")
Back to Journals » Journal of Pain Research » Volume 17
Nociceptive Flexion Reflex Threshold is No Suitable Marker for Diagnosing Opioid-Induced Hyperalgesia
Authors Trübenbacher L, Lindenberg N, Graf BM, Backmund M, Unglaub W, Lassen CL
Received 20 July 2023
Accepted for publication 30 January 2024
Published 14 March 2024 Volume 2024:17 Pages 1067—1076
DOI https://doi.org/10.2147/JPR.S421841
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Erica Wegrzyn
Luisa Trübenbacher,1 Nicole Lindenberg,1 Bernhard M Graf,1 Markus Backmund,2 Wilhelm Unglaub,3 Christoph L Lassen1
1Centre for Interdisciplinary Pain Medicine, Department of Anaesthesiology, University Hospital of Regensburg, Regensburg, 93053, Germany; 2“Praxiszentrum im Tal”, Tal 9, 80331, Ludwig-Maximilians-University, Munich, Germany; 3“medbo” District Hospital, Universitätsstraße 84, 93053, University of Regensburg, Regensburg, Germany
Correspondence: Luisa Trübenbacher, Department for Anaesthesiology, University Hospital of Regensburg, Franz-Josef-Strauss-Allee 11, Regensburg, 93053, Germany, Tel +49 941 944-7810, Fax +49 941 944-7832, Email [email protected]
Background: Opioid induced hyperalgesia (OIH) describes a state of altered pain sensation due to opioid exposure. It often occurs among persons with opioid use disorder receiving substitution therapy.
Methods: The purpose of this study was to find out, whether OIH diagnosis could be facilitated by an objective pain indicating marker: the Nociceptive Flexion Reflex (NFR). Forty persons with opioid use disorder, 20 of them maintained on methadone and 20 treated with buprenorphine, as well as a control group of 20 opioid-free subjects, were examined. It was aimed to find out whether and in which way these opioid agonists alter reflex threshold (NFR-T). A cold-pressor test was performed to investigate the prevalence of OIH. Furthermore, electrical stimulation and electromyography analyzation were used for NFR-T measurement. Subjective pain ratings were evaluated with a numeric rating scale.
Results: Significantly increased sensitivity to cold pressor pain was found in both maintenance groups when compared to their opioid-free counterparts (p < 0.001). Neither methadone nor buprenorphine showed any effect on NFR-T. This might be explained by the reflex approaching at the wrong location in the central nervous system. Consequently, NFR-T is not a suitable marker for diagnosing OIH.
Conclusion: Although methadone and buprenorphine have been proven to cause OIH, no effect on NFR-T was observed. A statistically significant effect could have been observed with a larger number of participants. Further research, with special focus on patients’ adjuvant medication, should be conducted in the future, to facilitate diagnosis of OIH and provide appropriate pain management for maintenance patients.
Keywords: hyperalgesia, analgesics, opioid, substance-related disorders, methadone, buprenorphine
Introduction
Despite being detected as an issue already decades ago, the phenomenon of opioid-induced hyperalgesia (OIH) remains a paradoxical occurrence, constituting a present problem in clinical everyday life. OIH names a state in which pain perception is altered because of opioid exposure.1 However, the precise mechanism underlying the origin of OIH is not completely understood. Multiple studies have shown that the neurobiological system that responds to opioids appears to increase pain sensitisation instead of providing analgesia.2 Angst and Clark described the process as neurobiologically multifactorial, meaning that liable changes are complex and concern the peripheral as well as the central nervous system.3 A multitude of studies proposes the central glutamatergic system and relating thereto the excitatory neurotransmitter N-methyl-D-aspartate (NMDA) to be involved in the development of OIH. Spinal dynorphins and descending facilitation also seem to be of great relevance in the genesis of the mentioned disease state.4 OIH is assumed to occur especially when the dosage is withdrawn or during maintenance therapy.3
Since opioid substitution therapy is the preferred treatment for persons with opioid use disorder according to international guidelines by the World Health Organisation, there is a large number of patients requiring this kind of treatment.5 In 2018, the European Monitoring Centre for Drugs and Drug addiction estimated that half of the 1.3 million high-risk opioid users in the European Union received opioid-substitution therapy.6 Pain is considered to be one of the most relevant comorbidities of opioid addiction.7 Voon et al ascertained that 40.9% of 823 inspected methadone maintained patients suffer from moderate and 11.1% from extreme pain.8 Still, diagnosis and treatment of pain syndromes often occur belated or not at all, partly because the demand for pain relief is often interpreted as drug seeking behaviour.9
Diagnosing hyperalgesia might be facilitated by resorting to objective pain-indicating parameters such as the Nociceptive Flexion Reflex (NFR), also known as withdrawal or R3 reflex. NFR is a polysynaptic, multisegmental spinal reflex. It provides withdrawal movement in the ipsilateral limb to prevent possible damage when painful stimuli are detected.10,11 The reflex is classified as an objective and reliable parameter for evaluating pain in humans.12,13 According to the guidelines of the European Federation of Neurological Societies, NFR is the nociceptive reflex that is most widely used. It is recommended as reliable for assessing the efficacy of different kinds of treatment, like, for instance, hypnosis, neurostimulation procedures or medication with opiates or NSAIDs.14 Several studies have demonstrated the impact of different drug groups on the NFR.15 It has been proven that opioids affect NFR at both spinal and supraspinal levels and significantly influence its threshold (NFR-T).11,16,17
This study involved methadone and buprenorphine, two opioid agonists commonly prescribed as maintenance treatments. Both are considered effective treatments for opioid addiction and pain as well as for detoxification.18–21
The purpose of this study was to determine whether and in which way opioids prescribed as substitution therapy change NFR-T. It was also aimed to find out if the reflex threshold is a suitable marker for the diagnosis of OIH.
