")
Back to Journals » Drug Design, Development and Therapy » Volume 16
Management of Axial Spondyloarthritis – Insights into Upadacitinib
Authors Braun J , Kiltz U , Baraliakos X
Received 21 June 2022
Accepted for publication 13 September 2022
Published 19 October 2022 Volume 2022:16 Pages 3609—3620
DOI https://doi.org/10.2147/DDDT.S330413
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Professor Anastasios Lymperopoulos
Jürgen Braun, Uta Kiltz, Xenofon Baraliakos
Rheumazentrum Ruhrgebiet and Ruhr University Bochum, Herne, Germany
Correspondence: Jürgen Braun, Rheumazentrum Ruhrgebiet, Claudiusstr.45, Herne, 44649, Germany, Tel +492325592131, Email [email protected]
Abstract: Although the pathogenesis of spondyloarthritis (SpA) has still not been elucidated our options to treat SpA have definitely improved in the last decades. There are two main types of SpA: (i) axial spondyloarthritis (axSpA), also covering the classical ankylosing spondylitis (AS) which is largely equivalent to radiographic (r)-axSpA but different from non-radiographic (nr)-axSpA, and (ii) peripheral SpA (pSpA) also covering psoriatic arthritis (PsA) as the main subtype. The subtype nr-axSpA has historically developed because the approval of drugs for AS did not cover forms without structural changes in the sacroiliac joints which is mandatory in the 1984 New York criteria. The definitions for axSpA are based on the 2009 Assessments in AxSpA International Society (ASAS) classification criteria. Several biologic disease modifying anti-rheumatic drugs (bDMARDs) such as the tumor necrosis factor alpha inhibitors (TNFi) and the interleukin-17-inhibitors (IL-17i) are approved mostly for the whole spectrum of SpA including axSpA and PsA but L-17i does not work in inflammatory bowel disease (IBD). Targeted synthetic (ts) DMARDs cover mainly the janus kinase (JAK)-inhibitors which have recently been developed to inhibit inflammation in several rheumatic and other immune mediated diseases such as IBD. Indeed, the physiologic mechanism of JAK-mediated signal transduction has been recognized as an important target because the inhibition of its actions was shown to successfully work as a therapeutic mechanism. There are now 4 small molecule JAK inhibitors (JAKi) that currently play a role in rheumatology with variable selectivity for the four different JAK isoforms: tofacitinib, baricitinib, upadacitinib and filgotinib. In this review, we summarize current clinical trial data and evaluate the use of the JAK1 selective inhibitor upadacitinib in the treatment of axSpA, including nr-axSpA and r-axSpA. Even though the efficacy and safety of upadacitinib over shorter periods of time has been convincing to date, long-term trials are needed to fully establish its performance and also evaluate the safety at higher doses, and its use in PsA.
Keywords: ankylosing spondylitis, axial spondyloarthritis, upadacitinib, JAK inhibition
Introduction
Upadacitinib exerts its mechanism of action by inhibiting the intracellular cytoplasmic enzyme Janus kinase (JAK) 1. The group of intracellular tyrosine kinase proteins comprises 4 isoforms: JAK 1, JAK 2, JAK 3 and tyrosine kinase (TYK) 2. These 4 JAK proteins and 7 signal transducer and activator of transcription (STAT) transcription factors mediate intracellular signal transduction downstream of cytokine receptors implicated in the pathology of autoimmune, allergic and inflammatory diseases.1–3 JAKs function by phosphorylation of STATs, regulation of gene expression, and influence on hematopoiesis and immune cell function including inhibitory effects on interleukins and interferons (Figures 1 and 2). Inhibition of JAK by targeted small-molecule therapies with selective inhibitory profiles have the capacity to target multiple aspects of those diseases by suppression of intracellular signaling mediated by multiple cytokines involved in the pathological processes of chronic inflammation.1–3
 |
Figure 1 Function and target of JAK kinases. Schematic representation of relevant Janus kinases (JAK) - signal transducers and activators of transcription (STAT) signaling pathways potentially involved in the pathogenesis of spondyloarthritides. Binding of the different Interleukins (IL) to their specific receptor subunits on different cell populations, eg T cells, innate lymphoid cells (ILC) or effector cells such as osteoblasts, fibroblasts or keratinocytes leads to activation of JAK-STAT pathways. The different isoforms of JAK are coupled to specific receptor/cytokine pairs and allow for a targeted inhibition with a specific JAK inhibitor. Adapted with permission from Hammitzsch A, Lorenz G, Moog P. Impact of Janus Kinase Inhibition on the Treatment of Axial Spondyloarthropathies. Front Immunol. 2020;11:591176.49 |
 |
Figure 2 Depiction of cytokines that activate and drugs that target Janus kinases (JAKs) presumably involved in the pathogenesis of immune-mediated inflammatory diseases. Top: efficacy of agents targeting specific JAK-inducing cytokines in different diseases. Centre: cytokines and respective receptors that trigger JAKs, types of JAKs activated and type of signal transducers and activators of transcription (STATs) activated by the respective JAKs. Bottom: JAK-inhibitors currently approved and their overall (including clinically derived) selectivity and presumed interference (+ or -) with certain cytokine pathways. Reprinted from Nash P, Kerschbaumer A, Dörner T et al. Points to consider for the treatment of immune-mediated inflammatory diseases with Janus kinase inhibitors: a consensus statement. Ann Rheum Dis. 2021; 80(1):71–87.6 Abbreviations: axSpA, axial spondyloarthritis; EPO, erythropoietin; GM-CSF, granulocyte- monocyte colony stimulating factor; IBD, inflammatory bowel diseases; IFN, interferon; IL, interleukin; ND, not done; PsA, psoriatic arthritis; PsO, psoriasis; R, receptor; RA, rheumatoid arthritis; TP, thrombopoietin. |
Indeed, JAK inhibition has been shown to work in rheumatoid arthritis (RA), ankylosing spondylitis (AS), psoriasis, psoriatic arthritis (PsA), inflammatory bowel disease (IBD), eg, ulcerative colitis (UC), atopic dermatitis and other immune-mediated diseases. AS is largely equivalent to radiographic axial spondyloarthritis (r-axSpA) which is differentiated on the basis of classification according to the modified New York criteria for AS from 19844 and the 2009 ASAS criteria for axSpA5 from non-radiographic axial spondyloarthritis (nr-axSpA). The cut-off between these two is based on the degree of structural changes in the sacroiliac joints (SIJ): anything > grade 2 unilateral will lead to a classification of r-axSpA.
