")
Back to Journals » Journal of Asthma and Allergy » Volume 15
Increase in FeNO Levels Following IL5/IL5R-Targeting Therapies in Severe Asthma: A Case Series
Authors Pelletier G , Godbout K, Boulay MÈ, Boulet LP, Morissette MC, Côté A
Received 19 January 2022
Accepted for publication 22 April 2022
Published 19 May 2022 Volume 2022:15 Pages 691—701
DOI https://doi.org/10.2147/JAA.S358877
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Amrita Dosanjh
Geneviève Pelletier,1 Krystelle Godbout,1,2 Marie-Ève Boulay,1 Louis-Philippe Boulet,1,2 Mathieu C Morissette,1,2 Andréanne Côté1,2
1Quebec Heart and Lung Institute – Laval University, Quebec, QC, Canada; 2Department of Medicine, Faculty of Medicine, Laval University, Quebec, QC, Canada
Correspondence: Andréanne Côté, Quebec Heart and Lung Institute – Laval University, 2725 chemin Sainte-Foy, Quebec, QC, G1V 4G5, Canada, Tel +1 418 656 4747, Fax +1 418 656 4762, Email [email protected]
Purpose: Monoclonal antibodies targeting interleukin-5 (IL5) and its receptor (IL5R), used for severe asthma treatment, reduce eosinophils to almost complete depletion. Fractional exhaled nitric oxide (FeNO), a surrogate marker of eosinophilic airway inflammation, is expected to decrease after their initiation. Our center noticed increased FeNO levels in a few patients in whom anti-IL5/IL5R therapy was initiated. Limited data are available on the kinetics of T2 inflammation biomarkers after initiation of a biologic in that population. This study aims to identify if a subgroup of severe asthma patients experiences increased FeNO levels after initiation of anti-IL5/IL5R therapy and to describe their clinical characteristics.
Patients and Methods: This is a retrospective case series of 5 patients on Benralizumab (4M:1F) and 8 on Mepolizumab (5M:3F) who showed a significant increase in FeNO (> 20% AND > 25 ppb) following initiation of an anti-IL5/IL5R treatment. Clinical data, expiratory flows, and inflammation were extracted from the patients’ chart at initiation of treatment (T0), 3 months (T1) and 12 months (T2) post-treatment. Descriptive statistics were used.
Results: In patients treated with Benralizumab, the increase in FeNO was observed between T0 and T1 (mean delta = 82 ± 72 ppb) with a subsequent decrease (N = 3). In most patients taking Mepolizumab (N = 6), the FeNO increase was observed between T1 and T2 (mean delta = 57 ± 35 ppb). Under treatment, no Benralizumab patient experienced asthma exacerbation while two on Mepolizumab did. All patients had a significant decrease in blood eosinophils.
Conclusion: Although initiation of anti-IL5/IL5R may cause a transient rise in FeNO levels in a subgroup of patients, it does not appear to affect clinical outcomes. A compensatory mechanism involving other inflammatory pathways such as IL13 or IL4, both involved in FeNO production, could theoretically explain these findings. Further investigation is needed to elucidate the actual underlying mechanisms.
Keywords: biologics, biomarkers, Benralizumab, Mepolizumab
Introduction
About 8% of individuals with asthma suffer from a severe form of the disease.1 Severe asthma is associated with a significant deterioration in quality of life2 and increased prevalence in asthma exacerbations and hospitalizations.3
Until recently, therapeutic options available for this population were limited. Our knowledge of the cellular and molecular pathophysiology of asthma has increased in the past two decades. Those complex inflammatory pathways can be divided into two main inflammatory types based on the presence of type 2 (T2) inflammation (T2 asthma) or not (non-T2 asthma). T2 asthma results in an exaggerated production of eosinophils and worst disease control. A high proportion of severe asthmatics display a T2 inflammation profile but fortunately, novel therapies targeting T2 inflammation have improved their disease burden.4 As interleukin-5 (IL5) is the main cytokine involved in the activation and survival of eosinophils, treatments targeting this cytokine (anti-IL5: Mepolizumab and Reslizumab) or its receptor (anti-IL5R: Benralizumab) have been shown particularly effective in reducing exacerbations and need for systemic corticosteroids in severe eosinophilic asthma.5
Fractional exhaled nitric oxide (FeNO) is a non-invasive and accessible marker of airway inflammation and helps predict asthma exacerbations.6 It is the most proximal readout of airway inflammation, and is often referred to as a surrogate marker of eosinophilic airway inflammation, although correlation is far from perfect.7 FeNO is expected to decrease after initiation of anti-IL5/IL5R therapies. Although Phase 2b studies for Mepolizumab8 and Benralizumab9 included longitudinal measurements of FeNO, this was not assessed in Phase 3 studies for either of these therapies, preventing identification of unusual FeNO patterns and correlation with clinical outcomes. Studies are therefore needed to determine if FeNO is a reliable biomarker of response to anti-IL5/IL5R treatment and to assess the effect of anti-IL5/IL5R on FeNO.
