")
Back to Journals » Psoriasis: Targets and Therapy » Volume 13
Management of Plaque Psoriasis in Adults: Clinical Utility of Tapinarof Cream
Authors Spencer RK, Jin JQ , Elhage KG, Davis MS, Liao W , Bhutani T
Received 13 September 2023
Accepted for publication 16 October 2023
Published 25 October 2023 Volume 2023:13 Pages 59—69
DOI https://doi.org/10.2147/PTT.S393997
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Uwe Wollina
Riley K Spencer,1,2 Joy Q Jin,2,3 Kareem G Elhage,2 Mitchell S Davis,2 Wilson Liao,2 Tina Bhutani2
1Arizona College of Osteopathic Medicine, Midwestern University, Glendale, AZ, USA; 2Department of Dermatology, University of California at San Francisco, San Francisco, CA, USA; 3School of Medicine, University of California at San Francisco, San Francisco, CA, USA
Correspondence: Riley K Spencer, Department of Dermatology, University of California at San Francisco, Box 1212, Floor 01, Room 101, 2340 Sutter Street, San Francisco, CA, 94115, USA, Tel +1 480 415 7224, Fax +1 415 502 4126, Email [email protected]
Abstract: Topical medications represent the most commonly used drugs in the treatment of psoriasis. However, topical steroids are mainly limited to short-term or intermittent use, and traditional non-steroidal topicals such as vitamin D analogues, topical calcineurin inhibitors, and topical retinoids are limited by low efficacy and poor local skin tolerability. Tapinarof (GSK2894512, DMVT-505) is a novel, topical aryl hydrocarbon receptor (AHR) agonist, which was recently approved by the FDA for the treatment of plaque psoriasis in adults. Tapinarof acts to improve psoriasis through diminished IL-17A production by CD4+ T cells, increased barrier gene expression in keratinocytes, and reduced production of reactive oxygen species. Both short-term and long-term efficacy and safety have been evaluated in two Phase II and two Phase III (PSOARING 1 and 2) clinical trials in addition to a long-term extension study (PSOARING 3). Overall, the drug has shown beneficial effects in achieving clear skin in adults with moderate-to-severe psoriasis, good local tolerability, and also a long duration of effect even after discontinuation of the drug. Therefore, this therapy provides a new, highly effective and safe non-steroidal option to add to our psoriasis treatment toolbox for both initial clearance and long-term maintenance of disease.
Keywords: tapinarof, vtama, psoriasis, PSOARING
Introduction
Psoriasis is a chronic, inflammatory disorder of the skin, nails, and joints that affects 3% of the US population.1 Psoriasis vulgaris represents the most common morphology and presents clinically with well-demarcated, erythematous plaques with overlying hyperkeratotic scale. Psoriasis may be painful, pruritic, and often causes detriments to the physical and psychosocial health of affected patients.2 Various treatment options for the management of psoriatic disease exist such as topicals, phototherapy, oral systemic agents, and injectable biologics.3 There has been prominent evolution in the treatment landscape of psoriasis, especially for biologic agents used to treat moderate-to-severe disease. However, for a variety of reasons including limited disease area or patient preference, biologic agents are not always preferred. Instead, topical medications, like corticosteroids, are the most commonly used treatments.3 However, limitations to the consistent use of these therapies exist. For example, use of high potency steroids needs to be avoided in areas like the face and intertriginous regions.4 Further, the potential for adverse effects with prolonged use (eg, steroid atrophy) limit the duration of use.4 Despite most patients with psoriasis having only mild, localized disease and not requiring treatment with oral systemic or biologic agents, the selection of available topical medications has remained mostly limited.3 Accordingly, advancements in the treatment of psoriasis in the form of new topical treatments are needed.
A novel topical treatment named tapinarof (GSK2894512, DMVT-505, VTAMA™) has been recently developed and was approved by the FDA in May 2022 for the treatment of plaque psoriasis in adults.5 Here, we review the clinical utility of tapinarof (ie, GSK2894512, DMVT-505), a novel, first-in-class, topically administered, small-molecule modulator of the aryl hydrocarbon receptor in the treatment of psoriasis.6
AHR Signaling in the Skin and Tapinarof’s Mechanism of Action
The aryl hydrocarbon receptor (AHR) is a ligand-dependent transcription factor that resides in the cytoplasm of various cell types.7 All cell types within the skin ubiquitously express AHR including keratinocytes, fibroblasts, melanocytes, endothelial cells, Langerhans cells, and lymphocytes (including CD4+, T-helper 17 (Th17) cells).8,9 In healthy skin, AHR serves as a chemical receptor, responding to ligands from endogenous sources like tryptophan photo-derivatives generated from ultraviolet light exposure, and exogenous sources like polycyclic aromatic hydrocarbons (PAHs) in smoke and indole derivatives produced by resident skin micro-organisms.9 AHR responds to this variety of ligands and maintains homeostasis within the skin, mediating end-organ effects including epidermal barrier maintenance, regulation of keratinocyte differentiation, skin pigmentation, and response to oxidative stress.10,11
AHR signaling represents a complex pathway composed of two primary signaling arms (canonical and non-canonical), which are influenced by many factors such as ligand identity, dimerization partner, and duration of AHR activation.12 Ligand binding to AHR may occur directly or indirectly, upon which AHR dissociates from its cytosolic multiprotein complex to translocate to the nucleus where it may then bind various dimerization partners to influence gene transcription.13 Canonical signaling refers to AHR dimerization with AHR nuclear translocator (ARNT), whereas non-canonical AHR signaling refers to AHR dimerization with partners including epidermal growth factor receptor (EGFR), mitogen-activated protein kinase (MAPK), NF-κB, and signal transducer and activator of transcription (STATs).12 In healthy skin, AHR is constitutively active with a balance between canonical and non-canonical activity, in turn helping to maintain skin homeostasis via the promotion of epidermal terminal differentiation and enhancement of repair of barrier disruptions through upregulation of structural proteins like filaggrin, loricrin, and involucrin.14,15
