")
Back to Journals » Degenerative Neurological and Neuromuscular Disease » Volume 13
Neuroimaging Correlates of Patient-Reported Outcomes in Multiple Sclerosis
Authors Jakimovski D , Wicks TR, Bergsland N, Dwyer MG, Weinstock-Guttman B , Zivadinov R
Received 13 October 2022
Accepted for publication 24 January 2023
Published 1 February 2023 Volume 2023:13 Pages 21—32
DOI https://doi.org/10.2147/DNND.S384038
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Thomas Müller
Dejan Jakimovski,1,* Taylor R Wicks,1,* Niels Bergsland,1,2 Michael G Dwyer,1 Bianca Weinstock-Guttman,3 Robert Zivadinov1,4
1Buffalo Neuroimaging Analysis Center, Department of Neurology, Jacobs School of Medicine and Biomedical Sciences, University at Buffalo, State University of New York, Buffalo, NY, USA; 2IRCCS, Fondazione Don Carlo Gnocchi, Milan, Italy; 3Department of Neurology, Jacobs Comprehensive MS Treatment and Research Center, Jacobs School of Medicine and Biomedical Sciences, University at Buffalo, State University of New York, Buffalo, NY, USA; 4Center for Biomedical Imaging at the Clinical Translational Science Institute, University at Buffalo, State University of New York, Buffalo, NY, USA
*These authors contributed equally to this work
Correspondence: Dejan Jakimovski, Buffalo Neuroimaging Analysis Center, Department of Neurology, Jacobs School of Medicine and Biomedical Sciences, University at Buffalo, State University of New York, 100 High Street, Buffalo, NY, 14203, USA, Tel +1 716-859-7040, Fax +1 716-859-7066, Email [email protected]
Background: Patient-reported outcomes (PROs) are increasingly associated with concurrent and future impairments in persons with multiple sclerosis (pwMS). The structural and pathological relationships with PROs in pwMS have not been elucidated.
Methods: One hundred and forty-two pwMS and 47 healthy controls (HCs) were scanned using 3T MRI and completed a PRO questionnaire named Lifeware® that outlines the physical and psychosocial abilities. Beck’s Depression Inventory (BDI) assessed levels of depression. T1- and T2-lesion volume, volumes of the whole brain (WBV), gray matter (GMV), white matter (WMV) and lateral ventricle (LVV) were derived using JIM and SIENAX software. Additional deep GM (DGMV) and nuclei-specific volumes of the thalamus, caudate, globus pallidus, putamen, and hippocampus were calculated using FIRST. Ordinal regression models adjusted for age and depression and mediation analyses were used.
Results: When compared to HCs, pwMS reported significantly greater limitations in mobility domains, including standing up from low seat (p < 0.001), climbing flight of stairs (p < 0.001), lower limb limitation (p < 0.001), limitations in bladder continence (p = 0.001) and fatigability (p < 0.001). Patient-reported limitations related to lower extremity function were explained by age, BDI, and all DGM nuclei volumes (p < 0.029). No such relationships were seen in the HCs. Fatiguability and the extent of life satisfaction were only related to depression (BDI p < 0.001) and not associated with any MRI-based outcomes. Most relationships between structural pathology and PROs were mediated by BDI scores (p < 0.001). In the pwMS group, there were no significant differences in any MRI-based brain volumes between the levels of reported life satisfaction.
Conclusion: PRO measures of lower extremity limitations were associated with DGM structures and DGM-specific nuclei. These findings promote the relevance of measuring DGM structures as measures directly related to subjective well-being and walking limitations. Depression is a significant mediator of PROs and in particular of life satisfaction.
Keywords: patient-reported outcomes, multiple sclerosis, MRI, deep gray matter
Introduction
Multiple sclerosis (MS) is a neurodegenerative and inflammatory disease of the central nervous system (CNS) primarily affecting the young working population.1 Persons with multiple sclerosis (PwMS) experience a wide array of neurological disabilities that range from cognitive to motor deficits, visual impairments, and fatigue that ultimately lead to lower quality of life (QoL).2 Most symptoms have an insidious start and progression, which is commonly under perceived by their social peers and clinicians alike.3 Additionally, living with a chronic disease such as MS is associated with higher incidence of psychosocial consequences like anxiety, lower life satisfaction, lower self-esteem and reoccurring feelings of guilt.4
In contrast to the self-perceived limitations of pwMS, MS disability is clinically quantified by clinicians and researchers using standardized measures that generally focus on physical and, in particular, walking disability. The most commonly utilized clinical measures within the field of MS are the Expanded Disability Severity Scale (EDSS), Timed 25-foot walk test and 9-hole peg test, which are heavily biased towards ambulation difficulties, upper and lower extremity impairments, respectively.5–7 In recent decades, the measurement of cognitive performance has emerged as an important and clinically relevant aspect of the comprehensive assessment of pwMS.8 The cognitive concerns are particularly emphasized in the ever increasing and aging MS population.9 Combinations of such measures were attempted in creating composite disability scores with varying clinical acceptance.10,11
None of the aforementioned clinical measures incorporate potentially useful patient-reported perspectives and self-evaluation. In the mid-2000s, the National Institutes of Health (NIH) recognized the lack of patient-reported outcomes (PROs) and the initiated development of two standardized sets of questionnaires. Neuro-QoL was developed as a standard PRO measure that can be used in neurological conditions and PROMIS, a PRO measure developed for chronic health conditions.12,13 Reimbursement policy changes have contributed to greater adoption of such measures as part of the routine MS clinical care. PROs generally consist of subjective information disclosed by patients about their current symptoms, their functions and limitations, the self-perceived QoL, and aspects related to the disease management. Multiple MS studies suggest a clear discrepancy between objective performance-based measures and PROs.14,15 Moreover, PROs can be used as a medium which supports and fosters patient-clinician communication.16 Lastly, PROs are becoming an integral part in the design of current and future large-scale clinical MS trials.17 One such measure is LIFEware System™, a short PRO questionnaire that has been previously validated in healthy aging population and in pwMS.18
One of the most commonly utilized diagnostic and prognostic paraclinical measures in MS is the use of magnetic resonance imaging (MRI) that allows for in vivo visualization of MS pathology and anatomical damage.19 However, conventional MRI-based measures of MS explain a small portion of clinical outcomes in MS.20 Better known as the clinico-radiological paradox, current research is looking to bridge the gap between MRI abnormalities and concurrent clinical presentation of MS.21 PROs may provide a plausible avenue that could rectify the discrepancy between objective disability measures and MS-based pathological changes. The current study aims at determining the neuroimaging correlates of PROs in PwMS. In particular, we hypothesized that PRO measures related to physical disability would be associated with previously suggested neuroanatomical drivers of disability in pwMS such as the deep gray matter (DGM) volume loss. On the other hand, we hypothesized that relationships between psychosocial PRO measures and neuroanatomy in pwMS may be significantly influenced by coexisting mood modifiers such as the level of depression.
