")
Back to Journals » Clinical Interventions in Aging » Volume 19
Outcome Comparison of Endovascular Treatment for Acute Large Vessel Occlusion Due to Large Artery Atherosclerosis and Cardioembolism in the Chinese Population: Data from the ANGEL Registry
Authors Shao G, Li X, Da M, Huo X, Zhang S
Received 20 October 2023
Accepted for publication 6 February 2024
Published 26 February 2024 Volume 2024:19 Pages 339—346
DOI https://doi.org/10.2147/CIA.S442339
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Nandu Goswami
Guangcai Shao,1 Xiang Li,2 Meiyue Da,1 Xiaochuan Huo,3 Shuheng Zhang1
1Department of Neurosurgery, Anshan Central Hospital, Anshan, People’s Republic of China; 2Department of Neurosurgery, The First Affiliated Hospital of China Medical University, Shenyang, People’s Republic of China; 3Cerebrovascular Disease Department, Neurological Disease Center, Beijing Anzhen Hospital, Capital Medical University, Beijing, People’s Republic of China
Correspondence: Shuheng Zhang, Department of Neurosurgery, Anshan Central Hospital, No. 77 South Zhonghua Road, Tiedong District, Anshan, 114009, People’s Republic of China, Tel +8618804120515, Email [email protected] Xiaochuan Huo, Cerebrovascular Disease Department, Neurological Disease Center, Beijing Anzhen Hospital, Capital Medical University, Beijing, People’s Republic of China, Email [email protected]
Background and Purpose: Studies on outcome comparison after endovascular treatment (EVT) for large vessel occlusion (LVO) between large artery atherosclerosis (LAA) and cardioembolism (CE) in the Asian population are scarce. We aimed to compare the baseline characteristics and clinical outcomes after EVT for anterior circulation LVO with LAA and CE in the Chinese population.
Methods: Patients were selected from the ANGEL registry and divided into LAA and CE groups. The primary outcome was the 90-day modified Rankin Scale (mRS) 0– 2. The secondary outcomes were 90-day mRS distribution, 90-day mRS 0– 1, 90-day mRS 0– 3, and early neurological improvement. The safety outcomes included death, symptomatic intracranial hemorrhage, and any intracranial hemorrhage. We conducted logistic regression models with adjustments to compare the outcomes.
Results: A total of 632 patients were included, of whom, 488 were in the LAA group and 144 were in the CE group. No significant difference in 90-day mRS 0– 2 was observed between LAA and CE groups (55.7%vs.43.1%, odds ratio[OR] 1.19, 95% confidence interval(CI), 0.92– 1.53, P=0.190). The LAA group exhibited a higher frequency of mRS 0– 3 compared to the CE group (69.1% vs 32.6%, OR1.32, 95% CI 1.02– 1.72, P=0.038). However, the incidence of death within 90 days did not significantly differ between the LAA and CE groups (10.9%vs.24.3%, OR0.91, 95% CI0.66– 1.25, P=0.545), nor did the occurrences of symptomatic intracranial hemorrhage(SICH) (4.5%vs.9.7%,OR1.08, 95% CI 0.65– 1.78, P=0.779) or intracranial hemorrhage(ICH) (21.9%vs.30.6%, OR 0.94, 95% CI0.71– 1.25, P=0.680). Moreover, no significant disparities were detected in other outcomes between the two groups (All P> 0.05).
Conclusion: In the ANGEL registry, a higher prevalence of patients undergoing EVT for acute anterior circulation LVO with LAA was found than those with CE. However, our study revealed that the efficacy and safety of EVT remained consistent regardless of the stroke’s etiology such as LAA or CE.
