")
Back to Journals » Nursing: Research and Reviews » Volume 13
Intersectional Stigma Among Older People with HIV and COPD in Alabama: A Qualitative Study of Three Cases
Authors Byun JY , Chapman Lambert C, Fazeli PL, Iyer AS , Batey DS, Vance DE
Received 3 August 2023
Accepted for publication 13 December 2023
Published 20 December 2023 Volume 2023:13 Pages 77—85
DOI https://doi.org/10.2147/NRR.S433715
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marie-Pierre Gagnon
Jun Y Byun,1 Crystal Chapman Lambert,1 Pariya L Fazeli,1 Anand S Iyer,1,2 David Scott Batey,3 David E Vance1
1School of Nursing, University of Alabama at Birmingham, Birmingham, AL, USA; 2Division of Pulmonary, Allergy, and Critical Care Medicine, University of Alabama at Birmingham, Birmingham, AL, USA; 3School of Social Work, Tulane University, New Orleans, LA, USA
Correspondence: Jun Y Byun, School of Nursing, University of Alabama at Birmingham, 1701 University Boulevard, Birmingham, AL, 35294-4410, USA, Tel +1 205 427 5878, Email [email protected]
Introduction: Approximately 10– 23% of people living with HIV (PLWH) experience chronic obstructive pulmonary disease (COPD) due to increased life expectancy. HIV- and COPD-related stigma have been studied, respectively, showing detrimental effects on health outcomes. Despite the number of PLWH with COPD and the potential negative synergistic effect of having both conditions, the intersectional stigma of HIV and COPD remains largely unexplored. Therefore, this qualitative study aimed to explore experiences related to intersectional stigma in older PLWH with COPD.
Methods: We recruited three PLWH with COPD aged 50 years or older from an HIV clinic in Alabama. The sample size was determined according to the purpose of the study to understand the depth of the phenomenon, rather than its breadth, using the qualitative approach. We conducted in-depth interviews and thematic analysis following an inductive coding process.
Results: Three major themes emerged: 1) stigma of HIV and stigma of COPD exist, 2) HIV stigma outweighs COPD stigma, and 3) the centrality of ignorance in HIV and COPD stigmas. When participants were questioned separately about HIV and COPD stigmas, they expressed stigma towards HIV due to misconceptions about the disease and towards COPD due to a smoking history, symptoms, and conspicuous treatment equipment. However, when participants were asked about both stigmas comprehensively, they described a more substantial stigma of HIV, causing it to eclipse that of COPD. In sharing their lived experiences, participants identified a lack of knowledge as the main factor contributing to stigmas related to both diseases.
Discussion: Understanding the stigma of older PLWH with COPD may improve how we help patients navigate disease-related stigma. Future research, interventions, and healthcare policies should focus on the pivotal role of education in reducing stigmas related to HIV and COPD.
Keywords: stigma, HIV, COPD, intersectionality, education
Introduction
Antiretroviral treatment has contributed to the increased life expectancy of people living with HIV (PLWH), yet this improvement has been accompanied by challenges. Even with this treatment, older PLWH experience accelerated lung function decline as well as earlier and more severe development of respiratory diseases than those without HIV.1 This often culminates in chronic obstructive pulmonary disease (COPD), the third leading cause of death worldwide.1 COPD is a chronic respiratory disease with progressive and largely irreversible airflow limitation, along with dyspnea, cough, and sputum.1,2 Risk factors of COPD are exposure to harmful particles (eg, smoking) and respiratory diseases (eg, asthma).2 Because of a high rate of cigarette smoking, lung abnormalities, and HIV infection in PLWH, COPD is the most common non-infectious lung disease experienced by them, with a prevalence of 10–23%.1,3,4 Despite this high prevalence, the existing literature reveals a significant gap in understanding their health outcomes. Previous studies mainly focused on the pathology of COPD in HIV,1,4,5 screening protocols for COPD in PLWH,6,7 and quality of life for those affected by both conditions,8 consistently highlighting the detrimental impact of concurrent HIV and COPD. Therefore, identifying factors that affect the health of older PLWH with COPD is an emerging topic for research and interventions, with one of those being stigma.
Stigmas stemming from sociodemographic characteristics such as age, race, gender identity, and/or sexual orientation significantly influence the health outcomes of older adults.9 In addition to these stigmas, older PLWH with COPD may encounter additional disease-related stigmas, which are the primary focus of this study. In this study, stigma refers to one’s experience of discrimination due to health problems,10 a phenomenon that affects people with HIV and/or COPD.11,12 As seen in Figure 1, PLWH experience stigma due to their HIV serostatus, age, substance use, gender identity, and sexual identity.13 People with COPD experience stigma because of the conspicuous use of an inhaler or oxygen equipment in a public place, excessive coughing or shortness of breath, and smoking history.14 Although the causes of the stigmas of the two diseases are different, both stigmas have negative effects on health outcomes such as poor self-management, feelings of isolation, and poor quality of life.11,12,15,16 Intersectionality is an acknowledgment that an individual’s health is shaped by overlapping multiple factors,17 which may lead to positive or negative synergetic effects. Given the negative association between stigma and health outcomes in both diseases, the intersectionality of stigma related to HIV and COPD may further worsen health outcomes. Despite the potential negative impact of the intersectionality of disease-related stigmas on health outcomes, the intersectional stigma of PLWH with COPD remains yet to be explored.
