")
Back to Journals » Clinical Epidemiology » Volume 15
Maternal Multiple Sclerosis and Health Outcomes Among the Children: A Systematic Review
Authors Andersen ML , Jølving LR , Stenager E , Knudsen T , Nørgård BM
Received 11 October 2022
Accepted for publication 20 February 2023
Published 19 March 2023 Volume 2023:15 Pages 375—389
DOI https://doi.org/10.2147/CLEP.S392273
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Eyal Cohen
Mette Louise Andersen,1– 3 Line Riis Jølving,1,2 Egon Stenager,4,5 Torben Knudsen,4,6 Bente Mertz Nørgård1,2
1Center for Clinical Epidemiology, Odense University Hospital, Odense, Denmark; 2Research Unit of Clinical Epidemiology, Department of Clinical Research, University of Southern Denmark, Odense, Denmark; 3Department of Gynecology and Obstetrics, University Hospital of Southern Jutland, Esbjerg, Denmark; 4Department of Regional Research, University of Southern Denmark, Odense, Denmark; 5Multiple Sclerosis Clinic Hospital of Southern Jutland, Aabenraa, University of Southern Denmark, Odense, Denmark; 6Department of Gastroenterology, University Hospital of Southern Jutland, Esbjerg, Denmark
Correspondence: Mette Louise Andersen, Center for Clinical Epidemiology, Odense University Hospital, Kloevervaenget 30, Entrance 216, Odense, DK- 5000, Denmark, Email [email protected]
Objective: To summarize the available literature and provide an overview of in utero exposure to maternal multiple sclerosis (MS) and the influence on offspring health outcomes.
Methods: We conducted a systematic review by searching Embase, Medline and PubMed.gov databases, and we used covidence.org to conduct a thorough sorting of the articles into three groups; 1) women with MS and the influence on birth outcomes; 2) women with MS treated with disease-modifying therapy (DMT) during pregnancy and the influence on birth outcomes; and 3) women with MS and the influence on long-term health outcomes in the children.
Results: In total, 22 cohort studies were identified. Ten studies reported on MS without DMT and compared with a control group without MS, and nine studies on women with MS and DMT prior to or during pregnancy met the criteria. We found only four studies reporting on long-term child health outcomes. One study had results belonging to more than one group.
Conclusion: The studies pointed towards an increased risk of preterm birth and small for gestational age among women with MS. In terms of women with MS treated with DMT prior to or during pregnancy, no clear conclusions could be reached. The few studies on long-term child outcomes all had different outcomes within the areas of neurodevelopment and psychiatric impairment. In this systematic review, we have highlighted the research gaps on the impact of maternal MS on offspring health.
Keywords: multiple sclerosis, pregnancy, neonatal outcomes, long-term health outcomes, reproduction
Introduction
Multiple sclerosis (MS) is one of several chronic immune diseases with an increasing incidence,1 and the majority of patients are women diagnosed between the ages of 20 and 40 years. During the past 25 years, the treatment options have improved, and with the introduction of disease-modifying therapy (DMT), people living with MS are now encouraged to pursue the life they want to live. With many females being diagnosed at childbearing age, this may include starting a family.2 Questions related to reproduction are naturally of great concern in the expanding population of young women with MS and it has become an important area of clinical care and research. Women with MS historically have fewer children than the general population,3 and this may be because of periods of active disease and treatments. Whether fertility is impaired is still debated,3,4 but it is certain that some patients with a chronic disease make an active choice not to have children.5 It has gradually become more routine for neurologists to discuss pregnancy when planning medical treatment in young women. Patients were previously concerned about the heritability of MS, but neuroepidemiological studies in this area have produced reassuring results. Previous studies have suggested that susceptibility to MS is a complex interplay of heritability and environment, and the question about heritability is an ongoing research topic.6–9 A meta-analysis from 2012 found the age-adjusted risk of recurrence among offspring with a parent with MS to be 1.45% (95% CI 1.23–1.67).10
In addition, patients are naturally worried about the impact of MS as a disease and its corresponding medications on the health of their offspring, which has led to increasing demands for conception counseling. The association between in utero exposure to maternal MS, with its accompanying medical treatments, and adverse short- and long-term offspring outcomes has been studied to a limited extent among researchers in neurology and obstetrics over the past two decades.11–14
The authors are aware of two reviews,15,16 which, from a neurological angle, summarize evidence on MS and short-term adverse birth outcomes. Another review examined the developmental trajectories of offspring and requested further studies on long-term outcomes in offspring.17 We performed this review because there have been no other reviews with a focus on long-term somatic health outcomes in the offspring of women with MS.
Material and Methods
Protocol and Registration
The review protocol was registered at the International Prospective Register of Systematic Reviews (PROSPERO.org) with ID number CRD42022338414, prior to initiation of the review process.
Search Strategy and Eligibility Criteria
A comprehensive literature search was undertaken in Embase and Medline in combination with a reference screening of the included studies conducted in PubMed, to pursue a complete coverage of the topic. The search running dates were 05.02.2022–06.15.2022 and all searches were repeated on 08.23.2022, which did not contribute any new publications meeting the inclusion and exclusion criteria. The last up-to-date search, conducted on 02.06.2023, added one new study.18 The search strategy was developed by MLA together with a trained librarian at the University of Southern Denmark, applying the PICOS format (population, intervention, comparison and outcomes of interest) and organized in search blocks. For the search string, see the Supportive File. For the connections between search blocks, the Boolean operators AND and OR were used.
The search results are presented in Figure 1. Both primary data collection and studies including secondary sources of data (eg claims databases, interviews with mothers) were considered. Duplicates were removed in Endnote. Abstracts, reviews, case reports, case series and spontaneous reports were excluded, as were other types of studies with no reference group. Offspring birth, neonatal, childhood and adolescence somatic and mental health outcomes were of interest. We included only studies reporting on child outcomes with a risk estimate (absolute or relative risk estimates [hazard ratio (HR), odds ratio (OR), relative risk (RR)]). After reviewing the search results, abstracts were screened and full-text articles read. Finally, appropriate studies were included based on the exclusion and inclusion criteria. Reasons for exclusion of papers were recorded in a table. The studies were sorted into three groups: 1) maternal MS and short-term outcomes in the offspring (birth and neonatal), 2) in utero exposure to medications used to treat maternal MS and short-term outcomes in the offspring (birth and neonatal), and 3) maternal MS and long-term health outcomes in the offspring (from 1 month to adulthood).
