")
Back to Journals » International Journal of General Medicine » Volume 17
Methods for Clinical Monitoring of Neuromuscular Transmission in Anesthesiology – A Review
Authors Radkowski P, Barańska A, Mieszkowski M , Dawidowska-Fidrych J, Podhorodecka K
Received 5 August 2023
Accepted for publication 8 November 2023
Published 3 January 2024 Volume 2024:17 Pages 9—20
DOI https://doi.org/10.2147/IJGM.S424555
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Paweł Radkowski,1– 3 Agnieszka Barańska,1 Marcin Mieszkowski,1,2 Justyna Dawidowska-Fidrych,4 Katarzyna Podhorodecka1
1Department of Anaesthesiology and Intensive Care, Regional Specialist Teaching Hospital, Olsztyn, Poland; 2Department of Anaesthesiology and Intensive Care, School of Medicine, Collegium Medicum, University of Warmia and Mazury, Olsztyn, Poland; 3Department of Anaesthesiology and Intensive Care, Hospital zum heiligen Geist, Fritzlar, Germany; 4Pediatric Department, Hospital Pro-Medica, Ełk, Poland
Correspondence: Katarzyna Podhorodecka, Email [email protected]
Abstract: The administration of general anesthesia is a crucial aspect of surgery. However, it can pose significant risks to patients, such as respiratory depression and prolonged neuromuscular blockade. To avoid such complications, it is essential to monitor neuromuscular transmission during anesthesia. While clinical tests have been used for decades to evaluate muscle function, they are now known to be unreliable, and relying on them increases the risk of postoperative complications. Thankfully, there are now six methods available for neuromuscular monitoring during anesthesia: mechanomyography, acceleromyography, electromyography, kinemyography, phonomyography, and compressomyography. Each of these methods differs in terms of their approach and methodology, and their importance in clinical practice varies accordingly. Mechanomyography involves measuring the mechanical response of a muscle to nerve stimulation, while acceleromyography measures the acceleration of muscle contraction. Electromyography records the electrical activity of muscles, while kinemyography tracks muscle movement. Phonomyography records the sound waves produced by contracting muscles, and compressomyography involves monitoring the pressure changes in a muscle during contraction. Overall, understanding the differences between these methods and their clinical significance is crucial for anesthesiologists. This review aims to provide an updated understanding of the current methods available for neuromuscular monitoring during anesthesia, so that anesthesiologists can make informed decisions about patient care and reduce the risk of postoperative complications.
Keywords: neuromuscular monitoring, neuromuscular blockade, peripheral nerve stimulation, anesthesiology, review
Introduction
Neuromuscular monitoring is a relatively young branch of medicine and neurophysiology. The discovery of its basic functions took place in 1941, when Harvey and Masland discovered a decrease in muscle response after repetitive stimulation.1 14 years later Botelho made the first measurements using mechanomyography and electromyography.2 In 1958, Christie and Churchill-Davidson constructed the first tool to monitor intraoperative neuromuscular transmission – St. Thomas Hospital’s Nerve Stimulator.3 The first reports of guidelines for dealing with patients treated with non-depolarizing muscle relaxants were published in 2009 at the initiative of the Working Party on Post Anaesthesia Care.4 In 2018, a group of experts set basic guidelines for dealing with patients treated with muscle relaxants.5 They argue that any patient given a non-depolarizing relaxant should be subjected to objective neuromuscular monitoring, as neither subjective methods nor clinical tests are sufficiently sensitive to detect residual neuromuscular blockade and should not be practiced. There is an emphasis on the fact that there should be guidelines for managing patients that are administered muscle relaxants and to standardize the time frames measured that are associated with this procedure.4 The most common technique for assessing the degree of muscle relaxation and neuromuscular conduction is by train of four (TOF).6 This method involves sending a series of four electrical pulses every 0.5 seconds in 10 second intervals, through electrodes attached to an easily accessible peripheral nerve. The muscle response to the stimulation described above is evaluated. On this basis, the TOF ratio is calculated, ie the ratio of 4th to the 1st response (T4/T1). Based on current knowledge, patients can be safely extubated once the TOF ratio > 0.9 whereas a TOF ratio <0.9 is predictive of striated muscle relaxation.7 In some countries, Anesthesiology Associations have already published detailed guidelines, eg in the UK and Ireland, it has been highlighted that the need for neuromuscular monitoring in all patients who have been administered muscle relaxants from the time of induction to the complete return of neuromuscular transmission (TOFR> 0.9) and the patient’s consciousness.8 Similar standards have been issued in Australia and New Zealand.9 In Poland, according to the “Regulation of the Minister of Health of December 2016 on the organizational standards of healthcare in the field of anaesthesiology and intensive care”, there should be a device for monitoring neuromuscular transmission designated for each patient station.10 Despite this rather long and well-documented history of guidelines, objective neuromuscular monitoring is still not routinely used in clinical practice in many centers. There are many reasons for this fact: some physicians believe that objective neuromuscular transmission monitoring is time-consuming and unnecessary (and relying solely on clinical symptoms is sufficient) despite having the appropriate equipment. Other clinicians, however, lack adequate equipment. Clinical dose-response of muscle relaxants is individual for each patient and is difficult to predict.6 In clinical practice, the necessary tool to assess the degree of muscle relaxation is objective monitoring of neuromuscular function. Preserving muscle relaxation after surgery could be fatal for the patient. The phenomenon of residual neuromuscular block is more common in elderly, female, and hypothermic patients.11 Fortunately, this can be avoided by the appropriate assessment of a patient and by carefully monitoring the degree of muscle relaxation.6
Assessment of muscle function on the basis of clinical tests, despite its long history of use, is today considered a very unreliable method and should not be applied in clinical practice. The instrumental method of objective monitoring is now the primary strategy used to avoid residual muscle relaxation during patient recovery from general anesthesia and involves electrical stimulation of the motor nerve and monitoring the response of the muscle supplied by this nerve (Table 1). Direct methods, which do not use any instruments, include the assessment of neuromuscular recovery and transmission only on the basis of clinical tests (Table 1). However, this method is unreliable even when carried out by an experienced anaesthesiologist which, unfortunately, is still often practiced and may lead to a situation in which the patient’s life will be endangered.
