")
Back to Journals » Journal of Blood Medicine » Volume 14
Magnitude of Red Blood Cell Alloimmunization Among Pregnant Women Attending Antenatal Care at Wolaita Sodo University Comprehensive Specialized Hospital, Southwest Ethiopia
Authors Kebamo TE, Kombe AT, Eticha T , Arkew M , Bolado GN , Ayalew TL , Haile K , Walano GA
Received 23 October 2023
Accepted for publication 21 December 2023
Published 23 December 2023 Volume 2023:14 Pages 663—669
DOI https://doi.org/10.2147/JBM.S440952
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Tamirat Ersino Kebamo,1 Abinet Tantu Kombe,1 Temesgen Eticha,1 Mesay Arkew,2 Getachew Nigussie Bolado,3 Tadele Lankrew Ayalew,3 Kassahun Haile,4 Getachew Alemu Walano1
1School of Medical Laboratory Sciences, College of Health Sciences and Medicine, Wolaita Sodo University, Wolaita Sodo, Ethiopia; 2School of Medical Laboratory Sciences, College of Health and Medical Sciences, Haramaya University, Harar, Ethiopia; 3School of Nursing, College of Health Sciences and Medicine, Wolaita Sodo University, Wolaita Sodo, Ethiopia; 4School of Medical Laboratory Sciences, College of Medicine and Health Sciences, Wolkite University, Wolkite, Ethiopia
Correspondence: Tamirat Ersino Kebamo, School of Medical Laboratory Sciences, College of Health Sciences and Medicine, Wolaita Sodo University, P.O. Box: 138, Wolaita Sodo, Ethiopia, Tel +251919675172, Email [email protected]
Background: Maternal red cell alloimmunization occurs when a woman’s immune system becomes sensitive to unfamiliar red blood cell antigens. This leads to the production of alloantibodies, which can have serious implications for the fetus and newborn. However, there is a lack of comprehensive information about the extent of red cell alloimmunization in underdeveloped countries like Ethiopia. Therefore, this study aimed to determine the magnitude of red cell alloimmunization among pregnant women attending antenatal care at Wolaita Sodo University Comprehensive Specialized Hospital from September 01 to November 30, 2022.
Methods: In this institutional-based cross-sectional study, 422 pregnant women were participated and recruited using a systematic random sampling technique. Data on sociodemographic characteristics, obstetric history, and other clinical information were collected using structured questionnaires through face-to-face interview. Blood grouping and indirect antihuman globulin tests were performed. The relationship between red cell alloimmunization and the independent variables was determined using the chi-square test. P-value < 0.05 was considered statistical significance.
Results: In this study, the blood group distributions among the participants were as follows: O, 177 (41.9%); A, 124 (29.4%); B, 76 (18%); and AB, 45 (3.86%). Among the pregnant women included in the study, a total of 51 (12.08%) were identified as RhD-negative. Out of these RhD-negative women, 5 (9.8%) were found to have developed alloimmunization with red blood cell antigens. Miscarriage and post-partum hemorrhage were found to be important factors associated with the occurrence of red cell alloimmunization in these women.
Conclusion: This study showed that one out of ten pregnant women was alloimmunized. Therefore, antenatal blood grouping and indirect antihuman globulin screening should be performed routinely to manage and minimize the undesirable outcomes of alloimmunization during pregnancy.
