")
Back to Journals » Clinical Interventions in Aging » Volume 19
Neutrophil Percentage as a Potential Biomarker of Acute Kidney Injury Risk and Short-Term Prognosis in Patients with Acute Myocardial Infarction in the Elderly
Authors Chen Q , Gu Q , Yin A, Cai D , Xiao T, Wang Y , Ji Y, Wang Q, Wei J, Sun L
Received 18 December 2023
Accepted for publication 12 March 2024
Published 18 March 2024 Volume 2024:19 Pages 503—515
DOI https://doi.org/10.2147/CIA.S455588
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Maddalena Illario
Qianwen Chen,1,* Qingqing Gu,1,* Anwen Yin,2,* Dabei Cai,1 Tingting Xiao,1 Yu Wang,1 Yuan Ji,1 Qingjie Wang,1 Jun Wei,3 Ling Sun1
1Department of Cardiology, the Affiliated Changzhou Second People’s Hospital of Nanjing Medical University, Changzhou, Jiangsu, 213000, People’s Republic of China; 2Department of Cardiology, the Affiliated Wuxi People’s Hospital of Nanjing Medical University, Wuxi, Jiangsu, 214023, People’s Republic of China; 3Department of Cardiovascular Surgery, the First Affiliated Hospital of Wannan Medical College, Wuhu, Anhui, 241000, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Qingjie Wang; Ling Sun, Department of Cardiology, the Affiliated Changzhou Second People’s Hospital of Nanjing Medical University, 29 Xinglong Alley, Changzhou, Jiangsu, 213003, People’s Republic of China, Email [email protected]; [email protected]
Objective: This study aimed to explore the association of preoperative neutrophil percentage (NEUT%) with the risk of acute kidney injury (AKI) in patients with acute myocardial infarction (AMI) having undergone coronary interventional therapy.
Methods: A single-center, retrospective and observational study was conducted. From December 2012 to June 2021, patients with AMI were enrolled and divided into AKI group and non-AKI group. The NEUT% in the two groups was compared. The association between NEUT% with the risk of post-AMI AKI was analyzed by univariate and multivariable logistic regression. Kaplan-Meier survival curve was drawn to evaluate the prognostic ability of NEUT% for short-term all-cause death following AMI.
Results: A total of 3001 consecutive patients were enrolled with an average age of 64.38 years. AKI occurred in 327 (10.9%) patients. The NEUT% was higher in the AKI group than in the non-AKI group ([76.65± 11.43]% versus [73.22± 11.83]%, P< 0.001). NEUT% was also identified as an independent risk factor for AKI in AMI patients after adjustment (OR=1.021, 95% CI: 1.010– 1.033, P < 0.001). Compared with those at the lowest quartile of NEUT%, the patients at quartiles 2– 4 had a higher risk of AKI (P for trend = 0.003). The odds of AKI increased by 29.0% as NEUT% increased by 1 standard deviation (OR=1.290, 95% CI: 1.087– 1.531, P = 0.004). After a median of 35 days follow-up, 93 patients died. Patients with a higher NEUT% presented a higher risk of all-cause death after AMI (Log rank: χ2 =24.753, P< 0.001).
Conclusion: In AMI patients, the peripheral blood NEUT% was positively associated with the odds of AKI and short-term all-cause mortality. NEUT% may provide physicians with more information about disease development and prognosis.
Keywords: neutrophil percentage, acute kidney injury, acute myocardial infarction
Introduction
According to the Global Burden of Cardiovascular Disease and Risk Factors report, the death toll, disability-adjusted life years (DALYs) and years of life lost (YLLs) due to cardiovascular diseases have seen a long-term sustained increase. Ischemic heart disease (IHD), the most prominent cardiovascular disease, causes 182 million DALYs and 9.14 million deaths in 2019 globally and was one of the two leading causes of YLLs in China in 2017.1,2 Acute myocardial infarction (AMI), the most serious type of IHD, manifests rapid onset, high morbidity and mortality. Acute kidney injury (AKI), a common secondary renal injury of AMI, brings with various short- or long-term adverse effects, such as immune dysfunction, bleeding, long hospital stay, and mortality.3,4
AKI may develop in 5.5% to 26.6% of AMI patients during hospitalization.5–7 As shown in previous studies, AKI is associated with a more than three-fold increase in early mortality and a more than two-fold increase in long-term mortality among acute coronary syndrome (ACS) patients,8 and bleeding in a short term and adverse cardiovascular events in a long term.9 At the 2008 consensus conference of the Acute Dialysis Quality Initiative group, cardio-renal syndrome (CRS) was defined to state the interaction between heart and kidney disease and classified into five subtypes. CRS type 1 involves acute deterioration of heart function, including acute heart failure and/or ACS that leads to kidney injury and/or dysfunction.10 Both infectious and non-infectious pathways trigger immune system-mediated inflammatory responses in AKI.11 Inflammation plays an important role in atherogenesis and plaque destabilization, acting as either a trigger or a long-term risk factor.12 During inflammatory responses in AKI, the innate immune system in the infarction area is activated first. Various inflammatory cells (such as neutrophils, macrophages and others) release inflammatory mediators to attack glomerular vascular endothelial cells and aggravate renal injury.13
Different kinds of biomarkers have been found in AKI after AMI, such as renal function indicators (baseline serum creatinine), cardiac function indicators (left ventricular ejection fraction and cardiac troponin I), inflammation-related indicators (neutrophil-to-lymphocyte ratio, high-sensitivity C-reactive protein and others) and others (free triiodothyronine, hemoglobin and others).14–16 AMI triggers a strong inflammatory response that leads to a rapid increase in neutrophils and mononuclear/macrophages in the heart tissue. Clinical data show that major adverse cardiovascular events in AMI patients are correlated with the increase of neutrophils.17,18 The neutrophil percentage (NEUT%) is easy and quickly to be obtained and monitored in clinical practice, thus offering it advantages in ultra-early risk assessment in patients. In previous studies, NEUT% has been associated with all-cause death from a number of diseases, such as ST elevation myocardial infarction (STEMI),19 atrial fibrillation,20 chronic heart failure,21 cardiogenic shock,22 and acute kidney injury.23 For STEMI patients undergoing percutaneous coronary intervention (PCI), some inflammation-related indicators have also a favorable performance in predicting various clinical outcomes or outcome-related events. For example, the ratio of neutrophils to lymphocytes is independently correlated with coronary blood flow,24 and the level of platelet-leukocyte aggregates is independently correlated with myocardial no-reflow.25 Due to the sudden onset of AKI in AMI patients, early prediction is critical for clinical decision-making, and conducive to improving the overall prognosis. It is unclear whether NEUT% is associated with AKI risk after AMI. Hence, this study aimed to explore the association of preoperative NEUT% and the risk of AKI in patients with AMI having undergone coronary interventional therapy.
Methods
Ethical Approval
Registered in the Chinese Clinical Trials Registry system (ChiCTR1800014583), this study abided by the Declaration of Helsinki and was approved by the Ethics Committee of the Affiliated Changzhou Second People’s Hospital of Nanjing Medical University (No.2020-KY253-01). Given the retrospective nature of the study, written informed consent was waived, but the data we obtained were kept anonymously.
Study Population
A total of 3742 hospitalized patients aged 18 years or over and diagnosed with AMI in our hospital between December 2012 to June 2021 were recruited (Figure 1). All enrolled patients received coronary intervention therapy during hospitalization. Of them, 503 patients were excluded because they (1) refused PCI therapy for personal reasons; (2) received coronary artery bypass grafting; (3) used intra-aortic balloon pump during hospitalization. Then, 238 patients were additionally excluded, because they (1) used contrast media or other nephrotoxic drugs within a week before admission; (2) had a recent serious infection, trauma or surgery, with a history of chronic kidney disease; (3) had end-stage renal diseases or received dialysis therapy; (4) did not have baseline or postoperative creatinine data. As a result, 3001 eligible patients were enrolled into the final analysis.