Materials and Methods
This study was conducted in accordance with the current Declaration of Helsinki, and approval was obtained from the Ethics Committee of the University of Regensburg (approval number: 21–2200–101). Data containing results of the NFR-T assessment and cold pressor test (CPT) were collected from three groups. Persons with opioid use disorder maintained on methadone (MM) were compared with those treated with buprenorphine (BM). Additionally, results of both opioid-maintained groups were set against those of the opioid-free control group (CG). Parameters of interest were NFR-T, measured with the Paintracker, as well as pain tolerance and latency of pain onset, measured using the CPT. Furthermore, the potential correlation between NFR-T and pain tolerance was investigated. Subjective pain sensation associated with both assessments was also considered relevant.
Subjects
The study population consisted of 40 adult patients receiving substitution treatment (20 MM and 20 BM) as well as an opioid-free control group of 20 participants selected to match for age and sex, variables known to affect the outcome of the CPT.22 All participants in the BM and MM groups were already participating in an opioid substitution program prior to the study. Substitution treatment took place at the medical offices under observation of the attending physician. The session supervisor was aware of the participant study group during the examination.
Inclusion criteria concerning all groups contained avoiding excessive physical activity for four hours prior to testing. Participating persons with opioid use disorder had to receive stabilised treatment with a steady dosage over the last 28 days. The exclusion criterion in the control group was current opioid intake, which was determined by self-report prior to the examination and not verified by urine drug screens.
The MM group was treated with methadone hydrochloride in the form of oral Methaddict tablets. The BM cohort consisted of patients maintained on Buprenaddict, Subutex and Suboxone sublingual tablets, the effects of which were generated by buprenorphine hydrochloride. One subject received a weekly subcutaneous injection of Buvedin, which is also based on buprenorphine hydrochloride. The dosage was adapted using the conversion table of the European Medicines Agency (EMA) to make it comparable to orally administered buprenorphine.23 Apart from this exception, all subjects received daily maintenance treatment, with doses varying from patient to patient.
The procedure and its side effects were explained to each individual, and written informed consent was obtained. All participants were instructed that they would be free to withdraw at any time. After the study visit, each participant received a 25€ voucher for compensation.
Patients receiving substitution therapy were recruited via posters in a local treatment centre in Regensburg, Germany, and via information sheets issued by medical staff on site. At a general practitioner’s office in Regensburg and two medical practices in Munich, Germany, subjects were recruited personally while waiting for their medication. An opioid-free control group was invited to participate with posters at the University of Regensburg and University Hospital Regensburg as well as via word of mouth.
Experimental Procedure
Every subject attended a single session, which included NFR-T measurement, consisting of electrical stimulation combined with recording of electromyography (EMG), and afterwards the CPT. All sessions were supervised by the same individual and took place in calm examination rooms.
Paintracker
To measure NFR-T, a stimulation-recording unit for nociceptive reflexes, called Paintracker (Dolosys, Berlin, Germany; software version: 1.2.402), was used. The device provided electrical stimulation and electromyography (EMG) recordings. Each participant was examined in supine position with right leg barring. For ideally relaxed leg muscles, back support was heightened by 135° from horizontal level, and a pillow was placed under the knee joint to provide flexion of 45°. The standardised method of measuring NFR includes transcutaneous electrical stimulation of the sural nerve in the retromalleolar space and recording the signal on the skin covering the short head of the ipsilateral biceps femoris muscle.10 The skin of the subjects was prepared prior to measurement to lower the impedance between the skin and the electrode. First, grease residues were wiped off using alcoholic disinfectant; then, a skin peeling gel (Nuprep Skin Prep Gel) was applied, followed by prep tape (3M™ Red Dot™ Trace Prep) to abrade skin to improve trace quality. Cutaneous electrodes (44 × 22 mm, Ambu, BlueSensor N) were placed on degreased skin overlying the right sural nerve. Each pair of surface electrodes was attached in parallel, without spacing. A reference electrode was located on the ipsilateral knee.
As basic setting of the Paintracker 1 mA increments were set, starting with a stimulation intensity of 1 mA. As soon as the NFR was detected, the intensity was reduced in steps of 1 mA. If no reflex was detectable at this intensity, the level was raised by 1 mA, making this approach an up-down staircase method. The current was reduced to 0.5 mA after three successive increases or decreases. Trains of five pulses of 1 ms duration each were delivered by an electrical stimulator at a frequency of 200 Hz, the time interval between two stimuli was randomised. All participants rated their subjective pain perception after every stimulus, categorising it using the Numeric Rating Scale (NRS), an 11-point scale that classifies the sensation from 0 (no pain) to 10 (worst pain imaginable). After detecting the first NFR, all subjects received nine additional stimuli. The final threshold was calculated as the average value of ten authentic measurements. For each valid reflex, the amplitude was quantified using EMG. Settings adjusted in Paintracker for EMG amplification were reviewed by Dincklage et al 24 The EMG recorded 90–180ms post-stimulus was interpreted as reflex amplitude. This time frame was chosen to prevent contamination of the NFR response, which might have occurred because of the RII reflex or spontaneous movements.11,25 The NFR Interval Peak z-score was suggested as a reliable criterion for defining NFR threshold; therefore, peak biceps femoris EMG activity was evaluated using the Paintracker.26 France et al defined this standardised peak criterion as the baseline mean subtracted from the NFR interval peak response divided by the standard deviation of the baseline.27 The cut-off value for the interval peak z-score, above which a reflex was rated as authentic, was set at 6.085.
