")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Occupational Risk Factors for Physical and Mental Health in Primary Healthcare Providers: A National Cross-Sectional Survey from 62 Urban Communities in China
Authors Yin T, Lu Y, Xiong W, Yu C, Yin D, He H
Received 18 December 2022
Accepted for publication 14 March 2023
Published 18 March 2023 Volume 2023:16 Pages 751—762
DOI https://doi.org/10.2147/JMDH.S401914
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Tao Yin,1,* Yan Lu,2,* Wei Xiong,3,* Chengdong Yu,4 Delu Yin,5 Huijing He6
1Department of Technology, Capital Institute of Pediatrics, Beijing, People’s Republic of China; 2Department of Cardiology, First Affiliated Hospital of Nanjing Medical University, Nanjing, People’s Republic of China; 3Department of Gynecology Endocrine & Reproductive Center, National Clinical Research Center for Obstetric & Gynecologic Diseases Department of Obstetrics and Gynecology, Peking Union Medical College Hospital, Peking Union Medical College/Chinese Academy of Medical Sciences, Beijing, People’s Republic of China; 4Department of Growth and Development, Capital Institute of Pediatrics, Beijing, People’s Republic of China; 5Department of Child Health Care, Capital Institute of Pediatrics, Beijing, People’s Republic of China; 6Department of Epidemiology and Statistics, Institute of Basic Medical Sciences, Chinese Academy of Medical Sciences & School of Basic Medicine, Peking Union Medical College, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Huijing He, Department of Epidemiology and Statistics, Institute of Basic Medical Sciences, Chinese Academy of Medical Sciences & School of Basic Medicine, Peking Union Medical College, 5 Dongdansantiao, Dongcheng District, Beijing, 100005, People’s Republic of China, Tel +8615010086743, Email [email protected] Delu Yin, Department of Child Health Care, Capital Institute of Pediatrics, 2 Yabao Road, Chaoyang District, Beijing, 100020, People’s Republic of China, Tel +8613810349722, Email [email protected]
Purpose: To understand the physical and mental health status of primary healthcare providers (PHPs) including physicians, nurses and other staff and the workplace risk factors for depression, anxiety and intention-to-leave.
Patients and Methods: In December 2021, a national cross-sectional survey was conducted from 62 urban communities in China, and all PHPs were invited to complete a standardized questionnaire. Information on demographic, health-related lifestyle, cardiovascular risk factors and physical health status, occupational stress and intention-to-leave was collected. Depression and anxiety were assessed using the Zung Self-Rating Anxiety/Depression Scale (SAS/SDS).
Results: A total of 4901 PHPs were included. 67.0% males currently drank alcohol vs 25.3% in females; 36.0% males currently smoked cigarettes vs 1.4% in females. Notably, more than half males were overweight or obese, but this proportion was 24.2% in females. The prevalence of chronic diseases, including hypertension, diabetes, dyslipidemia, non-alcoholic fatty liver disease, gout, and disease clustering were higher in males than in females. The prevalence of depression and anxiety were high, 50% had depression, of whom 15.6% had moderate/severe depression. Over 15% participants had varied levels of anxiety, and approximately 4% had moderate/severe anxiety. PHPs who aged 18– 29 (OR: 1.31, 95% CI: 1.05– 1.64), were males (OR: 1.34, 95% CI: 1.14– 1.57), with lower professional title (comparing with staff with senior title, the ORs of the intermedium, junior and none were 1.83, 2.18 and 2.49, respectively), took charge in nursing (OR: 1.41, 95% CI: 1.20– 1.65), with higher perceived stress level (OR: 1.82, 95% CI: 1.41– 2.34), and suffering from severe fatigue (OR: 2.55, 95% CI: 1.99– 3.27) were more likely to have depression. Likewise, PHPs who were younger, with intermedium professional title, had higher perceived pressure level, and higher fatigue levels were more likely to have anxiety.
Conclusion: The mental health of PHPs is worrisome, with a high burden of chronic diseases and occupational risk factors. Younger PHPs, nurses, and those with higher levels of work pressure and fatigue are more vulnerable to psychological problems. The high prevalence of intention-to-leave calls for strategies that relieve the workplace stress and enhance the human resource capability.