Keywords: large vessel occlusion, endovascular treatment, large artery atherosclerosis, cardioembolism
Introduction
The efficacy and safety of endovascular treatment (EVT) for acute ischemic stroke (AIS) due to proximal large vessel occlusion (LVO) in the anterior circulation have been extensively studied by several landmark randomized controlled trials.1 The Trial of ORG 10172 in Acute Stroke Treatment (TOAST) standard has been widely used to assess the stroke etiology widely.2 Large artery atherosclerosis (LAA) and cardioembolism (CE) are the two main etiologies of LVO. Previous studies reported that the characteristics such as stroke severity3 and collateral status4 of LVO and CE were different, potentially influencing the outcomes of EVT for LVO. The effect comparison of EVT between LAA and CE has been studied widely in the Western population.3–6 However, the literature on this topic in the Asian population still remains scarce.7,8
Hence, the present study based on a nationwide, multicenter, prospective registry database in China, aimed to compare baseline characteristics and clinical outcomes after EVT for anterior circulation LVO stemming from LAA and CE.
Methods
Study Population
Patients were selected from the ANGEL (Acute Ischemic stroke Cooperation Group of Endovascular Treatment) registry,9 which was a multicenter, nationwide, prospective registry study including 20 comprehensive stroke centers in China between June 2015 and December 2017. Full methods of the ANGEL registry such as inclusion/exclusion criteria were reported previously.9 The study protocol was approved by the Ethics Committees of Beijing Tiantan Hospital and all participating centers. Subjects or their legally authorized representatives provided written informed consent.
The inclusion criterion of the present study was that patients underwent EVT. The exclusion criteria of the present study were as follows: (1) posterior circulation stroke; (2) stroke of other determined etiology (SOE) or stroke of undetermined etiology (SUE).
Data Collection
We prospectively collected all variables including demographic characteristics, medical history, admission National Institutes of Health Stroke Scale (NIHSS), admission ASPECTS, antiplatelet therapy before EVT, IVT before EVT, imaging, procedural details, key time point, and clinical outcomes assessed by modified Rankin Scale (mRS).
The investigators received training to assess NIHSS and mRS.
Two independent experienced neuroradiologists blinded to all clinical information assessed baseline computed tomography (CT), magnetic resonance imaging (MRI), CT angiography (CTA), magnetic resonance angiography (MRA), digital subtraction angiography (DSA), and postprocedural CT, with a third available for adjudication when needed. The radiological assessment included Alberta Stroke Program Early CT Score (ASPECTS),10 tandem lesion,11 occlusion site, modified thrombolysis in cerebral ischemia score (mTICI)12 and intracranial hemorrhage (ICH) postprocedure.
Successful recanalization was defined as mTICI 2b-3 and complete recanalization was defined as mTICI 3. Heparin during the procedure was performed empirically at the individual operator’s discretion according to local protocols, which was defined as intravenous administration of unfractionated heparin, being infused at 50–100 IU/Kg at first and additional 1000 IU at intervals of an hour during the procedure.13 The protocol of the ANGEL registry recommended heparin during the procedure when patients were in a high coagulation state or expected operation for a long time.9
Stroke Etiology
Site investigators received training from the committee-assigned stroke specialists before enrollment to assess the stroke etiology according to the TOAST standard2 based on the patient’s clinical, imaging, and laboratory features.
LAA: Patients with clinical and brain imaging findings of either >50% of stenotic degree or occlusion of a large vessel without potential sources of cardiogenic embolism.2 CE: Patients with large vessel occlusion presumably due to a cardiogenic embolism without potential LAA source of thrombosis or embolism.2
Study Outcomes
The primary outcome was 90-day mRS 0–2. The secondary outcomes included 90-day mRS ordinal distribution, 90-day mRS 0–1, 90-day mRS 0–3, and early neurological improvement (ENI, defined as NIHSS decreased by≥8 points or NIHSS was 0–1 at 24h after the procedure). The safety outcomes included death within 90 days, symptomatic intracranial hemorrhage (SICH) within 48h defined as parenchymal, subarachnoid or intraventricular hemorrhage detected by CT or MRI and with an increase of ≥4 points on the NIHSS score,14 and any intracranial hemorrhage (ICH) within 48h.
