")
Back to Journals » Clinical, Cosmetic and Investigational Dermatology » Volume 17
KIT Mutation Associated with Depigmented Patches Regression and Multiple Café-au-lait Macules Development in a Patient with Piebaldism: A Case Report
Authors Budair FM
Received 13 November 2023
Accepted for publication 3 March 2024
Published 20 March 2024 Volume 2024:17 Pages 713—716
DOI https://doi.org/10.2147/CCID.S449691
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Jeffrey Weinberg
Fatimah Mohammad Budair
Department of Dermatology, King Fahd University Hospital, Al Khobar, College of Medicine, Imam Abdulrahman bin Faisal University, Dammam, Saudi Arabia
Correspondence: Fatimah Mohammad Budair, Department of Dermatology, King Fahd University Hospital, Al Khobar, College of Medicine, Imam Abdulrahman bin Faisal University, Bashar Ibn Burd Street, Al Aqrabiyah 34445, Dammam, Saudi Arabia, Tel +00966503881480, Email [email protected]
Abstract: Piebaldism is a rare genetic disorder caused by KIT mutations and clinically characterized by fixed depigmented patches throughout the body. Herein, a case of piebaldism in which the depigmented patches regressed as the patient grew older, along with the development of multiple café-au-lait macules, is described. The likely pathogenic, heterozygous KIT c.1991-2A>G variant was detected as the potential cause of this unusual piebaldism phenotype. This case provides new knowledge on genotype-phenotype correlation of KIT mutations for piebaldism etiology and presentation.
Keywords: genotype, phenotype, melanocyte, autosomal, rare disease
Introduction
Piebaldism is a rare autosomal dominant disease of congenital depigmentation that is caused by KIT and, less commonly, SNAI2 mutations.1–3 In particular, KIT encodes a transmembrane tyrosine kinase receptor for stem cell factors that is important for melanocyte survival and function. Hence, KIT mutations (more than 90 different variants have been reported) result in abnormalities in melanocyte migration and/or melanogenesis pathway.4–6
Piebaldism-related genetic mutations affect the skin and hair, resulting in white patches that are distributed on the trunk, abdomen, and limbs in addition to a distinct triangular pattern depigmentation of the forehead and white forelock (WF) of hair.1 In addition, some patients may present café-au-lait macules (CALMs) and intertriginous freckling, two skin lesions that are typically formed in neurofibromatosis7 but that have recently been considered part of a rare phenotypic variant of piebaldism.8 The depigmentation pattern remains stable throughout the life of the patient, although pigmentation of the white forelock has been previously reported;9 in rare cases, acquired pigmentation of body patches has been described after injury.10
Herein, a case of pigmentation of previously depigmented patches distributed throughout the body along with the additional development of multiple CALMs in a 7-year-old is described along with the genetic analysis of the KIT gene that is associated with this rare finding.
Case Report
A Saudi baby girl, resultant of spontaneous vaginal delivery from a healthy mother and a non-relative healthy father who already had two healthy boys, was referred to our clinic at the age of 3 months. She presented with WF and depigmented patches localized on the upper limbs, trunk, back, and lower limbs (none on the hands and feet), measuring up to 7 cm in length (Figure 1A). No CALMs or axial freckling were present at this age, and the infant was healthy and otherwise normal. Upon physical examination, the patient was provisionally diagnosed with piebaldism.
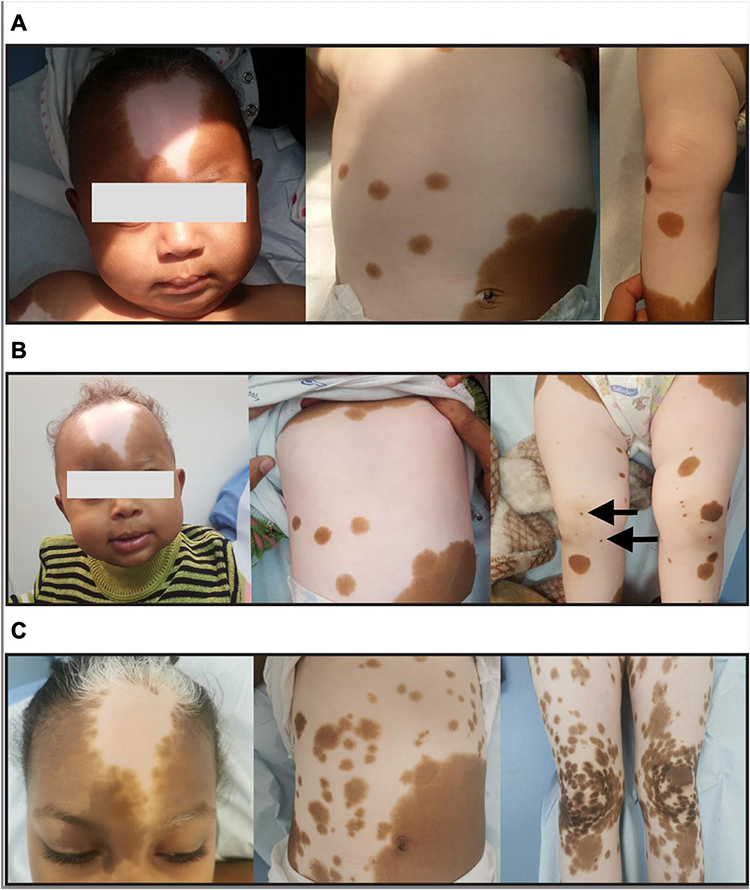 |
Figure 1 Regression of piebaldism-related depigmented body patches during the growth period of the patient. (A) At 3 months old, the patient presented with a distinct triangularly shaped depigmentation pattern of forehead and white forelock (WF) of hair (left), large depigmented patches in the abdomen with some patches and macules with normal pigmentation (middle), and a large depigmented patch on the right lower limb with some normal pigmented macules and patches (right). (B) At 8 months of age, the WF manifestation remained unchanged, indicating pigmentation absence (left); the abdominal skin features also remained unchanged, indicative of pigmentation absence (middle); however, the lower limbs started to show signs of pigmentation with the development of new hyperpigmented macules (black arrows, right). (C) At the age of 7 years, the skin of the WF showed signs of pigmentation (especially at the periphery of the lesion) but the hair remained white in color; furthermore, additional café-au-lait macules appeared as hyperpigmented patches (left), the abdominal skin area showed massive pigmentation in the depigmented patch (middle), and pigmentation on both lower limbs was noticeable (right). |