Keywords: depression, anxiety, stress, intention-to-leave, COVID-19, primary healthcare
Introduction
Stress, depression, and anxiety are key challenges for psychologists, psychiatrists, and behavioural scientists globally.1 Depression is one of the most common behavioural disorders associated with low mood, guilt, loss of interest, worthlessness, decreased energy and concentration, etc. Major depression ranks amongst the most burdensome health conditions. Depression is associated with diminished quality of life, and even a higher risk of mortality.2 Anxiety is a disorder associated with fear and uncertainty and is often accompanied by fatigue, restlessness, and palpitations.1 Globally, the prevalence of depression and anxiety are between 10% and 20%.2 Healthcare providers, such as doctors and nurses, are affected by a variety of stresses in the workplace and thus are vulnerable to suffering from depression and anxiety. In the past few years, the COVID-19 pandemic has caused severe health outcomes worldwide. Depression, anxiety, burnout and post-traumatic stress disorder were commonly observed in healthcare providers, especially in those fighting at the frontline, being a nurse, with longer shifts, etc.3 In addition, these psychological issues could have associations with decreased quality of life and suicidality.4–6 Furthermore, depression and anxiety can lead to negative effects on health and impair the productivity, work performance and availability of health human resource. Previous studies have revealed a correlation between mental health and physical health. For example, in a general Chinese population, psychological symptoms were more prevalent among individuals with noncommunicable chronic diseases (NCD).7 NCD patients had a higher risk of depression and anxiety.8 Therefore, in addition to monitoring mental health, it is also important to improve physical health and early identify NCD high-risk population.
Globally, healthcare workers are at the center of the fight against COVID-19 pandemic in the last few years. As part of China’s healthcare reform effort to provide citizens with universal access to healthcare, the primary healthcare, delivered by community health centers in urban areas, has received considerable attention recently.9 Along with the rapid urbanization and aging process in China, the effectiveness and quality of primary healthcare is of increased importance. Although there are studies exploring the mental health status of primary healthcare providers (PHPs) in China,10–12 most were conducted in rural or limited geographic areas. Furthermore, since there have been concerns about the quality of PHPs and its insufficient continuity in China,9 it is necessary to understand the occupational factors that may influence the staff’s work passion at community healthcare centers. Our previous study, which was conducted among 286 primary healthcare providers in limited areas in China, has revealed a moderate prevalence (43.7%) of intention-to-leave.13 However, more representative data covering a broad range of geographic areas and diverse study populations, especially those fight against COVID-19 pandemic in the primary healthcare settings, is urgently needed for policymakers to initiate targeted health enhancing strategies.
Therefore, to understand the physical and mental health status of PHPs, as well as to explore the potential occupational factors related to work continuity, we conducted a nationwide survey in 2021, enrolling PHPs from 62 urban communities in mainland China.
Materials and Methods
Study Population
An online cross-sectional survey was conducted in December 2021, using a multistage-stratified cluster sampling method, 62 urban community healthcare centers were selected from the Mainland China. In the first sampling stage, using typical sampling method, we selected one or two provinces from the North, South, West, and East China and finally seven provinces were selected. In the second stage, two cities, one is the provincial capital city, and another is a relatively small city, in each province, were selected. In the third stage, districts were selected based on the local GDP in each city (a total of 62 districts with varied levels of economic development). In the final stage, one healthcare centers in the selected districts were randomly selected, and finally, there were 62 community healthcare centers included. All staff in the selected settings were asked to finish an online questionnaire survey voluntarily based on WeChat.
The inclusion criteria for participant enrolment were as follows: 1) aged 18 or above; 2) has been worked as PHPs at the selected community healthcare centers for at least one year; 3) major in medicine, nursing, public health, or other medical related specialties. The exclusion criteria were people who cannot complete the online survey.
A meta-analysis has shown a depression rate of 22.8 and anxiety rate of 23.2% among healthcare workers.14 To ensure statistical efficacy, we used a lower prevalence of 22% to estimate the minimum required sample size in the study. The calculation was according to the following formula:

Alpha (α) is the significance level, p is the prevalence of depression, q equals 1-p, and d is the error tolerance, which can be estimated as 0.10 × p. To reach a significance level of 0.05 and error tolerance of 0.10p, the estimated minimum sample size is 1362. We added an additional 20% to the sample size, factoring in possible non-compliance. Finally, 4907 staff working in primary healthcare settings were recruited, and 4901 completed the survey. The sample size can satisfy the statistical power requirement.
The study was carried out in accordance with the Declaration of Helsinki. Ethical approval was obtained from the Bioethical Committee of Capital Pediatric Institute (SHERLL2020017). All participants were told the time of the survey, which data were stored and where and for how long, who the investigator was, and the purpose of the study, and provided informed consent before the survey.
Measurement and Definitions
An export panel was established to discuss the usability and technical functionality of the electronic questionnaire, and a pre-investigation was conducted before the formal survey. A standardized questionnaire was finally designed after consultation with epidemiologists, physicians and psychologists. Demographic information including sex, age, educational level, income, health-related lifestyle (cigarette smoking, alcohol drinking), height, weight, and personal disease history (hypertension, diabetes, dyslipidemia, non-alcoholic fatty liver disease and gout) was collected. Overweight and obesity were defined as 24 ≤ BMI < 28 kg/m2, and BMI ≥ 28 kg/m2, according to the classification criteria for Chinese people.15,16
Occupational information was collected, including the rank of profession title (none/primary/medium/senior), professional areas (doctor, nurse, pharmacist/administration/others), fatigue level, perceived stress, intention-to-leave the jobs, etc. In addition, information on workloads related to COVID-19 prevention and control was collected.
