")
Back to Journals » Clinical Interventions in Aging » Volume 17
Major Lower Limb Amputations and Amputees in an Aging Population in Southwest Finland 2007–2017
Authors Koivunen V, Dabravolskaite V, Nikulainen V, Juonala M, Helmiö P, Hakovirta H
Received 8 February 2022
Accepted for publication 19 May 2022
Published 8 June 2022 Volume 2022:17 Pages 925—936
DOI https://doi.org/10.2147/CIA.S361547
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Veerakaisa Koivunen,1 Vaiva Dabravolskaite,1,2 Veikko Nikulainen,1,2 Markus Juonala,1,3 Päivi Helmiö,1,2 Harri Hakovirta1,2,4
1University of Turku, Faculty of Medicine, Turku, 20521, Finland; 2Department of Vascular Surgery, Turku University Hospital, Turku, 20521, Finland; 3Department of Internal Medicine, Division of Medicine, Turku University Hospital, Turku, 20521, Finland; 4Department of Surgery, Satasairaala, Pori, 28500, Finland
Correspondence: Harri Hakovirta, Turku University, Kiinanmyllynkatu 4-8, Turku, 20520, Finland, Tel +358 40 5918811, Email [email protected]
Purpose: The aim of the present study was to describe and analyze changes in the incidences of lower extremity amputations (LEAs), patient characteristics, vascular history of amputees and survival in Southwest Finland.
Patients and Methods: This is a retrospective patient study in the Hospital District of Southwest Finland. All consecutive patients with atherosclerosis and diabetes-caused LEA, between 1st January 2007 and 31st December 2017, were included. The annual incidences of major LEA patients were statistically standardized. Patients’ diagnoses, functional status, previous revascularizations and minor amputations were recorded, and survival was analyzed.
Results: During the 11-year-period major LEAs were performed on 891 patients, 118 (13.2%) were urgent operations. The overall incidence of major LEA was 17.2/100 000 and was age-dependent (3.1 for ≤ 64 years, 34.3 for 65– 74 years, 81.5 for 75– 84 years, 216 for ≥ 85 years). A decrease in incidence was detected in the < 65 year-age-group (incidence 4.98 in 2007 and 1.88 in 2017; p = 0.0018). Among older age groups, there was no significant change. Half (50.6%) of all amputees were diabetics. Altogether, 472 patients (53.0%) had a history of revascularization before LEA. 80.1% of index amputations were transfemoral and 19.9% transtibial. Re-surgery was performed on 94 (10.5%) patients. The 1-, 3- and 5-year overall survival were 56%, 30%, and 18%, respectively.
Conclusion: Our results suggest that in an aging population, despite good availability of vascular services, a significant number of patients are not fit for active revascularization, and LEA is the only feasible treatment for critical limb ischemia.
Keywords: aging, major amputation, diabetes, peripheral artery disease
Introduction
Peripheral artery disease (PAD) is the most common cause of major lower extremity amputation (LEA).1,2 The prevalence of PAD increases with age and exposure to major cardiovascular risk factors, such as diabetes mellitus (DM), dyslipidemia, smoking, and hypertension.2,3 The disease may progress to critical limb threatening ischemia (CLTI), which is the end stage of PAD and which is associated with the poorest outcome and a significant risk of major LEA.4
According to a recent review by Beckman et al, the incidence of major LEA is directly proportional to the rates of PAD, DM-related soft tissue infection and neuropathy.3 Patients with DM were shown to have a nearly 13-fold greater risk of undergoing major LEA compared to patients without diabetes.3 In addition, aging is a significant risk factor associated with elevated risk of major LEA.5
The LEA carries a significant impact on an amputee’s functional abilities and quality of life. The current European Society for Vascular Surgery (ESVS) guidelines recommend active revascularization to prevent LEAs.2 The number of revascularizations performed has increased during recent years. For example, in Finland, the yearly rate of revascularizations nearly tripled from 66/100,000 to 172/100,000 from 2007 to 2017.5 Furthermore, a shift from open surgical revascularization (OSR) towards an endovascular strategy has occurred over recent decades.6–9
Despite increasing numbers of revascularizations, the incidence of major LEA has not considerably diminished. According to the VASCUNET report, the LEA incidence slightly decreased from 18.9/100,000 to 17.7/100,000, during 2010–2014.8 An earlier report by Winell et al10 has demonstrated a decreasing amputation trend among diabetic patients between 1997 and 2007. In Finland, the major LEA incidence from 2007 to 2018 remained stable.5,11
The burden of atherosclerosis, on lower extremities, is also associated with increasing age. Simultaneously, the risks of multiple comorbidities and increasing frailty increase. Decision-making between high-risk revascularization and primary LEA is demanding. The only option for a patient unfit for surgery with severe ischemic rest pain or a severely infected wound or gangrene is often LEA.
