in the intervention group. For the 1134 controls, 12-month PDC from the index adalimumab claim date was calculated. Average MA was significantly greater for those who partook in the intervention PSP than for the controls (64.8% versus 50.1%; p<0.0001). More so, the intervention group experienced a lower discontinuation rate than the controls (51.4% versus 65.9%; p<0.0001).53
A similar US-based longitudinal, retrospective, cohort study explored the impact of a PSP on MA to adalimumab by patients with chronic diseases including CD and UC.54 Respectively, 1199 and 1187 patients were in the intervention and control groups. The PSP featured in-person nurse-delivered sessions alongside supplying financial aid; providing pen/syringe disposal tools/skills; medication-taking reminders; short-distance travel optimum temperature storage containers for adalimumab; injection training; and nurse-led check-in telephone calls. The 12-month MA, per claims database-calculated PDC, was 67.0% for the intervention group and 58.8% for the control group, with the difference being statistically significant (p<0.001). The intervention group also discontinued the regimen at 14% lower rate than the controls.54
A multicomponent intervention package (MIP) involving behaviour contracts, “guided problem solving, self-management training, and disease education” was employed in a “longitudinal single-site nonconcurrent multiple baseline” study set in the US.55 The MIP focused on impacting the workings of patients’ families to promote MA monitoring, effective communication, and more besides; behaviour change via problem solving, behavioural contracts, etc.; inculcating problem-solving skills including training for self-monitoring and caregiver monitoring of MA, etc.; and education on IBD as a disease, treatment details, the importance of adherence, and more besides. The MIP was delivered via four weekly sessions. Mean MA, per MEMS, rose by 12% (from baseline to immediately post-MIP; p<0.01) and 6% (baseline – the one-month follow-up timepoint; p<0.025).55
In the UK, a “single-blind quasi-randomised trial” featured a three-step virtual intervention founded on the Perceptions and Practicalities Approach (PAPA) for aiding MA: Necessity – handling concerns about the importance of MA; Concerns – handling misgivings about possible medicines adverse effects; and Practical Barriers – handling practical matters concerning day-to-day medication use.56 MA, per VAS, was significantly higher in the intervention group than in the controls at both the 1- and 3-month follow-up timepoints, but no significant difference in MA, per the MARS, was found. Whereas the MARS is a validated scale, the VAS involved patients estimating their retrospective adherence for the previous week from 0% to 100% – although both MARS and VAS are self-reported.56
A Dutch study compared a telemedicine system, myIBDCoach, using an intervention cohort of 465 versus controls receiving standard care (444 participants).57 MyIBDCoach assesses medication adherence, work participation, smoking, quality of life, disease activity, fatigue, stress, side effects, nutrition, anxiety and depression, life-events, and provides e-learnings for patient empowerment.61 Results from the MMAS-8 showed a significantly higher MA in the intervention group as compared to the control group, with an estimated intervention effect of 0.46 (95% CI, 0.22–0.70; p=0.0002).57
The study further found that the intervention group reported fewer outpatient visits and hospitalisations than the control cohort.
Not all multicomponent interventions yielded positive results, however. A tailored multimedia intervention (TMI) employed in a Dutch cluster RCT did not produce a significant improvement in the MA of patients with IBD, per the MARS, at 3 weeks or six months follow-up timepoints. The TMI involved patients undergoing an online preparatory assessment (OPA) and receiving bespoke text messages.58 The nurses delivering the accompanying personalised counselling sessions also received communication skills training besides training on the OPA. The control group only received standard care.
Multicomponent interventions hold substantial promise for improving patients’ MA, but the feasibility of rolling them out in practice, with considerations of the resources needed in terms of personnel, funding, technology, and such like, needs evaluation.
Conclusion
This narrative evidence-based review has given a broad outline of medication adherence (MA) improvement interventions for patients with IBD contained in the literature. The interventions employed educational, behavioural, cognitive-behavioural, and multicomponent (combined) approaches but present mixed results as to their efficacy at improving MA. These findings might have been impacted by the heterogeneity of the studies in terms of the method of MA assessment, duration of interventions, among others. Notwithstanding the mixed results, HCPs could consider applying educational interventions (eg counselling).
