")
Back to Journals » Advances in Medical Education and Practice » Volume 14
Observational Study of Conformity in Yet Another Medical Learning Environment: Conformity to Preceptors During High-Fidelity Simulation
Authors Beran TN , Altabbaa G, Oddone Paolucci E
Received 13 September 2023
Accepted for publication 27 November 2023
Published 22 December 2023 Volume 2023:14 Pages 1445—1452
DOI https://doi.org/10.2147/AMEP.S427996
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Tanya N Beran,1 Ghazwan Altabbaa,2 Elizabeth Oddone Paolucci3
1Department of Community Health Sciences, University of Calgary, Calgary, Alberta, Canada; 2Department of Medicine, University of Calgary and Rockyview General Hospital, Calgary, Alberta, Canada; 3Department of Community Health Sciences and Department of Surgery, University of Calgary, Calgary, Alberta, Canada
Correspondence: Tanya N Beran, Department of Community Health Sciences, University of Calgary, 3330 Hospital Dr. N.W, Calgary, Alberta, T2N 4N1, Canada, Tel +1 403 220 5667, Fax +1 403 210 7507, Email [email protected]
Purpose: Altering one’s behavior to comply with inaccurate suggestions made by others (i.e., conformity) has been studied since the 1950s. Although several studies have documented its occurrence in medical education, it has yet to be examined in a high-fidelity simulation environment. It was hypothesized that a large majority of learners would conform to a preceptor.
Patients and Methods: A total of 42 student dyads (a medical student paired with a resident) participated in one of four clinical scenarios to manage the diagnosis and treatment of a simulated patient encounter. Once the learners became familiar with the patient’s case, a preceptor entered the simulation, offered an equivocal suggestion about diagnosis or management, and then left. Two raters observed the video recordings of how the learners managed the case after this suggestion was made. The nature of these interactions was also documented.
Results: Sixteen (38.10%) of the 42 medical student dyads conformed to the equivocal information presented by the preceptors. Observations of these interactions showed that all of the medical students conformed to the residents, but not all of the medical students conformed to the preceptors.
Conclusion: Many learners conform to preceptors by acting on their equivocal suggestion when managing a patient case during high-fidelity simulation.
Keywords: Adherence, medical students, Immersive learning, medical education, medical errors, patient safety
Introduction
Medical training in hospitals is intended to “imprint habits” that will “endure for many years” as novices transform into professionals who will provide society with competent and compassionate care.1 Although medical learners do indeed develop essential competencies to manage patient care, there is now considerable evidence that students in any year of their medical education program are at risk of conforming to information they believe may be incorrect.2
These studies have examined conformity to peers primarily, with little focus on how they manage pressure from preceptors. Given the trust and reliance that learners place on preceptors, it is plausible that learners would accept all instruction, regardless of its accuracy. A potential undesirable outcome is some misunderstanding of how to manage patient care. The present study examines how learners manage a simulated patient case upon receiving equivocal diagnosis or treatment information from a preceptor.
Conformity
Starting in the 1950s, researchers have been reporting that individuals in a variety of settings are likely to change what they say when they encounter contrary information held by people in a group to which they belong, even when they believe this information to be incorrect.3,4 Of note, over 96% of online learners provided at least one incorrect answer that was the same incorrect response provided by their peers.5 Within the last decade, conformity has been examined in the context of medical education. It has been shown to affect medical clerks’ procedural skills performance where they were likely to aspirate in the same incorrect location that they believed their peers had used.6 Particularly compelling is the finding that over 95% of learners reported at least one inaccurate vital sign after hearing these values reported by other learners, even after demonstrating their ability to take these vital signs correctly.7 These learners, moreover, were likely to select a diagnosis that corresponded with these incorrect values.8 These rates of observed conformity are similar to learners’ perceptions of pressure to conform. That is, over 85% of residents reported feeling the pressure to “go along with” other people’s ideas, even when these ideas seem wrong, during their clinical rotation in residency.9
A specific form of conformity is obedience to authority where an individual complies with instructions given by a person in authority.10 Although it is usually desirable, and indeed required, that medical learners follow the sound guidance given by instructors, obedience may also occur when the individual believes that the authority figure shares incorrect, equivocal, or uninformed information. If the medical education enterprise is to “turn out properly trained doctors”,11 or in today’s parlance, to acquire “foundational competencies”12 it is incumbent upon medical education researchers to examine whether learners are developing the ability to manage these types of information exchanges.
