")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 20
New Therapeutic Targets and Drugs for Schizophrenia Beyond Dopamine D2 Receptor Antagonists
Authors Peng A, Chai J, Wu H, Bai B, Yang H, He W, Zhao Y
Received 16 December 2023
Accepted for publication 27 February 2024
Published 20 March 2024 Volume 2024:20 Pages 607—620
DOI https://doi.org/10.2147/NDT.S455279
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Aineng Peng,1 Jianbo Chai,2 Haiyuan Wu,1 Bing Bai,3 Huihui Yang,1 Weizhi He,1 Yonghou Zhao2
1Heilongjiang University of Chinese Medicine, Harbin, 150040, People’s Republic of China; 2Heilongjiang Mental Hospital, Harbin, 150036, People’s Republic of China; 3Tongde Hospital of Zhejiang Province, Hangzhou, 311100, People’s Republic of China
Correspondence: Yonghou Zhao, Heilongjiang Mental Hospital, 153 Hengdao Street, Harbin, Heilongjiang, 150036, People’s Republic of China, Tel +86 13904638645, Email [email protected]
Abstract: Schizophrenia is a disease with a complex pathological mechanism that is influenced by multiple genes. The study of its pathogenesis is dominated by the dopamine hypothesis, as well as other hypotheses such as the 5-hydroxytryptamine hypothesis, glutamate hypothesis, immune-inflammatory hypothesis, gene expression abnormality hypothesis, and neurodevelopmental abnormality hypothesis. The first generation of antipsychotics was developed based on dopaminergic receptor antagonism, which blocks dopamine D2 receptors in the brain to exert antipsychotic effects. The second generation of antipsychotics acts by dual blockade of 5-hydroxytryptamine and dopamine receptors. From the third generation of antipsychotics onwards, the therapeutic targets for antipsychotic schizophrenia expanded beyond D2 receptor blockade to explore D2 receptor partial agonism and the antipsychotic effects of new targets such as D3, 5-HT1A, 5-HT7, and mGlu2/3 receptors. The main advantages of the second and third generation antipsychotics over first-generation antipsychotics are the reduction of side effects and the improvement of negative symptoms, and even though third-generation antipsychotics do not directly block D2 receptors, the modulation of the dopamine transmitter system is still an important part of their antipsychotic process. According to recent research, several receptors, including 5-hydroxytryptamine, glutamate, γ-aminobutyric acid, acetylcholine receptors and norepinephrine, play a role in the development of schizophrenia. Therefore, the focus of developing new antipsychotic drugs has shifted towards agonism or inhibition of these receptors. Specifically, the development of NMDARs stimulants, GABA receptor agonists, mGlu receptor modulators, cholinergic receptor modulators, 5-HT2C receptor agonists and alpha-2 receptor modulators has become the main direction. Animal experiments have confirmed the antipsychotic effects of these drugs, but their pharmacokinetics and clinical applicability still require further exploration. Research on alternative targets for antipsychotic drugs, beyond the dopamine D2 receptor, has expanded the potential treatment options for schizophrenia and gives an important way to address the challenge of refractory schizophrenia. This article aims to provide a comprehensive overview of the research on therapeutic targets and medications for schizophrenia, offering valuable insights for both treatment and further research in this field.
Keywords: schizophrenia, target, neurotransmitter, antipsychotic drugs
Introduction
Schizophrenia is a common clinical psychiatric disorder that most often begins in youth or early adulthood, with multiple impairments in perception, thinking, emotion, cognition, behavior, and social functioning. Schizophrenia affects about 1% of the global population and has a low cure rate, often accompanied by emotional apathy and impaired social functioning, which has a significant impact on the quality of life of both patients and their families.1 According to a survey, schizophrenia caused an economic loss of $343.2 billion in the United States in 2019, which places a significant burden on the economy.2 There are metabolic syndrome complications in schizophrenia, and the side effects of antipsychotic drugs further aggravate metabolic disorders and increase cardiovascular risk in patients, and these seriously affect the quality of life and survival age of patients; therefore, there is an urgent need to find more effective and safer medications for the treatment of schizophrenia.
The Hypothesis of Abnormal Neurotransmitter Systems in Schizophrenia
A variety of neurotransmitters are involved in regulating the mental activity of the body, and abnormal functioning of neurotransmitter receptors is closely related to schizophrenia. Dopamine, glutamate, 5-hydroxytryptamine, acetylcholine, and norepinephrine are the most common neurotransmitters affecting schizophrenia. Previous research on antipsychotic drugs has primarily focused on dopamine receptor antagonists. However, in recent years, there has been a gradual increase in research on drugs that act on glutamate receptors, 5-hydroxytryptamine receptors, acetylcholine receptors and norepinephrine receptors to treat psychiatric disorders.
Dopamine
Dopamine (DA) dysregulation is a significant cause of schizophrenia. Increased striatal dopamine activity has been observed in patients with psychotic prodromal symptoms, suggesting that dopamine hyperactivity occurs before the onset of schizophrenia.3 In animal models, such as repeated administration of amphetamine and methoxymethanol acetate (MAM), dopaminergic hyperactivity was induced, and there were schizophrenic changes such as stereotyped behavior and impaired cognitive function in behavior.4 Clinical studies have found that dopamine release from cortical regions of the brain is significantly reduced in patients with schizophrenia and that DA release from the dorsolateral prefrontal cortex (DLPFC) is significantly negatively correlated with DA release from the dorsal caudate (DCA).5 Dopamine receptors include the D1 and D2 classes, the D1 class includes D1 and D5 receptors, and the D2 class includes D2, D3, and D4 receptors, of which the D2 receptors are most closely related to schizophrenia, and the dopamine hypothesis suggests increased sensitivity of postsynaptic D2 receptors in schizophrenia.6 However, in recent studies, it has been shown that D3 receptors are also one of the therapeutic targets in schizophrenia and that D3 receptor antagonists have the potential to treat both negative and cognitive symptoms of schizophrenia.7 In addition, D1 and D4 receptors have also been implicated in schizophrenia, with reduced D1 activity appearing to contribute to the pathogenesis of schizophrenia-negative symptoms, and D4 receptor-associated genes being associated with increased genetic susceptibility to schizophrenia.8
Glutamic Acid
Glutamate (Glu) is a crucial excitatory neurotransmitter in the brain and also serves as a precursor for γ-aminobutyric acid, an inhibitory neurotransmitter in the nervous system. It binds to the ionotropic receptor N-methyl-D-aspartate receptor (NMDAR) and plays a significant role in influencing neuronal signaling and nerve cell communication. The glutamatergic system interacts with the dopamine system, and frontal cortical glutamatergic activity modulates midbrain DA neurons in a process related to the alteration of DARergic discharges in the middle limbic pathway induced by inhibitory GABA interneuron signals projecting to midbrain DA neurons, in conjunction with DA signals from the PFC that can also be projected to the glutamatergic PFC neurons, affecting local glutamatergic neurotransmission.9 It is generally accepted that patients with schizophrenia suffer from a decline in the function of the NMDA receptor of the glutamate receptor, resulting in a dysregulation of the balance of the glutamatergic neurotransmitter system, as evidenced by the success of N-methyl-D-aspartate receptor (NMDAR) antagonists, such as phencyclidine (PCP) and ketamine, as commonly used drugs in the modeling of schizophrenia.10 The “disinhibition model” of NMDAR hypofunction suggests that NMDAR hypofunction results in reduced GABAergic inhibition of glutamatergic pyramidal neurons and excessive release of glutamate.11 Glutamate concentration in the human brain is a dynamic process that declines with age and varies in different brain regions. Studies on glutamate changes in schizophrenia are mixed, but most of them show that schizophrenic patients have elevated levels of glutamate in the medial prefrontal ventral cortex (including the anterior cingulate cortex), whereas the hippocampus, thalamus, occipital, temporal, and parietal lobes are among the other brain regions that showed no significant differences in glutamate levels.12–14
