")
Back to Journals » Research and Reports in Urology » Volume 16
Outcomes of Hypospadias Repair Based on Surgical Techniques: A 4-Year Retrospective Study
Authors Gabra A , Beyari BM, AlNuwaiser SJ , Allaf SM, Alghanmi R, Alrayiqi R, Mosaad F, Kurdi M
Received 11 December 2023
Accepted for publication 21 March 2024
Published 27 March 2024 Volume 2024:16 Pages 79—87
DOI https://doi.org/10.2147/RRU.S451552
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Panagiotis J Vlachostergios
Aisha Gabra,1 Badr Mohammed Beyari,2 Sara Jamal AlNuwaiser,2 Sarah Mamdouh Allaf,2 Reem Alghanmi,2 Rahaf Alrayiqi,2 Faisal Mosaad,1 Mazen Kurdi1
1Division of Pediatric Surgery, Department of Surgery, King Abdulaziz University Hospital, Jeddah, Saudi Arabia; 2Faculty of Medicine and Surgery, King Abdulaziz University Hospital, Jeddah, Saudi Arabia
Correspondence: Aisha Gabra, Division of Pediatric Surgery, Department of Surgery, King Abdulaziz University Hospital, PO Box 80200, Jeddah, 21589, Saudi Arabia, Tel +966548545060, Email [email protected]
Purpose: This study aimed to report the outcomes of hypospadias repair performed at a tertiary-level hospital during 2018 to 2021.
Methods: A retrospective chart review of 119 patients was performed.
Results: The most frequent coronal hypospadias cases were distal. However, the most common scrotal hypospadias cases were proximal. The average age at the time of the first surgery was 2.4 years (standard deviation, ± 2.3 years). The tubularised incised plate technique was performed for 57 of these 119 patients. Urethral fistula was the most common complication associated with distal and proximal cases (23.96% and 30.43%, respectively). No significant correlation was observed between any complication and the surgical technique. Based on the logistic regression model, the duration of urethral stenting was statistically significant (p=0.025), indicating that a urinary catheter duration of more than 5 days resulted in a 2.9-times increased risk of postoperative urethral fistula.
Conclusion: Prolonged urethral stenting for more than 5 days may result in subsequent urethral fistula development. Neither the severity of hypospadias nor the surgical technique seems to affect postoperative complications.
Keywords: hypospadias, urethroplasty, tubularised incised plate
Introduction
Hypospadias is defined as arrested development of the normal urethra and foreskin on the ventral aspect of the penis resulting in an abnormal location of the external urethral meatus along the penile shaft to the scrotum or perineum.1 Hypospadias is the second-most common genital abnormality after undescended testis and the most common congenital penile abnormality among male patients. In the United States, hypospadias occurs in 1 of every 200 to 300 live births.2 The prevalence of hypospadias in Europe is approximately 18.6 of every 10000 live births, making it one of the most prevalent congenital defects among male newborns.3 Although the incidence of hypospadias in Saudi Arabia is undetermined, the high rate of consanguinity may contribute to the high number of cases of this congenital anomaly. The exact aetiology of hypospadias is unknown; however, a small number of cases (<5%) can be explained by androgen metabolism abnormalities or genetic defects, and the majority of cases are sporadic.4 The ideal duration of urethral catheterisation after hypospadias repair has been debated. Daher et al5 noted that complication rates after the Duplay procedure were positively associated with 7 days of catheterisation (p=0.008) and older age at the time of surgery (p=0.026). However, these factors were not significant when the Duckett technique was applied. In contrast, Zhou et al6 studied whether prolonged urethral catheterisation can reduce the incidence of urethral strictures after proximal hypospadias repair and found that 42 of 665 patients experienced urethral strictures. Therefore, to minimise the incidence of strictures, 4 to 6 weeks was the ideal duration of urethral stenting after proximal hypospadias repair.
This study presents the outcomes of hypospadias taking into consideration the effect of duration of urethral catheterisation at a tertiary-level hospital from 2018 to 2021.
Materials and Methods
This retrospective chart review study included all patients with distal or proximal hypospadias who underwent surgery at King Abdulaziz University Hospital. Patients who previously underwent hypospadias surgery at another hospital, patients with severe comorbidity, patients older than 13 years, and patients with megaureter were excluded.
The alternative hypothesis was as follows (There is a difference of the postoperative complications’ rate and types between Snodgrass and other surgical techniques.)
Approval was obtained from the Research Ethics Committee, Unit of Biomedical Ethics at King Abdul-Aziz University, Faculty of Medicine (reference number: 490–22). The medical records of 126 patients were reviewed. Initially, 650 records of patients who underwent hypospadias repair with International Classification of Diseases (10th revision) codes Q54.0, Q54.1, Q54.2, Q54.3, Q54.8, and Q54.9 were retrieved. The parents were contacted and fully consented to provide follow-up information. The guidelines outlined in the Declaration of Helsinki were followed.