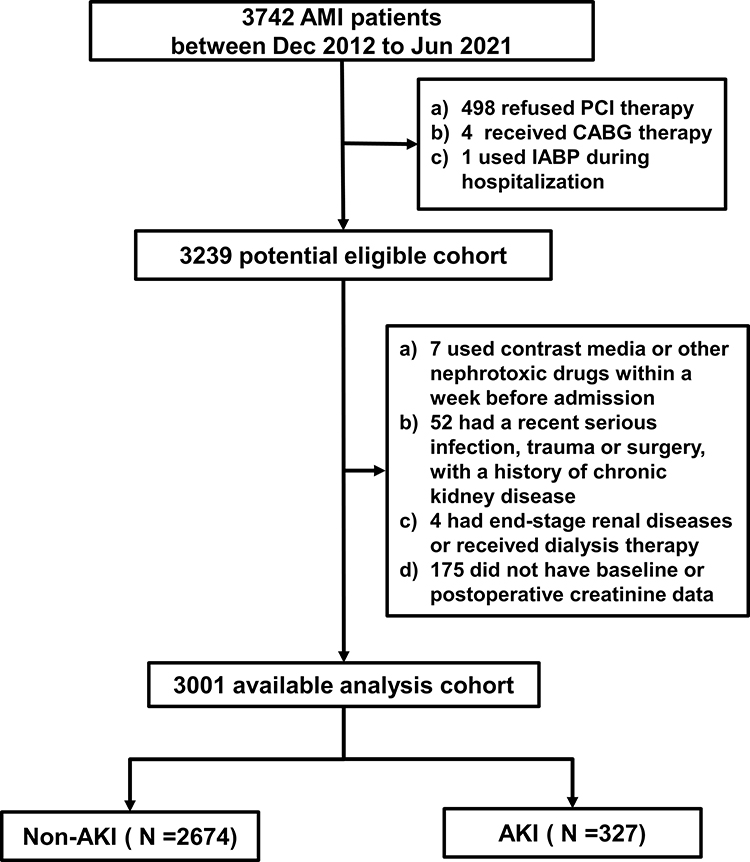 |
Figure 1 Study flow chart. Abbreviations: AMI, acute myocardial infarction; PCI, percutaneous coronary intervention; CABG, coronary artery bypass grafting; IABP, intra-aortic balloon pump; AKI, acute kidney injury. |
Definitions and Data Collection
According to the World Heart Federation’s uniform definition, AMI was defined based on symptoms, serum cardiac biomarkers, and electrocardiographic features.26 AKI was defined according to the 2012 criteria standardized by the Kidney Disease Improving Global Outcomes group, including a serum creatinine increasing to at least 0.3 mg/dL within past 48 h or 1.5 times baseline, or a urine volume of less than 0.5 mL/kg/h.27 In this retrospective study, baseline serum creatinine level was set as that measured at 24 h before operation, and this level was measured again within 48 hours after intervention. Given urine output was not measured in most patients, this index was not introduced into this study.
Collected were patients’ data about baseline demographics, initial vital signs, laboratory tests, angiographic data, medication administration. The in-hospital mortality was documented for all the patients. The therapeutic planning was based on the current guidelines. The PCI procedure was conducted by experienced physicians during the hospital stay.
Follow-Up and Endpoints
Every patient was followed up for about 1 month after intervention, during which events and death were recorded. The primary endpoint was AKI after AMI, and the secondary outcome was all-cause mortality within about 1 month after AMI. These outcomes were reviewed on patients’ medical records upon readmission.
Statistical Analysis
Continuous variables were presented as means with standard deviation (SD), if they conformed to normal distribution. Otherwise, they were displayed as the median with 25% to 75% interquartile range. Discrete variables were described as percentage. Variable normality was tested using the Kolmogorov–Smirnov test. Mann–Whitney U-test and independent sample T-tests were used to compare continuous variables, Chi-squared or Fisher’s exact test to compare categorical variables.
Significant variables in the univariate analysis were incorporated into the multivariable analysis (binary logistic regression) to screen independent predictors of AKI. The results were expressed as odds ratios (OR) and 95% confidence intervals (CI). The association of NEUT% with risk of AKI was evaluated on a continuous scale with restricted cubic spline curve. Kaplan-Meier survival curves were constructed and compared by Log rank test. Pearson analysis was used to evaluate the correlation of NEUT% with other metrics.
Chained equations were used for multiple imputation to handle systematically missing covariates and make best use of the available information and minimize potential bias in eliminating missing data. All statistical tests were two-sided, and P values <0.05 were considered statistically significant. All statistical analyses were performed with SPSS software version 22.0.
Results
Among the 3001 patients enrolled, 327(10.9%) suffered new AKI after PCI. The AKI group was more likely to be older, female, have pre-existing hypertension and diabetes than the non-AKI group (P<0.001) (Table 1). Both groups showed significant differences in body mass index (BMI), number of smokers, number of alcohol drinkers, left ventricular ejection fraction (LVEF), Killip classification, heart rate, absolute neutrophil count, hemoglobin, and cardiac troponin I (TNI) (P all <0.05), but not in baseline serum creatinine and white blood cell count (P>0.05). Particularly, NEUT% was different between the two groups ([76.65±11.43] % versus [73.22±11.83] %, P<0.001) (Figure 2A).