5-Hydroxytryptamine
Second-generation antipsychotics differ from first-generation antipsychotics in two main ways: first, they have fewer extrapyramidal side effects; second, these drugs have the ability to block not only the dopamine D2 receptor but also the 5-hydroxytryptamine (5-HT) receptor.5-hydroxytryptamine is a neurotransmitter that is widely present in the mammalian cerebral cortex and neural synapses, and its receptors are classified into seven subfamilies and fourteen receptor subtypes. Although the content of serotonin is small in human body, it plays an important role in regulating human mood, body temperature and memory. In the 5-hydroxytryptamine hypothesis, both 5-hydroxytryptaminergic dysfunction and an imbalance between 5-hydroxytryptamine and dopamine are thought to be responsible for the development of schizophrenia.15 In schizophrenic patients, the density of 5-hydroxytryptamine transporters is decreased in the frontal cortex and cingulate cortex, and the density of striatal 5-hydroxytryptamine transporters is increased.16 Studies have shown that topical application of 5-hydroxytryptamine dose-dependently increases extracellular dopamine levels in the prefrontal and striatal lobes and is more pronounced in the prefrontal lobes and that 5-hydroxytryptamine receptors, such as 5-HT1A, 5-HT2A, 5-HT1B, 5-HT2C, 5-HT4, and 5-HT6 receptors, may be involved in the regulatory process.17
Acetylcholine
Acetylcholine (ACh) is a neurotransmitter closely related to cognition, and when acetylcholine synthesis is reduced, it can cause learning, memory and recognition dysfunction. Acetylcholine has two types of receptors, nicotinic receptors as well as muscarinic receptors, and several animal experiments have shown that acetylcholine receptors play an important role in the recovery of cognitive dysfunction in schizophrenia.18 Nicotinic acetylcholine receptors bind to the endogenous neurotransmitter acetylcholine, modulate ion channels, and induce alterations in synaptic transmission, resulting in neurobiochemical and behavioral changes.19 The cholinergic hypothesis of schizophrenia suggests that the onset of schizophrenia may be related to in cholinergic dysfunction as well as a dopamine-acetylcholine imbalance, and it is generally accepted that there is a downregulation of the acetylcholine neuronal system as well as an increase in anticholinergic activity (AA) in patients with schizophrenia.20 Acetylcholinesterase inhibitors reduce the breakdown of acetylcholine by inhibiting acetylcholine esterase (AChE) and produce cholinomimetic effects, which are widely used in Alzheimer’s disease, and there have also been studies applying them to schizophrenia, which have found that the combination of acetylcholinesterase inhibitor and antipsychotics may be helpful for improving cognitive symptoms, although there are great differences in clinical practice, and the evidence is relatively weak, it also suggests that protection of acetylcholinergic function is a potential direction for the treatment of schizophrenia.21,22
Norepinephrine
Norepinephrine (NE) is synthesized and secreted by post-sympathetic ganglion neurons and adrenergic nerve endings in the brain, both as a neurotransmitter and a hormone, and its receptor types are classified as α and β. The most of the noradrenergic neurons of the brain are contained in the locus coeruleus (LC). Early evidence suggests that cerebrospinal fluid, brain, and serum norepinephrine levels are elevated in patients with SCZ that positive symptoms are consistent with hyperactivity of the NE system and that negative symptoms are consistent with hypoactivity of the NE system and that, furthermore, the locus coeruleus-norepinephrine (LC-NE) system has an effect on facilitating cognition and motivation.23 In schizophrenia, it is generally accepted that blocking α1-AR relieves positive symptoms, while blocking α2-AR improves negative and cognitive symptoms.24 In clinical trials, noradrenergic responses (eg, Task-evoked pupil dilation) have been found to be abnormal in patients with schizophrenia compared with healthy individuals, and the degree correlates with symptom severity.25 Norepinephrine and dopamine are both catecholamine transmitters, and dopamine is a precursor of norepinephrine. The functions of dopamine and norepinephrine are closely linked, and there are common targets for signaling, such as the dendritic spines of prefrontal cortical pyramidal neurons, as well as interacting intracellular hubs, such as the Akt/GSK-3β signaling pathway.26 Thus, modulation of norepinephrine levels as well as modulation of the corresponding receptors is also one of the possible pathways for the treatment of schizophrenia.
Novel Antipsychotic Drugs and Targets of Action
Antipsychotic drugs are currently the most important treatment for schizophrenia and are categorized into typical antipsychotic drugs and atypical antipsychotic drugs. Typical antipsychotics are D2 receptor antagonists, whose mechanism of action is to block the D2 receptor of dopaminergic neurons and reduce the function of the dopamine nervous system. Blockade of D2 receptors inhibits limbic dopaminergic overactivity in the midbrain and provides better control of positive symptoms, but powerful D2 receptor blockade is also responsible for side effects such as extrapyramidal disorders and hyperprolactinemia.27 Atypical antipsychotics are multi-targeted antipsychotics. Second-generation antipsychotics mainly block D2 and 5-HT2A receptors, and their blockade of D2 receptors is significantly lower than that of typical antipsychotics, the corresponding side effects are reduced, but does not weaken the antipsychotic efficacy, and it is generally believed that the modulation of the serotonin–dopamine interaction is the main mechanism by which the second-generation antipsychotics work.28 The advantages of the antipsychotic effects of D2 receptor partial agonists have been tapped since the third generation of antipsychotics. D2 receptor partial agonists (DRPAs) have high D2 receptor occupancy, but DRPAs have intrinsic D2 receptor activity lower than that of dopamine, and thus may reduce the risk of EPS while maintaining clinical efficacy, which can be of great value in minimizing antipsychotic side effects.29 At the same time, the development of D3, 5-HT1A, 5-HT7, TAAR1, mGlu2/3 receptor related agonists or antagonists is becoming more and more mature. The details are summarized in Table 1.
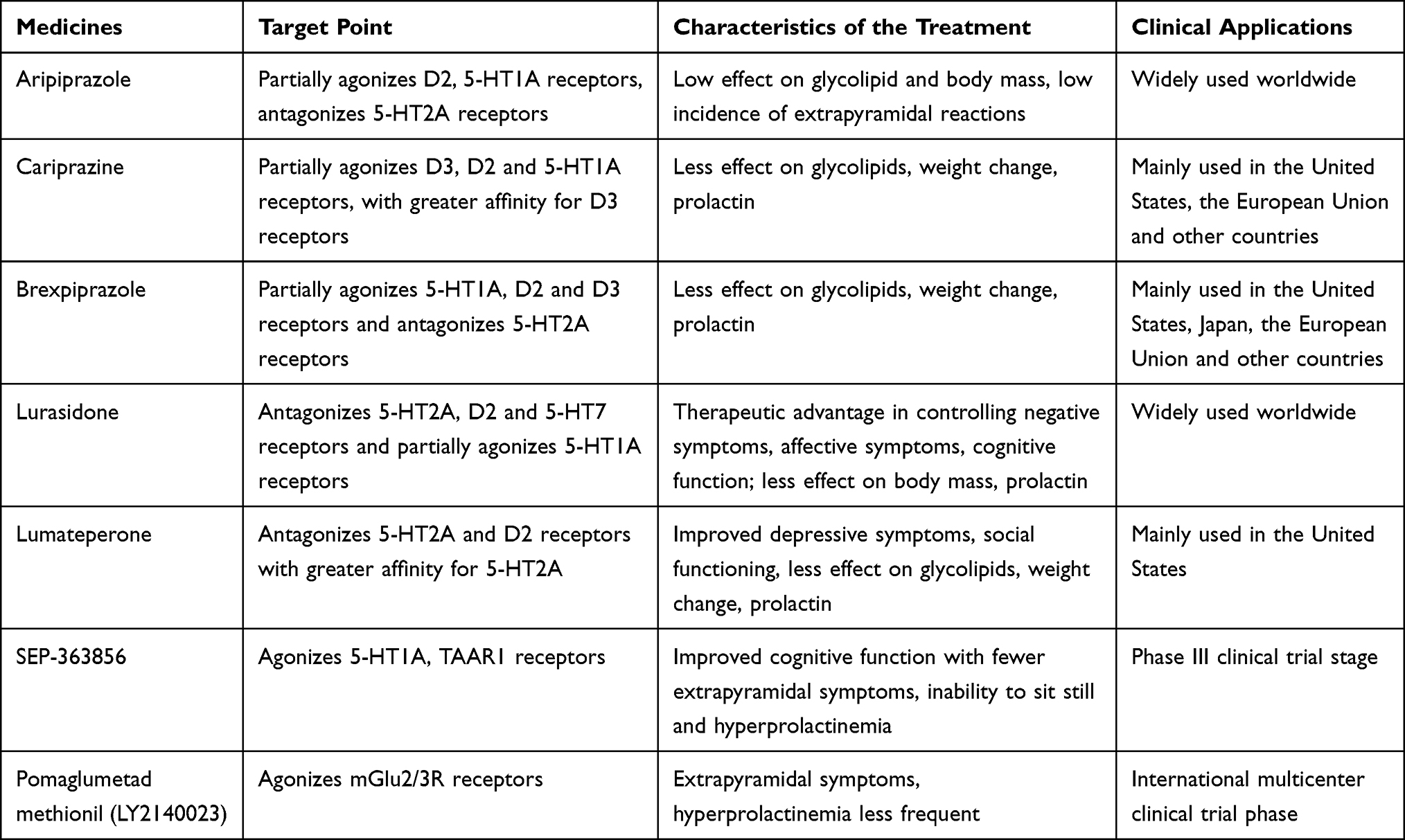 |
Table 1 Novel Antipsychotic Drug Targets and Therapeutic Characteristics |
Third-Generation Antipsychotics
Aripiprazole is a widely used third-generation antipsychotic that partially agonizes D2 receptors and 5-HT1A receptors. It has ameliorative effects on negative, positive, cognitive, and depressive symptoms.30 Cariprazine, a new atypical antipsychotic, has been approved by the US Food and Drug Administration (FDA). It is a partial agonist of dopamine D3 and 5-HT1A receptors and has a good effect on schizophrenia and bipolar disorder. Additionally, its side effects on the metabolic system and cardiovascular system are minor, making it a promising option for treatment.31 Brexpiprazole, an atypical antipsychotic, was approved for marketing in the United States in 2015. It acts as a partial agonist on 5-HT1A, D2, and D3 receptors, and has antagonistic effects on 5-HT2A, 5-HT2B, and 5-HT7 receptors, adrenergic α1A, α1B, α1D, and α2C receptors, as well as histamine H1 receptors. This multi-targeting antipsychotic is primarily used as an adjunctive treatment for schizophrenia and depression.32 Third-generation antipsychotics, currently in the promotion stage, have a wider range of receptors and act as partial agonists on the dopamine D2 receptor. They have a broader therapeutic range compared to second-generation antipsychotics and have improved safety, particularly in terms of metabolism and cardiovascular side effects. They can be used in patients with schizophrenia who are ineffective or have severe side effects of traditional antipsychotic drugs, or as adjuvant drugs of traditional antipsychotic drugs, which provide more choices for clinical use of drugs for schizophrenia.
