")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Management of Low Back Pain in Primary Health-Care Settings: Physician’s Awareness and Practices Based on Red Flags
Authors Arishy AM, Mahfouz MS , Khalafalla HE, Atteya MME , Khormi YH
Received 29 May 2022
Accepted for publication 5 August 2022
Published 25 August 2022 Volume 2022:15 Pages 1779—1788
DOI https://doi.org/10.2147/JMDH.S375567
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Alshaymaa M Arishy,1 Mohammed Salih Mahfouz,2 Husameldin E Khalafalla,2 Mostafa ME Atteya,3 Yahya H Khormi4
1Faculty of Medicine, Jazan University, Jazan, Saudi Arabia; 2Department of Family and Community Medicine, Faculty of Medicine, Jazan University, Jazan, Saudi Arabia; 3Department of Surgery, King Fahad Central Hospital, Jazan, Saudi Arabia; 4Department of Surgery, Faculty of Medicine, Jazan University, Jazan, Saudi Arabia
Correspondence: Alshaymaa M Arishy, Faculty of Medicine, Jazan University, Jazan, Saudi Arabia, Tel +966548339496, Email [email protected]
Background: Low back pain (LBP) is one of the most common health problems. Red flags (RFs) of LBP are risk factors that are reported during clinical assessment to determine serious illness. This study aimed to assess primary health-care physicians’ knowledge of and practices for RFs of LBP and identify variables associated with a high level of knowledge and awareness about it.
Methods: An observational cross-sectional survey was conducted in 2021 among a random sample of 261 primary health care (PHC) physicians in the Jazan Region in southwest Saudi Arabia. A web-based questionnaire was used to collect data on LBP red flags awareness and practices. Descriptive (frequency and percentage) and inferential statistics were used for data analysis.
Results: The overall mean score of RFs knowledge among physicians was 82.33 ± 36.3, with 95% confidence interval (CI); (77.7– 86.9). Regarding the Physician’s practices, more than 95% of the participants would refer patients to higher levels in the presence of symptoms or signs of RFs. General practitioners and residents were significantly more likely to ask for an Xray, even with symptoms that had persisted for less than 2 weeks without RF signs (p = 0.006). The overall percentage of patients with nonspecific LBP referrals was as high as 57.8%. The number of patients with LBP seen per month (fewer than 15) and female physician were associated with an increased level of knowledge (OR = 2.2, 95%, P < 0.05) and (OR = 2.2, 95%, P < 0.05) respectively.
Conclusion: Overall, awareness of RFs for LBP and referring critical patients who present with LBP is good among PHC physicians in the Jazan Region. Junior physicians have a low threshold to request images. The referral rate for nonspecific LBP is still high, which could overwhelm spinal clinics. Further educational programs for back pain management are recommended.
Keywords: cauda equina syndrome, low back pain, spinal fractures, red flags, spinal infection, spinal tumor
Introduction
Low back pain (LBP) is one of the most common health problems and is considered the second most frequent cause for seeking medical advice,1 and the leading cause of disability and work absenteeism around the world.1 It is also a significant economic burden on individuals and communities.2 In the Kingdom of Saudi Arabia, LBP is a common condition with a prevalence ranging between 53.2% and 79.2%.3
Because of the high prevalence of LBP and the burdens it creates, many evidence-based guidelines have been established to diagnose and effectively treat patients with LBP.1 Although most cases of acute LBP are self-limiting, LBP can be an indication of more serious conditions, such as malignancy, spinal fractures, infections, cauda equina syndrome, and aortic aneurysms.1 Most of the accepted contemporary guidelines focus on the determination of the presence of red flags (RFs) of LBP.1
RFs are “signs and symptoms that raise suspicion of serious pathology”.4,5 RFs reported during a medical history or discovered during physical examination are associated with a higher prevalence of serious conditions that may be related to back pain.6 Therefore, knowing these RFs helps early diagnosis and proper management of serious conditions.7 Identifying one or more of these RFs should be followed by a proper investigation6 because neglecting these RFs can lead to serious consequences and more morbidities and higher rates of mortality.1,8
Although some RFs have been criticized because they are not supported by empirical evidence for some conditions, RFs remain the best tool for clinical screening for more serious conditions.4 A study conducted among 1172 patients with LBP found that only 0.9% had serious conditions, whereas 80.4% of these patients had at least one RF, including using corticosteroids, being over 70 years of age, and having experienced trauma.9 Moreover, studies showed that ignoring LBP management guidelines could increase mortality from serious spinal pathologies.10 Primary care physicians play an important role in the diagnosis and management of LBP because they are the first physicians to have contact with patients and, thus, they can help reduce an unnecessary workload for the specialized services.11
The southwest region of Saudi Arabia is a heavily populated region, and the health care there is stepping forward but not as in the capital and other industrial cities. This region has its own health problems that are distinctive from other regions in Saudi Arabia. Low back pain and TB are two main areas to explore and modify nowadays to provide the health care provider with valid data to modify healthcare accordingly to serve our community.12 This should include the patterns of awareness among all doctor categories, wrong or defensive practices such as un-necessary investigations or referrals, points of strength to consolidate, and management protocols for LBP in this over-populated region.