EULAR has just published points to consider for the treatment of immune-mediated inflammatory diseases with JAK inhibitors.6 In addition, the usefulness of JAK inhibition is currently studied for the treatment of other autoimmune diseases such as systemic lupus erythematosus, giant cell arteritis, alopecia areata and allergic disorders, and they have even been used to reduce the COVID-19-related cytokine storm.7 Thus, treatments targeting JAK-STAT pathways have the potential to improve patient outcomes by reducing disease activity, glucocorticoid doses and/or non-specific immunosuppressants in immune-mediated inflammatory diseases.
The second-generation selective JAK inhibitor upadacitinib has a selective and potentially more prominent inhibitory influence on JAK1 relative to the other subtypes and approved for AS (see below), PsA10–12 and positive data on Crohn’s disease and ulcerative colitis have been published.13–15 There are 3 other JAK inhibitors: tofacitinib, baricitinib and filgotinib which are as approved as upadacitinib for different indications. The first generation agent tofacitinib preferentially inhibits JAK 1 and JAK 3 and baricitinib JAK 1 and JAK 2, while filgotinib also inhibits mainly JAK 1 (1–3,6 and Figures 1 and 2).
The targeted synthetic (ts) disease modifying antirheumatic drug (DMARD) upadacitinib was first approved for the treatment of moderate to severe RA unresponsive to first-line therapy with conventional (c) disease-modifying antirheumatic drugs (DMARDs),8 and then those unresponsive to biologic (b) DMARDs.9 The recommended daily dosage of upadacitinib is 15 mg orally as a monotherapy or combined with methotrexate or other nonbiological disease-modifying antirheumatic drugs (DMARDs) but there are also data for a dosage of 30 mg/day (not approved).
Studies in r-axSpA with Upadacitinib
There are now 3 published papers of one study called SELECT-AXIS on the treatment of patients with r-axSpA with upadacitinib (UPA).16–18 The first one, entitled “Efficacy and safety of UPA in patients with active AS: a multicentre, randomised, double-blind, placebo-controlled, Phase 2/3 trial”.16 SELECT-AXIS is a two-period, parallel-group study that enrolled patients in 20 countries in 62 sites, registered at ClinicalTrials.gov as NCT03178487. Eligible patients who had to fulfil the modified New York criteria for AS18 also had to have an inadequate response to at least two or intolerance or contraindication to non-steroidal anti-inflammatory drugs (NSAIDs). Previous treatment with bDMARDs was not allowed. A total of 187 patients were randomly assigned 1:1 using interactive response technology to take UPA 15 mg once or one placebo tablet daily up to 14 weeks (study period 1) when the primary endpoint, the Assessment of SpondyloArthritis international Society (ASAS) 40 response was assessed. Most patients (95%), with no difference between groups, completed the study. Many more patients achieved an ASAS 40 response in the UPA versus the placebo group: 52% vs 26% (p = 0.0003). There were slightly but not significantly more adverse events on UPA (62%) than on placebo (55%). The most common adverse event in the UPA group was any infection (28% versus 20% in verum and placebo). However, increased creatine phosphokinase and hepatic disorders were also noted: 9% vs 2% on placebo. No serious infections, herpes zoster, malignancy, venous thromboembolic events, or deaths were reported.
In the second publication the 1-year data of the trial were reported.17 Before entering this open-label extension at week 14, all patients randomized to receive placebo were switched to UPA. All 178 patients who completed week 14 continued to receive UPA up to week 104. The interim data obtained at week 64 showed that similar proportions of patients in both groups (continuous UPA or placebo-to-UPA) achieved an ASAS 40 response or an AS Disease Activity Score (ASDAS) showing low disease activity at week 64. In a nonresponder imputation (NRI) analysis ≥70% of patients achieved these endpoints and based on an as-observed analysis ≥81%. Furthermore, ≥34% (NRI) and ≥39% (as-observed analysis) achieved ASDAS inactive disease or ASAS partial remission at week 64. Mean changes from baseline (week 0) to week 64 in pain, function, and inflammation showed consistent improvement or sustained maintenance through the study. Importantly, function, as assessed by BASFI (initially 5.4), also improved substantially.
Among 182 patients receiving UPA (237.6 patient-years), 618 adverse events (260.1 per 100 patient-years) were reported. No serious infections, major adverse cardiovascular events (MACE), venous thromboembolic events (VTE), gastrointestinal perforation, or deaths were reported.
In the third paper, the 2-year data of UPA in AS with 187 randomised patients are presented.18 Most patients (n = 144) completed week 104 (77%). The ASAS 40 response rate in patients receiving continuous UPA at week 104 was 85.9% (as observed) and 65.6% (non-responder imputation). Again, there was no difference in patients who switched from placebo to UPA. See Figures 3 and 4 for more detail.