Lurasidone
Lurasidone was approved for marketing in the United States in 2010 and is now in widespread use worldwide, mainly for the treatment of schizophrenia and bipolar disorder. It has a high affinity for dopamine D2 receptors, 5-HT2A receptors, and 5-HT7 receptors, as well as a moderate affinity for norepinephrine receptors. Several clinical trials have confirmed its clinical efficacy, and it has a low impact on body fat, metabolism, and prolactin levels.33 Common adverse effects of lurasidone include somnolence, nausea, akathisia, and extrapyramidal reactions. It is generally recommended to take lurasidone with dinner or at bedtime and to start with a low dose.34 Studies have shown that lurasidone has a 24-week response rate of approximately 40% in the treatment of refractory schizophrenia, additionally, it has been found to be effective in about 60% of patients who have not responded to clozapine therapy.35 As a new antipsychotic, lurasidone offers promising clinical prospects for patients who are intolerant of antipsychotic metabolism and hyperprolactinemia. It also serves as a viable option for patients with refractory schizophrenia who do not respond to commonly used antipsychotics like olanzapine, risperidone, clozapine, and others.
Lumateperone
Lumateperone was approved by the FDA for the treatment of schizophrenia in the United States in 2019. Its main mechanism of action is related to the modulation of dopamine, 5-hydroxytryptamine, and glutamate neurotransmitter functions. It acts as an antagonist for the 5-HT2A and D2 receptors, with a higher affinity for 5-HT2A receptors.36 Animal experiments have confirmed that lumateperone enhances NMDA and AMPA receptor-mediated neurotransmission in the medial prefrontal cortex (mPFC), promotes dopamine and glutamate release from the mPFC in rats, and significantly inhibits the conditioned avoidance response (CAR) in rats, which has an antipsychotic effect.37 It was found that lumateperone’s improvement of psychiatric symptoms is also correlated with immune-inflammatory response, reducing the levels of pro-inflammatory cytokines IL-1b, IL-6 and TNF-a in the brain and serum of immune-stressed mice.38 The safety and efficacy of lumateperone in treating schizophrenia are continuously being explored. The available studies have found that lumateperone has a better effect on improving schizophrenia symptoms compared to second-generation antipsychotics like risperidone, additionally, lumateperone has fewer extravertebral side effects and fewer effects on blood lipids, body weight, and prolactin.39–41 However, it is important to note that studies have also shown that lumateperone increases the risk of death in patients with dementia-related psychiatric disorders. Therefore, lumateperone is contraindicated in patients with dementia-related psychiatric disorders.42
Sep-363856
SEP-363856 was granted breakthrough therapy designation for the treatment of schizophrenia by the US FDA in 2019 and is currently in Phase III clinical trials in multiple countries. SEP-363856 acts on the trace amine-associated receptor 1 (TAAR1) and 5-hydroxytryptamine type 1A (5-HT1a) receptors and has little to no effect on the dopamine D2 receptor. In animal experiments, SEP-363856 reached the maximum blood concentration within 0.25 to 0.5 hours and penetrated into the brain after oral administration, and it could still be detected in plasma and brain 8 hours after administration. After cross oral and intravenous administration, the oral bioavailability in rats and monkeys were 58–120% and 71%, respectively, showing good brain permeability and bioavailability.43 In clinical trials involving patients with schizophrenia, SEP-363856 was rapidly absorbed and cleared. It reached its maximum blood concentration in 2.8 hours and had an effective half-life of 7 hours. The blood concentration of SEP-363856 reached a steady state before and after the third dose, and it was essentially cleared from the body within 48 hours after discontinuing the dose.44 A clinical randomized controlled trial of SEP-363856 for the treatment of acute exacerbation of schizophrenia across five countries in Eastern Europe and North America with 34 clinical sites was found to significantly reduce PANSS scores in patients with acute exacerbation of schizophrenia, and in terms of adverse effects, the main ones were somnolence and gastrointestinal symptoms, with minimal effect on prolactin, which is consistent with the fact that SEP −363856 did not bind to D2 receptors, and therapeutically, SEP-363856 is more inclined to alleviate negative symptoms, which needs to be further investigated.45 The target of action of SEP-363856 is distinguished from the D2 receptors and 5HT2A receptors that were acted upon by previous antipsychotics, but it mainly acts on TAAR1 and 5-HT1a receptors. The dopamine D2 receptor blockade is important in alleviating positive symptoms of schizophrenia; however, D2 receptor blockade also has effects on the downstream of dopamine pathway, affecting motor, endocrine, and cardiac function, SEP-363856 makes up for these deficiencies and is of great significance in exploring the improvement of negative symptoms and cognitive function of schizophrenia.
Pomaglumetad Methionil
Pomaglumetad methionil (LY2140023) is a prodrug of LY404039, an agonist of the metabotropic glutamate 2/3 receptor (mGlu2/3R). LY2140023 selectively acts on the mGlu2/3 receptor to exert its antipsychotic effects. Currently, an international multicenter clinical trial is underway for this drug. In an adolescent rat model of MAM schizophrenia, LY2140023 treatment significantly reduced the firing frequency of pyramidal neurons in the ventral hippocampal (vHPC) region, and a certain dose of LY2140023 treatment was able to increase the discrimination index of rats with MAM schizophrenia model (novel-familiar)/(novel+familiar).46,47 The low oral utilization of LY404039 resulted in the development of LY2140023. In pharmacokinetic studies, when LY2140023 was administered orally, the blood concentration–time curve indicated a rapid absorption phase with a median Tmax of 4h and elimination was rapid, with a mean t1/2 of 1.86 h, the median Tmax at the end of the IV infusion was 1.98 h, the mean T1/2 for the active fraction was slightly faster after IV administration compared to oral administration.48 In the Phase II clinical trial, 40 mg of LY2140023 was administered twice daily for 4 weeks, which resulted in a significant improvement in the total PANSS score as well as other outcome measures such as the Clinical Global Impression-Severity (CGI-S) score and the PANSS positive and negative sub-scores, with no increase in prolactin and no signs of significant extrapyramidal side-effects, there were no clinically significant changes in vital signs, laboratory analyses, or electrocardiograms associated with treatment, and the most common adverse reactions were insomnia, mood disorders, nausea, headache, somnolence, and elevated blood creatine phosphokinase, which were generally well tolerated by patients.49 In phase III clinical trials, the rate of patients discontinuing LY2140023 due to adverse effects during treatment was significantly higher than that of aripiprazole, and the change in total PANSS score was significantly greater in the aripiprazole-treated group than in the pomaglumetad group.50 In a study of LY2140023 as an adjunct in combination with second-generation antipsychotics (aripiprazole, olanzapine, risperidone, or quetiapine) for the treatment of chronic schizophrenia, the addition of LY2140023 did not demonstrate a significant improvement in negative symptoms.51 Despite achieving better antipsychotic effects in animal experiments and clinical Phase II, pomaglumetad methionil did not meet the expected efficacy in the global clinical phase III trial. Subsequent studies revealed that LY2140023 may be more effective in specific subgroups of patients. Therefore, further in-depth studies will be conducted to maximize the effectiveness of LY2140023 and minimize its adverse effects in order to enhance its antipsychotic effect.
Potential Therapeutic Targets for Antipsychotics
The study of therapeutic targets for antipsychotic drugs is rooted in the hypothesis of neurotransmitter abnormalities in schizophrenia, and the mechanism involves inhibiting or stimulating the function of specific receptors to produce antipsychotic effects. Previous research on antipsychotic drugs has primarily focused on dopamine; however, some patients treated with dopamine antagonists may develop dopamine supersensitivity, leading to decreased effectiveness of the treatment. The blockade of dopamine receptors can cause extravertebral systemic reactions, metabolic abnormalities, and hyperprolactinemia. Therefore, researchers have focused on developing new antipsychotic drug targets that are not dopamine D2 receptors, and several studies have been conducted to confirm the effectiveness of these alternative neurotransmitter receptors for antipsychotic treatment. These studies have shown promising results, indicating the feasibility of these targets for antipsychotic effects. The details are summarized in Table 2.