Cold Pressor Test
A modified CPT was used to determine whether participants suffered from hyperalgesia. This method was established for analgesic evaluation by Wolff et al and is considered the most commonly used pain test for ascertaining OIH in human studies.22,28,29 As age and sex are relevant parameters for CPT, the control group was matched for these features.
For this assessment, a round container (diameter, 25 cm; depth, 11 cm) was filled with ice cubes and cold water. It was shown that temperature fluctuations of 2°C already have an impact on pain tolerance and intensity; therefore, water temperature was maintained at 1.6°C (±0.6°C), measured with a digital probe thermometer.30 Subjects were asked to immerse their non-dominant hand in a cold-water tank with fingers spread until the ice cubes covered the back of their hand. Prior to the test, they were instructed to verbally indicate the exact moment when the cold sensation began to elicit pain and to remove their hands from the CPT bath at the point of intolerable pain. The time from hand immersion to the first detection of pain was defined as “latency of pain onset”. The period between submerging and withdrawing the hand is described as “pain tolerance”. Both time intervals were measured in seconds. OIH can be detected by reduced pain tolerance.31
The test was terminated after 180 s for safety reasons. For subjects who did not withdraw their hands within this time period, a pain tolerance of 180 s was recorded. If no pain was felt during this time frame, a latency of pain onset of 180 s was noted as well. After hand withdrawal, participants rated their pain level using an 11-point NRS, as described previously.
Data Analysis and Statistics
A Kruskal–Wallis-Test was performed to compare all results between the BM, MM, and CG subgroups, clarifying whether they differed significantly from each other. Pairwise comparisons were conducted for the features that showed significant differences.
Results
MM included 13 males and seven female participants with a mean age of 41.5 years (range 27–62 years) and a daily methadone dosage of 100.75 mg (range 50–160 mg). The BM consisted of 12 males and eight females with a mean age of 41.7 years (range 28–51 years), receiving a mean buprenorphine dose of 13.1 mg per day (range 0.3 to 28 mg). The control group comprised 12 males and eight female participators aged averagely 42.4 years (range 27–57 years). As shown in Table 1, no significant differences in sex or age were found between subgroups. Therefore, it can be concluded that the groups successfully matched these features.
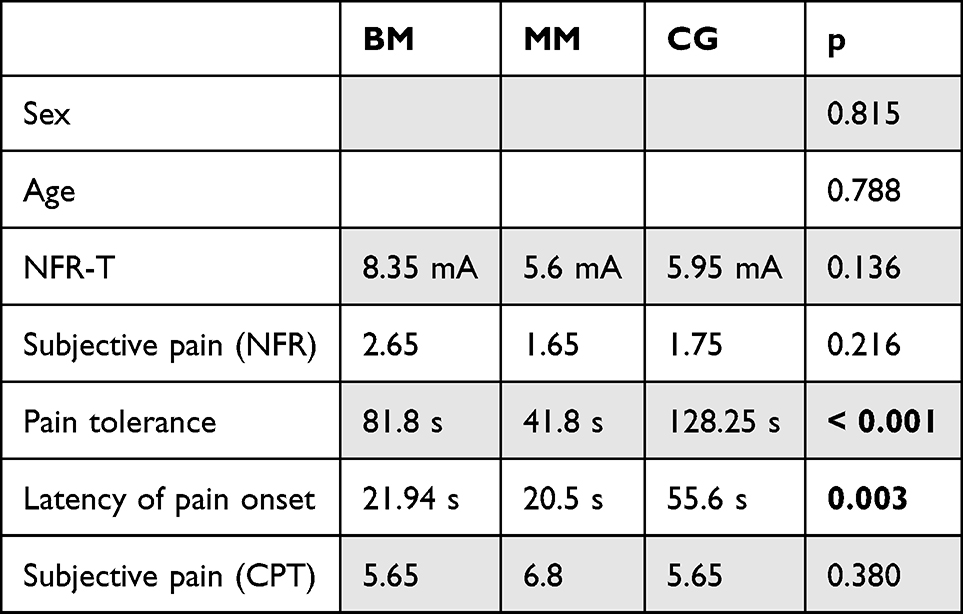 |
Table 1 Means of the NFR-T Assessment and the CPT with Related p-values; Comparison of BM, MM and CG; Significant Values (P < 0.05) are Given in Bold |
Two participants were excluded from this study. In one case, evaluation was not possible because the impedance of the EMG electrodes could not be reduced to a level measurable by the Paintracker. Another patient received a dose increase two weeks prior to the examination and therefore did not fulfil the required inclusion criteria. Data collection was successful for 60 subjects (96,7%).
Means of the captured data from the NFR assessment and CPT were compared between all groups and are presented in Table 1 together with the related p-values.
As summarised in Table 1, significant differences were evident in pain tolerance and latency of pain onset. Pairwise comparisons of these values suggest significant differences between the maintenance groups and CG. Comparing them to their opioid-free counterparts resulted in significantly shorter pain tolerance in patients treated with buprenorphine (p = 0.023) and those receiving methadone (p < 0.001). Latency of pain onset was also significantly lower in the BM (p = 0.006) and MM (p = 0.002) than in the CG.