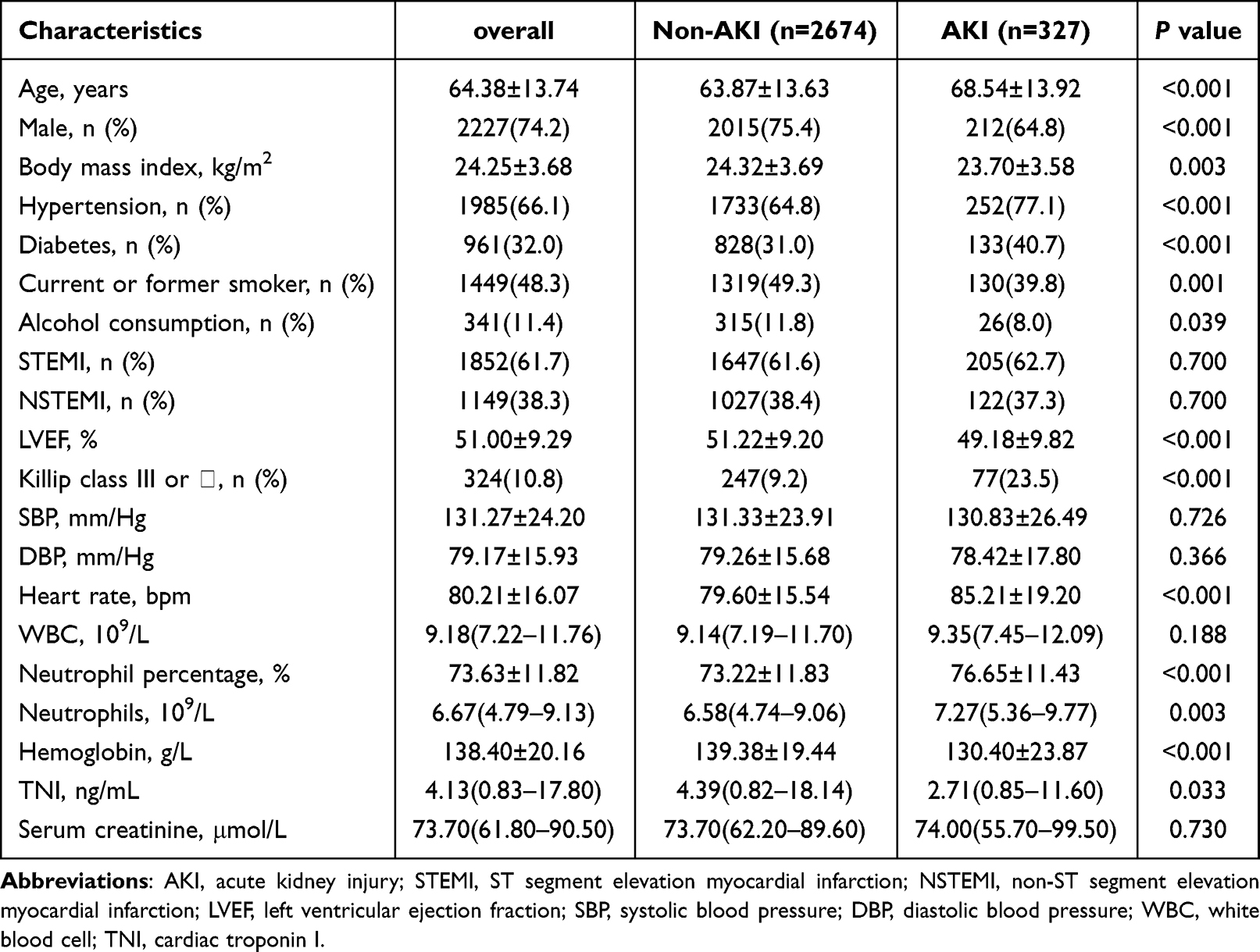 |
Table 1 Baseline Information of Enrolled AKI Patients and Participants |
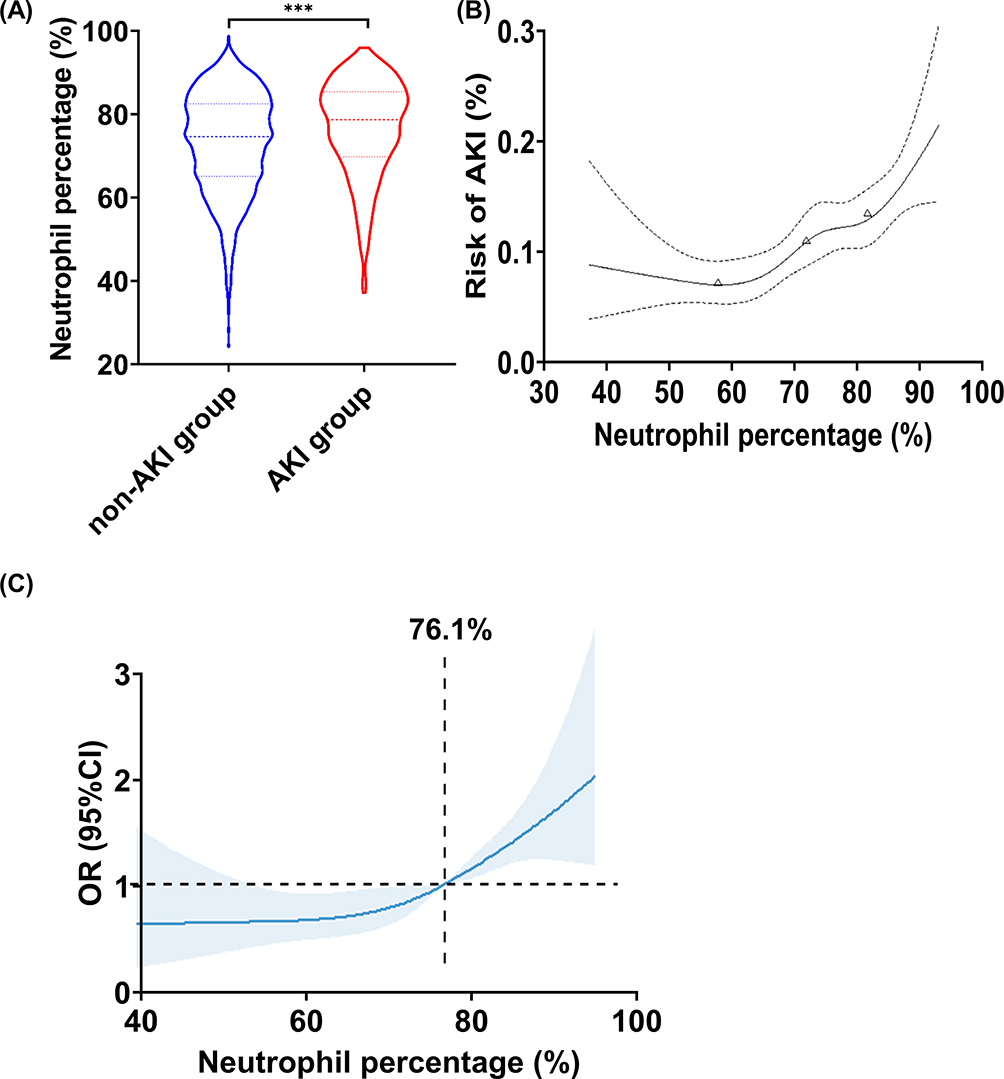 |
Figure 2 Neutrophil percentage levels in different groups and the relation of neutrophil percentage with the risk of AKI in a restricted cubic splines model. (A) The violin plot reflects the distribution and probability density of neutrophil percentage levels between the two groups, with dotted lines representing the 25th, 50th, and 75th percentiles. ***P <0.001. (B) The relation of neutrophil percentage with the risk of AKI on a continuous scale. X-axis represents neutrophil percentage. Y-axis represents the probability of AKI. Dashed lines indicate 95% CI. From left to right, the triangles indicate the 25th, 50th, and 75th percentile. (C) The relation between neutrophil percentage and the risk of AKI by restricted cubic splines. The odds ratio is indicated by the solid blue line, and the 95% CI is represented by the shaded regions derived from the three-node restricted cubic spline regression. The horizontal reference line represented by a dashed line indicates a odds ratio of 1.0, and the vertical reference line is the corresponding neutrophil percentage at this time. Abbreviations: OR, odds ratios; CI, confidence intervals. |
As show in Table 2, the AKI group received more clopidogrel bisulfate and less ticagrelor and statins (all P<0.05). But contrast volume >100 mL and contrast exposure time >60 min showed no between-group differences (P>0.05).