 |
Table 1 Methods of Neuromuscular Transmission Monitoring |
Instrumental methods of monitoring can be divided into subjective and objective ones. The subjective instrumental method is based on a visual or tactile assessment of the neuromuscular response to a given stimulus. No device for analyzing and recording the measurement result is required. Therefore, the quality of such assessment depends on the experience of the person conducting it. Unfortunately, at TOFR < 0.4, residual muscle relaxation is often ambiguously or incorrectly interpreted even by an experienced clinician. To minimize this problem, alternative stimulation modules such as DBS (double burst stimulation) have been introduced. Using this method, the detectability of the residual neuromuscular blockade was improved, but only to TOFR = 0.6.12 Taking into consideration the above stated and the fact that according to the current guidelines, the TOFR factor that is safe for extubation is when factor TOFR>0.9 (which cannot be determined by subjective methods), the best methods for monitoring neuromuscular transmission are currently considered to be the objective methods, which include: acceleromyography (AMG), mechanomyography (MMG), electromyography (EMG), kinemyography (KMG), phonomyography (PMG) and the newest with a non-official name “compressomyography”.
Currently, in clinical practice, the most common method of neuromuscular transmission objective monitoring is acceleromyography (eg TOF-Watch XS).13–15 PMG is a relatively new method that is still being researched and is not applicable in clinical practice. In addition to separate monitoring devices, modules added to dedicated monitors are also available on the market. The most frequently used stimulation mode by anaesthesiologists is TOF.16–21 When discussing the topic further, it should be noted that in order to increase the accuracy of measurements conducted with objective instrumental methods, each time before the first administration of the muscle relaxant, the device should be calibrated (which does not apply to new generation devices: TOF-Scan, Stimpod, Stimpod NMS 450X and wireless monitor-WiTOF) in order to determine the reference values. Calibration involves finding a supramaximal current that identifies the best stimulating current that minimizes background noise. Supramaximal stimulation is the electrical stimulus 15 to 20% above that is necessary to produce contraction of all the muscle fibers supplied to a nerve. Since such calibration is unpleasant for the patient, it is performed after administration of the analgesic and anesthetic.22–25 The advantage of objective methods of assessing the degree of muscle relaxation is the lack of influence on the result of simultaneously administered intravenous anesthetics, opioids and inhaled anesthetics. The methods used to monitor neuromuscular transmission are presented in Table 1.
The use of objective neuromuscular monitoring is of great clinical importance. It provides guidance on when it is necessary to administer a maintenance dose of the muscle relaxant when to start pharmacological termination of neuromuscular blockade, and helps determine the optimal time for intubation and, most importantly, extubation. It allows to adjust the degree of muscle relaxation to the needs of surgery that allows safe recovery of the patient from general anesthesia and to avoid postoperative respiratory failure. Monitoring of muscle relaxation is of particular importance for trainees, because it allows them to learn about the pharmacodynamics of drugs through clinical practice. It is not without significance that it allows the hospital to reduce costs incurred in the event of unjustified administration of excessive doses of muscle relaxants or the incidence of wrong-time errors such as administration of drugs that reverse the neuromuscular blockade. Therefore, this review aims to present an update on current methods for clinical neuromuscular monitoring in anesthesiology.
Literature Review
The following keywords were used: Neuromuscular monitoring, Neuromuscular blockade, Peripheral nerve stimulation, Anesthesiology, Review. This research analyzed themes emerging from 50 articles about neuromuscular monitoring. For the article, the most up-to- date manuscripts at the moment were used, from recognized journals. The analysis was performed using the search engines Pub med and Google Scholar.