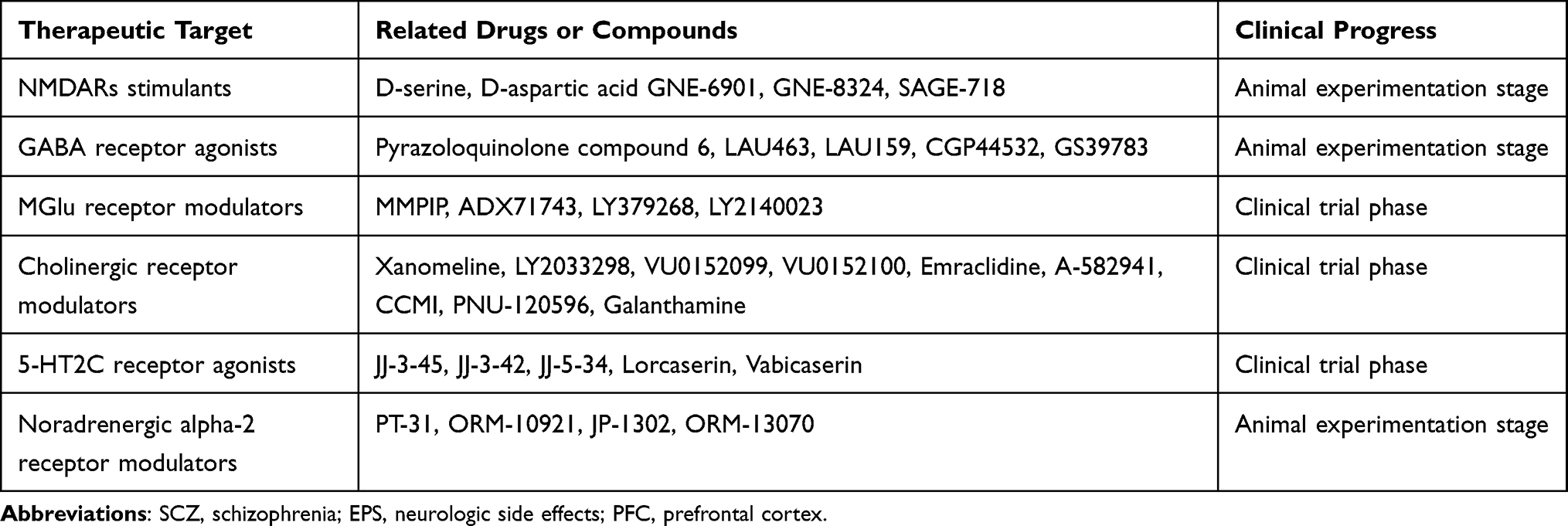 |
Table 2 Potential Therapeutic Targets and Related Drugs |
NMDARs Stimulants
N-methyl-D-aspartate receptor (NMDAR) dysfunction and excitatory/inhibitory (E/I) imbalance are important pathomechanisms in schizophrenia. NMDAR antagonists can induce behavioral and neurobiological changes similar to those in schizophrenia by interfering with NMDA signaling, and the use of NMDAR antagonists in nonhuman primates and rodents has induced a variety of schizophrenia like behaviors such as sensorimotor gating deficits, repetitive movements, and cognitive and social deficits.3 NMDAR agonists, such as D-serine and D-aspartate, modulate metabotropic glutamate receptors and dopaminergic neurons in the brain. In experiments with schizophrenic mice, D-aspartate supplementation attenuated the prepulse inhibition deficits induced by amphetamine and MK-801.52 In clinical studies, D-serine was used as an adjunctive medication in antischizophrenia, contributing to elevated serum serine levels and improvements in negative, positive, cognitive, and depressive symptoms.53 Selective NMDAR positive-altering modulators (PAMs), such as GNE-6901 and GNE-8324, have dose-dependent potentiation of NMDAR activation, but their pharmacokinetic deficiencies make them difficult to implement in the clinic at the present time.54 SAGE-718 is also a novel NMDA receptor positive-altering modulator, and it has been demonstrated in animal experiments that SAGE-718 has an equipotent potentiation of NMDAR in striatal medium spiny neurons GluN1/GluN2A-D, improves dysfunctions caused by NMDAR hypofunction, including deficits in social interactions due to subchronic administration of PCP and behavioral and electrophysiological dysfunctions induced by 7-dehydrocholesterol reductase (DHCR7) inhibition and is well tolerated, does not increase epileptiform activity in epilepsy models, and no signs of neurodegeneration or neurotoxicity have been observed with long-term chronic administration.55 Although research related to stimulants of NMDARs is currently at the stage of animal experiments and preclinical studies, they have demonstrated improvement of both negative and positive symptoms of schizophrenia and cognitive functioning in the current study, which warrants further exploration.
GABA Receptor Agonists
Gamma-aminobutyric acid (GABA) is an important inhibitory neurotransmitter found in neural tissues. Schizophrenia is associated with GABAergic dysfunction. It is generally believed that schizophrenia patients have weakened function of GABA, a central nervous inhibitory neurotransmitter, and hyperglutamatergic activity, which promotes the onset of psychotic symptoms. GABA receptors are divided into three types: GABAA, GABAB, and GABAC. Their functions are closely related to the opening of ion channels in cell membranes, neuronal inhibition, and synaptic conduction, and the research on antipsychotics based on the target of GABA receptors has made preliminary progress. According to the γ-aminobutyric acid hypothesis, a defective GABAergic system is one of the causes of schizophrenia; therefore, the focus of treatment is on activating the GABAergic system, currently, research is primarily focused on GABA receptor agonists and orthosteric modulators.56 The GABAA receptor, an ionotropic receptor, is a ligand-gated ion channel. It has 19 subunits, which are classified according to α 1–6, β 1–3, γ 1–3, δ, ε, π, θ and ρ 1–3.57 Examination of cerebellar GABAergic markers in postmortem schizophrenic patients revealed significantly lower levels of GAD67, GAD65, GAT-1, mGluR2, and neuronal-type nitric oxide synthase gene expression in patients with schizophrenia relative to nonpsychiatric patients. GAD67 gene expression was found to be significantly higher in schizophrenic patients receiving atypical antipsychotic medications compared to those treated with typical antipsychotic medications. These studies suggest that GABA transmission in the cerebellar cortex is reduced in schizophrenia patients and that the type of medication may influence the level of GABA-related gene expression.58 Preclinical studies have shown that pyrazoloquinolone compound 6 and its analogs, LAU463 and LAU159, are highly selective orthosteric modulators of α6GABAAR, these compounds, along with their tritium derivatives (DK-I-56-1, DK-I-58-1, and DK-I-59-1), have been shown to rescue methamphetamine-induced PPI disruption and ameliorate hyperactivity, social withdrawal, and cognitive deficits in an animal model of schizophrenia induced by methamphetamine and PCP.59 GABAB receptors are metabotropic receptors belonging to the class C family of G-protein-coupled receptors, consisting of two subunits, GABAB1 and GABAB2. In autopsy studies of schizophrenia, the proteins of GABBR1 and GABBR2 were significantly reduced in the lateral cerebellum of patients.60 In animal experiments, the GABAB receptor activators CGP44532 and GS39783 inhibited MK-801- and amphetamine-induced hyperactivity responses, as well as DOI ((+)1-(2.5-dimethoxy-4-iodophenyl)-2-aminopropane), induced head twitching responses, suggesting that CGP44532 and GS39783 have antipsychotic effects.61 GABAC receptors were discovered later than GABAA and GABAB receptors, with fewer studies, and are mainly found in the retina and other visual pathways, as well as in the hippocampus, spinal cord, and other nervous systems.62 GABAC receptor-related functions are mainly in memory, myopia, pain, and sleep, and the GABAC receptor agonist, cis4-aminocrotonic acid (CACA, 200 lM), inhibits ammonia-induced apoptosis of rat hippocampal neurons; however, the relationship between GABAC receptors and schizophrenia has not yet been clarified.63,64 The studies on GABAA, GABAB receptor agonists, and orthosteric modulators are currently in the animal experimentation stage, and the research on pharmacology and toxicology has not been extensively conducted yet. It is clear that GABAA, GABAB receptor agonists and orthotopic modulators can improve mental symptoms and are promising targets for the treatment of schizophrenia, but the stability, safety and clinical applicability of drugs need to be further studied.