Materials and Methods
Study Population
Both the pwMS and healthy controls (HCs) included in these analyses were part of a larger prospective study that investigated the role of cardiovascular, environmental and genetic factors in multiple sclerosis (CEG-MS). The inclusion criteria for the pwMS were: 1) 18–75 years old, 2) diagnosed as MS based on the 2010-revised McDonald criteria or as a person with clinically isolated syndrome (CIS), and 3) clinical visit and an MRI examination within 30 days of each other. Contrarily, the exclusion criteria were: 1) pregnant or nursing mothers, 2) contraindications that prevent performing a magnetic resonance imaging (MRI), 3) presence of another coexisting major neurological disorder, 4) presence of major psychiatric disorder such as major depressive syndrome that could influence the PRO-based outcomes and 5) clinically-defined relapse or use of intravenous corticosteroids 30 days before the MRI examination. Similarly, the inclusion criteria for the HCs were 1) 18–75 years old and 2) clinical visit and an MRI examination within 30 days of each other. The exclusion criteria for the HCs were 1) presence of major neurological or psychiatric disorder, 2) presence of major depressive disorder, and 3) pregnant or nursing mothers. The study was approved by the Institutional Review Board (IRB) of the University at Buffalo and all subjects signed written informed consent. All study procedures were in line with the Declaration of Helsinki.
All pwMS were examined by an experienced neurologist using the current standard of EDSS and using the multiple sclerosis severity score (MSSS).5 The pwMS were classified into clinically isolated syndrome (CIS)/relapsing-remitting MS (RRMS) or progressive MS (PMS) based on the latest Lublin classification.22 All study subjects were interviewed by trained research personal using structured questionnaires.
Patient-Reported Outcomes
PROs were assessed using the LIFEware System™, a short, single-page Likert questionnaire that can be completed within several minutes. LIFEware™ queries about both physical limitations (standing up from a low seat, climbing a flight of stairs, upper and lower extremity limitations, vision, fatigue, and bowel/bladder limitations) and psychosocial limitations such as life satisfaction.18 The LIFEware questionnaire is provided in the Supplement material of the manuscript. The questionnaire exhibits high intra-rater stability (between 0.9 and 0.99), was validated and re-calibrated by using the Rasch analysis.23 Such analysis allows cross-questionnaire comparison and re-classification of the outcomes into categorical, ordinal or numerical output.24 In our analysis, we utilized each question as a stand-alone measure. Additional composite measures of general physical and psychosocial measures can be calculated. The LIFEware system has been previously validated in multiple neurological, cardiovascular and orthopedic populations.25,26
MRI Acquisition and Analyses
The MRI analyses were performed on scans acquired on a 3T GE Signa Excite (GE, Milwaukee, WI, USA), and 8-channel head and neck coil. The detailed parameters of the MRI acquisition published elsewhere.27 There were no changes to the MRI hardware or software through the length of the study. The lesion burden in the pwMS and HCs was determined using a semi-automated, edge detecting contouring/thresholding technique. Both T1- and T2-lesion volumes were produced. The volumes of the whole brain (WBV), gray matter (GMV), white matter (WMV), lateral ventricular volume (LVV), and volumes of the deep gray matter (DGM) structures were obtained using SIENAX and FIRST software (version 2.6, Oxford, UK). In particular, the volumes of DGM nuclei of the thalamus, caudate, globus pallidus, putamen and hippocampus were acquired. In order to prevent tissue misclassification, lesions were in-painted on the 3D T1-weighted image prior to segmentation.28
Statistical Analyses
All statistical analyses were performed using SPSS version 26.0 (IBM, Armonk, NY, USA). The distribution of the data was determined by visual inspection of the histograms and Q-Q plots. Additional tests of normality using Kolmogorov–Smirnov test were performed. Comparison of categorical data was performed using chi-square test, comparison of parametric data was performed using Student’s t-test and analysis of variance (one-way ANOVA) and comparison of non-parametric data was performed using Mann–Whitney U-test and Kruskal Wallis H-test. Ordinal regression models determined the relationship between PRO-based limitations and MRI outcomes. After adjusting for effects derived by age, sex and level of depression (BDI-FS scores), a step-wise criteria determined the best MRI predictors of PROs with entry of 0.05 and removal of 0.1. P-values lower than 0.05 were considered statistically significant. Mediation analysis was performed using the PROCESS macro for SPSS (plugin version 4.0). The analysis consisted of the DGM volume as an independent variable, physical and psychosocial limitations as dependent variables and depression scores as the mediator. Total, direct, and indirect (mediating) effects were recorded and their ratios calculated.