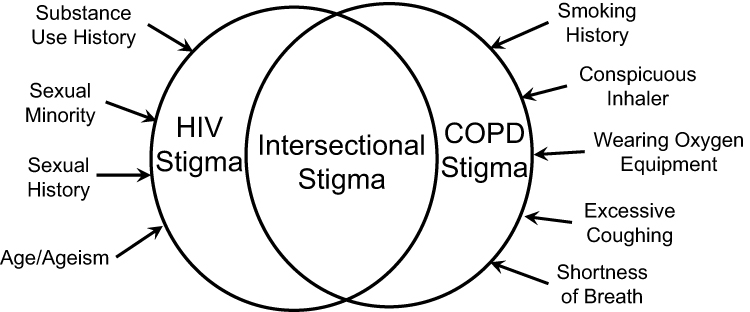 |
Figure 1 Conceptual overlap of HIV and COPD stigmas. Abbreviation: COPD, chronic obstructive pulmonary disease. |
Given the limited research on intersectional stigmas of HIV and COPD, it is crucial to initiate a preliminary exploration by understanding individuals’ experiences before proceeding to large-scale studies. Therefore, this qualitative study of three cases aimed to explore experiences related to intersectional stigma present in older PLWH with COPD in Alabama, located in the Deep South, an area with a higher prevalence of HIV and COPD than the US average.18,19
Methods
Participants
Participants were recruited via advertisement presented at an academic HIV clinic in Birmingham, Alabama. Three participants contacted the researcher via telephone, and the researcher confirmed their eligibility. Inclusion criteria included: a) ≥50 years of age, b) ≥ one year post HIV diagnosis, c) ≥ one year post COPD diagnosis, and d) able to read and understand written and spoken English. Exclusion criteria included: a) having communicable diseases (eg, hepatitis C) or terminal diseases (eg, breast cancer), b) having mental diseases (eg, schizophrenia), and c) being homeless. The inclusion/exclusion criteria were selected in order to have participants that would allow them to talk about their experiences regarding the stigma of HIV and COPD without severe overlapping comorbidities or life circumstances obfuscating the dialogue.
Instruments
Demographic Questionnaire
This self-reported pencil and paper questionnaire assessed age, race, gender, sexual orientation, occupation, education, household income, and marital status.
Clinical Questionnaire
This self-reported pencil and paper questionnaire assessed years diagnosed with HIV, years diagnosed with COPD, comorbidities, self-rated perception of health (1=excellent, 5=poor), smoking, alcohol consumption, and medications.
Semi-Structured Interview Guide
The interview guide included three main domains: HIV-related stigma, COPD-related stigma, and intersectional stigma of HIV and COPD (see Table 1). Under each domain, main questions and probes guided in-depth conversations related to the stigma of living with HIV and COPD. The questions were structured to include the contents of the internalized stigma (ie, having negative stereotypes about the disease and applying them to themselves), enacted stigma (ie, experiencing discrimination or stereotyping from others), and anticipated stigma (ie, expecting discrimination or stereotyping from others in the future) as presented by Earnshaw et a.20
