")
Back to Journals » Clinical Ophthalmology » Volume 8
Nasolacrimal duct obstruction following radioactive iodine 131 therapy in differentiated thyroid cancers: review of 19 cases
Authors Al-Qahtani KH, Al Asiri M, Tunio M , Aljohani NJ, Bayoumi Y, Munir I, AlAyoubi A
Received 24 July 2014
Accepted for publication 23 August 2014
Published 5 December 2014 Volume 2014:8 Pages 2479—2484
DOI https://doi.org/10.2147/OPTH.S71708
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Khalid Hussain Al-Qahtani,1 Mushabbab Al Asiri,2 Mutahir A Tunio,2 Naji J Aljohani,3 Yasser Bayoumi,4 Iqbal Munir,5 Ayman AlAyoubi6
1Department of Otolaryngology – Head and Neck Surgery, College of Medicine, Advanced Head and Neck Oncology, King Saud University, 2Radiation Oncology, Comprehensive Cancer Center, King Fahad Medical City, 3Endocrinology and Thyroid Oncology, King Fahad Medical City, Riyadh, Saudi Arabia; 4Radiation Oncology, NCI, Cairo University, Cairo, Egypt; 5Nuclear Medicine Sulaiman Al-Habib Hospital, 6Clinical Ophthalmology, King Fahad Medical City, Riyadh, Saudi Arabia
Background: Radioactive iodine 131 (131I) therapy has long been used in the treatment of differentiated thyroid cancers (DTC). While salivary and lacrimal glandular complications secondary to 131I therapy are well documented, there is little in the literature addressing nasolacrimal duct obstruction (NLDO). We aimed to evaluate the frequency of 131I therapy-acquired NLDO, its correlation to 131I therapy doses, and the surgical treatment outcome of this rare side effect.
Methods: From 2000–2012, a retrospective review of 864 among 1,192 patients with confirmed DTC who were treated with 131I therapy was performed to examine the frequency of NLDO, its causative factors, as well as imaging, surgical intervention, and outcomes.
Results: Nineteen (2.2%) patients were identified with NLDO. The mean age was 51.9±10.5 years (range: 39–72 years). Fifteen (78.9%) were female and four were male (21.1%). The mean individual 131I doses were 311.1±169.3 millicurie (mCi) (range: 150–600 mCi). The mean duration between the date of 131I therapy and the occurrence of NLDO was 11.6±4.1 months (range: 6.5–20). Fourteen (73.7%) patients had bilateral epiphora. Computed tomography dacryography allowed for the detection of all NLDO. Eighteen (94.7%) patients underwent dacryocystorhinostomy. Complete recovery was obtained in 14 (73.7%) patients. Age >45 years and 131I therapy doses >150 mCi were significantly correlated with NLDO (P=0.02 and P=0.03, respectively).
Conclusion: NLDO is an underestimated complication of 131I therapy in DTC patients. Clinicians should be aware of this rare complication for prompt intervention.
Keywords: nasolacrimal duct obstruction, radioactive iodine 131 therapy, differentiated thyroid cancers
Introduction
The use of post-thyroidectomy adjuvant radioactive iodine 131 (131I) therapy is associated with dramatic decreases in locoregional recurrences, distant metastasis, and disease-related mortality in patients with differentiated thyroid carcinomas (DTC).1 Although generally well tolerated, 131I therapy is associated with substantial, albeit rare, side effects. While gastrointestinal problems, salivary and lacrimal gland complications, gonadal dysfunction, and second malignancies are well documented side effects of 131I therapy, there is scant literature addressing nasolacrimal duct obstruction (NLDO).2,3 Different studies have mentioned that the incidence of NLDO was around 3% among DTC patients treated with 131I therapy. The common presentation is an excessive overflow of tears (epiphora). Other signs and symptoms are the medial canthus mass, recurrent conjunctivitis, or infection (dacryocystitis).4
In the Kingdom of Saudi Arabia, DTC has become the second most common malignancy, behind only breast cancer, accounting for more than 10% of all cancers among women.5 The majority of these patients require adjuvant 131I therapy at some point; only a small proportion of these patients can be at risk of 131I therapy-acquired NLDO, which was the aim of our study. We also aimed to determine the correlation between NLDO and 131I therapy along with other clinical and treatment parameters in DTC patients receiving 131I therapy in our population.