In this study, we examine behavioral data from physicians-in-training on a clinical rotation in Internal Medicine to determine if they conform when presented with equivocal information from a preceptor about a simulated patient case. This hierarchy, which consists of unavoidable authority gradients within and between clinical disciplines, can lead to significant patient harm if communication is hampered.13 Since self-reporting of conformity behaviors may be unreliable,14 studying conformity within this hierarchy during high-fidelity simulation (i.e., realistic patient environment) provides researchers with a repeatable method to study differences in authority between health professionals and clinical disciplines, while ensuring participant psychological safety.13 In this context, an equivocal suggestion occurs when a preceptor suggests a possible decision about diagnosis and treatment – but the clinical presentation would suggest a better one. Thus, the purpose of the study is to observe how many learners act on an equivocal diagnostic or treatment suggestion made by a preceptor. Given our previous studies demonstrating that over 80% of learners exhibit conformity, we hypothesized that a similar number would do so when managing a patient case in simulation. Simulation is an ideal method for observing people’s behaviors in a controlled and realistic environment, allowing for standardized stimuli across participants for the purposes of conducting research with the ultimate goal of enhancing patient care.15 To achieve this, we must understand how medical learners manage equivocal information when actively involved in patient care to ensure that they have developed the professional skills necessary to manage such information when practicing independently.
Materials and Methods
This study was approved by the Conjoint Research Ethics Board (CHREB) of the University of Calgary (REB15-1371), which included approval for the consent process used in this study. We employed a cross-sectional observational design, which allowed us to record learners’ behaviors as they interacted with members of a clinical team and a patient in simulation. Thus, we obtained an indication of the types of behaviors that may occur in clinical practice.
Participants
A convenience sample of physicians-in-training from various specialties enrolled at a mid-Western Canadian university was obtained. They were completing their Internal Medicine rotation at a local hospital where they were developing their skills in diagnostic and therapeutic recommendations, which are represented in the present study’s simulation scenarios. There was a total of 84 learners (n = 42, 50.0% third-year undergraduate medical students; n = 42, 50.0% first-year residents), and more than half were female (n = 47, 56.0%). Both residents and medical students were included because they are typically paired in the simulation teaching that takes place during their clinical rotations. Data were collected as part of another study in which a scoring rubric for conformity behaviors was developed and their association with other factors was examined.16 This sample consisted of 42 dyads, or 84 participants.
Procedures
Each individual session consisted of 10–15 minutes of prebriefing, a 15–20 minute scenario, and 25–30 minutes of debriefing. The pre-briefing session began with introductions from the simulation educator and the researchers – these researchers were introduced as PhD students with an interest in simulation. The learners were given instructions about the focus on learning and safety in simulation. They were also asked to sign a consent for recording the simulation as well as a confidentiality agreement. Specifically, they were told that the videos assisted with discussion and sharing feedback with the participants. They were also told that the scenario would create uncertainty and that different types of pressure might affect their decision making. The purpose of the simulation was, therefore, described as developing communication strategies to manage such situations.
Then a pair of learners was asked to volunteer for each session to ensure equal participation within the cohort. They were oriented to the simulator over a 15-minute pre-briefing period where the functionality of the mannequin (with its normal and abnormal findings) and availability of equipment in the room were explained.
The environment was set up as an emergency room, and it was equipped with a camera that framed the entire room to stream and record the activities that allowed those who did not participate in the simulation activity to also observe. The simulator was a SimMan®3G (Laerdal Medical Canada) with LLEAP software to set physical and physiological features. No modifications were made to the default technical specifications. Equipment included IV access equipment, fluids, and mini bags along with airway support, emergency room chart and forms, lab results and imaging studies, laptop with online access/resources, vital signs monitor, and cart with drawers containing patient care equipment.
After the simulation, debriefing of the patient case was conducted by the simulation instructor with input from the nurse, followed by a debriefing of the research by a student researcher. In this last phase, participants were informed about the general goals of the research, and they were asked if they would consent to the recorded simulations being used for research. Informed consent for the research had not been conducted before the simulation due to the likelihood that this information would have biased the learners and reduced the scientific validity of the study. All learners gave signed informed consent, and no concerns about this process were expressed or reported. Participants were also told that they had the option of withdrawing their data from the study up to six months after initial consent. This latter phase was conducted by the researcher, rather than the educator, to minimize the pressure to agree. All the debriefing guidelines for behavioral research of the American Psychological Association were followed.