Procedure
When scheduling the interview, all three participants preferred in-person interviews held in a meeting room located in a university building. Before participating in the study, all participants provided their informed consent, and they agreed to the publication of anonymized responses and case details. Participants completed demographic and clinical questionnaires. The first author conducted semi-structured interviews with each participant. Each interview lasted about one hour, and all interviews were audio-recorded and transcribed. During the interview, the researcher observed the participant’s non-verbal behavior and the overall atmosphere of the interview and recorded them in field notes. The University of Alabama at Birmingham’s Institutional Review Board (IRB) confirmed that the study did not meet the criteria for human subject research. The study was conducted in accordance with the Declaration of Helsinki.21
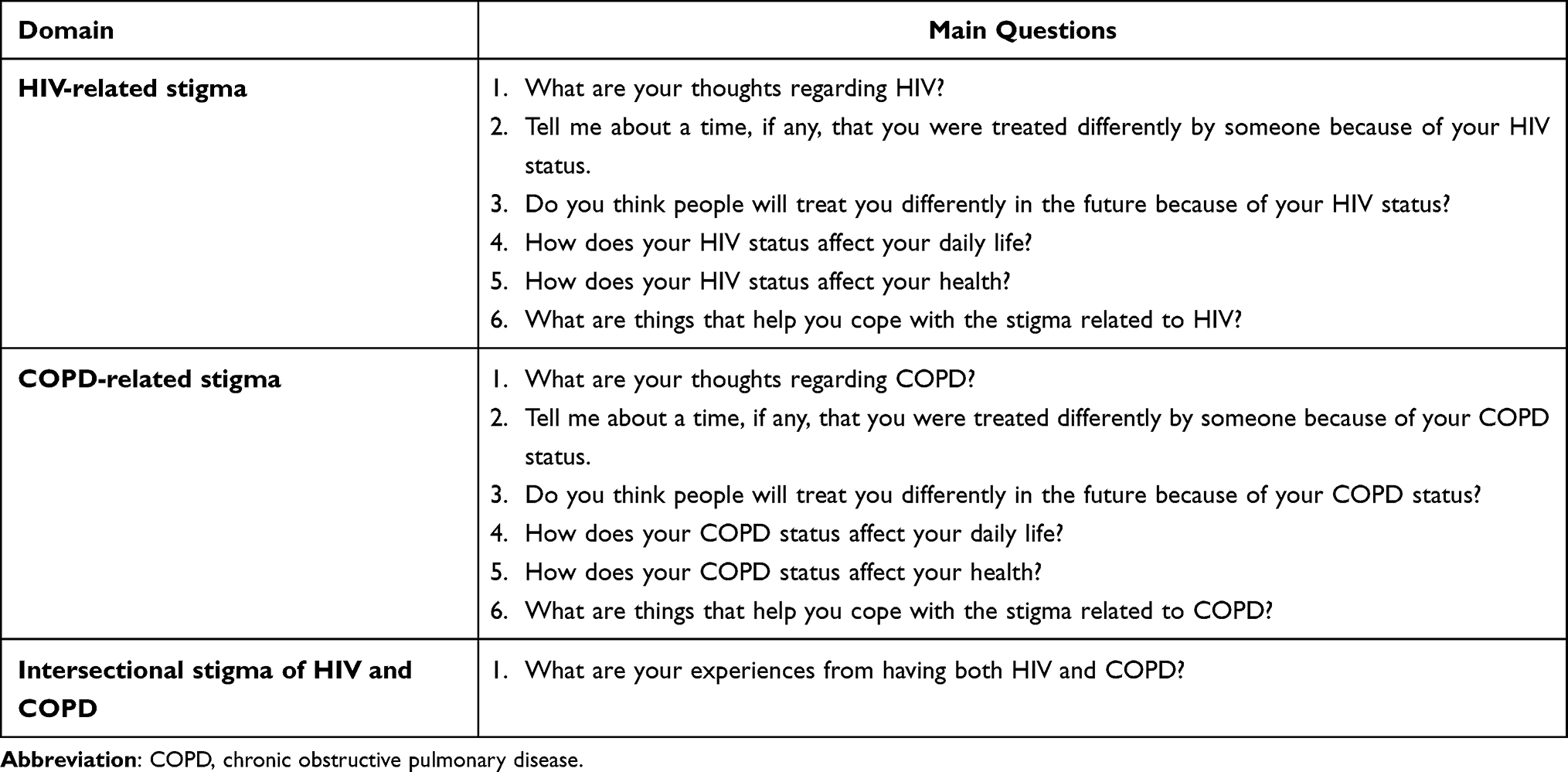 |
Table 1 Interview Questions |
Data Analysis
The data analysis followed the inductive coding process by Tomas:22 1) read the raw text several times until the researcher gets familiar with and understands the contents of the interviews, 2) identify and create categories derived from verbatim or meanings in the text segments, 3) reduce overlap and redundancy of categories, and 4) revision and refinement of categories, selecting quotations that convey the essence of the category or core theme. The field notes were included in the process to offer a comprehensive understanding. The analysis was manually conducted using Excel, and we maintained a detailed record of the data analysis to ensure transparency and scrutiny of the research process. Regular team meetings were held to discuss the preliminary analysis results to reach an agreement.
Results
Characteristics of Participants
As seen in Table 2, participants were African Americans, two females and a male, who were 55 to 65 years old. All were heterosexual and single. They had similar household incomes but had different levels of education, ranging from middle school to college. Only participant A was employed. All participants were diagnosed with HIV prior to COPD. The length of time diagnosed with HIV varied from 9 to 30 years and COPD from 2 to 8 years. Participants perceived their health at a level of good or above. Participants A and C smoked 3–7 cigarettes per day and were currently not under oxygen therapy. Participant B quit smoking, and she used 3 to 4 L/min of oxygen during the interview.