The aim of the present study is to analyze the changes in major LEA incidence in Southwest Finland between 2007 and 2017 and to describe the characteristics and survival of amputees with a focus on their earlier vascular history.
Materials and Methods
Study Design
This is a retrospective patient records study.
Patients
The present study includes all patients with a diagnosis of PAD and/or DM with major LEA in the Hospital District of Southwest Finland between 1st January 2007 and 31st December 2017.
The Structure of Vascular Surgery Services in the Area
The Hospital District of Southwest Finland comprises Turku University Hospital and three other regional hospitals, Salo, Loimaa, and Uusikaupunki hospitals. The catchment area of all four hospitals serves a population of 480,626 inhabitants (2017).
In 2004, a vascular surgery unit was established to serve the area of the Hospital District of Southwest Finland. A vascular surgeon in Turku University Hospital investigated individual patients that present signs of vascular insufficiency. A treatment strategy for each patient was devised based on the vascular status and the overall condition of the patient. Before the decision for major LEA, a consultation with a vascular surgeon is recommended and is usually done. Revascularizations have been performed solely at Turku University Hospital since 2004, whereas major LEAs were performed in all four hospitals of the hospital district. Although vascular surgeons had a central role in decision-making, operating surgeons were vascular surgeons, general surgeons and plastic surgeons of the hospital district.
Data Collection
Data were collected from the Hospital District of Southwest Finland electronic patient registry, which covers all operation and patient records of all four hospitals in the hospital region. Operations were recorded in the operation database according to the Finnish version of NCSP (Nordic Classification of Surgical Procedures) and diagnoses according to the Finnish version of the ICD-10 (International Statistical Classification of Diseases and Related Health Problems) classification system.
The inclusion criteria for the study were a major LEA, either an above-knee amputation (AKA) (operation codes NFQ10 and NFQ20) or below-knee amputation (BKA) (codes NGQ10, NGQ20) together with a diagnosis of PAD (I70.2) and/or DM (E10.0–E11.9).
The day of the major LEA was considered as the index date for the study. If more than one major LEA (for example BKA+AKA) was performed on the ipsilateral leg of the patient or an LEA was performed on both limbs, the first major LEA was considered as an index operation and entry to the study. Patient records were followed-up until 28th March 2018. This date was considered the end of the study.
Variables
Patients’ comorbidities were recorded according to the following ICD-10 coded comorbidities; coronary artery disease (I20.0–9), chronic heart failure (I50.9), hypertension (I10.0–9), atrial fibrillation (I48.0–9), DM (E10.0–E11.9), chronic obstructive pulmonary disease (J44.8), dyslipidemia (E78.0) and chronic kidney disease (N18.9) and the possible use of anticoagulants, antithrombotic agents and statins were recorded. Moreover, the previous surgical or endovascular revascularizations and minor (metatarsal and toe) amputations, in addition to reoperations (re-amputations and revisions) after index LEA and date of death, were recorded.
Statistical Analyses
Major LEA patients were grouped into four age groups of 0–64, 65–74, 75–84, and >85 years of age. The annual incidence of major LEA patients was statistically standardized by conventional methods using the annual population size and age structure of the area according to Official Statistics of Finland (OSF).12 P-values were calculated using the Mann-Kendall trend test.
Patient characteristics were given as continuous variables and were expressed as mean ± either standard deviation (SD) or standard error (SE). Categorical variables were expressed as frequencies and percentages.
Fisher’s Exact test and Kruskal–Wallis test were utilized for categorical variables, whereas the ANOVA followed by Student’s t-test was utilized for continuous variables if normally distributed. Normal distribution was assessed using the Shapiro–Wilk test. Kaplan–Meier survival analyses were assessed by Log-rank statistics. A model for cox regression analyses was created. Variables with p < 0.2 in univariate analyses were included into the final model.
Statistical analyses were performed using the IBM SPSS ® version 27 statistics program for most analyses. Additionally, the R-program and the package “Kendall” were used for Mann-Kendall trend testing.13 The statistical significance threshold was set at 0.05.
Ethical Considerations
The study protocol was approved by the local Ethics Committee of the Hospital District of Southwest Finland (Decision number TO3/022/16). Due to the retrospective nature of the study, patient written informed consent was not required. All accessed data comply with data protection and privacy regulations set by the European Community (general data protection regulations, GDPR).
Results
Incidences of Index LEAs
A total of 891 major LEAs were performed on 891 patients between 2007 and 2017 inclusive. The overall incidence of LEA was 17.2/100,000. The annual variation of incidence ranged from 14.8 to 19.3/100,000 over the 11-year study period.