Zung Self-Rating Anxiety/Depression Scale (SAS/SDS) was used to measure depression and anxiety. As short self-rated scales that can be used to assess the psychological and somatic symptoms of anxiety depression, the SAS/SDS has been widely used in the field of psychiatry.17,18 Both of them contain 20 items and were designed based on the diagnostic criteria for anxiety and depression. Users rate each item according to their feelings during the past few days using a 4-point Likert Scale. The original sum score of SAS/SDS ranges from 20 to 80 and then is converted to SAS/SDS index and further classified into light, moderate or severe anxiety/depression.19 To learn the current need for psychological health support, we added a related question in the online survey as “Do you need professional psychological support?”, with multiple choices including “Yes, I have sought for help already”. “Yes, but I have not sought for help yet”, “I don’t care”, “No, I am capable of selfcare” and “No, I am in good mental health”.
Statistical Analyses
Categorical variables were shown as frequencies and proportions. Chi-square tests were used to compare the prevalence of depression and anxiety among subgroups. Multivariable logistic regression models were used to explore factors associated with depression and anxiety, respectively. In addition, as there may be age-varied associations, we performed age-stratified multivariable logistic regression analyses. Adjusted odds ratios (ORs) with their 95% confidence intervals (CIs) were reported. A p-value of less than 0.05 (two-tailed) was considered statistically significant. Analyses were performed using SAS (version 9.4, SAS Institute Inc., Cary, NC, USA).
Results
Basic Characteristics
A total of 4901 PHPs from 62 urban communities in China were included in the final analyses. The average age was 36.45 (standard deviation: 9.70), and 80.6% were females. Most participants were married (75.4%), had a college educational level (52.5%), with a personal annual income less than 144,000 CHY (77.6%, 1 CHY≈0.14 USD), without or only with a junior professional title (64.5%), major in clinical medicine or nursing (64.5%), had been working for more than ten years (56.2%). More details are available in Table 1.
 |
Table 1 Basic Characteristics of Adults from 62 Communities in Mainland China (n = 4901) |
Cardiometabolic Risk Factors and Comorbidity
The age and sex-specific prevalence of lifestyle risk factors, such as alcohol drinking, cigarette smoking, self-reported hypertension, diabetes, dyslipidemia, non-alcoholic fatty liver disease, gout and disease clustering are shown in Figure 1. Men and women had significant differences in alcohol drinking and cigarette smoking. 67.0% males currently drank alcohol vs 25.3% in females; 36.0% males currently smoked cigarettes vs 1.4% in females. Notably, 56.11% males were overweight or obese, but this proportion was 24.22% in females. The self-reported prevalence of chronic diseases, including hypertension, diabetes, dyslipidemia, non-alcoholic fatty liver disease, gout, and disease clustering were higher in males than in females (Figure 1).
 |
Figure 1 The age- and sex-specific self-reported prevalence of cardiovascular risk factors, chronic diseases, and disease clustering among primary healthcare providers. The red lines represent the fitted age trend curves. Abbreviation: NAFLD, Non-alcoholic fatty liver disease. |
Mental Health, Work Stress and Fatigue
The prevalence of depression, anxiety, workload, fatigue, perceived stress, and pressure caused by COVID-19 related work are presented in Table 2. In general, the prevalence of depression and anxiety were high, approximately half of the participants had depression, of whom over 15% had moderate/severe depression. More than 15% participants had varied levels of anxiety and around 4% had moderate/severe anxiety (Table 2).