Imbalances in AHR signaling have been implicated in the pathogenesis of various cutaneous diseases including skin cancer, and inflammatory skin diseases like psoriasis and eczema.8 Dominance of canonical signaling (ie, overactivation of AHR-ARNT), which may occur in scenarios of excessive UVB exposure, is thought to induce carcinogenesis and propagate tumor formation via the negative regulation of apoptosis in UVB damaged keratinocytes and induction of matrix metalloproteases.12,16–18 AHR’s role in the development of skin cancer is supported by a reduced incidence of cutaneous squamous cell carcinoma in animal models with AHR knockdown.19 As such, inhibition of AHR-ARNT activity in the setting of high exposure to UVB may have an anti-photocarcinogenesis effect. On the other hand, dominance of non-canonical AHR signaling leads to impaired keratinocyte differentiation, defects in epidermal barrier function, and oxidative stress, designating it as a potential target in the treatment of inflammatory skin conditions.12
Involvement of AHR in psoriasis pathogenesis is supported by numerous findings, including elevated levels of AHR in the serum of patients with psoriasis relative to healthy controls.20
Interestingly, the dose and duration of AHR activation are important in the regulation of inflammation and may dictate immunophenotypes and cytokine expression profiles within cutaneous diseases like psoriasis. An experiment by Ehrlich et al demonstrated that high doses of high-affinity AHR ligands (6-formylindolo [3,2-b] carbazole (FICZ)) increased Treg cell number (responsible for production of anti-inflammatory cytokines like interleukin (IL)-10).21 In contrast, low doses of these same ligands led to increased production of IL-17, a cytokine which is centrally involved in psoriatic disease pathogenesis and the target of multiple available biologic medications.21,22 Psoriasis patients treated with the high-affinity AHR ligand FICZ demonstrated reductions in psoriasis-related gene transcription, which was most pronounced within psoriatic lesions.23 In contrast, patients treated with an AHR antagonist had increased transcription of psoriasis-related genes in non-lesional skin.23 In animal models of psoriasis, AHR deficiency resulted in exacerbations of imiquimod-induced psoriasiform skin inflammation, with significantly increased expression of IL-17 and IL-23 versus controls.23 Given these findings, AHR was designated as a potential therapeutic target for the treatment of psoriasis. In fact, modulation of AHR may represent the therapeutic mechanism of action of coal tar, one of the oldest known treatments for psoriasis.24
Tapinarof is a small-molecule modulator of AHR, which binds directly to AHR within keratinocytes and T-lymphocytes, as demonstrated by in situ fluorescence and gene expression assays.25 Molecular profiling of cellular targets of tapinarof revealed potent interactions of AHR with nuclear factor-erythroid 2-related factor-2 (Nrf2).25 AHR activation by tapinarof was shown to result in increased barrier gene expression in keratinocytes, an altered immunophenotype with dose-dependent reductions in IL-17A production by CD4+ T-cells and marked reductions in chemically induced reactive oxygen species.25 With regard to barrier gene expression, transcriptional activation of OVO-like 1 (OVOL1) via tapinarof mediated AHR activation leads to increased production of filaggrin, loricrin, and involucrin.25 Tapinarof’s mechanism of action within in the skin may also include antimicrobial effects towards gram-positive bacteria and fungi, leading to an altered microbiome.26
Materials and Methods
A literature search was conducted in PudMed (MEDLINE), Embase, and the Cochrane Central Register of Controlled Trials (CENTRAL) in April 2023 using a combination of the terms (“tapinarof” OR “vtama”) AND (“psoriasis”). All data used were non-identifiable and publicly available. Institutional review board approval was not required at the University of California, San Francisco. This study protocol and design are reported according to the Preferred Reporting Items for Systematic Review and Meta-Analysis Protocols 2020 Guidelines.27
Study Design and Eligibility Criteria
Studies included in this review were randomized controlled trials (RCTs) investigating human subjects with psoriasis (Phase II–IV trials) treated with tapinarof, as well as Phase I trials investigating the pharmacokinetics and biodistribution of tapinarof in subjects without plaque psoriasis. Excluded trials were phase II–IV trials not investigating subjects with psoriasis. Study characteristics including clinical trial name/number, number of patients, intervention dose and duration, clinical efficacy, and safety outcomes were obtained using a standardized table tailored to this review.
Outcomes of phase II–IV studies included in this review reported standardized, objective disease severity metrics including the Psoriasis Area and Severity Index (PASI), Physician Global Assessment (PGA), and Body Surface Area (BSA). Concomitant assessments of psychosocial health and quality of life with the Dermatology Life Quality Index (DLQI) were also reported. Pharmacokinetic properties reported in phase I studies included maximum serum concentration (Cmax) and median time to reach Cmax (Tmax).
Study Selection and Data Extraction
Initial screening of studies was performed manually by three independent reviewers (R.K.S., J.Q.J, K.G.E). Any queries in eligibility criteria were resolved via adjudication by an additional reviewer (T.B.). Data abstraction was performed by three independent reviewers (R.K.S., J.Q.J., K.G.E.). All randomized studies included for analysis were assessed for risk of bias by two independent authors (R.K.S., J.Q.J) using the Critical Appraisal Skills Programme (CASP) checklist for RCTs.28 Primary and secondary outcomes were defined and reported as in the corresponding clinical trials.
