")
Back to Journals » Nursing: Research and Reviews » Volume 14
Palliative Care Practice and Associated Factors Among Nurses Working in Chronic Care Units of Tertiary Hospitals in Ethiopia: A Cross-Sectional Study
Authors Gembe M , Tariku T, Tesfaye T , Hailu EH
Received 15 August 2023
Accepted for publication 3 February 2024
Published 8 February 2024 Volume 2024:14 Pages 45—58
DOI https://doi.org/10.2147/NRR.S431644
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pariya Fazeli
Maycas Gembe,1 Tizita Tariku,1 Temamen Tesfaye,2 Endalew Hailu Hailu2
1Department of Nursing, College of Health Science, Mattu University, Mattu, Ethiopia; 2School of Nursing, Faculty of Health Science, Jimma University, Jimma, Ethiopia
Correspondence: Maycas Gembe, Tel +251 936704900, Email [email protected]
Introduction: Palliative care is not yet widely available. Each year, approximately 58 million people worldwide require palliative care. In Africa, an estimated 9.7 million people require palliative care. In Ethiopia, the integration of palliative care into the country’s health system has taken several years. Previous studies conducted on palliative care have emphasized on the knowledge of nurses towards palliative care, and some studies have attempted to assess the practice of palliative care in specific areas of the country. However, we studied the practice of palliative care at a national level. So, the purpose of the study is to identify nurses’ palliative care practice level and factors associated with palliative care.
Methods: We employed a facility-based cross-sectional study design to assess palliative care practices. We considered tertiary hospitals with functional cancer centers. To conduct this study, we included nurses from three hospitals; we recruited 255 nurses from these hospitals. The dependent variable of palliative care practice of nurses was first measured in continuous scale measurement and then converted to dichotomous outcome variable based on a 75% score cutoff value. Based on the multivariable logistic regression output, we considered variables with a p-value of < 0.05 as the factors significantly associated with good palliative care practice.
Results: We collected data from 249 nurses, with a response rate of 98%. Based on our findings, 57% of nurses had good palliative care practices. We also identified that the type of healthcare facility, nurses’ knowledge of palliative care, nurses’ level of academic qualification, and nurses’ attitudes towards palliative care were factors associated with the level of palliative care practice.
Conclusion: This score of palliative care practice level should be improved. The Federal Ministry of Health, along with healthcare facilities in general and tertiary hospitals in particular, should strengthen good palliative care practice by providing up-to-date training for nurses.
Keywords: palliative care, nurses, tertiary hospital, Ethiopia
Introduction
According to the 2020 World Health Organization definition,
Palliative care is an approach that improves the quality of life for patients (adults and children) and their families who are struggling with life-threatening illnesses. It prevents and alleviates suffering through early identification, proper assessment, and treatment of pain and other physical, psychosocial, or spiritual problems.1
Palliative care is not widely available globally. Each year, approximately 58 million people are in need of palliative care worldwide, but only 14% of them receive it. 1,2 Again, of those people who are in need of palliative care, majority of them live in low- and middle-income countries.3 Particularly in Africa, an estimated 9.7 million people are in need of palliative care.4 Unnecessarily restrictive regulations for morphine, inadequate national policies, resources, and training on palliative care among health professionals are some of the reasons for poor implementation of palliative care.1
For wide range of life-limiting conditions, such as cancer, cardiovascular diseases, kidney failure, diabetes mellitus, multi-drug resistance tuberculosis, and human immune deficiency virus (HIV), palliative care relieves pain, promotes dignity, reduces unnecessary hospital admission, and ensures good death.5,6 The care begins early at diagnosis and continues through the course of the disease into family bereavement.7 A palliative care provider may help a patient in dealing with pain, shortness of breath, loss of appetite, nausea, fatigue, sleep problems, and many other symptoms. The primary goals of palliative care are to alleviate or ease suffering and to improve quality of life.6,8 For this to happen, it is essential for healthcare professionals to acquire adequate knowledge, the right attitude, and good interpersonal skills.9
