")
Back to Journals » Journal of Pain Research » Volume 17
Opioid Use Disorder: A Qualitative Exploratory Analysis of Potential Misunderstandings in Patients with Chronic Non-Cancer Pain
Authors Kufeld N , Weckbecker K , Michalak J , Häuser W , Petzke F, Scherbaum N , Specka M , Schmidt A , Piotrowski A, Kersting C , Just JM
Received 26 October 2023
Accepted for publication 5 February 2024
Published 5 March 2024 Volume 2024:17 Pages 873—885
DOI https://doi.org/10.2147/JPR.S445153
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Timothy Atkinson
Neele Kufeld,1 Klaus Weckbecker,1 Johannes Michalak,2 Winfried Häuser,3 Frank Petzke,4 Norbert Scherbaum,5 Michael Specka,5 Alexandra Schmidt,6 Alexandra Piotrowski,6 Christine Kersting,6 Johannes Maximilian Just1
1Chair of General Practice I and Interprofessional Care, Institute of General Practice and Primary Care, Faculty of Health, Witten/Herdecke University, Witten, Germany; 2Department of Psychology and Psychotherapy, Witten/Herdecke University, Witten, Germany; 3Department Psychosomatic Medicine and Psychotherapy, Technical University Munich, Munich, Germany; 4Department of Anesthesiology, Pain Medicine, University Medical Center Göttingen, Göttingen, Germany; 5Department of Psychiatry and Psychotherapy, LVR University Hospital Essen, University of Duisburg-Essen, Essen, Germany; 6Chair of General Practice II and Patient-Centredness in Primary Care, Institute of General Practice and Primary Care, Faculty of Health, Witten/Herdecke University, Witten, Germany
Correspondence: Neele Kufeld, General Practice I and Interprofessional Care, Institute of General Practice and Primary Care, Witten/Herdecke University, Alfred-Herrhausen-Straße 50, Witten, 58455, Germany, Tel +49 15120923736, Fax +49 2303 926-745, Email [email protected]
Purpose: Substance use disorders (SUD) are a challenging comorbidity in patients with chronic non-cancer pain (CNCP) as they complicate diagnosis and therapy, especially when opioids are part of the therapeutic regimen. A definite diagnosis of opioid use disorder (OUD) in patients with CNCP on long-term opioid therapy (LTOT) is a prerequisite for effective and targeted therapy but may be complicated as some criteria of OUD might be attributed to the desire of the patient to relieve the pain. For instance, the desire to increase the dose can be based on both a SUD as well as inadequate pain therapy. Many scientific studies use standardized questions. Therefore, potential misunderstandings due to possible diagnostic overlaps often cannot be clarified.
Methods: 14 qualitative guided interviews were conducted and analyzed (Kuckartz content analysis), with the intention to verify if patient’s initial response to simple questions based on the wording of the DSM-5, as commonly used in research and practice, were consistent with the results of a more in-depth inquiry.
Results: The results suggest that without in-depth investigation, there is a particular risk of false-positive assessment of the DSM-5 criteria for OUD when opioids are prescribed, especially when the questions are considered independently of chronic pain. The risk of a false-negative assessment has also been shown in isolated cases.
Conclusion: Only after asking for and describing specific situations it was possible to determine whether the patient’s positive or negative answers were based on a misunderstanding of the question. To avoid misdiagnosis, staff conducting DSM-5 interviews should be trained in pain-specific follow-up questions that may help to uncover diagnostic confounding.
Keywords: chronic pain, substance use disorder, diagnoses, DSM 5
Introduction
Substance use disorders are a common comorbidity in patients with chronic pain, which presents a challenge in diagnostics and therapy.1 Opioids are particularly important in pharmacological management, but they are also highly addictive substances. The use of questions based on the DSM-5 criteria to diagnose opioid use disorder (OUD) is widespread.2 There are eleven diagnostic criteria for the diagnosis of OUD in the DSM-5. Accounting for the special situation of patients who receive opioids solely under appropriate medical supervision, two of these criteria (development of tolerance and withdrawal symptoms) are omitted if opioids are prescribed for pain therapy seeking to improve diagnostic accuracy and avoid overdiagnosis. Opioid use is considered problematic if at least two criteria are met. It is divided into mild (2–3 symptoms), moderate (4–5 symptoms) and severe (6 or more symptoms) prescription OUD.2
High inconsistency has been found in the diagnosis of opioid use disorder among patients with CNCP who are receiving LTOT. Challenges emerge when diagnosing opioid use disorder using questions based on the DSM-5, due to the different understandings of the clinical picture among experts and the use and definition of terms.3–5 Boscarino et al argue that a patient’s understanding of the question they receive and their motivation behind their answer may also be crucial in making a diagnosis.6 Some DSM-5 criteria might not only represent use disorder and may be confounded with inadequately treated pain, leading to a flawed assessment of the presence and severity of OUD.4,7–9 The authors call for specific diagnostic adaptations for people receiving prescription opioids for CNCP and for investigations of the appropriateness of the DSM-5 criteria in the presence of CNCP.5,10,11 Furthermore, Manhapra et al propose complex persistent opioid dependence (CPOD) as a new disease concept or diagnosis, representing an intermediate stage between use disorder and physical dependency.12
In order to operationalize the use of the diagnostic criteria, standardized manuals based on the DSM-5 criteria, such as DIPS Open Accesses (German version) and the Composite International Diagnostic Interview (CIDI) as well as simple questions or self-questionnaires based on the DSM-5 criteria are commonly utilized in epidemiological studies.7,13–15 This practice is scientifically logical, as it allows for standardized procurement and increases interrater reliability. On the other hand, it increases the risk of omitting individual clarification of potential misunderstandings. However, this approach could prove problematic as there may be a diagnostic overlap between the symptoms of OUD and chronic pain that can only be distinguished by further inquiry from a trained clinician, not by standardized simple questions or questionnaires alone - for instance a patient’s desire to increase the dose can be based on both a substance use disorder and an inadequately treated pain.6
Confounding of diagnostic criteria may put patients at risk, for the following reasons:
This issue has been postulated for the DSM-IV but there is currently no study using questions according to the DSM-5 in individuals with chronic non-cancer pain (CNCP) receiving long-term opioid treatment.2,16 Some studies exist that address this issue from a quantitative perspective but in order to identify potential diagnostic misunderstandings, a qualitative design was chosen for this investigation.13,17,18 This study aims to examine which questions based on the DSM-5 criteria show problematic overlaps (false positives or false negatives) in this context. It was verified whether patients affirmed a criterion due to dependent behavior or because their pain was not being adequately treated.