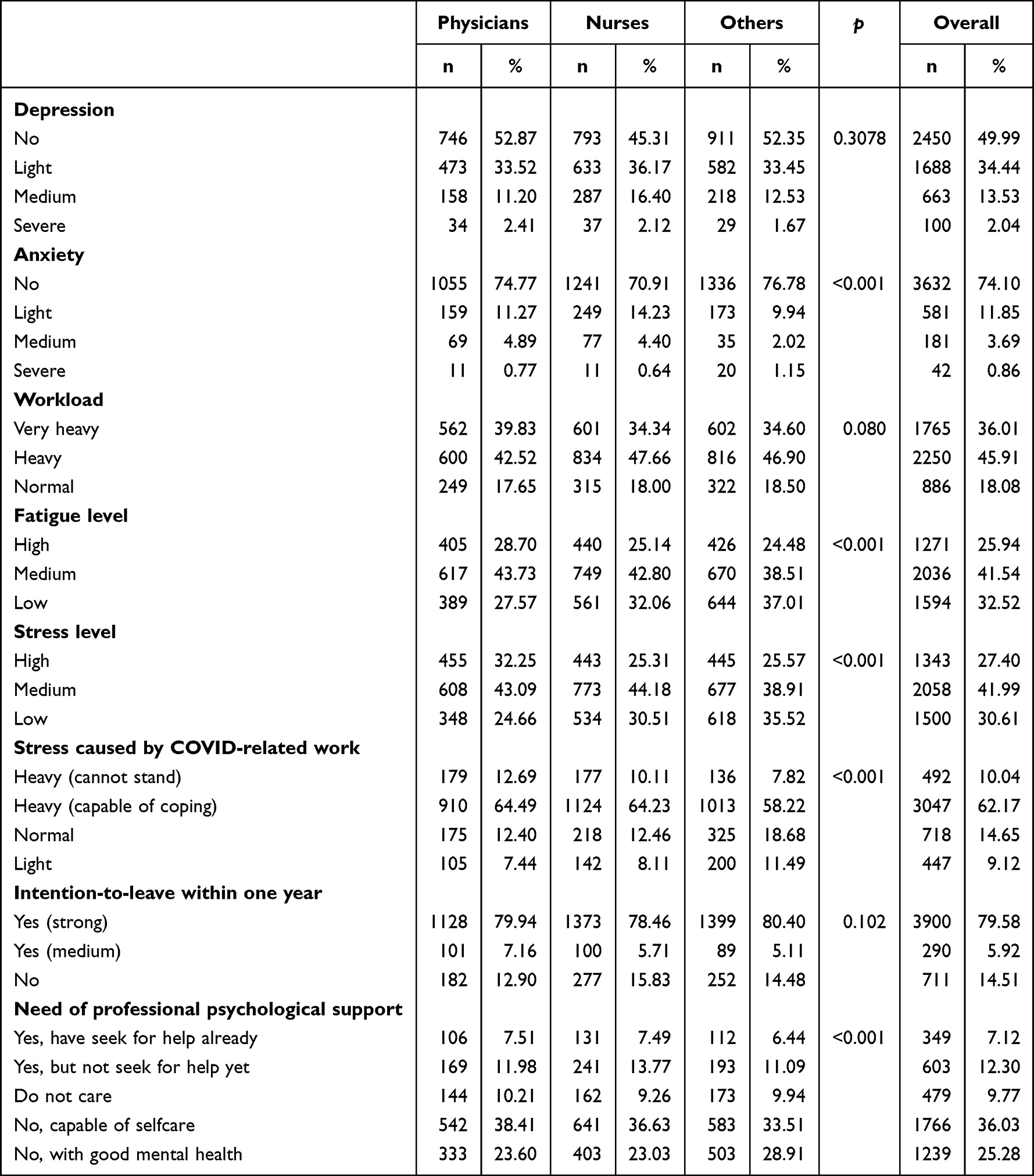 |
Table 2 Mental Health, Work Stress and Passion Among the Primary Healthcare Providers in the Study |
Over 80% participants perceived a heavy workload, and 26% had a high level of fatigue. 26% had a heavy level of the perceived stress. Notably, the stress caused by COVID-19 related work was remarkably high, over 70% subjects perceived a heavy stress level. Unfortunately, only 12.30% had ever sought help from a professional psychologist. In addition, nearly 80% of the PHPs had intention-to-leave. The mental health and occupational factor status had disparities in different professional majors (Table 2).
Work Related to COVID-19 Prevention and Control
During the COVID-19 epidemic, most PHPs were involved in the prevention and control work. Most participants (60.3%) were involved in the COVID nucleic acid tests, and this proportion was higher among nurses (71.6%), subjects with an intermediate professional title (65.7%), and those had worked for 5 to 9 years (68.6%). More details can be found in Table S1 and Figure S1.
Factors Associated with Depression and Anxiety
The associations between demographic, occupational related factors and mental health are shown in Table 3. Individuals aged 18–29 (OR: 1.31, 95% CI: 1.05–1.64), were males (OR: 1.34, 95% CI: 1.14–1.57), with lower professional title (comparing with staff with senior title, the ORs of the intermedium, junior and none were 1.83, 2.18 and 2.49, respectively), took charge in nursing (OR: 1.41, 95% CI: 1.20–1.65), with higher perceived stress level (OR: 1.82, 95% CI: 1.41–2.34), and suffering from heavy fatigue level (OR: 2.55, 95% CI: 1.99–3.27) were more likely to have depression. Heavy workload was found to be associated with depression in an opposite way, with the OR (95% CI) of 0.67 (0.54–0.85).
 |
Table 3 Associated Factors of Depression and Anxiety in Primary Healthcare Providers |
Similar to the risk factors of depression, PHPs who were younger, with intermedium professional title, had higher perceived pressure level, and higher fatigue levels were more likely to have anxiety. Workload level was also found to be inversely associated with anxiety (Table 3).