For an effective palliative care provision, a team-based multidisciplinary approach is required from healthcare providers. Palliative care providers include doctors, nurses, social workers, religious or spiritual advisors, pharmacists, counselors, and others.6,8,10 Furthermore, these healthcare professionals can provide palliative care in tertiary care facilities, in community health centers, and even in children’s homes. Even if palliative care is an interdisciplinary approach to patient-centered care, nurses play a significant role in caring activities. As a palliative care provider, nurses’ roles include keeping patients pain-free, making patients comfortable, providing psychological and spiritual support, educating patients and their families, and establishing link between care providers.11 Since nurses spend most of their time caring for seriously ill patients, they develop special connection and trust with patients.12
In Ethiopia, palliative care was initiated in response to the HIV epidemic. During this time, public hospitals were overfilled with HIV patients, and anti-retroviral therapy (ART) was not widely accessible to the majority of HIV-infected individuals. To manage the burden of the HIV epidemic, a type of palliative care was being administered to patients.13 In 2003, Hospice Ethiopia was established with the aim of providing hospice and palliative care.13,14 However, the integration of palliative care into the country’s health system has taken several years. After a series of palliative care-related activities and interventions, the palliative care guidelines were proposed in 2016. Even if significant efforts have been made towards palliative care practice, an interdisciplinary and integrated approach to palliative care is still lacking.13
So far, regarding palliative care, studies conducted in Ethiopia have emphasized on knowledge of nurses towards palliative care,15–17 and some studies have assessed the practice of palliative care in specific areas of the country,18 limiting the generalizability of these studies. For instance, a study in Shire town, Tigray Region, northern Ethiopia, has shown the practice of palliative care at public health facilities in one town. The aforementioned study identified that 78% of the study participants had poor palliative care knowledge. Limitations of this study are that it included only one town in the Tigray Region, Ethiopia, and it only considered primary-level hospitals and did not include secondary and tertiary hospitals.18 As far as we are concerned, no study has been conducted on this topic at a national level. We also tried to assess some of the important factors related to the practice of nurses towards palliative care in the chronic care units of healthcare facilities; these factors included but were not limited to knowledge of nurses on palliative care, nurses-to-patient communication, institutional factors towards palliative care, and practice-related knowledge questions. Some of these factors were not well studied in previously conducted studies as these studies were inconclusive.15–18 In summary, the purpose of this study was to identify nurses’ palliative care practice level and factors associated with palliative care in chronic care units of selected tertiary hospitals in Ethiopia.
Methods and Materials
Study Design and Setting
We employed a facility-based cross-sectional study design to assess palliative care practices in selected tertiary hospitals in Ethiopia. We considered tertiary hospitals with functional cancer centers; there are six hospitals with functional cancer centers. Of the six hospitals, three were randomly selected for this study. The three hospitals were Tikur Anbessa Specialized Hospital, St. Paul’s Hospital Millennium Medical College, and Hawassa University Comprehensive Specialized Hospital. The first two hospitals are located centrally in the capital of Ethiopia, Addis Ababa, and the third one is located 275 km from the capital city. These hospitals are the final healthcare setups in the country’s patient referral system. These healthcare facilities are often the healthcare settings in which rare and complicated medical cases are managed. Healthcare professionals working in these hospitals include sub-specialists, specialists, general practitioners, nurses, radiologists, pharmacists, lab technicians, other healthcare professionals, and supporting staff. Nurses working in these hospitals are frontline care providers; we purposefully selected nurses working in these hospitals’ ART clinics, cancer centers, and chronic inpatient wards. This study was conducted from August 20, 2021, to September 21, 2021.