MGlu Receptor Modulators
Glutamate receptors are mainly divided into ionotropic and metabotropic receptors. Metabotropic (mGlu) receptors belong to the G protein-coupled receptors and are divided into three classes. Class I includes mGlu1 and mGlu5, Class II includes mGlu2 and mGlu3, and Class III includes mGlu4, mGlu6, mGlu7, and mGlu8. MGlu receptors are found throughout the nervous system and play a role in neural synaptic signaling and are believed to be involved in the molecular mechanisms of cognition, learning, and memory, and have been linked to schizophrenia. In a study using the DBA/2J mouse model, it was found that mGlu1 receptor antagonists increased prepulse inhibition in these mice, indicating that targeting mGlu1 receptor function could be a new treatment strategy for schizophrenia.65 The mGlu7 receptor is the most highly expressed receptor in the brain among all the mGlu receptors.66 In animal models, both the mGlu7 negative allosteric regulator MMPIP and ADX71743 inhibited MK-801-induced hyperactivity and DOI-induced head-twitching and ADX71743 showed antipsychotic activity in a social interaction test, suggesting that the mGlu7 receptor may be a potential therapeutic target for schizophrenia.67 There is an interaction between mGlu receptor and 5-HT receptor. 5-HT2a and MGlu2 receptor co-immunoprecipitate in membrane preparation, which can form isomer complex, affect synaptic signal transduction, and may participate in the antipsychotic process of clozapine and mGlu2/3 agonist LY379268, which is a possible new target for the treatment of schizophrenia.68 In mouse experiments, combining the 5-HT2A receptor antagonist M100907 with the mGlu2/3 agonist prodrug LY2140023 resulted in a reduction of MK-801-induced dopamine efflux from the NAC and significantly lowered the level of psychomotor arousal, which was more effective than administering the drugs alone.69 MGlu2/3 agonists have been recognized as potential antipsychotic drugs, and researchers have developed corresponding agents with the aim of using them in the treatment of schizophrenia. In animal experiments, it was confirmed that LY379268 was able to repair MK-801-induced deficits in a variety of clinically relevant early sensory EEG biomarkers and neuronal function, additionally, LY2140023 was found to regulate dopamine and 5-hydroxytryptamine metabolism in the central nervous system.70,71 In clinical studies, the efficacy and safety results of LY2140023 are variable and require further studies to improve, but there is a lack of clinical studies related to LY379268.72,73 Overall, many studies have confirmed the efficacy of mGlu receptor modulators as targets of antischizophrenic action in terms of animal experiments; however, further exploration is needed to determine their clinical utility.
Cholinergic Receptor Modulators
Acetylcholine is an important neurotransmitter in the nervous system that has a significant impact on the development of schizophrenia. Acetylcholine receptors are potential drug targets for the treatment of schizophrenia. Cholinergic receptors include muscarinic (M)-type receptors and nicotinic (N)-type receptors. M-type receptors include five subtypes, while N-type receptors include two subtypes. Recently, muscarinic acetylcholine receptor (mAChR) variant modulators has entered the field of clinical development in schizophrenia with corresponding results. Xanomeline, a muscarinic M1 receptor selective agonist, has been found to have significant reductions in conduct disorder, suspicion, delusions, agitation, hallucinations, and a tendency to improve cognition, but its severe gastrointestinal and cardiovascular side effects limit its clinical application.74 M4 mAChR is found in the dorsal striatum, the nucleus ambiguus, substantia nigra, and the middle limbic dopaminergic pathway, which is associated with positive symptoms of schizophrenia as well as leading to negative symptoms in schizophrenic patients. Researchers have been actively developing highly selective, CNS-penetrating M4 PAMs for the treatment of schizophrenia, and several M4 PAMs including LY2033298, VU0152099, and VU0152100 have been shown to be effective in amphetamine and apomorphine-induced psychosis models show potent antipsychotic-like efficacy, but how useful they are in humans needs to be further investigated.75 The M4 receptor-positive variant modulator, emraclidine, significantly reduced PANSS scores and CGI-S scores in schizophrenia patients in a clinical trial, with the most common adverse effects being headache, dizziness insomnia, and weight gain, and the severity of the adverse events were mild and moderate, the treatment had no significant effect on extrapyramidal symptoms and suicidal ideation or behavior, the overall safety profile was good, but its long-term effect needs to be further verified by clinical practice.76 Nicotinic (N)-type receptors are also implicated in schizophrenia. Studies have shown that the expression of α7 nicotinic acetylcholine receptor (NAChR) is reduced in patients with schizophrenia and abnormal α7-nAChR activity contributes to cognitive deficits in schizophrenia patients.77 Administration of α7nAChR agonist (A-582941) and PAMs (CCMI and PNU-120596) reduced MK-801-induced avoidance behavior and reversed its alterations at the molecular level (p-Akt/Akt, p-GSK-3β/GSK-3β, and cAMP) in rats.78 In current clinical trials, the efficacy of α-7nAChR agonists or positive regulators in the treatment of schizophrenia is not ideal. For example, galantamine showed some improvement in cognitive deficits and negative and positive symptoms, but the results were not statistically significant (p > 0.05); however, when combined with cytidine 5’-diphosphorylcholine (CDP-choline), the patient’s verbal mismatch negativity (MMN) wave amplitude increased and auditory gating improved, it is hypothesized that these drugs may need to be used in combination with other drugs that have complementary mechanisms in order to achieve better antipsychotic effects.79,80
5-HT2C Receptor Agonists
Extensive research has been conducted on the role of 5-HT receptor modulators in schizophrenia. Common atypical antipsychotics such as risperidone and olanzapine, as well as newer antipsychotics like lurasidone and lumateperone, have been found to antagonize 5-HT2A receptors. On the other hand, third-generation antipsychotics like aripiprazole, cariprazine, and brexpiprazole have been shown to have a role in agonizing the 5-HT1A receptor. Studies have indicated that 5-HT2C receptors could be potential therapeutic targets for schizophrenia, and agonizing these receptors has been found to decrease dopamine levels in the nucleus accumbens and exert antipsychotic effects.81 A study analyzing the preclinical efficacy of three novel selective 5-HT2C agonists (JJ-3-45, JJ-3-42, and JJ-5-34) found that all three compounds possessed excellent brain penetration properties and showed efficacy in mice with persistent NMDAR function declining and in a hyperdopaminergic AMPH model of schizophrenia, they were effective in ameliorating schizophrenia-like behavior.82 At present, the main 5-HT2C receptor agonists studied are lorcaserin and vabicaserin. In the preclinical study, it was found that lorcaserin had the effect of reducing body mass, and vabicaserin was more effective in the treatment of acute schizophrenia, with less side effects of increased body weight and cardiovascular disease.83 The current application of 5-HT2C agonists in the field of schizophrenia is relatively small, for example, lorcaserin has been approved by the FDA primarily for assisting in weight loss or long-term weight management in overweight patients. However, subsequent studies on 5-HT2C agonists have increasingly focused on their potential in treating schizophrenia, and these studies have also indicated a promising outlook for the use of 5-HT2C agonists in schizophrenia treatment.
Noradrenergic Alpha-2 Receptor Modulators
Compared with the striatum, the density of DA transporter (DAT) in the prefrontal lobe was lower, while the density of NE transporter was higher, norepinephrine fibers were involved in the uptake/co-release of DA in mPFC, a2-adrenergic antagonists and NE reuptake inhibitors could selectively increase DA output in the prefrontal lobe.84 α 2-adrenoceptor is divided into three subtypes: α 2A, α 2B and α 2C, among which α 2A and α 2C are widely distributed in the central nervous system and more closely related to schizophrenia. α 2A is mainly distributed in the prefrontal cortex, and α 2C is mainly distributed in the striatum and hippocampus; it is generally believed that selective α 2A-AR agonists and α 2C-AR antagonists can improve the cognitive symptoms of schizophrenia.85,86 The α2A-adrenoceptor agonist PT-31 exhibits reduced prepulse inhibitory impairment and improved memory impairment in mice modeling schizophrenia without inducing catalepsy or motor impairment.87 ORM-10921, a novel α2C receptor antagonist, was found to increase extracellular dopamine levels in the prefrontal cortex in pharmacodynamic experiments, exhibit significant antidepressant and antipsychotic-like effects in the forced swimming test and prepulse-inhibition models, and increase its antipsychotic efficacy when combined with haloperidol.88,89 The α2C receptor antagonist JP-1302 reverses hyperdopaminergic activity in the striatum and improves cognitive deficits in a rat model of ketamine-induced schizophrenia.90 In rat experiments, the α2C receptor antagonist ORM-13070 ameliorated PCP-induced acute social behavioral deficits, whereas the α7nAChR partial agonist EVP-6124, as well as three atypical antipsychotics, clozapine, risperidone, and olanzapine, did not achieve this effect, reflecting a significant advantage of α2C receptor antagonism in treating the negative symptoms of social disorders in schizophrenia.91 α2A-AR agonists and α2C-AR antagonists modulate dopamine release in different parts of the brain tissue, improve negative and cognitive symptoms in schizophrenia, and can be used as adjuncts to typical antipsychotic medications or applied to schizophrenia with more severe negative symptoms.