Few studies have investigated the perceptions and practices of physicians regarding RFs in patient with LBP in Saudi Arabia.7,11 However, no studies have been conducted in southwest Saudi Arabia, the intended area and population of the current study. Furthermore, in compare to other regions in Saudi Arabia, the primary health care in the study area still mostly continued to be covered by a non-family physician with different levels of training and experiences and is still missing the complimentary role of nurse practitioners and physician assistance as a frontline for screening in a common clinical presentation like back pain. This different health care setting needs to be investigated to ensure adequate levels of RF awareness and limits un-necessary diagnostic imaging and higher center referrals, we mainly aim to assess primary health care physicians’ perceptions of and practices for RFs in patients with LBP and identify the variables associated with a high level of knowledge and practice including but not limited to level of training, degree and experience. This way, we can pin-point the areas of strength and weakness in the whole process and use the awareness of LBP RF to guide us to this. The results of this work in Jazan could lead to future interventions from the health authorities to address these areas of weakness.
Materials and Methods
Study Design, Setting, and Participants
An observational cross-sectional study was conducted in the Jazan Region, in southwest Saudi Arabia, in June 2021. The target population of the study was primary care physicians working in the Jazan region. Five-hundred physicians work under the umbrella of the Ministry of Health, Jazan Health Directorate. Inclusion criteria involved all physicians working in primary health care include general physicians and family medicine doctors, who signed the informed consent form. Exclusion criteria involved doctors working for less than six months in the selected health institution.
Health-care services in Saudi Arabia, including preventive and curative services, are provided by different governmental and private sectors. However, most health-care services in the country are provided by the Ministry of Health. Saudi patients suffering from LBP can benefit from the freely available health-care services that are provided in primary health-care centres (PHCs), hospitals, and specialized centres. Nonetheless, the main context of the study was PHCs because they are the main provider of health-care services for patients affected with the targeted condition.
Sampling Procedure
The initial sample size proposed for this study was calculated to be 218 physicians; this calculation was based on the prevalence of knowledge of 50% (because no previous studies have been conducted) and a 95% confidence interval, with an error rate of less than 5% and a population size of 500. The final sample size was increased by 20% to account for nonresponders, leading to a final sample size of 261 physicians. All provinces in the Jazan region were included in the study. The list of PHC physicians in each province was obtained from the Health Affairs Directorate in Jazan. We used a stratified random sampling technique with proportional allocation to select the PHC physicians.
Data Collection and Study Instrument
Data were collected electronically through a self-reported questionnaire. The questionnaire was prepared in English as all physicians were able to communicate fluently in English, read, spoken, and written. The developed questionnaire consisted of three parts. Part one consisted of participants’ demographic factors, including their age, gender, nationality, specialty and experience, and the number of patients with back pain they encounter per month. Part two was intended to assess the awareness of participants about RFs regarding three important conditions in patients with LBP, including cauda equina syndrome, tumors/infections, and trauma. All questions were prepared to be answered with “Yes” or “No”, and “Yes” was correct. Moreover, part three was prepared to assess the practice of participants for referring to the hospital and asking for lab tests, CT scans, and MRI scans. The validity and reliability of the developed questionnaire were tested via a pilot study on a sample of 28 to test its clarity, suitability, and the time needed to complete the questionnaire. The questions were reviewed by three experts with expertise in spine specialty to assess the face validity of the instrument. Finally, the reliability of the tool was tested by estimating the Cronbach’s alpha coefficient. The estimated coefficient of items assessing knowledge and practice was 0.70, indicating an acceptable internal consistency of the measurement tool.