Results
Demographic, Clinical and MRI Characteristics of the Study Groups
The demographic and clinical characteristics of the 142 patients (91 CIS/RRMS and 51 PMS) participants are shown in Table 1. The study population consisted of a ratio of 71.8% female, with the mean age being 53.1 years old (SD = 11.5). The average disease duration was 20.0 years, with a mean disease onset occurring at 32.7. The median disability score for the study population was an EDSS of 3.0 (interquartile range; IQR 2.0–6.0) and a median MSSS of 2.6 (IQR 1.2–5.6). There were 47 HCs involved in the study with a median age 51.5 years old (SD = 11.1) and a 70.2% female representation. There were no statistical differences in the demographic characteristics between the pwMS and HCs (age, sex and body mass index p > 0.05). The pwMS reported significantly greater level of depressive symptoms when compared to the HCs (median BDI-FS score of 2.6 vs 1.2, p < 0.001). The pwMS were most commonly treated with interferon-β (29.6%), followed by glatiramer acetate (27.5%), oral DMTs (12.7%), natalizumab (5.6%) and off-label DMTs (4.9%), A total of 28 pwMS were not treated with any DMT (19.7%). When compared to pwCIS/RRMS, the pwPMS were significantly older (48.9 vs 60.4 years old, p < 0.001), had longer disease duration (16.3 vs 26.7 years, p < 0.001) and were significantly more disabled when measureed both by EDSS (median 6.5 vs 2.0, p < 0.001) or MSSS (median 5.6 vs 1.6, p < 0.001). There were no differences in the age of MS onset nor in the distribution of DMTs between the pwCIS/RRMS and pwPMS.
 |
Table 1 Demographic and Clinical Characteristics of the Study Population |
Similarly, the pwPMS had significantly greater MRI-based pathology when compared to the pwCIS/RRMS in most MRI outcomes (T2-LV, WBV, GMV, WMV, DGM and the DGM-based nuclei). (Table 2) Only the volume of two DGM structures were not statistically different between the MS subtypes (globus pallidus, p = 0.137, and hippocampus, p = 0.111).
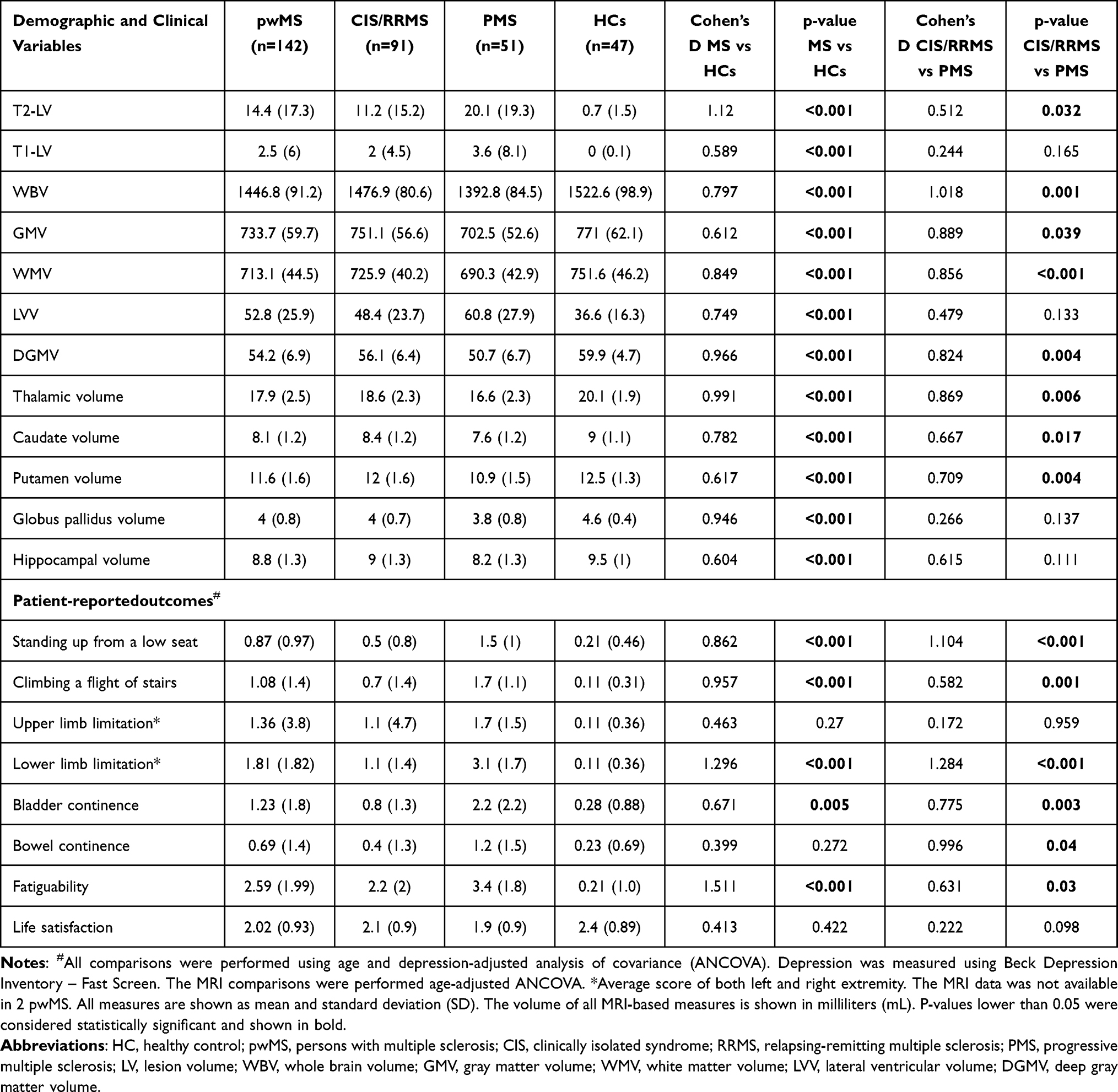 |
Table 2 Patient Reported Outcomes and MRI Measures of the Study Population |
Patient-Reported Outcomes in the Study Population
The PROs from the total pwMS population, the HCs, and each of the MS subtypes are also shown in Table 2. All PRO comparisons mentioned hereafter were adjusted for differences in age and depression scores. When compared to HCs, pwMS reported significantly greater limitations in mobility domains, including standing up from a low seat (p < 0.001), climbing a flight of stairs (p < 0.001), lower limb limitation (p < 0.001). Additional limitations in bladder continence (p = 0.001) and fatigability (p < 0.001) were recorded. These features were additionally and significantly greater in the pwPMS population when compared to the pwCIS/RRMS. Only bowel continence was specifically higher in pwPMS when compared to the pwCIS/RRMS (p = 0.03).
Relationship Between MRI-Based Outcomes and Patient-Reported Outcomes
Step-wise ordinal regression models determined which clinical and MRI-based factors were associated with the reported limitation in each domain. The regression models in the total pwMS population are shown in Table 3. Without an exception, all limitations in PRO domains were significantly influenced by the depression scores assessed through BDI-FS (p < 0.01). Standing up from a low seat limitation was further associated with higher age (Wald = 8.642, p = 0.003), as well as smaller DGMV (Wald = 8.642, p = 0.003) and smaller volume of each individual DGM-based nucleus (Wald >4.962, p < 0.026). Similar findings were seen in climbing stairs limitation, where lower total DGMV (Wald = 7.314, p = 0.007) and smaller volume of all DGM-based nuclei were associated with greater limitation (Wald >4.778, p < 0.029). Higher lower limb limitation was specifically related to higher T1-LV (Wald = 3.932, p = 0.047), lower DGMV (Wald = 4.968, p = 0.026) and lower volume of the caudate (Wald = 4.138, p = 0.042), putamen (Wald = 5.05, p = 0.025) and hippocampus (Wald = 3.96, p = 0.047).