The patient was examined again at the age of 8 months, showing the same clinical presentation as before but with new pigmented macules appearing in the lower limbs (Figure 1B), and later on at the age of 7 years, showing newly extensive pigmentation of the upper and lower limbs, and abdomen skin, as well as in the periphery of the WF (Figure 1C). In addition, the patient developed multiple CALMs in the upper eyelids of the right eye and right upper arm (Figure 1C). No skin freckles or tumors were detected on examination, and the patient was referred to the ophthalmology department to check for the presence of Lisch nodules and ENT team to check for extracutaneous abnormalities, such as impaired hearing or deafness. No abnormalities were detected.
Given the unusual piebaldism course presentation, a blood sample was collected at the last follow-up consultation for KIT sequencing after obtaining informed consent from the parents of the patient. Genetic analysis revealed a heterozygous KIT variant (NM_000222.2: c.1991–2A>G) that was likely pathogenic. A piebaldism diagnosis was confirmed, and the patient was scheduled regular health follow-up consultations.
Discussion
This case report highlights the possibility of generalized regression of the depigmented patches that characterize piebaldism, which commonly remain fixed over the life of the patients, during the growth stage. Noteworthily, a KIT mutation was found, for the first time, to be associated with this unusual clinical presentation. Nonetheless, WF regression, which has been rarely reported in the literature, was previously associated with a KIT variant in a familial case of piebaldism.11 In particular, the severity and clinical features of piebaldism have been correlated with the type and location of the pathological mutations in the KIT sequence.12 Two other reports described the spontaneous regression of depigmented patches in the body over period of years or following oral methoxsalen plus ultraviolet A light therapy.10,13 Interestingly, histological analysis of these depigmented lesions revealed lower density of tyrosinase-positive melanocytes within the dermis than healthy melanocytes, highlighting the molecular variability associated with piebaldism. However, no genetic analysis was performed in these cases to confirmed whether these particular time-dependent phenotypes and molecular findings were related to specific genetic mutations.
In the present piebaldism case, the KIT variant c.1991–2A>G, which is classified as highly pathogenic according to The American College of Medical Genetics and Genomics database, was identified with high recommendation for parental targeted testing to establish the origin of the variant. Based on the clinical presentation, it is reasonable to believe that this specific KIT variant may lead to the migration of melanocytes to the depigmented patches distributed throughout the body of the patient, despite their abnormal melanogenesis function. For unknown reasons, these melanocytes start functioning after birth, resulting in the regression of the depigmented patches. In addition, this KIT mutation was found to be clinically associated with CALMs. This clinical coexistence has been previously reported and is believed to be a rare piebaldism phenotype,14 and other KIT mutations were associated with those cases.15,16 However, as none of these mutations were similar to the herein identified genetic variant, more cases with the same genetic alteration mutation should be identified before correlating this uncommon piebaldism phenotype with this KIT genotype.
In conclusion, KIT variant c.1991–2A>G was identified in a patient with piebaldism who experienced regression of the depigmented lesions while growing up, along with the development of multiple CALMs. These clinical findings expand the current knowledge on the presentations and genetic etiology of this rare disease highlighting the significance of the genotype-phenotype correlation of KIT mutations in piebaldism. Moreover, these findings can reduce the cosmetic concerns expressed by the patient’s parents especially their concern that limited therapeutic options (eg cosmetic camouflage, hair dyes, and temporary pigmented agents) are available to address the disease-associated skin and hair depigmentation.17
Abbreviations
WF, white forelock; CALMs, café-au-lait macules.