We observed an increase in FeNO levels in a small proportion of patients treated at the severe asthma clinic of the Quebec Heart and Lung Institute (IUCPQ) whom recently initiated therapies targeting anti-IL5/IL5R. Two similar cases have been previously briefly presented,10 although to our knowledge no detailed report has been published.
Limited data are available on the kinetics of the various biomarkers involved in T2 inflammation after initiation of treatment with a biologic. Herein, we report a case series of patients with severe asthma treated with anti-IL5/IL5R monoclonal antibodies who showed an increase in FeNO levels after initiating treatment. Clinical characteristics and outcomes were analyzed along with changes in FeNO.
Patients and Methods
This is a retrospective case series of adult patients who initiated treatment with either Benralizumab or Mepolizumab at the IUCPQ’s severe asthma clinic between January 2016 and June 2020. Patients on Benralizumab received a dose of 30 mg every 4 weeks for the first 3 doses, then every 8 weeks, while patients on Mepolizumab received doses of 100 mg every 4 weeks.
Patients who received at least 3 doses of anti-IL5/IL5R therapy and showed a significant increase in FeNO, defined as >20% and >25 ppb difference between at least two visits, as defined by the American Thoracic Society (ATS),11,12 were identified. All patients had severe asthma, which was defined as asthma that required treatment with daily high-dose inhaled corticosteroids (ICS) (>500 mcg/day fluticasone or equivalent) and a second controller for the previous year, or systemic corticosteroids (OCS) for 50% of the previous year to prevent it from becoming uncontrolled, or which remained uncontrolled despite this therapy.1 Patients with confounding comorbidities such as eosinophilic granulomatosis with polyangiitis (EGPA) or hypereosinophilic syndrome were excluded.
Data was retrospectively collected from the patient’s hospital file at T0 (before treatment initiation, 0±3 months), T1 (3±3 months) and T2 (12±4 months) of therapy.
Baseline characteristics included age, sex, asthma onset, body mass index (BMI), smoking history and asthma comorbidities. The primary outcome was the change in FeNO between two visits (T0-T1, T1-T2 and T0-T2), expressed in parts per billion (ppb). Secondary outcomes included blood eosinophils (X106 cells/L), sputum eosinophils (cell %), forced expiratory volume in one second (FEV1 in L and %), concomitant use and dose of oral corticosteroids (OCS) and inhaled corticosteroids (ICS). Severe asthma exacerbations, defined as those requiring OCS, emergency room visit or hospitalization, were also extracted as a secondary outcome and reported for the year prior to baseline visit and between baseline and T1, or between T1 and T2 follow-up visits.
Cases are presented using descriptive statistics. Continuous variables are presented as means ± standard deviation (range), whereas categorical variables are reported as numbers (%). We also analyzed FeNO values by dividing them into 4 zones, according to Liu J et al’s cut-offs,13 inspired by the ATS FeNO guideline11 (green or normal: ≤25 ppb, yellow: 26–49 ppb, orange: 50–99 ppb and red or ultra-high: ≥100 ppb). SAS v9.4 (SAS Institute, Cary, NC) was used to generate summary statistics.
This case series was prepared following the CARE guidelines. The study was approved by the research ethics committee of the Quebec Heart and Lung Institute-Laval University (CÉR 21937) and complies with the Declaration of Helsinki. As all data were collected from the patients’ clinical files and no contact with participants was required, approval was obtained from the director of professional services, waiving the requirement for informed consent.
Results
Between January 2016 and June 2020, 222 patients received an anti IL5/IL5R therapy at the IUCPQ asthma clinic. Of those, 166 did not have at least two FeNO measurements and one had EGPA, leaving 55 eligible patients (Figure 1). 5/15 (33%) patients initiated on Benralizumab and 8/40 (20%) on Mepolizumab had a significant FeNO increase (Figure 1). Baseline characteristics of those 13 patients are presented in Table 1. More ex-smokers were found in the Benralizumab-treated group (60% vs 40% for Mepolizumab-treated). Atopy was the most frequent comorbidity (Benralizumab-treated 100%; Mepolizumab-treated 75%) followed by nasal polyposis (Benralizumab-treated 60%; Mepolizumab-treated 63%). All five Benralizumab patients were previously treated with Mepolizumab and switched to Benralizumab between their T0 and T1 visits. At their T1 follow-up visit, they all had received at least 3 doses of Benralizumab (Table 1).
