")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Mapping Current Organizational Structure and Improvement Points of Breast Cancer Multidisciplinary Team Meetings – An Interview Study
Authors Kočo L , Siebers CCN, Schlooz M, Meeuwis C, Oldenburg HSA, Prokop M, Mann RM
Received 6 July 2022
Accepted for publication 16 September 2022
Published 21 October 2022 Volume 2022:15 Pages 2421—2430
DOI https://doi.org/10.2147/JMDH.S380293
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Lejla Kočo,1 Carmen CN Siebers,1 Margrethe Schlooz,2 Carla Meeuwis,3 Hester SA Oldenburg,4 Mathias Prokop,1 Ritse M Mann1,5
1Department of Imaging, Radboud University Medical Center, Nijmegen, the Netherlands; 2Department of Surgery, Radboud University Medical Center, Nijmegen, the Netherlands; 3Department of Radiology, Rijnstate Hospital, Arnhem, the Netherlands; 4Department of Surgery, The Netherlands Cancer Institute, Amsterdam, the Netherlands; 5Department of Radiology, The Netherlands Cancer Institute, Amsterdam, the Netherlands
Correspondence: Lejla Kočo, Department of Imaging, Radboud University Medical Center, Nijmegen, the Netherlands, Tel +31 24 361 87 66, Email [email protected]
Purpose: The aim of the study was to map current organization, and document potential improvement points of breast cancer multidisciplinary team meetings (MDTMs), in order to support the optimization of the present breast cancer MDTM organization.
Methods: From January 2019 to February 2021, 24 core team members of the breast cancer multidisciplinary team (MDT) in three hospitals were interviewed. Semi-structured interviews were performed based on an interview guide. All interviews were recorded and transcribed verbatim. Deductive coding was performed on the transcripts by two independent researchers. The codes were organized in categories and themes.
Results: In total 24 healthcare professionals; surgeons, medical oncologists, radiotherapists, pathologists, radiologists, and specialized nurses, from three different hospitals were interviewed. According to the participants, improving efficiency before and during MDTMs is possible by ensuring proper preparation of attendees, implementing more structure during discussions, improving access to and availability of patient data and optimizing general meeting discipline.
Conclusion: Preparation, structure, data availability and meeting discipline were highlighted as essential factors for efficient breast cancer MDTM improvement. These topics seem to be applicable to other types of oncology MDTMs as well. Improving MDTM efficiency on the long term ensures high-quality discussions for all breast cancer patients.
Keywords: breast cancer MDTMs, breast cancer care efficiency, optimizing breast cancer care, MDTM evaluation, qualitative research
Simple Summary
Breast cancer multidisciplinary team meetings (MDTMs) are considered an essential part of the treatment pathway, despite being considered time-consuming and expensive. Future increasing breast cancer incidence could potentially disrupt current organizational structure and performance of breast cancer MDTMs, highlighting the importance of well-organized cancer MDTMs. The aim of this study was to identify potential improvement points to support the optimization of the current breast cancer MDTM organization by performing interviews. Participants stated that efficiency could be improved by ensuring proper preparation of attendees, structured discussions, improved availability of information and optimizing general meeting discipline. The identified topics also seem to be applicable to other types of oncology.
Introduction
Breast cancer is a highly complex disease. Many different types of breast cancer all require their own combined modality treatment. This makes breast cancer multidisciplinary team meetings (MDTMs) an essential part of the treatment pathway. MDTMs are performed to ensure proper evidence-based management of cancer patients.1 During MDTMs clinicians from different disciplines involved in the treatment of breast cancer get together to review patient cases, determine diagnosis and recommend management plans.2 In addition, important functions of MDTMs in (breast) cancer care include communication between disciplines and educational purposes.3
The combination of high disease complexity and high patient load implies that hospitals require efficient and well-organized breast cancer MDTMs. Albeit the performance of MDTMs is recommended in (inter)national guidelines, each hospital is free to organize cancer MDTMs independently, resulting in differences in MDTM organization tailored to the local situation.4–6 Despite their value in patient care and education, MDTMs are considered time consuming and expensive, since preparation time and attendance are required from all involved specialists. This highlights the importance of well-organized cancer MDTMs.1,7
Breast cancer incidence has been increasing continuously over the past decades.8 This increase can potentially disrupt the current structure and organization of breast cancer MDTMs. In order to sustain breast cancer MDTMs, the current situation needs to be mapped and potential improvements should be determined.
