")
Back to Journals » Clinical Interventions in Aging » Volume 19
Low HALP (Hemoglobin, Albumin, Lymphocyte, and Platelet) Score Increases the Risk of Post-Stroke Cognitive Impairment: A Multicenter Cohort Study
Authors Zuo L, Dong Y, Liao X, Hu Y, Pan Y, Yan H , Wang X, Zhao X , Wang Y, Seet RCS, Wang Y, Li Z
Received 28 July 2023
Accepted for publication 24 November 2023
Published 10 January 2024 Volume 2024:19 Pages 81—92
DOI https://doi.org/10.2147/CIA.S432885
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Zhi-Ying Wu
Lijun Zuo,1,* Yanhong Dong,2,* Xiaoling Liao,1 Yang Hu,1 Yuesong Pan,3 Hongyi Yan,3 Xingao Wang,1 Xingquan Zhao,1 Yilong Wang,1 Raymond CS Seet,4,5 Yongjun Wang,1,3 Zixiao Li1,3,6– 8
1Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, Beijing, People’s Republic of China; 2Alice Lee Centre for Nursing Studies, Yong Loo Lin School of Medicine, National University of Singapore, Clinical Research Centre, Singapore; 3China National Clinical Research Center for Neurological Diseases, Beijing Tiantan Hospital, Capital Medical University, Beijing, People’s Republic of China; 4Department of Medicine, Yong Loo Lin School of Medicine, National University of Singapore, Singapore; 5Division of Neurology, Department of Medicine, National University Hospital, Singapore; 6Beijing Tiantan Hospital, Capital Medical University, and the Research Unit of Artificial Intelligence in Cerebrovascular Disease, Chinese Academy of Medical Sciences, Beijing, People’s Republic of China; 7National Center for Healthcare Quality Management in Neurological Diseases, Beijing, People’s Republic of China; 8Chinese Institute for Brain Research, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zixiao Li, Department of Neurology, Beijing Tiantan Hospital, Capital Medical University, No. 119, South 4th Ring West Road, Fengtai District, Beijing, 100070, People’s Republic of China, Email [email protected]
Objective: The HALP (hemoglobin, albumin, lymphocyte, and platelet) score is a novel indicator that measures systemic inflammation and nutritional status that has not been correlated with the risk of post-stroke cognitive impairment in patients with acute ischemic stroke or transient ischemic attack (TIA).
Methods: Study participants were recruited from 40 stroke centers in China. The HALP score was derived using a weighted sum of hemoglobin, albumin, lymphocytes and platelets, and study participants were categorized into 4 groups of equal sizes based on quartiles cutoffs of the HALP score. The Montreal Cognitive Assessment (MoCA)-Beijing Cognitive Assessment Scale (MoCA-Beijing) was performed at 2 weeks and 12 months following stroke onset. Post-stroke cognitive impairment was considered in patients with MoCA-Beijing≤ 22. Multiple logistic regression methods were employed to evaluate the relationship between the HALP score and the subsequent risk of developing post-stroke cognitive impairment.
Results: The study population comprised 1022 patients (mean age 61.6± 11.0 years, 73% men). The proportion of individuals with MoCA-Beijing≤ 22 at 2 weeks was 49.2% and 32.4% at one year. Patients in the lowest quartile of HALP score (< 36.56) were observed to harbor the highest risk of post-stroke cognitive impairment at 12 months post-stroke/TIA compared to those in the highest quartile (odds ratio=1.59, 95% CI=1.07– 2.37, p=0.022), and lower domain scores for executive function, naming, and attention. There were no statistically significant differences between patients in the different quartiles of HALP score and HALP score at 2 weeks post-stroke/TIA.
Conclusion: The HALP score is a simple score that could stratify the risk of post-stroke cognitive impairment in stroke/TIA patients to facilitate early diagnosis and interventions.
Keywords: mild stroke, post stroke cognitive impairment, hemoglobin, albumin, lymphocyte, platelet
Introduction
Stroke is one of the most common causes of deaths and disability, and it is highly associated with an increased risk of cognitive impairment.1 Non-disabling cerebrovascular events including mild ischemic stroke (median NIHSS=2, median mRS=2) and transient ischemic attack (TIA) generally result in either short-lasting or mild neurological symptoms,2 but these patients are at an increased risk of a recurrent cerebrovascular event and often suffered from cognitive impairment. Inflammation and malnutrition may be involved in post-stroke cognitive impairment (PSCI).3,4 Some studies have demonstrated that lymphocytes could repair the injury via inflammation5 and were important immunomodulators for protection after acute ischemic stroke.6 Decreased lymphocytes level might indicate a poor outcome in systemic inflammatory disease. Recently, low lymphocyte to monocyte ratio was reported to be novel predictors of morbidity and mortality after ischemic stroke.7,8 One study found that the cardiovascular surgery process could increase monocyte and decrease lymphocyte quantities, and the decreased Lymphocyte-to-monocyte ratio was associated with cognitive dysfunction after cardiovascular surgery.9 Ischemic stroke may result in impaired platelet function and excessive activation and accumulation of platelets could hamper stroke recovery,10 while a high platelet-to-lymphocyte ratio has been observed in patients with symptomatic internal carotid artery stenosis,11 poor functional stroke outcomes,12 and cognitive impairment.13 One study found a link between increased platelet prothrombotic potential at the time of stroke and subsequent development of vascular cognitive impairment.14
Malnutrition is associated with PSCI. Stroke patients with low hemoglobin levels have been found to harbor increased risks of PSCI.15 Studies reported that decreased hemoglobin levels might lead to brain hypoxia, mitochondrial dysfunction, and neuronal damage. Patients who have ischemia stroke with hypoxic conditions are much more susceptible to Alzheimer’s disease.16 Moreover, a population-based study demonstrated that anemia was associated with the incidence of dementia and cognitive decline, and severe anemia may lead to an increased risk of dementia.17 Hemoglobin level is a significant independent predictor of PSCI.15 Serum albumin is widely considered a surrogate of nutrition where deficiencies in serum albumin have been associated with poorer stroke outcomes,12 explained in part by an impaired antioxidant capacity to protect neurons from ischemic injury.18 The geriatric nutritional risk index based on serum albumin has been similarly implicated in PSCI.19 Ischemic stroke patients with low albumin levels could not maintain normal neuronal metabolism and experience unfavorable outcomes. Moreover, albumin has a strong antioxidative activity that might protect the neurons from ischemic injury.18
In view of the above, we aggregated these inflammatory and nutritional indicators to explore the association between inflammation, nutrition, and PSCI in this study. In patients with multiple malignancies, the HALP (hemoglobin, albumin, lymphocyte, and platelet) score is a readily accessible measure of systemic inflammation and nutritional status linked with prognosis.20,21 Recent studies have shown that the HALP score could predict stroke recurrence and poor outcome.22,23 There is, however, only one study reporting the association between the HALP score and short-term PSCI, ie, within 2 weeks at subacute stroke phase.21
Malnutrition and inflammatory states can develop frailty. Frailty is a multidimensional geriatric syndrome manifested with accumulated deficits (energy, physical ability, cognition, and health) that give rise to vulnerability. A higher frailty index (FI) indicates more severe frailty.24 Recent reports suggest that frailty index based on common laboratory tests (FI-Lab) may serve as a diagnostic tool for frailty and is associated with mortality.25 Acute cerebral infarction subjects patients to adverse events, such as pneumonia26 and cognitive disorders.27 Pre-stroke frailty is often measured by the modified Rankin scale (mRS).