No significant differences in pain tolerance (p = 0.122) or latency of pain onset (p = 0.794) were found when both maintenance groups were compared to each other.
For better visualisation, the results for latency of pain onset (Figure S1), pain tolerance (Figure S2) and subjective pain in CPT (Figure S3) are shown in box plots.
Discussion
Lowered Pain Tolerance in the CPT as Sign for Hyperalgesia
The outcome of CPT shows that opioids prescribed as maintenance treatment have an impact on pain tolerance, in the sense of increased sensitivity and quicker hand withdrawal when compared to non-opioid users. It can be concluded that patients undergoing substitution therapy are markedly hyperalgesic to cold pressor pain, suggesting that they suffer from OIH.
This assumption is consistent with results of previous studies.28 Other investigators also compared opioid-maintained individuals with their opioid-free counterparts and reported significantly shorter times of pain tolerance measured by CPT in methadone-maintained individuals,32–37 as well as in subjects treated with buprenorphine.34,38
In the current study, the clinical utility of CPT, particularly its pain tolerance parameter, was evaluated for the diagnosis of OIH.
In addition, opioid intake seemed to influence the latency of pain onset, which was significantly shorter in both maintenance groups than in the control group. Although Doverty et al found a significantly shorter latency of pain onset in methadone-treated patients than in opioid-free controls,36 the study situation remains inconsistent, and latency of pain onset should not be counted as a relevant marker in diagnosing OIH. It is difficult to identify the exact beginning of pain perception during a constantly increasing sensation, which makes the parameter hard to capture. The assessment was not painful for some participants. For those, a latency of pain onset of 180 s was noted, which diminished the reliability of the parameter.
Clinical Utility of the NFR-T for Diagnosing OIH
The present study examined whether the data collected from the NFR-T assessment might indicate heightened pain sensation in opioid-maintained individuals. Unfortunately, no correlation between a shorter duration of pain tolerance and decreased NFR-T was found, since the latter, measured in both maintenance groups, did not significantly differ from opioid-free controls. Therefore, NFR-T may not be a suitable marker for OIH diagnosis.
One possible reason might be that NFR is a spinal reflex, while the exact origin of OIH has not yet been completely investigated, as mentioned previously.10
According to Sandrini et al, NFR in humans is entirely mediated by spinal structures.39 On the other hand, OIH is assumed to originate in higher centres of the central nervous system than the spinal cord, with a special focus on the midbrain periaqueductal gray and rostral ventromedial medulla. The descending analgesic systems of these supraspinal structures are also considered relevant.1,40 More precisely, long-term opioid administration is believed to lead to postsynaptic adaptions in the periaqueductal gray and other brain regions, which may induce neuroadaptations within the rostroventral medial medulla.41,42 Tonic activation of the facilitation of descending pain in this structure may lead to hyperalgesia.1,40,43
Although the NFR is modulated by supraspinal structures and descending systems, the origin of OIH may not be represented by a deviating threshold.39,44–46 Further investigation concerning a reflex generator of supraspinal derivation as a possible marker for OIH is required in the future.
What implied NFR-T assessment as considerable method for investigating OIH is that decreased NFR-T correlated with hyperexcitability of the central nervous system in patients with chronic pain.47 Furthermore, multiple studies have reported a decreased threshold in patients with secondary hyperalgesia.48,49
Subjective Pain Perception
The fact that subjective pain perception does not seem to be affected by long-term opioid intake may be elucidated by several theories.
During the NFR-T measurement, there was no significant difference in pain sensation between the MM and BM groups and the control group. One explanation might be the correlation between NFR-T and the threshold of sensation as well as between the amplitude of each reflex and the amount of pain experienced by the individual.12,39,50–53 Consequently, the absence of differences in subjective pain perception during the NFR-T assessment might be due to the lack of differences between reflex thresholds.
Furthermore, studies have shown that altered pain sensations due to OIH do not affect all types of pain in the same manner. Several studies have shown that pain sensations caused by electrical or mechanical stimulation do not vary between maintenance patients and those without opioid exposure.32,33,36,54
In contrast, the experimental data implied that hot, cold, and cold pressure perceptions became hypersensitive during opioid treatment.33,35–37,55–57 However, in this study, no significant difference was observed in subjective pain perception after CPT between the BM and MM groups as well as their opioid-free counterparts.
Comparison of Methadone and Buprenorphine
Studies on OIH have reported that this phenomenon generally occurs with opioid exposure. However, little research has been conducted to investigate potential differences in the degree of OIH following treatment with various opioid classes.
It was attempted to determine whether varying receptor behaviour might have an impact on the expression of hyperalgesia.
Methadone hydrochloride is a long-acting μ-opioid receptor agonist that also exhibits weak N-methyl-d-aspartate (NMDA)-receptor antagonism.21,58 Several studies have proposed that the central glutamatergic system and relating thereto, the excitatory neurotransmitter NMDA, is involved in the development of OIH.4,59 Buprenorphine hydrochloride is a partial agonist of the μ-opioid receptor and shows weak k-receptor antagonism but does not affect NMDA receptors.58 K-Opioid receptor agonists are also considered to play a role in the development of OIH.3 Studies have demonstrated hyperalgesic responses after intrathecal injection of κ-agonists in animals.60,61 In contrast, buprenorphine is an antagonist at this receptor site.