The mean major LEA incidence was age-dependent (3.1/100 000 for 0–64 years, 34.3/100,000 for 65–74 years, 81.5/100,000 for 75–84 years, 216/100,000 for ≥85 years). In the age group ≤64 years, major LEA incidence decreased over the study period (p = 0.0018). In the other age groups, no significant trends were observed. The annual incidences of major LEA by age group are presented in Table 1 and the size of the population in the hospital administration area at defined age categories in Figure 1A and B.
 |
Table 1 The Age Standardized Annual Incidences of Index LEAs per 100,000 Inhabitants in the Hospital District of Southwest Finland Over 2007–2017 |
 |
Figure 1 The annual population and age structure in the Hospital district of Southwest Finland 2007–2017 according to Official Statistics of Finland.12 Panel (A) total population and population aged ≤64 years. Panel (B) Population 65–74 years, 75–84 years and ≥85 years old. |
Patients
Among the 891 patients, 454 (51.0%) were men. The mean age of the patients was 77.4 years (SD 1.9). Most of the patients had multiple comorbidities. The most common comorbidity was hypertension (65.1%) and half (50.6%) of the patients had DM. The prevalence of diabetes was age dependent (patients ≤64 years 72.9%, 65–74 years 63.7%, 75–84 years 48.6% and ≥85 years 34.1%) p < 0.001. Of all patients, 406 (45.6%) were on antithrombotic medication and 400 (44.9%) were anticoagulated. Moreover, 374 patients (32.0%) were using statins. The patient characteristics for cohort are presented in Table 2 and age-dependent characteristics in Table 3.
 |
Table 2 Demographic Characteristics of 891 Patients with Major LEAs in the Hospital District of Southwest Finland 2007–2017 |
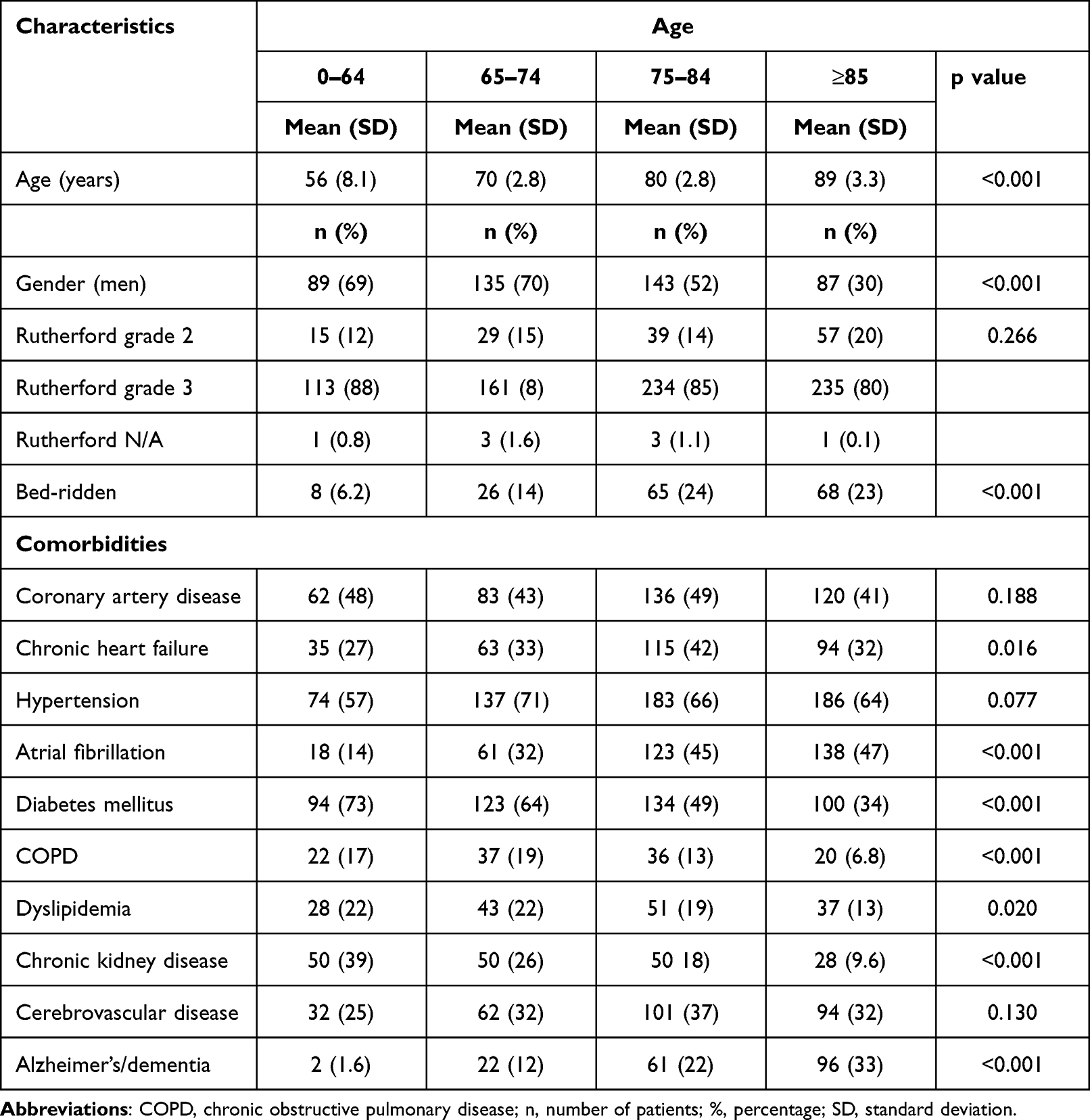 |
Table 3 Age-Dependent Demographic Characteristics of 891 Patients with Major LEAs in the Hospital District of Southwest Finland 2007–2017 |
Amputations
Prior to 891 index major LEAs, minor amputations had been performed on 300 (33.7%) legs. Of all index LEAs, 118 (13.2%) were performed urgently due to severe infection. In 80.1% of cases, the primary major LEA level was AKA and 19.9% BKA. Adjunct procedures were performed for 94 (10.5%) patients after index amputation, 71.3% of these re-operations were needed after BKA (Table 4.).