After getting the parents’ agreement, the following variables were collected which includes, demographic data, results of the preoperative evaluation of the anatomical location of the meatus, associated urogenital anomalies or other medical conditions, and age at the time of the first hypospadias repair. Intraoperative variables included the surgical technique and urinary catheter size. Postoperative variables included postoperative complications (urethral fistula, meatal stenosis, urethral stricture, wound infection, glans dehiscence, penile curvature, penile rotation, and unfavourable cosmetic results), and urinary catheter duration.
Statistical Analysis
The statistical methods used during this study were appropriate for the data and research questions. Frequencies and percentages were used to describe the categorical variables, and means and standard deviations were used to describe the numerical variables. A Sankey diagram was used to visualise the associations between the hypospadias type, surgical technique, and complications status. The chi-square and Fisher’s exact tests were performed to determine associations between categorical variables. Binary logistic regression was performed to predict the occurrence of a complication based on certain preoperative and intraoperative factors. Data were analysed using IBM SPSS Statistics version 26 and R statistical software, and p<0.05 was considered statistically significant.
Results
The records of 119 patients were included in our study. Twenty patients (16.8%) had various associated urogenital anomalies in the form of cryptorchidism, penoscrotal web, congenital hydronephrosis, bifid scrotum, medullary nephrocalcinosis, and other conditions. Ninety-six patients (80.7%) had distal hypospadias and 23 patients (19.3%) had proximal hypospadias. Coronal hypospadias was the most common distal type, followed by glandular, sub-coronal, and mid-shaft hypospadias. Scrotal hypospadias was the most common proximal type, followed by penoscrotal and perineal hypospadias. The average age at the time of surgery was 2.4 years (SD, ±2.3 years). The tubularised incised plate (TIP) technique was the most common procedure performed for distal hypospadias. All the used surgical techniques for the management of distal and proximal hypospadias cases and the resultant complications’ rate are summarised in Figure 1.
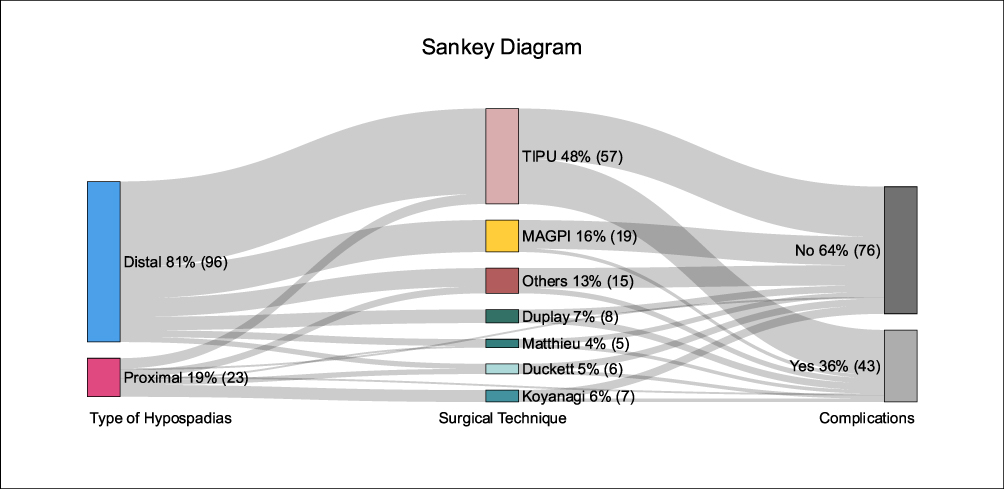 |
Figure 1 Sankey diagram visualizing the distribution of type hypospadias, surgical technique, and complications. Majority of cases were distal hypospadias and underwent TIP technique. Sixty-four% of the included patients had successful operations while 36% developed postoperative complications. TIP was applied to proximal hypospadias as well. |
A urethral stent was applied using an 8-Fr feeding tube catheter for 100 patients, 10-Fr feeding tube catheter for six patients, and 6-Fr feeding tube catheter for two patients. Patients were categorised into the following two groups based on the stenting duration: those whose duration was 5 days or less (53 patients; 54.6%) and those whose duration was more than 5 days (44 patients; 45.4%) (Table 1).