Keywords: alloimmunization, pregnant women, indirect antihuman globulin test
Introduction
Alloimmunization occurs when the immune system reacts to foreign antigens after being exposed to cells or tissues with different genetic characteristics. This immune response can happen during pregnancy or in individuals who receive frequent blood transfusions, such as those with hemoglobinopathies, myelodysplastic syndromes, chronic renal disease, and other medical conditions. Alloimmunization can be triggered by various factors, including human white blood cell antigens and red blood cell antigens.1 Red blood cell alloimmunization among pregnant women range from 0.4% to 2.7% globally.2–4
The most clinically relevant blood group antigen present on the surface of red blood cells is still the ABO and Rhesus (Rh) blood group system.5 Rh alloimmunization happens when the immune system of the mother becomes sensitive to the RhD erythrocyte surface antigens, but it also refers to sensitization to other Rh antigens, including c, C, E and e.6 Alloimmunization, a process that produces a template for the production of antibodies as well as small amounts of antibodies against the RhD antigen, can occur in a mother who is D-negative when fetal D-positive cells are present in her circulation.2,7
Although it can happen at any point in a pregnancy, the third trimester and labour are when it happens most frequently. It can occur after pregnancy-related occurrences that are linked to fetomaternal hemorrhage, such as terminations, late miscarriages, antepartum hemorrhage, abdominal trauma, ectopic pregnancy, intrauterine death, and stillbirth. These events include chorionic villus sampling, amniocentesis, and external cephalic version.7
When a woman’s immune system becomes sensitive to unfamiliar red blood cell antigens, which results in the production of alloantibodies, these antibodies develop as a result of the immunological reaction to the initial exposure to the same antigen after a prior transplant, transfusion, or pregnancy. During birth or other trauma, newborn or fetal red cells in pregnant women enter the maternal circulation and lead to maternal red cell alloimmunization. If the fetus is positive for the relevant red blood cell surface antigens, the resultant antibodies frequently cross the placenta during subsequent pregnancies from sensitized women to the fetus, causing hemolysis of fetal red blood cells and anemia.8,9
All pregnant women should be typed and screened to assess alloantibodies and for any unexpected RBC antibodies using indirect antiglobulin test is recommended for all pregnant women.10 The detection of Rh alloantibodies in pregnant women who are RhD-negative is crucial for predicting and treating hemolytic disease among newborns in resource limited nations.11 However, there is currently inadequate prevention of alloimmunization following potentially sensitizing events and during medical termination of pregnancy in RhD-negative women. One of the reasons for this is the lack of sufficient data and information management regarding prior pregnancies. Additionally, crucial details regarding pregnancy termination are often missing from patients’ medical records.7 Although various studies have been conducted throughout the world, there was a paucity of information on alloimmunization in our setting. Thus, this study aimed to assess the magnitude of red cell alloimmunization among pregnant women receiving antenatal care at Wolaita Sodo University Comprehensive Specialized Hospital.
Methods and Materials
Study Design, Period and Area
This institutional-based cross-sectional study was conducted from September 01 to November 30, 2022, at the Comprehensive Specialized Hospital of Wolaita Sodo University. The Hospital is located in Southern nations’ nationalities and populations away from 328 km from Addis Ababa, Ethiopia. The altitude of the town is 1200–2950 m above the sea level.
Data Collection and Laboratory Methods
Study Participants who had communication problems, mental health issues, or were taking anti-D prophylaxis were excluded from the study. During the study period, all voluntarily pregnant women who attended prenatal care clinics were included. After obtaining written informed consent, data on sociodemographic characteristics, obstetric history, and other clinical information were collected through interviews with participants using structured questionnaires.
The test tube method was used to determine the study participants’ ABO and Rh blood type using ABO and monoclonal IgM anti-D reagents. Blood samples collected from the study participants were washed four times with normal saline, and a 5% red cell suspension was prepared. Cell suspension mixed with known antiserum in a test tube; the mixture is incubated at room temperature and centrifuged. Finally, agglutination was observed both macroscopically and microscopically.12 To detect alloimmunization, an indirect antihuman globulin test was performed.13 Serum from each participant was mixed with 5% red blood cell suspension prepared from known O-positive individuals. Agglutination was then seen after the mixture was centrifuged for 1 minute at 3000 revolutions per minute (RPM). The mixture was incubated at 37 OC for 30 minutes if it did not agglutinate. After incubation, the samples were again centrifuged and checked for agglutination. If agglutination was not observed, the mixture was washed with normal saline four 4 times, and antihuman globulin reagent was added after completely discarding the last wash supernatant, followed by centrifugation for 1 min at 3000 RPM. Results were observed macroscopically and microscopically. Coombs control cells were added to all agglutination-negative samples to confirm the true negativity.
Data Management and Quality Assurance
All quality assurance programs were taken to ensure data quality. For accuracy and consistency, the questionnaire’s English translation was made into the native tongue of Wolayitsa, then back into English. Before beginning the actual data collection, the questionnaire was pretested and the data collectors received training. The collection, handling, processing, and storage of samples were all done in accordance with standard operating procedures (SOP). Known ABO and Rh blood groups were utilized to test the ABO and Rh blood grouping reagents, and Coomb’s control cells were employed to control the indirect antihuman globulin test quality.