Age-Stratified Analyses on the Associations
The occupational factors associated with depression and anxiety in the <40 and ≥40 age groups are presented in Figure 2. Subjects who perceived a heavy level of fatigue and stress, and were males, were more likely to have depression in both age groups. However, disparities were found in the associations between factors such as professional majors, rank of professional title and work load with depression and anxiety. For instance, in people aged 40 and over, lower professional title was positively associated with depression, compared to the senior group, the ORs (95% CI) for medium, junior and none title were 1.93 (1.43–2.62), 2.10 (1.51–2.90) and 3.20 (2.15–4.75), respectively. However, this positive association was not observed in the <40 year group. Likewise, compared to people taking other jobs, nurses younger than 40 years were more likely to have depression (OR: 1.58, 95% CI: 1.29–1.93), but this association was not found in the aged 40 and above group (Figure 2).
 |
Figure 2 The age-stratified analysis of the associated factors for depression and anxiety in primary healthcare providers. (A) depression; (B) anxiety. Abbreviations: OR, odds ratio; CI, confidence interval. |
Age-stratified associated factors of anxiety among the PHPs were similar to depression. More details can be found in Figure 2.
Discussion
To the best of our knowledge, this is the first and largest nationwide survey on health status, especially the occupational risk factors for physical and mental health among PHPs in urban China. Our study suggested that either the physical or mental health status in PHPs is alarming, with a high burden of chronic diseases and occupational risk factors. Notably, the work continuity is worrisome, and strategies that effectively deal with high work stress and enhance the human resource capability are urgent.
Even though some studies have explored the PHPs’ physical health and psychological well-being,10–12 our study looked deeper into the occupational factors that contribute to these health outcomes. The participants recruited during the COVID-19 pandemic were observed with a high burden of fatigue and perceived stress and a remarkably high proportion of intention-to-leave jobs, which is a great concern for the sustainability of human resources in primary health care settings.
Our study revealed a high prevalence of chronic disease and multiple modifiable risk factors in the PHPs. Although the prevalence of NCDs in the Chinese population has been well documented, the NCD status in PHPs is still unclear. Compared with the general population, PHPs in this study had lower self-reported prevalence of hypertension, diabetes, dyslipidemia and gout.20–23 It may be partially attributed to the lower prevalence based on self-reported data or better self-health management among healthcare professionals. However, the self-reported proportions of risk factors for NCDs were not optimistic. In particular, the alcohol drinking and overweight/obesity prevalence were extremely high. A latest meta-analysis suggested that alcohol consumption for recreational purposes significantly increased the risk of work-related accidents.24 In addition, the lifestyle modifiable risk factors have been proved to contribute substantially to chronic disease.25–27 Paired with the high prevalence of common chronic diseases, the need for health promotion and intervention among PHPs is imperative.
Another notable finding of this study is that the psychological wellbeing of PHPs in urban China is worrisome. Over half of the subjects suffered from depression, among which over 15% had moderate/severe depression, and 15% suffered from anxiety. Previous studies explored the mental health issues among healthcare providers.1,10,28–30 A meta-analysis showed that a considerable proportion of healthcare providers experience mood and sleep disturbances during the COVID-19 pandemic, and the pooled prevalence of depression and anxiety were 22.8% and 23.2%, respectively.14 A study in Swiss suggested that the reduced psychiatric emergency department admissions during the pandemic may be due to living alone and more severe psychopathologies, which raised the concern of access to mental health care.31 Nevertheless, none of these studies examined the mental health condition among PHPs. Data reported in this study highlights the need for psychological support among the previously neglected PHPs.
Revealed by this study, staff who were younger, with a lower professional title level, took charge in nursing, with a high level of perceived work stress and fatigue was more likely to have depression and anxiety. Although ageing with comorbidity of chronic diseases may reduce the levels of functioning and mental health,32 our study suggested that younger people were more likely to be affected by depression and anxiety. Previous study has revealed that younger people were more vulnerable to depression and anxiety during the COVID-19 pandemic.33 Younger people, who may have a lower professional title rank, may have to deal with more tedious and time-consuming work and lead to fatigue and even burnout, thus eventually resulting in psychological distress.34 Age-stratified analyses suggested a potential medication effect of age on the associations. Professional title rank was more likely to affect staff older than 40, and people with a lower professional title level were more vulnerable to depression and anxiety. Lower professional title may be related to less income and more stress in keeping the family fed and pursue career promotion, especially in the pandemic time.