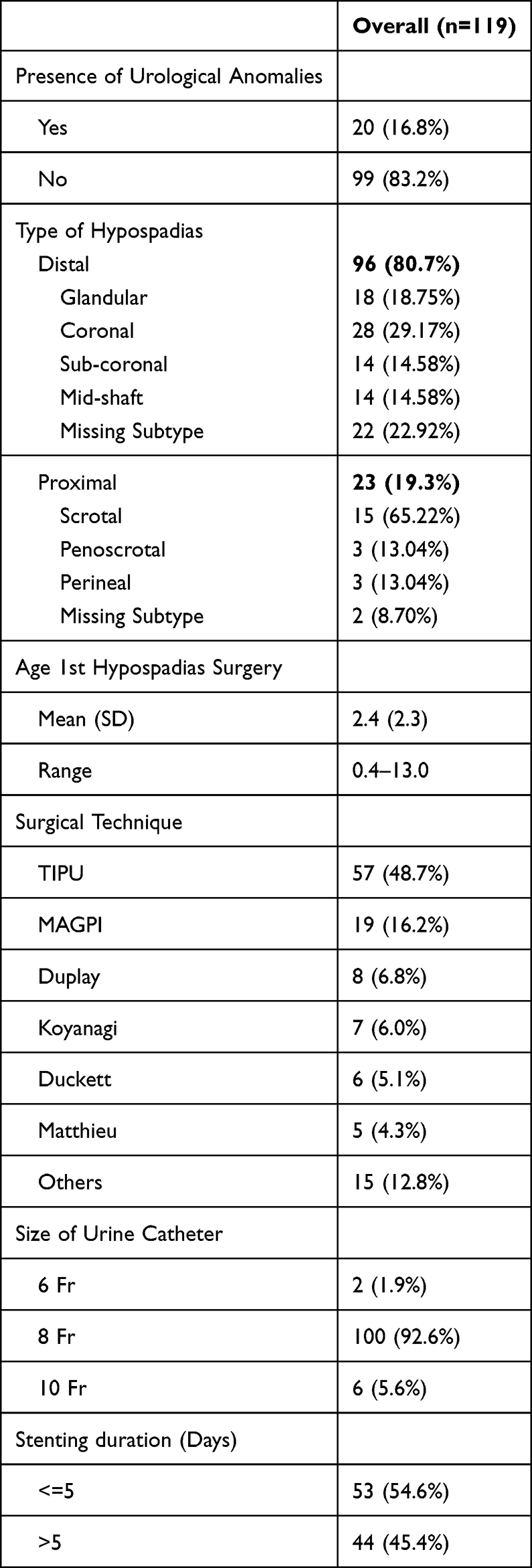 |
Table 1 Descriptive Analysis of the Clinical Features of Hypospadias |
Urethral fistula was the most common complication among distal and proximal cases (24% and 30%, respectively). Meatal stenosis was the second-most common complication among distal cases (12.5%). Among proximal cases, ventral penile curvature was the second-most common complication (13%). The rates and types of complications are detailed in Table 2. The correlation between postoperative complications and surgical techniques was not statistically significant (Table 3).
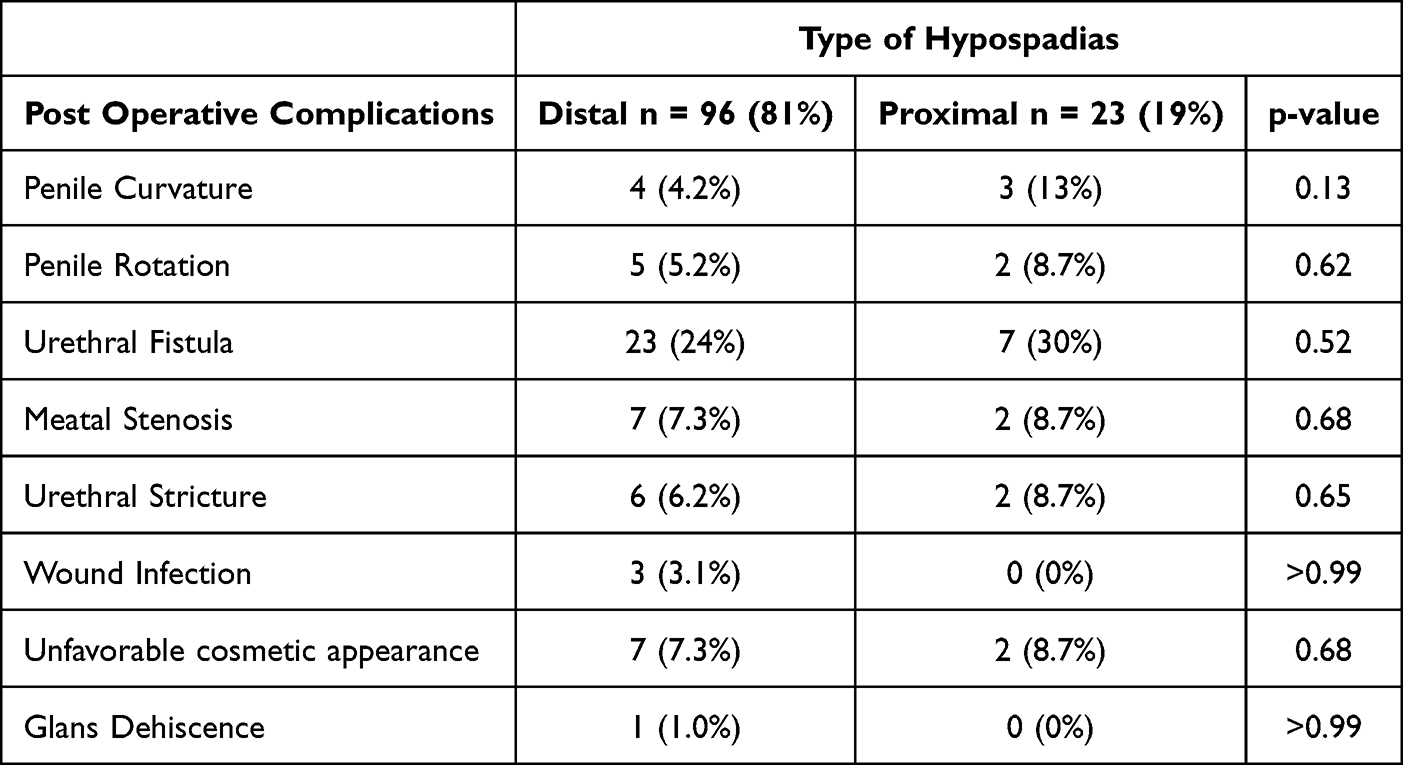 |
Table 2 Post-Operative Complications |
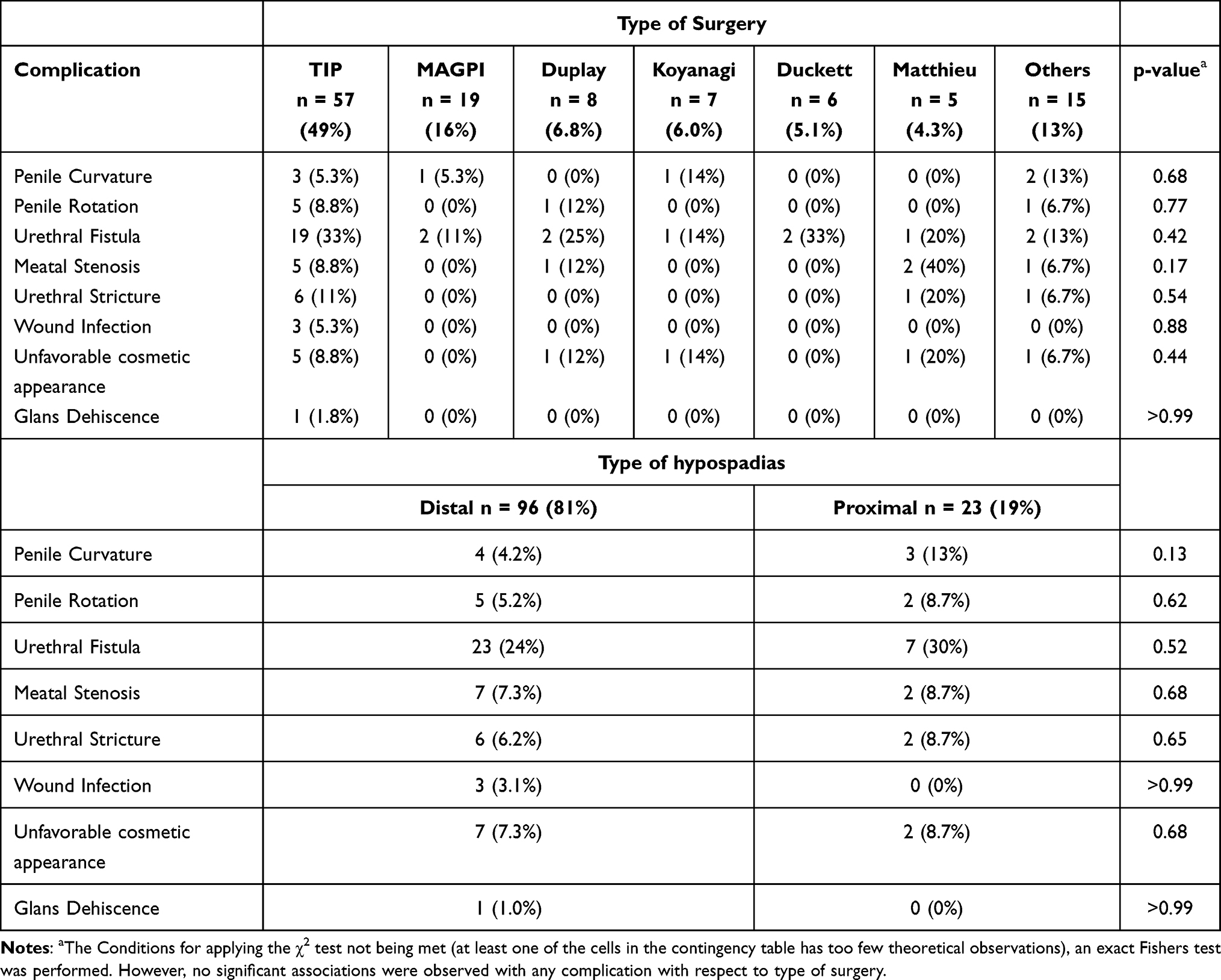 |
Table 3 Comparison of Complications by Type of Hypospadias and Type of Surgery |
A binary logistic regression model was used to evaluate the following predictors based on an alpha of 0.05: associated urological anomalies, associated medical conditions, age at surgery, hypospadias types, and urethral stent duration. The overall values of the model were insignificant [χ2(5)=8.89; p=0.114]. However, the regression coefficient for the urethral stent duration was statistically significant (β=1.0698; OR, 2.915; CI, 1.14–7.41; p=0.025), indicating that prolonged stenting for more than 5 days increases the risk of urethral fistula development by 2.9-times regardless of the surgical technique or severity of hypospadias. The other variables were insignificant.