Main Sections
Objective Instrumental Methods Used for Monitoring Neuromuscular Transmission
Mechanomyography
Mechanomyography (MMG) is a method considered to be the “gold standard”, it is a direct measurement of muscle contraction strength after its stimulation.26 In other words, it is a measure of the mechanical response to a given electrical stimulus. The most common technique used in this method is stimulating the ulnar nerve. The measuring device is placed on the thumb positioned in abduction with a load of 2–3N so that the direction of the measured force of the contracting muscle is consistent with the axis of the transducer. It should be noted that the key to this method is the preload and the position of the thumb in abduction. It is also necessary to calibrate the device and determine the contraction control value before administering the muscle relaxant and after administering the hypnotics (because calibration is painful). Only after the reference value has been determined, the muscle relaxants can be administered and the appropriate measurements started. Then, by means of a transducer, the contraction force value is converted into an electrical signal and displayed on the monitor as a numerical value or in an analog manner. Assessment of the depth of the neuromuscular blockade by MMG depends on many factors and is too time-consuming to be performed in everyday clinical practice. For this reason, it is not recommended for use in clinical settings, but is used in research on muscle relaxants, where it is considered the gold standard. Another limitation of MMG is that it can only be used to monitor certain muscles (including the adductor pollicis muscle and the flexor digitorum brevis muscle). However, it does not enable monitoring of the muscles of the larynx or the diaphragm which is most important for anesthesiologists. In addition, the company producing the “Myograph 2000” apparatus has suspended its production, which is why the importance of MMG is decreasing even in the context of scientific research.23
Compressomyography (non-official name of the method, suggested by the manufacturer), a new monitoring device has appeared in 2014 in Europe, in 2019 in the USA (approved by the Food and Drug Administration), and in 2017 on the Polish market. It is the TOF-Cuff Monitor, which is essentially a modified cuff for the non-invasive measurement of blood pressure. It has built-in electrodes that stimulate the peripheral nerves located on the arm (most often the ulnar or median nerves), it is also possible to make measurements on the lower limb.27,28 This monitoring system has been validated with mechanomyography, and the detected reaction is a change in cuff pressure generated by muscle contraction in response to a given stimulus. The great advantage of this device is the ability to make measurements at any patient position and the fact it has an autopilot mode, which detects changes in the patient’s position and automatically starts measuring vital functions. It can be used during surgical procedures where the arms are tucked as the measurements do not require a free-moving thumb.29 As it is a combination of a non-invasive blood pressure monitor with a neuromuscular blockade detecting monitor, it saves time spent on putting on the equipment in cases such as an urgent caesarean section under general anesthesia. TOF-Cuff offers the possibility of measuring neuromuscular transmission in adults, while developing a pediatric cuff is still in progress. However, due to the high price of the device, it is not a popular device on the market. In a recent study published in 2020 comparing TOF-Cuff with TOF-Scan during induction of anesthesia, a significant systematic difference in time achieved with a factor of TOFR=0 was found when using both devices in obese patients. There were large intra- individual variations and clinically significant differences in non-obese and obese patients. It was concluded that the two devices were not interchangeable.30 A 2018 study comparing TOF-Cuff with AMG showed that upper extremity neuromuscular transmission measurement with the TOF-Cuff should not be used interchangeably with EMG or AMG measurements on the adductor pollicis muscle. Recovery to TOFR> 0.9 took an average of 25 minutes longer with EMG or AMG compared to the TOF-Cuff. According to the authors of the above-mentioned work, EMG and AMG are more appropriate for excluding residual muscle relaxation.31 A 2020 study of the use of TOF-Cuff on the lower limb during upper limb procedures showed high compliance with TOF-Scan results after ulnar nerve stimulation in the time ranging from the administration of a standard dose of atracurium to TOFR=0. However, this study found a high failure rate for TOF-Cuff measurements on the lower limb.27 In contrast, another 2020 study comparing TOF-Cuff and TOF-Scan found that the cuff recorded endpoints earlier than TOF-Scan. The authors of the study stated that, despite these differences, the results obtained with these methods may be important in clinical settings.32 In another study comparing TOF-Cuff and TOF-Scan over the rapid intubation sequence, no statistically significant difference was found between these devices. However, due to high variability and wide compliance limits found, the authors concluded that these devices cannot be used interchangeably.33 In a 2017 study comparing TOF-Cuff with MMG and with invasive blood pressure measurement, TOF-Cuff was shown to be effective and safe in monitoring neuromuscular blockade and NIBP (Non-Invasive Blood Pressure), but it cannot be used interchangeably with MMG.34 In a study by Markle et al from 2017, technical problems were highlighted. Among the 56 patients participating in the study, technical problems occurred at least once in 14 patients in the TOF-Cuff measurements and in 7 patients in the TOF-Scan measurements. The need to test more patients in different groups and clinical situations with TOF-Cuff was also emphasized.35
Acceleromyography
Acceleromyography (AMG) is the most commonly used technique. Its operating principle is based on the piezoelectric effect and involves the registration of the contracting muscle acceleration after its stimulation.36 The piezoelectric effect is the appearance of electric charges on the surface of a material under the influence of mechanical stress. Due to the fact that the measured value is acceleration, in practice AMG is used in areas of the body where the effect of nerve stimulation is easy to measure. Most commonly, the ulnar nerve is used for this purpose and measures the acceleration of the adductor pollicis muscle. The electrodes are placed superiorly to where the ulnar nerve runs on the ventral side of the wrist, while the acceleration sensor is attached to the thumb. The movement of the finger (as a result of nerve stimulation) generates an electric current, the intensity depends on the acceleration of the moving finger. In summary, if the thumb is a solid, freely moving mass, the measured acceleration according to Newton’s Second Law of Motion (Force = Mass x Acceleration) is used to determine the force developed by the stimulated muscle. Moreover, it is also possible to measure the acceleration after stimulation of the posterior tibial nerve and the facial nerve (flexor digitorum brevis muscle, orbicularis oculi muscle, corrugator supercilii muscle).37,38 While the neuromuscular blockade at the orbicularis oculi muscle is similar to that of the adductor pollicis muscle, the corrugator supercilii muscle is much more resistant to NMBAs (Neuro-muscular Blocking Agents) and hence its blockade is more consistent with that observed on the laryngeal adductor muscles or the diaphragm. (Figure 1) 7 What is also important, AMG-based monitors are used in pediatric anesthesia.39 The first AMG-based device was invented in 1987.23 As early as 1994, the first battery-powered accelerometer was developed - the TOF-Guard, which is rarely used today. In clinical practice, AMG is easy to measure, but its use requires an appropriate position (allowing the limb to return to its initial position) and direction of movement, which will eliminate the influence of gravity (hand in supination, movement in the horizontal direction). The introduction of devices worn on the thumb has largely eliminated erroneous measurements that occur after changing the patient’s position or after the thumb has not fully returned to its original position. The value obtained is converted to TOFR and displayed on the monitor of the device.