Data Analysis
The data was analysed using the Statistical Package for the Social Sciences (SPSS) version 20, (Chicago, IL, USA). Descriptive (frequency and percentage) and inferential statistics were used. The total score of knowledge about RFs was computed using the questions about RF knowledge. Correct answers were assigned 10 marks. Means with their standard deviation were calculated and used to describe the total knowledge. Categorical variables were described as frequency and percentage, and the chi-squared test was used to test the associations. To assess the differences in the demographics and professional backgrounds, we compared the means knowledge scores using the Student’s t-test and one-way ANOVA, respectively. A logistic regression was used to estimate odds ratios with their 95% CI for the variables associated with physicians’ knowledge. All statistical tests were 2-sided, and a p-value of < 0.05 was used to indicate statistical significance.
Study Ethics
The ethical approval to conduct the project was granted by the Jazan Health Ethics Committee, with approval number REC2040 on September 8, 2020. We conducted this study following the ethical guidelines of the Helsinki Declaration and the local guidelines of the National Committee of Bioethics, Saudi Arabia. Physicians participating in this study were informed about the purpose of the study and signed a written consent to participate before data collection. All collected data were kept confidential and used for only the purpose of research. Also, the questionnaires did not include participants’ names, mobile phone numbers, or any other methods of identification. All the participants were given the right to continue or withdraw at any time from the study.
Results
The overall response rate was 96.1%, 251 of the planned sample of 261. Table 1 illustrates the demographic information, occupational profiles, and knowledge scores of RF among physicians participating in the study. Men represented 56% of the participants; 49.4% of the participants were aged 35–44 years; and 76.9% were non-Saudi. We found that 49.4% of participants were general practitioners, 25.5% were specialists, and 23.1% were residents. Forty-nine percent of the participants had experience of 1–9 years. Furthermore, 33.1% of participants indicated they deal with more than 30 patients with back pain per month. Table 1 also showed that the overall mean score of RF knowledge among the physicians was 82.33 ± 36.3, with 95% CI (77.7–86.9). There was no statistically significant in knowledge score between women and men (85.5 ± 33.6) and (79.9 ± 38.2) respectively (p = 0.230). Neither for Consultants/specialists and physicians with experience of more than 10 years and less than 10 years 90.0 ± 28.5 and 85.7 ± 34.3 respectively, (p > 0.05). Although Physicians who see less than 15 patients in the clinic had high scores (89.0 ± 30.6) compared with those who see more than 15 patients per month (78.4 ± 38.8) (p = 0.020).
 |
Table 1 Demographic, Professional Profile, and Knowledge Scores of RFs Among Physicians Involved in the Study |
Table 2 demonstrates the Physician’s Knowledge regarding the signs of red flags. Table 1 shows that the extent of awareness of red flags of acute low back by the primary health care physicians was mainly pronounced in history of trauma (98.4%) followed by a history of cancer (98.0%), Bladder dysfunction (97.4%), Neurologic deficit in the lower extremity (93.8%), whereas the lowest appreciated red flag of acute low back pain was younger than 20 years (53.3%). There was no significant difference in physicians’ responses according to job category except for minor trauma in elderly patients and age greater than 50 years (p-value <0.05 for both). According to Figure 1, we found that 88.1% of participants had good awareness of the RFs for cauda equina syndrome, whereas 92.7% did for tumors/infections and 86.2% did for trauma.
 |
Table 2 Physicians’ Knowledge Regarding the Signs and Symptoms of Red Flags |
 |
Figure 1 Primary health care physician’s awareness of serious LBP red flags domains. |
The overall percentage of referring patients with back pain is 10.6%, and the rate of referral is highest among general practitioners, followed by residents, specialists, and consultants. General practitioners and residents are more likely to refer patients with nonspecific back pain than specialists and consultants. Fortunately, more than 95% of participants would refer patients to the hospital if they noticed the presence of RFs. Specialists and consultants refer cases with osteoarthritis at a significantly lower rate than general practitioners and residents (p = 0.001) (Table 3).