 |
Figure 3 (A–C) ASAS 40 response, ASAS partial remission and ASDAS low disease activity in r-axSpA patients treated with upadacitinib 15 mg/day vs placebo over 2 years. Percentages of patients achieving ASAS40, ASAS PR and ASDAS LD over 104 weeks. Dashed line: all patients randomised to placebo in period 1 who received open-label upadacitinib starting from week 14. Descriptive statistics are provided. Reprinted from van der Heijde D, Deodhar A, Maksymowych WP et al. Upadacitinib in active ankylosing spondylitis: results of the 2-year, double-blind, placebo-controlled SELECT-AXIS 1 study and open-label extension. RMD Open. 2022;8(2): e002280.19 Abbreviations: r-axSpA, radiographic axial spondyloarthritis; AO, as observed; ASAS, Assessment of SpondyloArthritis international Society; NRI, non-responder imputation; PR, partial remission; LD, low disease activity; QD, once daily; W, week. |
 |
Figure 4 (A and B) ASDAS and BASFI in r-axSpA patients treated with upadacitinib 15 mg/day vs placebo over 2 years. Reprinted from van der Heijde D, Deodhar A, Maksymowych WP, Sieper J, Van den Bosch F, Kim TH, Kishimoto M, Östör AJ, Combe B, Sui Y, Duan Y, Wung PK, Song IH. Upadacitinib in active ankylosing spondylitis: results of the 2-year, double-blind, placebo-controlled SELECT-AXIS 1 study and open-label extension. RMD Open. 2022; 8(2): e002280.19 Abbreviations: ASDAS, Ankylosing Spondylitis Disease Activity Score; BASFI, Bath Ankylosing Spondylitis Functional Index; AO, as observed; MMRM, mixed-effect model for repeated measures; W, week. |
In the modified Stokes AS Spinal Score (mSASSS), the mean change from baseline to week 104 was 0.7 (95% CI 0.3–1.1). This is rather similar to other DMARD studies. The adverse event rate was 242.7 in 100 patient-years. No serious infections, adjudicated major adverse cardiovascular events, lymphoma, non-melanoma skin cancer, or gastrointestinal perforations were observed.
Thus, UPA 15 mg once daily showed sustained and consistent efficacy over 2 years with no difference in the group who had placebo in the first 14 weeks.
There is one more recent paper reporting data on 420 patients with active AS who had an insufficient response or were intolerant to at least one bDMARD (NCT04169373).19 Patients randomised to UPA 15 mg/day (n = 211) achieved the primary endpoint (ASAS 40) at week 14 significantly more often (45%) than those on placebo (n = 209; 18%).
Response rates are generally lower in patients who had not responded to a first bDMARD. However, a rate of 45% response is comparatively good in biologic-experienced AS patients,20–22 but these are indirect comparisons.
Positive data of other trials with JAK inhibitors clearly suggest that we are dealing with a class effect.4,23–27 No head-to-head trial has been organized to date.
The Study in nr-axSpA with Upadacitinib
To assess the efficacy and safety of UPA in patients with active nr-axSpA the study SELECT-AXIS 2 (NCT04169373) combined two independent studies, one in AS patients with an inadequate response to bDMARDs and one in nr-axSpA. The latter, a randomized, double-blind, PBO-controlled Phase 3 trial enrolled patients ≥18 years classified as nr-axSpA, who had objective signs of active inflammation on MRI of the SIJ and/or high sensitivity C-reactive protein (hs-CRP) >upper limit of normal (2.87 mg/L) at baseline.28 In addition, all patients had to have a BASDAI and a total back pain score ≥4 (0–10 NRS). Patients were randomized 1:1 to receive UPA 15 mg once daily or PBO during a 52-week double-blind treatment period but the primary endpoint was an ASAS40 response at week 14 (Figure 5). There were many secondary endpoints, and adverse events (AEs) reported through week 14 for all patients who received ≥1 dose of study drug. Out of 314 pts randomized, 313 received study drug (UPA 15 mg, n = 156; PBO, n = 157), and 295 (94%) received study drug through week 14. Baseline demographic and disease characteristics were consistent with an active nr-axSpA population (58% female; mean age 42.1 years; mean BASDAI 6.9; mean hs-CRP 12.1 mg/L).
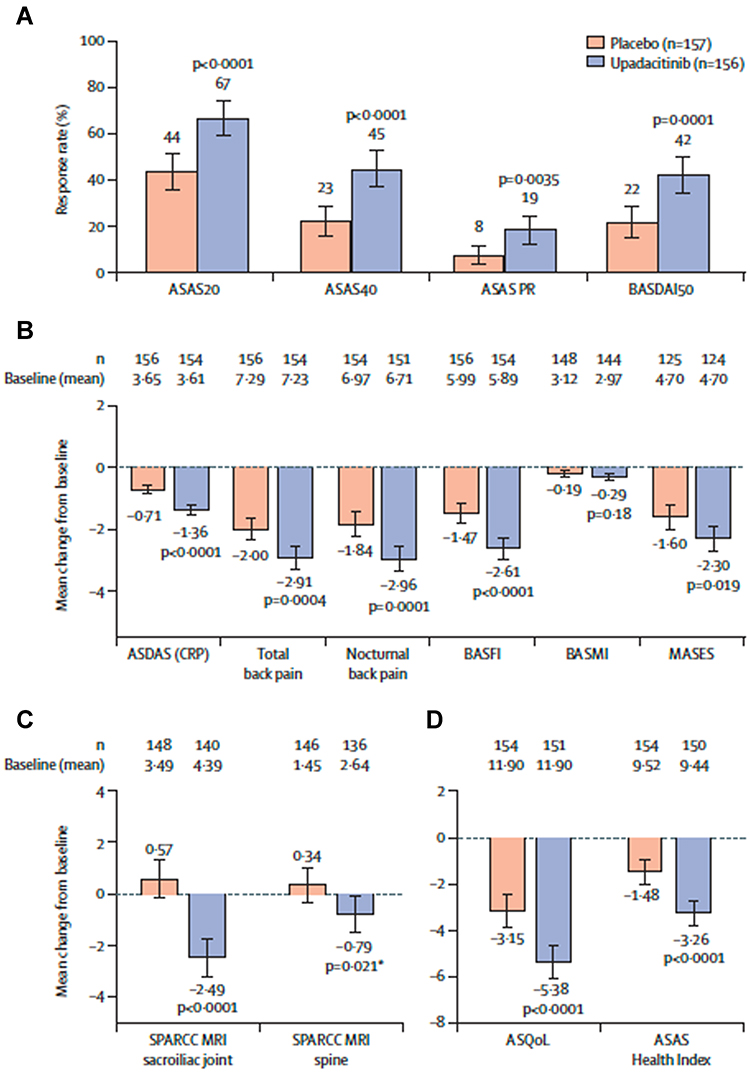 |
Figure 5 ASAS 20, ASAS 40 response, ASAS partial remission, BASDAI 50, ASDAS LDA and ID, ASDAS CRP, SPARCC SIJ, nocturnal back pain, BASFI, ASQoL, ASAS-HI, BASMI and MASES in nr-axSpA patients treated with upadacitinib 15 mg/day vs placebo. *Nominal p=0·021. Analysis of multiplicity-controlled primary and key secondary endpoints at week 14. (A) Based on non-responder imputation incorporating multiple imputation analysis. (B) Multiplicity-controlled key secondary endpoints; ANCOVA analysis based on observed data for BASMI; MMRM analysis based on observed data for other endpoints; MASES was assessed in patients with baseline enthesitis. (C) Based on ANCOVA analysis; SPARCC MRI was assessed in patients with available baseline data up to 3 days after the first dose of study drug and available week 14 data up to the first dose of study drug in the open-label period. (D) Based on MMRM analysis. All endpoints were multiplicity controlled and sequentially tested (appendix p 10), except for SPARCC MRI spine score. Error bars show 95% CIs. MASES was not tested as part of the multiplicity-controlled test