It is believed that the μ-opioid receptor system plays an essential role in the development of OIH and that different μ-opioid receptor agonists such as methadone and buprenorphine can cause this phenomenon.3 Li et al supported this statement by publishing an animal experiment in which no OIH development was observed in mice expressing fewer μ-opioid receptors than wild-type mice.62
In the current study, no differences in any results great enough to be detected were found between the group maintained on methadone and the subjects treated with buprenorphine.
The results of this study suggest μ-receptor agonism as decisive process leading to OIH. Different individual intrinsic activities of opioid receptors, as well as binding effects, such as receptor phosphorylation or G-protein activation, which are often suggested to influence pain sensation in different ways, might play a subordinate role.34,63,64
Limitations
This study has several limitations. Pain is a subjective construct that is influenced by many biological, psychological, and social factors.65 Several studies have shown that the NFR-T is also subject to biopsychosocial influences.39,66–69 It was not possible to establish all relevant influences as inclusion criteria for this study.
Another limiting factor is that the participants were recruited from different treatment centres, resulting in various regulations on co-consumption. The drug test results of participants were not considered in this study. Treatment-seeking persons with opioid use disorder are prone to relapse.70–73 Some participants were likely to be influenced by other substance classes or additional opioids. Owing to different handling at treatment sites, the proportion of co-users and choice of substances may vary between the groups.
Possible substance use by the CG was also not monitored. The CG being opioid-free was determined by self-report. To keep the study as simple as possible, adjuvant medication was not queried in any of the groups. These facts reduce the significance of the study because, as already mentioned in the introduction, the NFR-T appears to be influenced by various substances.15,74
Our study was designed as a pilot study. The group size of 20 participants per group was selected based on the practical feasibility of patients or subjects. Due to the small group size, it is possible that effects may have been overlooked, or a statistically significant effect could have been observed with a larger number of participants. Our study may serve as a foundation for future research to conduct a power analysis for determining an appropriate sample size. Concurrent drug use had a major impact on the data collected during this study. Compton et al performed CPT in methadone-maintained individuals and proposed a significantly longer duration of pain tolerance in subjects under concurrent cocaine influence than in those without recent cocaine use.75 Another study even reported a significant difference in pain tolerance between consumption-free groups maintained on methadone and those treated with buprenorphine.34
In conclusion, the lack of difference in the pain threshold between the MM and BM groups may be questionable because co-use was not monitored. Compton et al also formulated this hypothesis.34
Opioid dosages and time intervals between drug intake and measurement may also be considered relevant. Investigators found a correlation between higher methadone doses and shorter periods of pain tolerance but were not able to find a difference in pain tolerance when the period between methadone intake and measurement varied.75 In contrast, another study found different pain sensitivities when the assessment was performed at trough and peak plasma concentrations of maintenance drugs.36
In this study, doses were not included in the evaluation. Most individuals participated in the assessment immediately after the ingestion of their substitution treatment. However, there was no standardised setting for the exact time gap.
Finally, one limitation worth considering is that being more sensitive to pain may predispose individuals to develop opioid dependence.32 Therefore, a comparison with healthy volunteers might reveal differences even in the absence of opioid use.
Conclusion
Based on the present evidence, patients undergoing maintenance therapy show increased sensitivity to cold pressor pain regardless of the intrinsic activity of the opioid agonist they are treated with. In this context, CPT has proven to be a useful tool for investigating OIH.
The aim of this study was to determine whether diagnosing OIH could be facilitated by NFR-T, an objective and uninfluenceable marker for pain. Although methadone and buprenorphine have been proven to cause hyperalgesia, no effect on the reflex threshold was observed. NFR-T might not approach the exact location in the central nervous system where OIH originates and is therefore not helpful in its evaluation.
Owing to the high prevalence of opioid dependence already mentioned, the importance of OIH should not be underestimated. Further research should be conducted in the future to facilitate diagnosis and provide appropriate pain management for maintenance patients.
Acknowledgment
The authors would like to thank N. Lenuweit, who helped with recruiting probands.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
All authors report no conflicts of interest in this work.
References
1. Mercadante S, Arcuri E, Santoni A. Opioid-induced tolerance and hyperalgesia. CNS Drugs. 2019;33(10):943–955. doi:10.1007/s40263-019-00660-0
2. Yi P, Pryzbylkowski P. Opioid induced hyperalgesia. Pain Med. 2015;16 Suppl 1:S32–6:doi:10.1111/pme.12914
3. Angst MS, Clark JD. Opioid-induced hyperalgesia: a qualitative systematic review. Anesthesiology. 2006;104(3):570–587. doi:10.1097/00000542-200603000-00025
4. Silverman SM. Opioid induced hyperalgesia: clinical implications for the pain practitioner. Pain Physician. 2009;12(3):679–684. doi:10.36076/ppj.2009/12/679
5. Guidelines for the psychosocially assisted pharmacological treatment of opioid dependence. World Health Organization; 2009.
6. European Monitoring Centre for Drugs and Drug Addiction. Balancing Access to Opioid Substitution Treatment with Preventing the Diversion of Opioid Substitution Medications in Europe: Challenges and Implications. Publications Office; 2021.