Materials and Methods
Interview
Guideline interviews were conducted with the purpose of obtaining a more comprehensive understanding of patient`s perception of the questions according to the DSM-5 criteria, aiming to enhance the accuracy of diagnoses by incorporating patient`s perspectives. By better understanding the patient`s response form the diagnostician’s perspective, an appropriate diagnosis can be found. This study is reported in accordance with the COREQ guidelines.19
Methodologically, we followed the work of Elander et al.16 Simple questions based on the wording of the DSM-5 were followed by a more in-depth inquiry. For each item, the patients were asked whether it was true or had ever been true. If a patient answered “yes”, the interviewer would ask for a specific example. If a patient said “no”, the interviewer would ask whether the situation had never happened before.
Setting and Sample
A total of 14 telephone interviews were conducted. Recruitment was performed in cooperation with the treating primary care physicians. These primary care physicians were contacted through a research network at the University of Witten/Herdecke and asked to recruit suitable patients. Patients were informed about the project in an information letter. With the consent of the patients, contact details were provided if they wished to participate. The study complies with the Declaration of Helsinki. All participants provided written informed consent to participate, which also included the publication of anonymized responses. The interviewer, a female with a B.Sc. in Psychology, contacted patients who were referred by their treating physicians (GPs) and met the inclusion criteria. Inclusion criteria were the presence of chronic pain and LTOT, both for at least three months according to current guidelines.20,21 A maximum variation sample was chosen.22 Maximum variation in this study includes the existence of relevant additional characteristics besides chronic pain and LTOT. What was defined as relevant additional characteristics for this sample was worked out in a panel with the experienced pain therapists among the co-authors and based on literature.23–29 These are either commonly represented comorbidities or demographic characteristics (age). As shown in Table 1, the following characteristics were chosen for maximum variation based on expert opinion: younger than 40 years, older than 80 years, isolated chronic pain, depression and/or anxiety, somatoform pain and substance use disorder. This substance use disorder either existed currently or had led to challenges in the context of opioid treatment for pain. In addition, an attempt was made to ensure a balanced sex ratio in the recruitment process. GPs recruited individuals who specifically met inclusion criteria, such as an additional diagnosis of depression. These additional diagnoses were the leading comorbidity. Affective disorders and substance use disorder were more likely to be present in women in the recruited sample, so two women and one man were interviewed here. Patients with insufficient German language skills were excluded or not recruited, as the interviews were conducted in German. Patients were asked to provide their consent to participate. If they expressed interest, the author contacted them by phone.
 |
Table 1 Overview of Maximum Variation Sample |
The additional criterion of a diagnosis of “somatoform pain” was included, as this category corresponds to a DSM-IV diagnoses and was chosen because of its higher discriminatory power and use in clinical practice setting than new DSM-5 diagnosis of somatic symptom disorder. The interviews lasted between 15 and 40 minutes.
Based on use of a maximum variation sample, the group studied was very heterogeneous (age range: 29–87 years old). However, the group was similar in terms of their school education. Except for two patients, all worked in an apprenticed profession.
Data Analysis
For the qualitative analysis of the interview data a deductive-inductive approach based on thematic qualitative text analysis according to Kuckartz was used.30 Deductive categories were formed in advance from the theory, form a diagnostic perspective. Inductive categories were formed directly from the interview material. The transcripts were analyzed using the MAXQDA 2020 software.31 Initially, the first author coded 25% of the material. The interviews were analyzed in German, and the coding scheme is presented in additional file 1. Then three researchers with experience in qualitative research reviewed these categories. Subsequently, the rest of the material was coded by the first author, and another coding session was conducted. Finally, an expert panel (experts in pain and addiction therapy) was constituted with clinicians whose diagnostic experience was used to provide feedback.