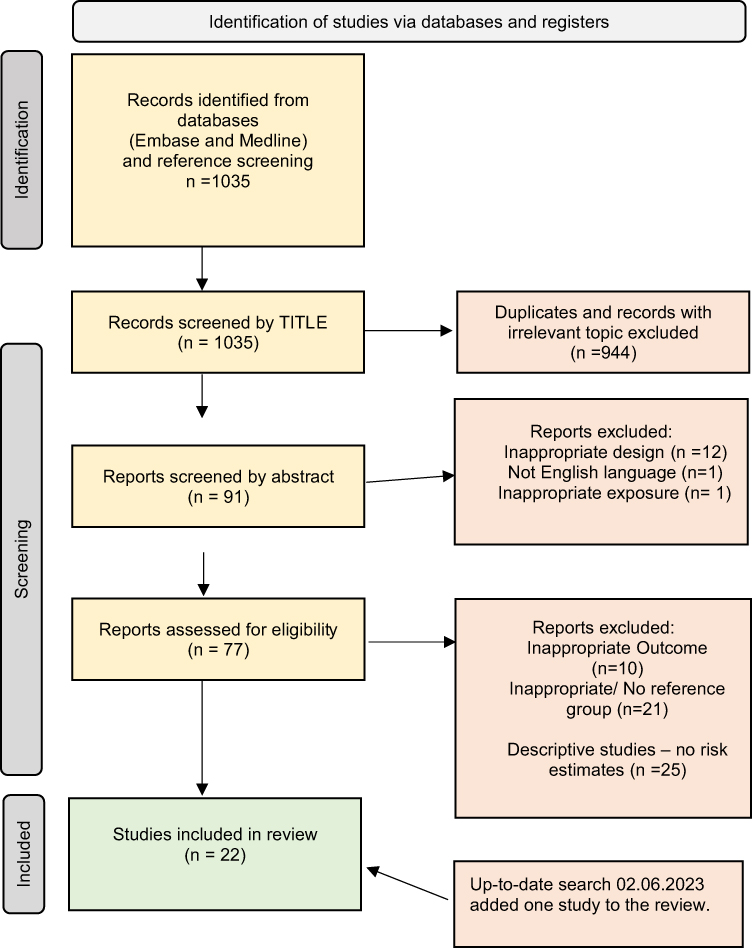 |
Figure 1 Search strategy and flowchart of exclusion and inclusion of studies. |
The eligibility criteria for this review were as follows.
- Exposure: Maternal MS diagnosis verified with the McDonald criteria or by International Classification of Diseases (ICD) diagnosis codes.19 Comparison with healthy controls was preferred. In studies with DMT exposure, stratification on each type of medication was mandatory, and comparison with women with MS but without DMT treatment was preferred.
- Studies with data from pharmacovigilance databases managed by pharmaceutical manufacturers were excluded, together with studies where the contributing authors were permanently employed by the industry.
- Outcomes: In all studies with the outcome of preterm birth, this was defined as birth before gestational age 37 weeks; low Apgar was defined as an Apgar score <7 at 5 minutes; and small for gestational age (SGA) was defined as a birth weight below –2 SD or <2500 g at completed 37 gestational weeks, according to the WHO definition. In contrast to low birth weight, SGA relates the birth weight to gestational week, sex and singleton or multiple gestation, and is influenced by the intrauterine growth conditions and genetic potential.20 No standardized nomenclature was used for the outcome of congenital anomalies, which were just referred to as “congenital malformations”, “congenital anomalies” or “birth defects”.
- Presentation of results: Risk estimates should be available in the article. Studies presenting only descriptive results, such as prevalence, proportions or percentages, were excluded.
Data Extraction
Screening was initially performed based on the title and abstract, followed by a full text screening by MLA. For the inclusion of records, the eligibility criteria were applied by two reviewers (MLA and LRJ) who independently screened the records for inclusion. To increase the reproducibility and accuracy of the review, the literature screening was conducted in accordance with the Preferred Reporting Items for Systematic reviews and Meta-Analyses (PRISMA 2020) checklist and using the web-based program covidence.org at the University Library of Southern Denmark. Disagreements were resolved through discussion and consensus with a third reviewer (BMN).
Data extracted from the included studies are presented in Tables 1–3. The analyses consist of summarizing the risks of adverse birth, childhood and adolescence health outcomes among offspring of women with MS. We considered a meta-analysis, but the number of studies identified within each group was too low, too few studies reported on specific outcomes and the exposures were too inhomogeneous. The authors were aware of a few existing systematic reviews and meta-analyses on birth outcomes among women with MS and DMT from 2000–2019,21,22 and decided to conduct an up-to-date search in this subgroup of studies.