 |
Table 3 Relationship Between MRI and Patient-Reported Outcomes in pwMS |
On the contrary, the extent of upper limb limitation, bladder continence, bowel continence, fatigability and general life satisfaction were not associated with any MRI-based measure. No significant relationships were seen in the HCs population. Additional analysis regarding the relationship between PROs and MRI-based measures in the CIS/RRMS and PMS subgroups are shown in Supplement Table 1. In the CIS/RRMS group, both BDI-FS and caudate volume were significant predictors of limitations in standing up from a low seat (<0.002) and limitations in climbing stairs (p < 0.039). For the remaining PRO measures including the psychosocial components, the BDI-FS score was the most consistent predictor. In the PMS group, the limitations in upper and lower limb function (including standing up from a low seat and climbing stairs) were most commonly explained by T1-LV, T2-LV and volumes of the putamen and globus pallidus.
The effect of depression scores on the relationship between DGMV with physical limitations and life satisfaction are shown in Figure 1. Depression was a significant mediator of the relationship between DGMV and reported limitations for “climbing stairs” (p = 0.002, indirect effect of 20%). Greater than 80% of the relationship between DGMV and lower extremity limitations were direct and unaffected by depression. On the other hand, depression had significant and opposite effect (p < 0.001) on the relationship between DGMV and reported life satisfaction rendering the association non-significant (total effect p = 0.878).
 |
Figure 1 The mediating effect of depression on the relationship between DGM volume with limitations in “climbing stairs” (A) and life satisfaction (B). Abbreviation: DGM, deep gray matter. Notes: Section A – demonstrates the mediation analysis between DGM volume, depression score and limitations in climbing stairs. Section B – demonstrates the mediation analysis between DGM volume, depression score and life satisfaction. Each effect is shown as effect coefficient and (standard error). P-value lower than 0.05 was considered statistically significant. The analysis was performed using PROCESS macro tool for SPSS (plugin version 4.0). |
The absolute and depression-adjusted, MRI-based volume differences between the four levels of life satisfaction in the pwMS population are shown in Table 4. There were no significant differences in any MRI-based brain volumes between the levels of life satisfaction. In particular, a trend of smaller volumes was seen going from “very satisfied” to “fairly satisfied” and “more satisfied than not”. However, the “not satisfied” responders did not continue these trends and had numerically equal or higher volume when compared to the previous group.
 |
Table 4 Differences in MRI-Based Volumes Based on Levels of Life Satisfaction in the pwMS Population |
Discussion
The findings from this cross-sectional study are multifold. Firstly, and as expected, pwMS report greater levels of depression, increased mobility limitations in areas associated with lower and upper limb function, and fatigability. Secondly, the lower limb-associated limitations in pwMS were significantly associated with total and nuclei-specific DGM structures but not with global brain volume measures or lesional pathology. Lastly, depressive feelings were a significant mediator of all PRO domains and the only factor associated with overall life satisfaction. The significance of these findings and their relationship with the existing data in the literature are discussed hereafter.
