")
Back to Journals » Clinical Pharmacology: Advances and Applications » Volume 15
Ipratropium Bromide/Salbutamol-Induced Acute Urinary Retention as a Result of Medication Error: A Case Report and Review of Cases in the Literature
Authors Kubas MA , Al-Ashwal FY , Babattah OK, Alsaqqaf AA
Received 30 July 2023
Accepted for publication 16 November 2023
Published 21 November 2023 Volume 2023:15 Pages 107—111
DOI https://doi.org/10.2147/CPAA.S433117
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Arthur E. Frankel
Mohammed Abdullah Kubas,1,2 Fahmi Y Al-Ashwal,1,3 Orwa Khaled Babattah,4 Akram Ameen Alsaqqaf4
1Department of Clinical Pharmacy and Pharmacy Practice, University of Science and Technology, Sana’a, Yemen; 2Clinical Pharmacy Department, University of Science and Technology Hospital (USTH), Sana’a, Yemen; 3Department of Clinical Pharmacy, College of Pharmacy, Al-Ayen University, Thi-Qar, Iraq; 4Urology Department, University of Science and Technology Hospital (USTH), Sana’a, Yemen
Correspondence: Fahmi Y Al-Ashwal, Department of Clinical Pharmacy and Pharmacy Practice, Faculty of Pharmacy, University of Science and Technology, Sana’a, Yemen, Tel +60146177642, Email [email protected]
Abstract: Medication errors have the potential to cause serious toxicity and hospitalization. This case report describes a 25-year woman who suffered serious side effects and was hospitalized after receiving intravenous ipratropium bromide/salbutamol. This was due to a medication error in its preparation and administration. The caregiver diluted an intravenous antibiotic with the incorrect diluent (nebulizer solution), which led to serious toxicity, including acute urine retention and sinus tachycardia, and then resulted in patient hospitalization. A literature review of case reports was conducted to compare and identify the pattern of ipratropium/salbutamol-induced acute urinary retention. The present report underscores the importance of clinical awareness about medication-induced acute urine retention. Furthermore, it is crucial that physicians inform and educate the patients and their carers about double-checking doses and labelling before administering medication, particularly for intravenous drugs.
Keywords: medication error, ipratropium bromide toxicity, acute urinary retention, parenteral administration
Introduction
Medication errors have the potential to cause harm and result in hospitalization. These errors can occur at different stages of the treatment process, starting from when a physician prescribes the medication to its administration.1 Using the wrong diluent to dilute medications during the preparation process, especially in cases involving IV antibiotics, is a specific area where medication errors may occur. This can lead to a variety of complications, such as a decrease in the stability and effectiveness of the medication, possible drug precipitation, and a heightened risk of harm to the patient.2 One severe consequence of such errors is medication-induced acute urinary retention (AUR).3 AUR can be a potentially serious issue, as it can lead to urinary tract infections and kidney damage.4 Medications, like anticholinergics, sympathomimetics (alpha and beta-adrenergic agents) and tricyclic antidepressants are examples of medications that have been associated with urinary retention.3,4
One specific medication called ipratropium bromide falls under the category of short-acting anticholinergics. It is commonly used to manage bronchospasm symptoms associated with pulmonary COPD and asthma. While this medication is generally safe, one rare side effect is acute urinary retention,5 which occurs because ipratropium hinders the activation of detrusor muscarinic receptors and, in turn, inhibits contraction, leading to urinary retention.3 The prevalence of ipratropium-induced AUR varies depending on patient characteristics (men with benign prostatic hyperplasia vs men with no comorbidity) and the route of administration (nebulizers vs dry powder inhalers).6
Very few case studies of ipratropium-induced AUR have been found, and all were taking a nebulized dose.7,8 However, there are no reports in the literature of AUR as a side effect of accidentally receiving an intravenous dose of ipratropium bromide. In this case report, we describe a 25-year-old woman who experienced ipratropium bromide/salbutamol toxicity due to an error in preparation and administration by using an incorrect diluent (nebulizer solution) for diluting an IV antibiotic. To the best of our knowledge, this is the first time that acute urinary retention has been reported as a negative side effect of accidentally receiving an intravenous dose of ipratropium bromide.