 |
Figure 1 Neuro-muscular Blocking Agents (NMBA) - specific sensitivity of various muscle groups. The diaphragm exhibits the lowest and the pharyngeal muscles the highest sensitivity. |
The most popular accelerometric device in clinical practice is the TOF-Watch SX, which enables an accurate assessment of the neuromuscular function during the intraoperative period. One of the latest devices is the TOF-Scan, which is also based on the AMG. The thumb movement is measured in three-dimensional (as opposed to TOF-Watch measurements only in one dimension), which gives high measurement accuracy in various clinical conditions. The device has a built-in battery, which after charging, has a limited battery-life, without being connected to a power source. The use of additional equipment makes it possible to measure not only on the adductor pollicis muscle, but also the alternative muscles: the flexor digitorum and the orbicularis oculi muscles, although the latter methods are not routinely used.38 Recent studies have shown a high correlation between the measurements obtained with the calibrated TOF-Watch and with TOF-Scan without calibration. However, this applies to the data collected at TOFR 0.9, and not in the initial phases of the recovery of muscle function.40 WiTOF - is a novel device, the first wireless NMT monitor, which is available from March 2021. It simplifies accessibility to the hand or the foot of the patient and allows for optimal positioning of the monitor in the operating theatre. A set of algorithms and protocols guarantee a secure wireless communication.41
A characteristic phenomenon for devices using AMG eq. TOF-Watch and TOF-Watch SX (the reverse fade phenomenon), which is not a measurement error, and which is not observed in the case of MMG and EMG, is marking TOFR> 1.0 in the period between the calibration and the administration of the muscle relaxant.23 Acceleromyography frequently produces slightly higher recovery values than mechanomyography and electromyography measurements, therefore, AMG values cannot be directly equated with the comparators’ measurements. For this reason, some authors have proposed to »normalize- the neuromuscular recovery values measured by acceleromyography, ie by first comparing them with the baseline value, and not to assume adequate neuromuscular recovery until this normalized value equals a TOF ratio of at least 0.9. According to Liang’s 2013 study, the measurement of neuromuscular transmission using AMG is less precise than the EMG measurement, for which the TOFR measurement is often overestimated by a minimum of 0.15. Such accuracy is sufficient for clinical evaluation, but insufficient for use in research.42
Electromyography
Electromyography (EMG) is the oldest method of monitoring neuromuscular transmission. It involves measuring the electrical response of a muscle (action potential) to a given electrical stimulus. This method is based on the principle of proportionality of the muscle’s electrical activity to the force of its contraction, therefore it is called the indirect method of measuring neuromuscular transmission. The most common measurement is the EMG of the adductor pollicis muscle after stimulation of the ulnar nerve, although it is possible to record the electrical response of other muscles, eg in the lower limb. In addition to the two stimulation electrodes, this method requires another three electrodes which increase the cost of using the EMG. Most often, the measurement is given as a percentage of the control value (100%) or as TOFR. This measurement method is very accurate, but there is a possibility of signal interference by direct muscle stimulation, diathermy, incorrect connection of the device (electrodes with the GE EMG-based monitors require appropriate placement; however, most of the other EMG devices (Stimpod, Stimpod450X, TetraGraph, TwitchView) use proprietary electrodes and pathologies in neuromuscular transmission.24 Cooling down the muscles leads to an increase in the nervous response and false high results of the EMG measurements. Two new electromyography devices TwichView (Blink Device Co, Seattle, United States) and TetraGraph (Senzime, Uppsala, Sweden) are recently accepted by the FDA. In the pilot study, which compares TetraGraph with TwichView authors find that the TetraGraph underestimated the post-tetanic-count, train-of-four count and train-of-four.43 The advantage of EMG in comparison with MMG is the freedom of positioning the limb to perform the measurement, with no need for preload and stabilization. This results in the possibility of measurements on various muscles, such as the diaphragm and laryngeal muscles. In a 2019 study on 101 people, it was shown that the placement of electrodes and neuromuscular transmission measurement within the posterior tibial nerve was not a problem compared to the examination in the upper limb.44 A different study suggests that there is no statistically significant difference between the onset and recovery of neuromuscular block using electromyography for the ulnar and posterior tibial nerves.45 The order of the electrodes marked with a color code from the distal to the proximal area of the body is important, according to the manufacturer’s recommendations.46 When measuring the diaphragm action potential, recording electrodes are placed on the right side of the spine (Th12 / L1 or L1 / L2) and the right phrenic nerve is stimulated transcutaneously in the cervical segment. Neuromuscular monitoring sites are included in Table 2. and Figure 2–4.