Using the Functional Assessment in MS (FAMS) questionnaire, a larger California-based study investigated the relationship between PROs and the same conventional MRI measures.29 While poorer scores in the Emotional Well-Being and Thinking/Fatigue subscales of the health-related QoL (HRQOL) have been correlated with greater lesion load (both T1 and T2 lesions), this HRQOL outcome does not investigate aspects related to the physical limitations.29 Similar findings were seen with the MSQOL-54 and Short Form-36 questionnaires, where only pain, cognition and overall QoL measures were correlated with greater LV and smaller global brain volumes.30 In the same sample, the walking measure was not associated with any global MRI measures.30 The relationship of self-reported limitations in lower extremity function and specifically with DGM structures seen in our study are further corroborated by corresponding objective data.27 In a heterogeneous group of pwMS, slower walking times measured through the timed 25-foot walk test are also associated with lower total DGMV and lower nuclei-specific volumes.27 The relationship between neurodegenerative changes and walking disability is of particular importance when determining and predicting progressive status of the pwMS. A recent longitudinal analysis of 5558 pwMS (164 pwMS with transition to SPMS) demonstrated greater worsening of PRO-based scores just prior to the SPMS transition than those who did not transition into SPMS.31 Similarly, an age, sex, EDSS and disease duration-matched analysis showed that pwMS that are transitioning into SPMS report worsened physical functioning QoL, depression and fatigue scores when compared to stable pwRRMS counterparts.32 Using the same LIFEware questionnaire, greater self-reported fatigue was also able to predict future sustained disability worsening and future psychosocial limitations.33 A much larger body of literature has investigated the relationship between subjective and objective discrepancies of cognitive functioning and MRI measures in pwMS.34–36 For example, hippocampal volume in the early stages of MS is associated with worse subjective memory outcomes when compared to lack of associations with objectively measured memory tests.37 Most importantly, PRO measures from the LIFEwareTM questionnaire have been recently shown to be able to predict the rate of future disability worsening in pwMS.38 In particular, worse baseline PRO measures related to the lower limb functionality such as difficulties in getting up and difficulties in standing for more than 30 minutes have been associated with 2.4-fold and 2.2-fold greater risk of future disability progression.38 Lastly, PROs can reflect the effectiveness of DMT and are starting to be used in conjunction with clinical and MRI-based activity.39
The depressive feelings measured through the stand-alone BDI questionnaire was a considerable mediator of the relationship between psychosocial PROs and MRI measures and may have obscured the MRI correlations. Although present, the relationship between depressive symptoms and physical PROs was less substantial. This relative independence of physical and mental subscores has been shown in the literature.40 For example, a study of 3339 orthopedic patients showed that improvement in the physical function subscore of the Patient-Reported Outcomes Measurement Information System (PROMIS) is not followed with changes in the PROMIS-based depression scores.40 It is also important to note that our study had low average BDI-FS scores with only 31.7% of subjects meeting the 4-point cut-off for minimal depressive symptoms (40pwMS and 5 HCs, respectively). That said, interventions targeting depressive symptoms have the potential to improve physical function, particularly in the older population and corroborates the relationship between the two domains.41
The discrepancy between life satisfaction and depression scores presents as one interesting and potentially contradicting finding. This could be explained by findings from a recent study that suggested that damage and disruption of the negative emotional salience network (connections between the amygdala, temporal lobe and insula) could paradoxically associate with lower self-reported depressive and cognitive symptoms.42 On the other hand, the same injury within that network is associated with poorer objective cognitive performance.42 Therefore, pwMS may report biased and contradictory PRO through their inability to recognize and process negative emotions related to their health and life satisfaction. On the other hand, damage in the front-limbic network and their respective tracts (relationship between the thalamus, amygdala with the anterior cingulate cortex, medial, dorsolateral and ventral prefrontal cortex) may result with greater depressive symptoms and worse life satisfaction.43,44 Therefore, pwMS with varying degrees/ratios of pathology between the two networks could affect the PROs. Further validation of these constructs is needed in separate populations and in a longitudinal design. On top of these features, the literature describes a more general disassociation between the MRI-detected damage and the severity of the clinical symptoms.45 These discrepancies can be in either direction, from large MRI changes and no clinical disability to significant clinical disability and no concurrent MRI damage.45 Apart from depression, the reported life satisfaction in pwMS can be influenced by a multitude of other psychological and psychiatric comorbidities such as presence of bipolar disorders, pseudobulbar affect and anxiety disorders.46