Data Analysis and Interpretation
The data were checked for completeness and its consistency. Then, data were entered into Epidata version 3.1 (Epidata Association, Odense, Denmark) and then exported to the Statistical Package for Social Sciences (SPSS) version 25 software (IBM Corporation, USA) for analysis. To ascertain the frequency and percentage of the variables, categorical data were analyzed using the chi-square test to see if red cell alloimmunization was associated with the independent factors. P-value <0.05 was considered statistical significance.
Ethical Consideration
This study was carried out according to the Declaration of Helsinki. Ethical clearance was obtained from the Ethical Review Committee of Wolaita Sodo University, College of Health Science and Medicine (reference number: CSHM/ER/01/15). A support letter from the Chief Research and Community Service Director Office of the College was submitted to Wolaita Sodo University Comprehensive Specialized Hospital and written permission was obtained. Written informed consent was obtained from each study participant after explaining the objective and procedures of the study. For participants below 18 years old, assent was obtained from the participant, and consent was signed by their husband or parents. The study participants were identified by codes rather than individual name or identifiers to maintain data confidentiality, and unauthorized individuals were unable to access the collected data. Antihuman globulin test positive results were sent to physicians working in antenatal care clinics for proper management.
Results
Socio-Demographic Characteristics of Study Participants
Data were collected from 422 participants with a 100% response rate. In age distribution, 194 (46%) respondents were aged 16–25 years. Concerning participants’ religions, 294 (69.7%) respondents were protestant religious followers. Regarding educational level, most of participants attended preparatory and above educational levels. Looking at the residence status of all participants, 230 (54.5%) were from urban areas, as shown in (Table 1).
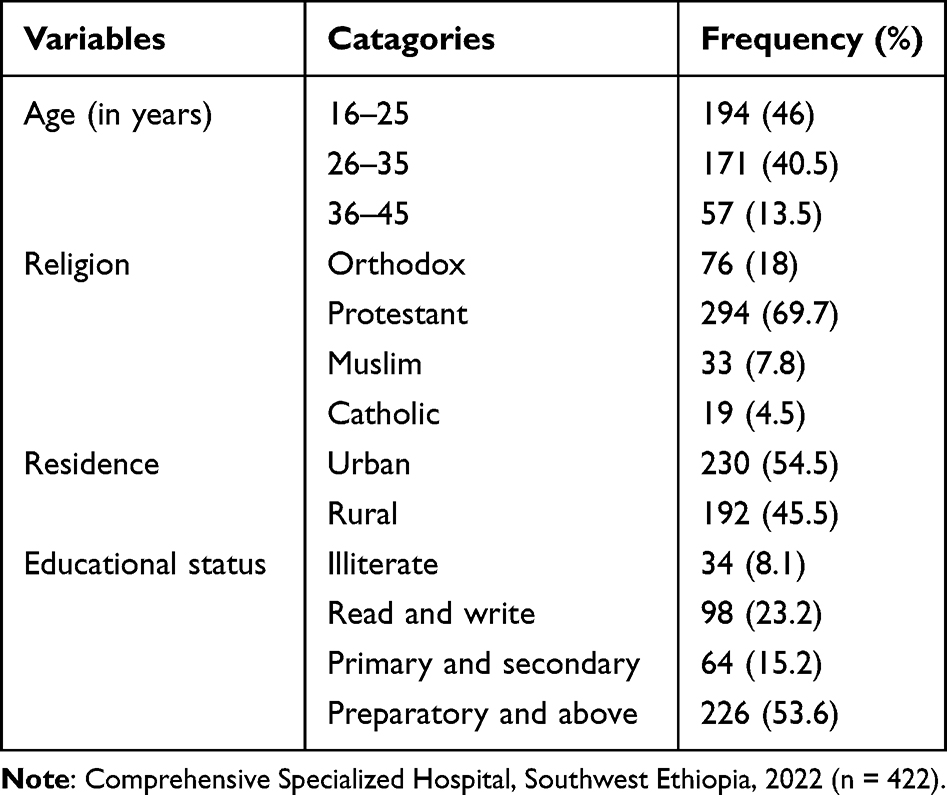 |
Table 1 Socio-Demographic Characteristics of the Study Participants in Wolaita Sodo University |
Obstetric and Clinical Characteristics of Study Participants
Regarding obstetric history, 47 women (11.1%) had a history of post-partum hemorrhage. Regarding pregnancy complications, 44 (10.4%) of the study participants had history of malaria infection and 49 (11.6%) had a reported history of bleeding. In addition, 361 (85.5%) pregnant women had no history of blood transfusion. Concerning previous history of abortion/miscarriage among the pregnant women, 44 (10.4%) had a history of abortion/miscarriage. Most gestational age of participants, 217 (51.5%) were in their third trimester, while 51 (12.1%) were in their first trimester of pregnancy. A total of 223 (64.8%) study participants responded that they had a history of health center delivery (Table 2).
