")
Back to Journals » Clinical Epidemiology » Volume 16
Microscopic Colitis and Risk of Incident Psoriasis: A Nationwide Population-Based Matched Cohort Study
Authors Bergman D, Roelstraete B, Sun J , Ebrahimi F, Lidström R, Svedbom A, Ståhle M, Ludvigsson JF
Received 13 December 2023
Accepted for publication 25 March 2024
Published 29 March 2024 Volume 2024:16 Pages 213—225
DOI https://doi.org/10.2147/CLEP.S454677
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Irene Petersen
David Bergman,1 Bjorn Roelstraete,1 Jiangwei Sun,1 Fahim Ebrahimi,1,2 Rickard Lidström,3 Axel Svedbom,4,5 Mona Ståhle,4 Jonas F Ludvigsson1,6,7
1Department of Medical Epidemiology and Biostatistics, Karolinska Institutet, Stockholm, Sweden; 2Department of Gastroenterology and Hepatology, Clarunis University Center for Gastrointestinal and Liver Diseases, Basel, Switzerland; 3Diagnostiskt Centrum Hud, Stockholm, Sweden; 4Division of Dermatology and Venereology, Department of Medicine, Karolinska Institutet, Stockholm, Sweden; 5Dermatology and Venereology Clinic, Karolinska University Hospital, Stockholm, Sweden; 6Department of Pediatrics, Orebro University Hospital, Orebro, Sweden; 7Department of Medicine, Columbia University College of Physicians and Surgeons, New York, NY, USA
Correspondence: David Bergman, Email [email protected]
Background: Microscopic colitis (MC) has been associated with several immune-mediated diseases including psoriasis, but earlier research has been limited to psoriasis occurring before MC. Data from large-scale cohort studies investigating MC and risk of future psoriasis are lacking.
Objective: To examine the association between MC and psoriasis.
Methods: In a nationwide, population-based, matched cohort study in Sweden from 2007 to 2021, we identified 8404 patients with biopsy-verified MC (diagnosed in 2007– 2017), 37,033 matched reference individuals, and 8381 siblings without MC. Information on MC was obtained through the ESPRESSO cohort (a Swedish histopathology database with nationwide coverage). Using Cox regression, we calculated hazard ratios (HRs) and 95% confidence intervals (CIs) for psoriasis up until 2021.
Results: During a median follow-up of 9.2 years (interquartile range = 6.7– 11.7), 179 MC patients and 440 reference individuals were diagnosed with psoriasis (241.1 vs 131.8 events per 100,000 person-years), corresponding to one extra case of psoriasis in 91 patients with MC over 10 years. After adjustment for the matching variables (birth year, sex, county of residence, and calendar period) and level of education, we computed an adjusted hazard ratio (aHR) of 1.82 (95% CI = 1.53– 2.17). Stratified by sex, estimates were similar and when examining the aHR across different lengths of follow-up, we found significantly elevated estimates up to 10 years after MC diagnosis. Compared to MC-free siblings, the aHR was 1.85 (95% CI = 1.36– 2.51).
Conclusion: Patients with MC are at an almost doubled risk of psoriasis compared to the general population. Clinicians need to consider psoriasis in MC patients with skin lesions.
Keywords: microscopic colitis, psoriasis, epidemiology
Introduction
Microscopic colitis (MC) is a recently recognized inflammatory disease of the large intestine.1 Typically, the disease affects patients aged 60 to 70 years and the disease is more common among women.2 MC is characterized by symptoms such as non-bloody, watery diarrhea, abdominal pain, and weight loss.3 Some patients may also report nocturnal diarrhea, urgency, and fecal incontinence.4
The term microscopic colitis is a unifying concept for two main subtypes, primarily collagenous colitis (CC) and lymphocytic colitis (LC), subdivided by their histopathological presentation. The main diagnostic feature of CC is a thickened collagenous layer in the colonic mucosa, whereas LC is characterized by an increased number of intraepithelial lymphocytes.5 Typically, there are no macroscopic aberrations in the colonic mucosa.
In a 2019 cohort study examining the incidence of MC in Sweden, our group computed an overall incidence of MC in Sweden of 10.5 cases per 100000 person-years from 2006 to 2015 with higher rates in women (72% of patients).
Psoriasis is a chronic immune-mediated disorder affecting primarily the skin.6 However, some 10–30%7–9 of patients also develop psoriatic arthritis with a typical onset approximately 10 years after the first signs of cutaneous lesions. Still, around 15% of patients will experience joint symptoms before the onset of skin manifestations.10 Globally, the prevalence of psoriasis is estimated to be around 3% and in Sweden 2–4%).11
There is a known link between psoriasis and other gastrointestinal (GI)-diseases such as celiac disease12 and inflammatory bowel disease (IBD),13 but data on the association between MC and psoriasis are scarce. A 2022 study from the USA14 examining risk factors for MC (n = 1130) estimated a univariately derived odds ratio (OR) of 10.9 for psoriasis. The published paper, however, contains no information on the validity of exposure or outcome information. Neither the analysis adjusted for multiple testing and temporality of exposure in relation to outcome was disregarded. In 2021, Wildt et al conducted a case–control study in Denmark,15 investigating the association between MC and several prior autoimmune conditions. This study found an OR of 1.84 for earlier psoriasis (95% confidence interval (CI)=1.59–2.13). Again, the validity of MC diagnosis had not been assessed, and multiple testing had not been taken into consideration.
As MC and psoriasis are both immune-mediated diseases, with known associations to several autoimmune disorders15,16 and since both conditions have been linked to genes coding for the major histocompatibility complex,17,18 we hypothesized that a correlation between the two disorders exists. Thus, this project aims to elucidate the association between MC and future psoriasis in a large, nationwide matched cohort study. Increased knowledge in this field may help physicians treating MC patients and may also aid in generating new hypotheses regarding shared pathogenic mechanisms.
Methods
Setting
Data for this study were collected from various Swedish healthcare registers as well as from registers on the Swedish population operated and maintained by the government. Healthcare in Sweden is funded by taxes and designed to provide citizens with equal access to medical care. Since all Swedish citizens are given a personal identity number19 researchers are able to link information from multiple sources, thus allowing for an almost complete follow-up. We set the starting point of our study period to January 1st, 2007. This date was chosen for us to be able to assess eligibility criteria using data from the Prescribed Drug Register20 which was introduced in 2005.