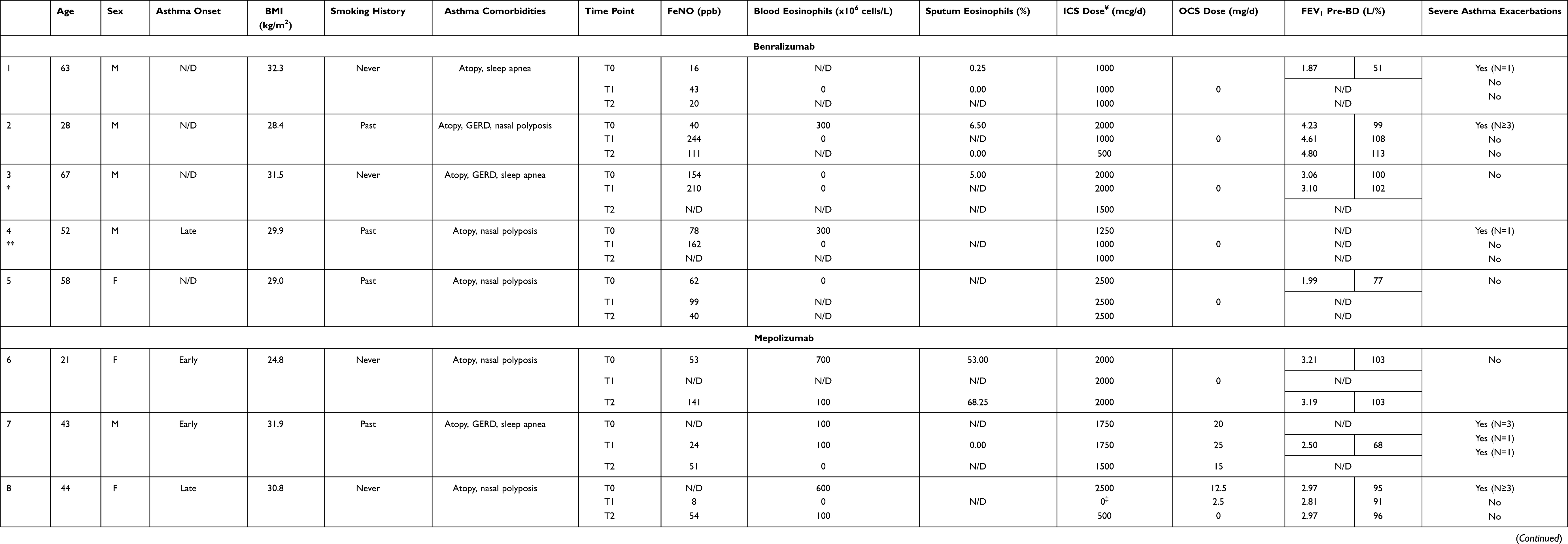 |
Table 1 Characteristics of Cases Before Initiating Anti-IL5/IL5R Therapies and at 3- and 12-Months Post-Treatment Initiation |
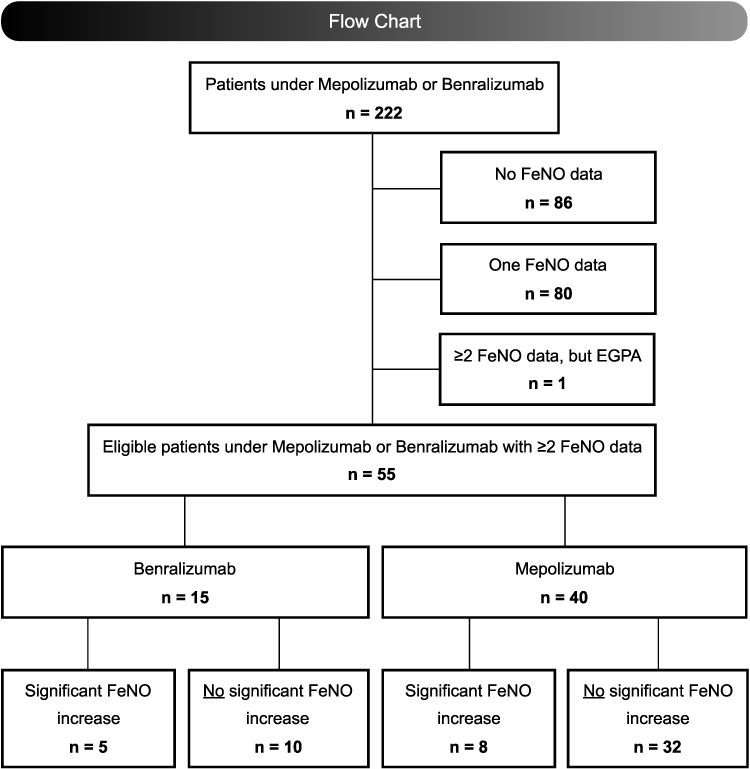 |
Figure 1 Flow chart of study participants. Abbreviations: FeNO, fractional exhaled nitric oxide; EGPA, eosinophilic granulomatosis with polyangiitis. |
FeNO
For all 5 patients on Benralizumab, the increase in FeNO levels happened shortly after initiation, between T0 and T1, with a mean increase of 82 ± 72 ppb (range = 27 to 204 ppb). Three patients with an available FeNO measurement at T2 showed that the value subsequently decreased but only one reached normal value (Figure 2A). Conversely, most patients treated with Mepolizumab (5/8, 63%) showed a late increase in FeNO (between T1 and T2) with a mean increase of 57 ± 35 ppb (range = 27 to 118 ppb) (Figure 2B). The magnitude of FeNO levels according to color zones is shown in Figure 2A and B. Overall, 7/13 patients reached the ultra-high level zone at some point after initiating their treatment.