Hence, we aim to explore the relationships between the HALP score and PSCI both at subacute stroke phase and 1 year late.
Methods
Study Population
Data of this study are drawn from the Impairment of Cognition and Sleep (ICONS) study. ICONS is one of the research subgroups of China National Stroke Registry-III (CNSR-III) database. The CNSR-III is a nationwide prospective hospital-based registry for patients with acute ischemic stroke (AIS) or TIA within 7 days performed in August 2015 to March 2018 in China.28 Patients’ stroke/TIA were diagnosed by neurologists and confirmed with brain computed tomography or magnetic resonance imaging. The acute ischemic stroke was diagnosed according to World Health Organization criteria.29 TIA was defined by the American Stroke Association.30 All the participating hospitals approved the protocol. All participants or their legal proxies signed written informed consent. A total of 40 study sites participated in ICONS subgroup. Finally, 1022 patients received the Montreal Cognitive Assessment (MoCA)-Beijing and HALP (hemoglobin, albumin, lymphocyte, and platelet) scores at baseline (within two weeks of index event) and at 1 year.
The study population included patients (1) aged > 18 years older; (2) with a diagnosis of AIS or TIA within 7 days;
The exclusion criteria included: (1) silent cerebral infarction diagnosed by MRI or CT without symptoms or signs; (2) patients who were illiteracy; (3) history of cognitive impairment, psychosis, or schizophrenia disease (documented in medical records); (4) physical disability affecting cognitive tests, eg, visual or hearing disorders, severe unilateral neglect, severe aphasia [defined as National Institutes of Health Stroke Scale (NIHSS) item 9>2].
Data collection for ICONS was approved by the ethics committee of all participating hospitals.28 All patients or participants provided their written informed consent for this study.
Baseline Data Collection
Baseline data, including age, gender, body mass index (BMI calculated as weight in kilograms divided by the square of height in meters, km/m2), smoking, drinking, body mass index, educational level, and medical histories (hypertension, diabetes, hyperlipidemia, coronary heart disease, atrial fibrillation, heart failure, stroke, epilepsy, smoking, and drinking) were collected.
A detailed physical examination was completed, and several parameters, including the mRS, Trial of ORG 10172 in Acute Stroke Treatment (TOAST) type and NIHSS score. Participants’ anxiety and depression status were assessed by the 7-item Generalized Anxiety Disorder Scale (GAD) and Patient Health Questionnaire-9 (PHQ-9). The blood samples were gathered within 24h of admission and transported through the cold chain to the central laboratory. All serum samples were kept frozen at −80◦C until ready for assay.
Sample Collection and Measurement
Fasting whole blood samples were routinely processed within 24 hours of admission and were tested at study sites or the center laboratory in Beijing Tiantan Hospital. Platelets, lymphocyte counts, and hemoglobin concentration were measured by automated hematology analyzers at each participating hospital. Serum albumin was also tested in participating hospital within 24 hours of admission. Bromocresol purple assay or bromocresol green assay were used to analyze the serum albumin levels according to the test reagent of participating hospital. The following formula was used to calculate HALP scores: hemoglobin (g/L) × albumin (g/L) × lymphocytes (/L) / platelets (/L).31 The patients were categorized according to quartiles of the HALP score.
Cognitive Assessment
The original MoCA is the most commonly used cognitive-screening scale with 30 points, including Visuospatial/executive abnormal (5 points), Naming (3 points), Attention (2 points), Language (2 points), Delayed recall (5 points) Orientation (6 points). There were several official language versions of the MoCA, and the cutoffs are different. The MoCA-Beijing was developed with some modifications as previous study presented.32 According to our previous work, a MoCA-Beijing cutoff score of 22/23 is optimally sensitive and specific for detecting cognitive impairment after mild stroke and TIA in the acute stroke phase.33 One point was added to the total score for those with education <12 years. All the participants were evaluated for cognitive status at 2-weeks, 3-months, and 1-year by trained neurologists at each center.
Assessment of Pre-Stroke Frailty Status
In stroke, the mRS is often used for measuring pre-stroke dependency. Pre-stroke mRS > 2 was also considered as pre-stroke frailty.34,35
Outcome Evaluation
The MoCA-Beijing was used to assess global cognition and detect PSCI. The MoCA-Beijing was developed with the following modifications as shown by a previous study.32 The primary outcome was PSCI at 2 weeks and at 1 year after AIS or TIA. Patients who have MoCA-Beijing ≤22 were regarded as having cognitive impairment, determined by formal neuropsychological tests.33 The optimal cutoff point of MoCA-Beijing ≤22 has excellent discriminant ability (sensitivity: 85% and specificity: 88%).33
Statistical Analysis
SAS 9.4 (SAS Institute Inc, Cary, NC) was used for data analysis. Measurement data were tested for normality using the Kolmogorov–Smirnov test. Continuous variables with normal distribution were expressed as mean± standard deviation (mean±SD), and statistical differences were calculated by analysis of variance. Skewed data were described as median (interquartile range) and analyzed using nonparametric tests. Categorical variables were analyzed by the Chi square test. Patients in this study were categorized into 4 groups by HALP quartiles. Multivariable logistic regression analysis was used to evaluate the associations among HALP and PSCI. All independent variables included in the multivariate analysis were independent from each other, and there was no multicollinearity (tolerance of all independent variables was greater than 0.1). The Box–Tidwell method calculated that there was a linear relationship between the independent variables included in the multivariate model and the logit transformation value of the dependent variable Two analysis models were performed with adjustment for demographics only and together with clinical factors. P < 0.05 was considered statistically significant.
Results
Baseline Characteristics
There were 2625 patients enrolled in the ICONS study. We excluded 1603 patients missing HALP on admission and MoCA results during the 1-year follow-up. Finally, 1022 patients were included in the current analysis. Most patients were at their 60s (61.59±11.00 years old), and 746 (72.99%) participants were male. The HALP score ranges based on quartiles (Q1–Q4) were defined as follows: Q1<36.56, Q2 36.56–48.83, Q3 48.83–65.08, and Q4>65.08. The differences in demographics and clinical characteristics of patients among different HALP scores is shown in Table 1. Patients in Q1 quartile are significantly older, have a more prevalent smoking history, have lower BMI, and lower scores in scores at 2 weeks and 1 year (Table 1). They also had lower scores on pre-stroke mRS, 2 week-mRS and 1-year mRS (Table 1). In cognitive sub-test domains, patients with HALP scores in Q1 layer had significantly lower scores than Q4 layer in executive function (3.16±1.65 vs 3.60±1.48, p=0.003), naming (2.66±0.73 vs 2.82±0.56, p=0.017) and attention (5.18±1.28 vs 5.42±1.03, p=0.044) (Table 1).