The aim of this qualitative interview study is to obtain a broad overview of the current organization of breast cancer MDTMs, to understand this from a specialist point of view and to identify potential points of improvement.
Methods
Design
In this study, a qualitative study design with semi-structured interviews was used. Participants of this study consisted of breast cancer specialists who are actively involved in the breast cancer MDTMs of their hospital. This approach offers an effective way of determining the views and opinions of experienced medical specialists regarding breast cancer MDTMs. Performing semi-structured interviews provides the possibility to explore relevant topics in a flexible manner, and in more detail when necessary.
Participants
For the semi-structured interviews specific participants were selected. In order to have a suitable and diverse group of participants, it was decided to approach breast cancer specialists who are actively participating as attendees in breast cancer MDTMS in their hospital. The core-team members of breast cancer MDTMs consist of ie, surgeons, oncologists, radiologists, radiation oncologists, pathologists and nurse specialists. To ensure a representative range of hospitals providing breast cancer care services, specialists from a regional hospital, an academic hospital and a specialized cancer institute were approached.
Each interview lasted between 25 and 45 min. The interviews were carried out by a researcher trained in performing qualitative methods (LK) either face-to-face, video call or by phone call. Face-to-face interviews were performed at the office or meeting room on location for the participant and recorded on an audio-recorder telephone app. Remote interviews via video call (skype) or by phone call were recorded on an audio-recorder computer app. All participants were informed about the audio recording in the interview invitation and verbally consented to audio recording prior to the start of the interview.
Interview Guide
As part of the methodology of semi-structured interviews,9 an interview guide was developed to structure the interviews while still allowing the possibility to further explore the participants’ thoughts and opinions (Supplementary A). The specific topics of conversation were determined according to the aim of this study and the research question. We paid specific attention to interview participants about factors of MDTMs that can potentially be improved according to breast cancer specialists. The following topics were incorporated: current MDTM organization and specialists’ role in the MDTM; specialists’ MDTM preparation routine; the current MDTM process, time management, success factors and points of improvement. All interviews were conducted with the same interview guide.
Data Analysis
To analyze the collected data, the audio-recordings of each interview were transcribed verbatim and anonymously by the researcher who also conducted the interviews (LK). In order to avoid researcher bias and ensure accurate analysis, a standardized approach for interview analysis, the Framework Method, was used.10 Two independent researchers (LK & CS) developed a codebook as an analytical framework, after which all transcripts were analyzed and coded. Prior to the coding process, researchers agreed that disagreements would be resolved through discussion, although this did not prove to be necessary. The obtained data was then charted into the framework matrix by summarizing the data from each transcript per category, and finally visualized in the form of graphs. The programs “Express Scribe” and “Atlas.ti” were used respectively for transcription of the audio-recordings and the analysis of the transcripts.
Results
Participant Overview
Table 1 provides an overview of the specialists who participated in this qualitative study. Of the 24 breast cancer specialists, nineteen were female (79%) and five were male (21%). Breast cancer specialists were approached in a general hospital (6 specialists), an academic hospital (9 specialists) and a cancer institute (9 specialists). All participants, who were also core team members, attended the breast cancer MDTMs at their hospital at least weekly.