Sample Size Determination and Sampling Procedure
In these 3 hospitals, there were a total of 267 nurses who were working at ART clinics, cancer centers, and chronic inpatient departments. Before the sampling procedure was commenced, eligible nurses were considered part of the study population based on our inclusion criteria. The inclusion criteria were nurses working in cancer centers, ART clinics, and chronic inpatient wards. Based on this, we included 255 nurses actively working in chronic case teams: 149 from the Tikur Anbessa Specialized Hospital, 73 from St. Paul’s Hospital Millennium Medical College, and 33 from Hawassa University Comprehensive Specialized Hospital. Since we included all nurses working at the time of data collection, except for those who were on maternity leave or who were ill for an extended period beyond our study period, we minimized bias regarding the selection of our study participants.
Data Collection Procedure
A structured, self-administered questionnaire was used to collect data from the participants. We prepared the questionnaire by reviewing related literature. The questionnaire has seven sections: Socio-demographic factors (11 items); institution-related factors (4 items);19 knowledge about palliative care (13 items);20 Attitude of nurses towards palliative care (21 items); nurse to patient communication level (14 items);21 palliative care practice (11 items).22 Knowledge-related questions were mainly constructed to assess the general understanding of nurses towards palliative care. Knowledge about palliative care consists of 13 items; correct answer coded as 1, and the incorrect one coded as 0. Knowledge assessment scores range between 0 and 13. Similarly, the attitude questions were measured using 5-point likert scale, with scores ranges from 21 to 105. For an individual study participant, the lowest score given was 21, and the highest score given was 105. According to our study, those who scored an average and above average would have a favorable attitude. The level of nurse-to-patient communication was measured by considering Likert scale response; the average score per question was 3, and for an individual who scored more than 42 for a total of 14 questions, she/he would have good communication. Palliative care practice questions were constructed to assess what actually the nurses do when they are assigned to give care to patients who need palliative care; these questions were skill-related knowledge questions. For practice-related questions, each eleven items had multiple responses, and the scores ranged from 0 to 27; for each 11 questions, there were correct and incorrect responses. For an individual respondent, the total score from 11 practice-related knowledge questions was summed with a score of minimum value of 0 and a maximum score of 27; these scores were then converted into good or poor practice binary response items based on evidence from previous related research.22 Generally, a score of 75% and above and 50% and above of the total knowledge and attitude questions were used to classify study participants as having good knowledge and attitude, respectively. Again, a score of 42 and above was considered for participants as having good communication with patients. In this study, a score of 75% was used as a cutoff point to dichotomize our measurement for the palliative care practice variable; those participants who correctly answered 75% or above of all practice-related questions were considered to have good practice.
Prior to data collection, the data collectors explained the study objectives to the respondents or nurses, and written consent was obtained. The data collectors then distributed the self-administered questionnaire to the respondents. After the nurses completed the questionnaire, the data collectors collected it. Finally, data collectors checked the questionnaires for completeness.
Operational Definition
Nurses’ Knowledge
Nurse’s understanding about palliative care and classified as:22
Good knowledge: Refers to Nurses who scored points greater than or equal to 75% of the total score of the knowledge-related questions of Palliative Care Quiz for Nursing (PCQN).
Poor knowledge: Refers to Nurses who scored points less than 75% of the total score on the knowledge-related questions of PCQN.
Nurses’ Attitude
Nurses’ perceptions towards palliative care were classified as:23
Favorable attitude: Refers to Nurses who scored points more than or equal to 50% of the total score of Frommelt attitude towards care of the dying (FATCOD) Scale.
Unfavorable attitude: Refers to Nurses who scored points less than 50% of the total score on FATCOD Scale.
Level of Communication
Nurse communication level to patients. Classified as:21
Good communication: Refers to nurses those who scored point more than 42.
Poor communication: Refers to nurses who answered below or equals to 42.
Nurses’ Practice
Nurses’ actual application of their palliative care knowledge and classified as:22
Good Practice: Refers to Nurses who scored points greater than or equal to 75% of the total score on knowledge aspect practice questions.
Poor practice: Refers to Nurses who scored points less than 75% of the total score on knowledge aspect practice questions.
Data Quality Management and Data Analysis
To ensure data quality, we recruited data collectors from hospitals that were not included in the study by emphasizing their experience in data collection. We provided training for data collectors for two days; the training focused on the purpose of the study and the contents of the study tool. Before the actual data collection was commenced, we had conducted a pre-test on 5% of the respondents from Jimma Medical Center, south-west Ethiopia, to check whether the questions were simple, clear, and easily understandable.