Conclusion
The etiology of schizophrenia is diverse, and its pathogenic mechanisms are complex, as a result, progress in the development and clinical application of related drugs has been slow. This is further compounded by the low adherence and communication difficulties experienced by individuals with schizophrenia, making clinical treatment and research more challenging. In the field of medicine, there is continuous development. The first generation of antipsychotics, known for their extrapyramidal side effects and hyperprolactinemia, has gradually been phased out as first-line drugs. The second generation of antipsychotics is now the most commonly used for schizophrenia, these drugs have a wide range of clinical effects, including relieving positive symptoms such as excitement, delusion, and impulsivity, as well as having some control over negative symptoms. The average life expectancy of schizophrenics is reduced by about 15 years compared to the general population, and the relative risk of coronary heart disease in patients with schizophrenia may be twice that of the general population, which is one of the reasons for the high mortality rate.92 However, the existing antipsychotic drugs such as olanzapine, quetiapine and risperidone have different degrees of cardiovascular side effects.93 Schizophrenia is a severe and intractable mental illness, and in the late stage of treatment, there is a phenomenon of “treatment resistance”, which makes it difficult to achieve the ideal treatment effect by applying conventional treatment. Therefore, the development of new antipsychotic drugs with better therapeutic effects and fewer clinical adverse effects is particularly necessary.
At present, the direction of new antipsychotic drugs mainly focuses on new targets and multi-target combination therapy. Dopamine receptors are the main target of antipsychotic drugs in the past, and with the deepening of the understanding of schizophrenia, the drugs targeting 5-hydroxytryptamine, glutamate, acetylcholine, γ-amino butyric acid and other receptors have been gradually developed, which make up for the blanks of the treatment of the mental diseases in the past. However, due to the complexity of schizophrenia itself and the accumulation of time needed for clinical and preclinical research processes, they are still under development, and further improvement is still needed for large-scale clinical application. Currently, about the development of antipsychotic drugs other than D2 receptor antagonists has achieved certain results, such as the third generation of antipsychotics, lurasidone has been promoted globally, the safety and efficacy of which has been confirmed by a large number of clinical data, but lumateperone is not applicable to dementia-related psychiatric disorders, and SEP-363856 and LY2140023 are still in the clinical trial stage, and should be used with be used with caution to observe patient response. Regarding potential targets and drugs for schizophrenia, their existence brings more hope for the treatment of schizophrenia, but there are still some unresolved issues regarding side effects and pharmacokinetics. For example, chronic D-serine supplementation impairs insulin secretion and may increase the risk of type 2 diabetes mellitus, and lorcaserin may have a risk of heart valve disease induction.94,95 The dopamine system is still the core of schizophrenia treatment in most of the current studies, so regarding the application of antipsychotics other than the dopamine system, they are preferred to be used as an adjunct to schizophrenia treatment and as an alternative to refractory schizophrenia, in order to improve the efficacy of the schizophrenia treatment and to minimize the side effects. Overall, the development of these new antipsychotic targets and novel drugs provides a new direction for schizophrenia treatment and research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by grant from the National Natural Science Foundation of China (82374438, 81973747).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Velligan DI, Rao S. The epidemiology and global burden of schizophrenia. J Clin Psychiatry. 2023;84(1):MS21078COM5. doi:10.4088/JCP.MS21078COM5
2. Kadakia A, Catillon M, Fan Q, et al. The economic burden of schizophrenia in the United States. J Clin Psychiatry. 2022;83(6):22m14458. doi:10.4088/JCP.22m14458
3. McCutcheon RA, Krystal JH, Howes OD. Dopamine and glutamate in schizophrenia: biology, symptoms and treatment. World Psychiatry. 2020;19(1):15–33. doi:10.1002/wps.20693
4. Howes OD, Montgomery AJ, Asselin MC, et al. Elevated striatal dopamine function linked to prodromal signs of schizophrenia. Arch Gen Psychiatry. 2009;66(1):13–20. doi:10.1001/archgenpsychiatry.2008.514
5. Frankle WG, Himes M, Mason NS, et al. Prefrontal and striatal dopamine release are inversely correlated in schizophrenia. Biol Psychiatry. 2022;92(10):791–799. doi:10.1016/j.biopsych.2022.05.009
6. Beaulieu JM, Gainetdinov RR. The physiology, signaling, and pharmacology of dopamine receptors. Pharmacol Rev. 2011;63(1):182–217. doi:10.1124/pr.110.002642
7. Gross G, Wicke K, Drescher KU. Dopamine D₃ receptor antagonism--still a therapeutic option for the treatment of schizophrenia. Naunyn Schmiedebergs Arch Pharmacol. 2013;386(2):155–166. doi:10.1007/s00210-012-0806-3
8. Collo G, Mucci A, Giordano GM, et al. Negative symptoms of schizophrenia and dopaminergic transmission: translational models and perspectives opened by iPSC techniques. Front Neurosci. 2020;14:632. doi:10.3389/fnins.2020.00632
9. Buck SA, Quincy Erickson-Oberg M, Logan RW, et al. Relevance of interactions between dopamine and glutamate neurotransmission in schizophrenia. Mol Psychiatry. 2022;27(9):3583–3591. doi:10.1038/s41380-022-01649-w
10. Jorratt P, Hoschl C, Ovsepian SV. Endogenous antagonists of N-methyl-d-aspartate receptor in schizophrenia. Alzheimers Dement. 2021;17(5):888–905. doi:10.1002/alz.12244
11. Egerton A, Grace AA, Stone J, et al. Glutamate in schizophrenia: neurodevelopmental perspectives and drug development. Schizophr Res. 2020;223:59–70. doi:10.1016/j.schres.2020.09.013
12. Poels EM, Kegeles LS, Kantrowitz JT, et al. Imaging glutamate in schizophrenia: review of findings and implications for drug discovery. Mol Psychiatry. 2014;19(1):20–29. doi:10.1038/mp.2013.136
13. Chen T, Wang Y, Zhang J, et al. Abnormal concentration of GABA and glutamate in the prefrontal cortex in schizophrenia.-An in Vivo 1H-MRS study. Shanghai Arch Psychiatry. 2017;29(5):277–286. doi:10.11919/j.issn.1002-0829.217004
14. Gao F, Edden RA, Li M, et al. Edited magnetic resonance spectroscopy detects an age-related decline in brain GABA levels. Neuroimage. 2013;78:75–82. doi:10.1016/j.neuroimage.2013.04.012
15. Eggers AE. A serotonin hypothesis of schizophrenia. Med Hypotheses. 2013;80(6):791–794. doi:10.1016/j.mehy.2013.03.013
16. Abi-Dargham A. Alterations of serotonin transmission in schizophrenia. Int Rev Neurobiol. 2007;78:133–164. doi:10.1016/S0074-7742(06)78005-9
17. Iyer RN, Bradberry CW. Serotonin-mediated increase in prefrontal cortex dopamine release: pharmacological characterization. J Pharmacol Exp Ther. 1996;277(1):40–47.