Ascertainment of Microscopic Colitis
Patients with MC were identified using relevant Systematized Nomenclature of Medicine21 (SNOMED) codes from the ESPRESSO (Epidemiology Strengthened by histoPathology Reports in Sweden) study.22 The specifics of this method have been previously described.23 Moreover, a previous validation study24 assessed the accuracy of our exposure information and found that 95% of patients with a SNOMED-code indicating MC also had a clinical presentation, according to medical charts, consistent with MC.
General Population Reference Individuals
Using the Total Population Register,25 for each MC patient, we identified up to 5 reference individuals (without previous MC or psoriasis) from the general population. Reference individuals and MC patients were matched according to sex, birth year, county of residence, and index year, all at the time of diagnostic biopsy.
Sibling Comparators
Leveraging the Multigeneration Register, a component of the Total Population Register,25 we were able to identify full siblings (without a prior diagnosis of MC) to our patients with MC. Using siblings as reference individuals allowed us, to some extent, to gauge the influence of shared genetics and early environmental factors.
Ascertainment of Outcomes
We defined our outcome, psoriasis, as having a relevant ICD-code (ICD-10: L40) recorded in the National Patient Register (NPR).26 Briefly, the NPR stores information on diagnoses and medical procedures in non-primary care. The register attained nationwide coverage for inpatient care in 1987 and, since 2001, also contains information from non-primary outpatient care. Generally, the PPV of ICD-codes in the NPR is ~90%.26
Follow-Up
Follow-up commenced on the date of MC diagnosis (for our exposed group) and on the corresponding date for our reference individuals. Study participants were then monitored until December 31st, 2021, or until they were diagnosed with psoriasis, died, or emigrated, whichever occurred first. In the event of a reference individual being diagnosed with MC, these were reclassified as exposed and received their own set of reference individuals. On the date of MC diagnosis, these individuals stopped contributing person-time as reference individuals.
Other Covariates
Background information on vital status, sex, birth year, emigration, county of residence, and country of birth was obtained from the Total Population Register.25 Data on level of education, defined as compulsory school (≤9 years), upper secondary school (10–12 years), or college (≥13 years), was gathered from the longitudinal integrated database for health insurance and labor market studies (LISA).27 Level of education was used as a proxy for socioeconomic status. If information on level of education was missing, we used the highest level of education of the parents. If information regarding the parents was missing as well, study participants were placed in a missing category. Since MC and psoriasis both have been associated with celiac disease12,15 (CD) and IBD,13,28 we retrieved information on all patients with a diagnosis of CD and/or IBD from the ESPRESSO-study.22 For a sensitivity analysis (see below), we also gathered data on diagnoses of chronic obstructive pulmonary disease (COPD) from the NPR.
Using the Prescribed Drug Register,20 we retrieved information on dispensed treatments for psoriasis (ATC-code: D05). This was, mainly, done to identify and exclude patients with a prior diagnosis of psoriasis registered in primary care. Moreover, as there is no validated instrument to classify disease intensity in MC, we gathered data on dispensed budesonide (ATC-code: A07EA06) as a proxy for severity of disease.
Exclusion Criteria
Figure 1 outlines the study flowchart. All exclusion criteria were applied uniformly for all individuals enrolled in the study. Briefly, we excluded study participants with data irregularities pertaining to date of emigration or date of death (Figure 1). Also, those with a prior colectomy, on or before enrollment, were excluded. Moreover, all individuals with a diagnosis (prior to index date) indicating psoriasis or psoriatic arthritis or with a recorded dispensation of drugs typically used for the treatment of psoriasis were omitted.
 |
Figure 1 Flowchart outlining exclusions for patients with MC, reference individuals and siblings. |
Sensitivity Analyses
To test the robustness of our observed association, we conducted several sensitivity analyses. First, we broadened the definition of our outcome measure to also include psoriatic arthritis (ICD-10: M070-3). This was also done to capture study participants where treatment for psoriatic arthritis may have prevented skin lesions to develop. Second, to also include patients that may have been diagnosed in primary care (and therefore not registered in the NPR), we defined psoriasis as either (or both) a relevant ICD-code or dispensed treatment for psoriasis. Third, as MC has been linked to both celiac disease29 and IBD28 and due to the known association between psoriasis and IBD13 and celiac disease,12 we carried out an analysis additionally adjusting for celiac disease and IBD. Fourth, as smoking is considered a risk factor for both MC30 and psoriasis,31 as a proxy for smoking, we added adjustment for COPD if diagnosed >40 years of age and prior to index date.
Fifth, in an effort to address surveillance bias, we excluded all individuals with a follow-up less than one year. Sixth, to investigate whether dispensed budesonide (as a proxy for severity of disease) had an impact on the risk for psoriasis, we computed adjusted hazard ratios (aHRs) for patients with MC with a record of dispensed budesonide and for patients with MC without such a dispensation.
Finally, to control for intrafamilial confounding and/or familial aggregation, we used MC-free siblings as comparators.
Patient and Public Involvement
No patient participated in the planning or design of this study.
Data Transparency Statement
In accordance with Swedish regulations, the data from this study are not publicly available. The data accessed complied with relevant data protection and privacy regulations.
Statistical Analysis
Using a matched cohort study-design, we compared the incidence rate (IR) of psoriasis in patients with MC to that of the general population comparators. Cumulative incidence, unadjusted for competing risks, for both groups was computed using a Kaplan–Meier estimator. By plotting the incidence curves we could determine absolute rate differences at 0, 5 and 10 years of follow-up. Moreover, aHRs were calculated using Cox proportional hazards modelling, and the proportional hazards assumption was examined by a Schoenfeld residuals test. To control for potential confounding by the matching variables32 (sex, birth year, county of residence, and year of biopsy), these variables, along with level of education, were added as covariates to our main model.