Methods
After formal approval from the institutional ethics committee, the medical records of 864 patients, among a total of 1,192 patients, with confirmed DTC who were treated with 131I therapy in two major tertiary care hospitals during the period from July 2000–December 2012 were reviewed using a computer-based institutional database system. Patients with NLDO were retrieved in the following manner:
- Demographic information (age at diagnosis and sex), as well as data regarding symptomatology, clinical procedures (anterior rhinoscopy and Jones fluorescein dye test), and 131I therapy doses in millicurie (mCi) were collected.
- Information on the different diagnostic imaging modalities used, including dacryoscintigraphy, computed tomography (CT) dacryography of the neck, and fluorodeoxyglucose positron emission tomography, was collected.
- Data regarding the surgical intervention used, including balloon dilation, stenting, dacryocystorhinostomy (DCR), type of DCR (external or endoscopic endonasal), symptoms relief, and duration of relief were also recorded.
- Any discrepancies in data acquisition were resolved by directly questioning the patients and treating physicians (ear, nose, and throat, oncology, ophthalmology, and nuclear medicine).
- However, no attempt to systematize other associated sinonasal problems (potential confounders) of the patients was performed.
Statistical analysis
The primary endpoint was the frequency of NLDO. All descriptive data were reported as the mean ± standard deviation, and percentages. The secondary endpoint was the correlation of NLDO with 131I therapy (as tested by Pearson’s correlation coefficients). Efforts were made to minimize the effects of potential confounders, which were controlled using multivariate analysis. Statistical analyses were performed using the computer program SPSS version 16.0. The Kaplan–Meier method was used to predict the cumulative risk of NLDO in our series.
Results