 |
Table 2 Neuromuscular Monitoring Sites |
 |
Figure 2 Facial EMG and AMG muscle list. |
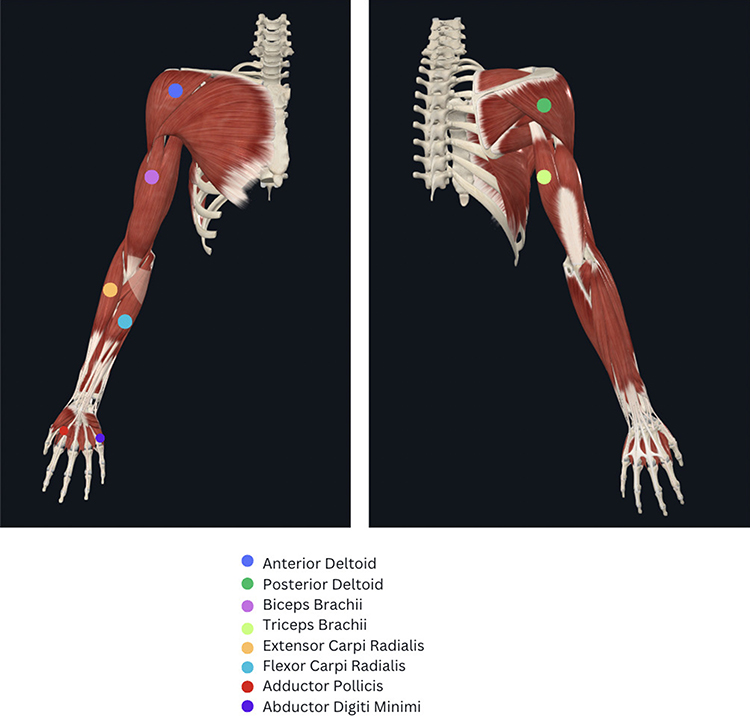 |
Figure 3 Upper Limb EMG and AMG muscle list. |
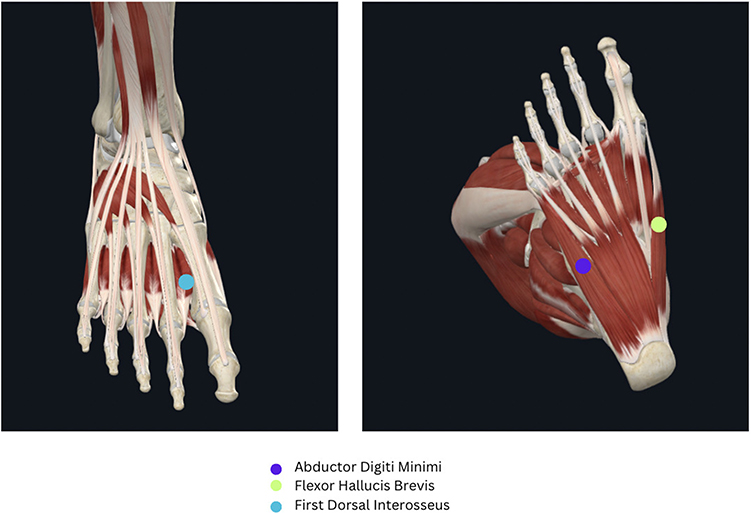 |
Figure 4 Lower Limb EMG and AMG muscle list. |
Kinemyography
Kinemyography (KMG) is the second method of monitoring neuromuscular transmission based on the piezoelectric phenomenon, but in this case, the electric current is generated not by acceleration (as in the case of AMG), but by deformation of the sensor (mechanosensor) containing piezoelectric material. A mechanical sensor is placed in the space between the thumb and forefinger. After stimulation of the ulnar nerve and contraction of the adductor pollicis muscle (causing deformation of the sensor), the neuromuscular transmission module (GE Datex-Ohmeda M- NMT Module - the most commonly known device) measures the electrical current generated during this process. Despite being based on the same phenomenon, the results collected from the KMG and AMG measurements are not completely consistent. In the study by Salminen et al from 2016 comparing the measurements of neuromuscular transmission obtained with KMG (M-NMT Mechanosensor) and EMG (ElectroSensor), it was shown that KMG gives overestimated results compared to EMG.47
Phonomyography
Phonomyography (PMG), the first studies with the use of PMG were carried out in 2004. In turn, work on an animal model appeared in 2006, which makes it a relatively new method that allows the monitoring of neuromuscular transmission, which, however, has not yet been used in clinical practice.13,48,49 During muscle contraction, a low-frequency sound is generated, which is picked up by a special microphone placed on the surface of the skin. The basis of this measurement method is the phenomenon in which the sound intensity is proportional to the contraction force generated by the muscle. This phenomenon was already described in the Baroque era by the Italian mathematician and physicist Francesco Grimaldi and published a year after his death in 1665.50 After the signal is processed - the result is displayed on the monitor in a graphic form. This method is mainly used for research purposes. PMG correlates well with MMG, EMG and AMG measurements,51,52 but is not available for clinical use. It is possible to monitor neuromuscular transmission using a variety of muscles, not just the adductor pollicis muscle.