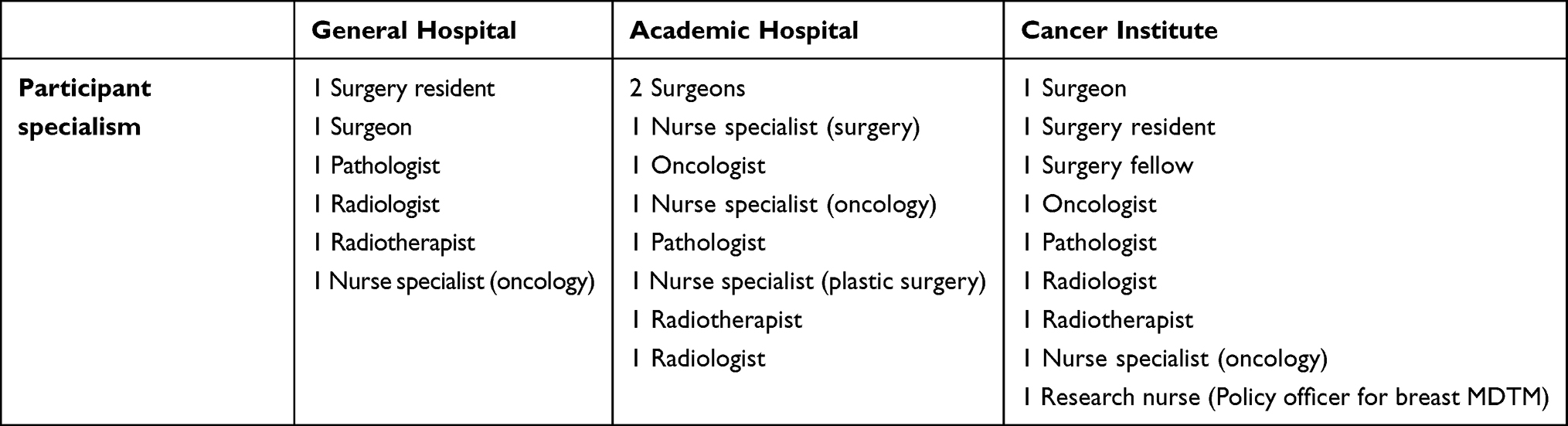 |
Table 1 An Overview of All Study Participant per Hospital. The Specialty of Nurse Specialists is Depicted Between Brackets |
Current Organization of Breast Cancer MDTMs
All patients with a malignant breast cancer diagnosis are pre-registered for the breast cancer MDTM. During the MDTMs a core team is present consisting of at least a surgeon, oncologist, radiologist, pathologist, radiotherapist and nurse specialist, all specialized in breast cancer. Other disciplines involved in breast cancer treatment, such as plastic surgeons or medical geneticists, attend on a regular basis as well. Each MDTM always has a designated chairperson and note-taker. Registration for MDTM discussion can be done by any of the treating physicians and can occur on multiple points during the care pathway. MDTM discussion topics consist of diagnosis and initial treatment plan, post-operative results, systemic therapy response evaluation, metastasis or recurrence, or any other question a treating physician might have about a case.
The three included hospitals used different organizational structures for the breast cancer MDTMs (Table 2). MDTMs are held either once or multiple times per week. In case MDTMs are organized multiple times per week, the different MDTMs are designated for specific patient subgroups. For time management purposes, some MDTMs have a limited number of patients that can be registered for discussion.
 |
Table 2 Overview of MDTM Organizational Structure per Included Hospital |
In general, participants agreed on the goal of breast cancer MDTMs despite differences between the organizational structure. According to half of the participants (n=11), the main purpose of breast cancer MDTMs is to review patient cases, determine diagnosis and propose management plans tailored to each patient. Another goal was to give specialists the opportunity to ask questions, have discussions and obtain new insights in a multidisciplinary setting (n=6). Furthermore, educational purpose and facilitation of referrals to other departments were mentioned (n=2).
Everyone [MDTM attendees] has a different point of view. Sometimes somebody will ask a clarifying question. There should be time for this [during the MDTM]. This is just the sort of thing that will benefit the patient in the end. – Radiologist
The Importance of MDTM Preparation
Preparation of the MDTM was considered an essential determining factor for efficient MDTM workflow. Differences between participants were identified in preparation time (Figure 1A: Duration of preparation) and extent of preparation (Figure 1B: Preparation methods). Participants indicated that their preparation time depends on personal preference, time availability and their role during the MDTM. Overall, estimated average preparation time varied between 15 minutes to up to 4 hours per MDTM for most participants (n=16), while others either did not need to prepare or used their outpatient clinic preparation (n=6). About preparation in general the following statements were made (Figure 1C: Preparation remarks). Some participants thought that all attendees of the MDTM should be familiar with all the cases on the list, despite their role (n=10). Also, it was stated that unpreparedness of attendees can lead to longer discussions (n=5). For most MDTMs one attendee (usually a specialist or resident) is responsible for preparing a case summary and presenting each patient case registered on the list during the MDTM. Usually, these summaries are not available to other attendees prior to the MDTM but are very time consuming to make for the presenting specialist or resident (n=5).
Because of the number of patients on the list, we need to go through that list very efficiently. Good preparation really helps to achieve that. – Surgeon
 |
Figure 1 Summary of participant comments regarding the preparation of breast cancer MDTMs. (A) Duration of preparation: estimated average time spent preparing the MDTM per participant. (B) Preparation methods: the method of preparation used per participant. (C) Preparation remarks: comments regarding the preparation of colleagues. (D) Benefits of preparation: factors related to preparation that were considered beneficial for MDTMs. |
Multiple benefits of preparation were identified (Figure 1D: Benefits of preparation). The preparation process serves as a learning opportunity for specialists in training (n=2) and provides a data completeness check prior to the MDTM (n=2). Furthermore, proper preparation prevents having to look up information during the discussion since this is considered as a delaying factor for discussion (n=7).