Following the example of Elander et al, it was decided that if the patient answered “yes”, a query about a specific situation would be asked. After this description, it was considered within the deductive categorization whether it was a true or false positive answer by health care providers (HCP).16 True positive means that the initial “yes” is confirmed by a description of a dependent behavior. False positive means that the initial “yes” turns out to be a misunderstanding of the question. In this case, a situation was described that does not indicate dependent behavior but shows how the question was understood from the patient’s point of view. The authors decided to call this category “false positive”, not because they believe that the patient’s answers are wrong, but because in the diagnostic sense a false positive decision would be caused by the misunderstanding.
Ethics
Participants were provided with written information and gave informed consent prior to the start of each interview. To protect the confidentiality of the participants, they were assigned numbers for each interview (I1–14), and all identifying information was removed during transcription and presentation of results. The study was reviewed and approved by the Ethics Committee of Witten/Herdecke University [no:246/2020].
Results
Results of the Literature Search
High inconsistency has been found in the diagnosis of opioid use disorder among patients with CNCP who are receiving LTOT. Challenges emerge when diagnosing opioid use disorder using questions based on the DSM-5, due to the different understandings of the clinical picture among experts and the use and definition of terms.3–5 Boscarino et al argue that a patient’s understanding of the question they receive and their motivation behind their answer may also be crucial in making a diagnosis.6 Some DSM-5 criteria might not only represent use disorder and may be confounded with inadequately treated pain, leading to a flawed assessment of the presence and severity of OUD.4,7–9 The authors call for specific diagnostic adaptations for people receiving prescription opioids for CNCP and for investigations of the appropriateness of the DSM-5 criteria in the presence of CNCP.5,10,11 Furthermore, Manhapra et al propose complex persistent opioid dependence (CPOD) as a new disease concept or diagnosis, representing an intermediate stage between use disorder and physical dependency.12
Deductive Categories
Based on the literature and the purpose of this study, deductive categories were developed prior to analyzing the interview content. These categories follow the structure of the interview, including the history of pain, DSM-5 criteria (nine categories), ambiguous questions and missing questions. The nine categories based on the DSM-5 criteria had four categories each. The reported results focus on the DSM-5 categories, which were each divided into two subcategories: “Agree” and “Disagree”, with an additional two subcategories each for false positives and false negatives (Figure 1). Emphasis was placed on identifying false positives and false negatives, as these highlight possible misunderstandings and carry the risk of an inaccurate diagnosis.
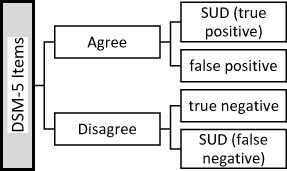 |
Figure 1 Scheme of deductive categorizing of the DSM Items; Not all subcategories were used for all items, but they all provided a guide for coding. |
Have You Ever Found That You Ended Up Taking More of the Opioid Than You Intended to, or Carried on Taking It for Longer Than You Intended to?
Four patients gave false positive answers to this question. For example, patient two stated, “Yes, of course. If I had more, more pain, and it was no longer bearable” (Figure 2). This response suggests that the reason for taking more opioids was not a desire for the medication itself, but rather the intensity of the pain. Another patient, who was asked to describe a specific situation in which they took more opioids than the prescribed amount, said,
[…] I had a pain attack, I live here with my brother, and I was so vicious because I had this pain. And then my brother brought me the tablets and said, “Now you take another one”. (Interview 11)
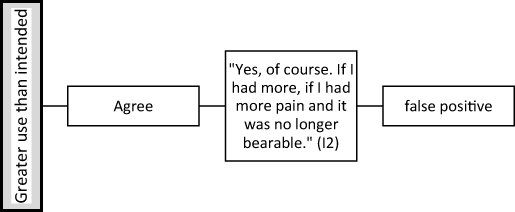 |
Figure 2 Example of misunderstanding of Item one; After the patient agreed, the interviewer asked a follow-up question about a concrete situation. |
Do You Have a Persistent Desire to Reduce or Better Control the Amount of Opioid You Take, or Have You Tried to Do so Without Success?
Five patients gave a false positive answer, and two patients gave a false negative answer to this question. With regards to this category, on one hand, the issue seems to be that patients often do not feel personally responsible for reducing their medication or discussing reduction with their physician, but rather feel trapped in the context of their patient-doctor relationship. On the other hand, it sometimes appears that the concept of dependency does not quite fit for pain medication as it does for substance abuse. For example, one patient stated
In any case, I have the desire to do that, but until now we’ve only had to increase the dose instead of reducing it. (Interview 6)
An example of a false negative answer can be seen in the response of a patient in Figure 3.
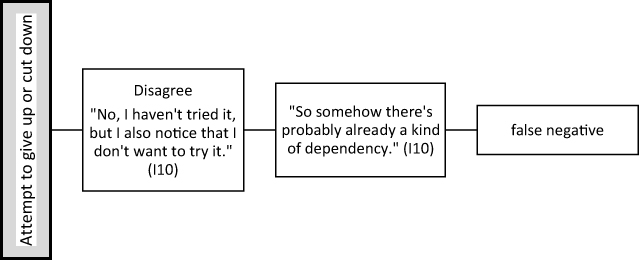 |
Figure 3 Example of misunderstanding of Item two; After the patient disagreed, the interviewer asked whether that ever happened. |
Have You Ever Found You Were Spending a Lot of Time on Getting the Opioid, or Getting Over the Effects of It?