Work stress is a common problem among the health personnel worldwide. A study conducted among PHPs in Spain reported that half of the subjects appeared to suffer from a high level of work-related stress.35 Excess health care pressure, increasingly demanding users for health needs and lack of support from managers and their superiors may become the source of stress.35 In response to the spread of COVID-19, China adopted the “Dynamic COVID-zero” strategy from Aug 2021.36 Most of our study sites were under multiple small-size outbreaks during the survey. As the pandemic coping strategy requires extensive community involvement, the workload and stress can be expected to be extremely high. PHPs who took charge of admitting and managing for suspected COVID-19 patients have been subjected to plenty of both individual and organizational stresses that may have an adverse impact on their mental health and job satisfaction. In the current study, most PHPs were involved in COVID-19 related work, which may cause additional stress beyond their routine duty. Our study emphasized the need to improve health with an integral form of tackling the mental and physical consequences of work stress in primary healthcare settings. Recognizing stressors and thereafter conducting targeted periodic trainings and psychological support activities will be an imperative and effective step towards prevention of mental disorders.
The high proportion of perceived fatigue in this study raised the concern of burnout prevention among staff working in primary healthcare settings. Burnout has been identified as an important occupational hazard in medical professions for many years but is often overlooked.37 Some studies have reported that, occupational factors, such as heavy workload and working hours, are associated with a high risk of suicide among healthcare professionals.4 Therefore, understanding the healthcare providers’ psychological well-being and related occupational risk factors and attending to it during system redesign may benefit them with long-term health welfare.
Our study indicated that PHPs who took charge of nursing were more likely to be depressive, especially in people younger than 40. A meta-analysis reported that the combined incidence of depression among nurses in the COVID-19 pandemic was 22% and 29% in anxiety.38 Nurses have to confront numerous problems which have an effect on the performance of their work and mental health.39–41 Increased workload dramatically worsened the existing nursing personnel shortage and thereafter led to increased stress and fatigue.
Worsening primary care provider workforce shortage threats many countries around the world. Unfortunately, our study revealed a high proportion of intention-to-leave the jobs, which raises great concern on work continuity. Compared to tertiary hospitals, there are still widespread gaps in the quality of healthcare, insufficient training and educational opportunities for the PHPs.9 The need for career promotion, better education and training opportunities, along with extensive work stress, may trigger the resignation. Availability of psychological support is important and could be a possible way to address barriers that drive providers burnout and contribute to providers' attrition.37,42
Limitations of this study are first in the nature of the online survey and cross-sectional design, which limited the causal inference between risk factors and outcomes, such as the inverse association between workload and mental health. Second, as the chronic disease information was based on self-report, there could be underestimations and recall bias. Third, this study was conducted in China, findings may not be appropriate to apply to other countries. Nevertheless, the main strength of our study should also be acknowledged: first is in its large and representative sample from 62 communities in urban China, and the findings could provide key information for the government and policymakers to optimize current strategies to improve mental health of PHPs; second, we collected various health-related information, including cardiovascular risk factors, chronic disease and disease clustering profile, thus could provide more comprehensive assessment on health wellbeing of PHPs.
Conclusion
Our study revealed an alarming mental health condition among primary healthcare providers in China and a comorbid high prevalence of chronic disease and cardiovascular risk factors. PHPs who were younger, took nursing jobs, and had high levels of fatigue and work pressure are at high-risk of psychological disorders. Furthermore, with high levels of work stress, perceived fatigue and intention-to-leave, the work continuity is worrisome.
Acknowledgments
The authors thank the participants, researchers and interviewers in this study.