We used EpiData version 3.1 and Statistical Package for Social Science (SPSS) version 25 statistical software for data entry and analysis, respectively. To identify the variables associated with palliative care practice, we first performed bivariate logistic regression analysis. Next, we checked the assumptions of logistic regression: we checked whether the log odds of nurses’ palliative care practice levels were linearly related to a continuous independent variable, and whether there was multicollinearity between independent variables. As a result, the log odds of the dependent variable was linearly related to a continuous independent variable, and there was no multicollinearity, with an independent variable variance inflation factor (VIF) of <10. Then, we transferred variables with a p-value of ≤0.2 in bivariate analysis into a multivariable logistic regression model to control for the effect of confounding factors. Finally, from multivariable logistic regression output, we considered variables with a p-value of <0.05, with 95% confidence interval (CI), as the factors significantly associated with palliative care practice. We checked inter-item consistencies for the variables using Cronbach’s alpha (knowledge 0.77 and attitude, 0.71). To check the adequacy of the final model, we performed the Hosmer–Lemeshow goodness-of-fit test. Based on the type of output, the results of the study are presented in text, tables, and graphs.
Ethics Approval and Consent to Participate
Ethical approval was obtained from the ethical review board of Jimma University (Ref. no. IHRPGD/376/21). We then submitted a copy of ethical clearance letter to each of the health facilities; these facilities, Tikur Anbessa Specialized Hospital, St. Paul Hospital Millennium Medical College, and Hawassa University Comprehensive Specialized Hospital, allowed us to conduct this study. All eligible study participants provided informed consent, and their participation was voluntary. We assured confidentiality by ensuring anonymity of names or any personal identity. We also assured them that there would be no exposition of data at the individual level.
Result
Socio-Demographic Characteristics
Out of 255 nurses who were expected to participate in the study, a total of 249 nurses filled out the self-administered questionnaire, with a response rate of 98%. Of these, 147 (59%) were from Tibur Anbessa Specialized Hospital, 71 (28.5%) were from St. Paul’s Hospital Millennium Medical College, and 31 (12.5%) were from Hawassa University Comprehensive Specialized Hospital. In this study, most respondents were females, 142 (57%). With regard to study participants’ age, the mean ± (standard deviation (SD)) age of the participants was 34 ± (6.79) year; higher proportions of nurses were in the age ranges of 20–30 (40.6%) and 31–40 (41.3%). More than half, 134 (53.8%), of the study participants were married, and 141 (56.6%) of them were Orthodox Christians. Of the total respondents, 132 (53%) were working in cancer centers. The following table (Table 1) shows socio-demographic characteristics of the study participants.