18. Zhou CH, Wang ZR, Liu XL, et al. Mechanism and treatment progress of cognitive impairment in patients with schizophrenia. J Internat Psych. 2017;44(2):204–206. doi:10.13479/j.cnki.jip.2017.02.003
19. Wang CZ, Meng ML, Fei H, et al. Research progress of nicotinic acetylcholine receptor and schizophrenia. J Psychiatry. 2017;30(5):378–381. doi:10.3969/j.issn.2095-9346.2017.05.017
20. Tani M, Akashi N, Hori K, et al. Anticholinergic Activity and Schizophrenia. Neurodegener Dis. 2015;15(3):168–174. doi:10.1159/000381523
21. Santos B, González-Fraile E, Zabala A, et al. Cognitive improvement of acetylcholinesterase inhibitors in schizophrenia. J Psychopharmacol. 2018;32(11):1155–1166. doi:10.1177/0269881118805496
22. Singh J, Kour K, Jayaram MB. Acetylcholinesterase inhibitors for schizophrenia. Cochrane Database Syst Rev. 2012;1(1):CD007967. doi:10.1002/14651858.CD007967.pub2
23. Mäki-Marttunen V, Andreassen OA, Espeseth T. The role of norepinephrine in the pathophysiology of schizophrenia. Neurosci Biobehav Rev. 2020;118:298–314. doi:10.1016/j.neubiorev.2020.07.038
24. Svensson TH. Alpha-adrenoceptor modulation hypothesis of antipsychotic atypicality. Prog Neuropsychopharmacol Biol Psychiatry. 2003;27(7):1145–1158. doi:10.1016/j.pnpbp.2003.09.009
25. Pelegrino A, Guimaraes AL, Sena W, et al. Dysregulated noradrenergic response is associated with symptom severity in individuals with schizophrenia. Front Psychiatry. 2023;14:1190329. doi:10.3389/fpsyt.2023.1190329
26. Xing B, Li YC, Gao WJ. Norepinephrine versus dopamine and their interaction in modulating synaptic function in the prefrontal cortex. Brain Res. 2016;1641(Pt B):217–233. doi:10.1016/j.brainres.2016.01.005
27. Riva MA. Antipsicotici di terza generazione: focus su cariprazina [Third-generation antipsychotics: focus on cariprazine]. Riv Psichiatr. 2021;56(2):1–9. doi:10.1708/3606.35842
28. Kuroki T, Nagao N, Nakahara T. Neuropharmacology of second-generation antipsychotic drugs: a validity of the serotonin-dopamine hypothesis. Prog Brain Res. 2008;172:199–212. doi:10.1016/S0079-6123(08)00910-2
29. Keks N, Hope J, Schwartz D, et al. Comparative tolerability of dopamine D2/3 receptor partial agonists for schizophrenia. CNS Drugs. 2020;34(5):473–507. doi:10.1007/s40263-020-00718-4
30. Xu J, Yi F, Liang JS, et al. A review of the efficacy, safety and economy of aripiprazole in the treatment of schizophrenia. J Internat Psych. 2022;49(4):602–604. doi:10.13479/j.cnki.jip.2022.04.054
31. Dong XD, Zhai JG, Zhao JP, et al. Advances of the clinical application of cariprazine, a novel atypical antipsychotic drug. The Chinese J Clin Pharmacol. 2017;33(16):1601–1603. doi:10.13699/j.cnki.1001-6821.2017.16.025
32. Wang LH, Wang JB, Zhang RL. A novel atypical antipsychotic drug: brexpiprazole. Chin J New Dru Clin Rem. 2016;35(9):635–639. doi:10.14109/j.cnki.xyylc.2016.09.007
33. Wang Y, Zhan Y, Li J. Research progress of pharmacology, pharmacokinetics and clinical research of lurasidone. Chin Pharmaceut. 2020;29(24):95–98. doi:10.3969/j.issn.1006-4931.2020.24.031
34. Si TM, Zhao JP, Yu X, et al. Expert advice on clinical application of lurasidone for treatment of schizophrenia. Chin Mental Health J. 2022;36(6):457–464. doi:10.3969/j.issn.1000-6729.2022.06.001
35. Meltzer HY, Share DB, Jayathilake K, et al. Lurasidone improves psychopathology and cognition in treatment-resistant schizophrenia. J Clin Psychopharmacol. 2020;40(3):240–249. doi:10.1097/JCP.0000000000001205
36. Greenwood J, Acharya RB, Marcellus V, et al. Lumateperone: a novel antipsychotic for schizophrenia. Ann Pharmacother. 2021;55(1):98–104. doi:10.1177/1060028020936597
37. Titulaer J, Radhe O, Danielsson K, et al. Lumateperone-mediated effects on prefrontal glutamatergic receptor-mediated neurotransmission: a dopamine D1 receptor dependent mechanism. Eur Neuropsychopharmacol. 2022;62:22–35. doi:10.1016/j.euroneuro.2022.06.009
38. Dutheil S, Watson LS, Davis RE, et al. Lumateperone normalizes pathological levels of acute inflammation through important pathways known to be involved in mood regulation. J Neurosci. 2023;43(5):863–877. doi:10.1523/JNEUROSCI.0984-22.2022
39. Correll CU, Vanover KE, Davis RE, et al. Safety and tolerability of lumateperone 42 mg: an open-label antipsychotic switch study in outpatients with stable schizophrenia. Schizophr Res. 2021;228:198–205. doi:10.1016/j.schres.2020.12.006
40. Correll CU, Davis RE, Weingart M, et al. Efficacy and safety of lumateperone for treatment of schizophrenia: a randomized clinical trial. JAMA Psychiatry. 2020;77(4):349–358. doi:10.1001/jamapsychiatry.2019.4379
41. Satodiya RM, Brown VR, Njuguna SW, et al. A systematic review of clinical trials on lumateperone and its effects on body weight. J Clin Psychopharmacol. 2022;42(5):495–499. doi:10.1097/JCP.0000000000001594
42. Blair HA. Lumateperone: first Approval. Drugs. 2020;80(4):417–423. doi:10.1007/s40265-020-01271-6
43. Koblan KS, Kent J, Hopkins SC, et al. A Non-D2-receptor-binding drug for the treatment of schizophrenia. N Engl J Med. 2020;382(16):1497–1506. doi:10.1056/NEJMoa1911772
44. Dedic N, Jones PG, Hopkins SC, et al. SEP-363856, a novel psychotropic agent with a unique, Non-D2 receptor mechanism of action. J Pharmacol Exp Ther. 2019;371(1):1–14. doi:10.1124/jpet.119.260281
45. Galluppi GR, Polhamus DG, Fisher JM, et al. Population pharmacokinetic analysis of ulotaront in subjects with schizophrenia. CPT Pharmacometrics Syst Pharmacol. 2021;10(10):1245–1254. doi:10.1002/psp4.12692
46. Sonnenschein SF, Grace AA. The mGluR2/3 agonist pomaglumetad methionil normalizes aberrant dopamine neuron activity via action in the ventral hippocampus. Neuropsychopharmacol. 2020;45(12):2106–2113. doi:10.1038/s41386-020-0764-2
47. Sonnenschein SF, Grace AA. Peripubertal mGluR2/3 agonist treatment prevents hippocampal dysfunction and dopamine system hyperactivity in adulthood in MAM model of schizophrenia. Schizophr Bull. 2021;47(6):1806–1814. doi:10.1093/schbul/sbab047
48. Annes WF, Long A, Witcher JW, et al. Relative contributions of presystemic and systemic peptidases to oral exposure of a novel metabotropic glutamate 2/3 receptor agonist (LY404039) after oral administration of prodrug pomaglumetad methionil (LY2140023). J Pharm Sci. 2015;104(1):207–214. doi:10.1002/jps.24226
49. Patil ST, Zhang L, Martenyi F, et al. Activation of mGlu2/3 receptors as a new approach to treat schizophrenia: a randomized Phase 2 clinical trial. Nat Med. 2007;13(9):1102–1107. doi:10.1038/nm1632
50. Adams DH, Zhang L, Millen BA, et al. Pomaglumetad Methionil (LY2140023 Monohydrate) and aripiprazole in patients with schizophrenia: a phase 3, multicenter, double-blind comparison. Schizophr Res Treat. 2014;2014:758212. doi:10.1155/2014/758212
51. Stauffer VL, Millen BA, Andersen S, et al. Pomaglumetad methionil: no significant difference as an adjunctive treatment for patients with prominent negative symptoms of schizophrenia compared to placebo. Schizophr Res. 2013;150(2–3):434–441. doi:10.1016/j.schres.2013.08.020
52. Errico F, Rossi S, Napolitano F, et al. D-aspartate prevents corticostriatal long-term depression and attenuates schizophrenia-like symptoms induced by amphetamine and MK-801. J Neurosci. 2008;28(41):10404–10414. doi:10.1523/JNEUROSCI.1618-08.2008
53. Heresco-Levy U, Javitt DC, Ebstein R, et al. D-serine efficacy as add-on pharmacotherapy to risperidone and olanzapine for treatment-refractory schizophrenia. Biol Psychiatry. 2005;57(6):577–585. doi:10.1016/j.biopsych.2004.12.037
54. Hackos DH, Lupardus PJ, Grand T, et al. Positive allosteric modulators of GluN2A-Containing NMDARs with distinct modes of action and impacts on circuit function. Neuron. 2016;89(5):983–999. doi:10.1016/j.neuron.2016.01.016
55. Beckley JT, Aman TK, Ackley MA, et al. Pharmacological characterization of SAGE-718, a novel positive allosteric modulator of N-methyl-d-aspartate receptors. Br J Pharmacol. 2023;9:1–23. doi:10.1111/bph.16235
56. Wassef A, Baker J, Kochan LD. GABA and schizophrenia: a review of basic science and clinical studies. J Clin Psychopharmacol. 2003;23(6):601–640. doi:10.1097/01.jcp.0000095349.32154.a5
57. Ghit A, Assal D, Al-Shami AS, et al. GABAA receptors: structure, function, pharmacology, and related disorders. J Genet Eng Biotechnol. 2021;19(1):123. doi:10.1186/s43141-021-00224-0
58. Bullock WM, Cardon K, Bustillo J, et al. Altered expression of genes involved in GABAergic transmission and neuromodulation of granule cell activity in the cerebellum of schizophrenia patients. Am J Psychiatry. 2008;165(12):1594–1603. doi:10.1176/appi.ajp.2008.07121845