Results
Five clinical trials were included for review following the application of inclusion and exclusion criteria (Figure 1), including six phase I trials,29–31 one phase IIa trial (NCT04042103),32 one phase IIb vehicle-controlled RCT (NCT02931838),33–35 and two phase III vehicle-controlled RCTs (PSOARING 1 and PSOARING 2),36 and the corresponding long-term-extension period study (PSOARING 3).37,38 A total of 1273 patients with moderate-to-severe psoriasis—including 818 treated with tapinarof and 455 who received vehicle cream. Overall, patients treated with tapinarof showed marked improvement in disease severity and quality-of-life outcomes compared to those receiving vehicle (Table 1).
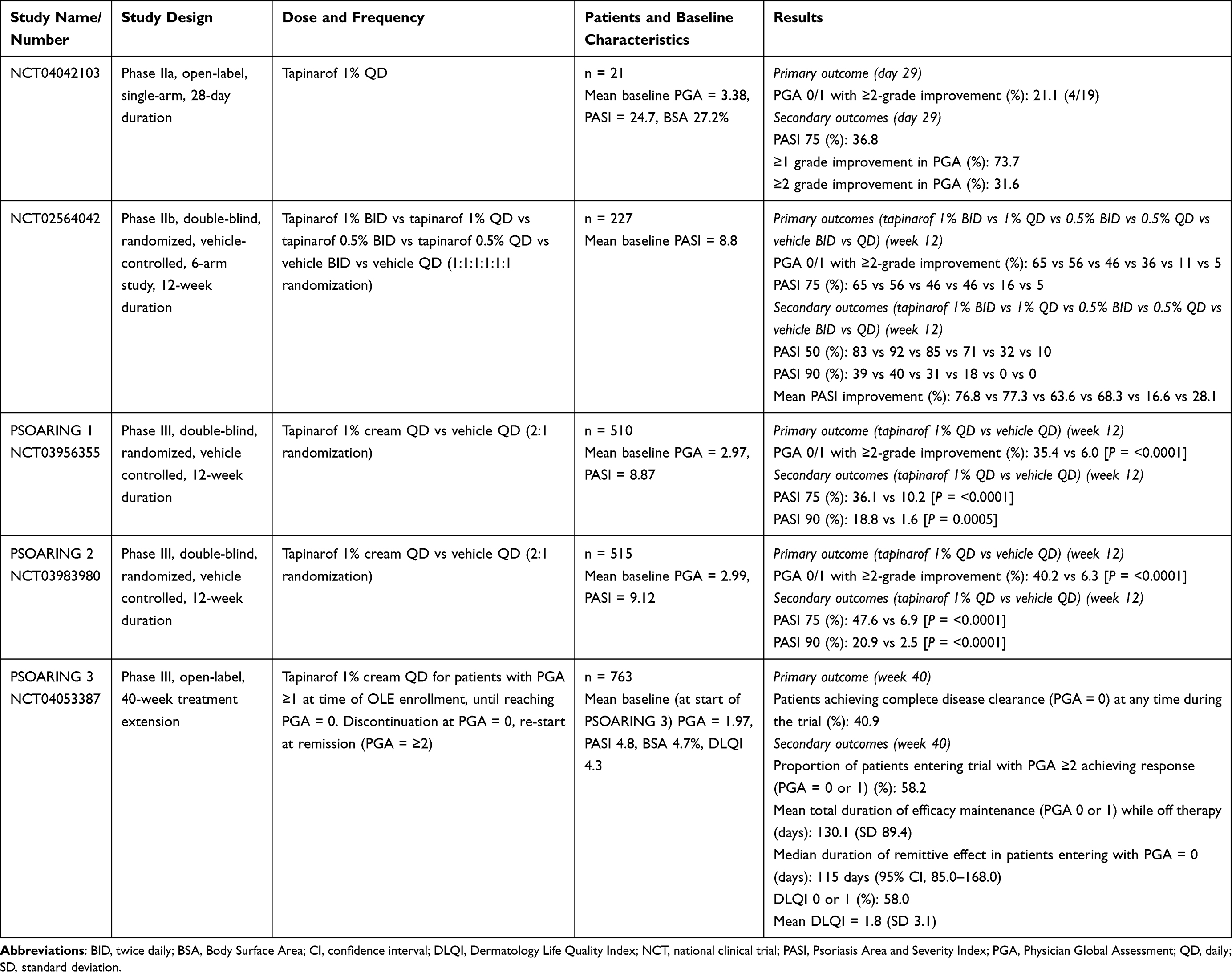 |
Table 1 Efficacy of Tapinarof in Plaque Psoriasis Across Clinical Trials |
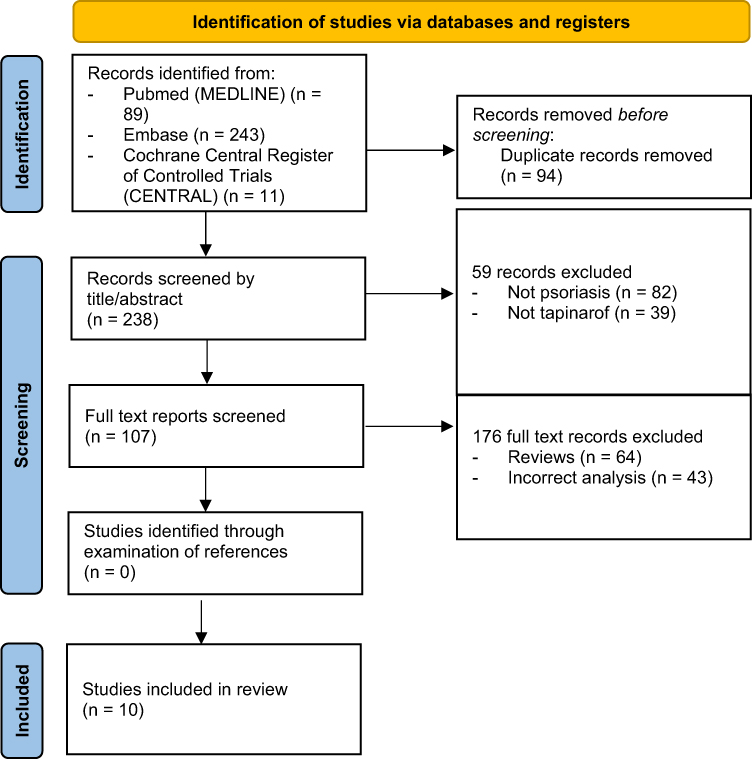 |
Figure 1 PRISMA diagram detailing identification of studies. |
Pharmacokinetics and Biodistribution
Regarding metabolism, preclinical animal model and human cell line studies demonstrated that hepatic cytochrome (CYP) P450 enzymes are primarily responsible for the oxidative metabolism of tapinarof.29 Namely, CYP1A2 and CYP3A4 with minor contributions from CYP2C9, CYP2C19, CYP2C20, and CYP2D6 are the major enzymes responsible for tapinarof’s metabolism.29
A phase IIa, open-label study (NCT04042103) evaluated the pharmacokinetic profile of tapinarof 1% cream applied once daily in patients with plaque psoriasis (n = 21).32 The mean maximum serum concentration (Cmax) of tapinarof and tapinarof sulfate (metabolite) was 898.3 pg/mL at day 1, decreasing to 116.1 pg/mL by day 29.32 The decreasing Cmax over time following repeated exposure demonstrated that there is no serum accumulation with regular drug administration. Mean time to reach Cmax (Tmax) was 4.39 and 4.02 hours at days 1 and 29, respectively.32 The elimination half-life (T½) could not be determined in 90.5% of the subjects at Day 1 and all subjects at Day 29 due to the lack of detectable tapinarof in plasma samples in the elimination phase.32
A phase I clinical trial investigated the spatial biodistribution and residency of tapinarof 1% cream following application to the bilateral forearms on 7 consecutive days.31 Fluorescent lifetime imaging microscopy (FLIM) demonstrated that most of the topical cream applied remained in the subcutaneous layer and accumulated along ridges of the skin.31 By day 10, there was no detectable fluorescence from tapinarof residing within the skin.31
Efficacy
The individual study name and number, study design, drug dose and administration frequency, patient baseline characteristics, and efficacy outcomes of the included RCTs are detailed in Table 1.
In a phase IIa (NCT04042103), open-label, single-arm trial, the efficacy of tapinarof 1% cream applied daily (QD) for 28 days was assessed in patients with moderate-to-severe plaque psoriasis (mean baseline PGA 3.38, PASI 24.7, BSA 27.2%) (n = 21).32 At day 29, 21.1% of the patients met the criteria for treatment success (defined as a PGA of 0 or 1 with a ≥2-grade improvement from baseline) after a 4-week treatment period.32 A ≥1 and ≥2 grade improvement in PGA was observed in 73.7% and 31.6% of the patients, respectively.32 A 75% improvement from baseline PASI (PASI 75) was achieved in 36.8% of the patients.32
A 12-week, phase IIb (NCT02564042), double-blind, randomized, vehicle controlled, 6-arm study investigated the use of tapinarof in two concentrations (0.5% and 1%) with two application frequencies (daily or twice daily (BID)).33 A total of 227 patients (mean baseline PASI 8.8) were enrolled and randomized 1:1:1:1:1:1 to receive tapinarof 1% cream BID, tapinarof 1% QD, tapinarof 0.5% BID, tapinarof 0.5% QD, vehicle BID, or vehicle QD.33 For those receiving the now FDA-approved dose of tapinarof (1% cream QD), 56% achieved both a PGA of 0/1 and PASI 75 at week 12 versus 5% in the vehicle QD cohort [P = <0.001].33 Outcomes of the differing concentration and application frequencies are shown in Table 1. Mean PASI reduction at week 12 was 77.3% in the tapinarof 1% QD versus 28.1% in the vehicle QD group.34 A 50% improvement from baseline PASI (PASI 50) was achieved by 92% of the patients receiving tapinarof cream 1% QD by week 12 versus 10% in the vehicle QD cohort [P = <0.001].34 Forty percent of patients receiving tapinarof 1% cream QD achieved a 90% improvement from baseline PASI (PASI 90) by week 12 compared to 0% of the patients receiving the vehicle cream [P = 0.001].34 Upon secondary analysis, tapinarof cream demonstrated consistent efficacy across different body regions (upper and lower extremities, trunk, head, and neck) and Fitzpatrick skin types.35