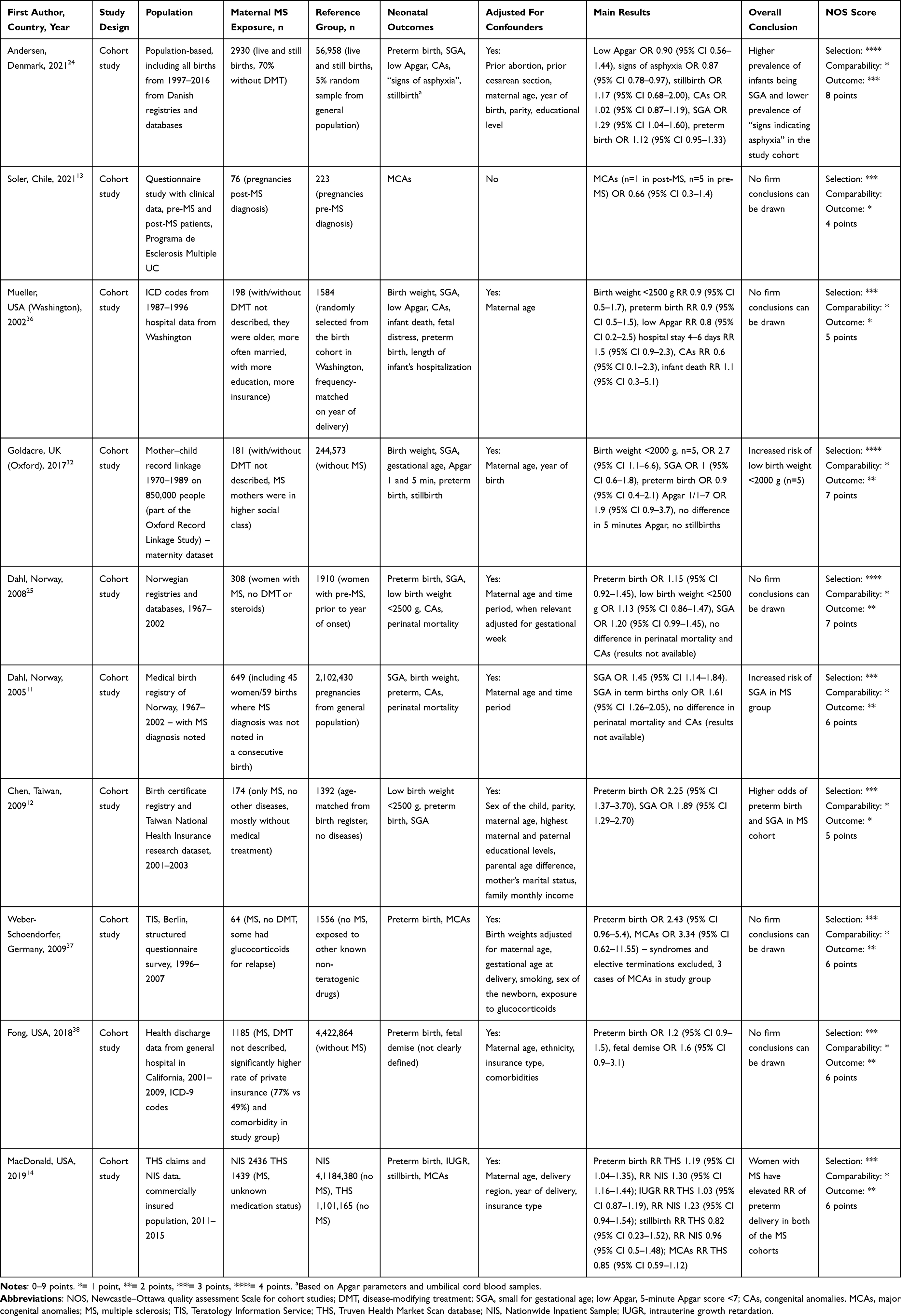 |
Table 1 Maternal Multiple Sclerosis and the Effect on Neonatal Outcomes |
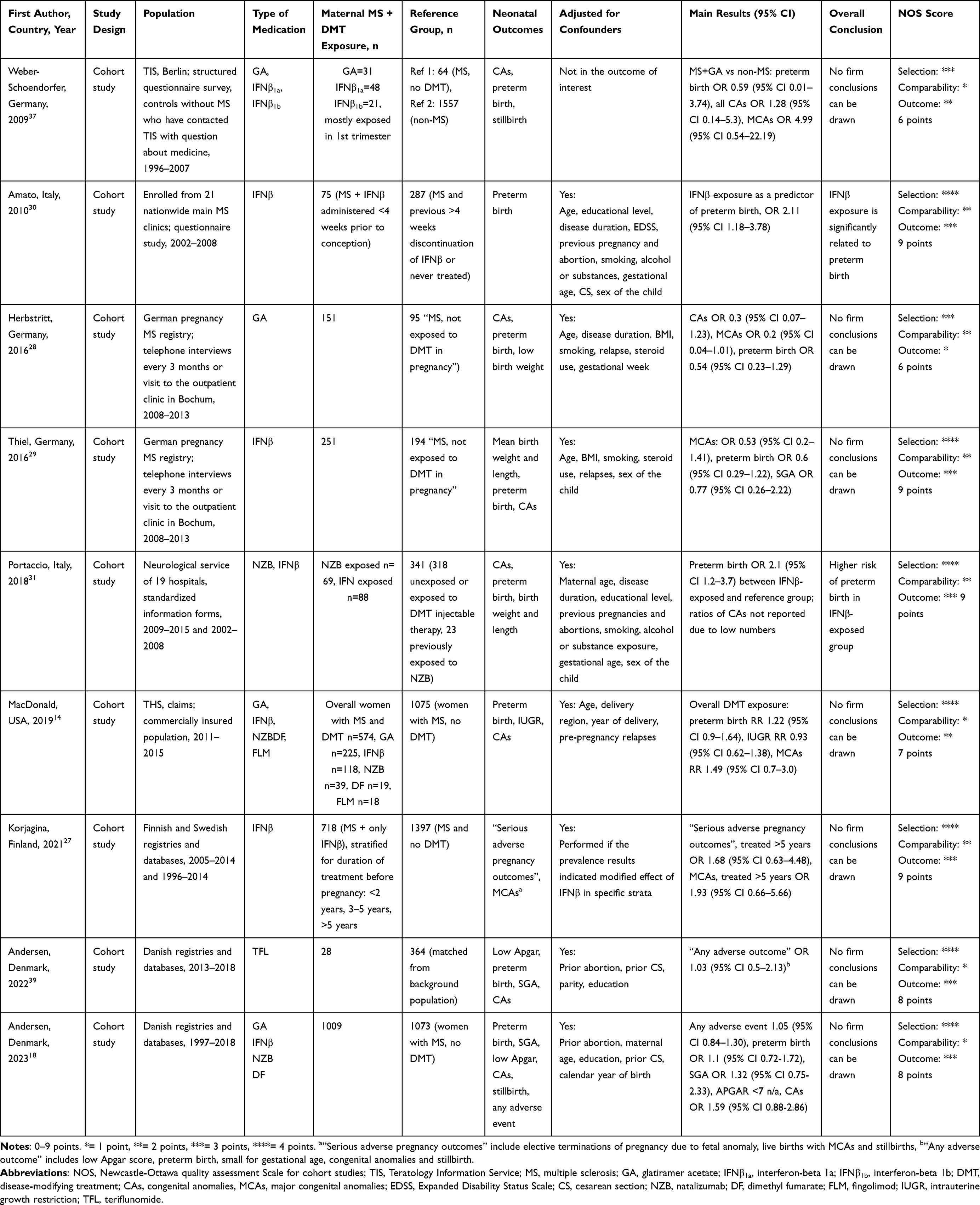 |
Table 2 Women with Multiple Sclerosis Treated with Disease-Modifying Treatment and the Effect on Neonatal Outcomes |
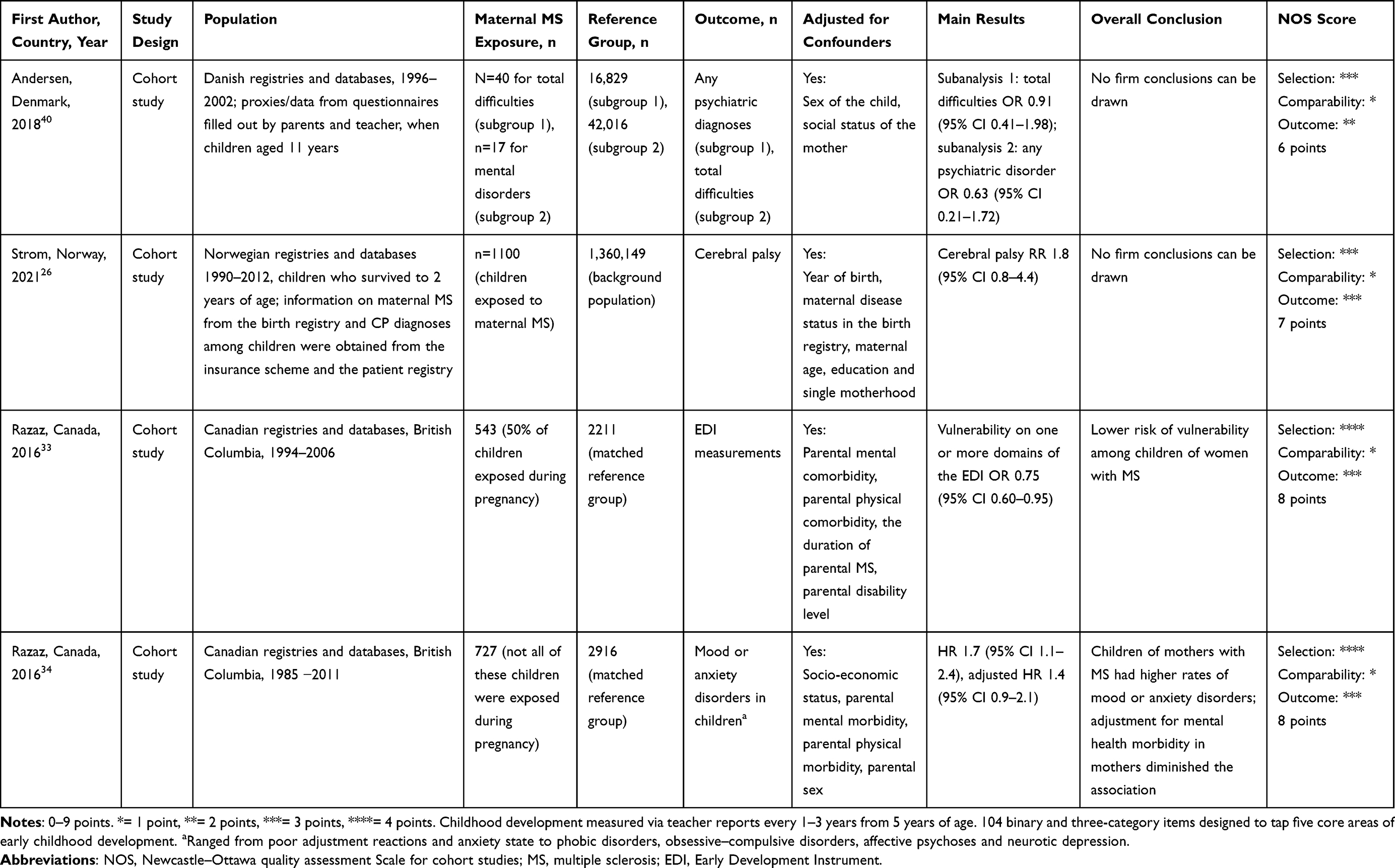 |
Table 3 In Utero Exposure to Maternal Multiple Sclerosis Health Outcomes During Childhood and Adolescence (1 Month to 18 Years) |
The quality of the included studies was assessed using the Newcastle–Ottawa Scale (NOS) tool for cohort studies, evaluating the risk of bias due to selection, comparability and outcome. A study could be awarded a maximum of one star for each numbered item in the selection and outcome categories.23 A maximum of two stars can be given for comparability. A maximum of 9 points can be given to studies of the highest quality. Two authors (MLA and LRJ) performed the assessment independently. In situations of disagreement, consensus was reached via discussion. The assessments of the risk of bias are presented in Tables 1–3.
Results
Literature Search and Study Selection
The initial literature search identified 1035 studies by title, of which 944 were outside the scope of the review. A total of 91 studies were screened by abstract, and 77 were assessed in full. Only 21 studies were included, and five of them were newly published in 2021/2022. An up-to-date search added one more study in group 2. Characteristics and summary data from the included studies are presented in Tables 1–3.
We found 10 studies that belonged to group 1: Maternal MS and short-term outcomes in the offspring (birth and neonatal). We found nine studies that belonged to Group 2: In utero exposure to medications used to treat maternal MS and short-term outcomes in the offspring (birth and neonatal). We found four studies that belonged to Group 3: Maternal MS and long-term health outcomes in the offspring (from 1 month to 18 years). One study had results that belonged to more than one group.