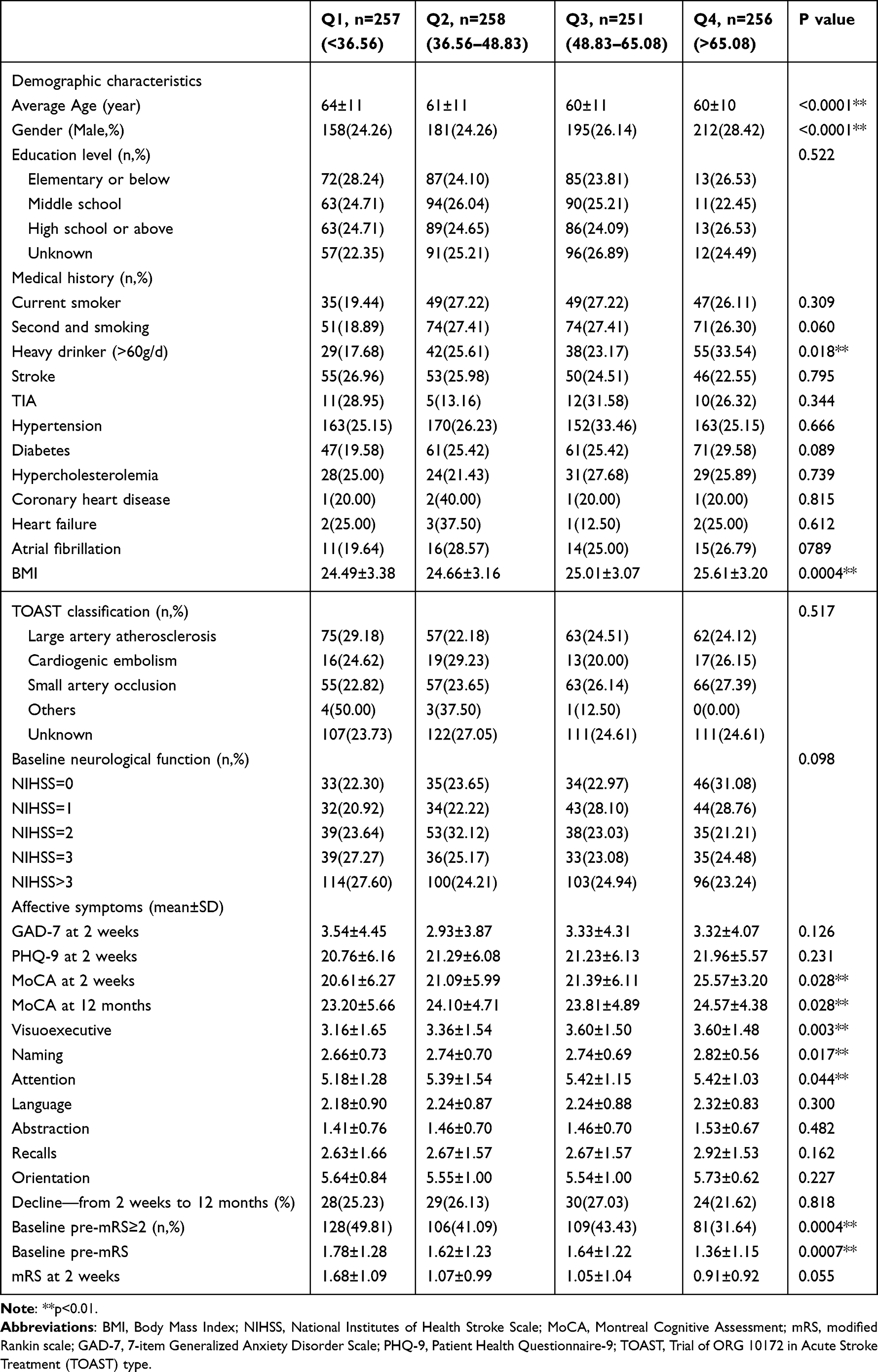 |
Table 1 Demographic, Clinical Characteristics and Outcomes of Patients with Different HALP Score Ranges |
Logistic Regression Analysis
A total of 503 participants (49.21%) suffered from PSCI at 2 weeks and 331 participants (32.39%) suffered from PSCI at 1-year follow-up (Table 2). The 2-week incidence of PSCI with different HALP scores (from low to high, ie, Q1 to Q4) were 54.86%, 46.90%, 49.80%, and 45.31%, respectively. After adjustment, the HALP score was not significantly associated with PSCI at 2-weeks follow-up (Table 2). The 1-year incidence of PSCI with different HALP scores (from low to high, ie, Q1 to Q4) were 40.84%, 31.78%, 30.28%, and 26.56%, respectively (Table 3). After adjustment for conventional covariables (Model 1) and further adjustment for smoking, history of stroke, hypertension, diabetes, coronary heart disease, atrial fibrillation, TOAST type, NIHSS score, mRS, and MoCA scores at baseline in model 2, patients in the lowest quartile of HALP score (Q1) had worse cognitive function (MoCA≤22) compared with the highest quartile [quartile (Q) 1 vs Q4: adjusted odds ratio (aOR) 1.13, 95% confidence interval: 0.74–1.75, p=0.022; Q2 vs Q4: aOR 1.16, 95% confidence interval: 0.75–1.77, p = 0.32; Q3 vs Q4: aOR 1.57, 95% confidence interval: 1.02–2.41, p=0.38]. (Figure 1).