Simulation Scenarios
Study participants managed one of the following four types of clinical scenarios (Table 1) taught by a physician simulation educator (i.e., preceptor) who is certified by the Society of Simulation in Healthcare. All preceptors were male and were known to the learners in some capacity as a preceptor or Internal Medicine physician. Also, a female simulation nurse, who had active clinical work experience on the medical unit and training in simulation-based education, participated in each simulation and was aware of this study but instructed not to prompt the learners so as not to influence their decisions. The simulations were developed by the simulation program director (author GA) at the hospital who typically teaches these learners and is familiar with their learning needs. This director was able to ensure that the simulations reflected the real expectations for learners’ abilities to diagnose at their specific level of training. Simulations also followed the 12 tips outlined by Altabbaa et al2 for using simulation to understand conformity. The simulation scenarios were scripted with no programming.
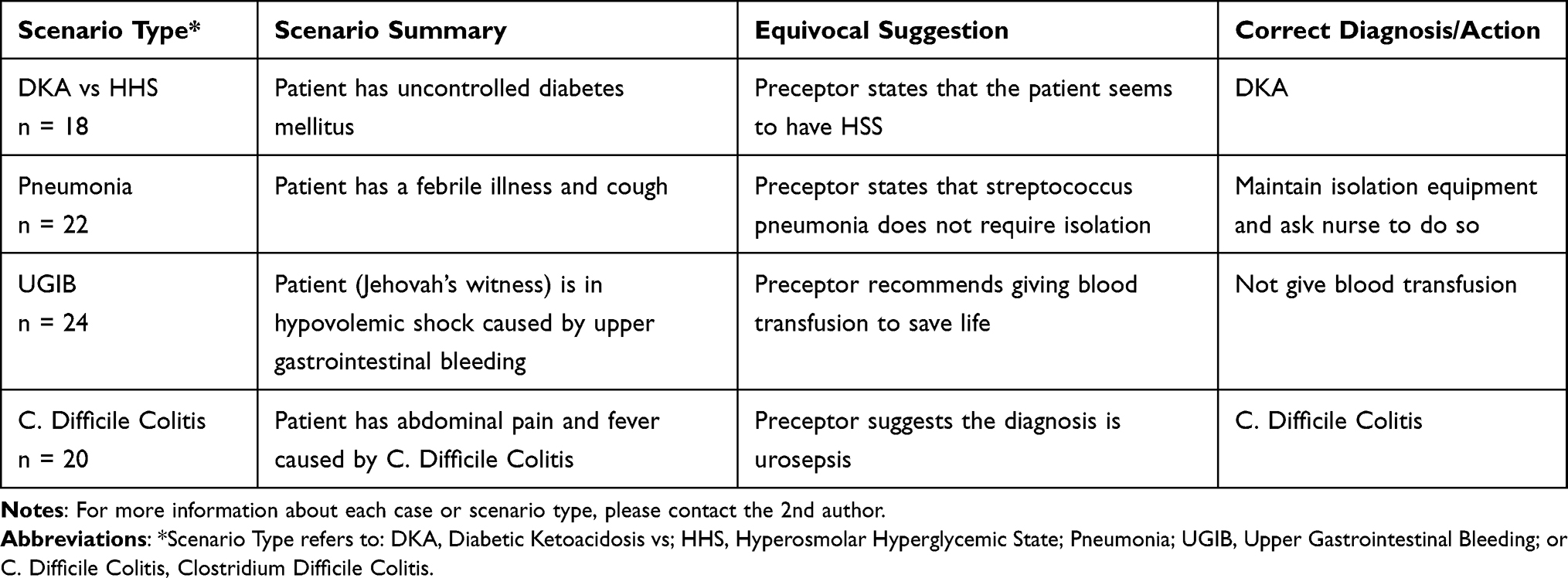 |
Table 1 Summary of the Simulation Scenarios |
The four simulation scenarios are part of the Internal Medicine simulation curriculum at this teaching hospital and were validated by a review of other Internal Medicine specialists. Additionally, learners had been on their rotation for three months to ensure that they would have had an opportunity in their clinical experiences to gain the level of knowledge that was presented in the simulation case. Pilot testing was conducted for each clinical scenario several times for feedback by learners and other clinical faculty. Also, the simulation educator rehearsed with colleagues and learners until the scripts were clear and met the specified learning objectives.