Two patients gave a false positive answer to this question. These false positive answers were focused on the second part of the question about the recovery from the effect of the medication. Patients also asked for clarification on the meaning of “getting over the effects”, which prompted the authors to place this question in the category of ambiguous questions. For example, one patient did not understand the question and asked
I don’t know how to describe this. What do you mean by recovery? (Interview 11)
Did You Have Such a Strong Craving for the Opioid That You Could Not Think of Anything Else or Could Not Resist Taking an Extra Dose?
There was one patient who gave a false positive answer to this question, one who gave a false negative answer, and another who gave a true positive answer. An example of a false positive answer was
If the pain was strong, yes (Interview 6)
In contrast, a true positive answer was
I know the pill is always there. I know I have to take it when I don’t have pain or when I have less pain. (Interview 7)
The patient who gave a false negative answer initially denied having a craving, but later commented
Yes, somehow there is something different than with other drugs. Probably already a bit of an addiction or so – could be. (Interview 10)
Have You Had Any Significant Problems at Work or School or in Taking Care of Your Household Related to Taking the Opioid, Such as Absenteeism, Poor Performance, Expulsion from School or Neglect of Children or Household?
Two patients gave false positives to this question. One patient said
I also have such a small garden and I love my garden, but I can just do something for half an hour at a time, then I just have to sit down again and wait until the pain has calmed down a bit and then I can continue again. (Interview 7)
Another patient explained
Yes, I have already said that regardless of the opioid, I am just so bad that I cannot answer the question at all. (Interview 10)
These responses highlight the issue of patients misunderstanding the question and focusing on their pain rather than their use of opioids.
Did a Relationship, Such as with a Partner, Friend or Family Member, Break Down Because of the Opioid?
One patient gave a false positive answer to this question. The first answer was “yes” and when asked by the interviewer if this was due to the pain or the medication, the patient said,
Generally, my friends couldn’t cope with it anymore because I constantly relied on help, whether it was in a wheelchair or on crutches. I had to leave early, or I simply couldn’t stand anymore. Or it was impossible to go somewhere with the wheelchair. Many friends withdrew from me at that time, and a long-term relationship that I was already in before broke apart. And then I had another short relationship, which also failed. (Interview 3)
Have You Ever Found That Using the Opioid Meant That You Stopped Important Activities Like Going to Work or Being with Friends or Family, or That You Spent Less Time on Your Hobbies?
Four patients gave a false positive response to this question. One patient (Interview 5), who stated that she no longer participates in family activities, provides an example shown in Figure 4.
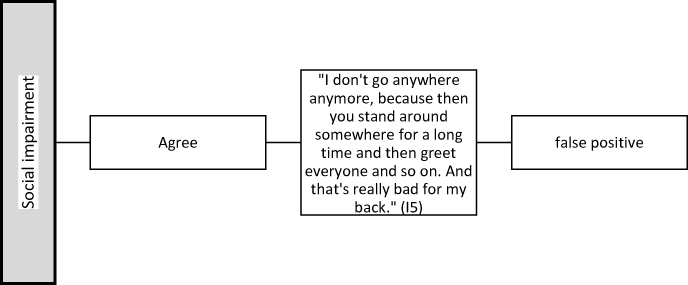 |
Figure 4 Example of misunderstanding of Item seven; After the patient agreed, the interviewer asked her to describe a concrete situation. |
Have You Ever Used the Opioid in Situations That Could Have Been Dangerous, Like When You Were Driving or Using Machinery and Could Have Had an Accident?
One patient gave a false positive answer to this question. Initially, the patient said that he had problems driving due to taking opioids. After a few more questions, it turned out that this answer referred to an opioid he had taken in the past, but there was no such problem with the buprenorphine he was taking now (Interview 9)
Did You Take the Opioid Knowing It Would Cause Physical or Psychological Problems or Make Them Worse?
Three patients gave a false positive answer. For example, one patient responded,
Yes, I knew what I was getting into. I also knew that if I stopped, I would have to go through physical withdrawal. So, I already know that. So, it’s not like that. Yes. Somehow, I got involved in it. (Interview 2)
One patient gave a false negative answer. This patient
Who initially answered “no” to this question, described dependent behavior in response to further questions. (Interview 7)
Ambiguous Questions
When asked some of the DSM-5 questions, patients not only interpreted the content of these questions differently from the interviewer, but also did not understand some of the questions at all. As this project aims to focus on patient understanding, these questions are categorized in this section. Four patients did not understand the second part of question three, and one patient each did not understand questions four, five, six, eight and nine, respectively.