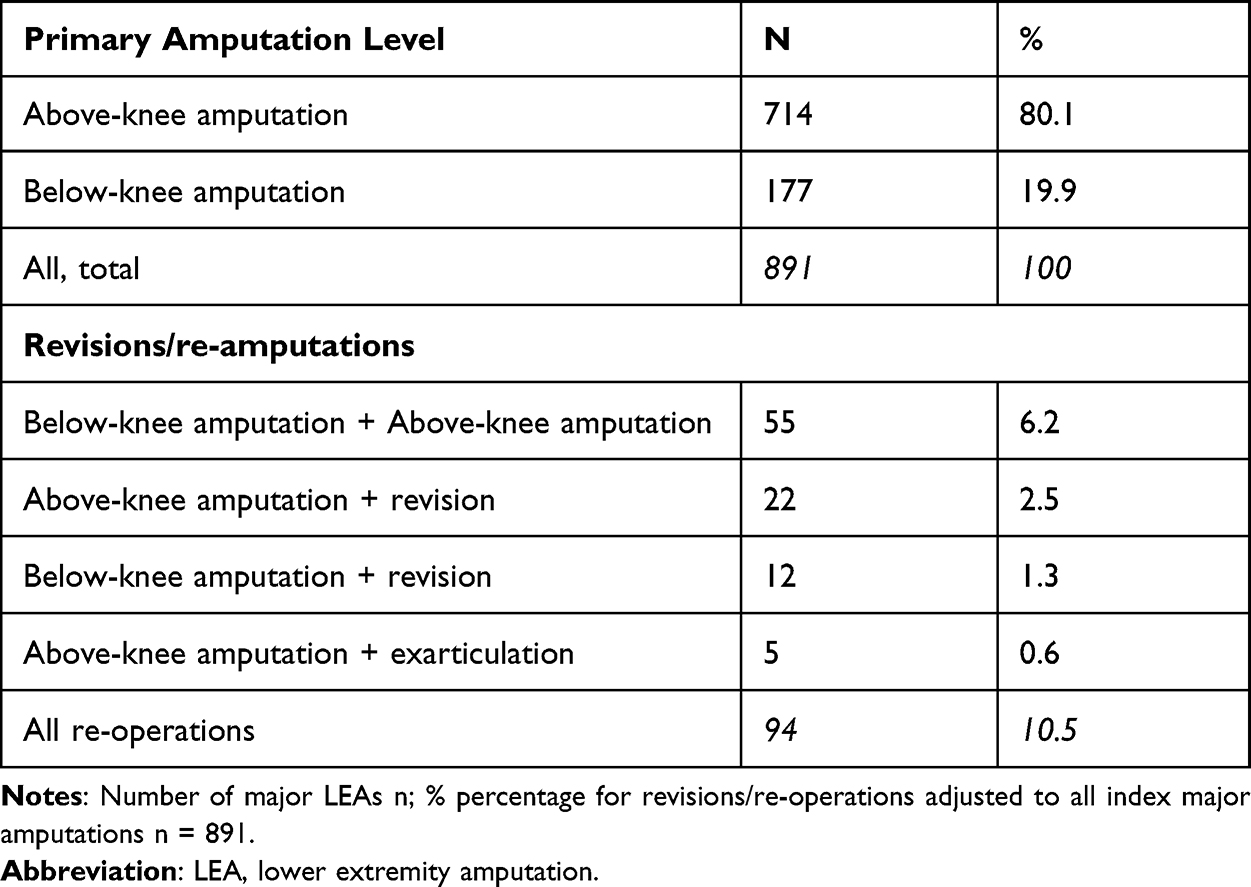 |
Table 4 The Primary Level of Amputation and Numbers of Revisions and Re-Operations Needed After 891 Major LEAs in the Hospital District of Southwest Finland 2007–2017 |
Revascularizations Prior to Major LEAs
Prior to the index major LEAs, 764 revascularization procedures on amputated limbs were performed on 472 patients (53.0%). Of these procedures, 360 were surgical (47.1%) and 404 (52.9%) were endovascular. The mean time from revascularization to major LEA was 26.8 months (CI 95% 22.4–31.3) for open revascularization. Correspondingly, the mean time from endovascular revascularization to major LEA was 33.2 months (CI 95% 28.7–37.7).