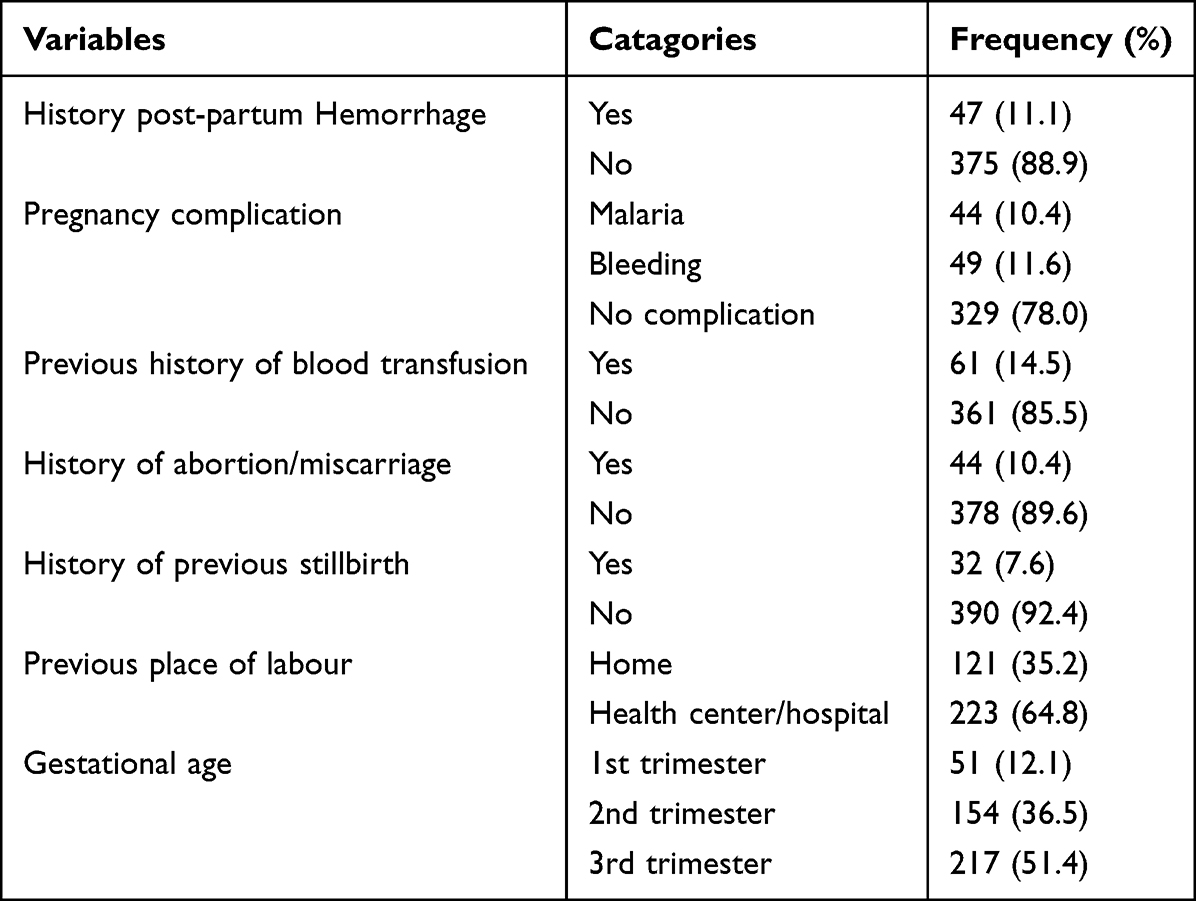 |
Table 2 Obstetric and Clinical Characteristics of Study Participants in Wolaita Sodo University Comprehensive Specialized Hospital, Southwest Ethiopia, 2022 (n = 422) |
Blood Group Distribution and Maternal Alloimmunization of the Study Participants
Regarding the blood group profile, among the total study participants, 177 (41.9%) were found to be blood group O, followed by 124 (29.4%), 76 (18%), and 45 (3.86%) with blood group A, B, and AB, respectively. From the total study participants, 51 (12.08%; 95 CI, 8.8–14.7) were RhD-negative, and 5 (9.8%; 95 CI, 0.2–2.1) were antihuman globulin (IAT) positive (Table 3).