Case Report
A 25-year-old female patient presented to the emergency department (ER) with fever and sinus tachycardia. One week before admission, the patient was complaining of a chest infection and was treated at home with ceftriaxone (1 g IV twice daily). On the day of presentation to the ER, her mother diluted the vial of ceftriaxone with a Combivent unit-dose vial instead of distal water. The active ingredients are ipratropium bromide (0.5 mg) and salbutamol sulfate (3.01 mg). To illustrate, administering IV medications at home is a common practice in Yemen, but it is usually done under the supervision of healthcare providers (eg, nurses, physicians, or pharmacists). When one family member is working or studying at medical faculties, they usually take the initiative and advise the patient on how to administrate the medicine, like in our case, the patient’s sister who is studying at medical school. The physician prescribed the antibiotic. Because the patient’s sister is studying medicine, she was familiar with the instructions for use. She then explained to the mom how to administer the antibiotic. However, the mom did not realize she had dissolved the antibiotic with a Combivent unit-dose vial instead of a distilled water vial.
On the day of presentation to the ER, the patient manifested signs of toxicity due to ipratropium bromide/salbutamol sulfate, characterized by tremors and dryness in the eyes and mouth. However, the most critical symptoms observed were sinus tachycardia and urinary retention. Then, she was admitted to the ICU for monitoring and was discharged the next day. The patient in the ICU was without a Foley catheter, and the specialist neglected her complaint of urinary retention. On the same day of discharge, the patient came back to the ER with complete retention of urine. Ultrasound of the abdomen revealed a distended bladder, pre-voiding urine: 720, and post-voiding residual urine: 702. A Foley catheter was inserted, and the patient was admitted. The catheter drained 1300 cc after insertion.
In the ward, the patient was conscious, oriented, had normal vital signs, and complained of fullness of the bladder with little urge to urinate and pain. The CBC was normal in the ward. However, the urine analysis was positive for protein, RBC (25–30), leukocytes (8–10), and Blood +, and the sodium level was 129 mmol/l. Catheter drained in first 8 hours 1500 cc. A nephrologist consultation was done, and the patient was put on 100 cc\hr D5NS, furosemide 20 mg twice daily, and ceftriaxone (1 g IV 1×2) for her chest infection. The next day, the patient was polyuric, so furosemide was stopped, and fluid was increased to 150 cc/hr. Trials of urination without Foley’s catheter failed. On the third day in the hospital, all lab results are within normal range, and the patient is still on Foley catheter with clump (opened every three hours). The clinical pharmacist was consulted and informed the physician that the side effects of ipratropium bromide are suspected to gradually disappear once it is discontinued; therefore, no intervention was recommended, and the clinical pharmacist suggested continued observation of the patient’s symptoms and monitoring of urine output. On the fourth day, the patient started to urinate without Foley’s catheter, and a control ultrasound was done and revealed 65 mL post-voiding residual urine (PVRU); the symptoms resolved, and the patient was discharged.
Discussion
In the present case, it is highly probable that the IV administration of ipratropium bromide/salbutamol caused the AUR. This is because no other medications known to cause AUR were used, and there were no signs of urinary tract infections or other conditions that could obstruct urine flow. Moreover, the urinary residual volume was found to be normal after the effects of the drug had worn off. More importantly, the discovery of the medication error by the doctor.
There are a few possible reasons for this medication error that resulted in the use of an incorrect diluent for an IV antibiotic. The first reason is that the Combivent solution unit-dose plastic container resembles that of sterile water available in Yemen pharmacies. Also, the labeling in both containers is printed in a very small font. Therefore, healthcare providers should counsel and educate the patients and their caregivers about the medications, particularly when similar containers with different substances are utilized by the same patient. These steps can help reduce the risk of such medication errors and ensure that patients receive the best possible care.
The prevalence of medication-induced acute urinary retention with ipratropium is not well established. However, a nested case–control study from the Netherlands involving 22,579 patients with COPD discovered that those who inhaled anticholinergic medications had a 40% increased risk for AUR in contrast to those who did not use such drugs. Moreover, this risk was even more pronounced among those who had recently begun this treatment.6 Also, the same study reported that the risk of AUR was linked to the route of administration rather than the dose, with the use of nebulizers being associated with the highest risk compared to metered dose inhalers and dry powder inhalers, and that the strongest association was observed in men with benign prostatic hyperplasia (BPH). Notably, the official labeling for Combivent (ipratropium bromide and albuterol sulfate) states that urinary retention was identified as an adverse effect in post-marketing surveillance and advises precaution in patients with bladder neck obstruction or BPH.9 Thus, healthcare providers should advise such patients and instruct them to seek medical attention if they experience any difficulties while urinating.