Statistical Analysis
Categorical variables were described by number (percentage) and continuous variables were expressed by median(interquartile range [IQR]). We performed the Pearson χ2 test or Fisher’s exact test for the categorical variables and the Mann–Whitney test for the continuous variables to compare the differences in the baseline characteristics between LAA and CE groups. To compare the outcomes between the two groups, we conducted the binary logistic or ordinal logistic regression models adjusting for the baseline variables with P < 0.05 to calculate the odd ratio (OR) or common OR with 95% confidence intervals (CIs). To perform the sensitivity analysis, we adjusted for the propensity score calculated from a logistic regression model that included all the baseline variables with a P < 0.05. All P <0.05 (2-sided) was considered statistically significant. SPSS version 26.0 (IBM, Armonk, NY, USA) was used to conduct the analyses.
Results
As Figure 1 shows, we excluded 283 patients from 915 patients enrolled in the ANGEL registry study due to posterior circulation stroke (n=203) and SOE or SUE (n=80). Finally, a total of 632 patients were included in the present analysis, of whom, 488 were in the LAA group and 144 were in the CE group.
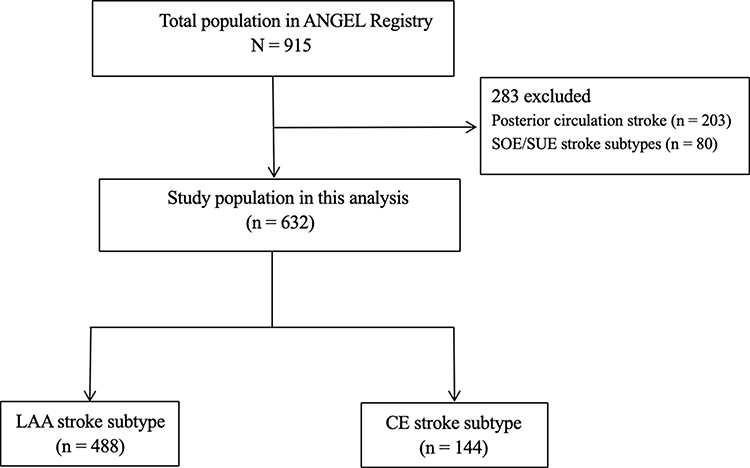 |
Figure 1 Flow chart of patient selection. Abbreviations: SOE, stroke of other determined etiology; SUE, stroke of undetermined etiology; LAA, large artery atherosclerosis; CE, cardioembolism. |
Baseline Characteristics
We observed that patients with LAA were younger (63[55–72] vs 67[59–75], P = 0.003) and had a higher rate of male (84.3% vs 44.4%, P<0.001), lower admission NIHSS (14[9–18] vs 20[14–23], P<0.001) and longer time from onset to puncture (300[220–440] vs 260[186–335], P<0.001) than those with CE. The prevalence of smoking history (37.9% vs 18.1%, P<0.001), hypertension (55.5% vs 40.3%, P=0.001), and tandem lesion (26.0% vs 0, P<0.001) were more in the LAA group than CE group; while the prevalence of atrial fibrillation was less in LAA group than CE group (10.7% vs 64.4%, P<0.001). Additionally, the rates of general anesthesia (39.3% vs 54.9%, P= 0.001) heparin during the procedure (39.3% vs 54.9%, P=0.001), stent retriever (69.5% vs 93.8%, P <0.001), and direct aspiration (6.4% vs 12.5%, P = 0.015) were lower in the LAA group than CE group; the rates of GP IIb/IIa receptor inhibitor (33.6% vs 20.8%, P=0.003), balloon angioplasty/stenting (24.8% vs 5.6%, P<0.001) and successful recanalization (93.4% vs 87.5%, P=0.020) were higher in the LAA group than CE group (Table 1).