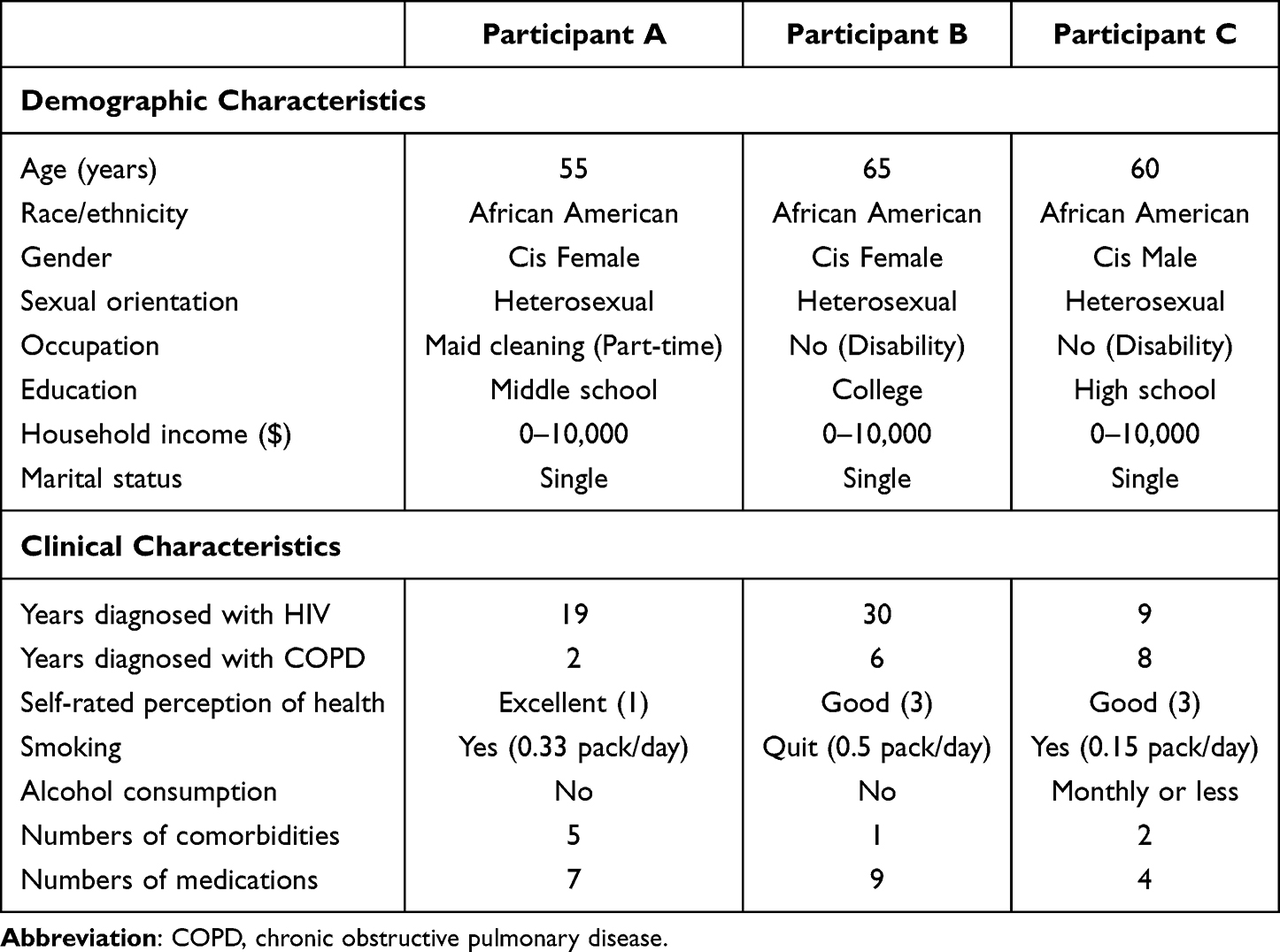 |
Table 2 Participants Characteristics |
Intersectional Stigma of Living with HIV and COPD
Three major themes emerged describing the intersectional stigma experienced by older PLWH with COPD: 1) stigma of HIV and stigma of COPD exist, 2) HIV stigma outweighs COPD stigma, and 3) the centrality of ignorance in HIV and COPD stigmas (Figure 2).