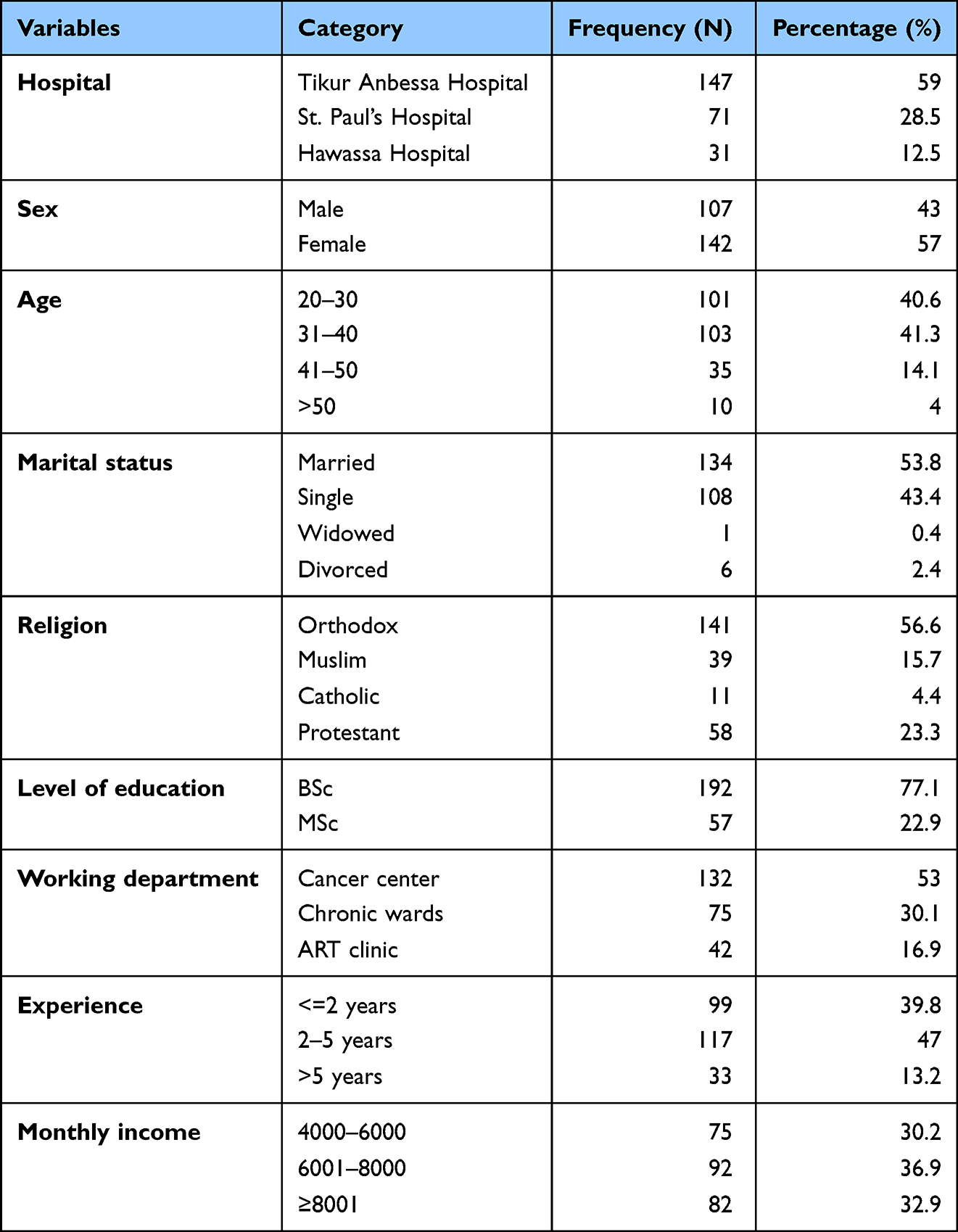 |
Table 1 Socio-Demographic Characteristics of Nurses Who Worked in Chronic Units of Tertiary Hospitals in Ethiopia |
Nurses Response to Institutional-Related Questions
Of the total respondents, only 81 (32.5%) of the study participants claimed they had received training on palliative care; of those who had received training, 12 (40.8%) received training in the last six months. In this study, the majority, 189 (75.9%), of nurses complained of a workload. Ninety-nine (39.8%) were using the palliative care guidelines; around 40 (40.4%) of nurses read palliative care guidelines on a monthly basis. The majority, 179 (71.9%), of nurses reported that there are barriers to delivering palliative care. Table 2 describes institutional-related factors for palliative care practice.