Using the above described model, we also computed aHRs for strata defined by sex, age (<50 or ≥50 years), calendar period at start of follow-up (2007–2010, 2011–2017), calendar period with a maximum of 3 years of follow-up (2007–2010, 2011–2017), years of follow-up (<1, 1-<5, 5-<10, ≥10 years), education level (≤9, 10–12, ≥13 years or missing) and country of birth (Nordic or other).
In a separate analysis, we used siblings (without MC) as reference population. In this analysis, MC patients were only compared to their own siblings.
A p-value of <0.05 was deemed statistically significant. All statistical analyses were conducted using Stata/IC 17.1 for Mac (StataCorp, 4905 Lakeway Dr, College Station, TX 77845). To estimate the influence of unmeasured confounding we used the E-value package by Linden et al.33
Ethics
This study was approved by the Stockholm Ethics Review Board. Because the study was strictly register-based, informed consent was not required.34 The study is in compliance with the Declaration of Helsinki.
Results
From 2007 to 2017 we identified 8404 patients with a first-time diagnosis of MC. These patients were matched to 37,033 reference individuals from the general population (Table 1). In addition, 8381 siblings without MC were identified. Some 70% of patients with MC were women, and median age at diagnosis was 62.8 years (interquartile range (IQR)=49.1–72.3). Educational attainment was evenly distributed between patients with MC and reference individuals. Approximately one-third of individuals had 13 years of schooling or more, corresponding to university or college. Nordic origin was somewhat more common in patients with MC (93.6%) compared to reference individuals (87.6%). Prior psoriasis and psoriatic arthritis were more common reasons for exclusion in the exposed population when comparing to reference individuals and siblings (Figure 1).
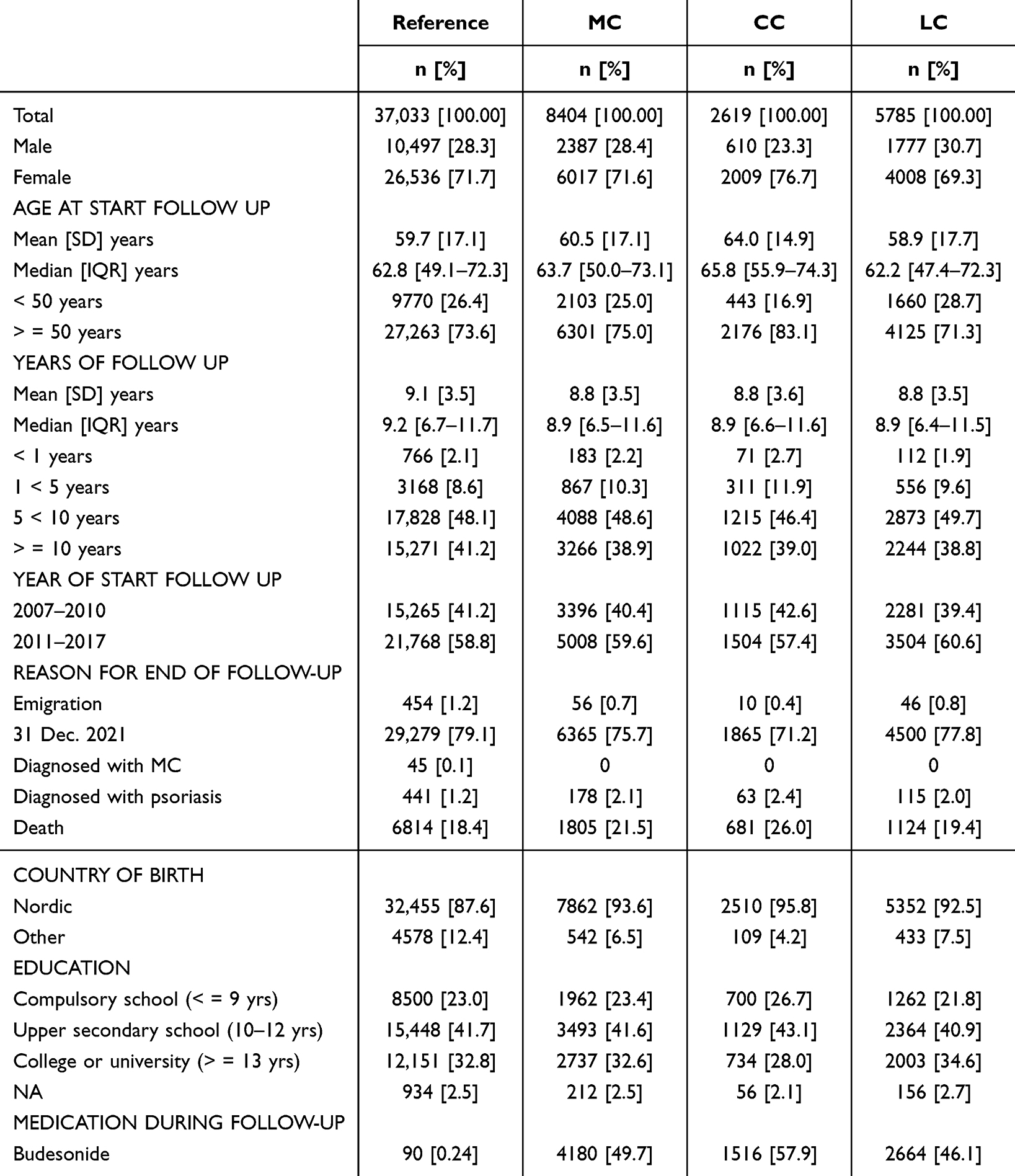 |
Table 1 Summary Statistics for MC Patients and Matched Reference Individuals |
MC and Later Psoriasis
During our study period 2.1% (n = 179) of patients with MC were diagnosed with psoriasis. Corresponding figures for reference individuals and siblings were 1.1% (n = 440) and 1.4% (n = 115), respectively. These proportions corresponded to the following IRs: patients with MC: 241.1 (95% CI = 208.3–279.2) per 100,000 person-years, reference individuals: 131.8 (95% CI = 120.1–144.7) (Table 2) and siblings: 145.0 (95% CI = 120.8–174.1). The rate difference between patients with MC and reference individuals is equivalent to one additional case of psoriasis in 91 patients with MC followed for 10 years. Figure 2 depicts the Kaplan-Meier curves for patients with MC and that of their matched reference individuals.