The patient history of revascularization procedures before major LEA was age dependent. Earlier revascularizations are shown in Figure 2 and were more common in the younger age groups (patients ≤64 years 58.1%, 65–74 years 62.7%, 75–84 years 51.1% and ≥85 years 46.1%). The mean age of the patients with a history of revascularization was 76.2 years (SD 11.5) and without a history of revascularization 78.6 years (SD 12.2) (p = 0.002). Even though patients with no history of revascularization were older, they still had fewer comorbidity diagnoses than patients with previous revascularization. A comparison of patient characteristics by prior revascularization of is presented in Table 5.
 |
Table 5 Comparisons of the Major LEA Patients, Based on History of Revascularization Before the Index Amputation in the Hospital District of Southwest Finland 2007–2017 |
 |
Figure 2 History of revascularizations before major LEA of 891 amputees at the index major LEA by age group in the Hospital District of Southwest Finland 2007–2017. NREV patients without history of revascularization before the major LEA; REV patients with history of revascularization before the major LEA. Abbreviation: N, number of patients. |
Survival
The follow-up time was 1.25–12 years. At the end of the study (28th March 2018) 78.1% of the cohort had died. The 1-, 3- and 5-year overall survival rates were 51.9%, 22.6%, and 10.1%, respectively.
Age and Survival After Amputation
Age-dependent 1-, 2- and 3-year survivals were 0–64; 62, 52 and 21%, 65–74; 46, 42 and 12% 75–84; 35, 26 and 6% and for patients ≥85 years 26, 15, 2%. Figure 3. A model for Cox regression analyses for survival was created. The following confounding factors were selected based on univariate analyses; coronary artery disease, atrial fibrillation, diabetes mellitus, chronic heart failure, dyslipidaemia, chronic kidney disease, Alzheimer’s disease or dementia and bed-ridden patients (p < 0.2). Age group <65 years as a reference the increased association with death was detected for patients 65–74 (HR 1.396; p = 0.018), 75–84 (HR 1.958; p < 0.001) and ≥85 years 2.621 (HR 2.621; p < 0.001).
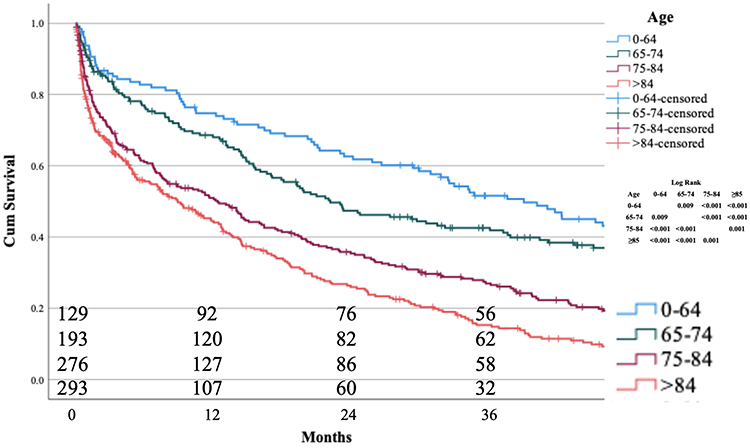 |
Figure 3 Age-dependent 3-year survival after the index major amputation. The number of patients entering each 12-month interval is indicated on horizontal axis. The Hospital District of Southwest Finland 2007–2017. |
In the Cox regression model, following confounding factors associated with increased risk of death; coronary artery disease (HR 1.184; p < 0.039), atrial fibrillation (HR 1.234; p = 0.012), chronic kidney disease (1.404; p = 0.001), Alzheimer’s disease or dementia (HR 1.296; p = 0.012) and bed-ridden patients (HR 1.385; p = 0.001).
Alzheimer’s Disease, Dementia, and Bed-Ridden Patients After Amputation
According univariate and multivariate analyses, Alzheimer’s disease and dementia were associated with an increased risk of death (HR1.3; 95% CI 1.06–1.59; p < 0.012) and the 1, 2 and 3-years survival was 29, 14 and 3%. Correspondingly the bed-ridden patients had increased risk of death (HR 1.4; 95% CI 1.14–1.69, p < 0.001) and corresponding 1,2 and 3-years survival 26, 13 and 3%.