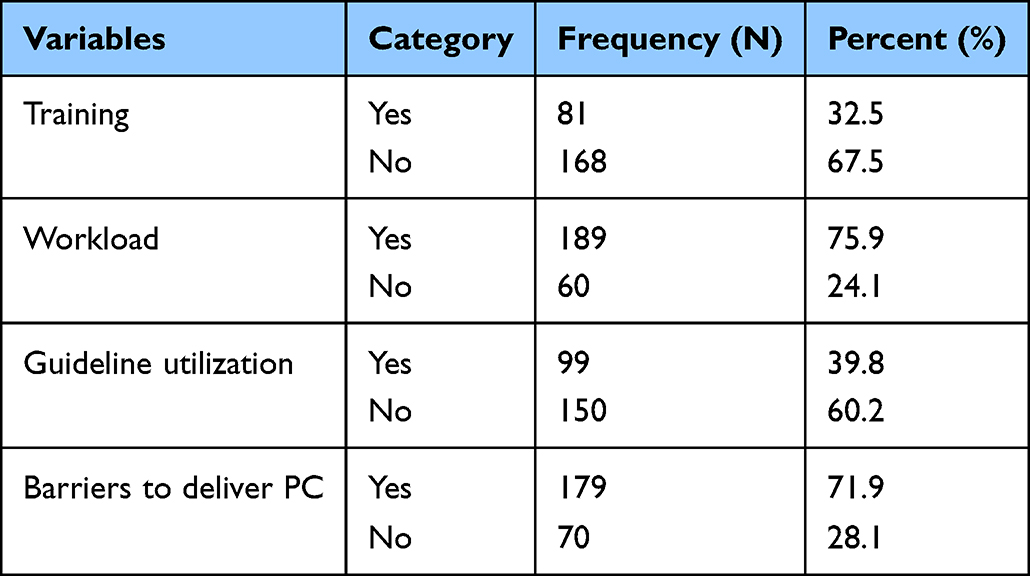 |
Table 2 Response of Tertiary Hospitals’ Nurses on Questions Related to Institutional Factors for Palliative Care |
Of the reported barriers (179), 88.1% of nurses mentioned time constraints as the major one. Again, 85.9%, 81.9%, and 85.3% of nurses stated insufficient staffing, lack of isolation room, and inadequate equipment, respectively, as the other institutional-related barriers to providing palliative care. Factors like unfavorable environment (80.6%) and lack of medications (34.1%) were also mentioned as barriers that hindered the quality of palliative care.
Knowledge and Attitude of Nurses Towards Palliative Care
Approximately 33.7% of the respondents said that palliative care was appropriate only in the downhill trajectory or deterioration of one’s health. The majority, 188 (75.5%), of nurses knew adjuvant therapies were important in managing pain. Similarly, 195 (78.9%) of nurses knew that the use of placebos was appropriate in the treatment of certain types of pain. Only 68 (27.3%) nurses knew that palliative care provision requires emotional detachment. One hundred and eighty-six (74.7%) study participants stated that terminally ill patients