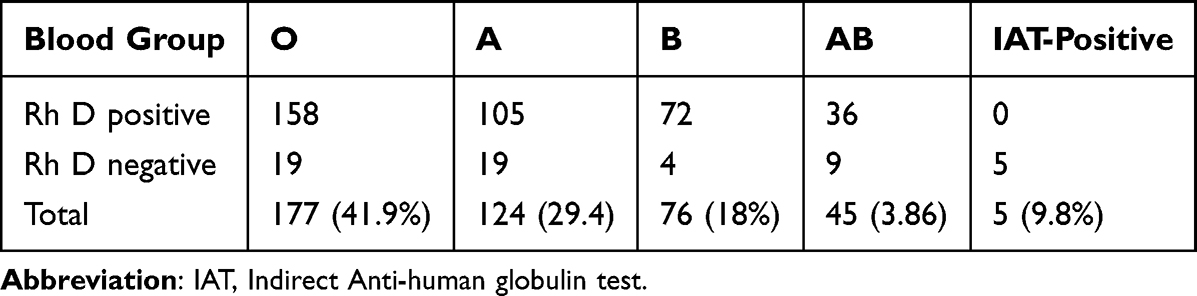 |
Table 3 Distribution of ABO, Rh Blood Groups and Alloimmunization Status Among the Pregnant Women at Wolaita Sodo University Comprehensive Specialized Hospital Southwest Ethiopia, 2022 (n = 422) |
Association Between Red Cell Alloimmunization and Other Variables
The variables associated with red cell alloimmunization among pregnant women that had been analyzed in this study included post-partum hemorrhage, blood transfusion, pregnancy complications, abortion/miscarriage, stillbirth, place of labor, and gestational age. Accordingly, the history of post-partum hemorrhage (p = 0001) and miscarriage (p = 0001) showed a statistically significant association with red cell alloimmunization. Other variables did not showed statistically a significantly associated with RBC alloimmunization (Table 4).
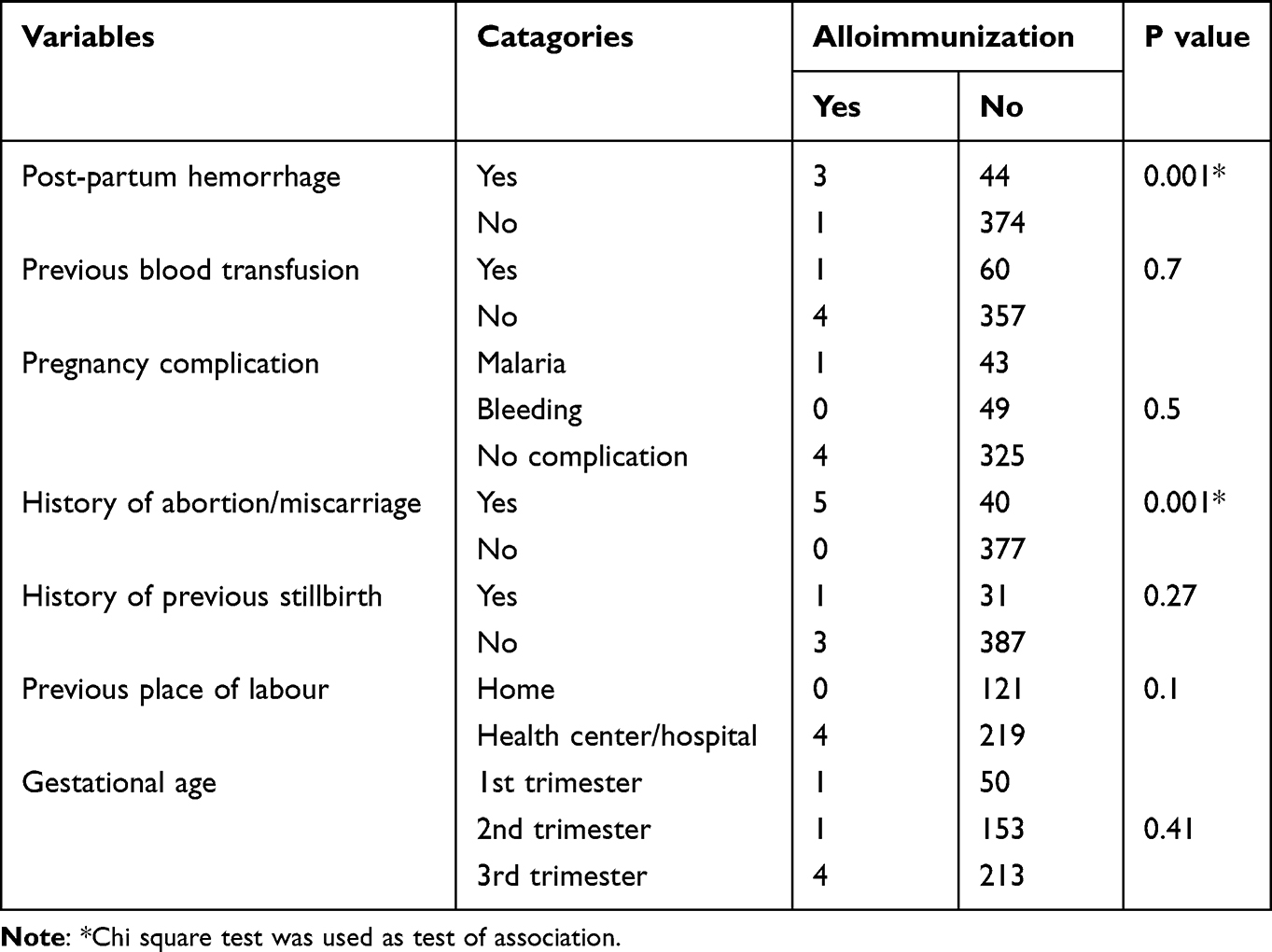 |
Table 4 Association Between Red Cell Alloimmunization and Variables at Wolaita Sodo University Comprehensive Specialized Hospital, Southwest Ethiopia, 2022 (n = 422) |
Discussion
The incidence of red cell alloimmunization is decreased in high socioeconomic countries; nonetheless, it is still an issues in sub-Saharan and poor socioeconomic countries like, Ethiopia.7 A crucial first step in minimizing pregnancy-related difficulties from RhD alloimmunization is studying the prevalence of RhD-negative women. Based on the obtained prevalence, this could help with the creation of screening and preventive management programs. The percentage of pregnant participants in our study who had RhD-negative blood was 12.08% (confidence interval 