Attending the MDTMs well prepared is an essential determinant for an efficient workflow (n=10) and was therefore also most often mentioned as an improvement point (n=9) as summarized in Table 3.
 |
Table 3 List of Points of Improvement for Breast Cancer MDTMs as Stated by the Participants |
Facilitators and Barriers of Time Management During the MDTM
Proper time management is necessary to ensure efficient MDTM workflow. Participants identified several factors that either had positive or negative effects on time management during MDTMs and subsequently provided potential improvement points. These factors can be divided in the following three topics: (case presentation) structure, data availability and meeting discipline (Figure 2).
 |
Figure 2 Summary of participant comments regarding the facilitators and barriers of time management during breast cancer MDTMs. (A) Structure: facilitators and barriers concerning the structure of breast cancer MDTMs. (B) Availability of information: facilitators and barriers concerning patient information. (C) Meeting discipline: facilitators and barriers concerning the way MDTMs are moderated. |
Actions to ensure structured discussions were mentioned most often to support time management (Figure 2A: Structure). Concise case presentations (n=12), especially when done by treating physicians (n=4), are the most efficient way to discuss cases. Sharing irrelevant information during these case presentations is not desirable, since it may result in longer discussions and can take away focus from the relevant question (n=7). For this reason, participants noted that having a clearly formulated question or reason for discussion is essential (n=8). Furthermore, structured discussions are also easier to follow for the notetaker (n=2) and having a maximum number of cases on the list ensures sufficient time per case discussion (n=3). Thus, working towards a more structured patient registration form which can also be used during case discussions, including a clear question for the MDT, was mentioned as a potential improvement point (n=6).
The challenge is to not present irrelevant information. Some information is important, during the consultation for example, but not necessarily to answer the question during the MDTM. – Nurse specialist (oncology)
Secondly, accessibility and availability of patient information were mentioned as a determining factor for efficiency during MDTMs (Figure 2B: Availability of information). Complete case information for each discussion is ideal (n=10), and missing data should be announced at the start of the meeting (n=2). Facilitation of easier access to patient information is important (n=2). Also having a patient summary available to all attendees would be useful according to some participants (n=4). Depending on the question or reason for discussion, the patient can either be postponed or discussed despite the lacking information. However, repeatedly discussing patients with incomplete information was considered inefficient (n=10). Participants also mentioned long loading times of imaging as a barrier to time management, disturbing an efficient workflow (n=3). Thus, availability of patient information, both prior to and during the MDTM, and its accessibility should be improved.
To have a patient summary available would be very useful [during the MDTM]. Discussions can be so fast, that it helps to quickly see the most important patient information. – Radiotherapist
The final topic influencing time management during MDTMs mentioned by participants was general meeting discipline (Figure 2C: Meeting discipline). Participants provided examples such as having a strict chairperson to lead a structured discussion (n=7), avoiding informal talk unrelated to the discussion topic (n=4), ensuring high focus and motivation (n=3) and arriving on time (n=2). The following improvements of aspects of general meeting discipline were strictly to-The-point discussions (n=5), a well-trained chairperson (n=4) and optimal focus and motivation of all attendees (n=3).
Sometimes people repeat themselves, the discussion keeps on going and no decision is made. Especially with more complicated cases. – Radiologist
All points of improvement per category as mentioned above are summarized in Table 3.
Discussion
Summary of Evidence
The value and importance of multidisciplinary teams (MDTs), after being implemented for years in cancer care, is irrefutable. Organizations such as the European Society of Breast Cancer Specialists (EUSOMA) and the European Partnership for Action Against Cancer (EPAAC) published statements with guidelines for MDT care and appeals for further MDT implementation and improvement.11–13
This study provides a synopsis of the current organization of breast cancer MDTMs and factors considered important for their efficient organization according to its key members in different hospitals. It also provides insight in the points that could potentially be improved to optimize its efficiency and value in the Netherlands. Within the current guidelines for the organization of breast cancer MDTMs, there is room for different organizational structures according to the hospitals’ needs. The results of this study also highlight the importance of certain factors such as appropriate preparation by all attendees and well-structured discussions for optimal functioning of the MDTMs. Since hospitals organize their breast cancer care independently, differences in MDTM organization are bound to occur.4 However, despite these differences in organizational structure, similar points for potential improvement of breast cancer MDTMs were suggested by all interviewed breast cancer MDT members.