Funding
This study was funded by the National Natural Science Foundation of China (82003531), Capital’s Funds for Health Improvement and Research, CFH (2022-2G-4211), National High level Hospital Clinical Research Funding (2022-PUMCH-A-235) and Public service development and reform pilot project of Beijing Medical Research Institute (BMR2021-3). The funders had no role in the design of the study and collection, analysis, and interpretation of data and in writing the manuscript.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Salari N, Khazaie H, Hosseinian-Far A, et al. The prevalence of stress, anxiety and depression within front-line healthcare workers caring for COVID-19 patients: a systematic review and meta-regression. Hum Resour Health. 2020;18:100. doi:10.1186/s12960-020-00544-1
2. Vilagut G, Forero CG, Barbaglia G, et al. Screening for depression in the general population with the center for epidemiologic studies depression (CES-D): a systematic review with meta-analysis. PLoS One. 2016;11:e155431. doi:10.1371/journal.pone.0155431
3. Chigwedere OC, Sadath A, Kabir Z, Arensman E. The impact of epidemics and pandemics on the mental health of healthcare workers: a systematic review. Int J Env Res Pub He. 2021;18:6695. doi:10.3390/ijerph18136695
4. Dutheil F, Aubert C, Pereira B, et al. Suicide among physicians and health-care workers: a systematic review and meta-analysis. PLoS One. 2019;14:e226361. doi:10.1371/journal.pone.0226361
5. Nobari H, Fashi M, Eskandari A, Villafaina S, Murillo-Garcia Á, Pérez-Gómez J. Effect of COVID-19 on health-related quality of life in adolescents and children: a systematic review. Int J Environ Res Public Health. 2021;18:4563. doi:10.3390/ijerph18094563
6. Amerio A, Lugo A, Stival C, et al. COVID-19 lockdown impact on mental health in a large representative sample of Italian adults. J Affect Disorders. 2021;292:398–404. doi:10.1016/j.jad.2021.05.117
7. Liu X, Cao H, Zhu H, et al. Association of chronic diseases with depression, anxiety and stress in Chinese general population: the CHCN-BTH cohort study. J Affect Disorders. 2021;282:1278–1287. doi:10.1016/j.jad.2021.01.040
8. Wu T, Jia X, Shi H, et al. Prevalence of mental health problems during the COVID-19 pandemic: a systematic review and meta-analysis. J Affect Disord. 2021;281:91–98. doi:10.1016/j.jad.2020.11.117
9. Li X, Krumholz HM, Yip W, et al. Quality of primary health care in China: challenges and recommendations. Lancet. 2020;395:1802–1812. doi:10.1016/S0140-6736(20)30122-7
10. Chen J, Liu X, Wang D, et al. Risk factors for depression and anxiety in healthcare workers deployed during the COVID-19 outbreak in China. Soc Psych Psych Epid. 2021;56:47–55. doi:10.1007/s00127-020-01954-1
11. Xu W, Pan Z, Li Z, et al. Job burnout among primary healthcare workers in rural china: a multilevel analysis. Int J Environ Res Public Health. 2020;17(3):727. doi:10.3390/ijerph17030727
12. Zheng R, Zhou Y, Fu Y, et al. Prevalence and associated factors of depression and anxiety among nurses during the outbreak of COVID-19 in China: a cross-sectional study. Int J Nurs Stud. 2021;114:103809. doi:10.1016/j.ijnurstu.2020.103809
13. Yin T, Yin D, He H, et al. The awareness and attitude of contracted service among general medical practitioners in community health service centers in Urban China: a cross-sectional study. Front Public Health. 2021;9:572311. doi:10.3389/fpubh.2021.572311
14. Pappa S, Ntella V, Giannakas T, et al. Prevalence of depression, anxiety, and insomnia among healthcare workers during the COVID-19 pandemic: a systematic review and meta-analysis. Brain Behav Immun. 2020;88:901–907. doi:10.1016/j.bbi.2020.05.026
15. Zhou BF. Predictive values of body mass index and waist circumference for risk factors of certain related diseases in Chinese adults – study on optimal cut-off points of body mass index and waist circumference in Chinese adults. Biomed Environ Sci. 2002;15:83–96.
16. He H, Pan L, Wang D, et al. Fat-to-muscle ratio is independently associated with hyperuricemia and a reduced estimated glomerular filtration rate in Chinese adults: the China National Health Survey. Nutrients. 2022;14(19):4193. doi:10.3390/nu14194193
17. Jokelainen J, Timonen M, Keinanen-Kiukaanniemi S, et al. Validation of the Zung self-rating depression scale (SDS) in older adults. Scand J Prim Health Care. 2019;37:353–357. doi:10.1080/02813432.2019.1639923
18. Mormont E, Jamart J, Jacques D. Symptoms of depression and anxiety after the disclosure of the diagnosis of Alzheimer's disease. J Geriatr Psychiatry Neurol. 2014;27:231–236. doi:10.1177/0891988714532021
19. Zung WW. A self-rating depression scale. Arch Gen Psychiatry. 1965;12:63–70. doi:10.1001/archpsyc.1965.01720310065008
20. Wang Z, Chen Z, Zhang L, et al. Status of hypertension in China. Circulation. 2018;137:2344–2356. doi:10.1161/CIRCULATIONAHA.117.032380