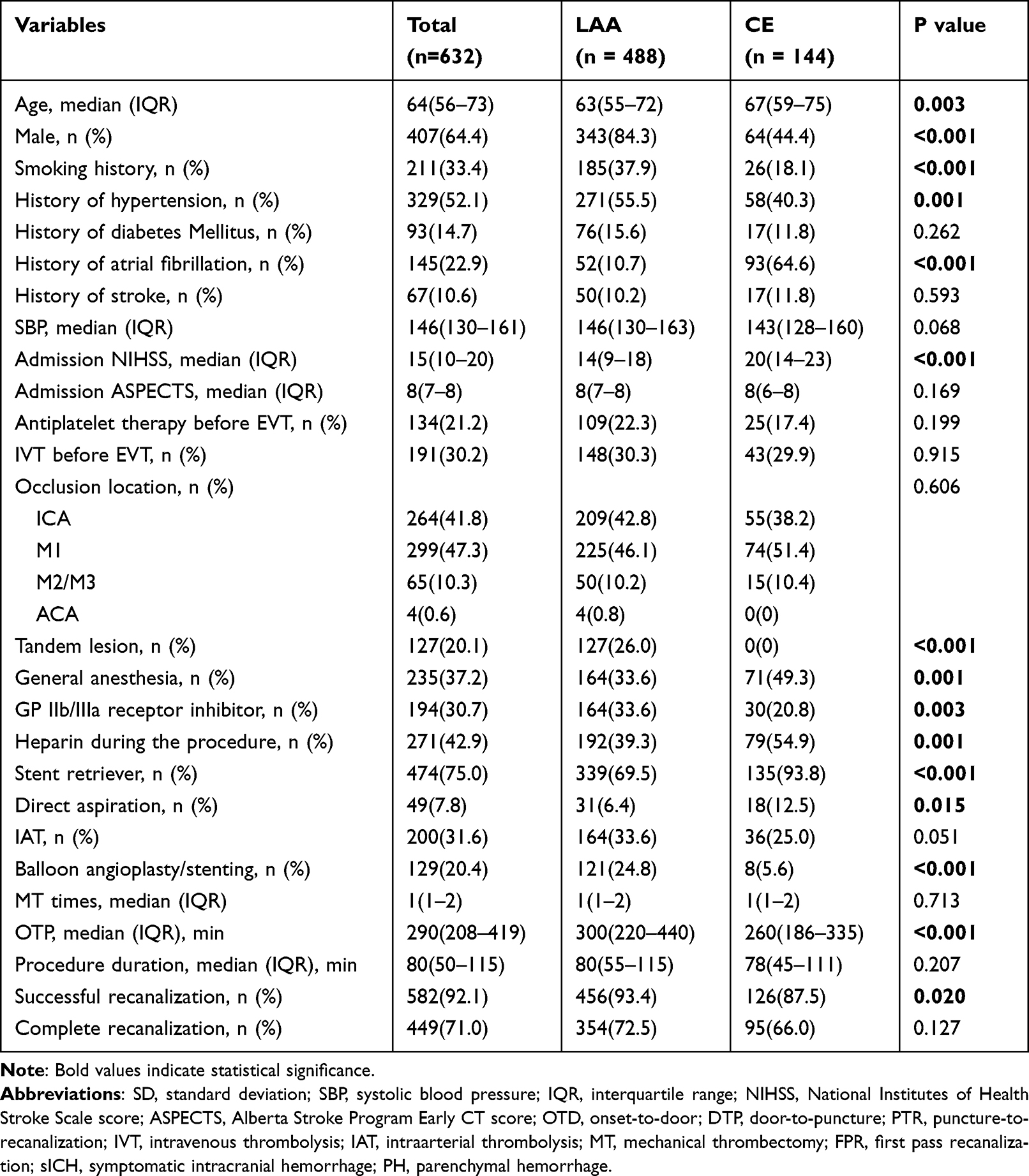 |
Table 1 Baseline Characteristics and Outcome of Between LAA and CE |
Study Outcomes
After adjusting for the confounders, the primary outcome (90-day mRS 0–2) was not significantly different between LAA and CE groups (55.7% vs 43.1%; OR: 1.19, 95% CI:0.92–1.53, P=0.190) (Figure 2). Similarly, However, the incidence of death within 90 days did not significantly differ between the LAA and CE groups (10.9% vs 24.3%, OR 0.91, 95% CI 0.66–1.25, P=0.545), nor did the occurrences of symptomatic intracranial hemorrhage (SICH) within 48 hours (4.5% vs 9.7%, OR 1.08, 95% CI 0.65–1.78, P=0.779) or intracranial hemorrhage (ICH) within 48 hours (21.9% vs 30.6%, OR 0.94, 95% CI 0.71–1.25, P=0.680). Other outcomes were also similar between LAA and CE groups (P > 0.05) except for the 90-day mRS 0–3 (69.1% vs 56.9%; OR:1.32, 95% CI:1.02–1.72, P=0.038). Moreover, we adjusted for the PS as the sensitivity analysis and also found that EVT could lead to comparable clinical outcomes between LAA and CE groups (Table 2).