Conclusions
According to current knowledge, return of neuromuscular transmission, defined as a factor of recovery from four consecutive stimulations (Train of Four Ratio, TOF R)> 0.9, is required for the safe extubation of the patient. The evaluation of this parameter is possible only when using objective instrumental methods of monitoring muscle strength. Subjective instrumental methods should not play a role in modern anaesthesiology because they can only detect residual neuromuscular blockade up to TOFR = 0.6. Objective instrumental methods are used to assess neuromuscular blockade by measuring the strength of muscle contraction (mechanomyography, MMG), acceleration (acceleromyography, AMG), action potential (electromyography, EMG), sensor deformation (kinemyography, KMG), sound wave (phonomyography, respectively, PMG) or pressure inside the pneumatic system (compressomyography - non-official name of the method, suggested by the manufacturer) that appear after the motor nerve that supplies the relevant muscles is stimulated.
The advantages and disadvantages of these subjective instrumental methods are set out in Table 3. The stages of operation of neuromuscular technology are included in Table 4.
 |
Table 3 Advantages and Disadvantages of Particular Methods of Neuromuscular Transmission Monitoring |
 |
Table 4 Stages of Operation of Neuromuscular Technology |
Future Directions
Despite the adoption of several standards and opinions concerning the need for objective neuromuscular monitoring during general anaesthesia with the use of muscle relaxants, the prevalence of this practice remains insufficient and, in view of the review of the following literature - mandatory. It seems necessary to provide training to raise clinicians’ awareness of the importance of objectification of the muscle relaxation degree that allows the patient to be safely carried through the process of anesthesia and recovery.
Disclosure
The authors declare that they have no competing interests.
References
1. Harvey AM, Masland RL. A method for study of neuromuscular transmission in human subjects. Bull John Hopkins Hosp. 1941;68:81–93.
2. Bothelo SY. Comparison of simultaneously recorded electrical and mechanical activity in myasthenia gravis patients and in partially curarized normal humans. Am J Med. 1955;19(5):693–696. doi:10.1016/s0002-9343(55)80010-1
3. Christie TH, Churchill-Davidson HC. The St. Thomas’s Hospital nerve stimulator in the diagnosis of prolonged apnoea. Lancet. 1958;12(7024):776–780. doi:10.1016/s0140-6736(58)91583-6
4. Vimlati L, Gilsanz F, Goldik Z. Quality and safety guidelines of postanaesthesia care: working party on post anaesthesia care (approved by the European Board and Section of Anaesthesiology, Union Eu-ropéenne des Médecins Spécialistes). Eur J Anaesthesiol. 2009;26(9):715–721. doi:10.1097/EJA.0b013e32832bb68f
5. Naguib M, Brull SJ, Kopman AF, et al. Consensus Statement on Perioperative Use of Neuromuscular Monitoring. Anesth Analg. 2018;127(1):71–80. doi:10.1213/ANE.0000000000002670
6. Cook D, Simons DJ. Neuromuscular Blockade. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2022. Available from: https://www.ncbi.nlm.nih.gov/books/NBK538301/.
7. Fuchs-Buder T. Neuromuscular Monitoring in Clinical Practice and Research. Springer Science & Business Media; 2010. doi:10.1007/978-3-642-13477-7
8. Checketts MR, Alladi R, Ferguson K, et al. Recommendations for standards of monitoring during anaesthesia and recovery 2015: association of Anaesthetists of Great Britain and Ireland. Anaesthesia. 2016;71(1):85–93. doi:10.1111/anae.13316
9. Australia and New Zealand College of Anesthetists (ANZCA). PG18(A) Guideline on monitoring during anaesthesia 2017. Available from: https://www.anzca.edu.au/getattachment/0c2d9717-fa82-4507-a3d6-3533d8fa844d/PS18-Guideline-on-monitoring-during-anaesthesia.
10. Journal of laws of the republic of Poland; Warsaw. Regulation of the minister of health of December 16, 2016. Appendix No. 1 “Conditions for anesthesiology and intensive care wards and anesthesiology wards in hospitals; 2016. Available from: https://isap.sejm.gov.pl/isap.nsf/DocDetails.xsp?id=WDU20160002218.