PSOARING 1 (NCT03956355) and PSOARING 2 (NCT03983980)36 were both 12-week, Phase III, double-blind, randomized, vehicle-controlled studies which included an optional 40-week open-label extension period (PSOARING 3).37 A total of 510 patients with moderate-to-severe plaque psoriasis (mean baseline PGA 2.97, PASI 8.87) were randomized in PSOARING 1, with 340 receiving tapinarof 1% cream QD, and 170 receiving vehicle.36 At week 12, patients receiving tapinarof achieved the primary outcome (PGA 0 or 1 with a ≥2 grade improvement) at a rate of 35.4% versus 6.0% of those receiving vehicle [P = <0.0001].36 Secondary outcomes included PASI 75 and PASI 90, which were achieved by 36.1% and 18.8%, respectively, of patients receiving tapinarof, versus 10.2% [P = <0.0001] and 1.6% [P = 0.0005] of those receiving vehicle.36 In PSOARING-2, 515 patients with moderate-to-severe plaque psoriasis (mean baseline PGA 2.99, PASI 9.12) were randomized to receive tapinarof 1% cream QD (n = 343) or placebo (n = 172).36 A significantly greater number of patients receiving tapinarof achieved PGA 0 or 1 with a ≥2 grade improvement (40.2% vs 6.3% [P = <0.0001]), PASI 75 (47.6% vs 6.9% [P = <0.0001]) and PASI 90 (20.9% vs 2.5% [P = <0.0001]) compared to those receiving the vehicle cream.36
Patients who completed the 12-week trial in PSOARING 1 or PSOARING 2 were eligible to participate in PSOARING 3 (NCT04053387), a 40-week open-label extension period.37 Of the 833 eligible patients (mean baseline at start of PSOARING 3: PGA 1.96, PASI 4.8, BSA 4.7%), 91.6% elected to participate in PSOARING 3 (n = 763).37 Treatment with tapinarof 1% cream QD was based on the patient’s PGA score, whereas patients with a PGA ≥1 received tapinarof until achieving clearance (PGA = 0). Upon achieving clearance, patients discontinued tapinarof and were monitored for remittive effect. In those experiencing relapse of disease (PGA ≥2) following discontinuation of tapinarof, these patients were re-treated until achieving clearance again. Continued treatment with tapinarof resulted in 40.9% of the patients achieving disease clearance (PGA = 0) at least once from the start of PSOARING 1 and PSOARING 2 to the end of PSOARING 3.37 For patients entering the open-label extension period with a PGA ≥1 (n = 680) or ≥2, 34.3% and 58.2%, respectively, achieved disease clearance at least once.37 Additionally, duration of remittive effect off-therapy (defined as time sustaining PGA = 0 or 1 while off tapinarof treatment) of tapinarof cream was examined in patients who discontinued tapinarof after achieving disease clearance. The mean duration of off-therapy remittive effect for patients achieving disease clearance (n = 312) was 130.1 days.37 No evidence of tachyphylaxis (ie, diminishing response to repeated drug administration) was demonstrated for up to 52 weeks.37 Regarding patient reported outcomes, mean Dermatology Life Quality Index (DLQI) scores at baseline in PSOARING 1/2 and PSOARING 3 were 8.5 and 4.3, respectively.38 By week 40, 68.0% of the patients reported a DLQI of 0/1 (n = 540), including a mean total DLQI score of 1.8 (SD 3.1).38 Reductions in mean DLQI scores were observed for every domain assessed in the DLQI (symptoms and feelings, daily activities, leisure, work and school performance, personal relationships, and treatment).38
Safety and Tolerability
Four phase I controlled trials were conducted which assessed for the cumulative skin irritation, sensitization, photosensitization, and phototoxicity potential of tapinarof 1% cream.30 Tapinarof was compared to vehicle, 0.2% sodium lauryl sulfate (SLS, positive control), and 0.9% saline (negative control). These trials included a total of 376 participants, the majority of which had Fitzpatrick skin types III–V.30 The mean irritation score was 0.92 for tapinarof 1% cream (n = 45) versus 0.02 for vehicle, 0.1 for 0.9% saline, and 2.45 for SLS [P = <0.0001 for all comparisons].30 Based on tapinarof’s normalized total irritation score (193/630), it was classified as having a slight potential for very mild cumulative irritation.30 Of the patients