 |
Table 3 Primary Health Care Physicians’ Practices Regarding the Red Flags |
Moreover, 93.6% and 90.8% of physicians would ask for laboratory tests in the case of tuberculosis (TB) infection or if suspecting there were rheumatological diseases, respectively, with no significant difference among different types of physicians. Furthermore, we found that 94.5% of participants would ask for an Xray when acute back pain persists for more than 2 weeks with RFs; 65.1% would ask for an Xray when acute back pain persists for more than 2 weeks without RFs; and 28% would ask for an Xray when acute back pain persists for less than 2 weeks without RF signs. General practitioners and residents were significantly more likely to ask for an Xray, even for symptoms that persist for less than 2 weeks without RFs (p = 0.006) (Table 2).
Considering computed tomography (CT), we found that most participants would ask for CT in cases of metastatic disease (92.7%), extra-spinal pathology (87.6%), and a cauda equina lesion (82.1%). General practitioners were more likely than other physicians to ask for a CT scan in patients with a nerve root or spinal cord compression. Moreover, we found that 93.1% of participants would ask for magnetic resonance imaging (MRI) in cases of a cauda equina lesion; 92.7% would ask for one in cases of nerve root/cord compression; and 84.4% would ask for one for metastatic conditions (Table 3). The percentage of physicians who will order a CT or MRI for patients with suspected infection are 46.8% and 42.2%, respectively. The overall percentage of referrals of patients with nonspecific LBP is considered high (57.8%).
A logistic regression analysis was conducted using the dependent variable level of PHC physicians’ knowledge that is categorized into two categories: high and low levels of knowledge. The analysis revealed the female gender was associated with a high level of knowledge (OR = 2.2, 95% CI = 2.3–4.8, P < 0.05). The number of patients with back pain seen per month (fewer than 15) was also associated with an increased level of knowledge (OR = 2.2, 95% CI = 1.1–4.5, P < 0.05). Being a consultant/specialist and older were not associated with higher knowledge (p-value > 0.05 for all) (Table 4).
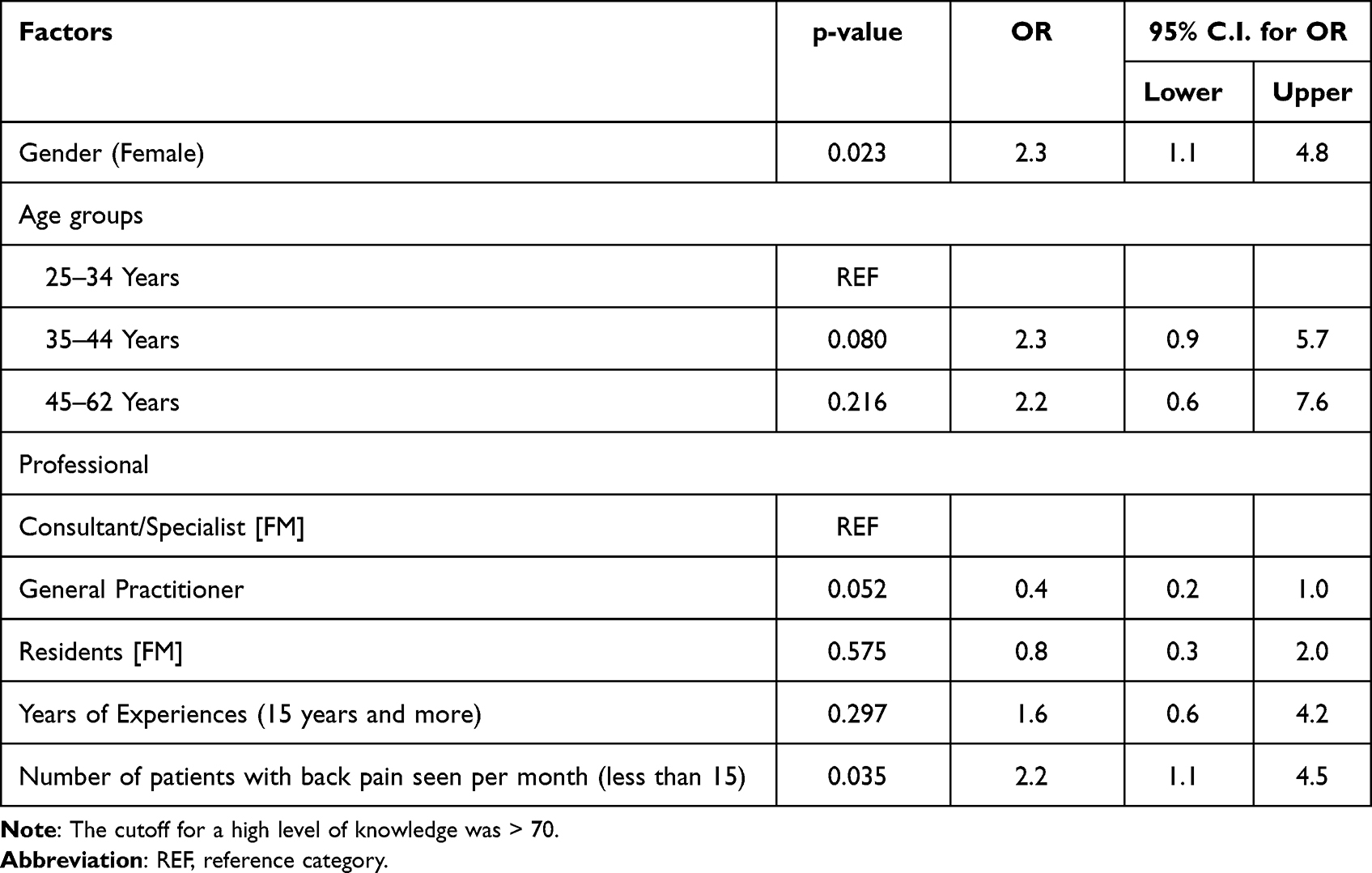 |
Table 4 Factors Associated with a High Level of RF Knowledge Using the Logistic Regression Model |
Discussion
Identification of serious pathological conditions among patients with LBP is a high-priority health issue worldwide. Reasonable tools should guide physicians to detect and triage those with potentially serious conditions among the large pool of patients with low back pain. It is important to avoid providing patients with false reassurance when they have critical conditions and exaggerating simple ones.4 This balance requires a certain level of knowledge and experience among the treating physicians, and ideally, a RF-based assessment method with reasonable sensitivity and specificity would help achieve this goal.