Discussion
Over the 11-years study period, almost half of the amputees had no earlier history of revascularization before the major LEA, despite the high availability of vascular surgery services. Also, a high proportion of patients were bed-ridden or had burden of memory defect (Alzheimer’s disease or dementia). These age-related issues are associated especially with older age groups. This result might suggest that in an aging population, the ability of vascular services to save limbs from major LEA is limited, and a large proportion of end-stage PAD patients are not fit for active revascularization or are even bed-ridden for other causes. For these patients, only LEA can be considered as a feasible treatment for end-stage CLTI.
LEA Incidence
According to the VASCUNET report of 12 countries, which covered 259 million inhabitants in 2014, the major LEA incidence slightly decreased from 18.9 to 17.7/100 000 in patients with PAD diagnosis between 2010 and 2014.8 Nikulainen et al reported stable all-cause major LEA incidence of 18–20/100,000 for the whole of Finland between 2007 and 2017, although the major LEA incidence decreased in patients over 65 years old.5 The present study from Southwest Finland had covered 480,626 inhabitants by 2017. We found that the overall incidence of LEA was slightly smaller (17.2/100,000) than that reported by Nikulainen et al, and the incidence stayed constant over the 11-year period.
Age
Age has been shown to be a risk factor for major LEA.8,14 Aging is associated with severe tibial atherosclerosis, which is known to be associated with poor limb-related outcome and mortality compared to extensive atherosclerosis in other vascular beds.15,16 Additionally, elderly patients generally have poorer overall condition and are more likely to be frailer than younger patients, which is further associated with a poor outcome after revascularization.17
The present study found that a majority of the major LEAs were performed on the elderly. The high proportion of the aged population in our material contributed to the present results because since 2017 more than a fifth of the population in Southwest Finland have reached the age of 65 years and older. This is high even compared to countries in the VASCUNET report.8 The present data agree with some previous studies, which found that a continuously growing proportion of elderly in a population is a strong predisposing factor to an increasing incidence of major LEA.14,18
Diabetes
Another predisposing factor for major LEA incidence is the high prevalence of DM in Finland.19 According to the present study, diabetes was a significant co-morbidity and comprised nearly half of the major LEAs. Similar to age, DM is a known risk factor for limb loss as diabetics are associated with extensive tibial lesions with the worst prognosis after revascularization.3,20
The spectrum of PAD in patients with DM is rather wide and ranges from non-healing wounds with underlying osteomyelitis to severely infected wounds that lead to septic shock.3 Therefore, the incidence of major LEA is not directly proportional to the rates of revascularizations as not all patients have significant limb threatening ischemia. Moreover, a three-fold higher risk of amputation has been reported in patients with diabetic foot syndrome without PAD compared to patients with only PAD.21
A decrease in major LEA incidence (13.6–9.3/100,000) has been observed among diabetics in Finland 1997–2007.10 We found that the major LEA incidence was significantly reduced among the <65-year-old population during the 11-year study period, although 72% of amputees in this age group were diabetics. This study could not fully investigate the exact cause of this positive trend. However, we know that revascularization procedures have been actively performed on young diabetics to an increasing degree over the same study-period.
Functional Status
A recent study by Ponkilainen et al11 reported a constant transfemoral (16–17/100,000) and decreasing transtibial (14–7/100 000) all-cause major LEA incidence in Finland between 1997 and 2018. This observation was explained by the high proportion of aged and immobile patients with reduced functional ability who are often considered not to benefit from prosthesis rehabilitation.11 Transtibial amputation is preferred and recommended for all patients with walking ability and sufficient blood circulation at the tibial level.
The level of primary LEA in the present study was chosen at the discretion of the operating surgeon and was based on the vascular status and overall condition of the patient. Overall, 80.1% of index amputations were transfemoral, which indicates a high portion of immobile patients.
Revascularizations
Active revascularization of patients fit for revascularization is essential to prevent LEA. It is also known that previously revascularized patients who were eventually amputated had a relatively good mean amputation-free survival before amputation. Successful revascularization significantly improves the clinical outcome and lowers the risk for major LEA.22,23 This may be one explanation for the decrease in major LEA incidence of patients <65 years found in the present study.
Patients with CLTI have multiple comorbidities, and operation risks are elevated.24,25 Moreover, young CLTI patients have a high prevalence of DM, poor glycemic control, coronary artery disease, smoking, renal insufficiency, and high WIfI stage.26 On the other hand, non-ambulatory associated conditions such as a higher BMI are less common in younger CLTI patients compared to older age groups,26 which therefore enables an active revascularization strategy to be used. In addition to the adequate provision of vascular services, the implementation of risk factor modification, such as better foot care, and more physician education are all essential factors to decrease major LEA incidence among all patients.3
Previous studies suggest that extreme frailty and functional impairment are associated with increased risk for major LEA.17,27 Nearly half of the major LEA amputees are considered unfit for revascularization at the time of the presentation of CLTI.21,27 Primary major LEA is the option that should be considered for frail patients with reduced functional ability in preference to unmeaningful repetitive revascularizations, multiple minor amputations, and revisions.