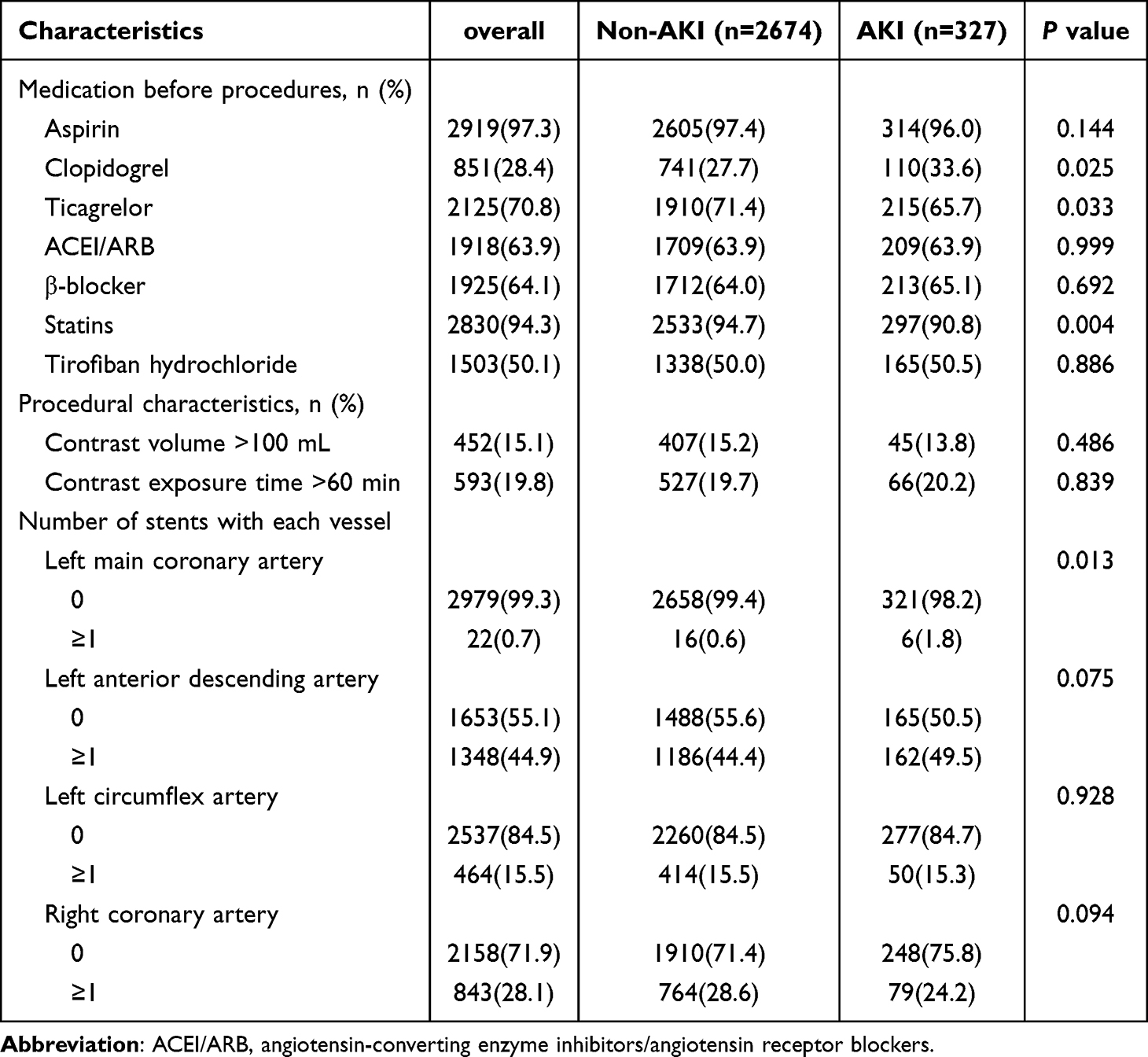 |
Table 2 Medication and Procedural Characteristics of Enrolled AKI Patients and Participants |
After univariate and multivariable analyses, we established three adjusted logistic models. Model 1 was adjusted for only age and gender; model 2 incorporated age, gender, and all significant variables in Table 1; model 3 was adjusted for all variables in model 2 plus those significant in Table 2. In model 3, the indicators screened by the multivariable logistic analysis, including hypertension (P=0.001), diabetes (P=0.040), Killip grade III or IV (P<0.001), elevated heart rate (P<0.001), elevated NEUT% (P<0.001), showed both OR positive and OR value >1, suggesting these variables might be predictors of AMI patients complicated with AKI; however, elevated hemoglobin (P=0.001), elevated TNI (P=0.042), use of statins (P=0.025) showed OR values <1, suggesting that these variables might be protective factors for renal function in patients with AMI (Table 3). Compared with absolute neutrophil count, NEUT% showed a stronger predictive power.
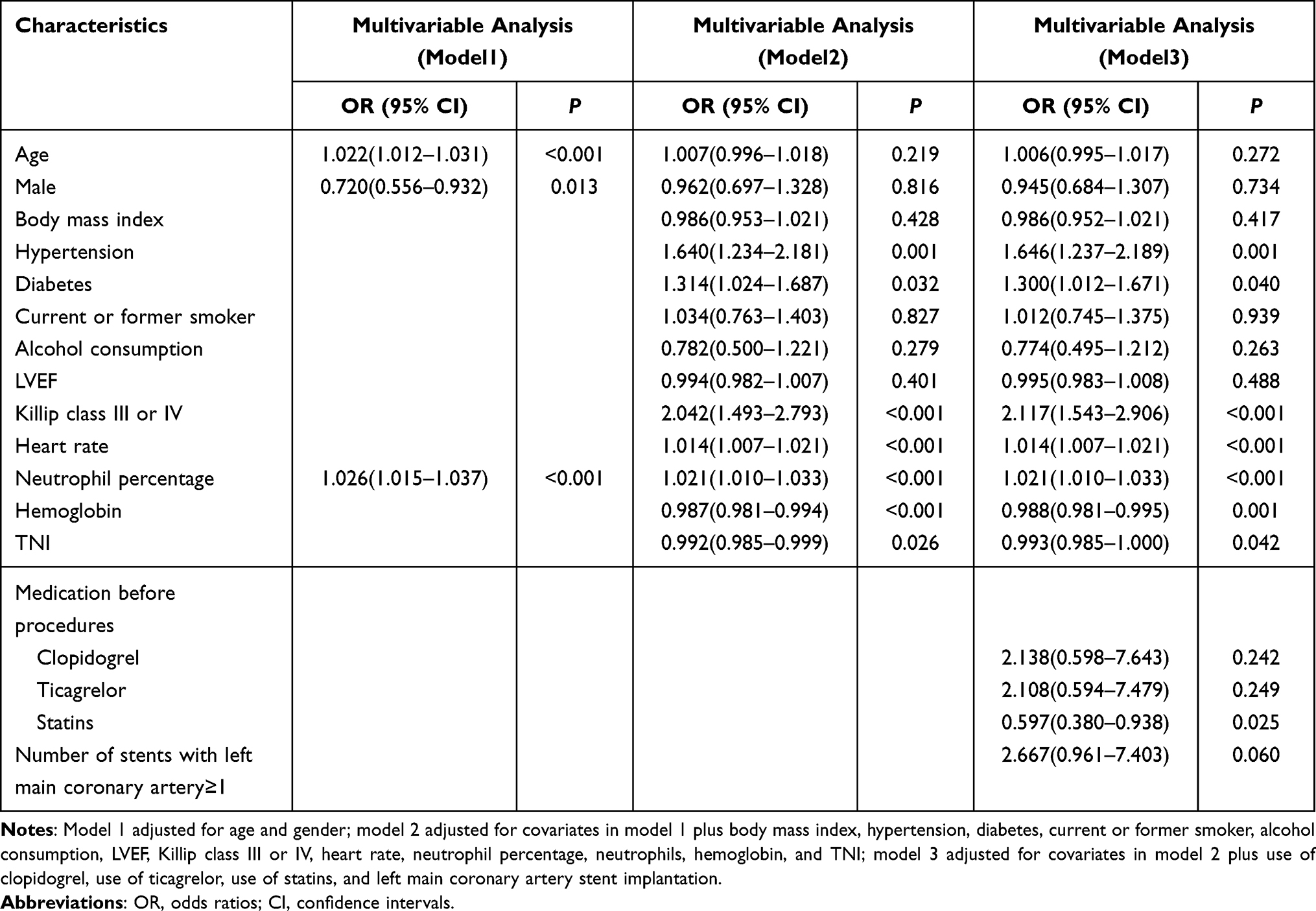 |
Table 3 Multivariable Logistic Regression Analysis of Risk of AKI in Entire Population |
The patients were divided into four quartiles of NEUT%. As shown in Table 4, a larger NEUT% was associated with a higher risk of AKI (ORunadjusted=2.18, 95% CI:1.55–3.06 for Q4 versus Q1, Ptrend < 0.001; ORmodel 3=1.90, 95% CI:1.22–2.97 for Q4 versus Q1, Ptrend=0.005). The odds of AKI increased by 29.0% when NEUT% increased