Among the 864 DTC patients who were treated with 131I therapy, 19 (2.2%) were identified with NLDO (Table 1). No event of NLDO was seen in any patient who was untreated with 131I therapy or was treated with 131I therapy doses below 150 mCi. The mean age of the study population was 51.9±10.5 years (range: 39–72 years), and our population consisted of 15 females (78.9%) and four males (21.1%), with a female-to-male ratio of 3.7:1. The mean individual 131I dose was 311.1±169.3 mCi (range: 150–600 mCi). The mean duration between the date of 131I therapy and the occurrence of apparent NLDO was 11.6±4.1 months (range: 6.5–20 months).
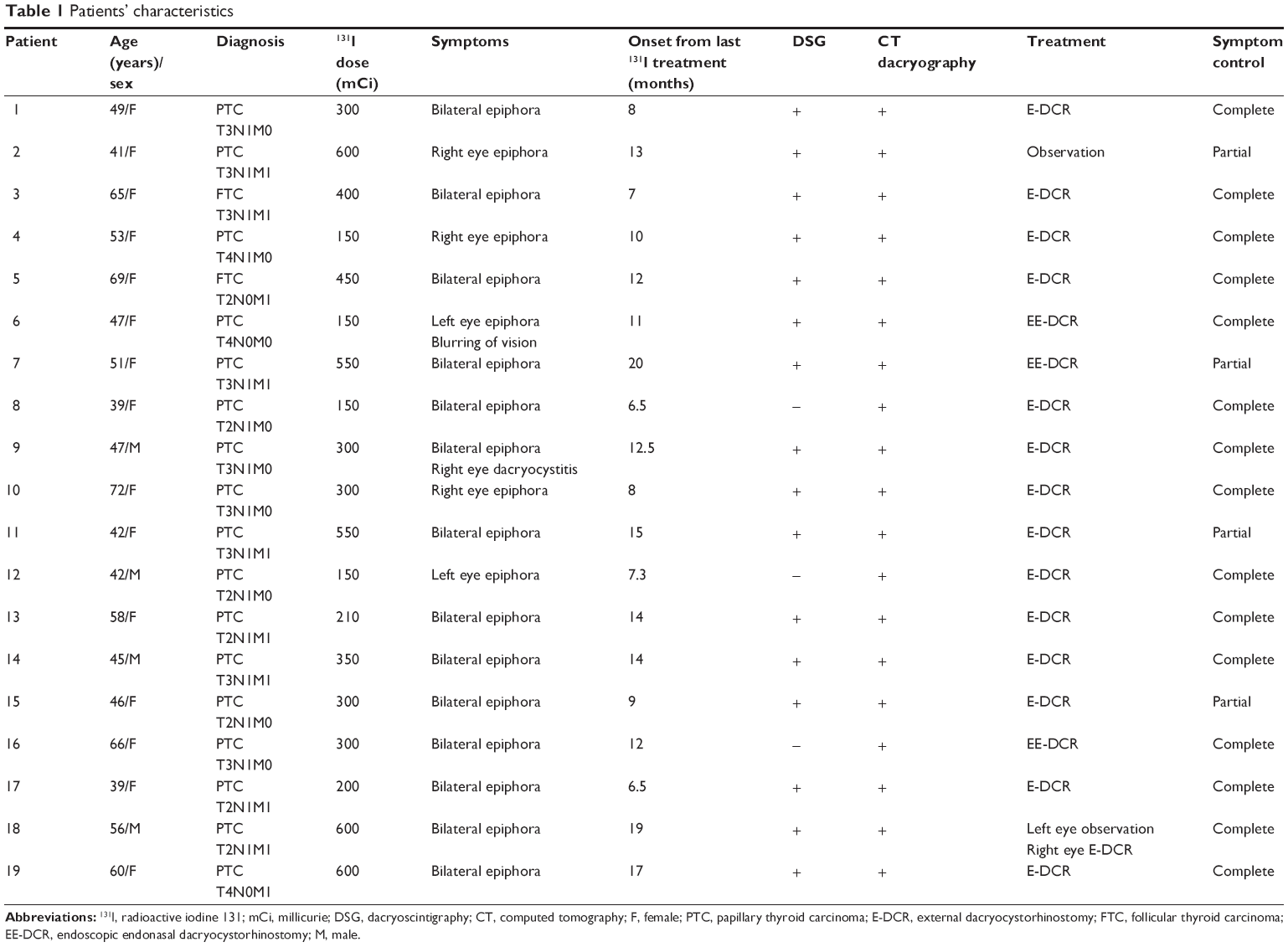 | Table 1 Patients’ characteristics |
Fourteen (73.7%) patients had bilateral epiphora. Dacryoscintigraphy allowed for the detection of 16 NLDO with a sensitivity of 84.2% (95% confidence interval [CI]: 60.4–96.4) and a specificity of 99.6% (95% CI: 98.9–99.9), while CT dacryography detected all cases of NLDO with a sensitivity of 100% (95% CI: 82.2–100) and a specificity of 100% (95% CI: 82.2–100).
DCR was performed in 32 completely stenosed nasolacrimal ducts of 18 (94.7%) patients – either bilaterally (63.2%) or unilaterally (26.3%). Three patients (15.8%) had endoscopic endonasal DCR. Observation was planned for one patient; but the patient had partial relief and was considered for DCR. Among the DCR patients, complete recovery was obtained in 14 (73.7%) patients, and partial relief was obtained in three (15.8%) patients. The success rates of external DCR and endoscopic endonasal DCR were 85.7% and 66.7%, respectively.
A significant correlation between NLDO and 131I therapy doses above 150 mCi was seen (R=0.92; R2=0.86; P=0.03). Multivariate analysis showed that 131I therapy doses above 150 mCi and an age >45 years were important prognosticators (Figure 1).
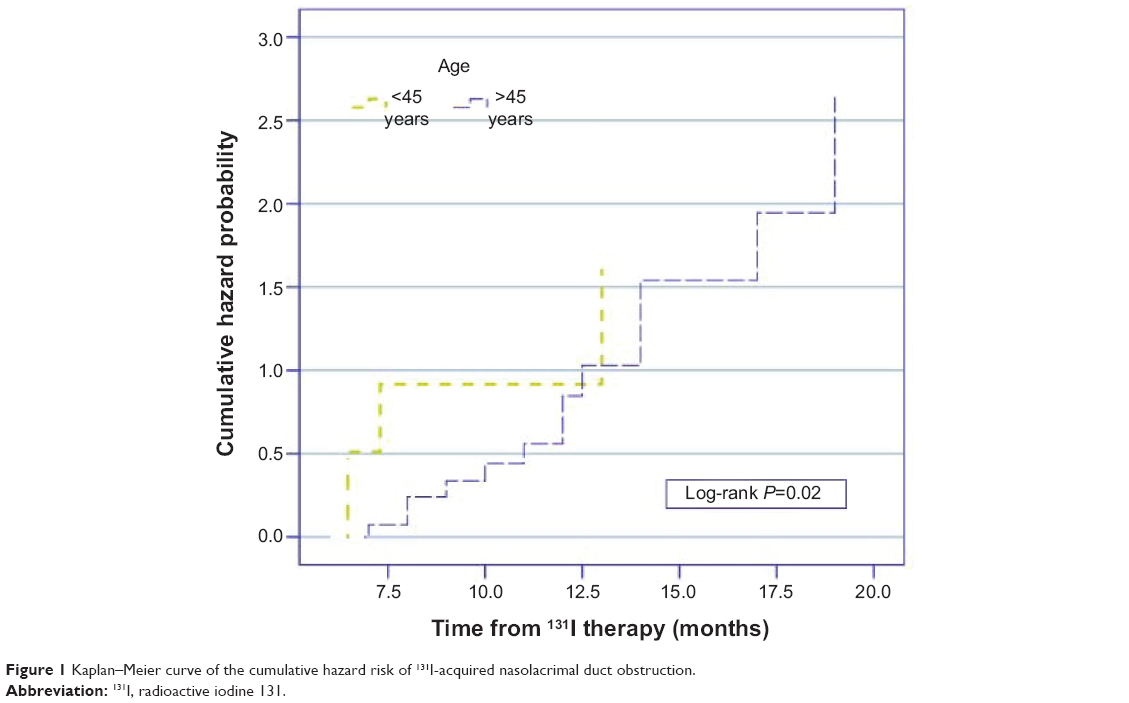 | Figure 1 Kaplan–Meier curve of the cumulative hazard risk of 131I-acquired nasolacrimal duct obstruction. |
Discussion