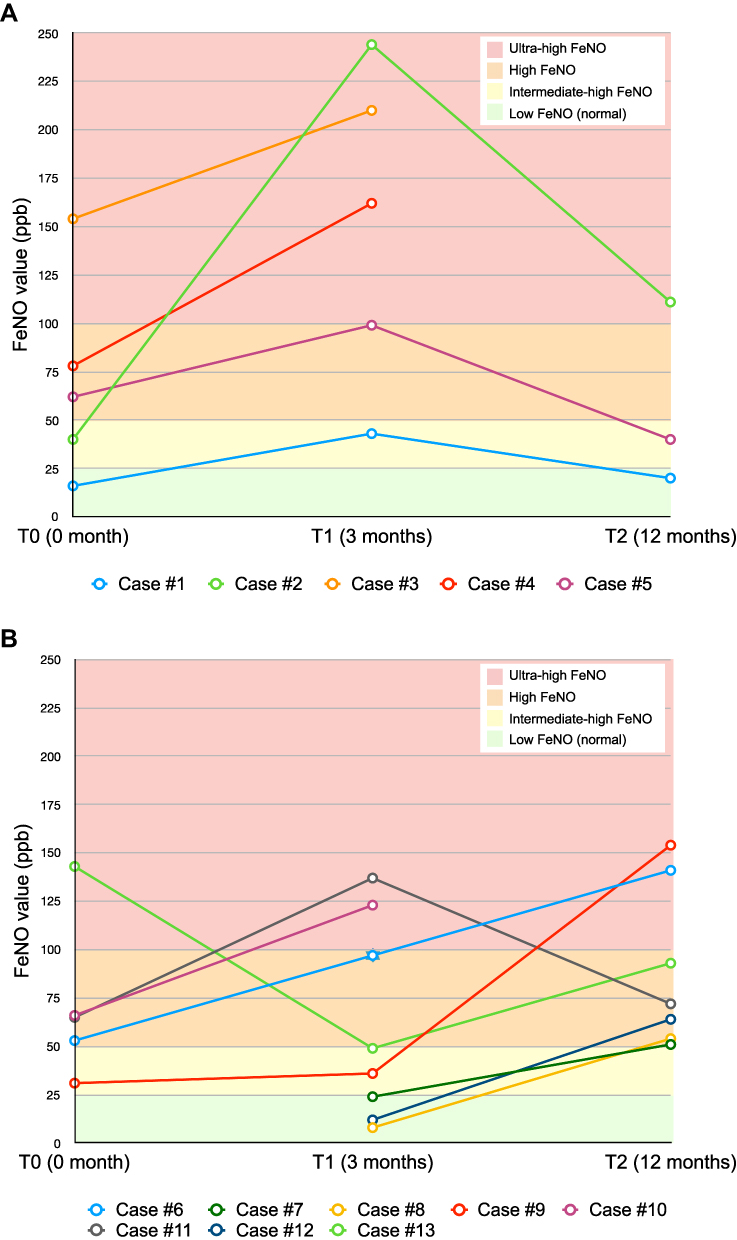 |
Figure 2 FeNO values at T0, T1 and T2 for patients who experienced a significant increase in FeNO between at least two time points on (A) Benralizumab and (B) Mepolizumab: The background colors (green, yellow, orange, red) help interpret FeNO levels: The green zone is low FeNO (≤25 ppb), which corresponds to normal values: Intermediate-high FeNO = 26–49 ppb, high FeNO = 50–99 ppb, and ultra-high FeNO = ≥100 ppb: Note that the incomplete curves are explained by missing data at T0 or T2: For case #6 who had missing data at T1, we assigned a fictive value at T1, representing the mean of T0 and T2: This estimated value is only used in this graph to help visualize the variation between T0 and T2 but was not considered in data analysis. |
Blood and Sputum Eosinophils
Despite that all Benralizumab patients were previously treated with Mepolizumab, 3/5 patients showed evidence of residual eosinophilic inflammation at their baseline visit on Benralizumab (blood eosinophils at 300x106 cells/L for 2 of them and sputum eosinophils at 5.00% for the other). Data is lacking for the two other patients to conclude in the absence of residual eosinophilic inflammation. At T1, blood eosinophils were undetectable (N = 4) while at T2, no data was available. Sputum eosinophils were also undetectable at T1 and T2 for the only 2 patients for whom we had data (Table 1).
Patients on Mepolizumab had baseline blood eosinophils between 100 and 1810×106 cells/L (N = 7). They subsequently decreased to undetectable levels (T1: N = 4, T2: N = 3) or 100×106 cells/L (T1: N = 3, T2: N = 3). Among the 4 patients for whom sputum eosinophils data were available at T1 or T2, 3 patients had residual eosinophilic inflammation (Table 1).