The correlation between the hypospadias type and urethral stenting duration was statistically significant (p<0.001). Patients with distal hypospadias were more likely to undergo catheter removal within 5 days compared to patients with proximal hypospadias. Patients with a urethral fistula were significantly more likely had catheter removal after 5 days compared to those who did not have a urethral fistula (p=0.037). The other postoperative complications were not significantly associated with longer urethral stent durations (Table 4).
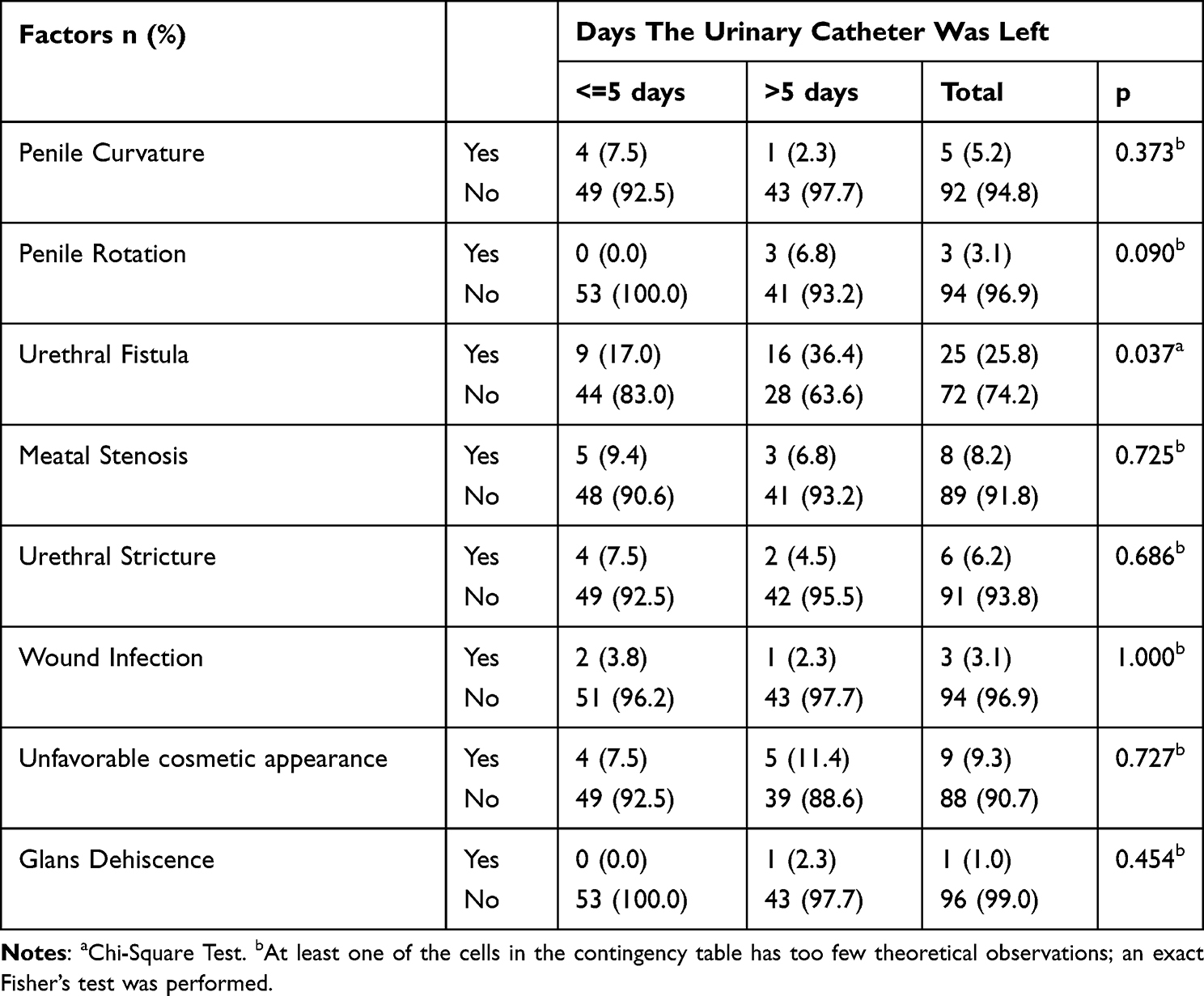 |
Table 4 Comparison of the Urethral Stent Duration with the Postoperative Complications |
Discussion
Because hypospadias impacts children psychologically and developmentally, the recommended age for surgery is 6 to 18 months.7 The mean age of the first hypospadias repair during our study was 2.4 years, and increased postoperative complications were not observed in regard to age. Most literature has stated that younger patients who undergo hypospadias surgery are less likely to experience complications than older patients. Dal et al7 found that patients older than two years were more prone to postoperative complications than younger patients. A retrospective study performed in China that included fifteen medical centres and patients with a mean age of 2.9 years found no significant correlation between age at the time of surgery and complications.8 Furthermore, Kim et al9 found no correlation between age at the time of surgery (younger than 1.5 years) and postoperative complications. Surgical repair at an older age may increase the risk of postoperative complications and that is attributable to the larger quantity of urethral secretions and overnight erections.3 Based on the previous literature, to increase patient safety, minimise the risk of complications, and obtain optimal results, surgeons and patients should plan surgery at an early age.