11. Firde M, Yetneberk T, Adem S, Fitiwi G, Belayneh T. Preventive strategies of residual neuromuscular blockade in resource-limited settings: systematic review and guideline. Int J Surg Open. 2020;26:73–80. doi:10.1016/j.ijso.2020.08.010
12. Engbaek J, Ostergaard D, Viby-Mogensen J, Skovgaard LT. Clinical recovery and train-of-four ratio measured mechanically and electromyographically following atracurium. Anesthesiology. 1989;71(3):391–395. doi:10.1097/00000542-198909000-00014
13. Trager G, Michaud G, Deschamps S, Hemmerling TM. Comparison of phonomyography, kinemyography and mechanomyography for neuromuscular monitoring. Can J Anaesth. 2006;53(2):130–135. doi:10.1007/BF03021816
14. Murphy GS, Szokol JW, Avram MJ, et al. Comparison of the TOFscan and the TOF-watch SX during recovery of neuromuscular function. Anesthesiology. 2018;129(5):880–888. doi:10.1097/ALN.0000000000002400
15. Claudius C, Viby-Mogensen J, Warner D, Warner M. Acceleromyography for use in scientific and clinical practice: a systematic review of the evidence. Anesthesiology. 2008;108(6):1117–1140. doi:10.1097/ALN.0b013e318173f62f
16. Döcker D, Walther A. Muskelrelaxanzien und neuromuskuläres Monitoring. Einführung für eine sichere klinische Anwendung. AINS. 2012;47(5):296–305. doi:10.1055/s-0032-1313567
17. Fuchs-Buder T, Mencke T. Neuromuskuläres monitoring [Neuromuscular monitoring]. Anaesthesist. 2001;50(2):129–138. German. doi:10.1007/s001010050976
18. Rossaint R, Werner C, Zwissler B. Die Anästhesiologie. Berlin: Verlag Springer; 2004:460–463.
19. Pedersen T, Viby-Mogensen J, Bang U, Olsen NV, Jensen E, Engboek J. Does perioperative tactile evaluation of the train-of-four response influence the frequency of postoperative residual neuromuscular blockade? [published correction appears in Anesthesiology 1991 Apr;74(4):797]. Anesthesiology. 1990;73(5):835–839. doi:10.1097/00000542-199011000-00007
20. Samet A, Capron F, Alla F, Meistelman C, Fuchs-Buder T. Single acceleromyographic train-of-four, 100-Hertz tetanus or double-burst stimulation: which test performs better to detect residual paralysis? Anesthesiology. 2005;102(1):51–56. doi:10.1097/00000542-200501000-00011
21. Capron F, Fortier LP, Racine S, Donati F. Tactile fade detection with hand or wrist stimulation using train-of-four, double-burst stimulation, 50-hertz tetanus, 100-hertz tetanus, and acceleromyography. Anesth Analg. 2006;102(5):1578–1584. doi:10.1213/01.ane.0000204288.24395.38
22. Brull SJ, Poloheimo M Paxisleitfaden zum Monitoring neuromuskulärer Funktionen. Anadic Medical System AG. Available from: https://www.anandic.com/bausteine.net/f/9662/Neuromuscularmonitoring-G.pdf?fd=2.
23. Fuchs-Buder T. Neuromuskuläres Monitoring in Klinik Und Forschung. Heidelberg: Springer Medizin Verlag; 2008:63–65.
24. Larsen R. Środki zwiotczające mięśnie szkieletowe. In: Anestezjologia.Vol. 1.
25. Nauheimer D, Gelder G. Monitoring in der Anästhesie. Überwachung der neuromuskulären Blockade-Methoden und Geräte. AINS. 2008;5:374–381.
26. Dahaba AA, von Klobucar F, Rehak PH, List WF. The neuromuscular transmission module versus the relaxometer mechanomyograph for neuromuscular block monitoring. Anesth Analg. 2002;94(3):591–596. doi:10.1097/00000539-200203000-00021
27. Dullenkopf A, Horn K, Steurer MP, Hess F, Welter J. Placement of TOF-Cuff® on the lower leg for neuromuscular and blood pressure monitoring during anesthetic induction for shoulder surgeries. J Anesth. 2020;34(1):79–85. doi:10.1007/s00540-019-02712-7
28. Honing GHM, Torensma B, Martini CH, et al. Comparison of neuromuscular block measured by compressomyography at the upper arm and electromyography at the adductor pollicis muscle in obese and non-obese patients: an observational study. J Clin Anesth. 2022;78:110673. doi:10.1016/j.jclinane.2022.110673