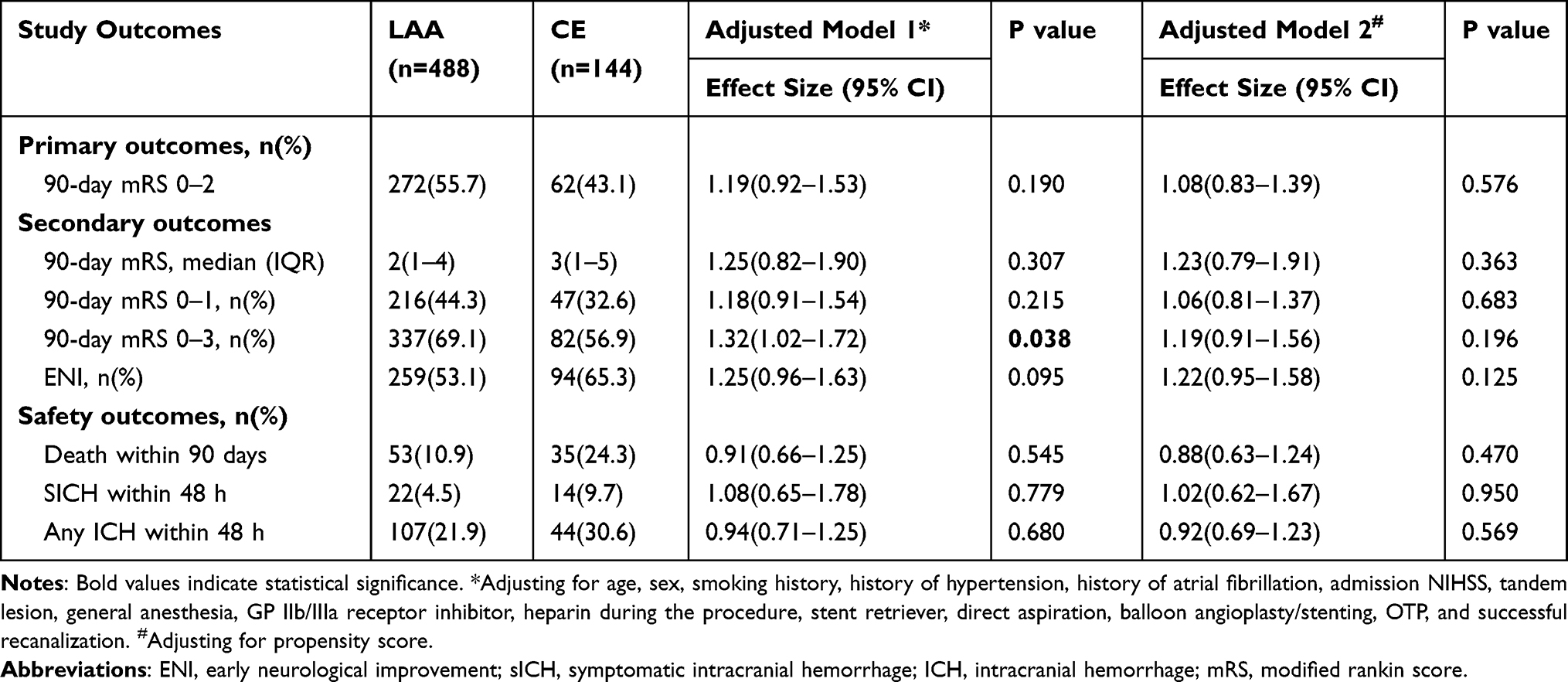 |
Table 2 Adjusted or/HR of Safety and Efficacy Outcome According to Different Pathogenic Subtypes |
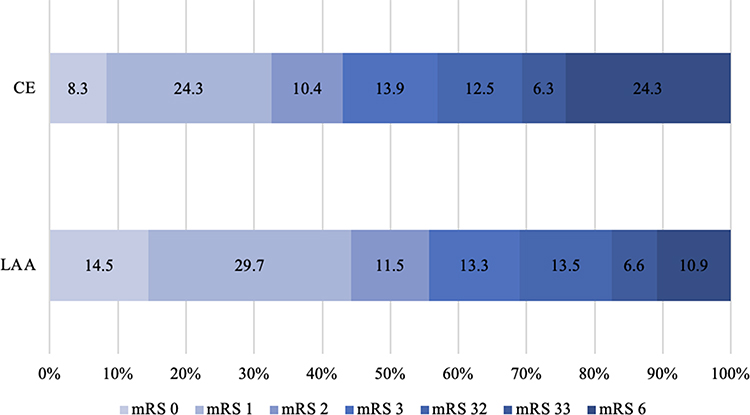 |
Figure 2 Shift on 90-day mRS score stratified by LAA and CE. Abbreviations: mRS, modified Rankin Scale; LAA, large artery atherosclerosis; CE, cardioembolism. |
Discussion
Our study based on the ANGEL registry found that (1) The rate of LAA was approximately three times higher than that of CE (77.2% vs 22.8%); (2) EVT could lead to similar clinical outcomes except 90-day mRS 0–3 between LAA and CE; (3) The 90-day mRS 0–3 rate is higher in LAA group than CE group; (4) Patients with LAA was younger, had lower NIHSS, longer OTP and higher successful recanalization rate than those with CE.
LAA and CE were the two main etiologies of LVO according to the TOAST standard. In the present study, the rate of LAA was higher than that of CE, which was different from the SITS registry,3 MR CLEAN registry,4 RESCUE-Japan Registry 2,7 and Bernese Stroke Registry.5 However, this result aligned with another Chinese registry, ANGEL-ACT registry,8 which reflected the distribution of TOAST classification of LVO in China. Similarly, a previous systematic review and meta-analysis further supported this trend, highlighting CE among whites and LAA among Asians as the predominant causes of ischemic stroke.15
Another finding of our study was that the efficacy and safety of EVT were not significantly different between LVO patients with LAA and CE, which was also found in RESCUE-Japan Registry 2,7 Bernese Stroke Registry,5 ANGEL-ACT registry,8 and a meta-analysis including 25 studies.3 Conversely, SITS registry indicated that a lower rate of functional independence in LVO patients with LAA than those with CE.3 Similarly, GSR-ET registry reported that EVT was more efficacy for LVO patients with CE than those with non-CE.6 However, MR CLEAN registry found that LVO patients with LAA had lower median 90-day mRS than those with CE but a similar functional independence rate between the two groups.4