assessed for skin sensitization (n = 240), no reactions were classified as indicative of sensitization to tapinarof cream, including 38.7% of the patients experiencing minimal, barely perceptible erythema (maximum sensitization score 1), 1.7% experiencing definite erythema and minimal edema/papulation (maximum sensitization score 2), and 0.4% experiencing definite erythema, edema, papules and/or a strong reaction spreading beyond test site (maximum sensitization score 3).30 Fifty-eight patients were assessed for photoallergy, of which the maximum photosensitization score observed was a score of 1 (mild erythema/edema) for both irradiated and non-irradiated sites treated with tapinarof 1% cream or vehicle.30 Thirty-three patients were assessed for phototoxicity, with no evidence of phototoxicity observed, including a lower mean dermal response (0.14, 0.17, and 0.20 respectively) observed in irradiated sites treated with tapinarof or vehicle, or untreated sites.30 Across these four trials, tapinarof was classified as having a very mild cumulative irritation with no evidence of sensitization, photosensitization, or phototoxicity.30
In the phase IIa trial (NCT04042103), 90.5% of the patients completed the trial (n = 21), with the two discontinuations due to loss of follow-up and study withdrawal.32 The most frequently observed treatment emergent adverse events (TEAEs) were folliculitis (19.0%), headache (19.0%), back pain (9.5%) and pruritus (9.5%), though none led to discontinuation of tapinarof.32 Cardiac effects were nonsignificant, with no relationship being observed between plasma tapinarof concentration and QTc.32
In the phase IIb trial (NCT02564042), 81.6% of the patients receiving tapinarof completed the trial (n = 152).33 Of the patients not completing the trial, 39.3% were due to adverse events and 42.9% were due to withdrawal by subject.33 Patients treated with tapinarof (56%, n = 152) experienced more TEAEs than those receiving vehicle (25%, n = 75).33 The rate of serious adverse events (SAE’s) was greater in those receiving tapinarof versus vehicle (4.6% vs 0.0%).33 The most commonly observed adverse effects in patients receiving tapinarof were mild-to-moderate in severity and included folliculitis (10.5%) and contact dermatitis (7.9%).33 ECG, vital sign, and laboratory changes were nonsignificant.33
In PSOARING 1 (NCT03956355) the most commonly reported adverse events occurring in the tapinarof group were folliculitis (23.2% vs 1.2%), nasopharyngitis (7.4% vs 5.9%), contact dermatitis (4.4% vs 0.6%), headache (2.9% vs 1.8%), and pruritis (2.4% vs 0%) (tapinarof 1% vs vehicle).36 Similarly, in PSOARING 2 (NCT03983980), folliculitis (17.2% vs 0.6%), nasopharyngitis (4.1% vs 2.9%), contact dermatitis (5.3% vs 0%), headache (3.8% vs 0.6%), and pruritis (2.0% vs 1.2%) (tapinarof vs vehicle) were the most common adverse effects in those receiving tapinarof.36 Tapinarof was also shown to be well tolerated in intertriginous and sensitive areas.36 During the long-term extension phase (PSOARING 3 (NCT04053387)), no new safety signals were observed, with the rate of serious adverse events being 2.49% overall.37 Folliculitis (26.7%) and contact dermatitis (5.5%) were the most common adverse events.37 Long-term treatment with tapinarof did not affect the incidence or severity of folliculitis or contact dermatitis.37 The mild-moderate severity of these events was accompanied by a low discontinuation rate due to folliculitis (1.2%) or contact dermatitis (1.4%).37
Discussion
Tapinarof (GSK2894512, DMVT-505) is a novel, first-in-class, topically administered, small-molecule modulator of AHR which was recently approved by the FDA for the treatment of plaque psoriasis in adults.5,6 For patients with moderate-to-severe plaque psoriasis, the rate of clearance/near clearance (PGA = 0/1) was 35–40% in the phase III trials, PSOARING 1 and PSOARING 2.36 Similar rates of clearance were observed in the long-term extension study, PSOARING 3, with 40.9% of patients achieving disease clearance (PGA = 0) at least once during the trial.37 The durability of response following tapinarof discontinuation at disease clearance was 130.1 days, meaning patients may stop use of tapinarof and experience continued disease clearance for up to 3 months on average after discontinuation.37 Tapinarof’s durability of response is noteworthy when considering topical medications