For each clinical scenario, the nurse greeted the learners and shared information about the simulated patient, and then the learners began conducting an examination and ordering tests. Then a preceptor entered the simulation approximately 10 minutes (M = 622.86 seconds, SD = 227.41) after the nurse greeted the learners. This amount of time allowed learners to become oriented to the case. The preceptor made an equivocal suggestion about the patient’s care, as shown in Table 1. Then the preceptor left the room to allow the learners to continue to manage the patient. The mean duration of the preceptors’ presence was almost three minutes (M = 151.12 seconds, SD = 75.91). Duration was measured from the time the preceptor came into the frame of the camera to the time they moved out of the frame. The simulation instructor then ended the simulation once the learners verbalized to the nurse or acted on their diagnosis or treatment plan. These videos were later observed by researchers to code conformity behaviors.
Measures
Since two learners participated in each case, each video was watched twice to code each learner’s behavior. The first two authors independently scored all of the videos: one a physician and the other a psychologist. Both authors have experience conducting research and teaching on the topic of conformity. Participants’ behaviours were coded as conforming if they stated, or acted in a manner consistent with, the equivocal suggestion made by the preceptor, as indicated in Table 1. For example, if a participant in the Diabetic Ketoacidosis (DKA) vs Hyperosmolar Hyperglycemic State (HHS) simulation case agreed and acted upon the diagnosis of HHS, as suggested by the preceptor, conformity was coded. Conversely, nonconformity was coded when they stated the correct diagnosis, as indicated in the last column on Table 1, or interpreted the patient’s information correctly. The non-physician coder was unable to determine if conformity occurred in 12 participants. Through discussion and watching videos more than once, a final decision was reached for those 12 by the physician rater. The rate of agreement was 0.63 according to Cohen’s kappa. This value is considered to be in the moderate to substantial range.17
Analyses
Descriptive statistics in the form of frequency counts are presented to describe the characteristics of the sample and the number of learners who did or did not conform. Chi-square tests were used to determine if conformity was related to these participant characteristics. The duration of the clinical scenario and the preceptor’s presence were analyzed using one-way analyses of variance to see if they differed according to conformity. Data were analyzed using SPSS 28 (International Business Machines).
Also, to capitalize on the opportunity to explore conformity behaviors that took place and their related contextual factors, we descriptively analyzed the video data post hoc. These descriptive analyses were conducted by the non-physician rater.
Results
Of the 42 learner dyads, 16 (38.10%) conformed to the equivocal information presented by the preceptors. There was no significant difference across type of case, sex, or learner education level, p > 0.05 (See Table 2). Duration of the preceptor’s presence in the room was similar for both the conforming (M = 153.28 seconds, SD = 100.06) and nonconforming groups (M = 159.88 seconds, SD = 75.37), F(1,82) = 0.12, p > 0.05.