Goal of MDTMs and Current Organization
In this study, participants were interviewed about improvements to the current format of breast cancer MDTMs, while changes to the goal and actual organization of breast cancer MDTMs were not included topics. According to the national Dutch guidelines on MDTMs, all patients with a malignancy should be discussed.4 However in the literature, one of the suggestions for changes in the MDTM organization was to streamline patients, which was defined as “discussing the cancer cases that do not follow well-established clinical pathways while discussing other cases more briefly or not at all”.14,15 However, objections to this approach were based on inequality of treatment and worries for quality and safety of care.14 Furthermore, reducing the number of discussed cases was not correlated to higher quality discussions according to a study by Lamb et al, hence leaving out patients that do conform to standardized pathways may not be the optimal solution for optimizing MDT logistics.16
MDTM Preparation
Having a team of well-prepared attendees was considered one of the most important determinators and improvement points for an efficient MDTM. Since proper preparation is time-consuming, full agendas or a limited role during the MDTM were reasons for attendees to minimize their preparation. Not only is this the case for breast cancer specialists, but it has also been shown for MDTMs of other cancer types.14–18 For example, improving preparation of cases seems to have a positive effect on quality of discussions and the decision-making process.16 Specialists attending MDTMs should thus have time available in their schedule outside of the MDTM, specifically dedicated to preparation. Specialists from certain disciplines do not need to prepare all cases on the MDTM list, since not all questions on the list directly require their expertise. Therefore, the amount of time allocated to preparation should match the role of the attendee during the MDTM since the amount of needed preparation can vary.15,19
Structure and Meeting Discipline
Both during preparation and during the MDTM itself, the need for more structure was expressed in order to prepare and discuss cases more efficiently. Participants suggested a clearly formulated question for each case and standardized registration forms that could be used for preparation and case presentations. Studies suggested using checklists to enhance the structure of discussions20,21 and well-structured MDTMs have been shown to support efficiency and positive outcomes.17,22 Meeting discipline was also considered to be a facilitator of efficient MDTMs and identified as an improvement point. Studies have shown that effective chairing and leadership supports interactions and communication between attendees.20,23
Availability of Patient Information
Another point of concern was the availability and completeness of patient information during MDTMs. Currently, incompleteness of case files may only become evident at the time of discussion or may be flagged at the start of the MDTMs. However, time could be saved if these cases could be identified earlier so the cases that remain undiscussed will not require preparation by the participants. Indeed, multiple studies identified incomplete information to be a barrier of MDTM progress for several different cancer types.17,19,21
Applicability of Results to Other Types of Oncology MDTMs
Responses from MDT members to optimize breast cancer MDTMs appear to be applicable to all settings. Our results are also in line with previous studies that analyzed MDTMs for other types of cancer. A national survey study from the UK showed high consensus of determinants for effective MDTM working for different cancer types of which the importance of preparation, education, availability of data and leadership were mentioned among others.24 Furthermore, multiple studies investigating the improvement of oncology MDTMs identified similar points of improvement, eg to improve preparation, structured discussions, using forms or checklists, improving meeting discipline and having a good chairperson to lead the discussions.18,25 It may thus be possible to use standardized improvement strategies for different types of oncology MDTMs. However, depending on factors, such as treatment complexity and prognosis of different cancer types, preparation times and the requirements for data completeness may vary.24
Strengths and Limitations
There are some limitations to this study. First, due to the perspective-based nature of qualitative research and the small sample size, statistical analysis was not possible to perform. For some disciplines, only one specialist per hospital was interviewed. Furthermore, not all respondents were asked the same exact questions. Therefore, classification of the importance of improvement points (as shown in the figures) was obtained from a partial study population and can only be inferred from the frequency with which they were mentioned by the interviewed MDT members.
Our study also has several strengths. Qualitative research methods like semi-structured interviews are an excellent method to examine the existing issues in depth and detail. Since the method is adaptable, we were able to gradually obtain more insight in the topic, generating new information from each interview until data saturation. Secondly, by including core members of the breast cancer MDTMs according to the Dutch and European guidelines,4,6 we avoided selection bias of participants as much as possible. Furthermore, we have tried to include potential differences in point of views by interviewing participants with different specialties, and from hospitals with different MDTM organization and patient populations. Finally, using a semi-structured interview style facilitated more room for variation and resulted in the possibility to discuss several different perspectives with participants.