Acquired NLDO secondary to 131I therapy is an extremely rare complication in patients with DTC. In our cohort, the frequency of NLDO of 2.2% is consistent with other reported results (Table 2).6–10 The incidence rate of NLDO in the general population is lacking, despite a detailed medical literature search. In the majority of cases, the diagnosis is made upon the basis of spontaneous reporting of epiphora by the patients.6 This diagnostic delay leads to complete stenosis of the nasolacrimal ducts, and thus renders these patients to aggressive treatment.6 In the clinical setting, the Jones fluorescein dye test is of significant value in NLDO patients.One Australian study has demonstrated that a negative single-drop Jones fluorescein dye test is also predictive of symptomatic improvement after DCR in patients with NLDO.11
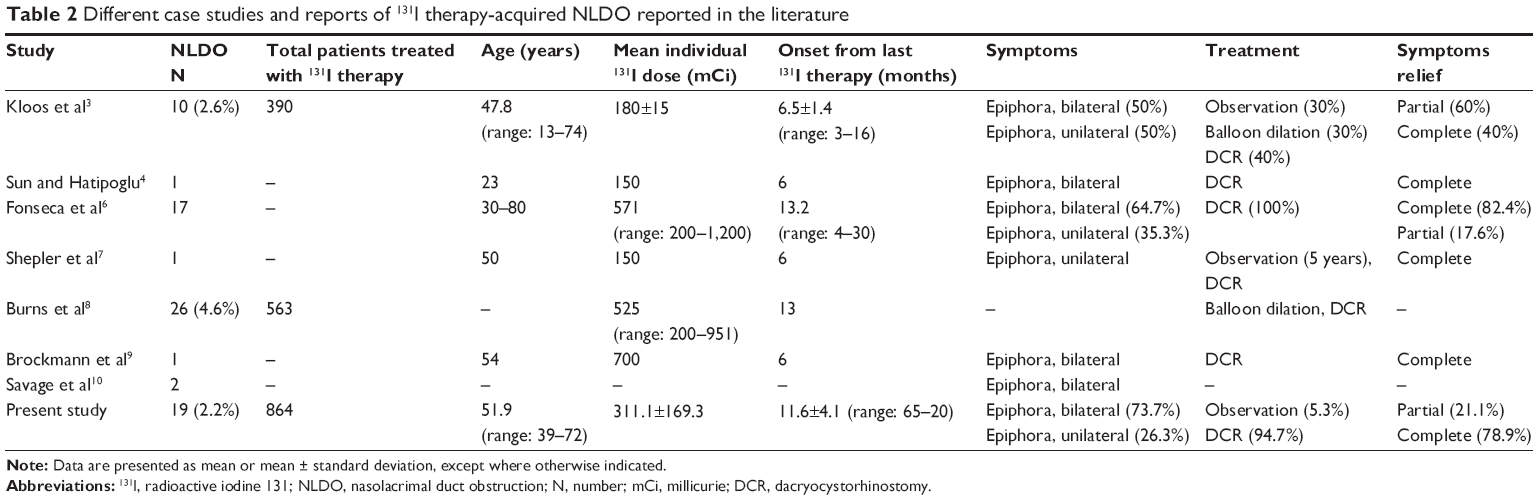 | Table 2 Different case studies and reports of 131I therapy-acquired NLDO reported in the literature |
The postulated mechanism for 131I therapy-acquired NLDO is the direct uptake of 131I in the nasolacrimal duct membrane epithelial cells via the sodium (Na+)/iodide (I) symporter (NIS) leading to radiation-induced cell damage (inflammation and fibrosis/stenosis).9 The NIS is a membrane glycoprotein that mediates 131I uptake in the thyroid gland and several other extrathyroid tissues (salivary glands, lacrimal glands, and ciliary body of the eye).12 Recently, Morgenstern et al13 have reported the overexpression of NIS in the nasolacrimal ducts using reverse transcriptase polymerase chain reaction and immunohistochemical analyses. In addition to the presence of sinonasal disease at the time of 131I therapy, the treatment may theoretically further decrease the flow in the nasolacrimal ducts and thus increase the exposure to 131I, which is secreted through the lacrimal system.3
The diagnosis of 131I therapy-acquired NLDO is challenging. Other possible causes (allergic or viral conjunctivitis, keratoconjunctivitis sicca, trichiasis, canaliculitis, iritis, and functional causes of excessive tears) should be ruled out to reach a definitive diagnosis of 131I therapy-acquired NLDO.14 131I therapy-acquired NLDO is defined as: 1) the presence of NLDO in 131I therapy-treated patients; 2) an 131I dose–NLDO relationship; 3) immediate onset of symptoms after 131I therapy; and 4) the bilateral nature of NLDO in most of cases. CT dacryography using diluted contrast medium was found to be an easy and highly sensitive tool to evaluate NLDO in our cohort, which endorsed the findings of Garcier et al.15