for the treatment of psoriasis given that it may not lose effect despite decreased compliance with drug use over time.39 Tapinarof was also shown to be well tolerated in intertriginous and sensitive skin areas, an important consideration given the limitations of topical corticosteroids in these areas.4,36,37 Improvements in quality-of-life domains were also observed.38 Similar rates of disease improvement to topical corticosteroids were seen in patients receiving treatment with tapinarof 1% cream. Across five clinical trials investigating various topical corticosteroids (triamcinolone, betamethasone dipropionate, betamethasone valerate) for the treatment of mild-to-severe body plaque psoriasis (n = 835), the mean percent improvement in PASI after 8 weeks of treatment ranged from 45 to 60.5%.40 In a phase IIb, double-blind, randomized trial (NCT02564042), the mean percent improvement from baseline PASI was 77.3% after 12 weeks of treatment with tapinarof 1% cream.34 Further, tapinarof cream demonstrated consistent efficacy across different body regions (upper and lower extremities, trunk, head, and neck) and Fitzpatrick skin types.35 Future RCTs may directly compare the efficacy and tolerability of tapinarof versus traditionally prescribed topical agents including topical corticosteroids and vitamin D analogues.
Regarding tapinarof’s mechanism of action, differential activation of AHR has been shown to have pro- or anti-inflammatory response depending on ligand identity, dose, and duration of binding13. AHR deficiency has been shown to exacerbate psoriasiform inflammation, and elevated levels of AHR in the serum of psoriasis patients likely represent dysfunctional AHR signaling.20 Molecular profiling studies demonstrated that AHR activation by tapinarof resulted in strong interactions with Nrf2, resulting in increased barrier gene expression in keratinocytes, an altered immunophenotype with dose-dependent reductions in IL-17A production by CD4+ T-cells, and marked reductions in chemically induced reactive oxygen species.23,25 Tapinarof may also harbor antimicrobial effects towards gram-positive bacteria and fungi, contributing to its mechanism of action within in the skin.26
In phase I trials, tapinarof was categorized as having a very mild cumulative irritation with no evidence of sensitization, photosensitization, or phototoxicity.30 The most commonly observed adverse events associated with tapinarof administration were folliculitis, contact dermatitis, headache, and pruritus. These adverse events infrequently led to drug discontinuation (<1.8% in the phase III trials) and were classified as mild-moderate in severity.36,37 With regard to cases of folliculitis seen with tapinarof administration, associations have been drawn between this and dioxin-induced chloracne, with dioxin being a known ligand for AHR. Bissonnette et al addressed this concern, noting that the downstream effects of AHR, a ligand-dependent transcription factor, following tapinarof binding are distinct versus dioxin compounds.41 It was also noted that the consistent morphology and severity of folliculitis (which was localized to hair follicles) across tapinarof clinical trials were not analogous to dioxin-induced chloracne or hidradenitis suppurativa, which involve sebaceous and apocrine glands, respectively.41
Conclusions
Tapinarof is a topically administered AHR agonist which is an effective treatment option for adults with plaque psoriasis. Patients with moderate-to-severe plaque psoriasis treated with tapinarof demonstrated significant improvements in psoriasis clinical parameters versus placebo, as well as quality-of-life domains. Tapinarof was well tolerated in intertriginous and sensitive skin areas, demonstrated consistent efficacy across body regions and various Fitzpatrick skin types, and had a mean remittive effect lasting more than 3 months. Tapinarof represents an alternative topical treatment for plaque psoriasis versus traditionally used agents like topical corticosteroids and Vitamin D analogues. Future RCTs may directly compare the efficacy and tolerability of tapinarof versus these medications. The most commonly observed adverse effects observed in patients treated with tapinarof were mild-to-moderate folliculitis, contact dermatitis, pruritus, and headache.
Funding
No funding or sponsorship was received for this study or publication of this article.