by 1 SD (OR=1.290, 95% CI: 1.087–1.531, P = 0.004) after multivariable adjustment. The results of restricted cubic splines were consistent. In the low quartile, the risk of AKI remained basically unchanged, and the OR increased gradually as NEUT% increased, with a cut-off of 76.1%. (Figure 2B and C)
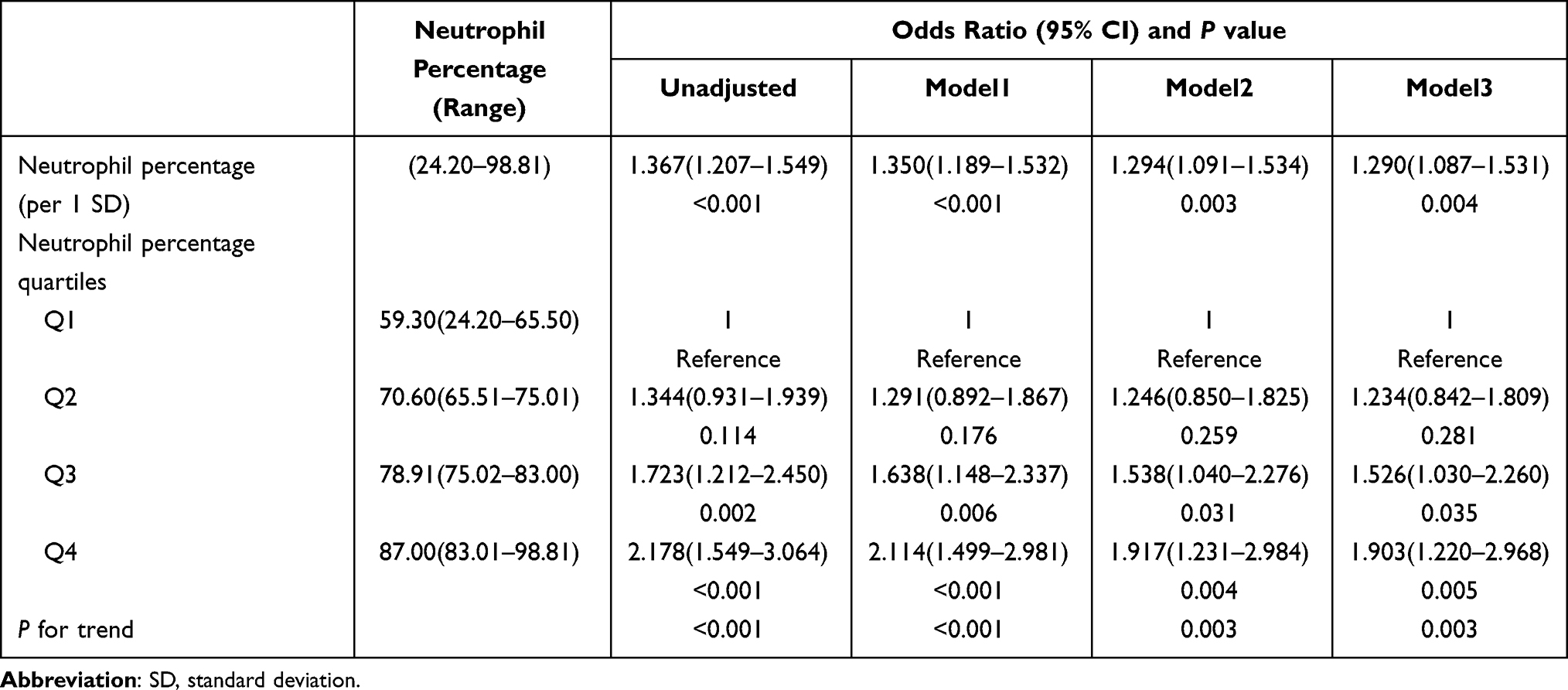 |
Table 4 Neutrophil Percentage Level and Risk of AKI in Entire Population |
After a median follow-up of 35 days, the mortality showed significant between-group difference (P<0.001), with 93 (3.10%) deaths (31 in the AKI group and 62 in the non-AKI group). As shown in the Kaplan–Meier survival analysis, AKI patients presented a higher risk of all-cause death within 1 month after AMI (Log rank: χ2=51.293, P<0.001), and patients with a larger NEUT% had a significantly worse short-term survival after AMI (Log rank: χ2 =24.753, P<0.001). The results are shown in Figure 3.
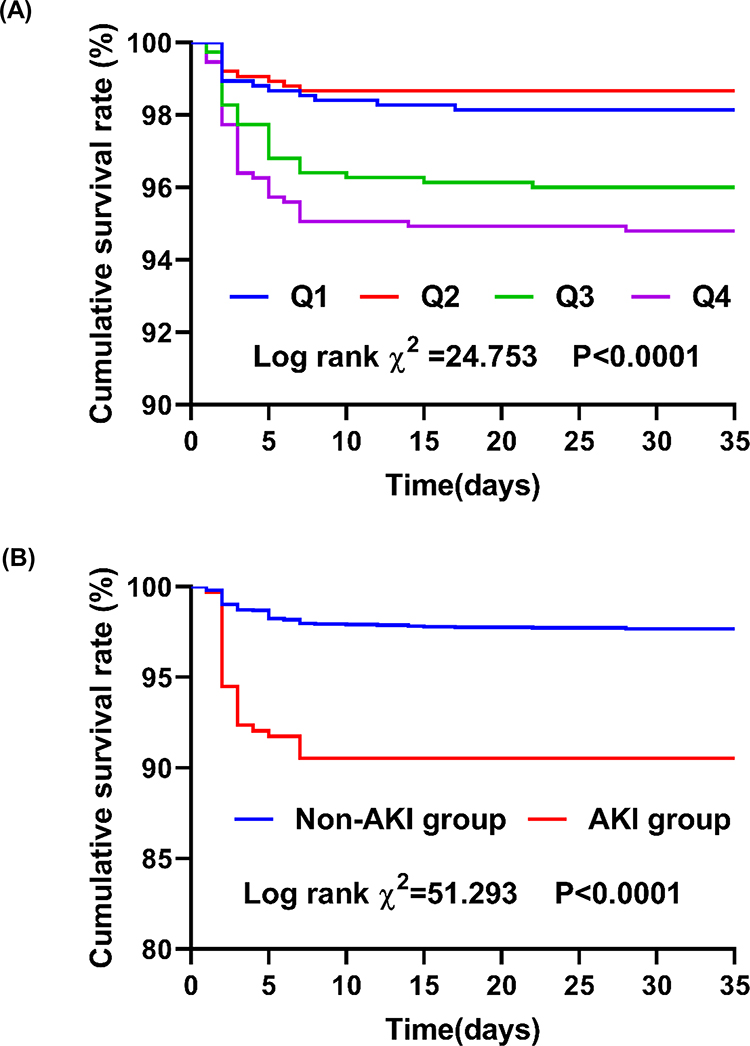 |
Figure 3 Survival analyses according to neutrophil percentage quartiles and the incidence of AKI. (A) Short-term survival rate according to neutrophil percentage quartiles (Q1 versus Q2 and Q3 and Q4); (B) Survival rate between AKI group and non-AKI group. |
In the correlation analysis, NEUT% was significantly positively correlated with heart rate (r=0.112, P<0.001) and age (r=0.075, P<0.001), and negatively correlated with BMI (r=−0.095, P<0.001), systolic blood pressure (r=−0.094, P<0.001), hemoglobin (r=−0.069, P<0.001), and LVEF (r=−0.132, P<0.001) (Figure 4).