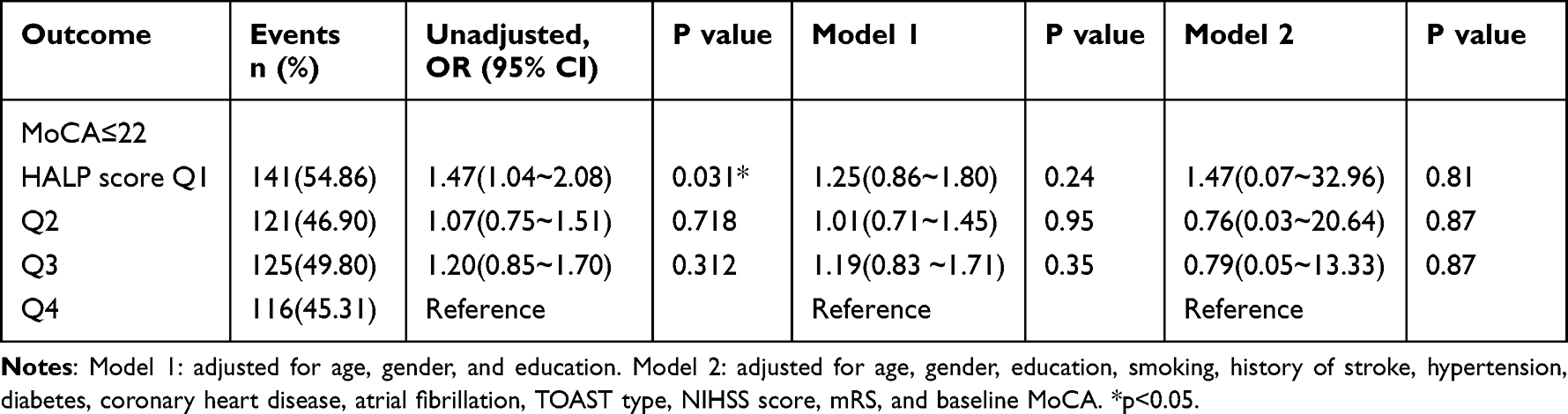 |
Table 2 Logistic Regression Analysis of Cognitive Outcomes at 2 Weeks in AIS/TIA Participants |
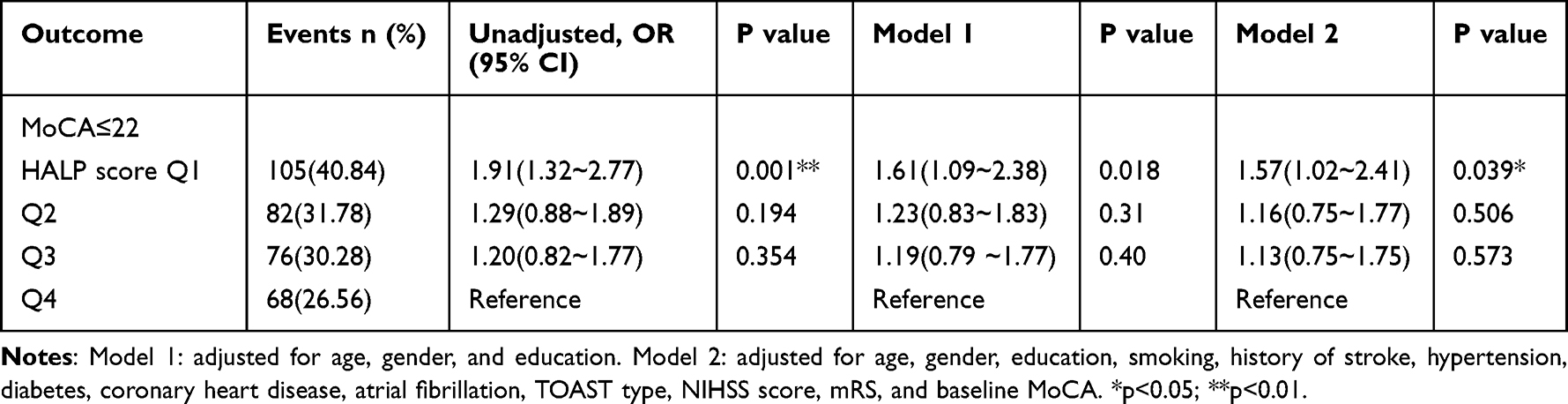 |
Table 3 Logistic Regression Analysis of Cognitive Outcomes at 12 Months in AIS/TIA Participants |
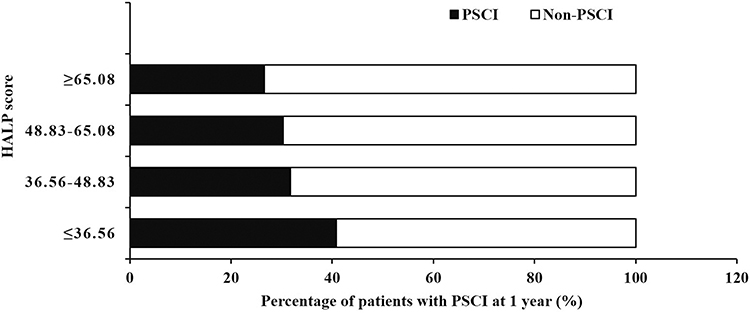 |
Figure 1 Percentage of patients with PSCI at 1 year. |
Subgroup Analysis
HALP score for 1-year incidence of cognitive impairment and ORs for cognitive impairment at 1-year by age, sex, and etiology of stroke are shown in Table 4. After adjusting for all potential confounding variables, the hazards or odds of PSCI were not modified by age, sex, and etiology of stroke (all P values for interaction >0.05). Significant associations were found between lower HALP scores and 1-year PSCI. Such associations are more pronounced in those who are older (≥60 years), male, and with the large artery atherosclerosis subtype (Figure 2).
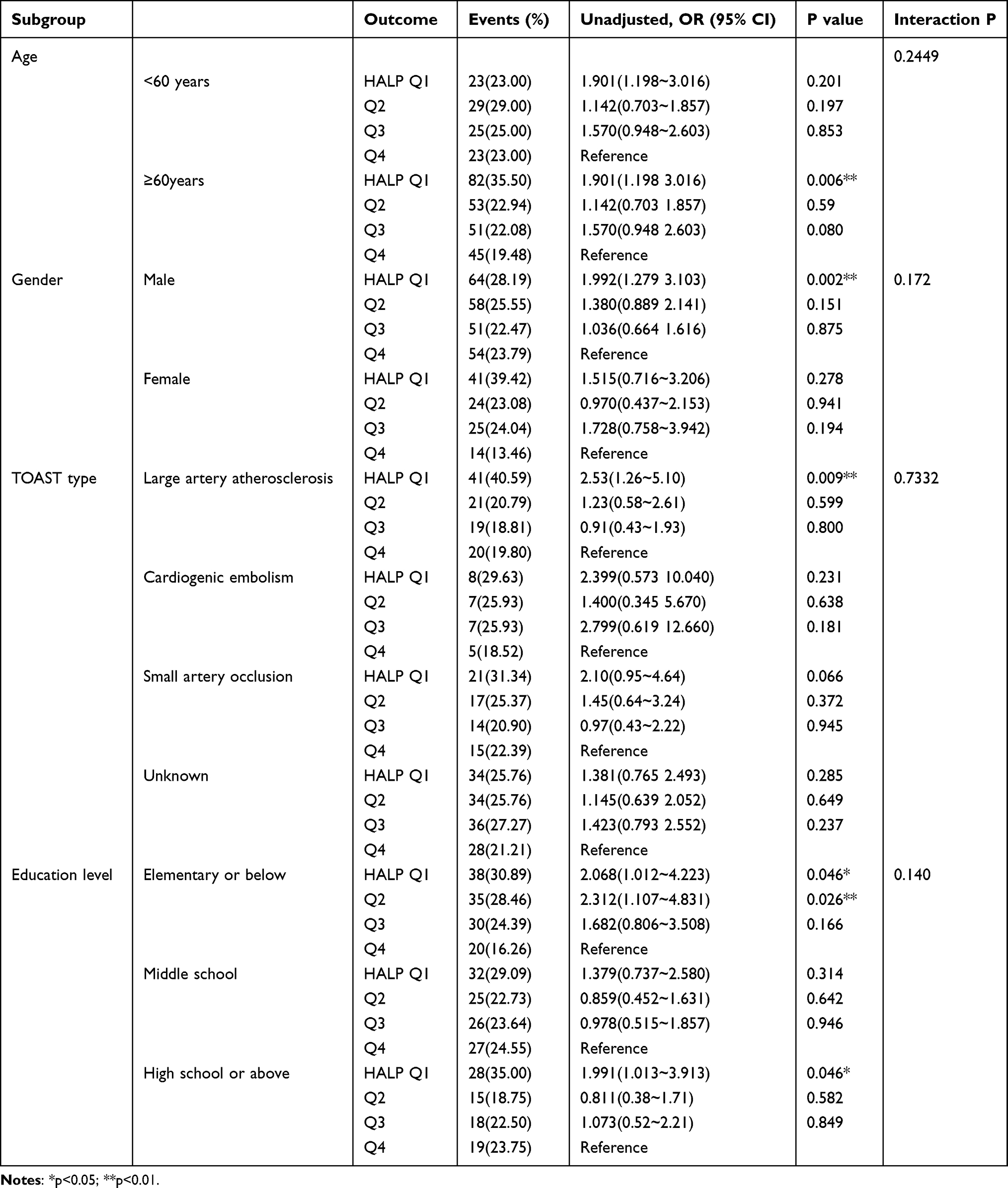 |
Table 4 Subgroup Analysis of Association Between HALP Score and Cognitive Function |
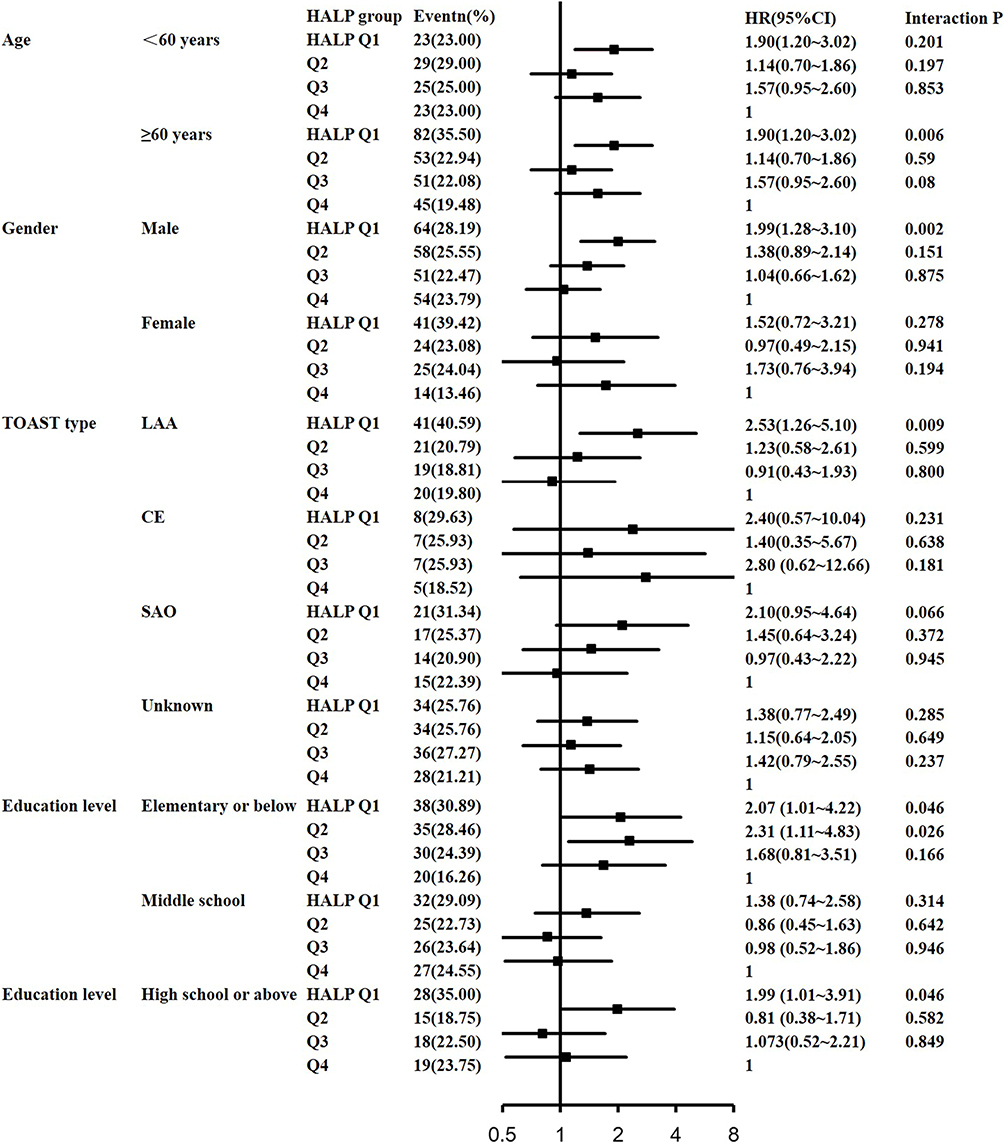 |
Figure 2 Subgroup analysis of association between HALP score quartiles and 1-year post-stroke cognitive impairment (PSCI) in patients with acute ischemic stroke/transient ischemic attack recurrence. |
Discussion
In this prospective study, we explored the relationships between HALP score and short-and long-term cognitive impairment after AIS/TIA. Patients with a lower HALP score at admission have more risk of frailty and were more likely to suffer from short-and long-term PSCI, suggesting that low HALP score might be a potential risk factor for cognitive impairment in the short and long term following stroke. And there was no heterogeneity in the effects of HALP score levels on the PSCI between subgroups classified by age, gender, TOAST subtypes, and educational level.