One patient gave the general feedback that
Some of the additional questions that came with the questions didn’t apply at all […] many things really didn’t apply in the end. (Interview 13)
Missing Questions
In every interview, the patients were asked whether they thought any question was missing. Only one patient mentioned a missing point:
How does the partner suffer from it as well? Because it’s not just me who’s affected, but over the years I’ve also realized that my partner is affected as well. Because during these really bad times, I didn’t allow any closeness anymore. So, the partner also suffers from it. (Interview 3)
History of Pain
Patients were asked about their history of pain. One patient stated,
[…] and so the dosage kept increasing and I also tried many medications. I went to different doctors and each one prescribed something different for me. I tried the whole gamut. I’ve gone through the whole range. (Interview 1)
Another patient said
I couldn’t avoid it because I had pain. Somewhere I was forced to endure it, but I couldn’t bear it anymore. (Interview 2)
Summary of Deductive Results
A summary of the coding of the deductive categories can be seen in Figure 5. Since this is a qualitative paper, the presentation does not aim to show significant results. The presentation serves as an overview of the comparison of a diagnosis based on the initial response of patients versus the diagnosis after coding in the false negative and false positive ratings. Thus, six patients would potentially have received a false positive diagnosis and one patient would have received a false negative diagnosis.
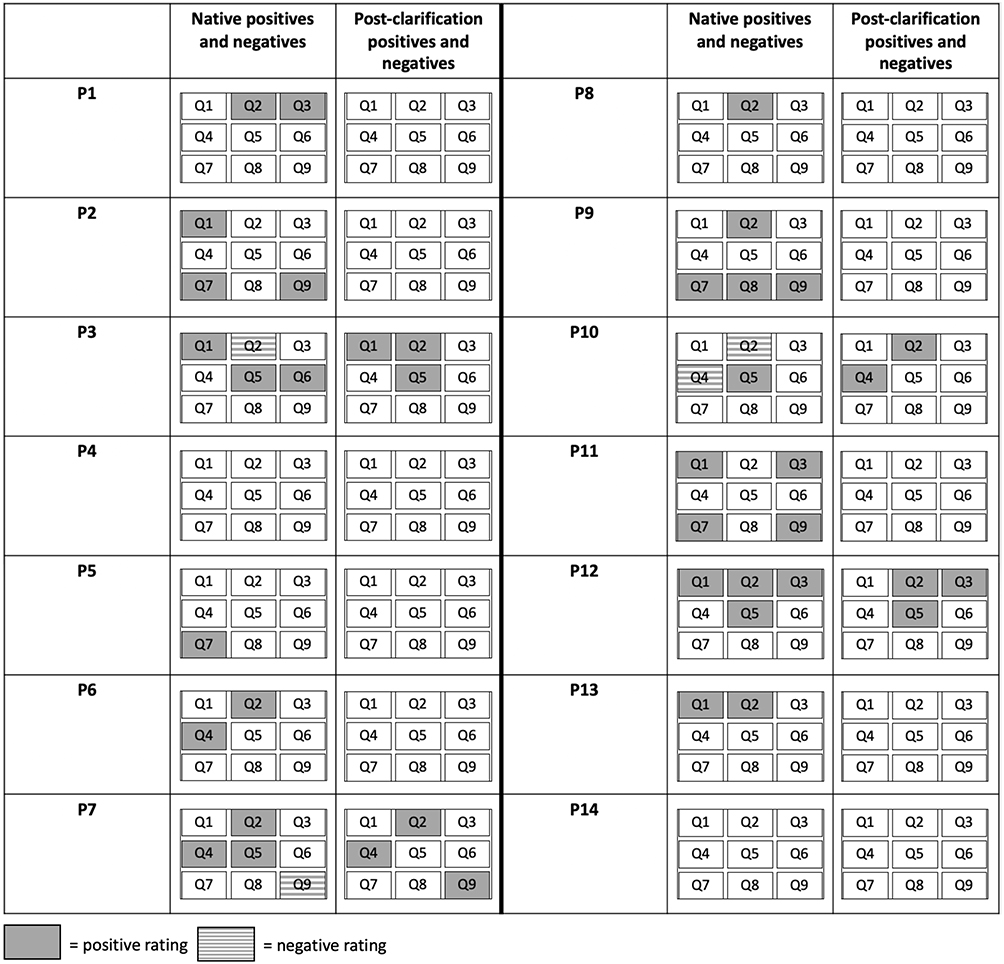 |
Figure 5 Summary of deductive results; P= Patient, Q= Question. |
Inductive Categories
This chapter gives an account of the inductive categories formed from the material. Seven inductive main categories were formed. These categories were not created as subcategories of the deductive categorization system, as would be usual according to Kuckartz; rather, they were created as independent main categories (Figure 6).30 However, in this study, the inductive categories are independent of the deductive categories themselves. They reflect not only aspects of addiction to opioids but more generally the experience of chronic pain and their ambivalence towards its treatment with opioids.