Study Characteristics
The studies were all cohort studies and several of them were population-based cohorts, and they represented four continents (North and South America, Asia and Europe). There were 15 European studies and eight of them were based on Scandinavian nationwide registers: Andersen et al studied the Danish population18,24,39,40 Dahl et al and Strom et al studied the Norwegian population,11,25,26 and Korjagina et al used data from Finland and Sweden in their register study.27 Two of the three German studies were based on the same dataset, but with different timeslots and exposures,28,29 and the two studies from Italy came from the same registry, but with different timeslots.30,31 One study from the UK reported as a part of the Oxford Record Linkage Study on a cohort from 1970–1989.32 Chen et al studied the population of Taiwan12 and Soler et al studied a cohort in Chile.13 The Canadian study group of Razaz et al conducted two population-based register studies from British Columbia on long-term outcomes in children.33,34 Three studies came from the USA: two cohort studies from Boston, using data from the same administrative claims database,14,35 and one study from Washington.36
Group 1 Studies: Maternal MS and Short-Term Outcomes in the Offspring (Birth and Neonatal)
We found 10 studies in total in this category. These studies examined the association between maternal MS diagnosed before the time of conception and birth and neonatal outcomes in the offspring. The majority focused on short-term birth outcomes, including 5-minute Apgar <7, SGA/low birth weight, preterm birth, congenital anomalies and stillbirth, among the offspring of women with MS.