Disclosure
JQJ is supported in part by research grant funding from the National Psoriasis Foundation. TB is a principal investigator for trials sponsored by AbbVie, Castle, CorEvitas, Dermavant, Galderma, Mindera, and Pfizer. She has received research grant funding from Novartis and Regeneron. She has been an advisor for AbbVie, Arcutis, Boehringer–Ingelheim, Bristol Myers Squibb, Janssen, Leo, Lilly, Novartis, Pfizer, Sun, and UCB. WL has received research grant funding from AbbVie, Amgen, Janssen, Leo, Novartis, Pfizer, Regeneron, and TRex Bio. The authors report no other conflicts of interest in this work.
References
1. Armstrong AW, Mehta MD, Schupp CW, Gondo GC, Bell SJ, Griffiths CEM. Psoriasis prevalence in adults in the United States. JAMA Dermatol. 2021;157(8):940–946. doi:10.1001/jamadermatol.2021.2007
2. Yan D, Blauvelt A, Dey AK, et al. New frontiers in psoriatic disease research, part II: comorbidities and targeted therapies. J Invest Dermatol. 2021;141(10):2328–2337. doi:10.1016/j.jid.2021.02.743
3. Griffiths CEM, Armstrong AW, Gudjonsson JE, Barker JNWN. Psoriasis. Lancet. 2021;397(10281):1301–1315. doi:10.1016/S0140-6736(20)32549-6
4. Lebwohl MG, Tan MH, Meador SL, Singer G. Limited application of fluticasone propionate ointment, 0.005% in patients with psoriasis of the face and intertriginous areas. J Am Acad Dermatol. 2001;44(1):77–82. doi:10.1067/mjd.2001.110046
5. Keam SJ. Tapinarof cream 1%: first approval. Drugs. 2022;82(11):1221–1228. doi:10.1007/s40265-022-01748-6
6. Bissonnette R, Stein Gold L, Rubenstein DS, Tallman AM, Armstrong A. Tapinarof in the treatment of psoriasis: a review of the unique mechanism of action of a novel therapeutic aryl hydrocarbon receptor–modulating agent. J Am Acad Dermatol. 2021;84(4):
7. Stevens EA, Mezrich JD, Bradfield CA. The aryl hydrocarbon receptor: a perspective on potential roles in the immune system. Immunology. 2009;127(3):299–311. doi:10.1111/j.1365-2567.2009.03054.x
8. Fernández-Gallego N, Sánchez-Madrid F, Cibrian D. Role of AHR ligands in skin homeostasis and cutaneous inflammation. Cells. 2021;10(11):3176. doi:10.3390/cells10113176
9. Gutiérrez-Vázquez C, Quintana FJ. Regulation of the immune response by the Aryl hydrocarbon receptor. Immunity. 2018;48:19–33. doi:10.1016/j.immuni.2017.12.012
10. Esser C, Bargen I, Weighardt H, Haarmann-Stemmann T, Krutmann J. Functions of the aryl hydrocarbon receptor in the skin. Semin Immunopathol. 2013;35:677–691. doi:10.1007/s00281-013-0394-4
11. Sutter C, Yin H, Li Y, et al. EGF receptor signaling blocks aryl hydrocarbon receptor-mediated transcription and cell differentiation in human epidermal keratinocytes. Proc Natl Acad Sci USA. 2009;106:4266–4271. doi:10.1073/pnas.0900874106
12. Haarmann-Stemmann T, Esser C, Krutmann J. The janus-faced role of aryl hydrocarbon receptor signaling in the skin: consequences for prevention and treatment of skin disorders. J Invest Dermatol. 2015;135(11):2572–2576. doi:10.1038/jid.2015.285
13. Denison MS, Soshilov AA, He G, DeGroot DE, Zhao B. Exactly the same but different: promiscuity and diversity in the molecular mechanisms of action of the aryl hydrocarbon (dioxin) receptor. Toxicol Sci. 2011;124(1):1–22. doi:10.1093/toxsci/kfr218
14. Napolitano M, Fabbrocini G, Martora F, Picone V, Morelli P, Patruno C. Role of aryl hydrocarbon receptor activation in inflammatory chronic skin diseases. Cells. 2021;10(12):3559. doi:10.3390/cells10123559
15. Furue M, Tsuji G, Mitoma C, et al. Gene regulation of filaggrin and other skin barrier proteins via aryl hydrocarbon receptor. J Dermatol Sci. 2015;80:83–88. doi:10.1016/j.jdermsci.2015.07.011
16. Frauenstein K, Sydlik U, Tigges J, et al. Evidence for a novel anti-apoptotic pathway in human keratinocytes involving the aryl hydrocarbon receptor, E2F1, and checkpoint kinase 1. Cell Death Differ. 2013;20(10):1425–1434. doi:10.1038/cdd.2013.102
17. Murphy KA, Villano CM, Dorn R, White LA. Interaction between the aryl hydrocarbon receptor and retinoic acid pathways increases matrix metalloproteinase-1 expression in keratinocytes. J Biol Chem. 2004;279(24):25284–25293. doi:10.1074/jbc.M402168200
18. Ono Y, Torii K, Fritsche E, et al. Role of the aryl hydrocarbon receptor in tobacco smoke extract-induced matrix metalloproteinase-1 expression. Exp Dermatol. 2013;22(5):349–353. doi:10.1111/exd.12148
19. Pollet M, Shaik S, Mescher M, et al. The AHR represses nucleotide excision repair and apoptosis and contributes to UV-induced skin carcinogenesis. Cell Death Differ. 2018;25:1823–1836. doi:10.1038/s41418-018-0160-1
20. Beranek M, Fiala Z, Kremlacek J, et al. Serum levels of aryl hydrocarbon receptor, cytochromes P450 1A1 and 1B1 in patients with exacerbated psoriasis vulgaris. Folia Biol. 2018;64:97–102.