Further work is required in order to understand which issues are universal for MDTMs of all cancer types, and what aspects of the MDTM require a more tailored disease-specific approach. Additionally, MDTMs may need to be adapted to facilitate the increasing number of patients and information availability within electronic medical records, while trying not to increase the workload for healthcare specialists. Finally, obtaining more knowledge from an organizational and financial point of view would also aid in estimating the feasibility of further improvement of MDTMs.
Conclusion
In conclusion, breast cancer MDTMs are in general well-organized and executed, while there is still room for improvement according to key members of breast cancer MDTMs. Preparation, structure, data availability and meeting discipline were highlighted as essential factors for efficient breast cancer MDMTs that could be improved. Based on the literature, these topics are not only relevant to breast cancer MDTMs but also to other types of oncology MDTMs. To guarantee high-quality healthcare on the long term it is essential to continue improving the current way of working during MDTMs, increasing the quality of MDTMs and anticipating on expected future changes in the medical field and patient populations.
Data Sharing Statement
Data sharing not applicable to this article as no datasets were generated or analyzed during the current study.
Ethics Approval
Ethical approval was not required for this research, since it is not subject to the Dutch law of Medical Research Involving Human Subjects (WMO).
Acknowledgments
This paper and research behind it would not have been possible without the participation of all breast cancer specialists, residents and nurses from the three included hospitals. We greatly appreciate their opinions and participation in this study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The authors declare that no funds, grants, or other support were received during the preparation of this manuscript.
Disclosure
Prof. Dr Mathias Prokop reports grants, personal fees from Siemens Healthineers, during the conduct of the study; grants, personal fees from Canon Medical Systems, personal fees from Bracco, outside the submitted work.
Dr Ritse M Mann reports grants, personal fees, non-financial support from Siemens, grants, personal fees from Bayer, grants, non-financial support from Screenpoint, grants, personal fees, non-financial support from BD, grants, non-financial support from Koning, grants, non-financial support from PA-Imaging, outside the submitted work. The authors declare that they have no known competing financial interests or personal relationships that could have appeared to influence the work reported in this paper.
References
1. El Saghir NS, Charara RN, Kreidieh FY, et al. Global practice and efficiency of multidisciplinary tumor boards: results of an American Society of Clinical Oncology International Survey. J Glob Oncol. 2015;1(2):57–64. doi:10.1200/jgo.2015.000158
2. Li J, Robertson T, Hansen S, Mansfield T, Kjeldskov J. Multidisciplinary medical team meetings: a field study of collaboration in health care; 2008: 73–80.
3. Harrison JD, Choy ET, Spillane A, Butow P, Young JM, Evans A. Australian breast cancer specialists’ involvement in multidisciplinary treatment planning meetings. Breast. 2008;17(4):335–340. doi:10.1016/j.breast.2008.03.001
4. Westerhuis W. Kwaliteitscriteria multidisciplinair overleg (EN: Quality criteria for multidisciplinary team meetings). Integraal Kanker Centrum Nederland (National Comprehensive Cancer Organization). https://iknl.nl/nkr/evaluatie-met-nkr-data/multidisciplinair-overleg#:~:text=Kwaliteitsnormen%20mdo,alle%20pati%C3%ABnten%20daar%20besproken%20wordt.