The current study has several limitations that should be considered. The study has a relatively small sample size, and future studies should look to increase the sample size of both the MS and HC groups. This particular limitation became apparent in the additional subgroup analysis of PRO measures in the pwRRMS and pwPMS groups. While the total pwMS group satisfied the commonly used assumption of 10 subjects per independent regression predictor (142 pwMS and 14 predictors; age, BDI-FS and 12 MRI outcomes), this was not the case for the subgroup analysis. Therefore, the lack of significant findings in the pwRRMS and pwMS groups may be due to insufficient power in detecting true associations. Due to the nature of self-reported questionnaires, a subjective bias and perception of the limitations may differ between two different patient groups. The level of limitations may be influenced by the local environment, the available help, and the interactions with similarly disabled peers. Severely-limited (non-ambulatory) pwMS that are living within a structured nursing home environment report significantly lower level of fatigue, pessimism and tension when compared to home-based care.47 The periodic fluctuations in MS symptoms can also result with different answers on questionnaires depending on the period the pwMS was recruited and administered. For example, heat-sensitive pwMS may report higher levels of fatigability that could be related to the current meteorological temperatures (pwMS interviewed during winter versus summer months).48 Moreover, rise in body temperature may cause pwMS to experience greater limitation in walking, rising from chair or have functional reach.49 The cultural aspect of the population can provide an additional subjective bias to the PRO measures.50 Development and validation of language and culturally-adapted PROs would allow greater diversity and inclusiveness of this important clinical tool.51 We acknowledge that the pwMS in our study have female predominance of ~75%, a feature that deliberately aimed at representing the global MS prevalence and widening sex ratios.52 Another limitation is the cross-sectional nature of the study. The temporal relationship between PROs and MRI measures and potential “causal” interpretation could only be determined with a longitudinal design. Each of the domains could be investigated as self-reported outcomes and through close reports of close observers such as partners, family or close friends. The informant report may be a better indicator of certain limitations when compared to the self-reported ones. Lastly, reported limitations related to lower extremity function may be better correlated with spinal cord or cerebellar pathology and not captured by our brain-only MRI investigation. In particular, one study showed that only the volume of the upper spinal cord (C1-C3) and not brain atrophy was associated with impaired extremity-related QoL outcomes.53
In conclusion, PROs related to lower limb limitations are significantly associated with neurodegenerative changes within the DGM structures. These findings promote the relevance of measuring DGM structures as measures directly related to subjective well-being and perception of walking limitations. It further corroborates the importance of DGM structures as drivers of disability in MS. Future studies should specifically determine the reciprocity in treatment effect/response in PROs and specific changes on DGMV measures.
Disclosure
Dejan Jakimovski serves as Associate Editor of Clinical Neurology and Neurosurgery and compensated by Elsevier B.V. Taylor Wicks and Niels Bergsland have nothing to disclose. Michael G. Dwyer received compensation from Keystone Heart for consultant fees. He received financial support for research activities from Bristol Myers Squibb, Novartis, Merck Serono, Mapi Pharma, Keystone Heart, Protembis and V-WAVE Medical. Bianca Weinstock-Guttman received honoraria as a speaker and/or as a consultant for Biogen Idec, Teva Pharmaceuticals, EMD Serono, Genzyme, Sanofi, Genentech, Novartis, Celgene/BMS, Janssen, Labcorp, TG therapeutics, and Horizon. Dr Weinstock-Guttman received research funds from Biogen Idec, EMD Serono, Genzyme, Genentech, Sanofi, Novartis. Robert Zivadinov has received personal compensation from Bristol Myers Squibb, EMD Serono, Sanofi, Protembis, Janssen, 415 Capital, and Novartis for speaking and consultant fees. He received financial support for research activities from Sanofi, Novartis, Bristol Myers Squibb, Octave, Mapi Pharma, CorEvitas, Protembis and V-WAVE Medical. The authors report no other conflicts of interest in this work.
References
1. Thompson AJ, Baranzini SE, Geurts J, Hemmer B, Ciccarelli O. Multiple sclerosis. Lancet. 2018;391(10130):1622–1636. doi:10.1016/S0140-6736(18)30481-1
2. Young CA, Mills R, Rog D, et al. Quality of life in multiple sclerosis is dominated by fatigue, disability and self-efficacy. J Neurol Sci. 2021;426:117437. doi:10.1016/j.jns.2021.117437
3. Lakin L, Davis BE, Binns CC, Currie KM, Rensel MR. Comprehensive approach to management of multiple sclerosis: addressing invisible symptoms-a narrative review. Neurol Ther. 2021;10:75–98. doi:10.1007/s40120-021-00239-2