since BASMI did not meet statistical significance; only the nominal p value is presented, nominal p<0·05. Reprinted from Lancet, 400 (10349), Deodhar A, Van den Bosch F, Poddubnyy D et al. Upadacitinib for the treatment of active non-radiographic axial spondyloarthritis (SELECT-AXIS 2): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet 369–379, with permission from Elsevier.28 Abbreviations: ASAS20, Assessment of SpondyloArthritis international Society 20 response; ASAS40, Assessment of SpondyloArthritis international Society 40 response; ASAS PR, Assessment of SpondyloArthritis international Society partial remission; ASDAS (CRP), Ankylosing Spondylitis (AS) Disease Activity Score C-reactive protein; ASQoL, AS Quality of Life Score; BASDAI50, at least 50% improvement from baseline in Bath Ankylosing Spondylitis Disease Activity Index; BASFI, Bath AS Functional Index; BASMI, Bath AS Metrology Index; MASES, Maastricht AS Enthesitis Score; MMRM, mixed-effect model for repeated measures; SPARCC, Spondyloarthritis Research Consortium of Canada. |
A higher ASAS40 response rate at week 14 was achieved with UPA vs PBO (45% vs 23%; P < 0.0001). All endpoints, except for BASMI and MASES, were statistically superior for UPA vs PBO at week 14 (12 of 14 multiplicity-controlled secondary endpoints), see Figure 5 for more details.
The proportion of patients with AE was similar (UPA 48%; PBO, 46%). Serious AEs and AEs leading to discontinuation were reported in 4 (2.6%) patients on UPA and 2 (1.3%) on PBO, respectively. Only few patients had a serious infection or herpes zoster (1.3% on UPA; 0.6% on PBO, respectively). Uveitis was reported in 1 patient on UPA who had a history of uveitis and none on PBO. No malignancy other than non-melanoma skin cancer, major adverse cardiovascular events, venous thromboembolic events, IBD, or death were reported in the study, there was one case of basal cell carcinoma that occurred on PBO.28
A daily dose of UPA 15 mg/day was shown to be efficacious in disease activity, pain, function, quality of life, and MRI-detected SI joint inflammation than PBO after 14 weeks of treatment in patients with active nr-axSpA. The safety profile of UPA 15 mg/day was consistent with what had been observed in other inflammatory musculoskeletal diseases.
The results of this study were presented at EULAR 2022 in Copenhagen. AbbVie has submitted applications for UPA (RINVOQ®) in nr-axSpA to FDA and European Medicines Agency (EMA) (EMA) on January 7th of 2022.24 On July 29th 2022 the company announced that the EMA has approved UPA in a daily oral dose of 15mg for this indication.
Pharmacology and Safety
UPA is metabolized in the liver by the cytochrome P450 (CYP) system, mainly the CYP3A4 enzyme, it has a drug half-life of 8–14 hours and is eliminated in feces and urine. Concomitant use with CYP3A4 Inhibitors and CYP3A4 inducers should be used with caution since it may intervene with drug pharmacokinetics, hereby increasing or decreasing plasma concentrations.30,31
In reproductive animal studies, UPA has been shown to cause injury to the developing fetus and be present in breastmilk. During pregnancy, women should be advised and counseled about UPA use and the likely negative effects while on therapy. Women should use contraceptives while being treated and 4 weeks after discontinuation of treatment.
In RA, the use of UPA in combination with csDMARDs such as methotrexate (MTX) is supported, since, combined with first-line MTX, UPA was shown to inhibit radiographic progression and maintained clinical efficacy.30,31 In contrast, the use of UPA with bDMARDS such as infliximab, adalimumab, etanercept, abatacept, and immunosuppressants such as azathioprine, tacrolimus and ciclosporine is not recommended.
Administration of a live attenuated vaccination soon before or during treatment with UPA should be avoided. However, approximately two-thirds of patients receiving UPA 15 mg once daily have been reported to achieve a satisfactory humoral response to 13-valent conjugated pneumococcal vaccination (PCV-13) despite receiving concomitant methotrexate (MTX). In addition, concomitant corticosteroid use did not negatively affect that immune response.32
Since no data are available from registers or Phase 4 trials yet, all safety informations come from placebo-controlled studies, in which several adverse effects have been observed in subjects administered 15 mg orally of UPA (see list below). Even more severe adverse effects (SAE) such as herpes zoster virus (HZV) and serious infections (<1%) were seen in subjects administered the higher dose of 30 mg/day in a double-blind, randomized, controlled phase 3 clinical trial.30,31 Malignancy, thrombosis, and gastrointestinal perforations with concomitant NSAID use have also been reported during clinical studies.15,27,30,32–35
In a recent meta-analysis of RCT data and reviews the VTE risk with JAK inhibitors has been defined as a class effect in patients with immune mediated diseases.15,33–36 However, the pooled IRRs do not provide evidence that support the current warnings of VTE risk for JAK inhibitors. These findings will aid continued development of clinical guidelines for the use of JAK inhibitors in IMIDs.