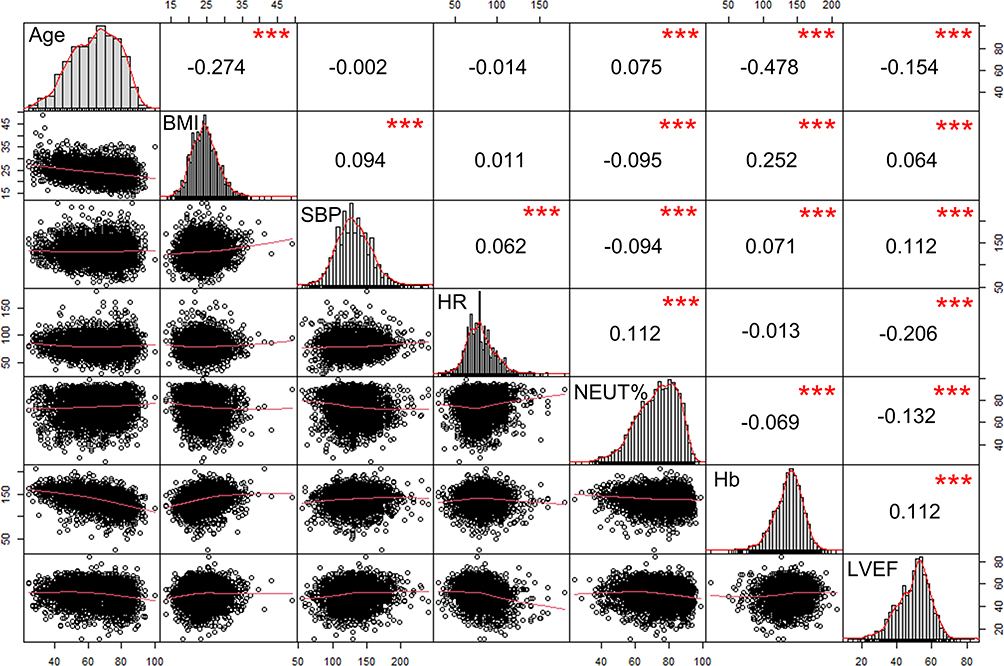 |
Figure 4 Correlation of variables in AMI patients. The diagonals show the distribution; the lower left part shows a two-variable scatter diagram with fitting lines; the upper right shows the correlation coefficient and significance level, and the numbers represent the correlation coefficient. ***P < 0.001. Abbreviations: BMI, body mass index; SBP, systolic blood pressure; HR, heart rate; NEUT%, neutrophil percentage; Hb, hemoglobin; LVEF, left ventricular ejection fraction. |
Discussion
The odds of AKI were calculated as 10.9% in AMI patients in the present study, which is broadly consistent with the results ever reported. AKI after AMI has been reported to correlate with advanced age, a history of diabetes, hypertension, lower left ventricular ejection fraction, higher level of cardiac troponin I, higher Killip grade, tachycardia, lower hemoglobin and statin free treatment.14,15 This is consistent with our conclusion. This correlation could be explained in many ways. With the increase of age, the immune defense function of the body, reserve capacity of the heart and kidneys decline. A history of serious hypertension, diabetes, and poorer cardiac and renal function may reflect renal hypoperfusion or vascular vulnerability. Our current analysis found that cardiac function had a relatively stronger impact on the occurrence of AKI, so special attention should be cast to prevent the occurrence of AKI in patients with a higher Killip grade.
Contrast medium has been widely used in imaging diagnosis and interventional therapy. Contrast medium-induced acute kidney injury (CI-AKI) has become a common concern.28 This complication can prolong hospital stay and worsen short-term and long-term prognosis. It is well known that contrast dose and exposure time are risk factors for contrast-induced AKI in the Mehran scoring system.29 In the current study, we found no significant differences in contrast dose between the two groups. This may be related to the following reasons: (1) The endpoint of the current study was not only contrast-induced AKI. In addition to contrast-induced AKI, postoperative AKI caused by various causes was recognized as the endpoint of current study. Other reasons, such as the age of enrolled patients, the complexity of coronary lesion and the baseline creatinine levels may also affect the occurrence of AKI. (2) The type and dose of contrast agent used in this study were different from those used in previous studies.
In this study, we found that increased NEUT% was a risk factor for AKI in AMI patients, and the odds of AKI increased by 29.0% with every 1 SD increase in NEUT%. To reduce the interference of confounding factors, we conducted a logistic regression analysis to better illustrate this association. The results suggested that the risk of AKI in AMI patients with NEUT% >76.1% exceeded that in those with NEUT% <76.1%. The risk of AKI in AMI patients was closely related to the prognosis of patients. Previous studies have reported the roles of some inflammatory indicators in post-AMI AKI. Neutrophil/lymphocyte ratio is associated with the severity of coronary artery disease30 and also independently associated with AKI following cardiac surgery.31,32 The elevated systemic immune inflammation index (platelet count × neutrophil/lymphocyte ratio) is correlated with a high probability of AKI in patients with ST segment elevation myocardial following primary percutaneous coronary intervention, as well as CI-AKI in patients who have undergone coronary angiography.33,34 In a prospective multicenter cohort and some other studies, neutrophils, neutrophil-to-lymphocyte ratio, and high-sensitivity C-reactive protein are closely associated with AKI occurrence and severity after an ACS.35,36 Inflammatory mediators, such as interleukin-10, interleukin-1β, interleukin-6, and endothelin-1, may be engaged in ACS-AKI.37 Neutrophil percentage-to-albumin ratio (NPAR) can independently predict the all-cause mortality in critically ill patients with AKI.23 A study of 5083 patients has demonstrated that NPAR can independently predict CI-AKI in patients without chronic kidney disease who have undergone elective PCI.38 Elevated neutrophil count post-AMI strongly, positively and independently correlated with heart failure and death.39,40
Neutrophils, produced in the bone marrow, have been considered as the short-lived phagocytes.41,42 AMI is a substantial sterile injury. Neutrophils, as the main effector cells in the inflammatory cascade, are recruited to construct the first line of defense against sterile inflammation; this process is mediated by the release of danger signals or damage associated molecular patterns (DAMPs) from necrotic cells and tissues.43 As neutrophils and macrophages infiltrate the infarcted myocardium in cardiac tissue following AMI, two major DAMPs, S100A8 and S100A9, increase their levels and bind to the Toll Like Receptor 4 and prime the Nod Like Receptor Family Pyrin Domain-Containing 3 inflammasome to release interleukin 1 (IL-1β).44 IL-1β then interacts with myeloid progenitor cells in the bone marrow to stimulates granulopoiesis.45 This initiates a positive feedback loop. Inflammasome activation in neutrophils leads to cleavage of Gasdermin D, which is widely expressed in different subsets of leukocytes, and then induces the release of IL-1β, eventuating in pyroptosis or neutrophil extracellular trap formation (NETosis).17,46,47 Platelets, perivascular macrophages and mast cells offer contributions to neutrophil recruitment in vivo.48,49 Platelets release granules containing numerous mediators, including platelet activating factor, adhesion molecules and chemokines and 5-hydroxyindoleacetic acid. On the other hand, ischemic injury rapidly mobilizes neutrophils from the splenic reserve to peripheral blood through the extracellular vesicles-dependent mechanism, explaining that the rise in blood neutrophil counts in humans precedes chemokine elevation.48 During ischemia reperfusion injury of kidney, the necrosis of tubular epithelial cells induces the release of DAMPs and NETosis that intensifies inflammation, oxidative stress, and coagulopathy in whole body organs.50,51 At the same time, in animal experiments, neutrophils demonstrate temporal heterogeneity, which is different from that in circulation, in inflammatory target organs, and this further reprogramming enhances inflammatory capacity.52,53 The effects of neutrophils on tissue repair and injury deserve further studies.