Preterm Birth
Nine of the group 1 studies reported on the outcome of preterm birth. Two of these studies found a significantly increased risk of preterm birth in women with MS.12,14 MacDonald et al used the Truven Health MarketScan Database (2011–2015; Truven Health Analytics Inc, Ann Arbor, Michigan) and the Nationwide Inpatient Sample (2007–2011) to identify birth cohorts. Women with MS were compared with the background population, and they found an RR of 1.19 (95% CI 1.04–1.35) for preterm birth in the Truven Database and RR 1.30 (95% CI 1.16–1.44) for preterm birth in the Nationwide Inpatient Sample.14 The main limitation of the Truven Health MarketScan Database was that 728,337 pregnancies (39.8%) were excluded owing to non-continuous enrollment during the period from 90 days before the last menstrual period to the delivery date, which could introduce selection bias. However, they have made a comparison of some of the covariates on the included and excluded women, stating them to be similar beside year of birth. In a study by Chen et al from Taiwan, the OR for preterm birth was 2.25 (95% CI 1.37–3.70).12 Comparison was made with an age-matched control group without any diseases. From our perspective, the two studies missed adjustment for some important potential confounders, such as maternal comorbidities, smoking, body mass index (BMI) and medical treatment. None of the other six studies reporting on preterm birth as an outcome had sufficient statistical power to draw conclusions on the risk of preterm birth.24,25,32,36–38
SGA and Low Birth Weight
Six studies reported SGA and three of them found a significantly increased risk, with OR 1.29–1.89, among children of women with MS compared to a reference group without MS.12,24,25 The study by Chen et al found an increased risk of SGA, with OR 1.89 (95% CI 1.29–2.70). It is worth noting that the study is classified as being nationwide and population based, but the cohort consists of only 174 women with MS compared with 1392 healthy controls, and the population of the island consists of 23 million people.12 One must therefore assume that the cohort constitutes only a small proportion of the women on the island with MS giving birth. A study by Dahl et al found an increased risk of SGA, with OR 1.45 (95% CI 1.14–1.84), in the MS group compared to the background population.25 A study by Goldacre et al found an increased risk of low birth weight <2000 g, with OR 2.7 (95% CI 1.10–6.60), but based on only five cases in the MS group, which should probably be interpreted as a random distribution.32 In contrast to these studies, three other studies reporting on SGA did not find any significant differences. Goldacre et al found an equal distribution, with OR 1.0 (95% CI 0.60–1.80), in their dataset from 1970–1989.32 Dahl et al found OR 1.20 (95% CI 0.99–1.45) in their study on a sample of MS patients in Norway.25 Mueller et al reported on the outcome of low birth weight <2500 g unadjusted for gestational age, and found RR 0.9 (95% CI 0.50–1.70).36 MacDonald et al reported on the outcome of poor fetal growth (diagnosed before birth) in their two study cohorts from different databases, and found OR 1.03 (95% CI 0.87–1.19) and OR 1.23 (95% CI 0.94–1.54). They did not present data on birth weight results in their study.14
Low Apgar Score
Three studies reported on low 5-minute Apgar score. None of these found an increased risk among children of women with MS.24,32,36 The Danish cohort study by Andersen et al reported an outcome called “signs of asphyxia”, including elements from the Apgar evaluation together with umbilical cord blood sample. This outcome was lower in the exposed group of children born to women with MS, with OR 0.87 (95% CI 0.78–0.97).24
Congenital Anomalies
Six of the group 1 studies reported on the outcome of congenital anomalies. MacDonald et al found OR 0.85 (95% CI 0.59–1.12) for congenital anomalies among offspring of women with MS,14 but only reported on major anomalies, whereas Weber-Schoendorfer and Schaefer reported OR 3.34 (95% CI 0.62–11.55) in the MS group, and they counted both minor and major anomalies.37 The confidence interval shows the low statistical precision, and the study was too small to provide firm conclusions. In the largest cohort study, by Andersen et al, the OR for congenital anomalies was 1.02 (95% CI 0.87–1.19).24 Mueller et al found RR 0.6 (95% CI 0.10–2.30) for congenital anomalies.36 The two Norwegian studies by Dahl et al did not report on the number of congenital anomalies, but just reported that they did not find any differences regarding congenital anomalies.11,25 Soler et al compared women with “pre-MS” and “post-MS”, but had no healthy controls in their study.13 They found OR 0.66 (95% CI 0.30–1.14) for congenital anomalies in women with pregnancy prior to MS diagnosis, compared with women who became pregnant after MS was diagnosed.
Stillbirths
Stillbirth was defined differently in the seven studies that reported on this outcome. The study by Fong et al found a risk of “fetal demise” in the MS group, with OR 1.6 (95% CI 0.90–3.10),38 whereas the largest study cohort, by Andersen et al (n=2930 women with MS), found OR 1.17 (95% CI 0.68–2.00) for stillbirth.24 Both cohort studies are, however, not large enough to draw a significant conclusion on this rare outcome. Mueller et al studied a cohort of differently insured MS patients giving birth at non-federal hospitals in Washington State, and found OR 1.1 (95% CI 0.30–5.10) on the outcome “infant death”, but did not further defined whether death was before or after birth.36 Goldacre et al found no stillbirths in their study group32 and Dahl et al reported “no difference” on the outcome “perinatal mortality”, but did not present their results as numbers.11,25 MacDonald et al found OR 0.82 (95% CI 0.23–1.52) and OR 0.96 (95% CI 0.50–1.48) in their two study cohorts.14,35
Group 2 Studies: In Utero Exposure to Medications to Treat Maternal MS and Short-Term Outcomes in the Offspring (Birth and Neonatal)
We found nine studies matching group 2 criteria. Eight reported on the outcome of congenital anomalies and preterm birth. Four studies reported on the outcome of SGA, low birth weight or intrauterine growth restriction (IUGR). Two studies meeting our criteria reported on the outcome of stillbirth. A systematic review and meta-analysis of pregnancy and fetal outcomes among women with MS and DMT was published in 2020.21 Here, Lopez-Leon et al included studies from the period January 2000 to August 2019 and reviewed the current literature on the impact of DMT. In contrast to this review, studies without calculated risk estimates were included. In their meta-analyses, they found no increased risk of preterm birth after stratification according to glatiramer acetate (two studies, n=288), with RR 0.79 (95% CI 0.56–1.12), interferon-β (four studies, n=704), with RR 0.92 (95% CI 0.58–1.46), or natalizumab (two studies, n=79), with RR 0.82 (95% CI 0.57–1.18). In all studies, the exposed children were compared with children of mothers with MS who did not take DMT before or during pregnancy. Regarding major congenital anomalies, they found four studies reporting this outcome among children exposed to interferons (n=423), with RR 0.70 (95% CI 0.3–1.6), and glatiramer acetate (n=188), RR 0.58 (95% CI 0.16–2.12).