In a recent trial comparing the combined tofacitinib doses with a TNF inhibitor in a cardiovascular risk-enriched population,35 risks of MACE and cancers were higher with tofacitinib and did not meet noninferiority criteria. Several adverse events were more common with tofacitinib.
In a recent meta analysis on the performance of UPA in ulcerative colitis31 this agent was the best performing agent for the induction of clinical remission (the primary outcome) but the worst performing agent in terms of adverse events in patients with moderate-to-severe ulcerative colitis.
Reported adverse effects of UPA include:
- Upper respiratory tract infections (14%)
- Nausea (4%)
- Elevated liver enzymes (2%)
- Fever (1%)
- Cough (2%)
- Upper respiratory tract infections include:
- Acute sinusitis
- Laryngitis
- Nasopharyngitis
- Oropharyngeal pain
- Pharyngitis
- Pharyngotonsillitis
- Rhinitis
- Sinusitis
- Tonsillitis
- Viral upper respiratory tract infection
JAKi Boxed Warning by the FDA and Comment by the ACR
On September 1st of 2021, the Federal Drug Administration (FDA) of the United States had announced required revisions to the Boxed Warning for all JAK inhibitors approved for RA, PsA, polyarticular-course Juvenile Idiopathic Arthritis (pcJIA) and.37 The American College of Rheumatology (ACR) statement on the safety of JAK inhibitors was updated on January 28th of 2022.38 The 2021 ACR RA Clinical Practice Guideline has recommended the addition of either a b or tsDMARD such as a JAK inhibitor to MTX non-responders.39 The guideline did note potential emerging safety signals and anticipated upcoming results of an FDA-mandated long term prospective open label non-inferiority safety clinical trial in RA patients. The recently completed international ORAL surveillance study36 compared two doses of tofacitinib (5 mg and 10 mg bid) to the TNFi adalimumab and etanercept concentrating on 2 co-primary endpoints of major adverse cardiac events (MACE) and malignancy. The study performed on 4362 RA patients older than 50 years who had at least one additional cardiovascular risk factor was published on January 27th of 2022.36 Although the trial was done in patients treated with tofacitinib, the FDA, citing a similar mechanism of action, broadened the change in indication to cover all JAK inhibitors approved across all approved indications related to the risks of serious heart-related events, cancer, blood clots, and death.37 Thus, these drugs are now approved for patients who have not responded to, or cannot tolerate, one or more TNFi.
The ACR has recommended to aim for a shared decision making between patient and provider regarding the risk/benefit of JAKi as a potential treatment option for patients in whom continued TNFi use is not a viable option.
Practical Issues and Monitoring
UPA is available as 15 mg extended-release tablets for oral consumption. The medication can be taken with or without food and recommended as a whole tablet without splitting or crushing it.
Before the initiation of treatment with UPA, screening for latent tuberculosis (TB) with a tuberculin skin test (TST) or interferon-γ release assay (IGRA) is required as the treatment may possibly activate a latent TB infection. Patients with a positive TB test must be treated according to national guidelines before starting UPA. During treatment with UPA, patients should routinely be tested for TB.40
A complete blood count (CBC) before starting therapy and also routinely is advised as it is relatively contraindicated to initiate UPA in subjects with an absolute lymphocyte count (ALC) below 500 cells/mm3 and absolute neutrophil count (ANC) below 1.000 cells/mm3. Lymphopenia, neutropenia, and anemia during therapy with UPA have been reported.
Liver function tests (LFT) should be checked before therapy with UPA and regularly thereafter, as patients with severe hepatic impairment are not recommended to start with or stay on treatment.
The lipid panel should be monitored about 3 months after treatment, as increases in total cholesterol, low-density lipoprotein (LDL) cholesterol, and high-density lipoprotein (HDL) cholesterol may occur on treatment.40
Patients should also be monitored for serious infections before and while on therapy, as severe bacterial, viral, fungal, tuberculous, and opportunistic infections have occurred, which have led to hospitalization and mortality in patients receiving upadacitinib. In that case, treatment must be interrupted.
Monitoring for reactivation of previous hepatitis B virus (HBV) or Herpes zoster (HZV) infections is recommended. UPA should be temporarily discontinued until an infection with HZV is resolved.40
Subjects at high risk for skin cancer who receive treatment with UPA are advised to have routine skin examinations as they have an increased chance for non-melanoma skin cancers (NMSCs).
Patients receiving UPA with concomitant use of non-steroidal anti-inflammatory agents (NSAIDs) should be monitored for gastrointestinal (GI) side effects as ulcers and GI perforations have occurred in clinical studies.15,30,31,33–36
Patients should generally be informed about the range of adverse effects that may occur during therapy, especially about the increased risk of severe infections. Routine follow-ups with are essential to prevent complications, hospitalization, and mortality. The rheumatologist and the interdisciplinary team in cooperation with general practitioners should should monitor patients and blood tests regularly.
International Recommendations
The most recent national and international recommendations for the treatment of AxSpA [from Assessment of SpondyloArthritis international Society (ASAS) and EULAR in 2016 did not include JAK inhibitors (JAKi) due to limited evidence at this point in time.41 An update of the recommendations, however, is in press. EULAR recommendations from 2020 consider using JAKi as second-line option for the treatment of PsA, namely following the inadequate response to csDMARDS and bDMARDs, including TNFi, and inhibitors of IL-17A and IL-12/23.42 Recommendations for RA43 have been updated by the points to consider when using JAK inhibitors.6
Structural Changes in the Sacroiliac Joints of Patients with axSpA
AxSpA is characterised by inflammation and new bone formation which are mainly assessed by conventional radiography (CR) and magnetic resonance imaging (MRI). TNFi and IL-17 antagonists have been shown to be efficacious in patients with axSpA. This treatment seems to also inhibit structural damage or at least retard radiographic progression. A reduction of new bone formation as assessed by CR of the spine has been reported to occur after about 4 years of therapy.44 Recently, a reduction of erosions and ankylosis in the SIJ has also been observed in axSpA patients treated with etanercept and filgotinib.45,46 However, there is some evidence that the clinical significance of very small changes in the structure of SIJ in patients with axSpA is rather limited.47 Indeed, the frequency of vertebral erosions in patients with AS is rather low48 which makes it unlikely that this pathology will be clinically relevant for clinical outcomes.