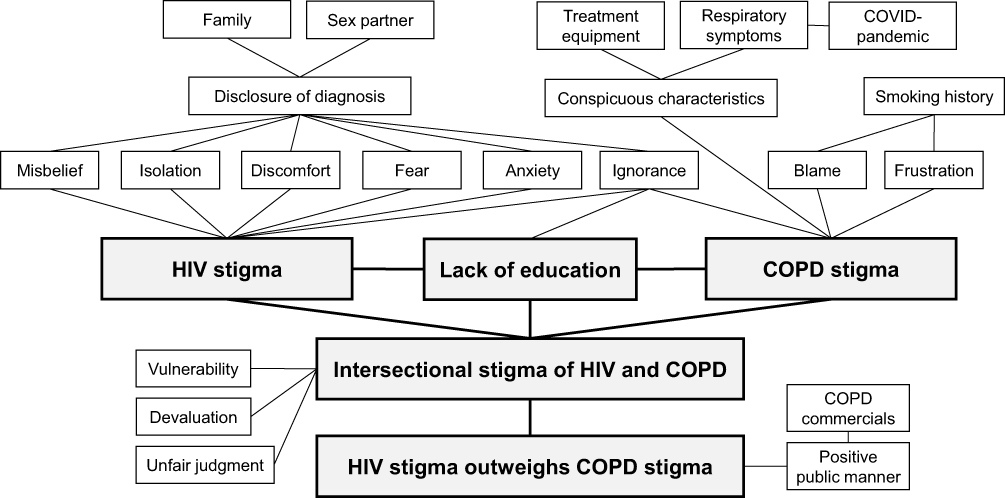 |
Figure 2 Map of HIV and COPD stigmas and related factors: Findings from the study. Abbreviation: COPD, chronic obstructive pulmonary disease. |
Stigma of HIV and Stigma of COPD Exist
Stigma of HIV
Participants were mixed in their HIV disclosure due to anticipated stigma. Participants A and B shared their status with family, but participant A had a hard time establishing an open relationship with her stepfather due to the stigma which is caused by misconceptions about HIV. She said,
They would fetch my plate and bring it to me in another part of the house or something. Or they would fetch the plate and they would put it in a paper plate or a plastic cup.
Occasionally, she signed with downcast eyes, suggesting a sense of isolation and discomfort throughout the conversation. On the other hand, participant C did not disclose his HIV status to his family because “there’s nothing good about HIV”.
Participants A and B, both females, had concerns about getting threatened by previous sex partners if they disclosed their health conditions. These concerns suggest the presence of fear and anxiety surrounding the disclosure of their HIV diagnoses. Participant A expressed concerns, “If I do tell them too late, then they gonna leave, or they’re gonna wanna do something to me”. Participant B explained it could be dangerous to disclose HIV status by bringing up a disclosure story shown on television:
He found out that she had AIDS, but she really don’t have AIDS…When she turned her back, he shot her in the back of the head. This was on T.V. He killed her. Then, when they put him to trial, went to trial, found out the girl wasn’t even HIV positive. (Participant B)
Stigma of COPD
The stigma of COPD was related to conspicuous treatment equipment (eg, oxygen tank) and symptoms as well as smoking history. Participant A did not want to use the inhaler in front of people because of stigma. She mentioned:
I just don’t wanna use that tank and stuff…‘Cause they happen to ask, “Did you bring your pump? Did you bring your pump?” Like oh God, why you lettin’ everybody know I’m on a pump. A lotta times you can’t let everybody know how ill you are because they’ll get you upset. (Participant A)
Participant C anticipated stigma caused by conspicuous characteristics of COPD (eg, oxygen tank, severe respiratory symptoms) even though he did not have those characteristics for his current health status. He mentioned:
Because people will look at you as if, like when you have oxygen tank, that you are terminally ill, very, very sick…So some COPD sufferers, they may tend to cough a lot, and people, it creates a stigma where people do not want to be around you. (Participant C)
Participants B and C mentioned difficulties living in the COVID-19 pandemic. For participant B, who needs oxygen therapy in daily life, she had to explain her health condition to others whenever she could not cover her nose with a mask because of shortness of breath. This also occurred a few times during the interview, highlighting the challenges that people with respiratory conditions face during the pandemic. She also experienced another person (eg, a nail shop staff) avoiding being around her, “She picked up her chair and moved away from me”. Participant B appeared visibly frustrated, her mouth downturned, as she shared this experience. Participant C also mentioned people mistake symptoms of COPD for those of COVID-19:
People who do not know you or know me may hear me occasionally cough. They may take it as, “Oh, he may have COVID”. There’s that, so it creates a stigma… they may take it as if you are, have some sort of contagious disease, but COPD is not contagious. (Participant C)
Participants’ family and friends focused on their smoking habits. Participant A’s father brought up a family history of smoking and respiratory disease and said, “I told you to leave them cigarettes alone”. Participant B’s family implicated her for getting COPD because of smoking and drugs, even though her family members also did drugs and smoked. She said, “Everybody wanna take the focus off of them and put it on me”. When sharing their experiences, both participants A and B expressed feelings of blame, frustration, and being unfairly singled out.