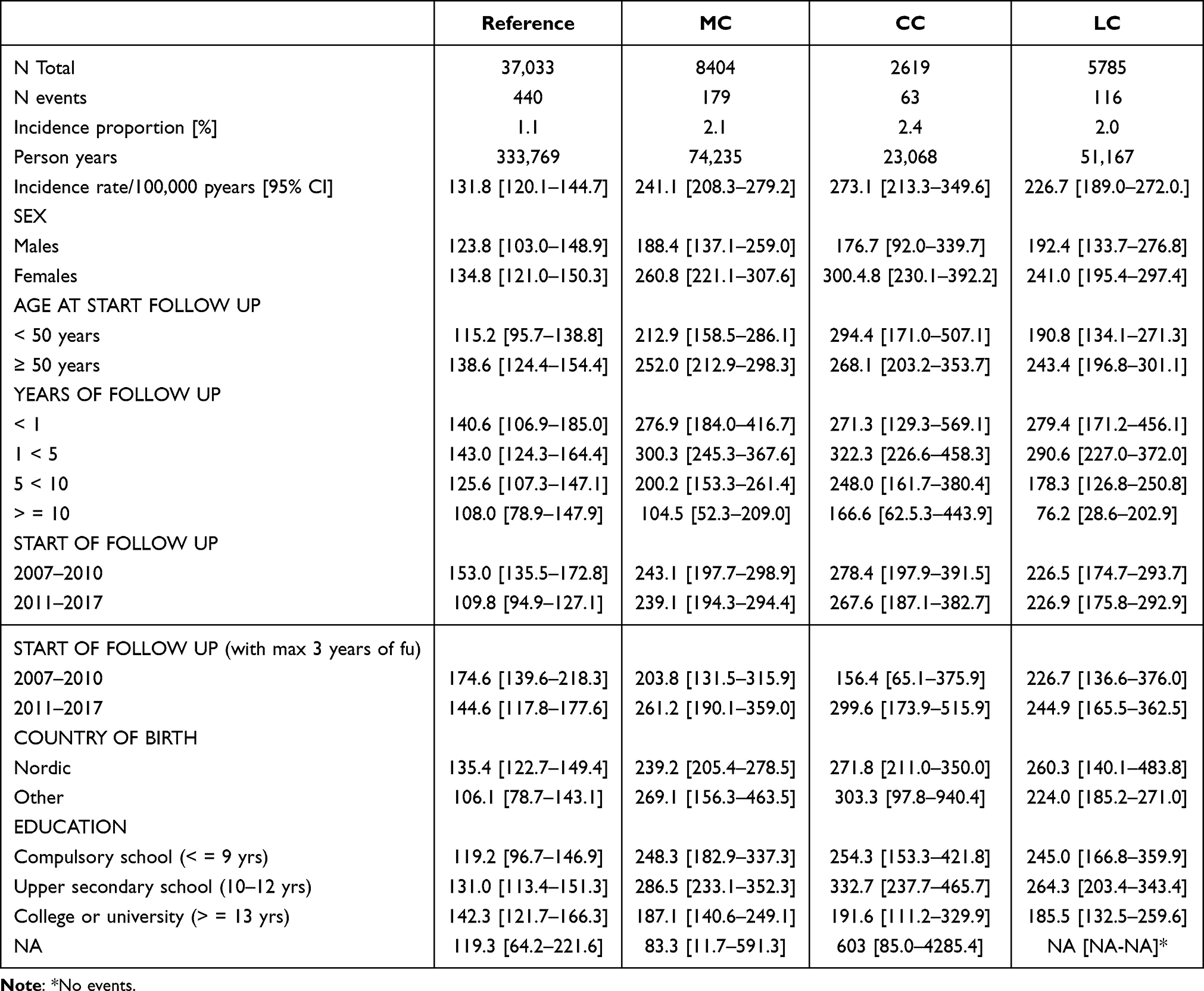 |
Table 2 Incidence Rates (Psoriasis) for MC Patients and Reference Individuals in Sweden 2007–2021 |
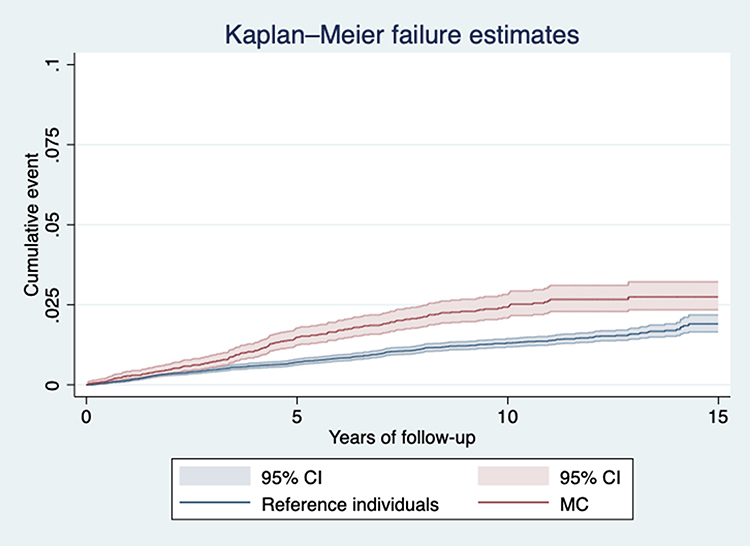 |
Figure 2 Absolute incidence rates (psoriasis) for patients with MC and reference individuals according to years of follow-up. |
After adjustments, we computed an aHR of 1.82 (95% CI = 1.53–2.17) (Table 3) for psoriasis in patients with MC. Estimates for women and men were 1.93 (95% CI = 1.59–2.35) and 1.51 (95% CI = 1.04–2.18), respectively. Stratifying on age (<50 vs ≥50 years of age), the aHRs were almost identical (Table 3) and, thus, naturally resembled our main result. When examining the association across various lengths of follow-up, we found the increased risk to be most pronounced between 1-<5 years of follow-up, aHR 2.10 (95% CI = 1.64–2.68) and only for individuals, with a follow-up exceeding 10 years did our estimate fail to reach statistical significance (Table 3).
 |
Table 3 Psoriasis Hazard Ratios for MC Patients Diagnosed in Sweden 2007–2017 Compared to Matched Reference Individuals. Adjusted for Age, Sex, County, Calendar Period and Level of Education |
Moreover, we examined the association according to start of follow-up (2007–2010 vs 2011–2017) and found the aHR for the most recent period to be somewhat higher, aHR 2.16 (95% CI = 1.68–2.79). The aHR for the earlier period was 1.58 (95% CI = 1.24–2.00). When restricting length of follow-up for each calendar period to three years, the same pattern emerged with a slightly higher aHR for the more recent interval (Table 3).