In summary, the rather small effect of b- and tsDMARDS on structural SIJ changes as assessed by MRI recently reported is not sufficient to make a claim for structural modification of any drug tested. Effects on new bone formation in axSpA need to be rather assessed in the spine.47
Conclusion
JAK inhibitors are important orally administered agents conferring different degrees of selectivity toward JAK1, JAK2, and JAK3 which may have implications on efficacy and safety in axSpA and PsA. Phase 2 and 3 clinical trials in PsA for tofacitinib and upadacitinib and phase 2 for filgotinib confirmed efficacy comparable to bDMARDs. In axSpA/AS, phase 2 and 2/3 studies confirmed significant efficacy of tofacitinib, filgotinib and upadacitinib compared to placebo. Safety was comparable to clinical trial, long-term extension, and registry data for rheumatoid arthritis. However, long-term data are still lacking.
Even though our understanding of the pathogenesis of SpA is still limited, the role of JAK-mediated signal transduction and inhibiting its actions as a therapeutic mechanism is constantly increasing, since several small molecule inhibitors of JAK have been shown to work. The significance of the variable selectivity of the different JAK isoforms is still not completely clear – and this is potentially relevant for efficacy and safety. This also includes the dosage which includes the observation that the higher dose is usually associated with more adverse events. Whether selective JAK1 inhibition is in the end advantageous remains to be demonstrated.
In this review, we have summarized the current clinical trial data, evaluating the use of JAK1 selective inhibitors especially in the treatment of r-axSpA/AS and nr-axSpA. Selective JAK1 inhibition offers a promising therapeutic approach; however, more long-term trials are needed to fully establish their efficacy and safety, especially at higher doses, and their use in the greater continuum of patients with SpA. Another review on emerging biological therapies in axSpA and PsA (without UPA) is currently in press.50
Disclosure
Prof. Dr. Jürgen Braun, PD Dr.Uta Kiltz and Prof.Dr.X.Baraliakos did not receive any grants for the conduct of this manuscript. Professor Jürgen Braun reports grants, personal fees from Abbvie, Lilly, Galapagos, but not during the conduct of the study; and grants, personal fees from Novartis, outside the submitted work. Dr Uta Kiltz reports personal fees and/or grants from Abbvie, Amgen, Lilly, Fresenius, Gilead, GSK, Hexal, Janssen, MSD, Novartis, Pfizer, and UCB, outside the submitted work. The authors report no other conflicts of interest in this work, and they confirm that there was no third party influence on the content of this review.
References
1. Spinelli FR, Colbert RA, Gadina M. JAK1: number one in the family; number one in inflammation? Rheumatology. 2021;60(Suppl 2):ii3–ii10. doi:10.1093/rheumatology/keab024
2. Traves PG, Murray B, Campigotto F, Galien R, Meng A, Di Paolo JA. JAK selectivity and the implications for clinical inhibition of pharmacodynamic cytokine signalling by filgotinib, upadacitinib, tofacitinib and baricitinib. Ann Rheum Dis. 2021;80(7):865–875. doi:10.1136/annrheumdis-2020-219012
3. Tanaka Y, Luo Y, O’Shea JJ, Nakayamada S. Janus kinase-targeting therapies in rheumatology: a mechanisms-based approach. Nat Rev Rheumatol. 2022;1–13. doi:10.1038/s41584-021-00711-1
4. van der Linden S, Valkenburg HA, Cats A. Evaluation of diagnostic criteria for ankylosing spondylitis. A proposal for modification of the New York criteria. Arthritis Rheum. 1984;27(4):361–368. doi:10.1002/art.1780270401
5. Rudwaleit M, van der Heijde D, Landewé R, et al. The development of assessment of SpondyloArthritis international society classification criteria for axial spondyloarthritis (part II): validation and final selection. Ann Rheum Dis. 2009;68(6):777–783. Erratum in: Ann Rheum Dis 2019 Jun; 78(6): e59. doi:10.1136/ard.2009.108233
6. Nash P, Kerschbaumer A, Dörner T, et al. Points to consider for the treatment of immune-mediated inflammatory diseases with Janus kinase inhibitors: a consensus statement. Ann Rheum Dis. 2021;80(1):71–87. doi:10.1136/annrheumdis-2020-218398
7. Kalil AC, Patterson TF, Mehta AK,…; ACTT-2 Study Group Members. Baricitinib plus remdesivir for hospitalized adults with Covid-19. N Engl J Med. 2021; 384(9):795–807. doi:10.1056/NEJMoa2031994
8. Burmester GR, Kremer JM, Van den Bosch F, et al. Safety and efficacy of upadacitinib in patients with rheumatoid arthritis and inadequate response to conventional synthetic disease-modifying anti-rheumatic drugs (SELECT-NEXT): a randomised, double-blind, placebo-controlled phase 3 trial. Lancet. 2018;391(10139):2503–2512. doi:10.1016/S0140-6736(18)31115-2
9. Genovese MC, Fleischmann R, Combe B, et al. Safety and efficacy of upadacitinib in patients with active rheumatoid arthritis refractory to biologic disease-modifying anti-rheumatic drugs (SELECT-BEYOND): a double-blind, randomised controlled phase 3 trial. Lancet. 2018;391(10139):2513–2524. doi:10.1016/S0140-6736(18)31116-4
10. McInnes IB, Anderson JK, Magrey M, et al. Trial of upadacitinib and adalimumab for psoriatic arthritis. N Engl J Med. 2021;384(13):1227–1239. doi:10.1056/NEJMoa2022516