Inflammation plays a critical role in the pathophysiology of stroke and dementia. Systemic inflammation may increase morbidity and mortality and cause cognitive decline in patients with stroke.36 Systemic inflammation processes are thought to be closely associated with endothelial dysfunction, damaged blood–brain barrier and reduced cerebral blood flow, thus lead to cognitive impairment.37 Leucocytes are important components of systemic inflammation and play a key role in immune regulation. Studies have shown that neuroprotective subtypes of lymphocytes decrease in response to stress-induced corticosteroids and lead to poor prognosis and neurological impairment after ischemic stroke.6 Previous studies have shown that immunosuppression and decreased levels of lymphocytes after a stroke lead to a poorer prognosis.38
Platelets have a primary role in the thrombo-inflammation of stroke10,12 and predict poor functional outcomes. When a stroke occurs, massive production of platelets accumulated to the injured endothelial regions. The inflammatory substances secreted by them can further recruit more inflammatory cells such as leukocytes to the site of injury, amplify the inflammatory response, and cause injury to both inside and outside blood vessels, as well as to neurons, eventually damaging brain tissue.39 In contrast, lymphocytes are known to control inflammatory response by modulating and repairing inflammation during cerebral ischemia. The platelet-to-lymphocyte ratio has recently been reported as a potential novel biomarker in acute ischemic stroke intravenous thrombolysis treatment.40,41 Apart from this, the platelet-to-lymphocyte ratio was found to be associated with lower cognitive performance in patients with breast cancer survivors and type 2 diabetes.42 This study has also shown the role of inflammation in long-term cognitive problems.