Literature Review of Case Reports
Table 1 summarizes the case reports found in the literature related to ipratropium bromide or salbutamol-induced urinary retention. As we can see, the cases involve either young children taking oral salbutamol or inhaled ipratropium bromide/salbutamol or elderly patients. The four cases of elderly male patients were aged 69 to 72 years old, and all were taking nebulized ipratropium bromide as a suspected agent for urinary retention. Interestingly, three cases had confirmed BPH, and one case revealed a moderately enlarged, non-tender, smooth prostate upon rectal examination. Moreover, all four cases were taking other suspected medications that could be associated with urinary retention, such as salbutamol, bromocriptine, diazepam, and calcium channel blockers.10 Furthermore, three of the four cases were initiated ipratropium bromide and the other suspected agent (salbutamol) simultaneously. Notably, urinary retention appeared within 4–10 days. Therefore, it is important for healthcare providers and caregivers to closely monitor patients at extremes of age, such as elderly individuals and preschool children, for the first two weeks of taking salbutamol and/or ipratropium bromide. By closely monitoring patients, healthcare providers and caregivers can identify voiding difficulties, any potential issues, or adverse reactions early on and take prompt and appropriate action. Also, high-quality studies that evaluate the association between ipratropium bromide and acute urinary retention after adjusting for all the confounders are needed. Also, there is a need for well-controlled studies to assess the difference in risk of urinary retention between those who were initiated anticholinergic alone (eg, ipratropium bromide alone) vs anticholinergic medication together with β adrenergic receptor agonists (eg, ipratropium bromide + salbutamol).
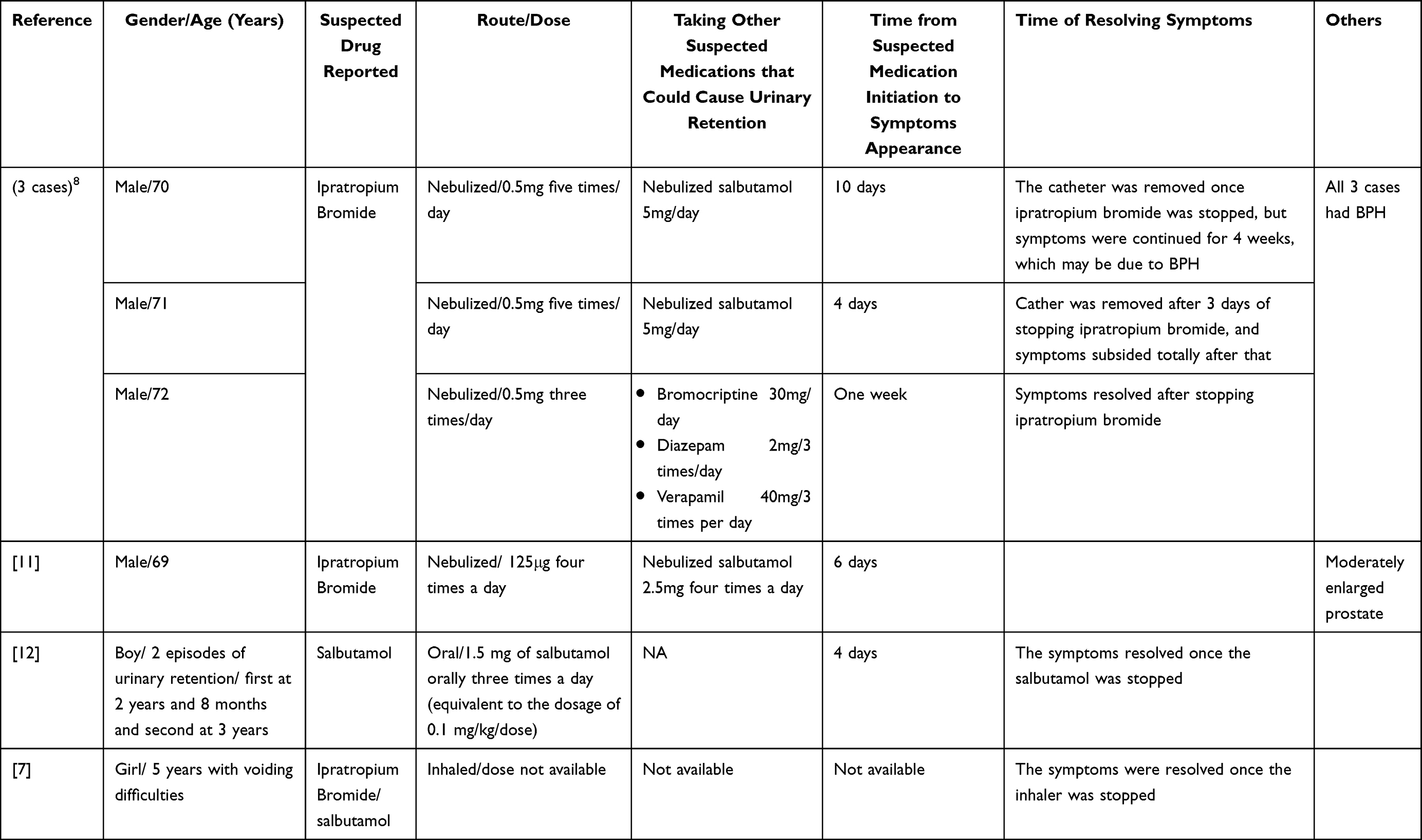 |
Table 1 Summary of Case Reports on Ipratropium/Salbutamol-Induced Urinary Retention |
Conclusions
A medication error resulted in serious toxicity and the hospitalization of the patient. We presented a case of IV ipratropium bromide/salbutamol-induced acute urinary retention and sinus tachycardia. This case underscores the importance of clinical vigilance regarding ipratropium-induced acute urinary retention. Moreover, it is essential that healthcare professionals educate and counsel the patients and their caregivers about double-checking doses and labeling before giving medication, particularly for parenteral route-administered medications.