To assess the impact of socioeconomic status, we also stratified by level of education finding higher aHRs for individuals, with an educational level corresponding to compulsory (aHR 2.10 (95% CI = 1.45–3.05)) or upper secondary school (aHR 2.19 (95% CI = 1.70–2.81)). For patients with MC who had an educational attainment equivalent to college or university, the aHR fell short of statistical significance 1.31 (95% CI = 0.95–1.82) (Table 3). Examining the association, stratified by subtype, we found the aHR for CC to be 2.17 (95% CI = 1.61–2.93) and for LC 1.68 (95% CI = 1.36–2.08) (Table 3). To address possible residual confounding, we computed an E-value. We found that the strength of an unmeasured confounder would have to be 3.0-fold to both our main exposure and outcome to reduce our observed aHR to 1. To shift the lower limit of the CI below 1, the strength of the unmeasured confounder would have to be 2.4-fold.
Sensitivity Analyses
To assess the robustness of our results, several sensitivity analyses were conducted. Briefly, these additional analyses corroborated our result. Results and definitions are summarized in Table 4.
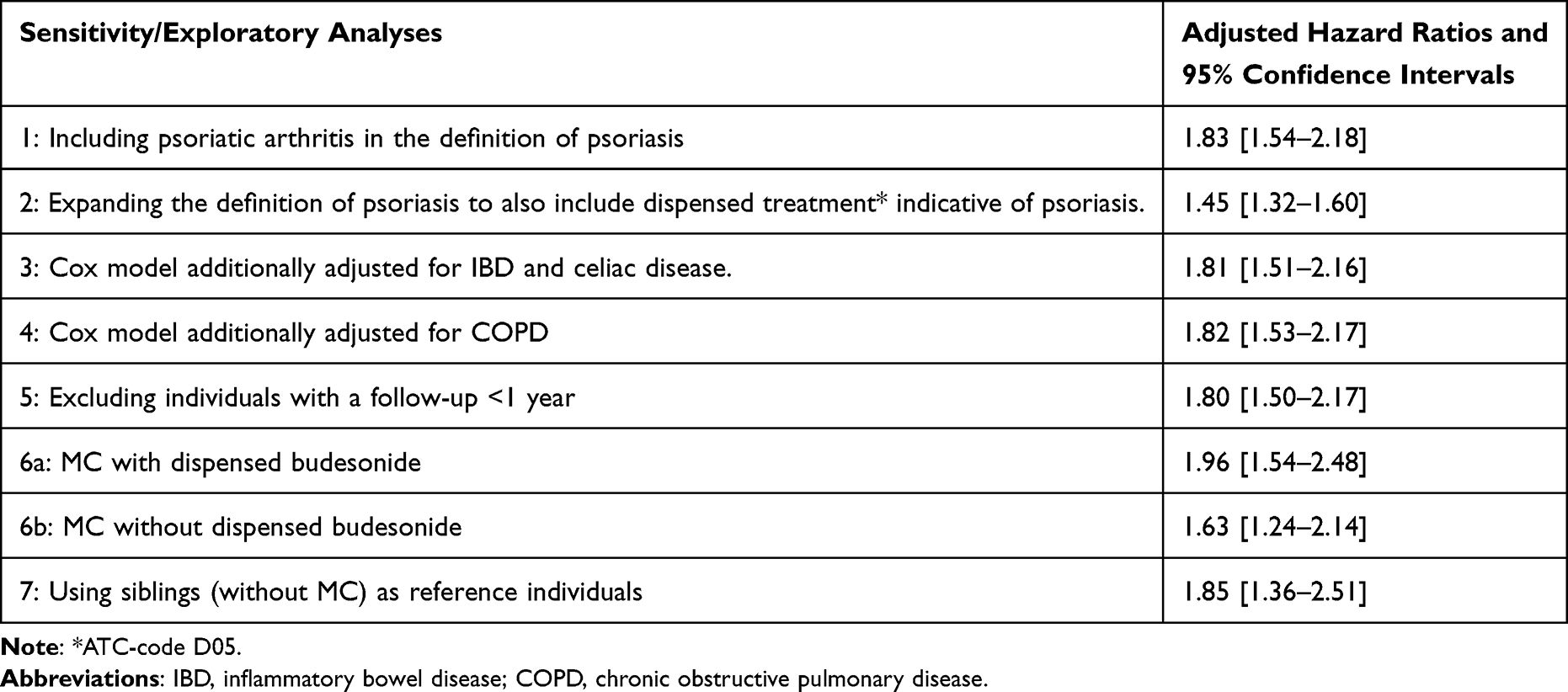 |
Table 4 Sensitivity and Exploratory Analyses. Adjusted Hazard Ratios for Psoriasis in Patients with MC in Sweden from 2007 to 2017 Compared to Reference Individuals |
Discussion
By contrasting some 8400 patients with MC to more than 37,000 reference individuals in a population-based, nationwide matched cohort study, we estimated an 83% increase in the risk for psoriasis among patients with MC. The association between our exposure (MC) and our outcome (psoriasis) was robust also when using siblings as reference individuals as well as across several sensitivity analyses.
Comparison with the Literature
Previously, and to the best of our knowledge, the association between MC and psoriasis has only been investigated in two studies focusing on psoriasis (among other conditions) as a risk factor for MC.14,15 Both these studies reported significantly elevated, but disparate, ORs. In addition, none of these studies reported stratified analyses or sensitivity analyses. However, the reported ORs are in line with the higher proportion of exclusions due to previous psoriasis in our MC population compared to the reference population. Nevertheless, the reciprocal association, MC, and later psoriasis have not been investigated so far. However, both IBD and celiac disease have been associated with both psoriasis12,13 and MC,28,29 strengthening our hypothesis that an association could exist between MC and psoriasis.