Intersectional Stigma
The intersectional stigmas associated with HIV and COPD existed among participants. Participant A said people viewed her as if she “messed up” for having both conditions. Participant C mentioned that PLWH with COPD are reluctant to talk about their health conditions because of anticipated stigma:
Some people do not want anyone to know that I have COPD, I have HIV, because again, there is the stigma of they do not want anybody to know, and when people find out, they may shy away from you…They say something negative like, “Oh, they’re dirty. They’re nasty. They’re unclean”, and that’s not necessarily true. Yes, so a lot of people are reluctant to talk about it. (Participant C)
The use of negative expressions such as “dirty”, “nasty”, and “unclean” indicated that PLWH may feel vulnerable, unfairly judged, and devalued.
HIV Stigma Outweighs COPD Stigma
When comparing HIV and COPD stigmas, participants’ overall reaction was that stigma of HIV eclipses that of COPD. Participant A said, “I’m fine with it (COPD). I wish I could get fine with the HIV”. Participant B said she is fine with COPD because “there’s nothin’ I can do”. Participant C illustrated the stigma of both diseases during the interview, but he emphasized a stronger stigma of HIV than COPD, “Those are two different. They are both diseases, but having HIV is in a way totally different from having COPD because they really—it really has a stigma”. He also mentioned that COPD commercial “is talking about (COPD) in a more positive public manner than HIV”. More specifically, he mentioned:
They don’t talk about HIV as much or in a more glorifying way than they do COPD or cancer. They may talk about it as if it’s not so bad, but COPD, they’re not saying that it’s bad, but they don’t discuss it as much. So people are less likely to know about it, to understand or to accept it. (Participant C)
The Centrality of Ignorance in HIV and COPD Stigmas
As the participants shared their experiences with HIV and COPD stigmas, a common thread emerged: the pivotal role of education. All participants mentioned the cause of stigma is “being uneducated” (ie, widespread ignorance about both diseases contributes to stigmas). The intensity of misbeliefs about HIV, exacerbated by a lack of education, results in HIV stigma being more severe than that of COPD. Participant A “had started bringing the literature home and let him (stepfather) start reading it” to reduce experienced HIV stigma. On the other hand, she explained why she does not disclose her HIV status to people other than family, “I don’t have the time. I don’t have the patience” to “teach them and make them understand and be mindful what it means”. Participant B employed open and expressive facial features, including raised eyebrows and widened eyes, coupled with animated gestures. This vivid presentation aimed to illustrate how easily HIV can be transmitted, comparing it to handing over a baseball. Through this, she underscored the importance of education in reducing HIV-related stigma and expressed a desire for better understanding.
Similar to HIV stigma, COPD stigma was thought to be caused by ignorance. Participant C wanted to tell others “what we people are going through” and information about COPD. He emphasized COPD is not only caused by smoking, but “it could have been from your occupation”. Furthermore, he mentioned the stigmas of HIV and COPD that happened at work:
Years ago, due to being uneducated, they would not hire me if they knew I had HIV, although it does not stop my performance. It does not define whether I have the ability, the know-how, or any of that. But with COPD, even now, they would not hire me with COPD versus in back then, they would have hired me with COPD. So a lot has to do with society. (Participant C)
In summary, the exploration of intersectional stigma among older PLWH with COPD revealed three major themes. This insight laid the groundwork for our discussion on the complex intersectionality of stigmas surrounding HIV and COPD and suggested broader implications of these findings for research and interventions needed to address the stigmas.
Discussion
Through in-depth qualitative interviews with three older PLWH with comorbid COPD, three themes concerning intersectional stigma emerged. The first theme, “stigma of HIV and stigma of COPD exist”, showed that stigmas of HIV and COPD exist when approached separately. However, as described in the second theme, the “HIV stigma outweighs COPD stigma” when stigmas of both diseases are approached together. As participants illustrated their experiences, the third theme highlighted how lack of knowledge, misconceptions, and prejudice contribute to the stigmas surrounding HIV and COPD.
We assumed the intersectionality of stigmas might lead to a negative synergetic effect. Yet, when participants were asked about the intersectionality of stigmas, they did not mention the synergetic effect of having HIV and COPD. This finding is different from previous studies regarding other types of intersectional stigma (eg, the intersectional stigma of sexual orientation and HIV), which showed potential synergistic effects.23 Reasons for this difference are posited. First, the intersectional stigma arising from disease-related stigmas may manifest a different dynamic when compared with the intersectional stigma derived from sociodemographic factors (eg, age, race, gender identity, sexual orientation).9 Second, the stigma of HIV could be much stronger than the stigma of COPD. As participant C mentioned, COPD-related commercials have a “more positive public manner” compared to HIV-related commercials. Also, some media (eg, news reports) frame PLWH as “sexual risk-takers”, which can cause a significant stigma.24 Third, PLWH who adhere to treatment of HIV may be more resilient.25 The resilience of PLWH might make them more capable of managing the next challenge, such as a diagnosis of COPD, a concept known as crisis competence.26
Study strengths and limitations are noted. The greatest strength of this study is that it is the first to extensively discuss intersectional stigma caused by both HIV and COPD. Second, it utilized a basic descriptive analysis for the phenomenon being studied. Third, the study was conducted in Alabama, in the Deep South, where the prevalence of HIV and COPD is higher than in other parts of the US Likewise, there are limitations to this study. First, it is difficult to generalize the results of the study because it was conducted with only three participants. This limitation may restrict the representativeness of our findings for diverse demographic groups or other contexts, such as those with severe respiratory symptoms. PLWH with severe COPD may have different experiences due to more frequent and conspicuous symptoms, leading to severe COPD stigma than participants of the current study. Also, the results may not fully capture the complexity of intersectional stigma in its entirety because we excluded those with communicable, terminal, or mental diseases to avoid the impact of disease-related stigma that may be prevalent in older PLWH. Second, considering the sensitivity of the topic, “stigma”, those who participated and provided information in the study may have potential biases.