7. Koller G, Schwarzer A, Halfter K, Soyka M. Pain management in opioid maintenance treatment. Expert Opin Pharmacother. 2019;20(16):1993–2005. doi:10.1080/14656566.2019.1652270
8. Voon P, Hayashi K, Milloy M-J, et al. Pain among high-risk patients on methadone maintenance treatment. J Pain. 2015;16(9):887–894. doi:10.1016/j.jpain.2015.06.003
9. Mitchell AM, Dewey CM. Chronic pain in patients with substance abuse disorder: general guidelines and an approach to treatment. Postgrad Med. 2008;120(1):75–79. doi:10.3810/pgm.2008.04.1763
10. Skljarevski V, Ramadan NM. The nociceptive flexion reflex in humans – review article. Pain. 2002;96(1):3–8. doi:10.1016/S0304-3959(02)00018-0
11. Willer J-C. Studies on pain. Effects of morphine on a spinal nociceptive flexion reflex and related pain sensation in man. Brain Res. 1985;331(1):105–114. doi:10.1016/0006-8993(85)90719-X
12. de WJC. Comparative study of perceived pain and nociceptive flexion reflex in man. Pain. 1977;3(1):69–80. doi:10.1016/0304-3959(77)90036-7
13. Willer JC. Exploration clinique de la nociception par des techniques de réflexologie. Neurophysiologie Clinique/Clinical Neurophysiology. 1990;20(5):335–356. doi:10.1016/S0987-7053(05)80203-5
14. Cruccu G, Anand P, Attal N, et al. EFNS guidelines on neuropathic pain assessment. Eur J Neurol. 2004;11(3):153–162. doi:10.1111/j.1468-1331.2004.00791.x
15. Willer JC, Bathien N. Pharmacological modulations on the nociceptive flexion reflex in man. Pain. 1977;3(2):111–119. doi:10.1016/0304-3959(77)90074-4
16. Willer JC, Bussel B. Evidence for a direct spinal mechanism in morphine-induced inhibition of nociceptive reflexes in humans. Brain Res. 1980;187(1):212–215. doi:10.1016/0006-8993(80)90507-7
17. Fields HL, Heinricher MM. Brainstem modulation of nociceptor-driven withdrawal reflexes. Ann N Y Acad Sci. 1989;563(1):34–44. doi:10.1111/j.1749-6632.1989.tb42188.x
18. Fishman MA, Kim PS. Buprenorphine for Chronic Pain: a Systemic Review. Curr Pain Headache Rep. 2018;22(12):83. doi:10.1007/s11916-018-0732-2
19. Dematteis M, Auriacombe M, D’Agnone O, et al. Recommendations for buprenorphine and methadone therapy in opioid use disorder: a European consensus. Expert Opin Pharmacother. 2017;18(18):1987–1999. doi:10.1080/14656566.2017.1409722
20. Bickel WK, Stitzer ML, Bigelow GE, Liebson IA, Jasinski DR, Johnson RE. A clinical trial of buprenorphine: comparison with methadone in the detoxification of heroin addicts. Clin Pharmacol Ther. 1988;43(1):72–78. doi:10.1038/clpt.1988.13
21. Eap CB, Buclin T, Baumann P. Interindividual variability of the clinical pharmacokinetics of methadone: implications for the treatment of opioid dependence. Clin Pharmacokinet. 2002;41(14):1153–1193. doi:10.2165/00003088-200241140-00003
22. Walsh NE, Schoenfeld L, Ramamurthy S, Hoffman J. Normative model for cold pressor test. Am J Phys Med Rehabil. 1989;68(1):6–11. doi:10.1097/00002060-198902000-00003
23. Annex I. Summary of product characteristics. In: Stolerman IP, Price LH, editors. Encyclopedia of Psychopharmacology. Berlin Heidelberg: Springer; 2015:1687.
24. von DF, Hackbarth M, Schneider M, Baars JH, Rehberg B. Introduction of a continual RIII reflex threshold tracking algorithm. Brain Res. 2009;1260:24–29. doi:10.1016/j.brainres.2009.01.001
25. Dowman R. Possible startle response contamination of the spinal nociceptive withdrawal reflex. Pain. 1992;49(2):187–197. doi:10.1016/0304-3959(92)90142-X
26. Rhudy JL, France CR. Defining the nociceptive flexion reflex (NFR) threshold in human participants: a comparison of different scoring criteria. Pain. 2007;128(3):244–253. doi:10.1016/j.pain.2006.09.024
27. France CR, Rhudy JL, McGlone S. Using normalized EMG to define the nociceptive flexion reflex (NFR) threshold: further evaluation of standardized NFR scoring criteria. Pain. 2009;145(1–2):211–218. doi:10.1016/j.pain.2009.06.022
28. Oaks Z, Stage A, Middleton B, Faraone S, Johnson B. Clinical utility of the cold pressor test: evaluation of pain patients, treatment of opioid-induced hyperalgesia and fibromyalgia with low dose naltrexone. Discov Med. 2018;26(144):197–206.