Our findings were robust across several sensitivity analyses. As some patients may be diagnosed with psoriatic arthritis before skin lesions develop, we examined whether including psoriatic arthritis in the outcome definition influenced our estimate. This analysis, however, yielded an almost identical result as our main analysis. Moreover, as stated above, IBD13,28 and celiac disease12,29 become potential confounders. Therefore, in a separate analysis, IBD and celiac disease (diagnosed prior to index date) were added as covariates. Again, our estimate was almost unchanged. In an effort to address the impact of smoking,31,35 we also carried out an analysis additionally adjusting for COPD. Again, this added adjustment did not result in a meaningful impact on the estimate. Moreover, we found no effect (PHeterogeneity=0.33) of disease intensity and/or dispensed budesonide on the association between MC and psoriasis. Whether this absence of effect modification is explained by disease intensity (defined as having a record of dispensed budesonide) not having an important role in the causal structure or whether the ingested budesonide hampers inflammation in the skin is unclear. We also conducted a sensitivity analysis with a wider definition of psoriasis, including dispensed treatment indicative of psoriasis. This was done to capture patients diagnosed and treated in primary care. Using this expanded definition of psoriasis, returned a somewhat lower estimate, aHR 1.45 (95% CI = 1.32–1.60). Whether this trend towards attenuation is a consequence of patients with MC more often being referred to specialist care due to severity of disease, gastroenterologists traditionally referring to a dermatologist rather than primary care for psoriasis, or due to non-differential misclassification of outcome (medications indicative of psoriasis are used to treat non-psoriatic disease) remains an unanswered question. Finally, to control for intrafamilial confounding (early environmental factors and shared genetics), we carried out an analysis where, instead of reference individuals from the general population, siblings were used as comparators. The aHR, however, remained essentially unchanged, further strengthening the notion that MC plays an integral part in the observed association.
Biologic Mechanisms
Our findings have biologic plausibility. First, both CC and psoriasis have been linked to the same alleles coding for genes in the MHC, namely the HLA-B*08:01-allele. This may explain the somewhat higher aHR seen in CC. Second, both MC and psoriasis share inflammatory features, as both diseases are characterized by cytokines involved in the TH1-/TH17-pathways. Previous studies have found elevated levels of IFN-γ, IL-17, IL-22, and TNF.36–38 Also, MC has been linked to increased levels of IL-23, a recently adopted therapeutic target for psoriasis.39 Third, both diseases are characterized by an increased dysbiosis40,41 and decreased ɑ-diversity42,43 in the gut microbiota. More specifically, decreased abundances in Akkermansia42,44 and Alistipes40,43 have been reported for both MC and psoriasis.
Strengths and Weaknesses
Our study has numerous strengths. First, the size of our cohort allowed for precise calculations of HRs across various strata, strengthening the clinical and scientific applications of our study. Second, as all patients with MC in Sweden were eligible for inclusion, the impact of selection bias was kept to a minimum. Third, the high validity24 of our exposure information makes misclassification of MC unlikely. The validity of ICD-codes indicating psoriasis has also been previously assessed.45 A fourth strength is the opportunities related to the Swedish personal identity number that allowed us to link data from various healthcare- and government-maintained registers. We also acknowledge several limitations. Our study was registry-based; hence, we did not have information on potential confounders such as body mass index (BMI) and smoking. However, psoriasis has been linked to a higher BMI,45 whereas MC is associated with a lean BMI.46 Hence, access to data on BMI would likely increase our point estimates. Moreover, our additional adjustment for COPD was aimed at, to some extent, controlling for the impact of smoking. This additional adjustment left our aHR virtually unchanged. Nevertheless, only a small proportion of smokers develop COPD. Therefore, we urge caution when interpreting this specific result. However, our calculated E-value suggests our finding, to a certain extent, is unlikely to reflect residual confounding. Naturally, surveillance bias may have influenced our result as patients with MC, generally, are followed by a gastroenterologist which may expediate and/or facilitate a referral to a dermatologist. Lastly, the external validity may be decreased due to our results are based, solely, on Swedish citizens of primarily white ethnicity.
To conclude, findings from this nationwide study indicate that patients with MC are at an almost two-fold increased risk of psoriasis compared to the general population. Our observed association was robust across several sensitivity analyses, strengthening the clinical and scientific implications of our study. Our results add to the knowledge of extraintestinal inflammatory conditions in MC and underscore the importance to study the mechanisms involved. Moreover, our findings indicate that clinicians should consider psoriasis in patients reporting skin lesions.
Abbreviations
aHRs, adjusted hazard ratios; ATC, anatomical therapeutic chemical; BMI, body mass index; COPD, chronic obstructive pulmonary disease; CC, collagenous colitis; CI, confidence interval; ESPRESSO, Epidemiology Strengthened by histoPathology Reports in Sweden; GI, Gastrointestinal; IBD, Inflammatory bowel disease; ICD, International Classification of Diseases and Related Health Problems; IQR, interquartile range; IR, incidence rate; LC, lymphocytic colitis; MC, microscopic colitis; NPR, National Patient Register; OR, odds ratio; PPV, positive predictive value; SNOMED, Systematized Nomenclature of Medicine.
Details of Ethics Approval
This study was approved by the Regional Ethics Committee, Stockholm, Sweden (Protocol no 2014/1287-31/4, 2018/972-32 and 2022-05774-02).
Data Transparency Statement
In accordance with Swedish regulations, the data from this study are not publicly available.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Karolinska Institutet (Ludvigsson), Stockholm County Council (Ludvigsson), the NIH (National Institutes of Health NIA R01 (AG068390; Ludvigsson)). None of the funding organizations has had any role in the design and conduct of the study, in the collection, management, and analysis of the data, or in the preparation, review, and approval of the manuscript.