The prevalence of malnutrition risk in AIS patients ranged from 15.99% to 57.86%, which has been considered to adversely affect the prognoses of stroke and PSCI.43,44 A total of 34 dietary factors were associated with stroke susceptibility.45 Our study showed that the nutritional conditions evaluated at acute stroke stage might affect the cognitive performance 1 year after stroke. The findings are consistent with previous studies. They revealed that malnutrition was associated with poor cognitive improvement after an ischemic stroke.3 Furthermore, another study revealed that the calorie-protein supplements could improve global cognition after a stroke.46 There are several potential mechanisms underlying the association between malnutrition and PSCI, including its influence on the stroke severity, and the premorbid vulnerability of specific brain structures. Malnutrition adversely affects neuronal plasticity and protein synthesis. It also correlates with increased risk for white matter hyperintensities, microbleeds, and mesial temporal lobe atrophy in the general population, and in patients with mild cognitive impairment or dementia.47 Further, malnutrition often results in an immunosuppressive state, increasing the chance of infection during the acute stroke phase.
The levels of hemoglobin and albumin, which were markers of nutritional health, had also been found to be essential indicators for predicting the development of PSCI.19 Hemoglobin transported oxygen to the whole tissues, and the brain consumed nearly 20%. The decreased hemoglobin levels might lead to brain hypoxia, mitochondrial dysfunction, neuronal injury, oxidative stress, and inflammation. Both oxidative stress and inflammation were correlated with cognitive impairment in patients with ischemic stroke.47 It is reported that anemia was associated with cognitive decline in general population, and severe anemia might
increase the risk of dementia.17 Another study showed that premorbid anemia was independently associated with an increased risk for PSCI after 1-month follow-up.48
The HALP score, as an index, combines hemoglobin, albumin, lymphocyte, and platelet, which results in the unique advantage of linking key pathways in both inflammation and nutritional condition.22 The previous study proved that lower HALP score correlated with an increased risk of early-onset PSCI.49 However, we did not find the relationship between HALP score and PSCI at 2 weeks in our study. Firstly, cognitive evaluation scales were different in the previous study and the present study [Mini-Mental State Examination (MMSE) vs MoCA], the MoCA has been reported to be sensitive to changes in acute cognitive impairment after mild stroke/TIA, whereas the MMSE is reportedly not.11 Secondly, patients’ cognition was poorer in the previous study (average MMSE=18) than the present study (average MoCA=23), indicating HALP is related to poorer cognitive status at the subacute phase and the residual cognitive impairment over a longer term. Additionally, the cognitive status was not stable and could be affected by many factors such as delirium and mood at acute phase. Some patients might have deteriorated, while others improved or keeping stable, respectively. Our novel finding is that the HALP score could predict long-term PSCI at 1 year, which was relatively stable and residual cognitive impairment, prompting for early intervention and targeted management.
The hemoglobin, albumin, lymphocyte, and platelet are important components of laboratory tests for frailty index assessment.50 Frailty represents multiple systems deficits such as comorbidity, weakness, malnutrition, and cognitive impairment. In stroke patients, the mRS>2 is often used for measuring stroke frailty.34,35 In this study, the prevalence of pre-stroke frailty (defined as mRS>2) were high in Q1 group than that in other groups. We suggest that the HALP score could partly reflect frailty, as it is a stronger predictor of post-stroke cognitive impairment and also prognosis. In subgroup analysis, the relationship between HALP and PSCI was more significant in patients aged ≥60 years old. Individuals age biologically at different rates. Frailty increases multisystem decline and its vulnerability with age. In frailty, this decline is accelerated in older individuals, which is consistent with our study.51 The relationship between HALP and PSCI was more significant in males, suggesting possible sex bias with HALP score. Females usually live longer than men.52 In previous studies on older individuals, a greater risk for mortality in males than females was found.53 Further study is required in this area.
Another novel finding of our study is to show differences in HALP scores under stroke etiology. In particular, among patients with large artery atherosclerosis, a lower HALP score was significantly associated with 1-year cognitive impairment. This might be due to different post-ischemic inflammatory responses and nutritional states in patients with different TOAST classifications. Atherosclerosis is due to chronic inflammation. In patients with large artery atherosclerosis, ischemic stroke might trigger a much stronger inflammatory response based on this chronic inflammatory process. Malnutrition may aggravate existing inflammation and accelerate atherosclerosis, worsening patients’ cognitive decline.54
There are some limitations to our study. Firstly, the HALP score was measured according to the data derived on admission. However, the HALP score was likely to fluctuate, so we were unable to examine the associations of HALP dynamic changes with 1-year PSCI; Secondly, as we all known, the platelet and lymphocyte count were not stable at acute phase, they might be different and fluctuate during 7 days. And it might have an effect on the results. In future studies, we will refine the analysis at 1 and 7 days after stroke to get a better understanding of the association of peripheral inflammation with PSCI. Thirdly, all patients with AIS or TIA were enrolled consecutively, and a minority of patients with TIA were included in the study, leading to results less generalizable to TIA patients. Fourthly, patient with a history of severe cognitive impairment were excluded from this study. Moreover, we did not assess the cognitive function before the stroke. Cognitive assessment was mainly evaluated in mild stroke patients (median NIHSS=3, median mRS=1). Hence, patients with severe stroke or severe aphasia could not undertake cognitive evaluation, which may lead to the underestimate of cognitive function and impede results generalization.
Conclusions
To sum up, the risks from malnutrition and inflammation, represented as low HALP score at subacute stroke phase, were independently associated with PSCI at 12 months after the occurrence of ischemic stroke. The HALP score may help identify high-risk patients for PSCI, enhance early targeted stroke care (swallowing assessments, nutritional intervention) for these patients, and follow-up with further management, such as anti-inflammatory therapy and nutritional intervention.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author on reasonable request.
Ethical Approval
This study involves human participants and was approved by the Ethics Committee of all participating hospitals (Appendix S1) in accordance with the Declaration of Helsinki, and the IRB approval number is KY2015-001-01.
Informed Consent
Prior to data collection, all participants or their legal representatives signed written informed consents.
Acknowledgments
The authors would like to thank all participants for their involvement.
Funding
This work was supported by the following institutions: The Capital’s Funds for Health Improvement and Research (2020-1-2041), Chinese Academy of Medical Sciences Innovation Fund for Medical Sciences (2019-I2M-5-029), Capital Medical University Cultivation Fund (PYZ22120). The National Key Research and Development Program of China (2022YFC2504902 and 2020YFC2004800) and Beijing Excellent Talents Training Program (2018000021469G237). Y. Dong is supported by the Singapore National Medical Research Council (NMRC) Transition Award [NMRC/TA/0060/2017].
Disclosure
The authors declare that they have no conflict of interest.