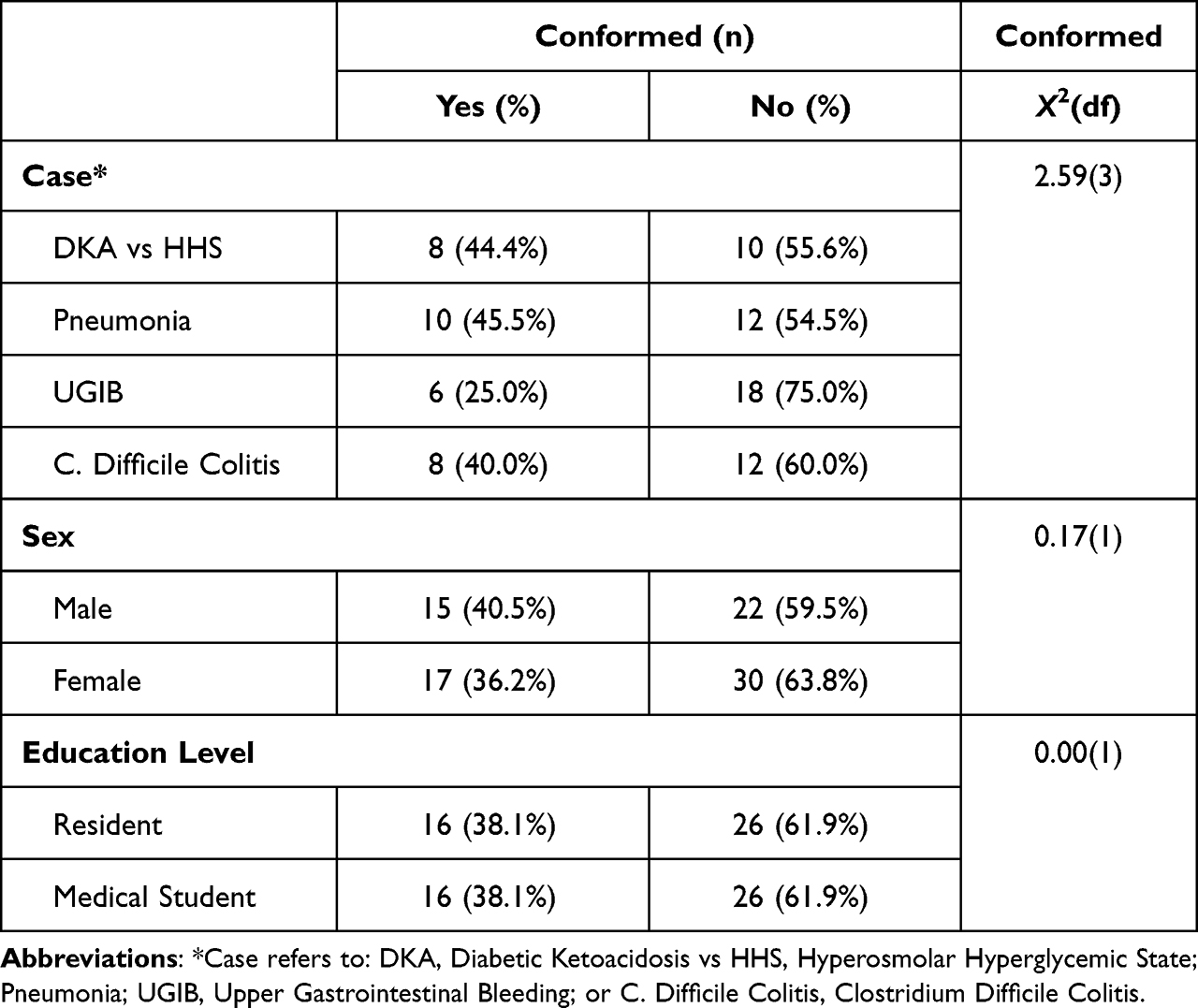 |
Table 2 Rate of Conformity (N = 84) |
Observed Interactions
As shown in Table 2, the same number of medical students and residents conformed. Upon closer inspection of these individuals, it was apparent that whenever the resident conformed, so did the medical student. Similarly, when the former did not conform, neither did the latter conform. Upon entering the simulation, the learners introduced themselves by stating their name and education level to the nurse. Thus, it was clear to everyone who was the learner with more education. In most cases, as is typical in real life, the resident took the lead in asking questions, requesting orders, suggesting diagnoses, and recommending treatment. Residents included the medical students by asking them questions, summarizing the information to them, asking them to look up information, asking them to call for assistance, or having them conduct tasks such as checking the monitor. These medical students also engaged in some initiative in all the above activities, but usually only when invited by the resident to do so or only while the resident was already engaged in an activity. The medical student also rarely suggested a diagnosis or treatment and more often talked with the patient offering comfort. This person also often followed the behaviors of the resident. For example, in one pneumonia case, the medical student started to remove her Personal Protective Equipment (PPE) when advised by the preceptor (thus conforming to the preceptor) but then noticed that the resident did not and so stopped removing it (thus changing to conform to the resident).
Regarding other interactions, attention promptly turned to the preceptor almost immediately upon entrance into the room. The preceptor spoke primarily to the learners, rather than the nurse or patient, and for most of the time while in the room. Thus, the learners turned their attention away from the nurse, patient, and each other to focus on the preceptor. Once the preceptor left, attention turned back to the others in the room. Interaction with the nurse involved asking questions about the patient, as well as making requests for tests and medications. Both learners interacted with the nurse in this manner, and the nurse did not make suggestions about diagnosis or treatment.