Only a few additional papers have been published in this category since the study by Lopez-Leon et al.21 Three studies, published in the period January 2019 to February 2023, met our inclusion criteria. A Swedish cohort study focused on interferon-β-exposed children (n=718),27 and one Danish cohort study focused on teriflunomide-exposed children (n=49)39 and another on injectable first-line treatments, dimethyl fumarate and natalizumab-exposed children (n=711 liveborns).18 None of the three studies found significant differences in the risk of adverse short-term birth outcome between DMT-exposed and unexposed children.
Group 3 Studies: Maternal MS and Long-Term Health Outcomes in the Offspring (from 1 Month to 18 Years)
We included four studies that reported on long-term outcomes in children.26,33,34,40 Two of the studies reported on psychiatric outcomes, one study reported on educational outcome and one study on neurological outcome. Andersen et al studied mental health at age 11 years among children of women with MS and did not find an association with psychiatric diagnoses, compared to children of mothers without MS.40 A register study by Strom et al followed a total of 1,360,149 Norwegian children for a period of 2–24 years. A total of 3575 children were diagnosed with cerebral palsy in the background population (2.6 per 1000 live births), and among children of mothers with MS, they found an increased prevalence of 3 per 1000 live births with cerebral palsy, RR 1.8 (95% CI 0.80–4.40). The result was not statistically significant.26 Razaz et al examined vulnerability in the social development domain according to the Early Development Instrument among 1- and 3-year-old children of parents with MS. Children exposed to maternal MS had a lower risk of vulnerability compared to children of women without MS, OR 0.75 (95% CI 0.60–0.95).33 Razaz et al also examined mood and anxiety disorders, ranging from poor adjustment reactions and anxiety to phobic disorders, obsessive–compulsive disorders, affective psychoses and neurotic depression, among children of parents with MS in another set-up. Outcomes of interest were identified using a combination of hospital diagnoses, outpatient physician diagnoses and prescription drug claims. In children of women with MS, the HR for the combined outcome “mood or anxiety disorders” was 1.7 (95% CI 1.10–2.40), but it decreased when adjusting for maternal mental comorbidity, HR 1.4 (95% CI 0.90–2.10).34
Discussion
Our objective was to provide an overview of the existing literature on the reproductive area of women with MS and to identify the research gaps in this area. Solid knowledge about short- and long-term child outcomes is imperative for clinicians to adequately counsel women with MS in reproductive matters. The studies pointed towards an increased risk of preterm birth and SGA among women with MS. In terms of women with MS treated with DMT prior to or during pregnancy, no clear conclusions could be drawn. The few studies on long-term child outcomes focused mainly on neurodevelopmental and psychiatric impairments, and one study reported on the long-term risk of cerebral palsy among children of women with MS. None of these studies reported any significant findings. In this systematic review, we have highlighted the research gaps on the impact of maternal MS on offspring health.
We focused on adverse offspring outcomes, such as low birth weight, SGA and preterm birth, which are outcomes that are important predictors of neonatal and childhood morbidity and mortality, but also predictors for morbidities in adulthood.41 Long-term health outcomes normally include the risk of diseases and development in the offspring during childhood, adolescence or as far as the follow-up time allows. However, the impact of maternal MS on long-term child outcomes has received minor attention, and we found only four studies on long-term child outcomes. One reason why this is the case may be related to the high demand for appropriate datasets with complete and long follow-up time on all individuals. We know from the literature that children of parents with MS have a minor increased risk of developing MS themselves,42 but otherwise we know very little about the impact of in utero exposure to maternal MS, DMT and the influence on the risk of the offspring developing diseases in the first years of life, and during childhood and adolescence.
We found results pointing towards children of women with MS being at higher risk of adverse birth outcomes, such as being born preterm, SGA or with low birth weight, but with the proviso that the relevant studies mostly were of mediocre quality (NOS scores 5–8). A significantly increased risk of congenital anomalies or stillbirth was not found in any of the present studies, which were, however, often underpowered to study this outcome. Furthermore, most of the exposed cohorts in this category were a mixture of patients with and without DMT and were not stratified for this, which means that the results have a limited applicability. Regarding the outcome of congenital anomalies, this is not a very well-described outcome in the available literature and, together with the outcome of stillbirth, no studies had the required statistical power to conclude on the calculated risk estimates. Typically, the cohorts were not only exposed to MS and not compared to healthy controls either, which would be the preferred study design on which to draw conclusions. We conclude that none of the present studies has the statistical power to conclude on the risk of congenital anomalies or stillbirth with certainty.
Regarding medical treatment of young women with MS, there are currently two preparations generally recognized by the European Medicines Agency and the American Food and Drug Administration as potential treatment options during pregnancy. These are the two most commonly used drugs for pregnant women with MS:35,43 glatiramer acetate, which hypothetically induces Th2 cells to release cytokines that are able to suppress inflammatory processes in the MS lesions, and interferon-β, which, among other things, reduces the expression of adhesion molecules of the lymphocytes and thereby the passage of activated T cells across the blood–brain barrier. Glatiramer acetate and interferon-β do not appear to increase the risk of adverse birth outcomes and are already prescribed for use during pregnancy to a great extent, but regarding the long-term health consequences in the offspring there is a critical research gap. These two preparations have been used for almost 25 years, and long-term consequences after maternal use at the time of conception ought to have been an important research area. The issue is naturally a great concern for young women with MS who are considering having children. To the best of our knowledge, no study has yet examined the association between maternal use of specific MS medication around the time of conception and long-term health consequences in the offspring.
Studies in the past decade have intended to shed light on the consequences in the offspring of in utero exposure to these preparations affecting the immune system, but the studies have been based on small cohorts, and the results have been divergent and characterized by exposure and outcome inhomogeneity. Therefore, a potential negative impact on the fetus still has to be investigated. Patients worry about the impact of MS and MS medication on short- and long-term health consequences in the offspring, and some women will choose not to continue their DMT during pregnancy37 or will decide not to have children owing to the lack of knowledge in this area.3 The authors found a number of pharmacovigilance studies produced by pharmaceutical companies, but since they lack control groups, these studies do not have the methodological quality to enable safety conclusions to be drawn from them. In addition, we decided to exclude studies that focused on biometric measures, emotional and behavioral difficulties or educational achievements in the offspring, instead of risk estimates of diseases in offspring of women with MS.44–46
To be able to provide precise results on rare and serious outcomes such as stillbirth and congenital anomalies, we need methodologically solid studies based on a larger number of children. We can fully endorse the conclusion from the systematic review and meta-analysis from 2020 by Lopez-Leon et al, that future studies including internal comparators are still needed.21
The cumulative amount of data is indeed sparse and there is a great need for more evidence in this area. There is still a large gap in the literature with regard to studies on long-term somatic health outcomes among children of women with MS, and only a few studies exist on the association between maternal MS and long-term health outcomes in the offspring. One study reported on the outcome of cerebral palsy, but the rest were on mental and social outcomes, which could be related to growing up in an environment with a parent with MS rather than the intrauterine exposure to the disease. It is challenging to advise patients about the safety of medications with regard to exposed offspring when most studies on adverse consequences in the offspring only look at outcomes within the first year of life.