The surgical principles of hypospadias repair are penile degloving, orthoplasty, urethroplasty with vascularised coverage, glanuloplasty, and acceptable cosmetic results. Several surgical techniques can be applied either as single-repair or staged-repair. Urethroplasty techniques can be classified into tubularisation, augmentation, or replacement. Tubularisation comprises the Duplay and TIP techniques. In contrast, augmentation involves Snodgraft, Mathieu, and Duckett repair techniques. Replacement is reserved for severe forms of proximal hypospadias with a poor urethral plate and involves two-stage urethroplasty with initial graft placement and tubularisation or Koyanagi repair after 6 months of age.2
Incision of the distal urethral plate, which was first described in 1987, is performed to achieve sufficient widening of the urethral plate to enable tubularisation of the neourethra in which the urethral plate is tubularised after midline plate incision without a skin flap.10 In contrast, in 1994, Snodgrass incised the entire length of the urethral plate at the midline to tubularise these well-vascularised strips as the neourethra, followed by the application of a dartos patch for reinforcement.11 This TIP procedure gained popularity because of its simplicity, low complication rate, and acceptable cosmetic results; therefore, the TIP technique was the method of choice for treating distal hypospadias.12
In Saudi Arabia, a national survey revealed that the TIP procedure is performed most often by Saudi surgeons.13 We consistently used the TIP technique most frequently for our patients with distal and proximal hypospadias as well.
Thiersch-Duplay repair uses the urethral plate after creating lateral incisions and circumscribing the meatus.2 With the Mathieu technique, the neourethra is created using a proximal penile skin flap with the hypospadiac meatus at its base before performing glanuloplasty; the lateral edges of the flap are sutured to the urethral plate, and a vascularised subcutaneous flap is used to cover the suture line.14 One prospective study concluded that repair using the Mathieu technique is associated with lower complication rates and better cosmetic results than repair using the TIP technique.12 Some authors have reported that if the Mathieu technique includes incision of the urethral plate, then it may be superior to the TIP technique for patients with small glans.15 The Duckett technique, also known as transverse preputial island flap urethroplasty, utilises the inner preputial tissue to create the neourethra, while the axial vascular pedicle remains attached to the dorsal layer of the prepuce.16 This method is technically demanding and results in a complication rate higher than that of the TIP and the Onlay Island flap techniques.17 The Onlay Island flap is harvested from the dorsal preputial skin while preserving the pedicle to the base of the penis, followed by anastomosis of the flap to the urethral plate.18 Modified Koyanagi repair involves urethroplasty and results in the additional benefit of correcting any associated penoscrotal transposition with a vascularised parameatal-based foreskin flap, thereby allowing the use of the distal urethral plate as the base for the distal neourethra.19
Snodgrass et al20 encouraged to incorporate the urethral plate in the hypospadias repair as it showed healthy, well-vascularized connective tissue microscopically. However, his study included mainly patients with distal hypospadias. On the other hand, M. Sennert et al21 recommended excising the dysplastic urethral plate in proximal hypospadias with severe chordee as they lack the elastic fibers in the ventral penis with disorganized muscle fibers leading to hypoplastic corpus spongiosum. Moreover, the blood sinusoids are abnormally large, contributing to poor healing.
In order to improve the postoperative outcomes, Marcou et al22 depended on the quality of the urethral plate to decide two-stage hypospadias repair for non-proximal hypospadias patients instead of a single stage, which includes meatal caliber less than 8 Fr, shallow urethral groove, very thin distal urethra, or thick web tissue between the native meatus and the urethral groove.
Regarding postoperative complications, penile oedema is the most frequent early consequence of hypospadias repair, and its incidence is inversely related to the length of the procedure.23 MAGPI comprises a longitudinal incision of the dorsal aspect of the meatus that is closed using the transverse Heineke-Mikulicz method to advance the meatus distally, followed by glanuloplasty. This technique is widely performed for mild hypospadias cases and is associated with good cosmetic results and fewer complications.18 During our study, 36% of patients developed postoperative complications regardless of the surgical technique used, and the most common complication was urethral fistula.
Kim et al9 reported a postoperative complication rate of 24.4% (201/823 patients; distal cases, 17.9%; proximal cases, 55.1%), which was lower than that observed during our study (36.56%; distal cases, 58.3%; proximal cases, 78.26%), and urethral fistula was the most common complication during their study and ours.
Although the study by Kim et al9 found significant results and had a large sample size, the frequency of follow-up was higher during our study; furthermore, we were able to contact the parents via telephone to inquire about complications and compensate for our limited sample size. Additionally, their study period was between 2001 and 2017, and ours was between 2018 and 2022; therefore, our study indicated that surgical techniques have improved over time, resulting in fewer postoperative complications during our study.
Dokter et al24 revealed that 31% of patients developed complications after being treated with modified Mathieu repair based on the hypospadias objective scoring evaluation. Most of which are the urethral fistulas (n=40).