29. TOF-Cuff Viridian user manual. Available from: https://viridian.com.pl/products/toff/.
30. Markle A, Horn K, Welter J, Dullenkopf A. An observational study comparing the performance of TOF-Cuff with TOF-Scan monitoring during anaesthetic induction in clinical routine. Anaesthesiol Intensive Ther. 2020;52(3):181–186. doi:10.5114/ait.2020.98124
31. Krijtenburg P, Honing G, Martini C, et al. Comparison of the TOF-Cuff® monitor with electromyography and acceleromyography during recovery from neuromuscular block. Br J Anaesth. 2019;122(2):e22–e24. doi:10.1016/j.bja.2018.11.011
32. Markle A, Graf N, Horn K, Welter JE, Dullenkopf A. Neuromuscular monitoring using TOF-Cuff® versus TOF-Scan®: an observational study under clinical anesthesia conditions. Minerva Anestesiol. 2020;86(7):704–711. doi:10.23736/S0375-9393.20.14272-X
33. Chau I, Horn K, Dullenkopf A. Neuromuscular monitoring during modified rapid sequence induction: a comparison of TOF-Cuff® and TOF-Scan®. Australas Emerg Care. 2020;23(4):217–220. doi:10.1016/j.auec.2020.02.005
34. Veiga Ruiz G, García Cayuela J, Orozco Montes J, Parreño Caparrós M, García Rojo B, Aguayo Albasini JL. Monitoring intraoperative neuromuscular blockade and blood pressure with one device (TOF-Cuff): a comparative study with mechanomyography and invasive blood pressure. Monitorización intraoperatoria del bloqueo neuromuscular y la presión arterial con un solo dispositivo (TOF-Cuff): estudio comparativo con la mecanomiografía y la presión arterial invasiva. Rev Esp Anestesiol Reanim. 2017;64(10):560–567. doi:10.1016/j.redar.2017.03.013
35. Markle A, Horn K, Dullenkopf A, Parreño Caparrós M, García Rojo B, Aguayo Albasini JL. TOF-Cuff for relaxometry during general anaesthesia. Rev Esp Anestesiol Reanim. 2017;64(10):560–567. doi:10.1016/j.redar.2017.03.013
36. Viby-Mogensen J, Jensen E, Werner M, Nielsen HK. Measurement of acceleration: a new method of monitoring neuromuscular function. Acta Anaesthesiol Scand. 1988;32(1):45–48. doi:10.1111/j.1399-6576.1988.tb02686.x
37. Heier T, Hetland S. A comparison of train-of-four monitoring: mechanomyography at the thumb vs acceleromyography at the big toe. Acta Anaesthesiol Scand. 1999;43(5):550–555. doi:10.1034/j.1399-6576.1999.430511.x
38. Larsen PB, Gätke MR, Fredensborg BB, Berg H, Engbaek J, Viby-Mogensen J. Acceleromyography of the orbicularis oculi muscle II: comparing the orbicularis oculi and adductor pollicis muscles. Acta Anaesthesiol Scand. 2002;46(9):1131–1136. doi:10.1034/j.1399-6576.2002.460912.x
39. Kitajima T, Ishii K, Ogata H. Assessment of neuromuscular block at the thumb and great toe using accelography in infants. Anaesthesia. 1996;51(4):341–343. doi:10.1111/j.1365-2044.1996.tb07744.x
40. Colegrave N, Billard V, Motamed C, Bourgain JL. Comparison of the TOF-Scan™ acceleromyograph to TOF-Watch SX™: influence of calibration. Anaesth Crit Care Pain Med. 2016;35(3):223–227. doi:10.1016/j.accpm.2016.01.003
41. Pamphlet with instruction was formed by Idmed. Available from: https://www.idmed.fr/en/witof-en/.
42. Liang SS, Stewart PA, Phillips S. An ipsilateral comparison of acceleromyography and electromyography during recovery from nondepolarizing neuromuscular block under general anesthesia in humans [published correction appears in Anesth Analg. 2017 May;124(5):1745]. Anesth Analg. 2013;117(2):373–379. doi:10.1213/ANE.0b013e3182937fc4
43. Bussey L, Jelacic S, Togashi K, Bowdle A. A pilot study of train-of-four and post-tetanic count monitoring with the tetragraph electromyograph compared to the twitchview monitor electromyograph. medRxiv. 2021;2021. doi:10.1101/2021.03.19.21249475
44. Radkowski P. Vergleich der elektromogragraphischen Relaxometrie zwischen Nervus ulnaris und Nervus tibialis posterior während klinisch durchgeführter Narkosen. Dissertation Hannover; 2019.
45. Radkowski P, Grond S, Brunner H, et al. Comparison of relaxometry between ulnar nerve and posterior tibial nerve after cisatracurium administration using electromyography. Anesth Pain Med. 2023;13(1). doi:10.5812/aapm-132866
46. Sugi Y, Nitahara K, Higa K, Kusumoto G, Shono S. Comparison of the neuromuscular profile of the first dorsal interosseous muscle and the flexor hallucis brevis muscle as measured by electromyography. ISRN Anesthesiol. 2011;2011:1–3. doi:10.5402/2011/298983
47. Salminen J, van Gils M, Paloheimo M, Yli-Hankala A. Comparison of train-of-four ratios measured with datex-ohmeda’s M-NMT MechanoSensor™ and M-NMT ElectroSensor™. J Clin Monit Comput. 2016;30(3):295–300. doi:10.1007/s10877-015-9717-4
48. Schmidt J. Evaluierung der Phonomyographie als neues Verfahren zur Uberwachung der neuromuskularen Blockade an verschiedenen Muskelgruppen eines Schweinemodells nach Applikation von Rocuroniumbromid. Deutsche Forschungsgemeinschaft (DGF) – Projektnummer 5388768. Available from: https://gepris.dfg.de/gepris/projekt/5388768?language=en.
49. Michaud G, Trager G, Deschamps S, Hemmerling TM. Dominance of the hand does not change the phonomyographic measurement of neuromuscular block at the adductor pollicis muscle. Anesth Analg. 2005;100(3):718–721. doi:10.1213/01.ANE.0000144067.42615.AD
50. Grimaldi FM. Physico-mathesis de lumine, coloribus, et iride, aliisque adnexis libri duo (Bologne: Ex typographia haeredis Victorii Benatii, impensis Hieronymi Berniae)1665.
51. Bellemare F, Couture J, Donati F, Plaud B. Temporal relation between acoustic and force responses at the adductor pollicis during nondepolarizing neuromuscular block. Anesthesiology. 2000;93(3):646–652. doi:10.1097/00000542-200009000-00012
52. Hemmerling TM, Michaud G, Trager G, Deschamps S. Phonomyographic measurements of neuromuscular blockade are similar to mechanomyography for hand muscles. Can J Anaesth. 2004;51(8):795–800. doi:10.1007/BF03018451
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.