Implications
The study suggests that HIV stigma is perceived to outweigh COPD stigma, and the intersectionality of these stigmas may not result in a synergistic effect. This raises questions about the unique dynamics of stigma in different health conditions and the factors influencing their intersectionality. Future research exploring the reasons behind the perceived differences in stigma strength between HIV and COPD is recommended. To achieve this, a qualitative study incorporating diverse perspectives from various groups of people (eg, patients, family caregivers, healthcare providers) or a quantitative study using validated measurements to assess HIV stigma, COPD stigma, and resilience could be conducted. The current study acknowledges its limitations, particularly the small sample; therefore, future research with larger and more diverse samples is needed to enhance the generalizability of findings. Including participants with severe respiratory symptoms or other comorbidities (eg, communicable, terminal, or mental diseases) would provide a more comprehensive understanding of intersectional stigma in a broader population and inform interventions and healthcare policies for older PLWH with COPD.
To address the challenges faced by older PLWH with COPD, it is essential to develop tailored interventions and healthcare policies that recognize the differential attributes related to HIV stigma and COPD stigma. For example, providing safe and comfortable ways to disclose diagnoses of HIV to family and sex partners or offering strategies to appropriately manage respiratory symptoms could be beneficial. We suggested that the resilience exhibited by PLWH who adhere to treatment, or crisis competence, could potentially positively influence coping with COPD stigma. This resilience could be explored and leveraged by healthcare providers to manage comorbid conditions.
Healthcare policies play a crucial role in addressing public perceptions that contribute to disease-related stigmas. Public health campaigns and educational initiatives are instrumental in reducing stigmas associated with HIV and COPD. This process may involve developing guidelines and interventions that recognize the coexistence of different stigmas and tailoring support accordingly.
Conclusion
This study explored the intersectional stigma experienced by older PLWH with COPD using a qualitative approach. The findings revealed that HIV stigma overshadows COPD stigma, and lack of knowledge, misconceptions, and prejudice significantly contribute to these stigmas. To mitigate stigmas of HIV and COPD and enhance overall well-being, future research, clinical care, and healthcare policy should reflect a comprehensive understanding of older PLWH with COPD.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
Dr Anand Iyer reports grants from NIH, personal fees from AstraZeneca, personal fees from Ascension, during the conduct of the study. Dr David Batey reports grants from National Institute of Mental Health (NIMH), National Institute of Nursing Research, National Institute of Allergy and Infectious Diseases, National Institute on Alcohol Abuse and Alcoholism and Centers for Disease Control and Prevention, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Bigna JJ, Kenne AM, Asangbeh SL, Sibetcheu AT. Prevalence of chronic obstructive pulmonary disease in the global population with HIV: a systematic review and meta-analysis. Lancet Glob Health. 2018;6(2):e193–e202. doi:10.1016/s2214-109x(17)30451-5
2. Global Initiative for Chronic Obstructive Lung Disease. 2021 Global strategy for prevention, diagnosis and management of COPD; 2021. Available from: https://goldcopd.org/wp-content/uploads/2020/11/GOLD-REPORT-2021-v1.1-25Nov20_WMV.pdf.