Meatal stenosis has a low occurrence rate postoperatively; however, our study showed that meatal stenosis was the second-most common complication. This may have occurred because we used multiple surgical techniques, which may have caused changes in the complication rates.
Glans dehiscence was observed in 14 of 34 patients in another study and in 1 of 119 patients in our study; however, these findings were insignificant. Because our study included many patients with glans dehiscence compared to the number of such patients included in other studies, glans dehiscence is considered to be overlooked in practice.25
In our study, chordee was more frequent in proximal hypospadias (13%) compared to distal hypospadias (4%) postoperatively. No significant result is found between the postoperative chordee and the duration of catheterization.
Zirong He et al26 found that postoperative constipation is an independent risk factor for complications after hypospadias repair (P=0.027; OR, 1.793; CI, 1.067–3.012) and recommended preoperative management of constipation for patients requiring hypospadias repair. During a controlled trial, Roth et al27 randomised seventy patients with mid-shaft or distal hypospadias who received either trimethoprim-sulfamethoxazole postoperatively or no antibiotic prophylaxis and found that antibiotic prophylaxis significantly decreased the incidence of asymptomatic bacteriuria but had no role in the prevention of other postoperative complications. Murakami et al28 assessed the role of preoperative and postoperative showering in the prevention of complications for 376 patients who underwent hypospadias repair by the same surgeon and found significantly fewer surgical site infections on the showering arm (P=0.023) and a low overall complication rate (P=0.0019); however, no significant difference in the urethral fistula rate was observed (P=0.081). They recommended that patients should shower two hours preoperatively, immediately after urethral stent removal, and after defecation to reduce the risk of complications after hypospadias repair.
Kumar and Dhayal29 compared the incidence of postoperative complications of 62 patients who underwent the TIP technique based on the urinary catheter duration (<5 days or >5 days) and found that early postoperative complications (wound infection, urinary tract infection, urinary retention) and the rates of urethral fistula (6.3% and 6.7%, respectively) and meatal stenosis (9.4% and 6.7%, respectively) were similar.
In Saudi Arabia, Alsowayan13 found that Saudi surgeons tended to prolong the stent duration with proximal hypospadias compared to that with distal hypospadias.
Although we relied on the parent’s evaluation of postoperative outcomes, which is considered a patient-important outcome, the lack of a unified objective postoperative assessment was an important limitation of our study. Recall bias was another limitation; however, it could be overcome by performing a cohort study instead of a retrospective chart review study. Our patients underwent surgery performed by seven different surgeons with variable skill levels; therefore, procedural preference bias related to the surgical technique occurred.
Conclusion
Histology of urethral plate may play a role in the postoperative outcomes. Therefore, further studies are needed to correlate between the urethral plate histological characteristics and the development of postoperative hypospadias outcomes. Prolonged urethral stenting is related to urethral fistula development after hypospadias repair. Urethral stenting after hypospadias surgery should be evaluated by a controlled prospective study that considers other related confounding factors and assesses long-term outcomes of surgical techniques for hypospadias.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not-for-profit sectors.
Disclosure
The authors certify that they have no affiliations with or involvement in any organization or entity with any financial or non-financial interests.
References
1. Baskin LS. Hypospadias and urethral development. J Urol. 2000;163(3):951–956. doi:10.1016/S0022-5347(05)67861-5
2. Keays MA, Dave S. Current hypospadias management: diagnosis, surgical management, and long-term patient-centred outcomes. Can Urol Assoc J. 2017;11(1–2):48–53. doi:10.5489/cuaj.4386
3. van der H, de Wall LL. Hypospadias, all there is to know. Eur J Pediatr. 2017;176(4):435–441. doi:10.1007/s00431-017-2864-5
4. Baskin LS, Ebbers MB. Hypospadias: anatomy, etiology, and technique. J Pediatr Surg. 2006;41(3):463–472. doi:10.1016/j.jpedsurg.2005.11.059
5. Daher P, Khoury A, Riachy E, Atallah B. Three-week or one-week bladder catheterization for hypospadias repair? A retrospective-prospective observational study of 189 patients. J Pediatr Surg. 2015;50(6):1063–1066. doi:10.1016/j.jpedsurg.2015.03.050