Most included studies adopted indirect methods40–43,45,46,48,51,52,57,58 in assessing MA, which might be due to their relative ease of use and low cost.38 However, self-reported indirect methods (eg patient medication diaries, questionnaires, etc.) are considered to provide more biased results (due to recall/interviewer bias etc.) than non-self-reported “objective” indirect methods such as MA calculated using MEMS/dispensing records.38 This might have impacted the findings, whether or not improved MA was the result. Although there is no “gold standard” for assessing MA, there is room for further research to trial the interventions whilst assessing MA using more “objective” methods as the results therefrom might be more accurate.27 Nevertheless, some reviewed studies employed such methods alone or in combination with subjective methods.44,47,49,50,53–56
There appear to be limited CBT interventions for promoting MA for patients with IBD as only one was identified in this review. Besides its possible utility in improving MA, CBT has been shown, by an RCT, to improve health-related quality of life of patients with IBD, significantly so for anxiety and depression, with this sustained three months post-intervention.62 However, another RCT with young participants did not find a significant improvement in psychological elements, including anxiety and depression, six and twelve months post-intervention.63 This again shows the mixed results in the literature as buttressed by a narrative review on psychotherapeutic approaches to improving MA in patients with IBD.64 The authors found few studies in the field with the evidence suggesting a possible helpful impact on MA from (cognitive-behavioural) psychotherapy-based interventions but concluded that further studies are needed to obtain more definitive evidence.64
Across studies, technologies have been used in facilitating IBD therapy, particularly in promoting MA,65 as shown by the reviewed studies. This indicates that the use of telemedicine in IBD care could enable more effective self-management and better delivery of personalised care.57 Generally, telemedicine holds promise in IBD management as its use has been recorded to result in better medication adherence, quality of life, as well as savings in health expenses.66 Telemedicine encompasses web-based patient monitoring systems as well as mobile applications which facilitate communication of symptoms and disease progression between patients and HCPs, allowing for prompt responses when problems arise. However, concerns about access inequities, acceptance, ethics, licensing, among others, persist.66
The reviewed studies have mainly been conducted within the confines of controlled settings with a focus on efficacy as opposed to effectiveness in real-world settings. Hence, factors necessary for translation into practice need to be considered; these include needed resources including personnel training and time commitment to the intervention, associated costs, scalability of the interventions, and more besides.39,60 This is important as, for instance, limited availability of healthcare professionals’ (HCPs) time and inadequate communication competencies of HCPs, among others, have been presented as barriers to effective communication in IBD.33 Moreover, the reviewed interventions operate at the patient level, and there is a dearth of research on health policy/system-level interventions aimed at promoting MA for patients with IBD. Given the range of factors impacting MA behaviours,38 such system-level strategies need research attention.
MA is impacted by multiple factors ranging from those pertaining to the patient, the disease, and the therapy to the patients’ socioeconomic status and the health system.21 Interventions in the literature have targeted individual or multiple factors using different strategies. In view of the mixed results provided by different intervention types, the most ideal interventions would likely be multifaceted, combining patient-level educational, behavioural, and cognitive-behavioural interventions alongside policy/system-level strategies, in order to maximise the potential for successfully improving patients’ MA.
Disclosure
The authors report no conflicts of interest in this work.
References
1. de Lange KM, Moutsianas L, Lee JC, et al. Genome-wide association study implicates immune activation of multiple integrin genes in inflammatory bowel disease. Nat Genet. 2017;49(2):256–261. doi:10.1038/ng.3760
2. Gastroenterological Society of Australia (GESA). Clinical Update for General Practitioners and Physicians - Inflammatory Bowel Disease. GESA; 2018.
3. Aluzaite K, Al-Mandhari R, Osborne H, et al. Detailed multi-dimensional assessment of fatigue in inflammatory bowel disease. Inflamm Intest Dis. 2019;3(4):192–201. doi:10.1159/000496054
4. Feldman PA, Wolfson D, Barkin JS. Medical management of Crohn’s disease. Clin Colon Rectal Surg. 2007;20(4):269–281. doi:10.1055/s-2007-991026
5. Amiesimaka OI, Braund R, Aluzaite K, Schultz M. Constraints on medication-based inflammatory bowel disease therapy in Aotearoa New Zealand - why medication adherence is important. NZ Med J. 2023;136(1574):82–89.