Similarly to the previous studies, the present study revealed that LVO patients with LAA presented with lower admission NIHSS and longer OTP than those with CE.3,5,7,8 The phenomenon could be explained by that better collateral circulation was found in LAA than CE, which could lead to slow core volume growth and a longer time to complete vessel occlusion.4,16,17 Interestingly, we observed that LVO patients with LAA had a higher successful recanalization rate than those with CE but similar procedure duration. The previous studies reported that the clot length was longer in LAA than CE,4,18–20 and LVO patients with LAA were always associated with more arterial tortuosity,21 which may suggest LVO patients with CE more often experience successful recanalization by MT. However, paradoxically, the thrombus composition of CE had fewer red blood cells and more fibrin/platelets, which was associated with a decreased recanalization rate regardless of the technique employed.22,23 Patients in the LAA group less often received heparin during the procedure than those in the CE group. Patients in the CE group were always in a high coagulation state, which was a condition recommended heparin during the procedure in the protocol of the ANGEL registry.9 However, another analysis of the ANGEL registry found that heparin during the procedure was associated with a high risk of sICH and distal embolization, as well as efficacy outcomes over the long-term poor outcome, which was aline with the MR CLEAN-MED trial.13,24 Moreover, LVO patients with LAA account for the higher proportion of etiology distribution in China, and Chinese neurointerventions accumulated more experience in achieving successful recanalization for such patients by EVT such as rescue balloon angioplasty/stenting, or use of GP IIb/IIIa receptor inhibitor during the peri-procedural period.