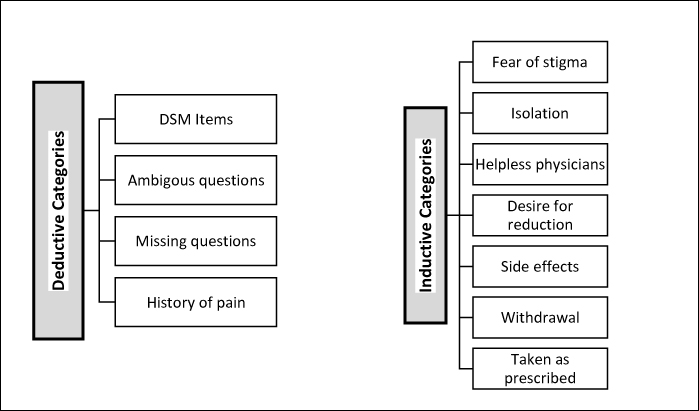 |
Figure 6 Overview of all deductive-inductive categories; The code of the “DSM Items” were chosen for all nine items and had four subcategories as shown in Figure 1. |
Fear of Stigma
This category was created because many patients were concerned about being labeled as addicts. This seems to be quite understandable, as the questions in the DSM-5 are not subtle in their intent. For example, one patient stated,
So addiction in the sense of being an addict, no. Only if/through this pain, I finally stopped getting this pressure. This pain. (Interview 3)
The same patient later mentioned, “I’ve never been high like a junkie or like a drug addict. There are still worlds apart. So, there are still worlds in between.”
Isolation
Some patients commented that they suffer from isolation and withdraw as their pain forces them to stay at home or prevents them from doing activities they used to do. Some also stated that their friends and family did not know how to handle the situation because they were somehow disabled. (Interview 3)
Another patient stated,
I don’t go anywhere anymore. We keep in touch with our children, and if there are any celebrations, like birthdays or something, I usually don’t go, because I just can’t. I wouldn’t feel comfortable there. (Interview 5)
One patient said that now that he is retired but in pain, he is not able to do what he had imagined doing in his retirement:
As I said, I have a lot of things I WANT to do, and I can’t do it. (Interview 13)
Helpless Physicians
Some patients have experienced doctors not knowing what to do with their case. One patient explained,
So I had the impression that he was just as clueless as I was. (Interview 1)
Desire for Reduction
There is the criterion of wanting to reduce opioid use, but there were also patients who mentioned the desire for reduction outside the context of this question. One patient said,
Of course, I would like to get rid of it completely, but after such a long time, I have little hope that I will ever get rid of it completely again. If it were possible, I would be very relieved, very happy. (Interview 6)
Side Effects
Many of the patients interviewed suffered from problematic side effects. One patient commented,
I’ve tried them all. […] Within 13 years, I took so many different ones: Some made me sick, others caused digestive issues, some gave me stomach pains, and others made me nauseous and vomit. So, of course, I didn’t feel like taking them for a longer period and eventually went back to the old medications that I could tolerate. Medicines that you can tolerate. (Interview 1)
Another patient said,
Because my head, my head was spinning. (Interview 12)
One patient reported,
It wasn’t going particularly well, and the only thing you get are stomach aches. (Interview 13)
One patient mentioned a positive psychotropic side effect indicating the risk of dependence:
I have become more relaxed. […]. That’s also a piece of quality of life when you don’t get upset or nervous about every little thing. And even if you’re a minute late somewhere, you don’t immediately get into a frenzy or whatever, so I find that very pleasant, if you will. (Interview 14)
Withdrawal
Some patients reported withdrawal symptoms. In the diagnosis of dependence on prescribed painkillers, the symptoms of withdrawal and development of tolerance are left out. However, since withdrawal symptoms were mentioned in many interviews, a category was created for them. On the one hand, it was reported that withdrawal itself worsened pain
It may be that the withdrawal symptoms manifest themselves in such a way that the pain gets worse – Interview 1
On the other hand, the symptoms of withdrawal were described
Yes, it started with a cold sweat and then I got a stomachache and flu-like symptoms, I would say – Interview 2
Taking the Opioid as Prescribed
Some patients felt it important to mention that they were taking the medication as prescribed by their doctor. This statement was made more frequently in the context of the question regarding whether more medication was taken or whether it was taken over a longer period than prescribed. For example, one patient said,
No, no I really don’t. I just take it as prescribed by the doctor, very well behaved. (Interview 11)
Discussion
The present work provides an indication that there is a risk of false-positive assessment of DSM-5 criteria for substance use disorder in patients with CNCP on LTOT, especially when diagnosticians rely on simple questions without considering the impact of chronic pain behavior on DSM-5 items. There was an accumulation of misunderstandings for the questions based on the DSM-5 criteria one, two, five and seven which were often only made transparent after intensive inquiry. These misunderstandings occurred, for example, when questions based on the DSM-5 criteria were answered positively because patients aimed for pain relief or because they attributed responsibility for medication dosage to their treating physicians. In addition, some questions were interpreted in terms of living with chronic pain rather than specifically addressing opioid use. While the degree of generalizability of these results is unknown, they nevertheless indicate an existing diagnostic overlap and may serve to inform the design and content of quantitative follow-up studies. Future projects should investigate what standardized follow-up questions are needed to make the items more understandable and selective, allowing for a more accurate distinction between substance use disorder and inadequately treated pain. A better diagnostic understanding of dependence on prescribed opioids is critical to improving the care of people with chronic pain, both in research and in practice.