Severe Asthma Exacerbation
In the year preceding the baseline visit (T0), 5 patients (63%) on Mepolizumab had ≥2 severe asthma exacerbations. 2/3 patients with zero or one asthma exacerbation were taking OCS at baseline. For Benralizumab patients, 4/5 experienced 0–1 exacerbation in the year preceding Benralizumab initiation (while on Mepolizumab) whereas one had ≥3 severe asthma exacerbations during the same period of time.
After starting their respective anti-IL5/IL5R treatment, no patient on Benralizumab experienced an asthma exacerbation compared to two (25%) on Mepolizumab. Those two patients, cases #7 and 12, however reduced their exacerbation numbers after the drug initiation, from 3 to 1 and 9 to 1, respectively (Table 1).
Inhaled Corticosteroids (ICS) and Oral Corticosteroids (OCS) Use
Of all patients taking Benralizumab, none used OCS at baseline or over the 12-month treatment period. Two patients (40%) had stable ICS doses throughout the 3 time points, whereas 3 (60%) underwent a dose reduction.
Among the 8 patients on Mepolizumab, 4 (50%) were taking OCS at treatment initiation (mean dose = 11.5 mg/day), 6 (75%) at T1 (mean dose = 9.2 mg/day) and one (13%) at T2 (15.0 mg/day (he had 20.0 mg/day at T0)). ICS doses remained stable for two patients (25%), while 4 (50%) had a dose reduction and two increased (25%). The two Mepolizumab’s patients who experienced a severe asthma exacerbation while on therapy previously had a dose reduction in their ICS and OCS doses.
Discussion
This retrospective case series describes 5 patients on Benralizumab and 8 on Mepolizumab who presented a significant FeNO increase between at least two visits in the year following treatment initiation. The increase in FeNO levels on Benralizumab appears to happen earlier and be more marked than with Mepolizumab. All cases had favorable clinical outcomes under anti-IL5/IL5R therapies suggesting that these remain effective despite this FeNO increase. Blood and sputum eosinophils were undetectable for patients on Benralizumab at 3 and 12 months, while they were low for most patients on Mepolizumab.
Exhaled nitric oxide (NO) is synthesized in the bronchial epithelium by the inducible nitric oxide synthase (iNOS) enzyme under physiological conditions.14 In asthmatic patients, cytokines and inflammatory mediators induce an excessive NO production by stimulating iNOS via activation of the IL13 and IL4 pathways. Therefore, FeNO is often used as a surrogate biomarker that reflects the underlying bronchial T2 inflammation.15 Hence, one would expect a decrease in FeNO following treatment with anti-IL5/IL5R antibodies although FeNO is not directly related to the IL5 pathway. However, as all inflammatory pathways are interrelated, it is possible that blocking the IL5 upregulates IL13 and IL4 pathways, which increases FeNO through compensatory mechanisms.
A similar phenomenon is observed with Dupilumab, a monoclonal antibody targeting IL4 and IL13, where a paradoxical rise in blood eosinophils occurs in a subset of patients. In phase 3 studies, very high blood eosinophils levels (≥3000 cells/mm3) were reported in 13% of Venture’s patients (all OCS-dependent patients)16 and 1.2% of Quest’s patients.16,17 This rise was transient, with a return to baseline levels by the end of treatment, and good clinical outcomes. An earlier phase 2 study also reported a marked blood eosinophils rise (>200%) in 4/44 Dupilumab patients.18 It is possible that this blood eosinophils rise reflects an upregulation of IL5 pathway when blocking IL4 and IL13 with Dupilumab, reinforcing the compensatory mechanism theory.
The precise effects of anti-IL5/IL5R antibodies on FeNO remain unknown since this outcome was not included in phase 3 studies. However, a prospective real-life study on Benralizumab (J-BEST),19 a retrospective study on anti-IL5 therapies by Ramonell et al20 and a real-world settings study on Mepolizumab21 reported no significant change in FeNO despite a significant reduction in blood eosinophils19,21 and significant clinical benefits from the therapy.19–21 These suggest that the therapeutic effect of anti-IL5/IL5R does not correlate with FeNO levels. Our findings support these studies since all our patients had good clinical outcomes despite FeNO increase. In addition, a real-world study by Pelaia et al suggested that blood eosinophil count is clinically more relevant than FeNO to evaluate the overall efficacy of IL5/IL5R-targeting therapies, even though FeNO might be useful as an accessory inflammatory biomarker.22
Many factors influence FeNO levels. Some of them increase FeNO, such as permanent and/or elevated exposure to allergens,11 atopy23 and nasal polyposis. Polyps are an expression site for iNOS, which stimulates NO production.24,25 Among our studied patients, 11/13 had atopy and 8/13 had nasal polyposis. These patient’s asthma pathophysiology is characterized by elevated IL5/IL13/IL4 that might predispose them to higher FeNO levels.26 Other factors reduce FeNO levels, such as cigarette smoke by its negative feedback on NO production27 and corticosteroids use which down-regulates iNOS expression.14 The variation in steroid medications in some of our patients possibly explains why we observed a FeNO rise instead of a maintenance.