References
1. Blackburn DJ, Bafadhel L, Randall M, et al. Cognitive screening in the acute stroke setting. Age Ageing. 2013;42(1):113–116. doi:10.1093/ageing/afs116
2. Fischer U, Baumgartner A, Arnold M, et al. What is a minor stroke? Stroke. 2010;41(4):661–666. doi:10.1161/STROKEAHA.109.572883
3. Tsutsumiuchi K, Wakabayashi H, Maeda K, et al. Impact of malnutrition on post-stroke cognitive impairment in convalescent rehabilitation ward inpatients. Eur Geriatr Med. 2021;12(1):167–174. doi:10.1007/s41999-020-00393-0
4. Clark C, Richiardi J, Maréchal B, et al. Systemic and central nervous system neuroinflammatory signatures of neuropsychiatric symptoms and related cognitive decline in older people. J Neuroinflammation. 2022;19(1):127. doi:10.1186/s12974-022-02473-3
5. Zou F, Wang J, Han B, et al. Early neutrophil-to-lymphocyte ratio is a prognostic marker in acute ischemic stroke after successful revascularization. World Neurosurg. 2022;157:e401–e409. doi:10.1016/j.wneu.2021.10.097
6. Ren X, Akiyoshi K, Dziennis S, et al. Regulatory b cells limit CNS inflammation and neurologic deficits in murine experimental stroke. J Neurosci. 2011;31(23):8556–8563. doi:10.1523/JNEUROSCI.1623-11.2011
7. Lux D, Alakbarzade V, Bridge L, et al. The association of neutrophil-lymphocyte ratio and lymphocyte-monocyte ratio with 3-month clinical outcome after mechanical thrombectomy following stroke. J Neuroinflammation. 2020;17(1):60. doi:10.1186/s12974-020-01739-y
8. Zhu B, Pan Y, Jing J, et al. Neutrophil counts, neutrophil ratio, and new stroke in minor ischemic stroke or tia. Neurology. 2018;90(21):e1870–e1878. doi:10.1212/WNL.0000000000005554
9. Zhao Q, Gao R, Liu C, et al. Dynamic change of lymphocyte-to-monocyte is associated with the occurrence of pocd after cardiovascular surgery: a prospective observational study. Front Behav Neurosci. 2021;15:646528. doi:10.3389/fnbeh.2021.646528
10. Chen C, Gu L, Chen L, et al. Neutrophil-to-lymphocyte ratio and platelet-to-lymphocyte ratio as potential predictors of prognosis in acute ischemic stroke. Front Neurol. 2020;11:525621. doi:10.3389/fneur.2020.525621
11. Massiot N, Lareyre F, Voury-Pons A, et al. High neutrophil to lymphocyte ratio and platelet to lymphocyte ratio are associated with symptomatic internal carotid artery stenosis. J Stroke Cerebrovascular Dis. 2019;28(1):76–83. doi:10.1016/j.jstrokecerebrovasdis.2018.09.001
12. Yang M, Pan Y, Li Z, et al. Platelet count predicts adverse clinical outcomes after ischemic stroke or tia: subgroup analysis of cnsr ii. Front Neurol. 2019;10:370. doi:10.3389/fneur.2019.00370
13. Du L, Hu X, Zhang B, et al. The relationship of platelet-to-lymphocyte ratio with cognitive decline in t2dm. Diabetol Metab Syndr. 2021;13(1):151. doi:10.1186/s13098-021-00772-y
14. Kirkpatrick AC, Stoner JA, Dale GL, et al. Higher coated-platelet levels in acute stroke are associated with lower cognitive scores at three months post infarction. J Stroke Cerebrovasc Dis. 2019;28(9):2398–2406. doi:10.1016/j.jstrokecerebrovasdis.2019.06.033
15. Gu Y, Wang F, Gong L, et al. A nomogram incorporating red blood cell indices to predict post-stroke cognitive impairment in the intracerebral hemorrhage population. Front Aging Neurosci. 2022;14:985386. doi:10.3389/fnagi.2022.985386
16. Zhang X, Le W. Pathological role of hypoxia in Alzheimer’s disease. Exp Neurol. 2010;223(2):299–303. doi:10.1016/j.expneurol.2009.07.033
17. Jeong SM, Shin DW, Lee JE, et al. Anemia is associated with incidence of dementia: a national health screening study in Korea involving 37,900 persons. Alzheimers Res Ther. 2017;9(1):94. doi:10.1186/s13195-017-0322-2
18. Ruan Y, Yuan C, Liu Y, et al. High fibrinogen-to-albumin ratio is associated with hemorrhagic transformation in acute ischemic stroke patients. Brain Behav. 2021;11(1):e01855. doi:10.1002/brb3.1855
19. Lee M, Lim JS, Kim Y, et al. Association between geriatric nutritional risk index and post-stroke cognitive outcomes. Nutrients. 2021;13(6):1776.
20. Cong L, Hu L. The value of the combination of hemoglobin, albumin, lymphocyte and platelet in predicting platinum-based chemoradiotherapy response in male patients with esophageal squamous cell carcinoma. Int Immunopharmacol. 2017;46:75–79. doi:10.1016/j.intimp.2017.02.027
21. Peng D, Zhang CJ, Gong YQ, et al. Prognostic significance of halp (hemoglobin, albumin, lymphocyte and platelet) in patients with bladder cancer after radical cystectomy. Sci Rep. 2018;8(1):794. doi:10.1038/s41598-018-19146-y
22. Xu SS, Li S, Xu HX, et al. Haemoglobin, albumin, lymphocyte and platelet predicts postoperative survival in pancreatic cancer. World J Gastroenterol. 2020;26(8):828–838. doi:10.3748/wjg.v26.i8.828
23. Tian M, Li Y, Wang X, et al. The hemoglobin, albumin, lymphocyte, and platelet (halp) score is associated with poor outcome of acute ischemic stroke. Front Neurol. 2020;11:610318. doi:10.3389/fneur.2020.610318
24. Buckinx F, Reginster JY, Petermans J, et al. Relationship between frailty, physical performance and quality of life among nursing home residents: the senior cohort. Aging Clin Exp Res. 2016;28(6):1149–1157. doi:10.1007/s40520-016-0616-4
25. Blodgett JM, Theou O, Howlett SE, et al. A frailty index based on laboratory deficits in community-dwelling men predicted their risk of adverse health outcomes. Age Ageing. 2016;45(4):463–468. doi:10.1093/ageing/afw054
26. Elkind MSV, Boehme AK, Smith CJ, et al. Infection as a stroke risk factor and determinant of outcome after stroke. Stroke. 2020;51(10):3156–3168. doi:10.1161/STROKEAHA.120.030429
27. Brainin M, Teuschl Y. Poststroke neurocognitive disorders are mostly defined by strategic lesions. Stroke. 2018;49(11):2563–2564. doi:10.1161/STROKEAHA.118.023090
28. Wang Y, Jing J, Meng X, et al. The third China national stroke registry (cnsr-iii) for patients with acute ischaemic stroke or transient ischaemic attack: design, rationale and baseline patient characteristics. Stroke Vasc Neurol. 2019;4(3):158–164. doi:10.1136/svn-2019-000242