There is evidence of misunderstanding of some of the questions based on the DSM-5. Inductive categories could reveal some of the aspects that are part of the lives of these chronic pain patients.
The patient’s responses can be used to get an idea of where the misconceptions are coming from and where more selectivity is needed. Further projects should quantify these misconceptions to see if they are robust measures.
There were several limitations and challenges during this project. There was only one interviewer in this study, whereas in the study by Elander et al, two psychologists rated the same situation.16 The use of only one interviewer could have affected the reliability of this study’s results. Furthermore, as with every qualitative study, there were slight variations in the questions asked during the interviews, which could have impacted the consistency of the responses. Social desirability bias may have also been a factor, especially for patients with a history of addiction, who may have been sensitive to the meaning of the questions.
As the sample was selected from mainly German patients recruited through their general practitioner, future research should determine the extent to which the present findings can be generalized to other care settings, such as specialized pain care as more severe patients may have been overlooked in this study design. The German cultural setting may also have led to cultural biases.
Conclusion
Based on the deductive categories and their results, it seems advisable that additional and focused inquiries are used to clarify if questions have been sufficiently understood. Patient responses show that there are questions based on the DSM-5 criteria that relate more to the management of chronic pain than to the use of medication. This should be taken into account when making a diagnosis. Therefore, implementation of DSM-5 criteria in written form is not advisable in patients with CNCP on LTOT. An approach for practice could be to train staff to ask standardized follow-up questions and to be able to assess the answers in the diagnostic sense in which they were intended. This work is a basis for follow-up studies, which may help to optimize diagnostic criteria and the way they are queried in research and practice. In this way, misdiagnosis and undertreatment of people with chronic pain can be avoided.
Abbreviations
SUD, Substance use disorders; CNCP, chronic non-cancer pain; OUD, opioid use disorder; LTOT, long-term opioid therapy; DSM-5, Statistical Manual for Mental Disorders Version 5; CIDI, Composite International Diagnostic Interview; GP, treating physicians; HCP, health care providers; CPOD, complex persistent opioid dependence.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
W. Häuser and F. Petzke collaborated on the German S3 guidelines on long-term opioid therapy for chronic non-cancer pain. W. Häuser has received a lecture fee from Janssen-Cilag and the Falk Foundation. N. Scherbaum has received honoraria for several activities (eg, advisory board membership, lecture, manuscripts) from AbbVie, Camurus, Hexal, Janssen-Cilag, MSD, Medice, Mundipharma, Reckitt-Benckiser/Indivior, and Sanofi-Aventis. During the last three years he has participated in clinical trials financed by the pharmaceutical industry. The other authors declare no conflicts with regard to the manuscript.
References
1. Søndergård S, Vaegter HB, Erlangsen A, Stenager E. Ten-year prevalence of mental disorders in patients presenting with chronic pain in secondary care: a register linkage cohort study. Eur J Pain. 2018;22(2):346–354. doi:10.1002/ejp.1124
2. Association AP. Diagnostic and Statistical Manual of Mental Disorders. American Psychiatric Association; 2013.
3. Boscarino JA, Withey CA, Dugan RJ, Hu Y, Auciello J, Alfieri T. Opioid medication use among chronic non-cancer pain patients assessed with a modified drug effects questionnaire and the association with opioid use disorder. J Pain Res. 2020;13:2697–2705. doi:10.2147/jpr.S275397
4. Gorfinkel L, Voon P, Wood E, Klimas J. Diagnosing opioid addiction in people with chronic pain. BMJ. 2018;362:k3949. doi:10.1136/bmj.k3949
5. Just J, Petzke F, Scherbaum N, Radbruch L, Weckbecker K, Häuser W. Kritische Auseinandersetzung mit neuen Daten zur Prävalenz von Opioidgebrauchsstörungen bei Patienten mit chronischen Schmerzen in Deutschland. [Critical discussion of new data regarding prevalence of opioid use disorder in patients with chronic pain in Germany]. Schmerz. 2022;36(1):13–18. doi:10.1007/s00482-021-00582-1
6. Weissman DE, Haddox DJ. Opioid pseudoaddiction-an iatrogenic syndrome. Pain. 1989;36(3):363–366. doi:10.1016/0304-3959(89)90097-3
7. Guillou-Landreat M, Quinio B, Le Reste JY, et al. Analgesic opioid misuse and opioid use disorder among patients with chronic non-cancer pain and prescribed opioids in a pain centre in France. Int J Environ Res Public Health. 2021;18(4):2097. doi:10.3390/ijerph18042097