Discussion
Our study demonstrated that the simulation environment elicited clinical behaviors that reveal the hierarchy of professional interactions during a patient encounter. That is, more than one third of the learner dyads in the simulation conformed to a preceptor’s equivocal suggestion about a patient’s diagnosis or treatment. Also, all the medical students conformed to the residents’ decision of whether to conform. There were no differences in rates of conformity across learner sex or type of case.
There may be many reasons why over a third of the learners followed the equivocal suggestions made by the preceptors. First, learners may have felt uncertain of how to manage the case, perhaps believing that they lacked knowledge. They may have also felt anxious, knowing that learners in the other room were watching them and that the session was videotaped. Indeed, research has pointed to the fear or concern that individuals may have of showing failure, being rejected, or doing something wrong18 – all of which may be legitimate concerns to learners when interacting with preceptors before an audience of peers. In addition, characteristics of the simulation itself may have imposed pressure on learners to conform. That is, learners are aware that there is a limited amount of time allocated for the session, and agreement with the preceptor may be a rapid means of completing the assessment and treatment of the patient. Similarly, conformity may have been a means by which to manage the sense of distraction created by the preceptors. Also, the nurses in the simulation did not make any suggestions for how to proceed, which may not be typical in real healthcare settings, especially among those with considerable expertise. Future studies may include measures of these variables to see if they are contributing factors to conformity.
It was rather surprising that the rate of conformity was lower than found in previous studies.5–8 The present study used higher fidelity simulation to represent patient encounters during clinical rotations than any of our previous studies on conformity. This newest study also required demonstration of combined clinical decision-making, communication, and professional skills rather than isolated skills. By providing a strong sense of realism in these simulations, learners may have been able to deploy their problem-solving skills to think comprehensively about the case and be able to reconcile all of the facts to come to an informed decision. Therefore, the results may more closely approximate the extent of conformity that occurs during patient interactions.
Furthermore, perhaps most learners did feel some sense of safety in acting on their own understanding of the case. The emphasis placed at the beginning of the simulation on safety and learning may have provided some reassurance to learners. Also unique to the study is that residents were accompanied by medical students, which may have given them confidence and support to follow the information about the patient that would lead them to a decision contrary to the equivocal suggestion. In other studies, learners were alone in managing the pressure to conform.5–8 Finally, another reason for lower conformity in the present study could be because the conforming or nonconforming behavior occurred after the preceptor left. Thus, the direct pressure to acquiesce was minimized. This “behind the back nonconformity” may be a safe way for learners to manage dissenting information shared by preceptors.
Also surprising was the finding that all the medical students conformed to the residents. The former may have had less knowledge and confidence than the latter, making it easier for them to imitate someone in the learner-to-expert hierarchy who was more similar in status to them. This learner hierarchy was also reported by Grendar et al,9 who reported that learners felt pressure to conform to those with more years of education, but not to those with fewer years of education. The present study revealed that medical students may experience more pressure to conform to residents than to preceptors, as suggested by the learner who stopped removing their PPE after noticing that a senior learner did not remove it. Thus, the greatest pressure may be exerted by the person holding the next higher status in the hierarchy and not necessarily the person with the highest status. This possibility warrants further study.
Regarding limitations, participants were not randomly selected and were recruited from only one rotation site; thus, they may not represent behaviors of other learners. Also, raters were not blinded to the purpose of the study. Only male preceptors and female nurses were included in the study as they were on staff at the time of data collection, and future studies should not be restricted to this gender pattern. Lack of representativeness of the simulation to a naturalistic setting may have also affected the learners’ behaviors. The mannequin was clearly not a real person. Perhaps learners conformed because they knew there would be no harm to the patient. Also, simulation requires the “suspension of disbelief” and engagement of all participants to accept the simulated exercise as being real for the duration of the scenario. However, it is not a real clinical event; thus, these results may not be generalizable to real clinical settings. The number of people who conformed to the preceptors’ suggestions must be interpreted with caution, as it is possible that some learners may have believed the proposed recommendations for patient management were indeed correct. Interviews or comparison groups can be added in future studies to examine this possibility.