The clinical benefits observed in this study are in line with previous studies. Anti-IL5/IL5R monoclonal antibodies lead to significant reduction in asthma exacerbations,8,28–30 corticosteroids use,31,32 and sputum and blood eosinophils33 in severe eosinophilic asthmatics. The greater decrease in eosinophils we observed with Benralizumab compared to Mepolizumab is consistent with their respective mechanisms of action. Mepolizumab reduces eosinophils in a passive manner as it binds to IL5 and prevents its action.34 Benralizumab’s complete eosinophilic suppression35 might induce greater upregulation of the IL4/IL13 pathways than Mepolizumab, and consequently, a greater FeNO rise. This may also explain the interesting observation that despite being previously on Mepolizumab, all Benralizumab patients experienced a significant FeNO rise after the transition of therapies. In fact, there was a residual eosinophilic inflammation under Mepolizumab that was confirmed in 4/5 of them.
The earlier rise in FeNO with Benralizumab could be explained by its mechanism of action, which results in a faster reduction in blood eosinophils.22,36 However, more Mepolizumab patients were on OCS at treatment initiation and those were subsequently weaned in all but one. As most of the patients who underwent OCS withdrawal showed a later rise in FeNO, OCS reduction rather than the drug mechanism is an alternative explanation for the late FeNO increase with Mepolizumab.
The greatest limitation of this study arises from its retrospective design. Most patients who initiated an anti-IL5/IL5R therapy at the IUCPQ’s severe asthma clinic could not be included due to insufficient FeNO measurements (<2 time points). There is also a great difference in the number of eligible patients for the two studied medications, Benralizumab (N = 15) and Mepolizumab (N = 40). This, especially for Benralizumab patients, can have overestimated the variation in FeNO. Although FeNO is frequently used in follow-up visits at our institution, it is not statutory and different practices exist among physicians. Even though our small sample does not allow for conclusions on the causes of these FeNO increases, nor on the relevance of using FeNO in monitoring patients under anti-IL5/IL5R monoclonal antibody therapies, we believe that this clinical phenomenon is not a coincidence and requires further investigation.
Conclusion
Initiation of anti-IL5/IL5R may cause a transient rise in FeNO levels in a subgroup of patients, without obvious clinical influence. Although this should be assessed in a larger cohort of patients, our observations raise questions about compensatory mechanisms triggered by eosinophilic depletion following the initiation of Benralizumab and Mepolizumab. By blocking the IL5 that acts at the end of the inflammatory cascade, without removal of the upstream trigger, anti-IL5/IL5R therapies may result in overactivation of parallel or more upstream inflammatory pathways which may include IL13 or IL4 pathways, both involved in FeNO production. The paradoxical increase in eosinophils following blockage of the IL13 and IL4 pathways with Dupilumab reinforces our theory of a possible compensatory mechanism. The mechanisms underlying these rises deserve further investigation as they could be key in the development of novel therapy or early identification of loss of response to the available actual monoclonal antibodies.
Abbreviations
BMI, Body-mass index; EGPA, Eosinophilic granulomatosis with polyangiitis; FeNO, Fractional exhaled nitric oxide; FEV1, Forced expiratory volume in one second; GERD, Gastroesophageal reflux disease; ICS, Inhaled corticosteroids; IL-4, Interleukin-4; IL-5, Interleukin-5; IL-5R, Receptor of the IL-5; IL-13, Interleukin-13; iNOS, inducible nitric oxide synthase; IUCPQ, Quebec Heart and Lung Institute; mcg, microgram; mg, milligram; NO, Nitric oxide; OCS, Oral corticosteroids; ppb, parts per billion; T2 inflammation, Type 2 inflammation.
Acknowledgments
There are no other collaborators to declare.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by AC research funds: There are no other financial disclosures or sponsors to declare.
Disclosure
KG reports grants and personal fees from AstraZeneca, Covis, Novartis, and Sanofi, personal fees from GSK, Merck, TEVA, and Valeo, outside the submitted work. LPB considers having no conflict of interest related to this study, but wishes to declare what can be perceived as potential conflicts of interest: Research grants for participation to multicentre studies, AstraZeneca, Boston Scientific, GlaxoSmithKline, Hoffman La Roche, Novartis, Ono Pharma, Sanofi, Takeda: Support for research projects introduced by the investigator, AstraZeneca, Boehringer-Ingelheim, GlaxoSmithKline, Merck, Takeda: Fee for consulting and advisory boards, Astra Zeneca, Novartis, Methapharm: Nonprofit grants for production of educational materials, AstraZeneca, Boehringer-Ingelheim, GlaxoSmithKline, Merck, Novartis: Conference fees, AstraZeneca, GlaxoSmithKline, Merck, Novartis. AC considers having no conflict of interest related to this study, but wishes to declare what can be perceived as potential conflicts of interest: Research grants for participation to multicentre studies, AstraZeneca: Fee for consulting and advisory boards, AstraZeneca, Sanofi: The authors report no other conflicts of interest in this work.