8.8–14.7). This is significantly higher than studies done in southwest and southeast Nigeria, which, respectively, found 5.5 and 4.5% of women of reproductive age with Rh D-negative factors.14,15 This difference might be due to variations in the ethnic or racial groups of the population. The current study differs from that of a study carried out in Gambella, Southwest Ethiopia, which found a Rh D-negativity rate of 19.37%.16 This indicates that the Rh D-negative distribution among pregnant women varied across Ethiopia. There is evidence that, in addition to regional, ethnic, and racial variations, the frequency of Rh D-negative individuals fluctuates over time within a single population in various parts of the same country.17
The overall prevalence of red cell alloimmunization in this study was 9.8% (confidence interval 0.2–2.2) which is consistent with a study done in Southwestern Uganda, which was 9.8%18 and study conducted in Oman, the Arabian Peninsula in southwestern Asia, reported 10% alloimmunization in pregnant women.19 In this study, the prevalence of alloimmunization was lower than that reported for Uganda (12.1%).20 This might be due to the relatively reduced sample size and differences in phenotype of population. Red cell alloimmunization in our study was much higher than previous reports from developed countries such as the Netherlands,21 Sweden22 and Southwest Saudi Arabia23 with 1.2%, 0.5%, and 1.8%, respectively. This gap might be brought about by racial variations resulting from the heterogeneity of various populations, and probably due to the routine antenatal use of anti-D prophylaxis.