Limitations
The present study had several limitations. First, our study was not a randomized controlled study, which could result in selection bias. Second, we did not collect some variables that influence our findings, such as collateral circulation, baseline infarct-core volume, penumbra volume, clot burden, and clot composition. Finally, all patients in our study were Chinese population, which limited our findings generalized to other ethnic populations.
Conclusions
Patients with acute anterior circulation LVO with LAA undergoing EVT were much more than those with CE in the ANGEL registry. The present study found the efficacy and safety of EVT were not modified by the stroke etiology such as LAA or CE.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study was performed in accordance with the guidelines of the 1964 Declaration of Helsinki and was approved by the ethics committees of all participating centers. Subjects or their legally authorized representatives provided written informed consent prior to commencing the study.
Acknowledgments
We thank all clinicians, statisticians, and imaging and laboratory technologists who were involved in the ANGEL registry. Dr. Huo moved to Beijing Anzhen Hospital, Capital Medical University from Beijing Tiantan Hospital, Capital Medical University in 2023.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agreed to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
All authors report no conflicts of interest in this work.
References
1. Goyal M, Menon BK, van Zwam WH, et al. Endovascular thrombectomy after large-vessel ischaemic stroke: a meta-analysis of individual patient data from five randomised trials. Lancet. 2016;387(10029):1723–1731. doi:10.1016/s0140-6736(16)00163-x
2. Adams HP, Bendixen BH, Kappelle LJ, et al. Classification of subtype of acute ischemic stroke. Definitions for use in a multicenter clinical trial. TOAST. Trial of Org 10172 in Acute Stroke Treatment. Stroke. 1993;24(1):35–41. doi:10.1161/01.str.24.1.35
3. Matusevicius M, Cooray C, Rand VM, et al. Stroke etiology and outcomes after endovascular thrombectomy: results from the SITS Registry and a Meta-Analysis. J Stroke. 2021;23(3):388–400. doi:10.5853/jos.2021.00850
4. Guglielmi V, LeCouffe NE, Zinkstok SM, et al. Collateral circulation and outcome in atherosclerotic versus cardioembolic cerebral large vessel occlusion. Stroke. 2019;50(12):3360–3368. doi:10.1161/strokeaha.119.026299
5. Zotter M, Piechowiak EI, Balasubramaniam R, et al. Endovascular therapy in patients with large vessel occlusion due to cardioembolism versus large-artery atherosclerosis. Ther Adv Neurol Disord. 2021;14:1756286421999017. doi:10.1177/1756286421999017
6. Tiedt S, Herzberg M, Küpper C, et al. Stroke etiology modifies the effect of endovascular treatment in acute stroke. Stroke. 2020;51(3):1014–1016. doi:10.1161/strokeaha.119.028383
7. Shirakawa M, Matsukawa H, Sakai N, et al. Endovascular therapy for acute ischemic stroke in patients with large-vessel occlusion due to atherosclerotic stenosis. J Stroke Cerebrovasc Dis. 2021;30(10):105960. doi:10.1016/j.jstrokecerebrovasdis.2021.105960
8. Huo X, Sun D, Raynald Jia B. Endovascular treatment in acute ischemic stroke with large vessel occlusion according to different stroke subtypes: data from ANGEL-ACT Registry. Neurol Ther. 2022;11(1):151–165. doi:10.1007/s40120-021-00301-z
9. Huo X, Ma N, Mo D, et al. Acute Ischaemic Stroke Cooperation Group of Endovascular Treatment (ANGEL) registry: study protocol for a prospective, multicentre registry in China. Stroke Vasc Neurol. 2019;4(1):57–60. doi:10.1136/svn-2018-000188