Data Sharing Statement
Data sharing is not applicable to this article as no new data were created or analyzed in this study.
Ethics Approval and Informed Consent
The requirement for ethical approval was waived as ethical approval is not required for case reporting in the university.
The patient’s parents provided written informed consent for the publication of this case report and the accompanying images.
Acknowledgments
The genetic testing was performed by Centogene – the rare disease company.
Funding
There is no funding to report.
Disclosure
The author reports no conflict of interest in this work.
References
1. Shah M, Patton E, Zedek D. Piebaldism. Treasure Island (FL): StatPearls Publishing; 2023.
2. Giebel LB, Spritz RA. Mutation of the KIT (mast/stem cell growth factor receptor) protooncogene in human piebaldism. Proc Natl Acad Sci U S A. 1991;88(19):8696–8699. doi:10.1073/pnas.88.19.8696
3. Sánchez-Martín M, Pérez-Losada J, Rodríguez-García A, et al. Deletion of the SLUG (SNAI2) gene results in human piebaldism. Am J Med Genet A. 2003;122A(2):125–132. doi:10.1002/ajmg.a.20345
4. Saleem MD. Biology of human melanocyte development, Piebaldism, and Waardenburg syndrome. Pediatr Dermatol. 2019;36(1):72–84. doi:10.1111/pde.13713
5. Pham DDM, Guhan S, Tsao H. KIT and melanoma: biological insights and clinical implications. Yonsei Med J. 2020;61(7):562–571. doi:10.3349/ymj.2020.61.7.562
6. Hu S, Chen Y, Zhao B, et al. KIT is involved in melanocyte proliferation, apoptosis and melanogenesis in REX rabbit. PeerJ. 2020;8:e9402. doi:10.7717/peerj.9402
7. Friedman JM. Neurofibromatosis 1: clinical manifestations and diagnostic criteria. J Child Neurol. 2002;17(8):548–651. doi:10.1177/088307380201700802
8. Akarsu S, Ilknur T, Avcı C, Fetil E. Piebaldism Associated with Café-au-lait Macules and Intertriginous Freckling: a Case Report and Review of the Literature. Ann Dermatol. 2019;31(5):567–570. doi:10.5021/ad.2019.31.5.567
9. Gaudiello F, Ferrillo M, Vastarella M, Fabbrocini G, Patrì A. Repigmentation of white forelock in a familial case of piebaldism reported via teledermatology in the COVID-19 era. Skin Appendage Disord. 2021;7(2):120–122. doi:10.1159/000512033
10. Fukai K, Hamada T, Ishii M, Kitajima J, Terao Y. Acquired pigmented macules in human piebald lesions. Ultrastructure of melanocytes in hypomelanotic skin. Acta Derm Venereol. 1989;69(6):524–527.
11. Matsunaga H, Tanioka M, Utani A, Miyachi Y. Familial case of piebaldism with regression of white forelock. Clin Exp Dermatol. 2008;33(4):511–512. doi:10.1111/j.1365-2230.2008.02703.x
12. Ward KA, Moss C, Sanders DS. Human piebaldism: relationship between phenotype and site of kit gene mutation. Br J Dermatol. 1995;132(6):929–935. doi:10.1111/j.1365-2133.1995.tb16951.x
13. Hayashibe K, Mishima Y. Tyrosinase-positive melanocyte distribution and induction of pigmentation in human piebald skin. Arch Dermatol. 1998;124(3):381–386. doi:10.1001/archderm.1988.01670030047020
14. Chiu YE, Dugan S, Basel D, Siegel DH. Association of Piebaldism, multiple cafe-au-lait macules, and intertriginous freckling: clinical evidence of a common pathway between KIT and sprouty-related, ena/vasodilator-stimulated phosphoprotein homology-1 domain containing protein 1 (SPRED1). Pediatr Dermatol. 2013;30(3):379–382. doi:10.1111/j.1525-1470.2012.01858.x
15. Li X, Xing X, Liang X, et al. Piebaldism with café-au-lait macules resulting from a novel mutation of KIT gene in a three-generation Chinese family. Skin Res Technol. 2023;29(6):e13352. doi:10.1111/srt.13352
16. Hegde SS, Srinivas SM, Nanjundappa N. KIT gene mutation causing piebaldism associated with multiple café au-lait like macules and freckling: delineating a cause of this coexistence. Indian Dermatol Online J. 2022;14(2):240–244. doi:10.4103/idoj.idoj_368_22
17. Suga Y, Ikejima A, Matsuba S, Ogawa H. Medical pearl: DHA application for camouflaging segmental vitiligo and piebald lesions. J Am Acad Dermatol. 2002;47(3):436–438. doi:10.1067/mjd.2002.119670
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.