21. Ehrlich AK, Pennington JM, Bisson WH, Kolluri SK, Kerkvliet NI. TCDD, FICZ, and other high affinity ahr ligands dose-dependently determine the fate of CD4+ T cell differentiation. Toxicol Sci. 2017;161:310–320. doi:10.1093/toxsci/kfx215
22. Ghoreschi K, Balato A, Enerbäck C, Sabat R. Therapeutics targeting the IL-23 and IL-17 pathway in psoriasis. Lancet. 2021;397(10275):754–766. doi:10.1016/S0140-6736(21)00184-7.
23. Di Meglio P, Duarte JH, Ahlfors H, et al. Activation of the aryl hydrocarbon receptor dampens the severity of inflammatory skin conditions. Immunity. 2014;40(6):989–1001. doi:10.1016/j.immuni.2014.04.019
24. van den Bogaard EH, Bergboer JG, Vonk-Bergers M, et al. Coal tar induces AHR-dependent skin barrier repair in atopic dermatitis. J Clin Invest. 2013;123(2):917–927. doi:10.1172/JCI65642
25. Smith SH, Jayawickreme C, Rickard DJ, et al. Tapinarof is a natural AhR agonist that resolves skin inflammation in mice and humans. J Invest Dermatol. 2017;137(10):2110–2119. doi:10.1016/j.jid.2017.05.004
26. Haarmann-Stemmann T, Sutter TR, Krutmann J, Esser C. The mode of action of tapinarof may not only depend on the activation of cutaneous aryl hydrocarbon receptor signaling but also on its antimicrobial activity. J Am Acad Dermatol. 2021;85(1):e33–e34. doi:10.1016/j.jaad.2021.01.103
27. Page MJ, McKenzie JE, Bossuyt PM, et al. The PRISMA 2020 statement: an updated guideline for reporting systematic reviews. BMJ. 2021;372:105906.
28. CASP CHECKLISTS - CASP - Critical Appraisal Skills Programme. Available from: https://casp-uk.net/casp-tools-checklists/.
29. Bissonnette R, Vasist LS, Bullman JN, Collingwood T, Chen G, Maeda-Chubachi T. Systemic pharmacokinetics, safety, and preliminary efficacy of topical AhR agonist tapinarof: results of a Phase 1 study. Clin Pharmacol Drug Dev. 2018;7(5):524–531. doi:10.1002/cpdd.439
30. Jett J, McLaughlin M, Wilson T, et al. Dermal safety of tapinarof cream 1%: results from 4 phase 1 trials. J Drugs Dermatol. 2022;21(10):1084–1090. doi:10.36849/JDD.6627
31. Alex A, Frey S, Angelene H, et al. In situ biodistribution and residency of a topical anti-inflammatory using fluorescence lifetime imaging microscopy. Br J Dermatol. 2018;179(6):1342–1350. doi:10.1111/bjd.16992
32. Jett J, McLaughlin M, Lee M, et al. Maximal use study of tapinarof cream 1% in subjects with extensive plaque psoriasis. SKIN J Cutan Med. 2020;4(6):s74. doi:10.25251/skin.4.supp.74
33. Robbins K, Bissonnette R, Maeda-Chubachi T, et al. Phase 2, randomized dose-finding study of tapinarof (GSK2894512 cream) for the treatment of plaque psoriasis. J Am Acad Dermatol. 2019;80(3):714–721. doi:10.1016/j.jaad.2018.10.037
34. Gold LS, Bhatia N, Tallman AM, Rubenstein D. Secondary efficacy outcomes from a phase 2b, randomized dose-finding study of tapinarof cream for the treatment of plaque Psoriasis. J Psoriasis Psoriatic Arthritis. 2019;4(3):162–163.
35. Lebwohl M, Del Rosso JQ, Hong C-H, Tailman AM, Kircik L. Tapinarof cream for the treatment of plaque psoriasis: efficacy and safety by baseline disease characteristics and skin type in a phase 2b randomized study. SKIN J Cutan Med. 2020;4(5):s30. doi:10.25251/skin.4.supp.30
36. Lebwohl MG, Stein Gold L, Strober B, et al. Phase 3 trials of tapinarof cream for plaque psoriasis. N Engl J Med. 2021;385(24):2219–2229. doi:10.1056/NEJMoa2103629
37. Strober B, Stein Gold L, Bissonnette R, et al. One-year safety and efficacy of tapinarof cream for the treatment of plaque psoriasis: results from the PSOARING 3 trial. J Am Acad Dermatol. 2022;87(4):800–806. doi:10.1016/j.jaad.2022.06.1171
38. Bagel J, Gold LS, Del Rosso J, et al. Tapinarof cream 1% once daily for the treatment of plaque psoriasis: patient-reported outcomes from the PSOARING 3 trial. J Am Acad Dermatol. 2023;89(23):936–944.
39. Devaux S, Castela A, Archier E, et al. Adherence to topical treatment in psoriasis: a systematic literature review. J Eur Acad Dermatol Venereol. 2012;26:
40. Castela E, Archier E, Devaux S, et al. Topical corticosteroids in plaque psoriasis: a systematic review of efficacy and treatment modalities. J Eur Acad Dermatol Venereol. 2012;26(Suppl 3):36–46. doi:10.1111/j.1468-3083.2012.04522.x
41. Bissonnette R, Gold LS, Rubenstein DS, Tallman AM, Armstrong AW. Tapinarof-associated folliculitis is generally mild, self-limiting, and rarely interferes with therapy. J Am Acad Dermatol. 2021;85(1):e39–e40. doi:10.1016/j.jaad.2021.03.006
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.