Acute LBP bouts are usually nonspecific and tend to be self-limiting with time. History and physical examination alone could provide reliable clues to detect serious etiologies of LBP.6 This concept constituted the basis on which different diagnostic roadmaps were designed. Because the knowledge and the level of experience determine the outcome of patient care, the authors focused on the assessment of health-care providers’ awareness of different levels of RFs, which highlight serious spine pathologies such as cancer, infections, and fractures.
In this study, we found that the physician’s overall mean score of RF knowledge was 82.33 ± 36.3, which indicates a good level of awareness about RFs in patients with LBP in compare to other studies conducted in Saudi Arabia.1,7 Moreover, 94.5% were aware they should order X-rays for patients who were symptomatic for more than 2 weeks despite being dedicated to conservative medical treatment. The study also showed a comparable high awareness level regarding the proper radiological investigations in cases of suspected cauda equina syndrome, metastatic diseases, radiculopathy, and extraspinal pathologies.
A study conducted in Riyadh, central region of Saudi Arabia, to assess the level of knowledge of PHC physicians about RFs for patients with LBP, it was found that most physicians (68%) had good knowledge of RFs, including neurological deficits (72%), age (45%), and history of spinal trauma (41%). However, only 30% would suspect these signs in acute cases.1
Another study conducted in Jeddah, western region of Saudi Arabia, in 2014 to assess the level of knowledge and practice of physicians found that among 180 physicians, bladder dysfunctions were the most known RF at 83.9%, an age of over 50 years was recognized by 77%, a history of trauma was recognized by 73.3%, and weight loss as a RF for acute LBP was known by 68.9%, which is lower than the level of knowledge of this study participants. Acute pain for less than 2 weeks was not recognized by most of the sample. Moreover, the consultants seem to have a higher level of knowledge than general practitioners.7
The southwest region of Saudi Arabia is a heavily populated region, and the health care there is stepping forward but not as in the capital and industrial cities. This region has its own health problem that is distinctive from other regions in Saudi Arabia.12
Due to differences in healthcare conditions and health problem of Jazan, we will utilize the results and conclusions of this work to consolidate areas of strength and improves areas with low awareness, modify the management process to limit unnecessary referrals to higher centers and improve the diagnostic image utilization profile by providing these conclusions to local health authorities and planning future training programs to improve management of these patients in our over-populated region.