29. Wolff BB, Kantor TG, Jarvik ME, Laska E. Response of experimental pain to analgesic drugs. 3. Codeine, aspirin, secobarbital, and placebo. Clin Pharmacol Ther. 1969;10(2):217–228. doi:10.1002/cpt1969102217
30. Mitchell LA, MacDonald RAR, Brodie EE. Temperature and the cold pressor test. J Pain. 2004;5(4):233–237. doi:10.1016/j.jpain.2004.03.004
31. Yang DZ, Sin B, Beckhusen J, Xia D, Khaimova R, Iliev I. Opioid-induced hyperalgesia in the nonsurgical setting: a systematic review. Am J Ther. 2019;26(3):e397–e405. doi:10.1097/MJT.0000000000000734
32. Chu LF, Angst MS, Clark D. Opioid-induced hyperalgesia in humans: molecular mechanisms and clinical considerations. Clin J Pain. 2008;24(6):479–496. doi:10.1097/AJP.0b013e31816b2f43
33. Doverty M, Somogyi AA, White JM, et al. Methadone maintenance patients are cross-tolerant to the antinociceptive effects of morphine. Pain. 2001;93(2):155–163. doi:10.1016/S0304-3959(01)00306-2
34. Compton P, Charuvastra V, Ling W. Pain intolerance in opioid-maintained former opiate addicts: effect of long-acting maintenance agent. Drug Alcohol Depend. 2001;63(2):139–146. doi:10.1016/S0376-8716(00)00200-3
35. Compton P, Charuvastra V, Kintaudi K, Ling W. Pain responses in methadone-maintained opioid abusers. J Pain Sympt Manage. 2000;20(4):237–245. doi:10.1016/S0885-3924(00)00191-3
36. Doverty M, White JM, Somogyi AA, Bochner F, Ali R, Ling W. Hyperalgesic responses in methadone maintenance patients. Pain. 2001;90(1):91–96. doi:10.1016/S0304-3959(00)00391-2
37. Hay JL, White JM, Bochner F, Somogyi AA, Semple TJ, Rounsefell B. Hyperalgesia in opioid-managed chronic pain and opioid-dependent patients. J Pain. 2009;10(3):316–322. doi:10.1016/j.jpain.2008.10.003
38. Athanasos P, Ling W, Bochner F, White JM, Somogyi AA. Buprenorphine maintenance subjects are hyperalgesic and have no antinociceptive response to a very high morphine dose. Pain Med. 2019;20(1):119–128. doi:10.1093/pm/pny025
39. Sandrini G, Serrao M, Rossi P, Romaniello A, Cruccu G, Willer JC. The lower limb flexion reflex in humans. Prog Neurobiol. 2005;77(6):353–395. doi:10.1016/j.pneurobio.2005.11.003
40. Lee M. A comprehensive review of opioid-induced hyperalgesia. Pain Physician. 2011;14(2):145–161. doi:10.36076/ppj.2011/14/145
41. Wilson-Poe AR, Lau BK, Vaughan CW. Repeated morphine treatment alters cannabinoid modulation of GABAergic synaptic transmission within the rat periaqueductal grey. Br J Pharmacol. 2015;172(2):681–690. doi:10.1111/bph.12809
42. Wilson-Poe AR, Jeong H-J, Vaughan CW. Chronic morphine reduces the readily releasable pool of GABA, a presynaptic mechanism of opioid tolerance. J Physiol. 2017;595(20):6541–6555. doi:10.1113/JP274157
43. Vanderah TW, Suenaga NMH, Ossipov MH, Malan TP, Lai J, Porreca F. Tonic descending facilitation from the rostral ventromedial medulla mediates opioid-induced abnormal pain and antinociceptive tolerance. J Neurosci. 2001;21(1):279–286. doi:10.1523/JNEUROSCI.21-01-00279.2001
44. Miller JC, Boureau F, Albe-Fessard D. Supraspinal influences on nociceptive flexion reflex and pain sensation in man. Brain Res. 1979;179(1):61–68. doi:10.1016/0006-8993(79)90489-X
45. Jones SL. Descending noradrenergic influences on pain. In: Pompeiano O, Barnes CD, editors. Progress in Brain Research. Elsevier; 1991:381–394.
46. Jure FA, Arguissain FG, Biurrun Manresa JA, Andersen OK. Conditioned pain modulation affects the withdrawal reflex pattern to nociceptive stimulation in humans. Neuroscience. 2019;408:259–271. doi:10.1016/j.neuroscience.2019.04.016
47. Amiri M, Esmaili H, Hamad AH, Alavinia M, Masani K, Kumbhare D. Nociceptive flexion reflex threshold in chronic pain patients: a needed update for the current evidence. Am J Phys Med Rehabil. 2021;100(8):750–759. doi:10.1097/PHM.0000000000001626
48. Leone C, Di Lionardo A, Di Pietro G, et al. How different experimental models of secondary hyperalgesia change the nociceptive flexion reflex. Clin Neurophysiol. 2021;132(12):2989–2995. doi:10.1016/j.clinph.2021.08.018
49. Grönroos M, Pertovaara A. Capsaicin-induced central facilitation of a nociceptive flexion reflex in humans. Neurosci Lett. 1993;159(1–2):215–218. doi:10.1016/0304-3940(93)90837-B
50. Bromm B, Treede D-R. Withdrawal reflex, skin resistance reaction and pain ratings due to electrical stimuli in man. Pain. 1980;9(3):339–354. doi:10.1016/0304-3959(80)90048-2
51. Chan C, Dallaire M. Subjective pain sensation is linearly correlated with the flexion reflex in man. Brain Res. 1989;479(1):145–150. doi:10.1016/0006-8993(89)91344-9
52. Dowman R. Spinal and supraspinal correlates of nociception in man. Pain. 1991;45(3):269–281. doi:10.1016/0304-3959(91)90051-X