11. McInnes IB, Kato K, Magrey M, et al. Upadacitinib in patients with psoriatic arthritis and an inadequate response to non-biological therapy: 56-week data from the phase 3 SELECT-PsA 1 study. RMD Open. 2021;7(3):e001838. [Erratum in: RMD Open 2021 Nov; 7 (3)]. doi:10.1136/rmdopen-2021-001838
12. White JPE, Coates LC. JAK1 selective inhibitors for the treatment of spondyloarthropathies. Rheumatology. 2021;60(Suppl 2):ii39–ii44. doi:10.1093/rheumatology/keaa815
13. Harris C, Cummings JRF. JAK1 inhibition and inflammatory bowel disease. Rheumatology. 2021;60(Supple2):ii45–ii51. doi:10.1093/rheumatology/keaa896
14. Sandborn WJ, Feagan BG, Loftus EV Jr, et al. Efficacy and safety of upadacitinib in a randomized trial of patients with crohn’s disease. Gastroenterology. 2020;158(8):2123–2138.e8. doi:10.1053/j.gastro.2020.01.047
15. Lasa JS, Olivera PA, Danese S, Peyrin-Biroulet L. Efficacy and safety of biologics and small molecule drugs for patients with moderate-to-severe ulcerative colitis: a systematic review and network meta-analysis. Lancet Gastroenterol Hepatol. 2022;7(2):161–170. doi:10.1016/S2468-1253(21)00377-0
16. van der Heijde D, Song IH, Pangan AL, et al. Efficacy and safety of upadacitinib in patients with active ankylosing spondylitis (SELECT-AXIS 1): a multicentre, randomised, double-blind, placebo-controlled, phase 2/3 trial. Lancet. 2019;394(10214):2108–2117. doi:10.1016/S0140-6736(19)32534-6
17. Deodhar A, van der Heijde D, Sieper J, et al. Safety and efficacy of upadacitinib in patients with active ankylosing spondylitis and an inadequate response to nonsteroidal antiinflammatory drug therapy: one-year results of a double-blind, placebo-controlled study and Open-label extension. Arthritis Rheumatol. 2022;74(1):70–80. doi:10.1002/art.41911
18. van der Heijde D, Deodhar A, Maksymowych WP, et al. Upadacitinib in active ankylosing spondylitis: results of the 2-year, double-blind, placebo-controlled SELECT-AXIS 1 study and open-label extension. RMD Open. 2022;8(2):e002280. doi:10.1136/rmdopen-2022-002280
19. van der Heijde D, Baraliakos X, Sieper J, et al. Efficacy and safety of upadacitinib for active ankylosing spondylitis refractory to biological therapy: a double-blind, randomised, placebo-controlled phase 3 trial. 2022. Ann Rheum Dis. annrheumdis-2022–222608.
20. Rudwaleit M, Van den Bosch F, Kron M, Kary S, Kupper H. Effectiveness and safety of Adalimumab in patients with ankylosing spondylitis or psoriatic arthritis and history of anti-tumor necrosis factor therapy. Arthritis Res Ther. 2010;12(3):R117. doi:10.1186/ar3054
21. D’Angelo S, Tirri E, Giardino AM, et al. Effectiveness of golimumab as second anti-TNFα drug in patients with rheumatoid arthritis, psoriatic arthritis and axial spondyloarthritis in Italy: GO-BEYOND, a prospective real-world observational study. J Clin Med. 2022;11(14):4178. doi:10.3390/jcm11144178
22. Dougados M, Wei JC, Landewé R, et al.; COAST-V and COAST-W Study Groups. Efficacy and safety of ixekizumab through 52 weeks in two phase 3, randomised, controlled clinical trials in patients with active radiographic axial spondyloarthritis (COAST-V and COAST-W). Ann Rheum Dis. 2020;79(2):176–185. Erratum in: Ann Rheum Dis 2020 Jun; 79(6): e75. doi:10.1136/annrheumdis-2019-216118
23. van der Heijde D, Deodhar A, Wei JC, et al. Tofacitinib in patients with ankylosing spondylitis: a Phase II, 16-week, randomised, placebo-controlled, dose-ranging study. Ann Rheum Dis. 2017;76(8):1340–1347. doi:10.1136/annrheumdis-2016-210322
24. Deodhar A, Sliwinska-Stanczyk P, Xu H, et al. Tofacitinib for the treatment of ankylosing spondylitis: a Phase III, randomised, double-blind, placebo-controlled study. Ann Rheum Dis. 2021;80(8):1004–1013. doi:10.1136/annrheumdis-2020-219601
25. van der Heijde D, Baraliakos X, Gensler LS, et al. Efficacy and safety of filgotinib, a selective Janus kinase 1 inhibitor, in patients with active ankylosing spondylitis (TORTUGA): results from a randomised, placebo-controlled, phase 2 trial. Lancet. 2018;392(10162):2378–2387. doi:10.1016/S0140-6736(18)32463-2
26. Keeling S, Maksymowych WP. JAK inhibitors, psoriatic arthritis, and axial spondyloarthritis: a critical review of clinical trials. Expert Rev Clin Immunol. 2021;17(7):701–715. doi:10.1080/1744666X.2021.1925541
27. McInnes IB, Ostor AJK, Mease PJ, et al. Effect of upadacitinib on reducing pain in patients with active psoriatic arthritis or ankylosing spondylitis: post hoc analysis of three randomised clinical trials. RMD Open. 2022;8(1):e002049. doi:10.1136/rmdopen-2021-002049
28. Deodhar A, Van den Bosch F, Poddubnyy D, et al. Upadacitinib for the treatment of active non-radiographic axial spondyloarthritis (SELECT-AXIS 2): a randomised, double-blind, placebo-controlled, phase 3 trial. Lancet. 2022;400(10349):369–379. doi:10.1016/S0140-6736(22)01212-0
29. AbbVie. Submits Applications for Upadacitinib (RINVOQ®) in Non-Radiographic Axial Spondyloarthritis to U.S. Food and Drug Administration (FDA) and European Medicines Agency (EMA). Available from: https://news.abbvie.com/news/press-releases/abbvie-submits-applications-for-upadacitinib-rinvoq-in-non-radiographic-axial-spondyloarthritis-to-us-food-and-drug-administration-fda-and-european-medicines-agency-ema.htm.