A study by Abou-Zamzam et al28 demonstrated that increasing revascularization may not further lower the major LEA incidence due to high proportions of inoperable patients, the elderly, and diabetics. This finding is in accordance with the present results. The vascular surgery resources in the catchment area of the present study have been and still are sufficient to provide the revascularization for all patients fit for surgery. Even so, almost half of the amputees had no revascularization before having a major LEA.
Strengths and Limitations
This study is based on data obtained from a single health care district that covers a primary catchment area of 480,626 inhabitants (2017). Finland has a public national health care system, and an electronic patient record system covers the population, and therefore, all patients could be included for the study. Both strength and limitation are the retrospective nature of this study. The present data is based on the procedural data from the same database serving all four hospitals of the district. Due to the nature of retrospective study, the level of major LEA depended on the discretion of the vascular status and overall condition of the patient and not on the study protocol. Demographic information was obtained from patients’ medical records, thus there is a heavy reliance on accurate recording of the comorbidities. A prospective study would be warranted to reliably measure the frailty score of this cohort of patients with heavy burden of cardiovascular disease and aging. Unfortunately, this issue could not be reliably assessed in the present retrospective study.
The adequate provision of vascular services is essential to control the rates of major LEAs, but despite this major LEA often remains the only realistic treatment for a significant proportion of patients to reduce ischemic pain or eliminate severe wound infection.
Conclusions
The present study confirms that despite the adequate availability of vascular surgery services, only half of the patients had a history of revascularization before major LEA. A high proportion of major LEAs in an aging population are performed on elderly and diabetic patients, who would not be considered to benefit from vascular interventions. The aging of the population can be considered as an antagonistic factor for vascular services to achieve the aim of reducing the incidence of major LEA.
Abbreviations
PAD, peripheral artery disease; CLTI, chronic limb-threatening ischemia; LEA, lower extremity amputation; DM, diabetes mellitus; AKA, above knee amputation; BKA, below knee amputation.
Acknowledgments
The authors want to thank Alisdair McLean for reviewing and editing the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work has been supported by federal research grants from both Turku University Hospital and Satasairaala. The Suomen Kulttuurirahasto; Satakunta fund also financially supported the work; Grant number 75212239. Funders had no role in the study design, data collection and analysis, decision to publish, or preparation of the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Eskelinen E, Lepantalo M, Hietala EM, et al. Lower limb amputations in Southern Finland in 2000 and trends up to 2001. Eur J Vasc Endovasc Surg. 2004;27(2):193–200. doi:10.1016/j.ejvs.2003.10.011
2. Aboyans V, Ricco JB, Bartelink MEL, et al. Editor’s Choice – 2017 ESC guidelines on the diagnosis and treatment of peripheral arterial diseases, in collaboration with the European Society for Vascular Surgery (ESVS). Eur J Vasc Endovasc Surg. 2018;55(3):305–368. doi:10.1016/j.ejvs.2017.07.018
3. Beckman JA, Creager MA, Libby P. Diabetes and atherosclerosis: epidemiology, pathophysiology, and management. JAMA. 2002;287(19):2570–2581. doi:10.1001/jama.287.19.2570
4. Davies MG. Critical limb ischemia: introduction. Methodist Debakey Cardiovasc J. 2012;8(4):2. doi:10.14797/mdcj-8-4-2
5. Nikulainen V, Helmio P, Hakovirta H. Changes in rates of vascular procedure types and lower extremity amputations in Finland for 2007–2017 inclusive, a population cohort study of 69,523 revascularizations. Int J Surg. 2019;72:118–125. doi:10.1016/j.ijsu.2019.10.039
6. Bolibar I, Gich I, Angles A, Romero JM, Escudero JR. Variability of revascularization techniques among Catalan hospitals and impact on leg salvage in patients with peripheral arterial disease. Int Angiol. 2019;38(1):54–61. doi:10.23736/S0392-9590.18.04041-5
7. Garimella PS, Balakrishnan P, Correa A, et al. Nationwide trends in hospital outcomes and utilization after lower limb revascularization in patients on hemodialysis. JACC Cardiovasc Interv. 2017;10(20):2101–2110. doi:10.1016/j.jcin.2017.05.050
8. Behrendt CA, Sigvant B, Szeberin Z, et al. International variations in amputation practice: a VASCUNET report. Eur J Vasc Endovasc Surg. 2018;56(3):391–399. doi:10.1016/j.ejvs.2018.04.017
9. Hussain MA, Al-Omran M, Salata K, et al. Population-based secular trends in lower-extremity amputation for diabetes and peripheral artery disease. CMAJ. 2019;191(35):E955–E961. doi:10.1503/cmaj.190134
10. Winell K, Venermo M, Ikonen T, Sund R. Indicators for comparing the incidence of diabetic amputations: a nationwide population-based register study. Eur J Vasc Endovasc Surg. 2013;46(5):569–574. doi:10.1016/j.ejvs.2013.07.010
11. Ponkilainen VT, Vuorlaakso M, Kaartinen I, et al. The development of lower limb amputations in Finland from 1997 to 2018: a nationwide retrospective registry study. Eur J Vasc Endovasc Surg. 2021;63(1):138–146. doi:10.1016/j.ejvs.2021.09.030
12. (OSF) OSoF. Available from: http://www.stat.fi/til/ksyyt/index_en.htm.