8. Manhapra A, Becker WC. Pain and addiction: an integrative therapeutic approach. Med Clin North Am. 2018;102(4):745–763. doi:10.1016/j.mcna.2018.02.013
9. Kathiresan P, Rao R, Joshi T, et al. Chronic noncancer pain and opioid addiction: diagnostic and management challenges. Indian J Palliat Care. 2020;26(4):544–547. doi:10.4103/ijpc.Ijpc_232_19
10. Just JM, Scherbaum N, Specka M, Puth M-T, Weckbecker K, Gomes T. Rate of opioid use disorder in adults who received prescription opioid pain therapy-A secondary data analysis. PLoS One. 2020;15(7):e0236268. doi:10.1371/journal.pone.0236268
11. Young SR, Azari S, Becker WC, et al. Common and challenging behaviors among individuals on long-term opioid therapy. J Addict Med. 2020;14(4):305–310. doi:10.1097/adm.0000000000000587
12. Manhapra A, Sullivan MD, Ballantyne JC, MacLean RR, Becker WC. Complex persistent opioid dependence with long-term opioids: a gray area that needs definition, better understanding, treatment guidance, and policy changes. J Gen Intern Med. 2020;35(Suppl 3):964–971. doi:10.1007/s11606-020-06251-w
13. Bialas P, Böttge-Wolpers C, Fitzcharles M-A, et al. Cannabis use disorder in patients with chronic pain: overestimation and underestimation in a cross-sectional observational study in 3 German pain management centres. Pain. 2023;164(6):1303–1311. doi:10.1097/j.pain.0000000000002817
14. Degenhardt L, Bruno R, Lintzeris N, et al. Agreement between definitions of pharmaceutical opioid use disorders and dependence in people taking opioids for chronic non-cancer pain (POINT): a cohort study. Lancet Psychiatry. 2015;2(4):314–322. doi:10.1016/s2215-0366(15)00005-x
15. Piontek D, Kraus L, Matos EGD, Atzendorf J. Der Epidemiologische Suchtsurvey 2015. SUCHT. 2016;62(5):259–269. doi:10.1024/0939-5911/a000444
16. Elander J, Lusher J, Bevan D, Telfer P. Pain management and symptoms of substance dependence among patients with sickle cell disease. Soc sci med. 2003;57(9):1683–1696. doi:10.1016/s0277-9536(02)00553-1
17. Hasin DS, Shmulewitz D, Stohl M, et al. Diagnosing prescription opioid use disorder in patients using prescribed opioids for chronic pain. Am J Psychiatry. 2022;179(10):715–725. doi:10.1176/appi.ajp.21070721
18. Lauff S, Petzke F, Brill S, et al. Face validity of the ICD-10 criteria of substance abuse and dependence for patients prescribed cannabis-based medicines for chronic pain-A survey of pain medicine physicians in Canada, Germany and Israel. Eur J Pain. 2023;27(5):588–601. doi:10.1002/ejp.2082
19. Tong A, Sainsbury P, Craig J. Consolidated criteria for reporting qualitative research (COREQ): a 32-item checklist for interviews and focus groups. Int J Qual Health Care. 2007;19(6):349–357. doi:10.1093/intqhc/mzm042
20. Häuser W, Bock F, Hüppe M, et al. Empfehlungen der zweiten Aktualisierung der Leitlinie LONTS [Recommendations of the second update of the LONTS guidelines (Long-term opioid therapy for chronic noncancer pain)]. Der Schmerz. 2020;34(3):204–244. doi:10.1007/s00482-020-00472-y
21. Treede RD, Rief W, Barke A, et al. Chronic pain as a symptom or a disease: the IASP classification of chronic pain for the International Classification of Diseases (ICD-11). Pain. 2019;160(1):19–27. doi:10.1097/j.pain.0000000000001384
22. Merriam SB, Tisdell EJ. Qualitative Research: A Guide to Design and Implementation.
23. Baigent M. Managing patients with dual diagnosis in psychiatric practice. Curr Opin Psychiatry. 2012;25(3):201–205. doi:10.1097/YCO.0b013e3283523d3d
24. Lavin R, Park J. Depressive symptoms in community-dwelling older adults receiving opioid therapy for chronic pain. J Opioid Manag. 2011;7(4):309–319. doi:10.5055/jom.2011.0072
25. Schrier E, Geertzen JH, Dijkstra PU. Subjective cognitive dysfunction in rehabilitation outpatients with musculoskeletal disorders or chronic pain. Eur J Phys Rehabil Med. 2017;53(4):582–589. doi:10.23736/s1973-9087.16.04470-1
26. Kroenke K, Outcalt S, Krebs E, et al. Association between anxiety, health-related quality of life and functional impairment in primary care patients with chronic pain. Gen Hosp Psychiatry. 2013;35(4):359–365. doi:10.1016/j.genhosppsych.2013.03.020
27. Schmid CW, Maurer K, Schmid DM, et al. Prevalence of medication overuse headache in an interdisciplinary pain clinic. J Headache Pain. 2013;14(1):4. doi:10.1186/1129-2377-14-4
28. Annagür BB, Uguz F, Apiliogullari S, Kara I, Gunduz S. Psychiatric disorders and association with quality of sleep and quality of life in patients with chronic pain: a SCID-based study. Pain Med. 2014;15(5):772–781. doi:10.1111/pme.12390
29. Jones JD, Vogelman JS, Luba R, Mumtaz M, Comer SD. Chronic pain and opioid abuse: factors associated with health-related quality of life. Am J Addict. 2017;26(8):815–821. doi:10.1111/ajad.12637
30. Kuckartz U. Qualitative Text Analysis: A Guide to Methods, Practice & Using Software. SAGE Publications Ltd; 2014.
31. MAXQDA; 2020. Available from: maxqda.com.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.