Ethical Considerations
Written informed consent for publication of the patient’s deidentified case details was obtained from the patient before submission.
Disclosure
The authors have no conflicts of interest for this study.
References
1. Aronson JK. Medication errors: what they are, how they happen, and how to avoid them. QJM. 2009;102(8):513–521. doi:10.1093/qjmed/hcp052
2. Cousins D, Sabatier B, Begue D, Schmitt C, Hoppe-Tichy T. Medication errors in intravenous drug preparation and administration: a multicentre audit in the UK, Germany and France. BMJ Qual Saf. 2005;14(3):190–195. doi:10.1136/qshc.2003.006676
3. Verhamme KM, Sturkenboom MC, Stricker BHC, Bosch R. Drug-induced urinary retention: incidence, management and prevention. Drug Safety. 2008;31(5):373–388. doi:10.2165/00002018-200831050-00002
4. Selius BA, Subedi R. Urinary retention in adults: diagnosis and initial management. Am Fam Physician. 2008;77(5):643–650.
5. Loke YK, Singh S. Risk of acute urinary retention associated with inhaled anticholinergics in patients with chronic obstructive lung disease: systematic review. Therap Adv Drug Safety. 2013;4(1):19–26. doi:10.1177/2042098612472928
6. Afonso A, Verhamme K, Stricker B, Sturkenboom M, Brusselle G. Inhaled anticholinergic drugs and risk of acute urinary retention. BJU Int. 2010;107(8):1265–1272. doi:10.1111/j.1464-410X.2010.09600.x
7. Hooimeijer H, Van Der Deure J, de Langen J. Voiding difficulties in a child attributed to the use of ipratropium and salbutamol. Ned Tijdschr Geneeskd. 2007;151(49):2726–2728.
8. Lozewicz S. Bladder outflow obstruction induced by ipratropium bromide. Postgrad Med J. 1989;65(762):260–261. doi:10.1136/pgmj.65.762.260
9. Boehringer Ingelheim Pharmaceuticals. Combivent® (ipratropium bromide and albuterol sulfate). Prescribing information. [package insert]. The USA: Food and Drug Administration. Available from: https://www.accessdata.fda.gov/drugsatfda_docs/label/2012/020291s031lbl.pdf.
10. Serlin DC, Heidelbaugh JJ, Stoffel JT. Urinary retention in adults: evaluation and initial management. Am Fam Physician. 2018;98(8):496–503.
11. Pras E, Stienlauf S, Pinkhas J, Sidi Y. Urinary retention associated with ipratropium bromide. DICP. 1991;25(9):939–940. doi:10.1177/106002809102500907
12. D’Auria E, Mandelli M, Di Dio F, Riva E. Urine retention in a child treated with oral salbutamol. Indian J Pharmacol. 2012;44(4):519. doi:10.4103/0253-7613.99338
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.