References
1. FitzGerald JMLC, Lougheed MD, Lougheed MD, et al. Recognition and management of severe asthma, A Canadian Thoracic Society position statement. Can J Respir Crit Care Sleep Med. 2017;1(4):199–221. doi:10.1080/24745332.2017.1395250
2. Shaw DE, Sousa AR, Fowler SJ, et al. Clinical and inflammatory characteristics of the European U-BIOPRED adult severe asthma cohort. Eur Respir J. 2015;46(5):1308–1321. doi:10.1183/13993003.00779-2015
3. Global initiative for asthma. Difficult-to-treat & Severe asthma in adolescent and adult patients - diagnosis and management. Available from: www.ginasthma.org.
4. Schleich FN, Chevremont A, Paulus V, et al. Importance of concomitant local and systemic eosinophilia in uncontrolled asthma. Eur Respir J. 2014;44(1):97–108. doi:10.1183/09031936.00201813
5. Coverstone AM, Seibold MA, Peters MC. Diagnosis and management of T2-high asthma. J Allergy Clin Immunol Pract. 2020;8(2):442–450. doi:10.1016/j.jaip.2019.11.020
6. Donohue JF, Jain N. Exhaled nitric oxide to predict corticosteroid responsiveness and reduce asthma exacerbation rates. Respir Med. 2013;107(7):943–952. doi:10.1016/j.rmed.2013.02.018
7. Szefler SJ, Wenzel S, Brown R, et al. Asthma outcomes, biomarkers. J Allergy Clin Immunol. 2012;129(3Suppl):S9–23. doi:10.1016/j.jaci.2011.12.979
8. Pavord ID, Korn S, Howarth P, et al. Mepolizumab for severe eosinophilic asthma (DREAM), a multicentre, double-blind, placebo-controlled trial. Lancet. 2012;380(9842):651–659. doi:10.1016/s0140-6736(12)60988-x
9. Castro M, Wenzel SE, Bleecker ER, et al. Benralizumab, an anti-interleukin 5 receptor α monoclonal antibody, versus placebo for uncontrolled eosinophilic asthma, a phase 2b randomised dose-ranging study. Lancet Respir Med. 2014;2(11):879–890. doi:10.1016/s2213-2600(14)70201-2
10. Hsu C, Diaz J. M201 should FENO be used as a biomarker to measure response to benralizumab? Ann Allergy Asthma Immunol. 2019;123(5):S99. doi:10.1016/j.anai.2019.08.188
11. Dweik RA, Boggs PB, Erzurum SC, et al. An official ATS clinical practice guideline, interpretation of exhaled nitric oxide levels (FENO) for clinical applications. Am J Respir Crit Care Med. 2011;184(5):602–615. doi:10.1164/rccm.9120-11ST
12. Jeppegaard M, Veidal S, Sverrild A, Backer V, Porsbjerg C. Validation of ATS clinical practice guideline cut-points for FeNO in asthma. Respir Med. 2018;144:22–29. doi:10.1016/j.rmed.2018.09.014
13. Liu J, Xu R, Zhan C, et al. Clinical utility of ultrahigh fractional exhaled nitric oxide in predicting bronchial hyperresponsiveness in patients with suspected asthma. Postgrad Med J. 2019;95(1128):541–546. doi:10.1136/postgradmedj-2018-136333
14. Guo FH, De Raeve HR, Rice TW, Stuehr DJ, Thunnissen FB, Erzurum SC. Continuous nitric oxide synthesis by inducible nitric oxide synthase in normal human airway epithelium in vivo. Proc Natl Acad Sci U S A. 1995;92(17):7809–7813. doi:10.1073/pnas.92.17.7809
15. Duong-Quy S. Clinical utility of the exhaled Nitric Oxide (NO) measurement with portable devices in the management of allergic airway inflammation and asthma. J Asthma Allergy. 2019;12:331–341. doi:10.2147/jaa.S190489
16. Rabe KF, Nair P, Brusselle G, et al. Efficacy and safety of dupilumab in glucocorticoid-dependent severe asthma. N Engl J Med. 2018;378(26):2475–2485. doi:10.1056/NEJMoa1804093
17. Castro M, Corren J, Pavord ID, et al. Dupilumab efficacy and safety in moderate-to-severe uncontrolled asthma. N Engl J Med. 2018;378(26):2486–2496. doi:10.1056/NEJMoa1804092
18. Wenzel S, Ford L, Pearlman D, et al. Dupilumab in persistent asthma with elevated eosinophil levels. N Engl J Med. 2013;368(26):2455–2466. doi:10.1056/NEJMoa1304048
19. Izumo T, Tone M, Kuse N, et al. Effectiveness and safety of benralizumab for severe asthma in clinical practice (J-BEST), a prospective study. Ann Transl Med. 2020;8(7):438. doi:10.21037/atm.2020.04.01