3. Lambert AA, Kirk GD, Astemborski J, Mehta SH, Wise RA, Drummond MB. HIV infection is associated with increased risk for acute exacerbation of COPD. J Acquir Immune Defic Syndr. 2015;69(1):68–74. doi:10.1097/qai.0000000000000552
4. Byanova K, Kunisaki KM, Vasquez J, Huang L. Chronic obstructive pulmonary disease in HIV. Expert Rev Respir Med. 2021;15(1):71–87. doi:10.1080/17476348.2021.1848556
5. Cribbs SK, Crothers K, Morris A. Pathogenesis of HIV-related lung disease: immunity, infection, and inflammation. Physiol Rev. 2020;100(2):603–632. doi:10.1152/physrev.00039.2018
6. Ghadaki B, Kronfli N, Vanniyasingam T, Haider S. Chronic obstructive pulmonary disease and HIV: are we appropriately screening? AIDS Care. 2016;28(10):1338–1343. doi:10.1080/09540121.2016.1189499
7. Quiros-Roldan E, Pezzoli MC, Berlendis M, et al. A COPD case-finding program in a large cohort of HIV-infected persons. Respir Care. 2019;64(2):169–175. doi:10.4187/respcare.06247
8. Drummond MB, Kirk GD, McCormack MC, et al. HIV and COPD: impact of risk behaviors and diseases on quality of life. Qual Life Res. 2010;19(9):1295–1302. doi:10.1007/s11136-010-9701-x
9. Turan JM, Elafros MA, Logie CH, et al. Challenges and opportunities in examining and addressing intersectional stigma and health. BMC Med. 2019;17(1):7. doi:10.1186/s12916-018-1246-9
10. Weiss MG, Ramakrishna J, Somma D. Health-related stigma: rethinking concepts and interventions. Psychol Health Med. 2006;11(3):277–287. doi:10.1080/13548500600595053
11. Chin ED, Armstrong D. Anticipated stigma and healthcare utilization in COPD and neurological disorders. Appl Nurs Res. 2019;45:63–68. doi:10.1016/j.apnr.2018.12.002
12. Engelhard EAN, Smit C, van Dijk PR, et al. Health-related quality of life of people with HIV: an assessment of patient related factors and comparison with other chronic diseases. AIDS. 2018;32(1):103–112. doi:10.1097/qad.0000000000001672
13. Slater LZ, Moneyham L, Vance DE, Raper JL, Mugavero MJ, Childs G. The multiple stigma experience and quality of life in older gay men with HIV. J Assoc Nurses AIDS Care. 2015;26(1):24–35. doi:10.1016/j.jana.2014.06.007
14. Woo S, Zhou W, Larson JL. Stigma experiences in people with chronic obstructive pulmonary disease: an integrative review. Int J Chron Obstruct Pulmon Dis. 2021;16:1647–1659. doi:10.2147/copd.S306874
15. Kteily-Hawa R, Andany N, Wang Y, et al. Quality of life of older women living with HIV: comparative assessment of physical and mental health-related markers using a large Canadian sexual and reproductive health cohort study. HIV Res Clin Pract. 2019;20(2):35–47. doi:10.1080/15284336.2018.1554373
16. Rose S, Paul C, Boyes A, Kelly B, Roach D. Stigma-related experiences in non-communicable respiratory diseases: a systematic review. Chron Respir Dis. 2017;14(3):199–216. doi:10.1177/1479972316680847
17. Bauer GR. Incorporating intersectionality theory into population health research methodology: challenges and the potential to advance health equity. Soc Sci Med. 2014;110:10–17. doi:10.1016/j.socscimed.2014.03.022
18. AIDSVu. Local data: United States. 2023. Available from: https://aidsvu.org/local-data/united-states/.
19. Sullivan J, Pravosud V, Mannino DM, Siegel K, Choate R, Sullivan T. National and state estimates of COPD morbidity and mortality - United States, 2014–2015. Chronic Obstr Pulm Dis. 2018;5(4):324–333. doi:10.15326/jcopdf.5.4.2018.0157
20. Earnshaw VA, Smith LR, Chaudoir SR, Amico KR, Copenhaver MM. HIV stigma mechanisms and well-being among PLWH: a test of the HIV stigma framework. AIDS Behav. 2013;17(5):1785–1795. doi:10.1007/s10461-013-0437-9
21. World Medical Association. World medical association declaration of Helsinki: ethical principles for medical research involving human subjects. JAMA. 2013;310(20):2191–2194. doi:10.1001/jama.2013.281053
22. Thomas DR. A general inductive approach for analyzing qualitative evaluation data. Am J Eval. 2006;27(2):237–246. doi:10.1177/1098214005283748
23. Slater LZ, Moneyham L, Vance DE, Raper JL, Mugavero MJ, Childs G. Support, stigma, health, coping, and quality of life in older gay men with HIV. J Assoc Nurs AIDS Care. 2013;24(1):38–49. doi:10.1016/j.jana.2012.02.006
24. Vaughan E, Power M. The discursive construction of HIV stigma in Irish print media. Health. 2023;27(3):398–416. doi:10.1177/13634593211038525
25. Wen J, Yeh TP, Xie H, Yu X, Tang J, Chen Y. Resilience, self-esteem, self-efficacy, social support, depression and ART adherence among people living with HIV in Sichuan, China. AIDS Care. 2021;33(11):1414–1421. doi:10.1080/09540121.2020.1828800
26. Vance DE, Struzick TC, Masten J. Hardiness, successful aging, and HIV: implications for social work. J Gerontol Soc Work. 2008;51(3–4):260–283. doi:10.1080/01634370802039544
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.