13. Kendall MA Kendall rank correlation and Mann-Kendall trend test; 2011.
14. Londero LS, Hogh A, Houlind K, Lindholt JS. Danish trends in major amputation after vascular reconstruction in patients with peripheral arterial disease 2002–2014. Eur J Vasc Endovasc Surg. 2019;57(1):111–120. doi:10.1016/j.ejvs.2018.08.047
15. Diehm N, Shang A, Silvestro A, et al. Association of cardiovascular risk factors with pattern of lower limb atherosclerosis in 2659 patients undergoing angioplasty. Eur J Vasc Endovasc Surg. 2006;31(1):59–63. doi:10.1016/j.ejvs.2005.09.006
16. Jalkanen JM, Wickstrom JE, Venermo M, Hakovirta HH. The extent of atherosclerotic lesions in crural arteries predicts survival of patients with lower limb peripheral artery disease: a new classification of crural atherosclerosis. Atherosclerosis. 2016;251:328–333. doi:10.1016/j.atherosclerosis.2016.04.016
17. Takeji Y, Yamaji K, Tomoi Y, et al. Impact of frailty on clinical outcomes in patients with critical limb ischemia. Circ Cardiovasc Interv. 2018;11(7):e006778. doi:10.1161/CIRCINTERVENTIONS.118.006778
18. Carmona GA, Hoffmeyer P, Herrmann FR, et al. Major lower limb amputations in the elderly observed over ten years: the role of diabetes and peripheral arterial disease. Diabetes Metab. 2005;31(5):449–454. doi:10.1016/s1262-3636(07)70215-x
19. Forssas E, Arffman M, Manderbacka K, Keskimaki I, Ruuth I, Sund R. Multiple complications among people with diabetes from Finland: an 18-year follow-up in 1994–2011. BMJ Open Diabetes Res Care. 2016;4(1):e000254. doi:10.1136/bmjdrc-2016-000254
20. Chen Q, Smith CY, Bailey KR, Wennberg PW, Kullo IJ. Disease location is associated with survival in patients with peripheral arterial disease. J Am Heart Assoc. 2013;2(5):e000304. doi:10.1161/JAHA.113.000304
21. Malyar NM, Freisinger E, Meyborg M, et al. Amputations and mortality in in-hospital treated patients with peripheral artery disease and diabetic foot syndrome. J Diabetes Complications. 2016;30(6):1117–1122. doi:10.1016/j.jdiacomp.2016.03.033
22. Dick F, Diehm N, Galimanis A, Husmann M, Schmidli J, Baumgartner I. Surgical or endovascular revascularization in patients with critical limb ischemia: influence of diabetes mellitus on clinical outcome. J Vasc Surg. 2007;45(4):751–761. doi:10.1016/j.jvs.2006.12.022
23. Faglia E, Clerici G, Clerissi J, et al. Early and five-year amputation and survival rate of diabetic patients with critical limb ischemia: data of a cohort study of 564 patients. Eur J Vasc Endovasc Surg. 2006;32(5):484–490. doi:10.1016/j.ejvs.2006.03.006
24. Krievins D, Zellans E, Latkovskis G, et al. Diagnosis of silent coronary ischemia with selective coronary revascularization might improve 2-year survival of patients with critical limb-threatening ischemia. J Vasc Surg. 2021;74(4):1261–1271. doi:10.1016/j.jvs.2021.03.059
25. Bonaca MP, Bauersachs RM, Anand SS, et al. Rivaroxaban in peripheral artery disease after revascularization. N Engl J Med. 2020;382(21):1994–2004. doi:10.1056/NEJMoa2000052
26. Takahara M, Iida O, Soga Y, et al. Heterogeneity of age and its associated features in patients with critical limb ischemia. Ann Vasc Dis. 2020;13(3):300–307. doi:10.3400/avd.oa.20-00067
27. Abou-Zamzam AM
28. Abou-Zamzam AM
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.