Considering practices for RFs in patients with LBP, we found physicians would refer patients if they had osteoarthritis symptoms. Moreover, tuberculosis is a possible cause of LBP, and back pain is the main symptom of spinal tuberculosis; the intensity of pain varies from constant and mild aching to severely disabling pain that is generally localized to the thoracic region.13 In our study, 93.6% of physicians would ask for lab tests if they suspected TB and 90.8% if they suspected rheumatological diseases.
Radiography may not be useful in determining the cause of LBP complaints because it can assess only the bone.14,15 Diagnostic tests such as a CT or MRI should be performed in patients with a history or who have received an examination that strongly indicates a serious cause of back pain, such as cauda equina syndrome, infections, or tumors. Early imaging is not required in patients whose sciatica is likely due to a herniated disc or spinal stenosis unless significant neurological abnormalities are identified. Early imaging is not required because many patients will improve with conservative treatment.6,16,17
Moreover, in another study, it was found that 26.9% of physicians would manage cases of LBP without sciatica and 4.3% of physicians manage cases of LBP with sciatica by following the Agency for Healthcare Research and Quality guidelines for back pain. However, most PHC physicians are noncompliant with this guidelines.18 These results showed that physicians in our sample had good knowledge and awareness of RFs for LBP, although they are over-investigating patients and making early referrals for patients with non-specific and short-duration low back pain in the absence of RFs, in particular among the junior physician which may reflect a low level of experience and confidence which may need future interventions from the health authorities to address these areas of weakness.
Study Limitations
This study is a cross-sectional based on self-reported questionnaires, which has its limitations and potential biases, the external generalizability of the study result is limited to Jazan region as well as similar health care settings worldwide.
Implication for Clinical Practice
This study is the first to assess the awareness of physicians in PHC settings about RFs for LBP in the Jazan Region, Southwest Saudi Arabia. This study, demonstrate a high level of awareness and knowledge of the RFs for LBP among PHC physicians, although they have a very low threshold for referring LBP patients to the specialized clinics and for requesting investigations specially among junior physicians. This kind of attitude and practice overwhelms spine clinics by unnecessary consultations and increases the waiting time which may affect patients with a serious spine disease. Further educational programs and courses with a focus on junior physicians are needed based on this study result. To enhance their practice to be able to diagnose and manage a non-specific LBP and minimize the unnecessary and premature referral to spine clinics.
We will utilize the results and conclusions of this work to consolidate areas of strength and improves areas with low awareness, modify the management process to limit unnecessary referrals to higher centers and improve the diagnostic image utilization profile.
Conclusion
Overall, awareness of RFs for LBP and referring critical patients who present with low back pain is good among primary health care (PHC) physicians in the Jazan Region. Junior physicians have a low threshold to request images. The referral rate for nonspecific LBP is still high, which could overwhelm spinal clinics. Further educational programs for back pain management are recommended to ensure adequate levels of RF awareness and limits un-necessary diagnostic imaging and higher center referrals.
Abbreviation
CT, Computed tomography; LBP, Low back pain; MRI, Magnetic resonance imaging; PHCs, Primary healthcare centers; RF, Red flags; TB, Tuberculosis.
Ethical Approval
The ethical approval to conduct the project was granted from the Jazan Health Ethics Committee with approval number REC2040. We conducted this study following the ethical guidelines of the Helsinki Declaration and the local guidelines of the National Committee of Bioethics, Saudi Arabia.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The abstract of this paper was presented at the Saudi Association of Neurological Surgery, SANS Conference as a poster presentation with interim findings. The poster’s abstract was Published as “Poster Abstracts” in the Spine Practice Journal: [https://doi.org/10.18502/jsp.v1i1.9780]. The authors report no conflicts of interest in this work.