53. Dowman R. A noninvasive strategy for identifying and quantifying innocuous and nociceptive peripheral afferent activity evoked by nerve stimulation. Physiol Behav. 1993;53(6):1163–1169. doi:10.1016/0031-9384(93)90374-O
54. Schall U, Katta T, Pries E, Klöppel A, Gastpar M. Pain perception of intravenous heroin users on maintenance therapy with levomethadone. Pharmacopsychiatry. 1996;29(5):176–179. doi:10.1055/s-2007-979567
55. Athanasos P, Smith CS, White JM, Somogyi AA, Bochner F, Ling W. Methadone maintenance patients are cross-tolerant to the antinociceptive effects of very high plasma morphine concentrations. Pain. 2006;120(3):267–275. doi:10.1016/j.pain.2005.11.005
56. Peles E, Schreiber S, Hetzroni T, Adelson M, Defrin R. The differential effect of methadone dose and of chronic pain on pain perception of former heroin addicts receiving methadone maintenance treatment. J Pain. 2011;12(1):41–50. doi:10.1016/j.jpain.2010.04.009
57. Eyler ECH. Chronic and acute pain and pain management for patients in methadone maintenance treatment. Am J Addict. 2013;22(1):75–83. doi:10.1111/j.1521-0391.2013.00308.x
58. O’Connor PG, Fiellin DA. Pharmacologic treatment of heroin-dependent patients. Ann Intern Med. 2000;133(1):40–54. doi:10.7326/0003-4819-133-1-200007040-00008
59. Andersen OK, Felsby S, Nicolaisen L, Bjerring P, Jensen TS, Arendt-Nielsen L. The effect of Ketamine on stimulation of primary and secondary hyperalgesic areas induced by capsaicin -- a double-blind, placebo-controlled, human experimental study. Pain. 1996;66(1):51–62. doi:10.1016/0304-3959(96)02995-8
60. Leighton GE, Hill RG, Hughes J. Intrathecal injection of a ϰ opioid agonist produces hyperalgesia in the Guinea pig. Eur. J. Pharmacol. 1988;157(2–3):241–242. doi:10.1016/0014-2999(88)90390-1
61. Wu KM, Martin WR, Kamerling SG, Wettstein JG. Possible medullary κ hyperalgesic mechanism I. A new potential role for endogenous opioid peptides in pain perception. Life Sci. 1983;33(18):1831–1838. doi:10.1016/0024-3205(83)90691-4
62. Li X, Angst MS, Clark J. A murine model of opioid-induced hyperalgesia. Mol Brain Res. 2001;86(1–2):56–62. doi:10.1016/S0169-328X(00)00260-6
63. Emmerson PJ, Clark MJ, Mansour A, Akil H, Woods JH, Medzihradsky F. Characterization of opioid agonist efficacy in a C6 glioma cell line expressing the mu opioid receptor. J Pharmacol Exp Ther. 1996;278(3):1121–1127.
64. Yu Y, Zhang L, Yin X, Sun H, Uhl GR, Wang JB. Mu opioid receptor phosphorylation, desensitization, and ligand efficacy. J Biol Chem. 1997;272(46):28869–28874. doi:10.1074/jbc.272.46.28869
65. Fillingim RB. Individual differences in pain: understanding the mosaic that makes pain personal. Pain. 2017;158 Suppl 1:S11-S18:doi:10.1097/j.pain.0000000000000775\
66. Ang DC, Chakr R, France CR, et al. Association of nociceptive responsivity with clinical pain and the moderating effect of depression. J Pain. 2011;12(3):384–389. doi:10.1016/j.jpain.2010.09.004
67. Rhudy JL, Bartley EJ, Williams AE, et al. Are there sex differences in affective modulation of spinal nociception and pain? J Pain. 2010;11(12):1429–1441. doi:10.1016/j.jpain.2010.04.003
68. Rhudy JL, Bartley EJ. The effect of the menstrual cycle on affective modulation of pain and nociception in healthy women. Pain. 2010;149(2):365–372. doi:10.1016/j.pain.2010.02.041
69. Rhudy JL, Williams AE, McCabe KM, Matv N, Rambo P. Affective modulation of nociception at spinal and supraspinal levels. Psychophysiology. 2005;42(5):579–587. doi:10.1111/j.1469-8986.2005.00313.x
70. Wang R, Ding Y, Bai H, et al. Illicit heroin and methamphetamine use among methadone maintenance treatment patients in dehong prefecture of Yunnan province, China. PLoS One. 2015;10(7):e0133431. doi:10.1371/journal.pone.0133431
71. Tang X, Fan C, Wang C, et al. The risk assessment of relapse among newly enrolled participants in methadone maintenance treatment: a group-LASSO based Bayesian network study. Front Public Health. 2022;10:1032217. doi:10.3389/fpubh.2022.1032217
72. Dobler-Mikola A, Hättenschwiler J, Meili D, Beck T, Böni E, Modestin J. Patterns of heroin, cocaine, and alcohol abuse during long-term methadone maintenance treatment. J Subst Abuse Treat. 2005;29(4):259–265. doi:10.1016/j.jsat.2005.08.002
73. Gollnisch G. Multiple predictors of illicit drug use in methadone maintenance clients. Addict Behav. 1997;22(3):353–366. doi:10.1016/S0306-4603(96)00024-X
74. Bromm B, Seide K. The influence of tilidine and prazepam on withdrawal reflex, skin resistance reaction and pain rating in man. Pain. 1982;12(3):247–258. doi:10.1016/0304-3959(82)90156-7
75. Ma C. Cold-pressor pain tolerance in opiate and cocaine abusers: correlates of drug type and use status. J Pain Sympt Manage. 1994;9(7):462–473. doi:10.1016/0885-3924(94)90203-8
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.