Limitations
We did not measure NEUT% levels continuously and dynamically during hospitalization. Besides, we did not use urine volume as one of the diagnostic indicators to improve the sensitivity of diagnosis, which may have let us misclassify some patients. Meanwhile, we did not collect more markers of inflammation such as C-reactive protein and interleukin-6 to refine our experimental results. A prospective, multicenter, larger-size and long-term follow-up study should be conducted to validate the prognostic value of NEUT% on post-AMI AKI.
Conclusion
In AMI patients, a high peripheral blood NEUT% was associated with the occurrence of AKI and short-term all-cause mortality. This index may provide physicians with more information about disease development and prognosis.
Funding
This study was supported by National Natural Science Foundation of China (Grant No.82270328), Natural Science Foundation of Jiangsu Province (BK20221229), China Postdoctoral Science Funding Program (2022M720544), Changzhou High-Level Medical Talents Training Project (2022CZBJ054, 2022CZBJ053), the Technology Development Fund of Nanjing Medical University (NMUB2020069), Major Research plan of Changzhou Health Commission of Jiangsu Province of China (ZD202215), Changzhou Sci&Tech Program (CE20225051). Major Research plan of Wannan Medical College (WK2022F19) and Major Research plan of Anhui Education Commission (KJ2021A0822).
Disclosure
The authors declare no competing interests in this work.
References
1. Roth GA, Mensah GA, Johnson CO, et al. Global burden of cardiovascular diseases and risk factors, 1990–2019: update From the GBD 2019 Study. J Am Coll Cardiol. 2020;76(25):2982–3021. doi:10.1016/j.jacc.2020.11.010
2. Zhou M, Wang H, Zeng X, et al. Mortality, morbidity, and risk factors in China and its provinces, 1990–2017: a systematic analysis for the Global Burden of Disease Study 2017. Lancet. 2019;394(10204):1145–1158. doi:10.1016/S0140-6736(19)30427-1
3. Hoste EAJ, Kellum JA, Selby NM, et al. Global epidemiology and outcomes of acute kidney injury. Nat Rev Nephrol. 2018;14(10):607–625. doi:10.1038/s41581-018-0052-0
4. Wang C, Pei YY, Ma YH, et al. Risk factors for acute kidney injury in patients with acute myocardial infarction. Chinese Med J. 2019;132(14):1660–1665. doi:10.1097/CM9.0000000000000293
5. Wilhelm-Leen E, Montez-Rath ME, Chertow G. Estimating the risk of radiocontrast-associated nephropathy. J Am Soc Nephrol. 2017;28(2):653–659. doi:10.1681/ASN.2016010021
6. Parikh CR, Coca SG, Wang Y, Masoudi FA, Krumholz HM. Long-term prognosis of acute kidney injury after acute myocardial infarction. Archives of Int Med. 2008;168(9):987–995. doi:10.1001/archinte.168.9.987
7. Amin AP, Salisbury AC, McCullough PA, et al. Trends in the incidence of acute kidney injury in patients hospitalized with acute myocardial infarction. Archives of Int Med. 2012;172(3):246–253. doi:10.1001/archinternmed.2011.1202
8. Pickering JW, Blunt IRH, Than MP. Acute kidney injury and mortality prognosis in acute coronary syndrome patients: a meta-analysis. Nephrology. 2018;23(3):237–246. doi:10.1111/nep.12984
9. Giacoppo D, Madhavan MV, Baber U, et al. Impact of contrast-induced acute kidney injury after percutaneous coronary intervention on short- and long-term outcomes: pooled analysis from the HORIZONS-AMI and ACUITY trials. Circulation. 2015;8(8):e002475. doi:10.1161/CIRCINTERVENTIONS.114.002475
10. Ronco C, McCullough P, Anker SD, et al. Cardio-renal syndromes: report from the consensus conference of the acute dialysis quality initiative. Eur Heart J. 2010;31(6):703–711. doi:10.1093/eurheartj/ehp507
11. Bonavia A, Singbartl K. A review of the role of immune cells in acute kidney injury. Pediatr Nephrol. 2018;33(10):1629–1639. doi:10.1007/s00467-017-3774-5
12. Ridker PM, Everett BM, Thuren T, et al. Antiinflammatory therapy with canakinumab for atherosclerotic disease. New Engl J Med. 2017;377(12):1119–1131. doi:10.1056/NEJMoa1707914
13. Akcay A, Nguyen Q, Edelstein CL. Mediators of inflammation in acute kidney injury. Media Inflamm. 2009;2009:137072. doi:10.1155/2009/137072
14. Maksimczuk J, Galas A, Krzesiński P. What promotes acute kidney injury in patients with myocardial infarction and multivessel coronary artery disease-contrast media, hydration status or something else? Nutrients. 2022;15(1). doi:10.3390/nu15010021
15. Xu FB, Cheng H, Yue T, Ye N, Zhang HJ, Chen YP. Derivation and validation of a prediction score for acute kidney injury secondary to acute myocardial infarction in Chinese patients. BMC Nephrol. 2019;20(1):195. doi:10.1186/s12882-019-1379-x
16. Sun L, Zhu W, Ji Y, et al. Association of plasma free triiodothyronine levels with contrast-induced acute kidney injury and short-term survival in patients with acute myocardial infarction. Endocr Connect. 2022;11(7). doi:10.1530/EC-22-0120
17. Jiang K, Tu Z, Chen K, et al. Gasdermin D inhibition confers antineutrophil-mediated cardioprotection in acute myocardial infarction. J Clin Invest. 2022;132(1). doi:10.1172/JCI151268
18. Frangogiannis NG. The inflammatory response in myocardial injury, repair, and remodelling. Nat Rev Cardiol. 2014;11(5):255–265. doi:10.1038/nrcardio.2014.28
19. Cui H, Ding X, Li W, Chen H, Li H. The neutrophil percentage to albumin ratio as a new predictor of in-hospital mortality in patients with ST-segment elevation myocardial infarction. Med Sci Monit. 2019;25:7845–7852. doi:10.12659/MSM.917987
20. Cai J, Li M, Wang W, Luo R, Zhang Z, Liu H. The relationship between the neutrophil percentage-to-albumin ratio and rates of 28-day mortality in atrial fibrillation patients 80 years of age or older. J Inflamm Res. 2023;16:1629–1638. doi:10.2147/JIR.S400924
21. Wang X, Zhang Y, Wang Y, et al. The neutrophil percentage-to-albumin ratio is associated with all-cause mortality in patients with chronic heart failure. BMC Cardiovasc Disorders. 2023;23(1):568. doi:10.1186/s12872-023-03472-9
22. Yu Y, Liu Y, Ling X, et al. The neutrophil percentage-to-albumin ratio as a new predictor of all-cause mortality in patients with cardiogenic shock. Biomed Res. Int. 2020;2020:7458451. doi:10.1155/2020/7458451
23. Wang B, Li D, Cheng B, Ying B, Gong Y. The neutrophil percentage-to-albumin ratio is associated with all-cause mortality in critically ill patients with acute kidney injury. Biomed Res. Int. 2020;2020:5687672. doi:10.1155/2020/5687672