6. Zhou G, Jiang M, Liu X, et al. Effect of prolonging the duration of stenting on urethral stricture in proximal hypospadias with severe curvature repair: a prospective cohort study. Eur J Pediatr Surg. 2023. doi:10.1055/s-0043-1769797
7. Dale J, Woodward B, Elagami H. Age-dependent early complications of hypospadias repair: a single institutional experience. Pediatr Surg Int. 2023;39(1). doi:10.1007/s00383-023-05388-z
8. Fang YW, Sun N, Song HC, et al. A multicenter study on surgical procedure selection and risk factor analysis of postoperative complications after TIP and Duckett hypospadias repair. BMC Urol. 2022;22(1). doi:10.1186/s12894-022-01051-2
9. Kim JK, Shiff M, Chua ME, et al. Time to event analysis for post-hypospadias repair complications: a single-surgeon experience. World J Urol. 2021;39(10):3913–3919. doi:10.1007/s00345-021-03689-3
10. Sozubir S, Snodgrass W. A new algorithm for primary hypospadias repair based on tip urethroplasty. J Pediatr Surg. 2003;38(8):1157–1161. doi:10.1016/S0022-3468(03)00261-6
11. Eliçevik M, Tireli G, Sander S. Tubularized incised plate urethroplasty: 5 Years’ experience. Eur Urol. 2004;46(5):655–659. doi:10.1016/j.eururo.2004.05.007
12. Braga HLP, Lorenzo AJ, Pippi Salle JL. Tubularized incised plate urethroplasty for distal hypospadias: a literature review. Indian J Uro. 2008;24(2):219–225. doi:10.4103/0970-1591.40619
13. Alsowayan OS. Management of hypospadias in Saudi Arabia: a national survey. Urol Ann. 2018;10(4):391–394. doi:10.4103/UA.UA_88_18
14. Wilkinson DJ, Farrelly P, Kenny SE. Outcomes in distal hypospadias: a systematic review of the Mathieu and tubularized incised plate repairs. J Pediatr Urol. 2012;8(3):307–312. doi:10.1016/j.jpurol.2010.11.008
15. Kurdi MO, Eldessouki NI, Khirallah MG. Hybrid Mathieu urethroplasty vs. tubularized incised plate urethroplasty for the management of distal penile hypospadias with a small glans. Front Pediatr. 2022;2022:10. doi:10.3389/fped.2022.876791
16. ElBakry A. Complications of the preputial island flap-tube urethroplasty. BJU Int. 1999;84:89–94. doi:10.1046/j.1464-410x.1999.00097.x
17. Wang C, Zhang ZC, Zhang DY, et al. A new modified Duckett urethroplasty for repair of proximal hypospadias with severe chordee: outcomes of 133 patients. BMC Urol. 2022;22(1). doi:10.1186/s12894-022-00993-x
18. Subramaniam R, Spinoit AF, Hoebeke P. Hypospadias repair: an overview of the actual techniques. Semin Plast Surg. 2011;25(3):206–212. doi:10.1055/s-0031-1281490
19. Vepakomma D, Alladi A, Ramareddy RS, Akhtar T. Modified koyanagi repair for severe hypospadias. Indian Assoc Pediatr Surg J. 2013;18(3):96–99. doi:10.4103/0971-9261.116041
20. Snodgrass W, Patterson K, Plaire JC, Grady R, Mitchell ME. Histology of the urethral plate: implications for hypospadias repair. J Urol. 2000;164:988–990. doi:10.1016/S0022-5347(05)67233-3
21. Sennert M, Perske C, Wirmer J, Fawzy M, Hadidi AT. The urethral plate and the underlying tissue: a histological and histochemical study. J Pediatr Urol. 2022;18(3):364.e1–364.e9. doi:10.1016/j.jpurol.2022.02.006
22. Marcou M, Bobbe SM, Wullich B, Hirsch-Koch K. Urethral plate characteristics in cases of non-proximal hypospadias may not be associated with a higher risk of complications when a two-stage repair is applied. Front Pediatr. 2022;10. doi:10.3389/fped.2022.900514
23. Shah H, Qazi UA, Gul H, Khan SA, khan R. Frequency of early complications after two staged AIVAR BRACKA (AB) repair of hypospadias. Khyber Med Univ J. 2015;8(3):334–338.
24. Dokter EM, Mouës CM, van Rooij IA, Van Der BJJ. Complications after hypospadias correction: prognostic factors and impact on final clinical outcome. Eur J Pediatr Surg. 2018;28(2):200–206. doi:10.1055/s-0037-1599230
25. Durante L, Ghidini F, Panchieri F, et al. Glans dehiscence after severe hypospadias repair. Is it a real complication? Clues from a study in post-pubertal patients. Pediatr Surg Int. 2023;39(1). doi:10.1007/s00383-023-05387-0
26. Zirong H, Bo Y, Yunman T, Yu M. Analysis of factors associated with postoperative complications after primary hypospadias repair: a retrospective study. Transl Androl Urol. 2022;11(11):1577–1585. doi:10.21037/tau-22-691
27. Roth EB, Kryger JV, Durkee CT, Lingongo MA, Swedler RM, Groth TW. Antibiotic prophylaxis with trimethoprim-sulfamethoxazole versus no treatment after mid-to-distal hypospadias repair: a prospective, randomized study. Adv Urol. 2018;2018. doi:10.1155/2018/7031906
28. Murakami H, Seo S, Ochi T, Yazaki Y, Takeda M, Yamataka A. A useful tip for preventing surgical site infections after hypospadias repair. A single surgeon’s experience of 376 cases. Afr J Paediatr Surg. 2021;18(1):5–8. doi:10.4103/ajps.AJPS_17_18
29. Kumar A, Ram Dhayal I. A comparative study on the outcomes of hypospadias surgery following early versus late bladder catheter removal. Cureus. 2022;2022:1. doi:10.7759/cureus.26104
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.