59. Lee MT, Mouri A, Kubota H, et al. Targeting α6GABAA receptors as a novel therapy for schizophrenia: a proof-of-concept preclinical study using various animal models. Biomed Pharmacother. 2022;150:113022. doi:10.1016/j.biopha.2022.113022
60. Fatemi SH, Folsom TD, Thuras PD. Deficits in GABA(B) receptor system in schizophrenia and mood disorders: a postmortem study. Schizophr Res. 2011;128(1–3):37–43. doi:10.1016/j.schres.2010.12.025
61. Wierońska JM, Kusek M, Tokarski K, et al. The GABA B receptor agonist CGP44532 and the positive modulator GS39783 reverse some behavioural changes related to positive syndromes of psychosis in mice. Br J Pharmacol. 2011;163(5):1034–1047. doi:10.1111/j.1476-5381.2011.01301.x
62. Bormann J, Feigenspan A. GABAC receptors. Trends Neurosci. 1995;18(12):515–519. doi:10.1016/0166-2236(95)98370-e
63. Johnston GA, Chebib M, Hanrahan JR, et al. Neurochemicals for the investigation of GABA(C) receptors. Neurochem Res. 2010;35(12):1970–1977. doi:10.1007/s11064-010-0271-7
64. Yang L, Omori K, Omori K, et al. GABAC receptor agonist suppressed ammonia-induced apoptosis in cultured rat hippocampal neurons by restoring phosphorylated BAD level. J Neurochem. 2003;87(3):791–800. doi:10.1046/j.1471-4159.2003.02069.x
65. Hikichi H, Nishino M, Fukushima M, et al. Pharmacological effects of metabotropic glutamate receptor ligands on prepulse inhibition in DBA/2J mice. Eur J Pharmacol. 2010;639(1–3):99–105. doi:10.1016/j.ejphar.2010.03.046
66. Cieślik P, Wierońska JM. The mGlu7 receptor in schizophrenia - An update and future perspectives. Pharmacol Biochem Behav. 2022;218:173430. doi:10.1016/j.pbb.2022.173430
67. Cieślik P, Woźniak M, Kaczorowska K, et al. Negative allosteric modulators of mGlu7 receptor as putative antipsychotic drugs. Front Mol Neurosci. 2018;11:316. doi:10.3389/fnmol.2018.00316
68. Ibi D. Role of interaction of mGlu2 and 5-HT2A receptors in antipsychotic effects. Pharmacol Biochem Behav. 2022;221:173474. doi:10.1016/j.pbb.2022.173474
69. Uslaner JM, Smith SM, Huszar SL, et al. Combined administration of an mGlu2/3 receptor agonist and a 5-HT 2A receptor antagonist markedly attenuate the psychomotor-activating and neurochemical effects of psychostimulants. Psychopharmacol. 2009;206(4):641–651. doi:10.1007/s00213-009-1644-y
70. Dormann OD, Schuelert N, Rosenbrock H. Effects of the mGlu2/3 receptor agonist LY379268 on two models of disturbed auditory evoked brain oscillations in mice. Transl Psychiatry. 2023;13(1):150. doi:10.1038/s41398-023-02455-w
71. Lowe S, Dean R, Ackermann B, et al. Effects of a novel mGlu₂/₃ receptor agonist prodrug, LY2140023 monohydrate, on central monoamine turnover as determined in human and rat cerebrospinal fluid. Psychopharmacol. 2012;219(4):959–970. doi:10.1007/s00213-011-2427-9
72. Kinon BJ, Zhang L, Millen BA, et al. A multicenter, inpatient, phase 2, double-blind, placebo-controlled dose-ranging study of LY2140023 monohydrate in patients with DSM-IV schizophrenia. J Clin Psychopharmacol. 2011;31(3):349–355. doi:10.1097/JCP.0b013e318218dcd5
73. Downing AM, Kinon BJ, Millen BA, et al. A double-blind, placebo-controlled comparator study of LY2140023 monohydrate in patients with schizophrenia. BMC Psychiatry. 2014;14:351. doi:10.1186/s12888-014-0351-3
74. Mirza NR, Peters D, Sparks RG. Xanomeline and the antipsychotic potential of muscarinic receptor subtype selective agonists. CNS Drug Rev. 2003;9(2):159–186. doi:10.1111/j.1527-3458.2003.tb00247.x
75. Moran SP, Maksymetz J, Conn PJ. Targeting muscarinic acetylcholine receptors for the treatment of psychiatric and neurological disorders. Trends Pharmacol Sci. 2019;40(12):1006–1020. doi:10.1016/j.tips.2019.10.007
76. Krystal JH, Kane JM, Correll CU, et al. Emraclidine, a novel positive allosteric modulator of cholinergic M4 receptors, for the treatment of schizophrenia: a two-part, randomised, double-blind, placebo-controlled, phase 1b trial. Lancet. 2022;400(10369):2210–2220. doi:10.1016/S0140-6736(22)01990-0
77. Terry AVJ, Callahan PM. α7 nicotinic acetylcholine receptors as therapeutic targets in schizophrenia: update on animal and clinical studies and strategies for the future. Neuropharmacology. 2020;170:108053. doi:10.1016/j.neuropharm.2020.108053
78. Unal G, Bekci H, Cumaoglu A, et al. Alpha 7 nicotinic receptor agonist and positive allosteric modulators improved social and molecular deficits of MK-801 model of schizophrenia in rats. Pharmacol Biochem Behav. 2020;193:172916. doi:10.1016/j.pbb.2020.172916
79. Choueiry J, Blais CM, Shah D, et al. An α7 nAChR approach for the baseline-dependent modulation of deviance detection in schizophrenia: a pilot study assessing the combined effect of CDP-choline and galantamine. J Psychopharmacol. 2023;37(4):381–395. doi:10.1177/02698811231158903
80. Koola MM, Looney SW, Hong H, et al. Meta-analysis of randomized controlled trials of galantamine in schizophrenia: significant cognitive enhancement. Psychiatry Res. 2020;291:113285. doi:10.1016/j.psychres.2020.113285
81. Wang XQ. Potential mechanism of antischizophrenic effect of serotonin 2C receptor agonist. Southwest Univer. 2018;2018:1.
82. Pogorelov VM, Rodriguiz RM, Cheng J, et al. 5-HT2C agonists modulate schizophrenia-like behaviors in mice. Neuropsychopharmacol. 2017;42(11):2163–2177. doi:10.1038/npp.2017.52
83. Wang YW, Zhang C. Progress in 5-HT2C receptor as a therapeutic target for treatment of schizophrenia. J Shangh Jiaot Univ. 2018;38(7):801. doi:10.3969/j.issn.1674-8115.2018.07.016
84. Masana M, Bortolozzi A, Artigas F. Selective enhancement of mesocortical dopaminergic transmission by noradrenergic drugs: therapeutic opportunities in schizophrenia. Int J Neuropsychopharmacol. 2011;14(1):53–68. doi:10.1017/S1461145710000908
85. Brosda J, Jantschak F, Pertz HH. α2-Adrenoceptors are targets for antipsychotic drugs. Psychopharmacol. 2014;231(5):801–812. doi:10.1007/s00213-014-3459-8.v
86. Brocos-Mosquera I, Gabilondo AM, Diez-Alarcia R, et al. α2A- and α2C-adrenoceptor expression and functionality in postmortem prefrontal cortex of schizophrenia subjects. Eur Neuropsychopharmacol. 2021;52:3–11. doi:10.1016/j.euroneuro.2021.05.012
87. Betti AH, Antonio CB, Herzfeldt V, et al. PT-31, a putative α2-adrenoceptor agonist, is effective in schizophrenia cognitive symptoms in mice. Behav Pharmacol. 2019;30(7):574–587. doi:10.1097/FBP.0000000000000494
88. Sallinen J, Holappa J, Koivisto A, et al. Pharmacological characterisation of a structurally novel α2C-adrenoceptor antagonist ORM-10921 and its effects in neuropsychiatric models. Basic Clin Pharmacol Toxicol. 2013;113(4):239–249. doi:10.1111/bcpt.12090
89. Uys M, Shahid M, Sallinen J, et al. The α2C-adrenoceptor antagonist, ORM-10921, has antipsychotic-like effects in social isolation reared rats and bolsters the response to haloperidol. Prog Neuropsychopharmacol Biol Psychiatry. 2016;71:108–116. doi:10.1016/j.pnpbp.2016.07.002
90. Tekin N, Karamahmutoğlu TE, Aykaç A, et al. The α2C-adrenoceptor antagonist JP-1302 controls behavioral parameters, tyrosine hydroxylase activity and receptor expression in a rat model of ketamine-induced schizophrenia-like deficits. Pharmacol Biochem Behav. 2022;221:173490. doi:10.1016/j.pbb.2022.173490
91. Savolainen K, Ihalainen J, Jalkanen AJ, et al. Selective adrenergic alpha2C receptor antagonist ameliorates acute phencyclidine-induced schizophrenia-like social interaction deficits in rats. Psychopharmacol. 2019;236(4):1245–1253. doi:10.1007/s00213-018-5130-2
92. Hennekens CH, Hennekens AR, Hollar D, et al. Schizophrenia and increased risks of cardiovascular disease. Am Heart J. 2005;150(6):1115–1121. doi:10.1016/j.ahj.2005.02.007
93. Rognoni C, Bertolani A, Jommi C. Second-generation antipsychotic drugs for patients with schizophrenia: systematic literature review and meta-analysis of metabolic and cardiovascular side effects. Clin Drug Investig. 2021;41(4):303–319. doi:10.1007/s40261-021-01000-1
94. Suwandhi L, Hausmann S, Braun A, et al. Chronic d-serine supplementation impairs insulin secretion. Mol Metab. 2018;16:191–202. doi:10.1016/j.molmet.2018.07.002
95. Gorelik E, Gorelik B, Masarwa R, et al. The cardiovascular safety of antiobesity drugs-analysis of signals in the FDA adverse event report system database. Int J Obes Lond. 2020;44(5):1021–1027. doi:10.1038/s41366-020-0544-4
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.