4. Hanna M, Strober LB. Anxiety and depression in Multiple Sclerosis (MS): antecedents, consequences, and differential impact on well-being and quality of life. Mult Scler Relat Disord. 2020;44:102261. doi:10.1016/j.msard.2020.102261
5. Kurtzke JF. Rating neurologic impairment in multiple sclerosis: an expanded disability status scale (EDSS). Neurology. 1983;33(11):1444–1452. doi:10.1212/WNL.33.11.1444
6. Motl RW, Cohen JA, Benedict R, et al. Validity of the timed 25-foot walk as an ambulatory performance outcome measure for multiple sclerosis. Mult Scler. 2017;23:704–710. doi:10.1177/1352458517690823
7. Feys P, Lamers I, Francis G, et al. The nine-hole peg test as a manual dexterity performance measure for multiple sclerosis. Mult Scler. 2017;23:711–720. doi:10.1177/1352458517690824
8. Benedict RHB, Amato MP, DeLuca J, Geurts JJG. Cognitive impairment in multiple sclerosis: clinical management, MRI, and therapeutic avenues. Lancet Neurol. 2020;19:860–871. doi:10.1016/S1474-4422(20)30277-5
9. Vaughn CB, Jakimovski D, Kavak KS, et al. Epidemiology and treatment of multiple sclerosis in elderly populations. Nat Rev Neurol. 2019;15(6):329–342. doi:10.1038/s41582-019-0183-3
10. Fischer JS, Rudick RA, Cutter GR, Reingold SC. The Multiple Sclerosis Functional Composite Measure (MSFC): an integrated approach to MS clinical outcome assessment. National MS society clinical outcomes assessment task force. Mult Scler. 1999;5:244–250. doi:10.1177/135245859900500409
11. Weideman AM, Barbour C, Tapia-Maltos MA, et al. New multiple sclerosis disease severity scale predicts future accumulation of disability. Front Neurol. 2017;8:598. doi:10.3389/fneur.2017.00598
12. Cella D, Lai JS, Nowinski CJ, et al. Neuro-QOL: brief measures of health-related quality of life for clinical research in neurology. Neurology. 2012;78:1860–1867. doi:10.1212/WNL.0b013e318258f744
13. Gershon RC, Lai JS, Bode R, et al. Neuro-QOL: quality of life item banks for adults with neurological disorders: item development and calibrations based upon clinical and general population testing. Qual Life Res. 2012;21(3):475–486. doi:10.1007/s11136-011-9958-8
14. Goverover Y, Kalmar J, Gaudino-Goering E, et al. The relation between subjective and objective measures of everyday life activities in persons with multiple sclerosis. Arch Phys Med Rehabil. 2005;86(12):2303–2308. doi:10.1016/j.apmr.2005.05.016
15. Ozel O, Vaughn CB, Eckert SP, Jakimovski D, Lizarraga AA, Weinstock-Guttman B. Dimethyl fumarate in the treatment of relapsing-remitting multiple sclerosis: patient reported outcomes and perspectives. Patient Relat Outcome Meas. 2019;10:373–384. doi:10.2147/PROM.S168095
16. Greenhalgh J, Gooding K, Gibbons E, et al. How do patient reported outcome measures (PROMs) support clinician-patient communication and patient care? A realist synthesis. J Patient Rep Outcomes. 2018;2:42. doi:10.1186/s41687-018-0061-6
17. Nowinski CJ, Miller DM, Cella D. Evolution of patient-reported outcomes and their role in multiple sclerosis clinical trials. Neurotherapeutics. 2017;14(4):934–944. doi:10.1007/s13311-017-0571-6
18. Granger C. The LIFEware system^ s^ m. J Rehabil Outcomes Meas. 1999;3:63–69.
19. Jakimovski D, Ramasamy DP, Zivadinov R. Magnetic resonance imaging and analysis in multiple sclerosis. In: Rizvi SA, Cahill JF, Coyle PK, editors. Clinical Neuroimmunology: Multiple Sclerosis and Related Disorders. Cham: Springer International Publishing; 2020:109–136.
20. Uher T, Krasensky J, Sobisek L, et al. Cognitive clinico-radiological paradox in early stages of multiple sclerosis. Ann Clin Transl Neurol. 2018;5(1):81–91. doi:10.1002/acn3.512
21. Barkhof F. The clinico-radiological paradox in multiple sclerosis revisited. Curr Opin Neurol. 2002;15(3):239–245. doi:10.1097/00019052-200206000-00003
22. Lublin FD, Reingold SC, Cohen JA, et al. Defining the clinical course of multiple sclerosis: the 2013 revisions. Neurology. 2014;83(3):278–286. doi:10.1212/WNL.0000000000000560
23. Ottenbacher KJ, Mann WC, Granger CV, Tomita M, Hurren D, Charvat B. Inter-rater agreement and stability of functional assessment in the community-based elderly. Arch Phys Med Rehabil. 1994;75(12):1297–1301. doi:10.1016/0003-9993(94)90276-3
24. Baker JG, Granger CV, Fiedler RC. A brief outpatient functional assessment measure: validity using rasch measures. Am J Phys Med Rehabil. 1997;76(1):8–13. doi:10.1097/00002060-199701000-00003
25. Granger CV, Cotter AC, Hamilton BB, Fiedler RC. Functional assessment scales: a study of persons after stroke. Arch Phys Med Rehabil. 1993;74(2):133–138.
26. Mithal M, Mann WC, Granger CV. The role of Coronary Heart Disease (CHD) in functional limitation in community dwelling elders. Phys Occup Ther Geriatr. 2001;19(3):35–48. doi:10.1080/J148v19n03_03
27. Jakimovski D, Weinstock-Guttman B, Hagemeier J, et al. Walking disability measures in multiple sclerosis patients: correlations with MRI-derived global and microstructural damage. J Neurol Sci. 2018;393:128–134. doi:10.1016/j.jns.2018.08.020
28. Gelineau-Morel R, Tomassini V, Jenkinson M, Johansen-Berg H, Matthews PM, Palace J. The effect of hypointense white matter lesions on automated gray matter segmentation in multiple sclerosis. Hum Brain Mapp. 2012;33(12):2802–2814. doi:10.1002/hbm.21402
29. Mowry EM, Beheshtian A, Waubant E, et al. Quality of life in multiple sclerosis is associated with lesion burden and brain volume measures. Neurology. 2009;72(20):1760–1765. doi:10.1212/WNL.0b013e3181a609f8