Patients with incomplete NLDO have an excellent outlook with the use of balloon dilation and stenting, as complete recovery of symptoms is observed in 100% of cases.3 Although the literature supports the hypothesis of complete symptom recovery with observation alone, in a few cases of incomplete NLDO, we did not find that observation was a feasible option. The reason for this can be explained by the fact that NLDO is possibly a chronic radiation-induced injury that progresses over a period of time.16 The DCR success rate of 78.9% in our cohort is consistent with the findings of Fonseca et al.6 However, the endoscopic endonasal DCR success rate of 60% is much inferior to that reported in the literature, which warrants more personnel training in this area in our region.17
Because NLDO impairs the quality of life of a patient significantly, prevention of NLDO is a key issue. Currently, there is no mechanism available to stop the blockage of 131I uptake in the nasolacrimal ducts via the NIS during 131I therapy,3 and there is scant data available regarding the prophylactic use of 2-(S)-(3-aminopropylamino) ethylphosphorothioic acid (amifostine) during 131I therapy.18 Further, the effectiveness of topical saline drops, nasolacrimal duct massage, and delaying 131I therapy in patients with acute or chronic sinonasal problems as preventive measures needs to tested. Low 131I therapy doses, whenever possible, can reduce the incidence of NLDO.19
The limitations of our study were: 1) no systematic attempt to screen for NLDO or the presence of other potential confounders (sinonasal problems) was performed; and 2) the presence of possible selection and recall bias in our cohort.
Conclusion
In conclusion, NLDO following 131I therapy in DTC patients is an under-recognized and rare complication, especially at higher 131I doses (>150 mCi). A multidisciplinary approach (nuclear medicine/oncology, ear, nose, and throat, and ophthalmology) is very important in the prevention and treatment of NLDO.