20. Ramonell RP, Lee FE, Levy JM, Kuruvilla M. Exhaled nitric oxide measurements are not influenced by anti-eosinophil therapy in patients with asthma, A retrospective analysis. Ann Allergy Asthma Immunol. 2021;126(1):102–104. doi:10.1016/j.anai.2020.09.005
21. Crimi C, Campisi R, Nolasco S, et al. Mepolizumab effectiveness in patients with severe eosinophilic asthma and co-presence of bronchiectasis, A real-world retrospective pilot study. Respir Med. 2021;185:106491. doi:10.1016/j.rmed.2021.106491
22. Pelaia C, Crimi C, Benfante A, et al. Therapeutic effects of benralizumab assessed in patients with severe eosinophilic asthma, real-life evaluation correlated with allergic and non-allergic phenotype expression. J Asthma Allergy. 2021;14:163–173. doi:10.2147/jaa.S297273
23. Gratziou C, Lignos M, Dassiou M, Roussos C. Influence of atopy on exhaled nitric oxide in patients with stable asthma and rhinitis. Eur Respir J. 1999;14(4):897–901. doi:10.1034/j.1399-3003.1999.14d28.x
24. Galli J, Montuschi P, Passàli GC, Laruffa M, Parrilla C, Paludetti G. Exhaled nitric oxide measurement in patients affected by nasal polyposis. Otolaryngol Head Neck Surg. 2012;147(2):351–356. doi:10.1177/0194599812442322
25. Watkins DN, Lewis RH, Basclain KA, et al. Expression and localization of the inducible isoform of nitric oxide synthase in nasal polyp epithelium. Clin Exp Allergy. 1998;28(2):211–219. doi:10.1046/j.1365-2222.1998.00215.x
26. Maniscalco M, Calabrese C, D’Amato M, et al. Association between exhaled nitric oxide and nasal polyposis in severe asthma. Respir Med. 2019;152:20–24. doi:10.1016/j.rmed.2019.04.017
27. Clearie KL, McKinlay L, Williamson PA, Lipworth BJ. Fluticasone/Salmeterol combination confers benefits in people with asthma who smoke. Chest. 2012;141(2):330–338. doi:10.1378/chest.11-0392
28. Bleecker ER, FitzGerald JM, Chanez P, et al. Efficacy and safety of benralizumab for patients with severe asthma uncontrolled with high-dosage inhaled corticosteroids and long-acting β(2)-agonists (SIROCCO), a randomised, multicentre, placebo-controlled phase 3 trial. Lancet. 2016;388(10056):2115–2127. doi:10.1016/s0140-6736(16)31324-1
29. FitzGerald JM, Bleecker ER, Nair P, et al. Benralizumab, an anti-interleukin-5 receptor α monoclonal antibody, as add-on treatment for patients with severe, uncontrolled, eosinophilic asthma (CALIMA), a randomised, double-blind, placebo-controlled phase 3 trial. Lancet. 2016;388(10056):2128–2141. doi:10.1016/s0140-6736(16)31322-8
30. Ortega HG, Liu MC, Pavord ID, et al. Mepolizumab treatment in patients with severe eosinophilic asthma. N Engl J Med. 2014;371(13):1198–1207. doi:10.1056/NEJMoa1403290
31. Haldar P, Brightling CE, Hargadon B, et al. Mepolizumab and exacerbations of refractory eosinophilic asthma. N Engl J Med. 2009;360(10):973–984. doi:10.1056/NEJMoa0808991
32. Nair P, Wenzel S, Rabe KF, et al. Oral glucocorticoid-sparing effect of benralizumab in severe asthma. N Engl J Med. 2017;376(25):2448–2458. doi:10.1056/NEJMoa1703501
33. Flood-Page P, Swenson C, Faiferman I, et al. A study to evaluate safety and efficacy of mepolizumab in patients with moderate persistent asthma. Am J Respir Crit Care Med. 2007;176(11):1062–1071. doi:10.1164/rccm.200701-085OC
34. GlaxoSmithKline. PRODUCT MONOGRAPH – NUCALA. Updated Nov 5; 2021. Available from: https://ca.gsk.com/media/6195/nucala-pm-en.pdf.
35. AstraZeneca. Product Monograph – Fasenra. Updated August 20; 2021. Available from: https://www.astrazeneca.ca/content/dam/az-ca/downloads/productinformation/fasenra-product%20monograph-en.pdf.
36. Moran AM, Ramakrishnan S, Borg CA, et al. Blood eosinophil depletion with mepolizumab, benralizumab, and prednisolone in eosinophilic asthma. Am J Respir Crit Care Med. 2020;202(9):1314–1316. doi:10.1164/rccm.202003-0729LE
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.