Disclosure
Dr. Ludvigsson has coordinated a study on behalf of the Swedish IBD quality register (SWIBREG). That study received funding from the Janssen corporation. Dr Ludvigsson has also received financial support from MSD to develop a paper reviewing national healthcare registers in China. Dr. Ebrahimi has served as an advisory board member for Boehringer Ingelheim. Dr Svedbom has received consultancy fees from ICON plc, AbbVie, BMS, Novartis, and Eli Lilly. Dr Svedbom has received lecture fees from Janssen Cilag and UCB. Dr Ståhle has received lecture fees and consulted for Leo Pharma, AbbVie, Eli-Lilly, Lipidor, UCB Pharma, Bristol-Myers Squibb and Janssen. Dr Ståhle serves as scientific chairman in Swedish Dermatology Foundation (Hudfonden) receiving honoraria. The authors report no other conflicts of interest in this work.
References
1. Burke KE, D’Amato M, Ng SC, Pardi DS, Ludvigsson JF, Khalili H. Microscopic colitis. Nat Rev Dis Primers. 2021;7(1):39.
2. Bergman D, Clements MS, Khalili H, Agreus L, Hultcrantz R, Ludvigsson JF. A nationwide cohort study of the incidence of microscopic colitis in Sweden. Aliment Pharmacol Ther. 2019;49(11):1395–1400. doi:10.1111/apt.15246
3. Mellander MR, Ekbom A, Hultcrantz R, Lofberg R, Ost A, Bjork J. Microscopic colitis: a descriptive clinical cohort study of 795 patients with collagenous and lymphocytic colitis. Scand J Gastroenterol. 2016;51(5):556–562. doi:10.3109/00365521.2015.1124283
4. Miehlke S, Verhaegh B, Tontini GE, Madisch A, Langner C, Munch A. Microscopic colitis: pathophysiology and clinical management. Lancet Gastroenterol Hepatol. 2019;4(4):305–314. doi:10.1016/S2468-1253(19)30048-2
5. Langner C, Aust D, Ensari A, et al. Histology of microscopic colitis-review with a practical approach for pathologists. Histopathology. 2015;66(5):613–626. doi:10.1111/his.12592
6. Lebwohl M. Psoriasis. Lancet. 2003;361(9364):1197–1204. doi:10.1016/S0140-6736(03)12954-6
7. Gelfand JM, Gladman DD, Mease PJ, et al. Epidemiology of psoriatic arthritis in the population of the United States. J Am Acad Dermatol. 2005;53(4):573. doi:10.1016/j.jaad.2005.03.046
8. Reich K, Kruger K, Mossner R, Augustin M. Epidemiology and clinical pattern of psoriatic arthritis in Germany: a prospective interdisciplinary epidemiological study of 1511 patients with plaque-type psoriasis. Br J Dermatol. 2009;160(5):1040–1047. doi:10.1111/j.1365-2133.2008.09023.x
9. Mease PJ, Gladman DD, Papp KA, et al. Prevalence of rheumatologist-diagnosed psoriatic arthritis in patients with psoriasis in European/North American dermatology clinics. J Am Acad Dermatol. 2013;69(5):729–735. doi:10.1016/j.jaad.2013.07.023
10. Gladman DD, Antoni C, Mease P, Clegg DO, Nash P. Psoriatic arthritis: epidemiology, clinical features, course, and outcome. Ann Rheum Dis. 2005;64 Suppl 2(Suppl 2):ii14–7.
11. Parisi R, Symmons DP, Griffiths CE, et al.; Identification, Management of P. Global epidemiology of psoriasis: a systematic review of incidence and prevalence. J Invest Dermatol. 2013;133(2):377–385. doi:10.1038/jid.2012.339
12. Ludvigsson JF, Lindelof B, Zingone F, Ciacci C. Psoriasis in a nationwide cohort study of patients with celiac disease. J Invest Dermatol. 2011;131(10):2010–2016. doi:10.1038/jid.2011.162
13. Fu Y, Lee CH, Chi CC. Association of psoriasis with inflammatory bowel disease: a systematic review and meta-analysis. JAMA Dermatol. 2018;154(12):1417–1423. doi:10.1001/jamadermatol.2018.3631
14. Mohammed A, Ghoneim S, Paranji N, Waghray N. Quantifying risk factors for microscopic colitis: a nationwide, retrospective cohort study. Indian J Gastroenterol. 2022;41(2):181–189. doi:10.1007/s12664-021-01199-z
15. Wildt S, Munck LK, Winther-Jensen M, Jess T, Nyboe Andersen N. Autoimmune diseases in microscopic colitis: a Danish nationwide case-control study. Aliment Pharmacol Ther. 2021;54(11–12):1454–1462. doi:10.1111/apt.16614
16. Vashist S, Mahajan VK, Mehta KS, et al. Association of psoriasis with autoimmune disorders: results of a Pilot Study. Indian Dermatol Online J. 2020;11(5):753–759. doi:10.4103/idoj.IDOJ_648_19
17. Westerlind H, Mellander MR, Bresso F, et al. Dense genotyping of immune-related loci identifies HLA variants associated with increased risk of collagenous colitis. Gut. 2017;66(3):421–428. doi:10.1136/gutjnl-2015-309934
18. Winchester R, Minevich G, Steshenko V, et al. HLA associations reveal genetic heterogeneity in psoriatic arthritis and in the psoriasis phenotype. Arthritis Rheum. 2012;64(4):1134–1144. doi:10.1002/art.33415
19. Ludvigsson JF, Otterblad-Olausson P, Pettersson BU, Ekbom A. The Swedish personal identity number: possibilities and pitfalls in healthcare and medical research. Eur j Epidemiol. 2009;24(11):659–667. doi:10.1007/s10654-009-9350-y
20. Wettermark B, Hammar N, Fored CM, et al. The new Swedish prescribed drug register--opportunities for pharmacoepidemiological research and experience from the first six months. Pharmacoepidemiol Drug Saf. 2007;16(7):726–735. doi:10.1002/pds.1294
21. Evelyn Hovenga TB. Systematized Nomenclature of Medicine. Fragmented global standards development organisations; 2022.