Author contributions
KHAQ and MAA designed the concept of the study. MAT, MAA, and YB carried out data collection; NJA, IM, and AAA carried out manuscript writing. MAT, YB, and AAA performed statistical analysis. All authors read and approved the final manuscript. All authors contributed toward data analysis, drafting and revising the paper and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
Patel SS, Goldfarb M. Well-differentiated thyroid carcinoma: the role of post-operative radioactive iodine administration. J Surg Oncol. 2013;107(6):665–672. | ||
Fard-Esfahani A, Emami-Ardekani A, Fallahi B, et al. Adverse effects of radioactive iodine-131 treatment for differentiated thyroid carcinoma. Nucl Med Commun. 2014;35(8):808–817. | ||
Kloos RT, Duvuuri V, Jhiang SM, Cahill KV, Foster JA, Burns JA. Nasolacrimal drainage system obstruction from radioactive iodine therapy for thyroid carcinoma. J Clin Endocrinol Metab. 2002;87(12):5817–5820. | ||
Sun GE, Hatipoglu B. Epiphora after radioactive iodine ablation for thyroid cancer. Thyroid. 2013;23(2):243–245. | ||
Hussain F, Iqbal S, Mehmood A, Bazarbashi S, ElHassan T, Chaudhri N. Incidence of thyroid cancer in the Kingdom of Saudi Arabia, 2000–2010. Hematol Oncol Stem Cell Ther. 2013;6(2):58–64. | ||
Fonseca FL, Lunardelli P, Matayoshi S. [Lacrimal drainage system obstruction associated to radioactive iodine therapy for thyroid carcinoma]. Arq Bras Oftalmol. 2012;75(2):97–100. Portuguese. | ||
Shepler TR, Sherman SI, Faustina MM, Busaidy NL, Ahmadi MA, Esmaeli B. Nasolacrimal duct obstruction associated with radioactive iodine therapy for thyroid carcinoma. Ophthal Plast Reconstr Surg. 2003;19(6):479–481. | ||
Burns JA, Morgenstern KE, Cahill KV, Foster JA, Jhiang SM, Kloos RT. Nasolacrimal obstruction secondary to I(131) therapy. Ophthal Plast Reconstr Surg. 2004;20(2):126–129. | ||
Brockmann H, Wilhelm K, Joe A, Palmedo H, Biersack HJ. Nasolacrimal drainage obstruction after radioiodine therapy: case report and a review of the literature. Clin Nucl Med. 2005;30(8):543–545. | ||
Savage MW, Sobel RK, Hoffman HT, Carter KD, Finkelstein MW, Shriver EM. Salivary gland dysfunction and nasolacrimal duct obstruction: stenotic changes following I-131 therapy. Ophthal Plast Reconstr Surg. Epub 2014 May 15. | ||
O’Donnell BA, Clement CI. Assessing patients with epiphora who are patent to syringing: clinical predictors of response to dacryocystorhinostomy. Ophthal Plast Reconstr Surg. 2007;23(3):173–178. | ||
Jhiang SM, Cho JY, Ryu KY, et al. An immunohistochemical study of Na+/I− symporter in human thyroid tissues and salivary gland tissues. Endocrinology. 1998;139(10):4416–4419. | ||
Morgenstern KE, Vadysirisack DD, Zhang Z, et al. Expression of sodium iodide symporter in the lacrimal drainage system: implication for the mechanism underlying nasolacrimal duct obstruction in I(131)-treated patients. Ophthal Plast Reconstr Surg. 2005;21(5):337–344. | ||
Fard-Esfahani A, Farzanefar S, Fallahi B, et al. Nasolacrimal duct obstruction as a complication of iodine-131 therapy in patients with thyroid cancer. Nucl Med Commun. 2012;33(10):1077–1080. | ||
Garcier JM, Napon M, Chiambaretta F, et al. [CT dacryography without selective lacrimal duct catheterization: review of 39 patients]. J Radiol. 2002;83(11):1743–1747. French. | ||
Pediatric Eye Disease Investigator Group. A randomized trial comparing the cost-effectiveness of 2 approaches for treating unilateral nasolacrimal duct obstruction. Arch Ophthalmol. 2012;130(12):1525–1533. | ||
Ali MJ, Psaltis AJ, Bassiouni A, Wormald PJ. Long-term outcomes in primary powered endoscopic dacryocystorhinostomy. Br J Ophthalmol. Epub 2014 Jul 4. | ||
Bohuslavizki KH, Klutmann S, Jenicke L, et al. Salivary gland protection by S-2-(3-aminopropylamino)-ethylphosphorothioic acid (amifostine) in high-dose radioiodine treatment: results obtained in a rabbit animal model and in a double-blind multi-arm trial. Cancer Biother Radiopharm. 1999;14(5):337–347. | ||
Mallick U, Harmer C, Hackshaw A. The HiLo trial: a multicentre randomised trial of high- versus low-dose radioiodine, with or without recombinant human thyroid stimulating hormone, for remnant ablation after surgery for differentiated thyroid cancer. Clin Oncol (R Coll Radiol). 2008;20(5):325–326. |
 © 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2014 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.