6. Talley NJ, Abreu MT, Achkar JP, et al. An evidence-based systematic review on medical therapies for inflammatory bowel disease. Am J Gastroenterol. 2011;106(Suppl 1):S2–25; quiz S26. doi:10.1038/ajg.2011.58
7. Hanzel J, Hulshoff MS, Grootjans J, D’Haens G. Emerging therapies for ulcerative colitis. Expert Rev Clin Immunol. 2022;18(5):513–524. doi:10.1080/1744666X.2022.2069562
8. Coskun M, Vermeire S, Nielsen OH. Novel targeted therapies for inflammatory bowel disease. Trends Pharmacol Sci. 2017;38(2):127–142. doi:10.1016/j.tips.2016.10.014
9. Khan S, Rupniewska E, Neighbors M, Singer D, Chiarappa J, Obando C. Real-world evidence on adherence, persistence, switching and dose escalation with biologics in adult inflammatory bowel disease in the United States: a systematic review. J Clin Pharm Ther. 2019;44(4):495–507. doi:10.1111/jcpt.12830
10. Vrijens B, De Geest S, Hughes DA, et al. A new taxonomy for describing and defining adherence to medications. Br J Clin Pharmacol. 2012;73(5):691–705. doi:10.1111/j.1365-2125.2012.04167.x
11. Tae CH, Jung S-A, Moon HS, et al. Importance of patients’ knowledge of their prescribed medication in improving treatment adherence in inflammatory bowel disease. J Clin Gastroenterol. 2016;50(2):157–162. doi:10.1097/MCG.0000000000000431
12. Samson CM, Mager D, Frazee S, Yu F. Remission in pediatric inflammatory bowel disease correlates with prescription refill adherence rates. J Pediatr Gastroenterol Nutr. 2017;64(4):575–579. doi:10.1097/MPG.0000000000001304
13. Vrijens B, Antoniou S, Burnier M, de la Sierra A, Volpe M. Current situation of medication adherence in hypertension. Front Pharmacol. 2017;8:100. doi:10.3389/fphar.2017.00100
14. Selinger CP, Eaden J, Jones DB, et al. Modifiable factors associated with nonadherence to maintenance medication for inflammatory bowel disease. Inflamm Bowel Dis. 2013;19(10):2199–2206. doi:10.1097/MIB.0b013e31829ed8a6
15. Severs M, Mangen MJ, Fidder HH, et al. Clinical predictors of future nonadherence in inflammatory bowel disease. Inflamm Bowel Dis. 2017;23(9):1568–1576. doi:10.1097/MIB.0000000000001201
16. Aluzaite K, Braund R, Seeley L, Amiesimaka OI, Schultz M. Adherence to inflammatory bowel disease medications in Southern New Zealand. Crohns Colitis 360. 2021;3(3). doi:10.1093/crocol/otab056
17. Pellegrino R, Pellino G, Selvaggi F, Federico A, Romano M, Gravina AG. Therapeutic adherence recorded in the outpatient follow-up of inflammatory bowel diseases in a referral center: damages of COVID-19. Dig Liver Dis. 2022;54(10):1449–1451. doi:10.1016/j.dld.2022.07.016
18. van der Have M, Oldenburg B, Kaptein AA, et al. Non-adherence to Anti-TNF therapy is associated with illness perceptions and clinical outcomes in outpatients with inflammatory bowel disease: results from a prospective multicentre study. J Crohns Colitis. 2016;10(5):549–555. doi:10.1093/ecco-jcc/jjw002
19. National Institute for Health and Care Excellence (NICE). Medicines Adherence: Involving Patients in Decisions About Prescribed Medicines and Supporting Adherence. London: NICE; 2009.