29. Stroke--1989. Recommendations on stroke prevention, diagnosis, and therapy. Report of the who task force on stroke and other cerebrovascular disorders. Stroke. 1989;20(10):1407–1431. doi:10.1161/01.STR.20.10.1407
30. Easton JD, Saver JL, Albers GW, et al. Definition and evaluation of transient ischemic attack: a scientific statement for healthcare professionals from the American Heart Association/American Stroke Association Stroke Council; Council on Cardiovascular Surgery and Anesthesia; Council on Cardiovascular Radiology and Intervention; Council on Cardiovascular Nursing; and the Interdisciplinary Council on Peripheral Vascular Disease. The American Academy of Neurology affirms the value of this statement as an educational tool for neurologists. Stroke. 2009;40(6):2276–2293. doi:10.1161/STROKEAHA.108.192218
31. Chen XL, Xue L, Wang W, et al. Prognostic significance of the combination of preoperative hemoglobin, albumin, lymphocyte and platelet in patients with gastric carcinoma: a retrospective cohort study. Oncotarget. 2015;6(38):41370–41382. doi:10.18632/oncotarget.5629
32. Nasreddine ZS, Phillips NA, Bedirian V, et al. The Montreal cognitive assessment, moca: a brief screening tool for mild cognitive impairment. J Am Geriatr Soc. 2005;53(4):695–699. doi:10.1111/j.1532-5415.2005.53221.x
33. Zuo L, Dong Y, Zhu R, et al. Screening for cognitive impairment with the Montreal cognitive assessment in Chinese patients with acute mild stroke and transient ischaemic attack: a validation study. BMJ Open. 2016;6(7):e011310. doi:10.1136/bmjopen-2016-011310
34. Myint PK, O. Bachmann M, Loke YK, et al. Important factors in predicting mortality outcome from stroke: findings from the Anglia Stroke Clinical Network Evaluation Study. Age Ageing. 2017;46(1):83–90. doi:10.1093/ageing/afw175
35. Munthe-Kaas R, Aam S, Saltvedt I, et al. Is frailty index a better predictor than pre-stroke modified rankin scale for neurocognitive outcomes 3-months post-stroke? BMC Geriatr. 2022;22(1):139. doi:10.1186/s12877-022-02840-y
36. Atif F, Yousuf S, Espinosa-Garcia C, et al. Post-ischemic stroke systemic inflammation: immunomodulation by progesterone and vitamin d hormone. Neuropharmacology. 2020;181:108327. doi:10.1016/j.neuropharm.2020.108327
37. Evans LE, Taylor JL, Smith CJ, et al. Cardiovascular comorbidities, inflammation, and cerebral small vessel disease. Cardiovasc Res. 2021;117(13):2575–2588. doi:10.1093/cvr/cvab284
38. Li J, Wang J, Wu B, et al. Association between early cognitive impairment and midterm functional outcomes among Chinese acute ischemic stroke patients: a longitudinal study. Front Neurol. 2020;11:20. doi:10.3389/fneur.2020.00020
39. Rawish E, Nording H, Münte T, et al. Platelets as mediators of neuroinflammation and thrombosis. Front Immunol. 2020;11:548631. doi:10.3389/fimmu.2020.548631
40. Sun YY, Wang MQ, Wang Y, et al. Platelet-to-lymphocyte ratio at 24h after thrombolysis is a prognostic marker in acute ischemic stroke patients. Front Immunol. 2022;13:1000626. doi:10.3389/fimmu.2022.1000626
41. Gong P, Liu Y, Gong Y, et al. The association of neutrophil to lymphocyte ratio, platelet to lymphocyte ratio, and lymphocyte to monocyte ratio with post-thrombolysis early neurological outcomes in patients with acute ischemic stroke. J Neuroinflammation. 2021;18(1):51. doi:10.1186/s12974-021-02090-6
42. van der Willik KD, Koppelmans V, Hauptmann M, et al. Inflammation markers and cognitive performance in breast cancer survivors 20 years after completion of chemotherapy: a cohort study. Breast Cancer Res. 2018;20(1):135. doi:10.1186/s13058-018-1062-3
43. Zhang G, Pan Y, Zhang R, et al. Prevalence and prognostic significance of malnutrition risk in patients with acute ischemic stroke: results from the third China national stroke registry. Stroke. 2022;53(1):111–119. doi:10.1161/STROKEAHA.121.034366
44. Zielińska-Nowak E, Cichon N, Saluk-Bijak J, et al. Nutritional supplements and neuroprotective diets and their potential clinical significance in post-stroke rehabilitation. Nutrients. 2021;13(8):2704. doi:10.3390/nu13082704
45. Guo N, Zhu Y, Tian D, et al. Role of diet in stroke incidence: an umbrella review of meta-analyses of prospective observational studies. BMC Med. 2022;20(1):194. doi:10.1186/s12916-022-02381-6
46. Aquilani R, Scocchi M, Boschi F, et al. Effect of calorie-protein supplementation on the cognitive recovery of patients with subacute stroke. Nutr Neurosci. 2008;11(5):235–240. doi:10.1179/147683008X301586
47. Verhaar BJH, De Leeuw FA, Doorduijn AS, et al. Nutritional status and structural brain changes in Alzheimer’s disease: the nudad project. Alzheimers Dement. 2020;12:e12063.
48. He W, Ruan Y, Yuan C, et al. Hemoglobin, anemia, and poststroke cognitive impairment: a cohort study. Int J Geriatr Psychiatry. 2020;35(5):564–571. doi:10.1002/gps.5272
49. Xu M, Chen L, Hu Y, et al. The halp (hemoglobin, albumin, lymphocyte, and platelet) score is associated with early-onset post-stroke cognitive impairment. Neurol Sci. 2022;44(1):237–245.
50. Sapp DG, Cormier BM, Rockwood K, et al. The frailty index based on laboratory test data as a tool to investigate the impact of frailty on health outcomes: a systematic review and meta-analysis. Age Ageing. 2023;52(1). doi:10.1093/ageing/afac309
51. Blodgett JM, Theou O, Mitnitski A, et al. Associations between a laboratory frailty index and adverse health outcomes across age and sex. Aging Med. 2019;2(1):11–17. doi:10.1002/agm2.12055
52. Hubbard RE, Rockwood K. Frailty in older women. Maturitas. 2011;69(3):203–207. doi:10.1016/j.maturitas.2011.04.006
53. Bahat G, Tufan F, Bahat Z, et al. Observational cohort study on correlates of mortality in older community-dwelling outpatients: the value of functional assessment. Geriatr Gerontol Int. 2015;15(11):1219–1226. doi:10.1111/ggi.12422
54. Maraj M, Kuśnierz-Cabala B, Dumnicka P, et al. Malnutrition, inflammation, atherosclerosis syndrome (mia) and diet recommendations among end-stage renal disease patients treated with maintenance hemodialysis. Nutrients. 2018;10(1):69. doi:10.3390/nu10010069
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.