24. Pan W, Zhao D, Zhang C, et al. Application of neutrophil/lymphocyte ratio in predicting coronary blood flow and mortality in patients with ST-elevation myocardial infarction undergoing percutaneous coronary intervention. J Cardiol. 2015;66(1):9–14. doi:10.1016/j.jjcc.2014.10.014
25. Ren F, Mu N, Zhang X, et al. Increased platelet-leukocyte aggregates are associated with myocardial no-reflow in patients with ST elevation myocardial infarction. Am J Med Sci. 2016;352(3):261–266. doi:10.1016/j.amjms.2016.05.034
26. Thygesen K, Alpert JS, Jaffe AS, et al. Third universal definition of myocardial infarction. J Am Coll Cardiol. 2012;60(16):1581–1598. doi:10.1016/j.jacc.2012.08.001
27. Stevens PE, Levin A. Evaluation and management of chronic kidney disease: synopsis of the kidney disease: improving global outcomes 2012 clinical practice guideline. Ann Internal Med. 2013;158(11):825–830. doi:10.7326/0003-4819-158-11-201306040-00007
28. Lakhal K, Robert-Edan V, Ehrmann S. In the name of contrast-induced acute kidney injury. Chest. 2020;157(4):751–752. doi:10.1016/j.chest.2019.12.009
29. Mehran R, Aymong ED, Nikolsky E, et al. A simple risk score for prediction of contrast-induced nephropathy after percutaneous coronary intervention: development and initial validation. J Am Coll Cardiol. 2004;44(7):1393–1399. doi:10.1016/j.jacc.2004.06.068
30. Du J, Deng S, Du J. The neutrophil/lymphocyte ratio is associated with different stages of development of coronary artery disease. Cardiovasc Innov Appl. 2022;7(1). doi:10.15212/CVIA.2022.0018
31. Weedle RC, Da Costa M, Veerasingam D, Soo AWS. The use of neutrophil lymphocyte ratio to predict complications post cardiac surgery. Ann Translat Med. 2019;7(23):778. doi:10.21037/atm.2019.11.17
32. Wheatley J, Liu Z, Loth J, et al. The prognostic value of elevated neutrophil-lymphocyte ratio for cardiac surgery-associated acute kidney injury: a systematic review and meta-analysis. Acta Anaesthesiol Scandinavica. 2023;67(2):131–141. doi:10.1111/aas.14170
33. Öcal L, Keskin M, Cerşit S, et al. Systemic immune-inflammation index predicts in-hospital and long-term outcomes in patients with ST-segment elevation myocardial infarction. Coronary Artery Disease. 2022;33(4):251–260. doi:10.1097/MCA.0000000000001117
34. Lai W, Zhao X, Huang Z, et al. Elevation of preprocedural systemic immune inflammation level increases the risk of contrast-associated acute kidney injury following coronary angiography: a multicenter cohort study. J Inflamm Res. 2022;15:2959–2969. doi:10.2147/JIR.S364915
35. Rossi VA, Denegri A, Candreva A, et al. Prognostic value of inflammatory biomarkers and GRACE score for cardiac death and acute kidney injury after acute coronary syndromes. Eur Heart J Acute Cardiovasc Care. 2021;10(4):445–452. doi:10.1093/ehjacc/zuab003
36. Yuan Y, Qiu H, Hu X, et al. Predictive value of inflammatory factors on contrast-induced acute kidney injury in patients who underwent an emergency percutaneous coronary intervention. Clin Cardiol. 2017;40(9):719–725. doi:10.1002/clc.22722
37. Ortega-Hernández J, Springall R, Sánchez-Muñoz F, Arana-Martinez JC, González-Pacheco H, Bojalil R. Acute coronary syndrome and acute kidney injury: role of inflammation in worsening renal function. BMC Cardiovasc Disorders. 2017;17(1):202. doi:10.1186/s12872-017-0640-0
38. He HM, Zhang SC, He C, et al. Association between neutrophil percentage-to-albumin ratio and contrast-associated acute kidney injury in patients without chronic kidney disease undergoing percutaneous coronary intervention. J Cardiol. 2022;79(2):257–264. doi:10.1016/j.jjcc.2021.09.004
39. Kong T, Kim TH, Park YS, et al. Usefulness of the delta neutrophil index to predict 30-day mortality in patients with ST segment elevation myocardial infarction. Sci Rep. 2017;7(1):15718. doi:10.1038/s41598-017-15878-5
40. Arruda-Olson AM, Reeder GS, Bell MR, Weston SA, Roger VL. Neutrophilia predicts death and heart failure after myocardial infarction: a community-based study. Circ Cardiovasc Qual Outcomes. 2009;2(6):656–662. doi:10.1161/CIRCOUTCOMES.108.831024
41. Ballesteros I, Rubio-Ponce A, Genua M, et al. Co-option of neutrophil fates by tissue environments. Cell. 2020;183(5):1282–97.e18. doi:10.1016/j.cell.2020.10.003
42. Malech HL, DeLeo FR, Quinn MT. The role of neutrophils in the immune system: an overview. Methods Mol Biol. 2020;2087:3–10.
43. Pittman K, Kubes P. Damage-associated molecular patterns control neutrophil recruitment. J Innate Immun. 2013;5(4):315–323. doi:10.1159/000347132
44. Toldo S, Abbate A. The NLRP3 inflammasome in acute myocardial infarction. Nat Rev Cardiol. 2018;15(4):203–214. doi:10.1038/nrcardio.2017.161
45. Sreejit G, Abdel-Latif A, Athmanathan B, et al. Neutrophil-Derived S100A8/A9 Amplify Granulopoiesis After Myocardial Infarction. Circulation. 2020;141(13):1080–1094. doi:10.1161/CIRCULATIONAHA.119.043833
46. Tall AR, Westerterp M. Inflammasomes, neutrophil extracellular traps, and cholesterol. J Lipid Res. 2019;60(4):721–727. doi:10.1194/jlr.S091280
47. De Giovanni M, Tam H, Valet C, Xu Y, Looney MR, Cyster JG. GPR35 promotes neutrophil recruitment in response to serotonin metabolite 5-HIAA. Cell. 2022;185(5):815–30.e19. doi:10.1016/j.cell.2022.01.010
48. Maas SL, Soehnlein O, Viola JR. Organ-specific mechanisms of transendothelial neutrophil migration in the lung, liver, kidney, and aorta. Front Immunol. 2018;9:2739. doi:10.3389/fimmu.2018.02739
49. Akbar N, Braithwaite AT, Corr EM, et al. Rapid neutrophil mobilization by VCAM-1+ endothelial cell-derived extracellular vesicles. Cardiovasc Res. 2023;119(1):236–251. doi:10.1093/cvr/cvac012
50. Nakazawa D, Kumar SV, Marschner J, et al. Histones and neutrophil extracellular traps enhance tubular necrosis and remote organ injury in ischemic AKI. J Am Soc Nephrol. 2017;28(6):1753–1768. doi:10.1681/ASN.2016080925
51. Hashemi P, Nouri-Vaskeh M, Alizadeh L, et al. NETosis in ischemic/reperfusion injuries: an organ-based review. Life Sci. 2022;290:120158. doi:10.1016/j.lfs.2021.120158
52. Vafadarnejad E, Rizzo G, Krampert L, et al. Dynamics of cardiac neutrophil diversity in murine myocardial infarction. Circ Res. 2020;127(9):e232–e49. doi:10.1161/CIRCRESAHA.120.317200
53. Shafqat A, Khan JA, Alkachem AY, et al. How neutrophils shape the immune response: reassessing their multifaceted role in health and disease. Int J Mol Sci. 2023;24(24). doi:10.3390/ijms242417583
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.