had the right to choose “Do not resuscitate” (DNR). Overall, we found that more than half (58.6%) of the respondents had good knowledge of palliative care. Knowledge-related characteristics of the study participants are presented in (Table 3).
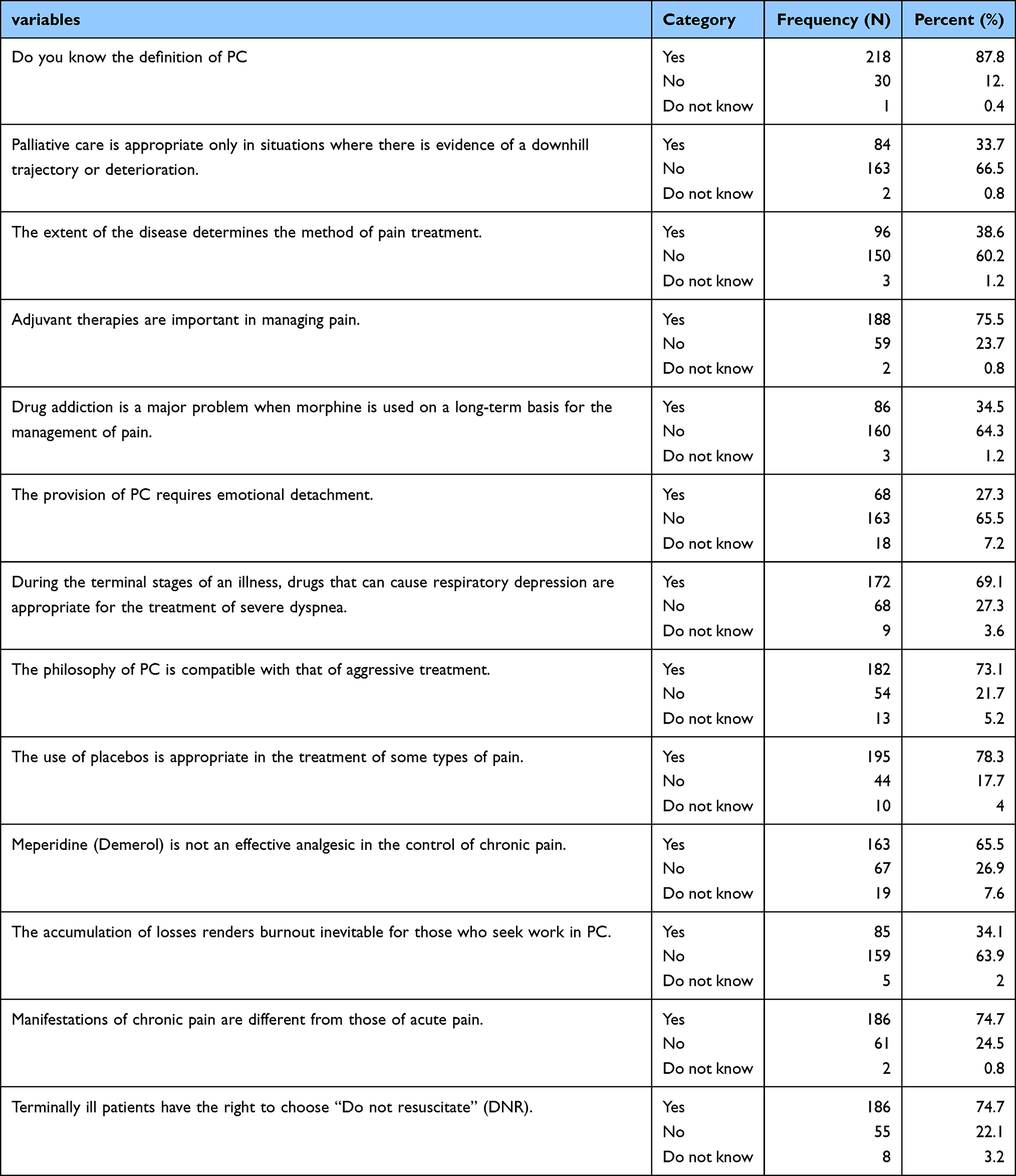 |
Table 3 Tertiary Hospitals’ Nurses’ Responses to Questions Regarding Their Knowledge of Palliative Care |
Among the study participants, the majority (71.1%) agreed that providing nursing care to patients was a worthwhile learning experience. About more than half, 128 (51.3%) of nurses stated that they would not want to be assigned to care for a dying person. With respect to relationship with family, 106 (42.5%) reported that it was difficult to form a close relationship with the family of a dying person. One hundred and forty-five (59.1%) nurses agreed that family should be involved in the physical care of a dying person. Approximately 158 (63.3%) of the study participants believed that it was beneficial for the dying person to verbalize his or her feelings. In general, among 249 respondents, 60 (71.9%) had a favorable attitude towards palliative care. Table 4 shows the attitude score of the study participants.