10. Barber PA, Demchuk AM, Zhang J, Buchan AM. Validity and reliability of a quantitative computed tomography score in predicting outcome of hyperacute stroke before thrombolytic therapy. ASPECTS Study Group. Alberta Stroke Programme Early CT Score. Lancet. 2000;355(9216):1670–1674. doi:10.1016/s0140-6736(00)02237-6
11. Anadani M, Marnat G, Consoli A, et al. Endovascular therapy of anterior circulation tandem occlusions: pooled analysis from the TITAN and ETIS Registries. Stroke. 2021;52(10):3097–3105. doi:10.1161/strokeaha.120.033032
12. Zaidat OO, Yoo AJ, Khatri P, et al. Recommendations on angiographic revascularization grading standards for acute ischemic stroke: a consensus statement. Stroke. 2013;44(9):2650–2663. doi:10.1161/strokeaha.113.001972
13. Yang M, Huo X, Gao F, et al. Safety and efficacy of heparinization during mechanical thrombectomy in acute ischemic stroke. Front Neurol. 2019;10:299. doi:10.3389/fneur.2019.00299
14. Huo X, Raynald Gao F, Gao F. Characteristic and prognosis of acute large vessel occlusion in anterior and posterior circulation after endovascular treatment: the ANGEL registry real world experience. J Thromb Thrombolysis. 2020;49(4):527–532. doi:10.1007/s11239-020-02054-2
15. Ornello R, Degan D, Tiseo C, et al. Distribution and temporal trends from 1993 to 2015 of ischemic stroke subtypes: a systematic review and meta-analysis. Stroke. 2018;49(4):814–819. doi:10.1161/strokeaha.117.020031
16. Rebello LC, Bouslama M, Haussen DC, et al. Stroke etiology and collaterals: atheroembolic strokes have greater collateral recruitment than cardioembolic strokes. Eur J Neurol. 2017;24(6):762–767. doi:10.1111/ene.13287
17. Lee JS, Bang OY. Collateral Status and Outcomes after Thrombectomy. Transl Stroke Res. 2023;14(1):22–37. doi:10.1007/s12975-022-01046-z
18. Fitzgerald S, Rossi R, Mereuta OM, et al. Large artery atherosclerotic clots are larger than clots of other stroke etiologies and have poorer recanalization rates. J Stroke Cerebrovasc Dis. 2021;30(1):105463. doi:10.1016/j.jstrokecerebrovasdis.2020.105463
19. Boodt N, Compagne KCJ, Dutra BG, et al. Stroke etiology and thrombus computed tomography characteristics in patients with acute ischemic stroke: a MR CLEAN Registry Substudy. Stroke. 2020;51(6):1727–1735. doi:10.1161/strokeaha.119.027749
20. Fitzgerald S, Rossi R, Mereuta OM, et al. Per-pass analysis of acute ischemic stroke clots: impact of stroke etiology on extracted clot area and histological composition. J Neurointerv Surg. 2021;13(12):1111–1116. doi:10.1136/neurintsurg-2020-016966
21. Kim BJ, Kim SM, Kang D-W, Kwon SU, Suh DC, Kim JS. Vascular tortuosity may be related to intracranial artery atherosclerosis. Int J Stroke. 2015;10(7):1081–1086. doi:10.1111/ijs.12525
22. Hund HM, Boodt N, Hansen D, et al. Association between thrombus composition and stroke etiology in the MR CLEAN Registry biobank. Neuroradiology. 2023;65(5):933–943. doi:10.1007/s00234-023-03115-y
23. Yeo LLL, Bhogal P, Gopinathan A, Cunli Y, Tan B, Andersson T. Why does mechanical thrombectomy in large vessel occlusion sometimes fail? A review of the literature. Clin Neuroradiol. 2019;29(3):401–414. doi:10.1007/s00062-019-00777-1
24. van der Steen W, van de Graaf RA, Chalos V, et al. Safety and efficacy of aspirin, unfractionated heparin, both, or neither during endovascular stroke treatment (MR CLEAN-MED): an open-label, multicentre, randomised controlled trial. Lancet. 2022;399(10329):1059–1069. doi:10.1016/s0140-6736(22)00014-9
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.