Future studies on long-term health consequences in the offspring of mothers with MS are important for these patients.
Funding
This work has been supported by Region of Southern Denmark [grant no. 20/14788, 2022], Odense University Hospital [grant no. 122-A5119 and 128-A5300, 2021], Jascha Foundation [grant no. 3630, 2020], Consultant Schou and Wife Else-Marie Schou, born Wanges Foundation [grant no. 85832].
Disclosure
Dr Mette Louise Andersen reports grants from the Region of Southern Denmark, grants from the Jascha Foundation, and grants from the Consultant Schous Foundation, during the conduct of the study. The authors declare no competing interests.
References
1. Sevelsted A, Chawes B, Stokholm J, Bonnelykke K, Bisgaard H. Time trends of chronic immune diseases by year of birth in Danish registries. Eur J Epidemiol. 2021;36:1179–1185. doi:10.1007/s10654-021-00804-x
2. Koch-Henriksen N, Magyari M. Apparent changes in the epidemiology and severity of multiple sclerosis. Nat Rev Neurol. 2021;17:676–688. doi:10.1038/s41582-021-00556-y
3. Moberg JY, Laursen B, Thygesen LC, Magyari M. Reproductive history of the Danish multiple sclerosis population: a register-based study. Mult Scler. 2020;26:902–911. doi:10.1177/1352458519851245
4. Jolving LR, Larsen MD, Fedder J, Norgard BM. Live birth in women with multiple sclerosis receiving assisted reproduction. Reprod Biomed Online. 2020;40:711–718. doi:10.1016/j.rbmo.2020.01.013
5. Lopez-Reyes L, Guio-Sanchez C, Gonzalez-Uribe C, Cardenas-Robledo S. Fertility preferences and unmet need for family planning in women with multiple sclerosis. Front Neurol. 2022;13:1035596. doi:10.3389/fneur.2022.1035596
6. Sadovnick AD, Baird PA. The familial nature of multiple sclerosis: age-corrected empiric recurrence risks for children and siblings of patients. Neurology. 1988;38:990–991. doi:10.1212/WNL.38.6.990
7. Sadovnick AD, Ebers GC, Dyment DA, Risch NJ; The Canadian Collaborative Study Group. Evidence for genetic basis of multiple sclerosis. Lancet. 1996;347:1728–1730. doi:10.1016/S0140-6736(96)90807-7
8. Robertson NP, O’Riordan JI, Chataway J, et al. Offspring recurrence rates and clinical characteristics of conjugal multiple sclerosis. Lancet. 1997;349:1587–1590. doi:10.1016/S0140-6736(96)07317-5
9. Xia Z, White CC, Owen EK, et al. Genes and Environment in Multiple Sclerosis project: a platform to investigate multiple sclerosis risk. Ann Neurol. 2016;79:178–189. doi:10.1002/ana.24560
10. O’Gorman C, Lin R, Stankovich J, Broadley SA. Modelling genetic susceptibility to multiple sclerosis with family data. Neuroepidemiology. 2013;40:1–12. doi:10.1159/000341902
11. Dahl J, Myhr KM, Daltveit AK, Hoff JM, Gilhus NE. Pregnancy, delivery, and birth outcome in women with multiple sclerosis. Neurology. 2005;65:1961–1963. doi:10.1212/01.wnl.0000188898.02018.95
12. Chen YH, Lin HL, Lin HC. Does multiple sclerosis increase risk of adverse pregnancy outcomes? A population-based study. Mult Scler. 2009;15:606–612. doi:10.1177/1352458508101937
13. Soler B, Ciampi E, Uribe-San-Martin R, et al. Pregnancy outcomes in women with multiple sclerosis. Mult Scler Relat Disord. 2021;48:102682. doi:10.1016/j.msard.2020.102682
14. MacDonald SC, McElrath TF, Hernandez-Diaz S. Pregnancy outcomes in women with multiple sclerosis. Am J Epidemiol. 2019;188:57–66. doi:10.1093/aje/kwy197
15. Coyle PK, Oh J, Magyari M, Oreja-Guevara C, Houtchens M. Management strategies for female patients of reproductive potential with multiple sclerosis: an evidence-based review. Mult Scler Relat Disord. 2019;32:54–63. doi:10.1016/j.msard.2019.04.003
16. Bove RM, Houtchens MK. Pregnancy management in multiple sclerosis and other demyelinating diseases. Continuum. 2022;28:12–33. doi:10.1212/CON.0000000000001108
17. Siracusano M, Carloni E, Riccioni A, et al. Maternal multiple sclerosis and offspring’s cognitive and behavioral development: what do we know until now? Children. 2022;9:1. doi:10.3390/children9111716
18. Andersen JB, Sellebjerg F, Magyari M. Pregnancy outcomes after early fetal exposure to injectable first-line treatments, dimethyl fumarate, or natalizumab in Danish women with multiple sclerosis. Eur J Neurol. 2023;30:162–171. doi:10.1111/ene.15559
19. McDonald WI, Compston A, Edan G, et al. Recommended diagnostic criteria for multiple sclerosis: guidelines from the International Panel on the diagnosis of multiple sclerosis. Ann Neurol. 2001;50:121–127. doi:10.1002/ana.1032
20. Marsal K, Persson PH, Larsen T, Lilja H, Selbing A, Sultan B. Intrauterine growth curves based on ultrasonically estimated foetal weights. Acta Paediatr. 1996;85:843–848. doi:10.1111/j.1651-2227.1996.tb14164.x
21. Lopez-Leon S, Geissbuhler Y, Sabido M, Turkson M, Wahlich C, Morris JK. A systematic review and meta-analyses of pregnancy and fetal outcomes in women with multiple sclerosis: a contribution from the IMI2 ConcePTION project. J Neurol. 2020;267:2721–2731. doi:10.1007/s00415-020-09913-1
22. Simone IL, Tortorella C, Ghirelli A. Influence of pregnancy in multiple sclerosis and impact of disease-modifying therapies. Front Neurol. 2021;12:697974. doi:10.3389/fneur.2021.697974