Conclusion
The major strength of this study is that we obtained behavioral evidence of how many learners may conform during patient case management. It is encouraging that the majority of learner dyads did not conform to equivocal suggestions, but it is discouraging that over a third of them actually did and that all of the medical students conformed to the residents. With the cumulative evidence of conformity through various research methods,5–9 it is becoming evident that it is ubiquitous in education. Thus, we call on medical educators to actively and directly teach learners (especially those with fewer years of education) and their preceptors that it is appropriate and even expected that they address how to manage equivocal information to ensure that physicians develop superior communication skills early in their practice.
Acknowledgments
The authors wish to thank all medical learners who participated in this research for taking the risk of learning through simulation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work nor sources of funding to declare.
References
1. Newton P, Bazemore A, Magill M, et al. The future of family medicine residency training is our future: a call for dialogue across our community. J Am Board Fam Med. 2020;33(4):636–640. doi:10.3122/jabfm.2020.04.200275
2. Altabbaa G, Beran TN, Oddone Paolucci E. Twelve tips for using simulation to teach about conformity behaviors in medical education. Med Teach. 2021;43(12):1360–1367. doi:10.1080/0142159X.2021.1879375
3. Asch SE. Social Psychology. Englewood Cliffs, NJ: Prentice-Hall; 1952.
4. Wright DB, Schwartz SL. Conformity effects in memory for actions. Mem Cognit. 2010;38(8):1077–1086. doi:10.3758/MC.38.8.1077
5. Beran TN, Drefs M, Kaba A, et al. Conformity of responses among graduate students in an online environment. Internet High Educ. 2015;25:63–69. doi:10.1016/j.iheduc.2015.01.001
6. Beran TN, McLaughlin K, Alansari A, et al. Conformity of behaviors among medical students: impact on performance of knee arthrocentesis in simulation. Adv Health Sci Educ. 2012;18(4):589–596. doi:10.1007/s10459-012-9397-5
7. Kaba A, Beran TN. The impact of peer pressure on the accuracy of reporting vital signs: an interprofessional comparison between nursing and medical students. J Interprof Care. 2016;30(1):116–122. doi:10.3109/13561820.2015.1075967
8. Kaba A, Beran TN, White D. Accuracy of interpreting vital signs in simulation. an empirical study of conformity between medical and nursing students. JIEP. 2016;3:9–18.
9. Grendar J, Beran T, Oddone-Paolucci E. Experiences of pressure to conform in postgraduate medical education. BMC Med Educ. 2018;18(1):4. doi:10.1186/s12909-017-1108-8
10. Abelson RP, Frey KP, Gregg AP. Experiments with People: Revelations from Social Psychology. New York, NY: Psychology Press; 2012. ISBN 9781135680145.
11. Pickering G. The purpose of medical education. BMJ. 1956;2(4985):113–116. doi:10.1136/bmj.2.4985.113
12. Royal College of Physicians and Surgeons of Canada. Terminology in medical education project; 2012. Available from: http://www.royalcollege.ca/rcsite/educational-initiatives/terminology-medical-education-project-e.
13. Calhoun AW, Boone MC, Porter MB, Miller KH. Using simulation to address hierarchy-related errors in medical practice. Perm J. 2014;18(2):14–20. PMID: 24867545; PMCID: PMC4022552. doi:10.7812/TPP/13-124
14. Beran TN, Drefs M, Altabbaa G, Al Harbi N, Al Baz N, Oddone Paolucci E. Observations of conformity in the health professions. World Academy of Science, Engineering, and Technology. 2022;16(12):762–767.
15. Lamé G, Dixon-Woods M. Using clinical simulation to study how to improve quality and safety in healthcare. BMJ Simul Technol Enhanc Learn. 2020;6(2):87–94. PMID: 32133154; PMCID: PMC7056349. doi:10.1136/bmjstel-2018-000370
16. Al Harbi N Assessment of Conformity: instrument Development. Doctoral dissertation. Calgary, Canada: University of Calgary; 2017. Available from: https://prism.ucalgary.ca/handle/1880/100031/discover.
17. Cohen J. A coefficient of agreement for nominal scales. Educ Psychol Meas. 1960;20(1):37–46. doi:10.1177/001316446002000104
18. Harris N. Australian National University. Regulatory Institutions Network. Shame, Ethical Identity and Conformity Lessons from Research on the Psychology of Social Influence. Canberra: Regulatory Institutions Network; 2007. Available from: http://pandora.nla.gov.au/pan/67415/200801230746/ctsi.anu.edu.au/publications/OccPaper12.pdf.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.