22. Ludvigsson JF, Lashkariani M. Cohort profile: ESPRESSO (Epidemiology Strengthened by histoPathology Reports in Sweden). Clin Epidemiol. 2019;11:101–114. doi:10.2147/CLEP.S191914
23. Bergman D, Khalili H, Roelstraete B, Ludvigsson JF. Microscopic colitis and risk of cancer - a population-based cohort study. J Crohns Colitis. 2020. doi:10.1093/ecco-jcc/jjaa156
24. Svensson M, Bergman D, Olen O, et al. Validating microscopic colitis (MC) in Swedish pathology registers. Scand J Gastroenterol. 2019;2019:1–7.
25. Ludvigsson JF, Almqvist C, Bonamy A-KE, et al. Registers of the Swedish total population and their use in medical research. Eur j Epidemiol. 2016;31(2):125–136. doi:10.1007/s10654-016-0117-y
26. Ludvigsson JF, Andersson E, Ekbom A, et al. External review and validation of the Swedish national inpatient register. BMC Public Health. 2011;11:450. doi:10.1186/1471-2458-11-450
27. Ludvigsson JF, Svedberg P, Olen O, Bruze G, Neovius M. The longitudinal integrated database for health insurance and labour market studies (LISA) and its use in medical research. Eur J Epidemiol. 2019;34(4):423–437. doi:10.1007/s10654-019-00511-8
28. Khalili H, Burke KE, Roelstraete B, Sachs MC, Olen O, Ludvigsson JF. Microscopic colitis and risk of inflammatory bowel disease in a Nationwide Cohort Study. Gastroenterology. 2020;158(6):1574–83 e2. doi:10.1053/j.gastro.2019.12.028
29. Bergman D, Khalili H, Lebwohl B, Roelstraete B, Green PHR, Ludvigsson JF. Celiac disease and risk of microscopic colitis: a nationwide population-based matched cohort study. United Eur Gastroenterol J. 2023;11(2):189–201. doi:10.1002/ueg2.12374
30. Yen EF, Pokhrel B, Du H, et al. Current and past cigarette smoking significantly increase risk for microscopic colitis. Inflamm Bowel Dis. 2012;18(10):1835–1841. doi:10.1002/ibd.22838
31. Naldi L. Psoriasis and smoking: links and risks. Psoriasis. 2016;6:65–71. doi:10.2147/PTT.S85189
32. Sjolander A, Greenland S. Ignoring the matching variables in cohort studies - when is it valid and why? Stat Med. 2013;32(27):4696–4708. doi:10.1002/sim.5879
33. Linden A. Conducting sensitivity analysis for unmeasured confounding in observational studies using E-values: the evalue package. Stata J. 2020;20(1):162–175. doi:10.1177/1536867X20909696
34. Ludvigsson JF, Haberg SE, Knudsen GP, et al. Ethical aspects of registry-based research in the Nordic countries. Clin Epidemiol. 2015;7:491–508. doi:10.2147/CLEP.S90589
35. Jaruvongvanich V, Poonsombudlert K, Ungprasert P. Smoking and risk of microscopic colitis: a systematic review and meta-analysis. Inflamm Bowel Dis. 2019;25(4):672–678. doi:10.1093/ibd/izy296
36. Kumawat AK, Strid H, Tysk C, Bohr J, Hörnquist EH. Microscopic colitis patients demonstrate a mixed Th17/Tc17 and Th1/Tc1 mucosal cytokine profile. Mol Immunol. 2013;55(3–4):355–364. doi:10.1016/j.molimm.2013.03.007
37. Coimbra S, Oliveira H, Reis F, et al. Interleukin (IL)-22, IL-17, IL-23, IL-8, vascular endothelial growth factor and tumour necrosis factor-alpha levels in patients with psoriasis before, during and after psoralen-ultraviolet A and narrowband ultraviolet B therapy. Br J Dermatol. 2010;163(6):1282–1290. doi:10.1111/j.1365-2133.2010.09992.x
38. Arican O, Aral M, Sasmaz S, Ciragil P. Serum levels of TNF-alpha, IFN-gamma, IL-6, IL-8, IL-12, IL-17, and IL-18 in patients with active psoriasis and correlation with disease severity. Mediators Inflamm. 2005;2005(5):273–279. doi:10.1155/MI.2005.273
39. Hawkes JE, Yan BY, Chan TC, Krueger JG. Discovery of the IL-23/IL-17 Signaling Pathway and the Treatment of Psoriasis. J Immunol. 2018;201(6):1605–1613. doi:10.4049/jimmunol.1800013
40. Morgan DM, Cao Y, Miller K, et al. Microscopic colitis is characterized by intestinal dysbiosis. Clin Gastroenterol Hepatol. 2020;18(4):984–986. doi:10.1016/j.cgh.2019.06.035
41. Zhang X, Shi L, Sun T, Guo K, Geng S. Dysbiosis of gut microbiota and its correlation with dysregulation of cytokines in psoriasis patients. BMC Microbiol. 2021;21(1):78. doi:10.1186/s12866-021-02125-1
42. Rindom Krogsgaard L, Kristian Munck L, Bytzer P, Wildt S. An altered composition of the microbiome in microscopic colitis is driven towards the composition in healthy controls by treatment with budesonide. Scand J Gastroenterol. 2019;54(4):446–452. doi:10.1080/00365521.2019.1599064
43. Hidalgo-Cantabrana C, Gomez J, Delgado S, et al. Gut microbiota dysbiosis in a cohort of patients with psoriasis. Br J Dermatol. 2019;181(6):1287–1295. doi:10.1111/bjd.17931
44. Buhas MC, Gavrilas LI, Candrea R, et al. Gut Microbiota in Psoriasis. Nutrients. 2022;14(14):2970. doi:10.3390/nu14142970
45. Lofvendahl S, Theander E, Svensson A, Carlsson KS, Englund M, Petersson IF. Validity of diagnostic codes and prevalence of physician-diagnosed psoriasis and psoriatic arthritis in southern Sweden--a population-based register study. PLoS One. 2014;9(5):e98024. doi:10.1371/journal.pone.0098024
46. Liu PH, Burke KE, Ananthakrishnan AN, et al. Obesity and weight gain since early adulthood are associated with a lower risk of microscopic colitis. Clin Gastroenterol Hepatol. 2019;17(12):2523–32.e1. doi:10.1016/j.cgh.2018.11.057
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.