30. Fritz NE, Roy S, Keller J, Prince J, Calabresi PA, Zackowski KM. Pain, cognition and quality of life associate with structural measures of brain volume loss in multiple sclerosis. NeuroRehabilitation. 2016;39(4):535–544. doi:10.3233/NRE-161384
31. Conway DS, Thompson NR, Meng X, Johnson K, Fox RJ. Patient reported outcomes and performance metrics at diagnosis of secondary progressive multiple sclerosis. Mult Scler. 2021;27(5):742–754. doi:10.1177/1352458520936214
32. Healy BC, Zurawski J, Chitnis T, Weiner HL, Glanz BI. Patient-reported outcomes associated with transition to secondary progressive multiple sclerosis. Qual Life Res. 2022;31(6):1799–1805. doi:10.1007/s11136-021-03034-6
33. Vaughn CB, Kavak KS, Dwyer MG, et al. Fatigue at enrollment predicts EDSS worsening in the New York state multiple sclerosis consortium. Mult Scler J. 2020;26(1):99–108. doi:10.1177/1352458518816619
34. Kletenik I, Alvarez E, Honce JM, Valdez B, Vollmer TL, Medina LD. Subjective cognitive concern in multiple sclerosis is associated with reduced thalamic and cortical gray matter volumes. Mult Scler J Exp Transl Clin. 2019;5(1):2055217319827618. doi:10.1177/2055217319827618
35. Macaron G, Baldassari LE, Nakamura K, et al. Cognitive processing speed in multiple sclerosis clinical practice: association with patient-reported outcomes, employment and magnetic resonance imaging metrics. Eur J Neurol. 2020;27(7):1238–1249. doi:10.1111/ene.14239
36. Bergsland N, Benedict RHB, Dwyer MG, et al. Thalamic nuclei volumes and their relationships to neuroperformance in multiple sclerosis: a cross-sectional structural MRI study. J Magn Reson Imaging. 2021;53:731–739. doi:10.1002/jmri.27389
37. Glukhovsky L, Brandstadter R, Leavitt VM, et al. Hippocampal volume is more related to patient-reported memory than objective memory performance in early multiple sclerosis. Mult Scler. 2021;27(4):568–578. doi:10.1177/1352458520922830
38. Vaughn C, Kavak KS, Jakimovski D, et al. Patient-reported outcomes are the strongest predictors of disease disability in intramuscular interferon beta-1a users. Neurodegener Dis Manag. In Press 2023.
39. Manchon E, Laplaud D, Vukusic S, et al. Efficacy, safety and patient reported outcomes in patients with active relapsing multiple sclerosis treated with ocrelizumab: final results from the PRO-MSACTIVE study. Mult Scler Relat Disord. 2022;68:104109. doi:10.1016/j.msard.2022.104109
40. Beleckas CM, Guattery J, Chamberlain AM, Khan T, Kelly MP, Calfee RP. Using patient-reported outcomes measurement information system measures to understand the relationship between improvement in physical function and depressive symptoms. J Am Acad Orthop Surg. 2018;26(24):e511–e518. doi:10.5435/JAAOS-D-17-00039
41. Callahan CM, Kroenke K, Counsell SR, et al. Treatment of depression improves physical functioning in older adults. J Am Geriatr Soc. 2005;53(3):367–373. doi:10.1111/j.1532-5415.2005.53151.x
42. Fuchs TA, Vaughn CB, Benedict RHB, et al. Patient-reported outcome severity and emotional salience network disruption in multiple sclerosis. Brain Imaging Behav. 2022;16:1252–1259. doi:10.1007/s11682-021-00614-5
43. van Geest Q, Boeschoten RE, Keijzer MJ, et al. Fronto-limbic disconnection in patients with multiple sclerosis and depression. Mult Scler. 2019;25:715–726. doi:10.1177/1352458518767051
44. Ashton K, Fuchs TA, Oship D, et al. Diagnosis of depression in multiple sclerosis is predicted by frontal-parietal white matter tract disruption. J Neurol. 2021;268:169–177. doi:10.1007/s00415-020-10110-3
45. Healy BC, Buckle GJ, Ali EN, et al. Characterizing clinical and MRI dissociation in patients with multiple sclerosis. J Neuroimaging. 2017;27:481–485. doi:10.1111/jon.12433
46. Kosmidis MH, Bozikas VP, Giannouli V, Karavatos A, Fokas K. Familial comorbidity of bipolar disorder and multiple sclerosis: genetic susceptibility, coexistence or causal relationship? Behav Neurol. 2012;25:341–349. doi:10.1155/2012/894128
47. Younus Z, Vaughn CB, Sanai SA, et al. Fatigue and mood states in nursing home and nonambulatory home-based patients with multiple sclerosis. Int J MS Care. 2017;19:297–302. doi:10.7224/1537-2073.2016-058
48. Grothe M, Gross S, Süße M, Strauss S, Penner IK. The seasonal fluctuation of fatigue in multiple sclerosis. Front Neurol. 2022;13. doi:10.3389/fneur.2022.900792
49. Romberg A, Ikonen A, Ruutiainen J, Virtanen A, Hämäläinen P. The effects of heat stress on physical functioning in persons with multiple sclerosis. J Neurol Sci. 2012;319:42–46. doi:10.1016/j.jns.2012.05.024
50. Calvert MJ, Cruz Rivera S, Retzer A, et al. Patient reported outcome assessment must be inclusive and equitable. Nat Med. 2022;28:1120–1124. doi:10.1038/s41591-022-01781-8
51. Theofilou P, Giannouli V, Kolias S, Tsolaki M. Perception of pain self-efficacy and fatigue in Greek patients with multiple sclerosis: a study protocol. Health Psychol Res. 2015;3:1556. doi:10.4081/hpr.2015.1556
52. Westerlind H, Boström I, Stawiarz L, Landtblom AM, Almqvist C, Hillert J. New data identify an increasing sex ratio of multiple sclerosis in Sweden. Mult Scler. 2014;20:1578–1583. doi:10.1177/1352458514530021
53. Zurawski J, Glanz BI, Healy BC, et al. The impact of cervical spinal cord atrophy on quality of life in multiple sclerosis. J Neurol Sci. 2019;403:38–43. doi:10.1016/j.jns.2019.04.023
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.