Alloimmunization against RBC antigens may occur following blood transfusion, miscarriage, post-partum hemorrhage, stillbirth, place of labour, and pregnancy complications.20 However, in this study, miscarriage (p = 0.001) and post-partum hemorrhage (p = 0.001) were significantly associated with red cell alloimmunization. Other variables did not show any statistically significant differences. In contrast to the present study, there was a significant association between parity and place of labor with red cell alloimmunization, as reported by Jimma.24 This variation might be due to the differences in the relatively small sample sizes used in this study. No significant difference was observed in alloimmunization status across the three trimesters. This is possibly due to the unequal proportions of participants across the trimester groups and the relatively small sample size.
This study should be interpreted in the light of the following limitations: Firstly, it does not included the antibody identification panel of cells to resolve specificities of antibodies. Also, screening of autoantibody was not done due to resource constraints.
Conclusions and Recommendations
In our study population, the total prevalence of red cell alloimmunization was 9.8%, which is much higher than the prevalences recorded in European nations like the Netherlands, Sweden, and southern Arabia and slightly lower than those reported in African nations like Uganda. This variety is probably brought about by racial and genetic differences throughout the globe, sample sizes, and study methodologies. In this overall prevalence of D-negative women was 12.08%. Miscarriages/abortions and post-partum hemorrhage were significantly associated with red cell alloimmunization. Only pregnant patients who visited the hospital were included in our study, which does not accurately reflect the prevalence of anti-D among the many Ethiopian women who do not have access to obstetric care. It is important to look into additional population-specific antigens that may contribute to the significant amount of unidentified antibodies found in the current study.
Acknowledgment
We express our sincere gratitude to Wolaita Sodo University for ethical sanctions for this study. Moreover, we place on record our wholehearted thanks to the heads and staff of obstetrics and gynecology, neonatal care unit, and clinical laboratory staff, Wolaita Sodo University Comprehensive Specialized Hospital, and those who consented to participate in the study.
Author Contributions
All authors contributed to the work that was in the ideation, study design, execution, data collection, analysis, and interpretation processes as well as in the writing, and editing of the manuscript. All authors have agreed on the approval of the final manuscript to be published in the current journal and to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors affirm that they have no conflict of interest for this work.
References
1. Mota MA. Red cell and human leukocyte antigen alloimmunization in candidates for renal transplantation: a reality.. Rev Bras Hematol Hemoter. 2013;35(3):160–161. doi:10.5581/1516-8484.20130046
2. Ngoma AM, Mutombo PB, Ikeda K, et al. Red blood cell alloimmunization in transfused patients in sub-Saharan Africa: a systematic review and meta-analysis. Transfus Apheresis Sci. 2016;54(2):296–302. doi:10.1016/j.transci.2015.10.017
3. Pahuja S, Gupta SK, Jain M, Pujani M. The prevalence of irregular erythrocyte antibodies among antenatal women in Delhi. Blood Transfus. 2011;9(4):388. doi:10.2450/2011.0050-10
4. Gothwal M, Singh P, Bajpayee A, et al. Red cell alloimmunization in pregnancy: a study from a premier tertiary care centre of Western India. Obstet Gynecol Sci. 2023;66(2):84–93. doi:10.5468/ogs.22190
5. Cheesbrough MJUK. District Laboratory Practice in Tropical Countries, Part 1.
6. Duplantie J, Gonzales OM, Bois A, et al. Cost-effectiveness of the management of rh-negative pregnant women. Obstet Gynaecol. 2013;35(8):730–740.