20. Lam WY, Fresco P. Medication adherence measures: an overview. Biomed Res Int. 2015;2015:217047. doi:10.1155/2015/217047
21. World Health Organisation (WHO). Adherence to Long-Term Therapies: Evidence for Action. Geneva: WHO; 2003.
22. Brown MT, Bussell J, Dutta S, Davis K, Strong S, Mathew S. Medication adherence: truth and consequences. Am J Med Sci. 2016;351(4):387–399. doi:10.1016/j.amjms.2016.01.010
23. Tabyshova A, Sooronbaev T, Akylbekov A, et al. Medication availability and economic barriers to adherence in asthma and COPD patients in low-resource settings. NPJ Prim Care Respir Med. 2022;32(1):20. doi:10.1038/s41533-022-00281-z
24. Khan R, Socha-Dietrich K. Investing in Medication Adherence Improves Health Outcomes and Health System Efficiency: Adherence to Medicines for Diabetes, Hypertension, and Hyperlipidaemia. Paris: OECD; 2018:18152015.
25. Osterberg L, Blaschke T. Adherence to medication. New Engl J Med. 2005;353(5):487–497. doi:10.1056/NEJMra050100
26. Zullig LL, Gellad WF, Moaddeb J, et al. Improving diabetes medication adherence: successful, scalable interventions. Patient Prefer Adherence. 2015;9:139–149. doi:10.2147/PPA.S69651
27. Brown MT, Bussell JK. Medication adherence: WHO cares? Mayo Clin Proc. 2011;86(4):304–314. doi:10.4065/mcp.2010.0575
28. Viswanathan M, Golin CE, Jones CD, et al. Interventions to improve adherence to self-administered medications for chronic diseases in the United States. Ann Internal Med. 2012;157(11):757–836. doi:10.7326/0003-4819-157-11-201212040-00538
29. Amiesimaka OI, Aluzaite K, Braund R, Schultz M. “It’s just like putting your socks on”: patients’ perspectives on inflammatory bowel disease medication adherence. Explor Res Clin Soc Pharm. 2023;12:100385.
30. Pharmaceutical Management Agency (PHARMAC). Achieving Medicine Access Equity in Aotearoa New Zealand: Towards a Theory of Change. Wellington, New Zealand: PHARMAC; 2019.
31. Bager P, Jäghult S. Adherence in inflammatory bowel disease (IBD): a clinical review. Gastrointestinal Nurs. 2019;17(6):24–27. doi:10.12968/gasn.2019.17.6.24
32. Devlen J, Beusterien K, Yen L, Ahmed A, Chiefetz AS, Moss AC. Barriers to mesalamine adherence in patients with inflammatory bowel disease: a qualitative analysis. J Manag Care Spec Pharm. 2014;20(3):309–314. doi:10.18553/jmcp.2014.20.3.309
33. Wheat CL, Maass M, Devine B, Thornton T, Grembowski D, Ko CW. Educational needs of patients with inflammatory bowel disease IBD and nonadherence to medical therapy: a qualitative study. J Inflam Bowel Dis Disord. 2016;1(1):1000106.
34. Broekman M, Coenen MJH, Wanten GJ, et al. Patients’ beliefs about medicine are associated with early thiopurine discontinuation in patients with inflammatory bowel diseases. Eur J Gastroenterol Hepatol. 2018;30(2):167–173. doi:10.1097/MEG.0000000000001025
35. Ribaldone DG, Vernero M, Saracco GM, et al. The adherence to the therapy in inflammatory bowel disease: beyond the number of the tablets. Scand J Gastroenterol. 2018;53(2):141–146. doi:10.1080/00365521.2017.1405070
36. Amiesimaka OI, Braund R, Aluzaite K, Schultz M. Using electronic health records in analysing medication adherence in southern New Zealand patients with inflammatory bowel diseases. N Z Med J. 2024;137(1588):25–36. doi:10.26635/6965.6209
37. Vangeli E, Bakhshi S, Baker A, et al. A systematic review of factors associated with non-adherence to treatment for immune-mediated inflammatory diseases. Adv Ther. 2015;32(11):983–1028. doi:10.1007/s12325-015-0256-7
38. Chan W, Chen A, Tiao D, Selinger C, Leong R. Medication adherence in inflammatory bowel disease. Intest Res. 2017;15(4):434–445. doi:10.5217/ir.2017.15.4.434