23. D’Andrea E, Vinals L, Patorno E, et al. How well can we assess the validity of non-randomised studies of medications? A systematic review of assessment tools. BMJ Open. 2021;11:e043961. doi:10.1136/bmjopen-2020-043961
24. Andersen JB, Kopp TI, Sellebjerg F, Magyari M. Pregnancy-Related and perinatal outcomes in women with multiple sclerosis: a nationwide Danish cross-sectional study. Neurol Clin Pract. 2021;11:280–290. doi:10.1212/CPJ.0000000000001035
25. Dahl J, Myhr KM, Daltveit AK, Gilhus NE. Pregnancy, delivery and birth outcome in different stages of maternal multiple sclerosis. J Neurol. 2008;255:623–627. doi:10.1007/s00415-008-0757-2
26. Strom MS, Tollanes MC, Wilcox AJ, Lie RT, Forthun I, Moster D. Maternal chronic conditions and risk of cerebral palsy in offspring: a national cohort study. Pediatrics. 2021;147:1. doi:10.1542/peds.2020-1137
27. Korjagina M, Hakkarainen KM, Burkill S, et al. Prevalence of adverse pregnancy outcomes after exposure to interferon beta prior to or during pregnancy in women with MS: stratification by maternal and newborn characteristics in a register-based cohort study in Finland and Sweden. Mult Scler Relat Disord. 2021;48:102694. doi:10.1016/j.msard.2020.102694
28. Herbstritt S, Langer-Gould A, Rockhoff M, et al. Glatiramer acetate during early pregnancy: a prospective cohort study. Mult Scler. 2016;22:810–816. doi:10.1177/1352458515623366
29. Thiel S, Langer-Gould A, Rockhoff M, et al. Interferon-beta exposure during first trimester is safe in women with multiple sclerosis-A prospective cohort study from the German multiple sclerosis and pregnancy registry. Mult Scler. 2016;22:801–809. doi:10.1177/1352458516634872
30. Amato MP, Portaccio E, Ghezzi A, et al. Pregnancy and fetal outcomes after interferon-beta exposure in multiple sclerosis. Neurology. 2010;75:1794–1802. doi:10.1212/WNL.0b013e3181fd62bb
31. Portaccio E, Annovazzi P, Ghezzi A, et al. Pregnancy decision-making in women with multiple sclerosis treated with natalizumab: I: fetal risks. Neurology. 2018;90:e823–e31. doi:10.1212/WNL.0000000000005067
32. Goldacre A, Pakpoor J, Goldacre M. Perinatal characteristics and obstetric complications in mothers with multiple sclerosis: record-linkage study. Mult Scler Relat Disord. 2017;12:4–8. doi:10.1016/j.msard.2016.11.011
33. Razaz N, Joseph KS, Boyce WT, et al. Children of chronically ill parents: relationship between parental multiple sclerosis and childhood developmental health. Mult Scler. 2016;22(11):1452–1462. doi:10.1177/1352458515621624
34. Razaz N, Tremlett H, Boyce T, Guhn M, Marrie RA, Joseph KS. Incidence of mood or anxiety disorders in children of parents with multiple sclerosis. Paediatr Perinat Epidemiol. 2016;30(4):356–366. doi:10.1111/ppe.12290
35. MacDonald SC, McElrath TF, Hernández‐Díaz S. Use and safety of disease-modifying therapy in pregnant women with multiple sclerosis. Pharmacoepidemiol Drug Saf. 2019;28(4):556–560. doi:10.1002/pds.4735
36. Mueller BA, Zhang J, Critchlow CW. Birth outcomes and need for hospitalization after delivery among women with multiple sclerosis. Am J Obstet Gynecol. 2002;186(3):446–452. doi:10.1067/mob.2002.120502
37. Weber-Schoendorfer C, Schaefer C. Multiple sclerosis, immunomodulators, and pregnancy outcome: a prospective observational study. Mult Scler. 2009;15(9):1037–1042. doi:10.1177/1352458509106543
38. Fong A, Chau CT, Quant C, Duffy J, Pan D, Ogunyemi DA. Multiple sclerosis in pregnancy: prevalence, sociodemographic features, and obstetrical outcomes. J Matern Fetal Neonatal Med. 2018;31(3):382–387. doi:10.1080/14767058.2017.1286314
39. Andersen JB, Wandall-Holm MF, Magyari M. Pregnancy outcomes following maternal or paternal exposure to teriflunomide in the Danish MS population. Mult Scler Relat Disord. 2022;59:103529. doi:10.1016/j.msard.2022.103529
40. Andersen JB, Moberg JY, Niclasen J, Laursen B, Magyari M. Mental health among children of mothers with multiple sclerosis: a Danish cohort and register-based study. Brain Behav. 2018;8(10):e01098. doi:10.1002/brb3.1098
41. Barker DJ. The origins of the developmental origins theory. J Intern Med. 2007;261(5):412–417. doi:10.1111/j.1365-2796.2007.01809.x
42. Compston A, Coles A. Multiple sclerosis. Lancet. 2002;359(9313):1221–1231. doi:10.1016/S0140-6736(02)08220-X
43. Tillaut H, Degremont A, Kerbrat S, et al. Pregnancy in women with multiple sclerosis in France from 2010 to 2015: incidence, outcomes, and exposure to disease-modifying therapies. Mult Scler. 2022;28(5):778–789. doi:10.1177/13524585211035376
44. Marozio L, Cavalla P, Sottemano S, et al. Fetal and post-natal growth in infants of mothers with multiple sclerosis: a case-control stud. Mult Scler Relat Disord. 2022;65:104087. doi:10.1016/j.msard.2022.104087
45. Moberg JY, Magyari M, Koch-Henriksen N, Thygesen LC, Laursen B, Soelberg Sorensen P. Educational achievements of children of parents with multiple sclerosis: a nationwide register-based cohort study. J Neurol. 2016;263(11):2229–2237. doi:10.1007/s00415-016-8255-4
46. Diareme S, Tsiantis J, Kolaitis G, et al. Emotional and behavioural difficulties in children of parents with multiple sclerosis: a controlled study in Greece. Eur Child Adolesc Psychiatry. 2006;15(6):309–318. doi:10.1007/s00787-006-0534-7
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.