References
1. Alsaleh K, Alluhaidan A, Alsaran Y, et al. Acute back pain: a survey of primary health care physicians′ awareness and knowledge of “red flag” signs. Saudi J Med Med Sci. 2016;4(1):15. doi:10.4103/1658-631x.170882
2. Hoy D, March L, Brooks P, et al. The global burden of low back pain: estimates from the Global Burden of Disease 2010 study. Ann Rheum Dis. 2014;73(6):968–974. doi:10.1136/annrheumdis-2013-204428
3. Awaji M. Epidemiology of low back pain in Saudi Arabia. J Adv Med Pharm Sci. 2016;6(4):1–9. doi:10.9734/jamps/2016/24173
4. Finucane LM, Downie A, Mercer C, et al. International framework for red flags for potential serious spinal pathologies. J Orthop Sports Phys Ther. 2020;50(7):350–372. doi:10.2519/jospt.2020.9971
5. Pennella D, Giagio S, Maselli F, et al. Red flags useful to screen for gastrointestinal and hepatic diseases in patients with shoulder pain: a scoping review. Musculoskeletal Care. 2022. doi:10.1002/msc.1628
6. Atlas SJ, Deyo RA. Evaluating and managing acute low back pain in the primary care setting. J Gen Intern Med. 2001;16(2):120–131. doi:10.1046/j.1525-1497.2001.91141.x
7. Alghamdi M, Mattar A, Yamani O. Assessment of knowledge, attitude and practice of red flags related to acute low back pain among primary health care physician, ministry of health, Jeddah 2013–2014. Int J Adv Res. 2016;4(12):1809–1816. doi:10.21474/ijar01/2586
8. Maselli F, Palladino M, Barbari V, Storari L, Rossettini G, Testa M. The diagnostic value of Red Flags in thoracolumbar pain: a systematic review. Disabil Rehabil. 2022;44(8):1190–1206. doi:10.1080/09638288.2020.1804626
9. Henschke N, Maher CG, Refshauge KM, et al. Prevalence of and screening for serious spinal pathology in patients presenting to primary care settings with acute low back pain. Arthritis Rheum. 2009;60(10):3072–3080. doi:10.1002/art.24853
10. Major-Helsloot ME, Crous LC, Grimmer-Somers K, Louw QA, Major-Helsloot ME, Grimmer-Somers K. Management of LBP at primary care level in South Africa: up to standards? Afr Health Sci. 2014;14(3):698–706. doi:10.4314/ahs.v14i3.28
11. Albahlal JM, Alhandi AA, Aldihan KA, et al. Primary healthcare physicians’ adherence to acute lower back pain referral guidelines in Riyadh, Saudi Arabia. Saudi Med J. 2018;39(8):838–841. doi:10.15537/smj.2018.8.22539
12. Alnaami I, Awadalla NJ, Alkhairy M, et al. Prevalence and factors associated with low back pain among health care workers in southwestern Saudi Arabia. BMC Musculoskelet Disord. 2019;20(1):1–7. doi:10.1186/s12891-019-2431-5
13. Garg RK, Somvanshi DS. Spinal tuberculosis: a review. J Spinal Cord Med. 2011;34(5):440–454. doi:10.1179/2045772311Y.0000000023
14. Van Tulder MW, Assendelft WJJ, Koes BW, Bouter LM. Spinal radiographic findings and nonspecific low back pain: a systematic review of observational studies. Spine. 1997;22(4):427–434. doi:10.1097/00007632-199702150-00015
15. Rao D, Scuderi G, Scuderi C, et al. The use of imaging in management of patients with low back pain. J Clin Imaging Sci. 2018;8(1):30. doi:10.4103/jcis.JCIS
16. Mathews JA. Back pain and sciatica. Rheumatology. 1988;27(4):331. doi:10.1093/rheumatology/27.4.331
17. Deyo RA, Bigos SJ, Maravilla KR. Diagnostic imaging procedures for the lumbar spine. Ann Internal Med. 2017;111(11):865–867.
18. Webster BS, Courtney TK, Huang YH, Matz S, Christiani DC. Brief report: physicians’ initial management of acute low back pain versus evidence-based guidelines. Influence of sciatica. J Gen Intern Med. 2005;20(12):1132–1135. doi:10.1111/j.1525-1497.2005.0230.x
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.