39. Greenley RN, Kunz JH, Walter J, Hommel KA. Practical strategies for enhancing adherence to treatment regimen in inflammatory bowel disease. Inflamm Bowel Dis. 2013;19(7):1534–1545. doi:10.1097/MIB.0b013e3182813482
40. Ashok K, Mathew AA, Thomas A, Mohan D, Gopalakrishna R, Reghu R. Clinical Pharmacist’s Interventions on medication adherence and knowledge of inflammatory bowel disease patients. J Young Pharm. 2017;9(3):381–385. doi:10.5530/jyp.2017.9.76
41. Tiao DK, Chan W, Jeganathan J, et al. Inflammatory bowel disease pharmacist adherence counseling improves medication adherence in crohn’s disease and ulcerative colitis. Inflamm Bowel Dis. 2017;23(8):1257–1261. doi:10.1097/MIB.0000000000001194
42. Jeganathan J, Lee CH, Rahme A, et al. Pediatric-to-adult transition and medication adherence in patients with inflammatory bowel disease. Inflamm Bowel Dis. 2017;23(7):1065–1070. doi:10.1097/MIB.0000000000001114
43. Nikolaus S, Schreiber S, Siegmund B, et al. Patient education in a 14-month randomised trial fails to improve adherence in ulcerative colitis: influence of demographic and clinical parameters on non-adherence. J Crohns Colitis. 2017;11(9):1052–1062. doi:10.1093/ecco-jcc/jjx062
44. Lofland JH, Johnson PT, Ingham MP, Rosemas SC, White JC, Ellis L. Shared decision-making for biologic treatment of autoimmune disease: influence on adherence, persistence, satisfaction, and health care costs. Patient Prefer Adherence. 2017;11:947–958. doi:10.2147/PPA.S133222
45. Miloh T, Shub M, Montes R, Ingebo K, Silber G, Pasternak B. Text messaging effect on adherence in children with inflammatory bowel disease. J Pediatr Gastroenterol Nutr. 2017;64(6):939–942. doi:10.1097/MPG.0000000000001399
46. Carlsen K, Jakobsen C, Houen G, et al. Self-managed eHealth disease monitoring in children and adolescents with inflammatory bowel disease: a randomized controlled trial. Inflamm Bowel Dis. 2017;23(3):357–365. doi:10.1097/MIB.0000000000001170
47. Gillespie D, Hood K, Farewell D, Stenson R, Probert C, Hawthorne AB. Electronic monitoring of medication adherence in a 1-year clinical study of 2 dosing regimens of mesalazine for adults in remission with ulcerative colitis. Inflamm Bowel Dis. 2014;20(1):82–91. doi:10.1097/01.MIB.0000437500.60546.2a
48. Park SK, Park SH, Eun CS, et al. Adherence to asacol once daily versus divided regimen for maintenance therapy in ulcerative colitis: a prospective, multicenter, randomized study. Intest Res. 2019;17(3):349–356. doi:10.5217/ir.2018.00064
49. Schultheiss JPD, Altena S, Clevers MR, Baas D, Jharap B, Fidder HH. Adherence to adalimumab was not improved by a reminder-based intervention with an electronic needle container. Dig Dis Sci. 2021;66(5):1477–1487. doi:10.1007/s10620-020-06395-z
50. Greenley RN, Gumidyala AP, Nguyen E, et al. Can you teach a teen new tricks? Problem solving skills training improves oral medication adherence in pediatric patients with inflammatory bowel disease participating in a randomized trial. Inflamm Bowel Dis. 2015;21(11):2649–2657. doi:10.1097/MIB.0000000000000530
51. Pedersen N, Thielsen P, Martinsen L, et al. eHealth: individualization of mesalazine treatment through a self-managed web-based solution in mild-to-moderate ulcerative colitis. Inflamm Bowel Dis. 2014;20(12):2276–2285. doi:10.1097/MIB.0000000000000199
52. Del Hoyo J, Nos P, Faubel R, et al. A web-based telemanagement system for improving disease activity and quality of life in patients with complex inflammatory bowel disease: pilot randomized controlled trial. J Med Internet Res. 2018;20(11):e11602. doi:10.2196/11602