30. Serhal L, Edwards CJ. Upadacitinib for the treatment of rheumatoid arthritis. Expert Rev Clin Immunol. 2019;15(1):13–25. doi:10.1080/1744666X.2019.1544892
31. Duggan S, Keam SJ. Upadacitinib: first approval. Drugs. 2019;79(16):1819–1828. doi:10.1007/s40265-019-01211-z
32. Winthrop K, Vargas JI, Drescher E, et al. Evaluation of response to 13-valent conjugated pneumococcal vaccination in patients with rheumatoid arthritis receiving upadacitinib: results from a phase 2 open-label extension study. RMD Open. 2022;8(1):e002110. doi:10.1136/rmdopen-2021-002110
33. Olivera PA, Lasa JS, Bonovas S, Danese S, Peyrin-Biroulet L. Safety of janus kinase inhibitors in patients with inflammatory bowel diseases or other immune-mediated diseases: a systematic review and meta-analysis. Gastroenterology. 2020;158(6):1554–1573.e12. doi:10.1053/j.gastro.2020.01.001
34. Yates M, Mootoo A, Adas M, et al. Venous thromboembolism risk with JAK inhibitors: a meta-analysis. Arthritis Rheumatol. 2021;73(5):779–788. doi:10.1002/art.41580
35. Ytterberg SR, Bhatt DL, Mikuls TR, et al.; ORAL Surveillance Investigators. Cardiovascular and cancer risk with tofacitinib in rheumatoid arthritis. N Engl J Med. 2022;386(4):316–326. doi:10.1056/NEJMoa2109927
36. Witte T. Januskinaseinhibitoren [Janus kinase inhibitors]. Z Rheumatol. 2022;81(2):94–99. doi:10.1007/s00393-021-01125-w
37. US Food & Drug Administration. FDA requires warnings about increased risk of serious heart-related events, cancer, blood clots, and death for JAK inhibitors that treat certain chronic inflammatory conditions Available from: https://www.fda.gov/drugs/drug-safety-and-availability/fda-requires-warnings-about-increased-risk-serious-heart-related-events-cancer-blood-clots-and-death.
38. American College of Rheumatology. Search results for JAK FDA. Available from: https://www.rheumatology.org/Search/sb-bhvr/1/sb-logid/320106-kb5qq2gmlri6b81k?sb-search=JAK+FDA.
39. Fraenkel L, Bathon JM, England BR, et al. 2021 American college of rheumatology guideline for the treatment of rheumatoid arthritis. Arthritis Rheumatol. 2021;73(7):1108–1123. doi:10.1002/art.41752
40. Padda IS, Bhatt R, Parmar M. Upadacitinib. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022.
41. van der Heijde D, Ramiro S, Landewé R, et al. 2016 update of the ASAS-EULAR management recommendations for axial spondyloarthritis. Ann Rheum Dis. 2017;76(6):978–991. doi:10.1136/annrheumdis-2016-210770
42. Gossec L, Baraliakos X, Kerschbaumer A, et al. EULAR recommendations for the management of psoriatic arthritis with pharmacological therapies: 2019 update. Ann Rheum Dis. 2020;79(6):700–712. doi:10.1136/annrheumdis-2020-217159
43. Smolen JS, Landewé RBM, Bijlsma JWJ, et al. EULAR recommendations for the management of rheumatoid arthritis with synthetic and biological disease-modifying antirheumatic drugs: 2019 update. Ann Rheum Dis. 2020;79(6):685–699. doi:10.1136/annrheumdis-2019-216655
44. Molnar C, Scherer A, Baraliakos X, et al.; Rheumatologists of the Swiss Clinical Quality Management Program. TNF blockers inhibit spinal radiographic progression in ankylosing spondylitis by reducing disease activity: results from the Swiss Clinical Quality Management cohort. Ann Rheum Dis. 2018;77(1);63–69. doi:10.1136/annrheumdis-2017-211544
45. Maksymowych WP, Claudepierre P, de Hooge M, et al. Structural changes in the sacroiliac joint on MRI and relationship to ASDAS inactive disease in axial spondyloarthritis: a 2-year study comparing treatment with etanercept in EMBARK to a contemporary control cohort in DESIR. Arthritis Res Ther. 2021;23(1):43. doi:10.1186/s13075-021-02428-8
46. Maksymowych WP, Østergaard M, Landewé R, et al. Impact of filgotinib on sacroiliac joint MRI structural lesions at 12 weeks in patients with active ankylosing spondylitis (TORTUGA trial). Rheumatology. 2021;3:keab543.
47. Braun J, Kiltz U, Baraliakos X. Significance of structural changes in the sacroiliac joints of patients with axial spondyloarthritis detected by MRI related to patients symptoms and functioning. Ann Rheum Dis. 2022;81(1):11–14. doi:10.1136/annrheumdis-2021-221406
48. Ramiro S, van Tubergen A, van der Heijde D, et al. Brief report: erosions and sclerosis on radiographs precede the subsequent development of syndesmophytes at the same site: a twelve-year prospective follow up of patients with ankylosing spondylitis. Arthritis Rheumatol. 2014;66(10):2773–2779. doi:10.1002/art.38775
49. Hammitzsch A, Lorenz G, Moog P. Impact of janus kinase inhibition on the treatment of axial spondyloarthropathies. Front Immunol. 2020;11:591176. doi:10.3389/fimmu.2020.591176
50. Braun J, Kiltz U, Baraliakos X Emerging biological therapies in spondyloarthritides with focus on axial spondyloarthritis Expert Opin Biol Ther In press 2022
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.