5. Parker S. Clinical guidelines for the management of breast cancer. England: NHS; 2019.
6. Biganzoli L, Cardoso F, Beishon M, et al. The requirements of a specialist breast centre. Breast. 2020;51:65–84. doi:10.1016/j.breast.2020.02.003
7. Lamb BW, Green JS, Benn J, Brown KF, Vincent CA, Sevdalis N. Improving decision making in multidisciplinary tumor boards: prospective longitudinal evaluation of a multicomponent intervention for 1421 patients. J Am Coll Surg. 2013;217(3):412–420. doi:10.1016/j.jamcollsurg.2013.04.035
8. Vondeling GT, Menezes GL, Dvortsin EP, et al. Burden of early, advanced and metastatic breast cancer in The Netherlands. BMC Cancer. 2018;18(1):262. doi:10.1186/s12885-018-4158-3
9. Kallio H, Pietilä A-M, Johnson M, Kangasniemi M. Systematic methodological review: developing a framework for a qualitative semi-structured interview guide. J Adv Nurs. 2016;72(12):2954–2965. doi:10.1111/jan.13031
10. Gale NK, Heath G, Cameron E, Rashid S, Redwood S. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol. 2013;13(1):1–8. doi:10.1186/1471-2288-13-117
11. Borras JM, Albreht T, Audisio R, et al. Policy statement on multidisciplinary cancer care. Eur J Cancer. 2014;50(3):475–480. doi:10.1016/j.ejca.2013.11.012
12. Cardoso F, Cataliotti L, Costa A, et al. European Breast Cancer Conference manifesto on breast centres/units. Eur J Cancer. 2017;72:244–250. doi:10.1016/j.ejca.2016.10.023
13. Eusoma. The requirements of a specialist breast unit. Eur J Cancer. 2000;36(18):2288–2293. doi:10.1016/S0959-8049(00)00180-5.
14. Hoinville L, Taylor C, Zasada M, Warner R, Pottle E, Green J. Improving the effectiveness of cancer multidisciplinary team meetings: analysis of a national survey of MDT members’ opinions about streamlining patient discussions. BMJ Open Qual. 2019;8(2):e000631. doi:10.1136/bmjoq-2019-000631
15. Warner R, Hoinville L, Pottle E, Taylor C, Green J. Refocusing cancer multidisciplinary team meetings in the United Kingdom: comparing urology with other specialties. Ann R Coll Surg Engl. 2021;103(1):10–17. doi:10.1308/rcsann.2020.0212
16. Lamb B, Sevdalis N, Benn J, Vincent C, Green J. Multidisciplinary cancer team meeting structure and treatment decisions: a prospective correlational study. Ann Surg Oncol. 2013;20(3):715–722. doi:10.1245/s10434-012-2691-x
17. Rosell L, Alexandersson N, Hagberg O, Nilbert M. Benefits, barriers and opinions on multidisciplinary team meetings: a survey in Swedish cancer care. BMC Health Serv Res. 2018;18(1):1–10. doi:10.1186/s12913-018-2990-4
18. Lamb B, Taylor C, Lamb J, et al. Facilitators and barriers to teamworking and patient centeredness in multidisciplinary cancer teams: findings of a national study. Ann Surg Oncol. 2013;20(5):1408–1416. doi:10.1245/s10434-012-2676-9
19. Gandamihardja TA, Soukup T, McInerney S, Green J, Sevdalis N. Analysing breast cancer multidisciplinary patient management: a prospective observational evaluation of team clinical decision-making. World J Surg. 2019;43(2):559–566. doi:10.1007/s00268-018-4815-3
20. Oeppen RS, Davidson M, Scrimgeour DS, Rahimi S, Brennan PA. Human factors awareness and recognition during multidisciplinary team meetings. J Oral Pathol Med. 2019;48(8):656–661. doi:10.1111/jop.12853
21. Jalil R, Ahmed M, Green JS, Sevdalis N. Factors that can make an impact on decision-making and decision implementation in cancer multidisciplinary teams: an interview study of the provider perspective. Int J Surg. 2013;11(5):389–394. doi:10.1016/j.ijsu.2013.02.026
22. El Saghir NS, Keating NL, Carlson RW, Khoury KE, Fallowfield L. Tumor boards: optimizing the structure and improving efficiency of multidisciplinary management of patients with cancer worldwide. Am Soc Clin Oncol Educ Book. 2014;34(1):e461–e466. doi:10.14694/EdBook_AM.2014.34.e461
23. Wihl J, Rosell L, Bendahl P-O, et al. Leadership perspectives in multidisciplinary team meetings; observational assessment based on the ATLAS instrument in cancer care. Cancer Treat Res Commun. 2020;25:100231. doi:10.1016/j.ctarc.2020.100231
24. Lamb B, Sevdalis N, Taylor C, Vincent C, Green J. Multidisciplinary team working across different tumour types: analysis of a national survey. Ann Oncol. 2012;23(5):1293–1300. doi:10.1093/annonc/mdr453
25. Sarkar S, Arora S, Lamb BW, Green JS, Sevdalis N, Darzi A. Case review in urology multidisciplinary team meetings: what members think of its functioning. J Clin Surg. 2014;7(6):394–402. doi:10.1177/2051415814532459
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.