53. Brixner D, Rubin DT, Mease P, et al. Patient support program increased medication adherence with lower total health care costs despite increased drug spending. J Manag Care Spec Pharm. 2019;25(7):770–779. doi:10.18553/jmcp.2019.18443
54. Rubin DT, Mittal M, Davis M, Johnson S, Chao J, Skup M. Impact of a patient support program on patient adherence to adalimumab and direct medical costs in crohn’s disease, ulcerative colitis, rheumatoid arthritis, psoriasis, psoriatic arthritis, and ankylosing spondylitis. J Manag Care Spec Pharm. 2017;23(8):859–867. doi:10.18553/jmcp.2017.16272
55. Maddux M, Ricks S, Delurgio S, Hommel K. A pilot study evaluating the impact of an adherence-promoting intervention among nonadherent youth with inflammatory bowel disease. J Pediatr Nurs. 2017;35:72–77. doi:10.1016/j.pedn.2017.03.006
56. Chapman S, Sibelli A, St-Clair Jones A, Forbes A, Chater A, Horne R. Personalised adherence support for maintenance treatment of inflammatory bowel disease: a tailored digital intervention to change adherence-related beliefs and barriers. J Crohns Colitis. 2020;14(10):1394–1404. doi:10.1093/ecco-jcc/jjz034
57. de Jong MJ, van der Meulen-de Jong AE, Romberg-Camps MJ, et al. Telemedicine for management of inflammatory bowel disease (myIBDcoach): a pragmatic, multicentre, randomised controlled trial. Lancet. 2017;390(10098):959–968. doi:10.1016/S0140-6736(17)31327-2
58. Linn AJ, van Dijk L, van Weert JCM, Gebeyehu BG, van Bodegraven AA, Smit EG. Creating a synergy effect: a cluster randomized controlled trial testing the effect of a tailored multimedia intervention on patient outcomes. Patient Educ Couns. 2018;101(8):1419–1426. doi:10.1016/j.pec.2018.03.017
59. Arnet I, Greenland M, Knuiman MW, et al. Operationalization and validation of a novel method to calculate adherence to polypharmacy with refill data from the Australian pharmaceutical benefits scheme (PBS) database. Clin Epidemiol. 2018;10:1181–1194. doi:10.2147/CLEP.S153496
60. Kini V, Ho PM. Interventions to Improve Medication Adherence: a Review. JAMA. 2018;320(23):2461–2473. doi:10.1001/jama.2018.19271
61. de Jong M, van der Meulen-de Jong A, Romberg-Camps M, et al. Development and feasibility study of a telemedicine tool for all patients with IBD: myIBDcoach. Inflamm Bowel Dis. 2017;23(4):485–493. doi:10.1097/MIB.0000000000001034
62. Hunt MG, Loftus P, Accardo M, Keenan M, Cohen L, Osterman MT. Self-help cognitive behavioral therapy improves health-related quality of life for inflammatory bowel disease patients: a randomized controlled effectiveness trial. J Clin Psychol Med Settings. 2020;27(3):467–479. doi:10.1007/s10880-019-09621-7
63. Stapersma L, van den Brink G, van der Ende J, et al. Psychological outcomes of a cognitive behavioral therapy for youth with inflammatory bowel disease: results of the HAPPY-IBD randomized controlled trial at 6- and 12-month follow-up. J Clin Psychol Med Settings. 2020;27(3):490–506. doi:10.1007/s10880-019-09649-9
64. Gravina AG, Pellegrino R, Palladino G, et al. Targeting the gut-brain axis for therapeutic adherence in patients with inflammatory bowel disease: a review on the role of psychotherapy. Brain-Apparatus Commun. 2023;2(1):2181101.
65. Ankersen DV, Carlsen K, Marker D, Munkholm P, Burisch J. Using eHealth strategies in delivering dietary and other therapies in patients with irritable bowel syndrome and inflammatory bowel disease. J Gastroenterol Hepatol. 2017;32(Suppl 1):27–31. doi:10.1111/jgh.13691
66. George LA, Cross RK. Remote Monitoring and Telemedicine in IBD: are We There Yet? Curr Gastroenterol Rep. 2020;22(3):12. doi:10.1007/s11894-020-0751-0
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.