21. Wang L, Peng W, Zhao Z, et al. Prevalence and treatment of diabetes in China, 2013–2018. JAMA. 2021;326:2498–2506. doi:10.1001/jama.2021.22208
22. Lu Y, Zhang H, Lu J, et al. Prevalence of dyslipidemia and availability of lipid-lowering medications among primary health care settings in China. JAMA Network Open. 2021;4(9):e2127573. doi:10.1001/jamanetworkopen.2021.27573
23. Tang YM, Zhang L, Zhu SZ, et al. Gout in China, 1990–2017: the global burden of disease study 2017. Public Health. 2021;191:33–38. doi:10.1016/j.puhe.2020.06.029
24. Bufano P, Poma AM, Frumento S, Persechino B, Menicucci D, Laurino M. Gemignani, A Meta-analytic study on substance intake and work-related accidents calls for attention to bio-psycho-social factors. Neurosci Biobehav Rev. 2023;144:104987. doi:10.1016/j.neubiorev.2022.104987
25. Gou J, Wu H. Secular trends of population attributable risk of overweight and obesity for hypertension among Chinese adults from 1991 to 2011. Sci Rep. 2021;11:6371. doi:10.1038/s41598-021-85794-2
26. He H, Pan L, Ren X, et al. The Effect of body weight and alcohol consumption on hyperuricemia and their population attributable fractions: a National Health Survey in China. Obes Facts. 2022;15:216–227. doi:10.1159/000521163
27. He H, Guo P, He J, et al. Prevalence of hyperuricemia and the population attributable fraction of modifiable risk factors: evidence from a general population cohort in China. Front Public Health. 2022;10:936717. doi:10.3389/fpubh.2022.936717
28. Firew T, Sano ED, Lee JW, et al. Protecting the front line: a cross-sectional survey analysis of the occupational factors contributing to healthcare workers’ infection and psychological distress during the COVID-19 pandemic in the USA. BMJ Open. 2020;10:e42752. doi:10.1136/bmjopen-2020-042752
29. Mosheva M, Hertz Palmor N, Dorman Ilan S, et al. Anxiety, pandemic-related stress and resilience among physicians during the COVID‐19 pandemic. Depress Anxiety. 2020;37:965–971. doi:10.1002/da.23085
30. Chew N, Lee G, Tan B, et al. A multinational, multicentre study on the psychological outcomes and associated physical symptoms amongst healthcare workers during COVID-19 outbreak. Brain Behav Immun. 2020;88:559–565. doi:10.1016/j.bbi.2020.04.049
31. Ambrosetti J, Macheret L, Folliet A, et al. Impact of the COVID-19 pandemic on psychiatric admissions to a large Swiss emergency department: an observational study. Int J Environ Res Public Health. 2021;18:1174. doi:10.3390/ijerph18031174
32. Yang H, Deng Q, Geng Q, et al. Association of self-rated health with chronic disease, mental health symptom and social relationship in older people. Sci Rep. 2021;11:14653. doi:10.1038/s41598-021-94318-x
33. Varma P, Junge M, Meaklim H, et al. Younger people are more vulnerable to stress, anxiety and depression during COVID-19 pandemic: a global cross-sectional survey. Prog Neuropsychopharmacol Biol Psychiatry. 2021;109:110236. doi:10.1016/j.pnpbp.2020.110236
34. Bentley SA, Black A, Khawaja N, et al. The mental health and wellbeing survey of Australian optometrists. Ophthalmic Physiol Opt. 2021;41:798–807. doi:10.1111/opo.12823
35. Magallón-Botaya R, Pérula-de Torres LA, Verdes-Montenegro Atalaya JC, et al. Mindfulness in primary care healthcare and teaching professionals and its relationship with stress at work: a multicentric cross-sectional study. BMC Fam Pract. 2021;22:29. doi:10.1186/s12875-021-01375-2
36. Liu J, Liu M, Liang W. The dynamic COVID-zero strategy in China. China CDC Wkly. 2022;4:74–75. doi:10.46234/ccdcw2022.015
37. Spinelli WM, Fernstrom KM, Galos DL, et al. Extending our understanding of burnout and its associated factors: providers and staff in primary care clinics. Eval Health Prof. 2016;39:282–298. doi:10.1177/0163278716637900
38. Ślusarska B, Nowicki GJ, Niedorys-Karczmarczyk B, et al. Prevalence of depression and anxiety in nurses during the first eleven months of the COVID-19 pandemic: a systematic review and meta-analysis. Int J Environ Res Public Health. 2022;19:1154. doi:10.3390/ijerph19031154
39. Cena L, Rota M, Calza S, et al. Mental health states experienced by perinatal healthcare workers during COVID-19 pandemic in Italy. Int J Environ Res Public Health. 2021;18:6542. doi:10.3390/ijerph18126542
40. Halcomb E, McInnes S, Williams A, et al. The experiences of primary healthcare nurses during the COVID‐19 pandemic in Australia. J Nurs Scholarship. 2020;52:553–563. doi:10.1111/jnu.12589
41. Kim SC, Quiban C, Sloan C, et al. Predictors of poor mental health among nurses during COVID-19 pandemic. Nurs Open. 2021;8:900–907. doi:10.1002/nop2.697
42. Schwartz R, Frayne SM, Friedman S, et al. Retaining VA women’s health primary care providers: work setting matters. J Gen Intern Med. 2021;36:614–621. doi:10.1007/s11606-020-06285-0
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.