7. Osaro E, Charles AT. Rh isoimmunization in Sub-Saharan Africa indicates need for universal access to anti-RhD immunoglobulin and effective management of D-negative pregnancies. Int J Women’s Health. 2010;429–437. doi:10.2147/IJWH.S15165
8. Altuntas N, Yenicesu İ, Himmetoglu Ö, et al. The risk assessment study for hemolytic disease of the fetus and newborn in a University Hospital in Turkey. Transfus Apheresis Sci. 2013;48(3):377–380. doi:10.1016/j.transci.2013.04.021
9. Bricca P, Guinchard E, Bliem C. Management of feto-maternal red cell allo-immunizations. Transfus Clin Bio. 2011;18(2):269–276. doi:10.1016/j.tracli.2011.01.005
10. Urbaniak S, Greiss M. RhD haemolytic disease of the fetus and the newborn. Blood Rev. 2000;14(1):44–61. doi:10.1054/blre.1999.0123
11. Jennifer W, Meghan D. Red Blood Cell Alloimmunization in the pregnant patient. Transfus Med Rev. 2018;32(4):213–219. doi:10.1016/j.tmrv.2018.07.002
12. Liu KL, Li N, Li BJ, Peng JY, Shu XW, Yu YY. Clinical significance of anti-D IgG screening and titer detection in 286 RhD negative pregnant women. Chinese J Contemp Pediatr. 2009;11(3):185–187.
13. Gupta A, Mirza S, Khurana S, et al. Enigmatic weak D antigen: an experience in a Tertiary Care Hospital of East Delhi. J Clin Diagn Res. 2016;10(6):EC12–EC15. doi:10.7860/JCDR/2016/16278.7972
14. Samson A, Hajara B, Health P. Prevalence of Rhesus D-negative blood type and the challenges of Rhesus D immunoprophylaxis among obstetric population in Ogbomoso, Southwestern Nigeria. Ann Trop Med Public Health. 2016;9(1):1–5.
15. Okeke T, Ocheni S, Nwagha U, et al. The prevalence of Rhesus negativity among pregnant women in Enugu, Southeast Nigeria. Niger J Clin Pract. 2012;15(4):400–402.
16. Golassa L, Tsegaye A, Erko B, et al. High rhesus (Rh (D)) negative frequency and ethnic-group based ABO blood group distribution in Ethiopia. BMC Res Notes. 2017;10(1):1–5. doi:10.1186/s13104-017-2644-3
17. Pourfathollah A, Oody A, Honarkaran N. Geographical distribution of ABO and Rh (D) blood groups among Iranian blood donors in the year 1361 (1982) as compared with that of the year 1380 (2001). Sci J Iran Blood Transfus Organ. 2004;1(1):11–17.
18. Mbalibulha Y, Natukunda B, Okwi AL, et al. Alloimmunization to Rh Antigen (D, C, E, C, E) among pregnant women attending antenatal care in South Western Uganda. J Blood Med. 2022;Volume 13:747–752. doi:10.2147/JBM.S385737
19. Al-Dughaishi T, Al Harrasi Y, Al-Duhli M, et al. Red cell alloimmunization to Rhesus antigen among pregnant women attending a tertiary care hospital in Oman. Oman Med Journal. 2016;31(1):77. doi:10.5001/omj.2016.15
20. Mbalibulha Y, Muwanguzi E, Mugyenyi GR, et al. Occurrence of anti-D alloantibodies among pregnant women in Kasese District, Western Uganda. J Blood Med;2015. 125–129. doi:10.2147/JBM.S80977
21. Koelewijn J, de Haas M, Vrijkotte T, et al. Gynaecology. Risk factors for RhD immunisation despite antenatal and postnatal anti‐D prophylaxis. Int J Obstetr Gynaecol. 2009;116(10):1307–1314. doi:10.1111/j.1471-0528.2009.02244.x
22. Filbey D, Hanson U, Wesström G. The prevalence of red cell antibodies in pregnancy correlated to the outcome of the newborn: a 12 year study in central Sweden. AGOS. 1995;74(9):687–692.
23. Sarhan MA, Saleh KA, Bin-Dajem S. Distribution of ABO blood groups and rhesus factor in Southwest Saudi Arabia. Saudi Med J. 2009;30(1):116–119.
24. Nair SP, Segni H, Kassim M. Maternal alloantibodies and foetal complications in Jimma specialized hospital, South-Western Ethiopia. World J Pharm Res. 2016;5(2):1130–1140.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.