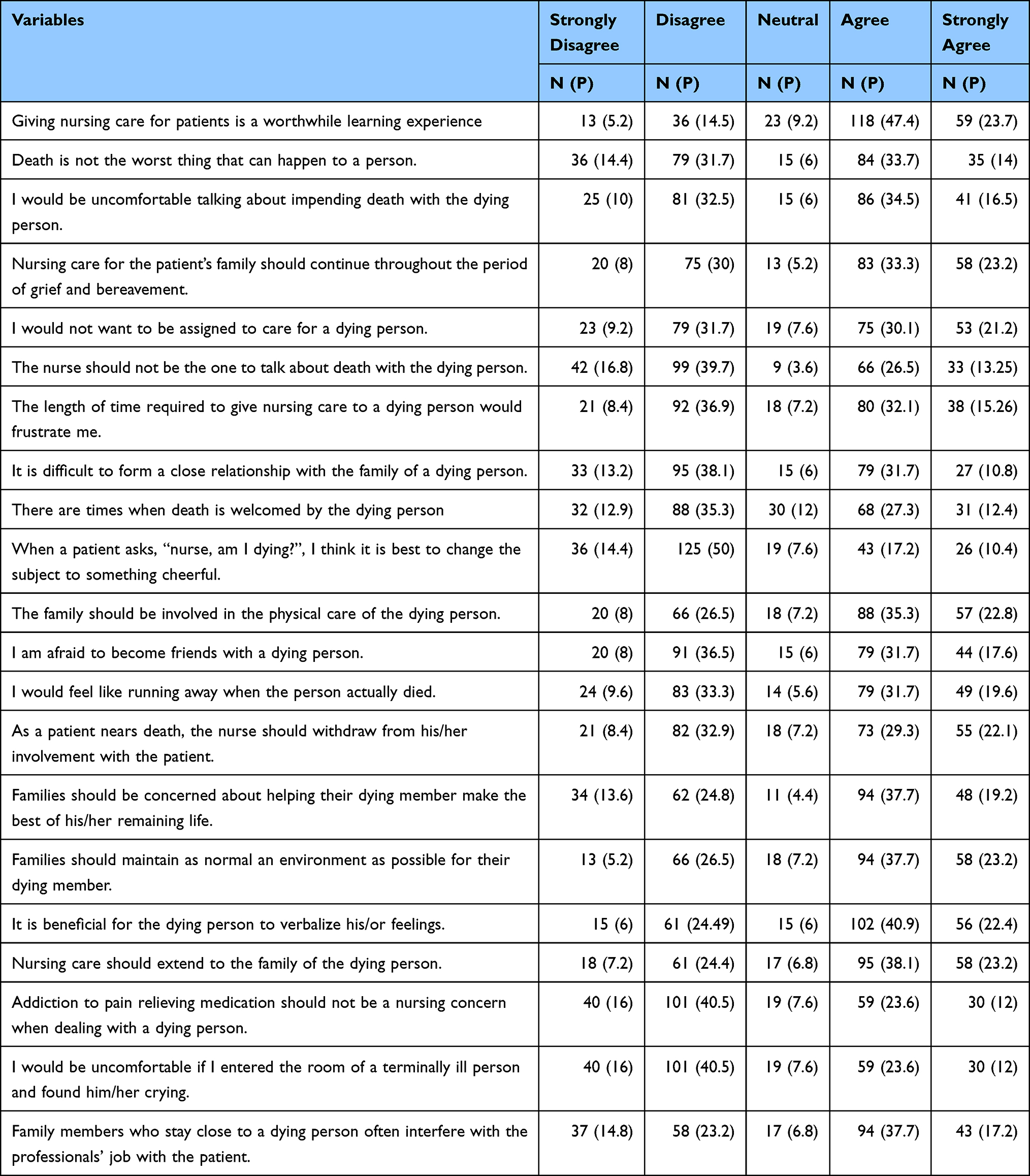 |
Table 4 Tertiary Hospitals’ Nurses’ Response to Questions on Attitude Towards Palliative Care |
Level of Nurse to Patient Communication
We identified that among the total respondents, about 129 (51.8%) of them often informed patients about their rights. Twenty-two percent of nurses always provided information on any diagnostic test, and 32% of nurses often provided this information. On the other hand, 39.9% and 20.8% of nurses informed their families about the health conditions of critically ill adult or child patients often and always, respectively. Approximately 61.4% of the respondents stated that they responded to patients’ concerns and complaints during patient stay at their hospital. The following table (Table 5) gives information about the nurse-to-patient communication score of the study participants. In summary, we found that approximately 67.1% of nurses had good communication with patients.
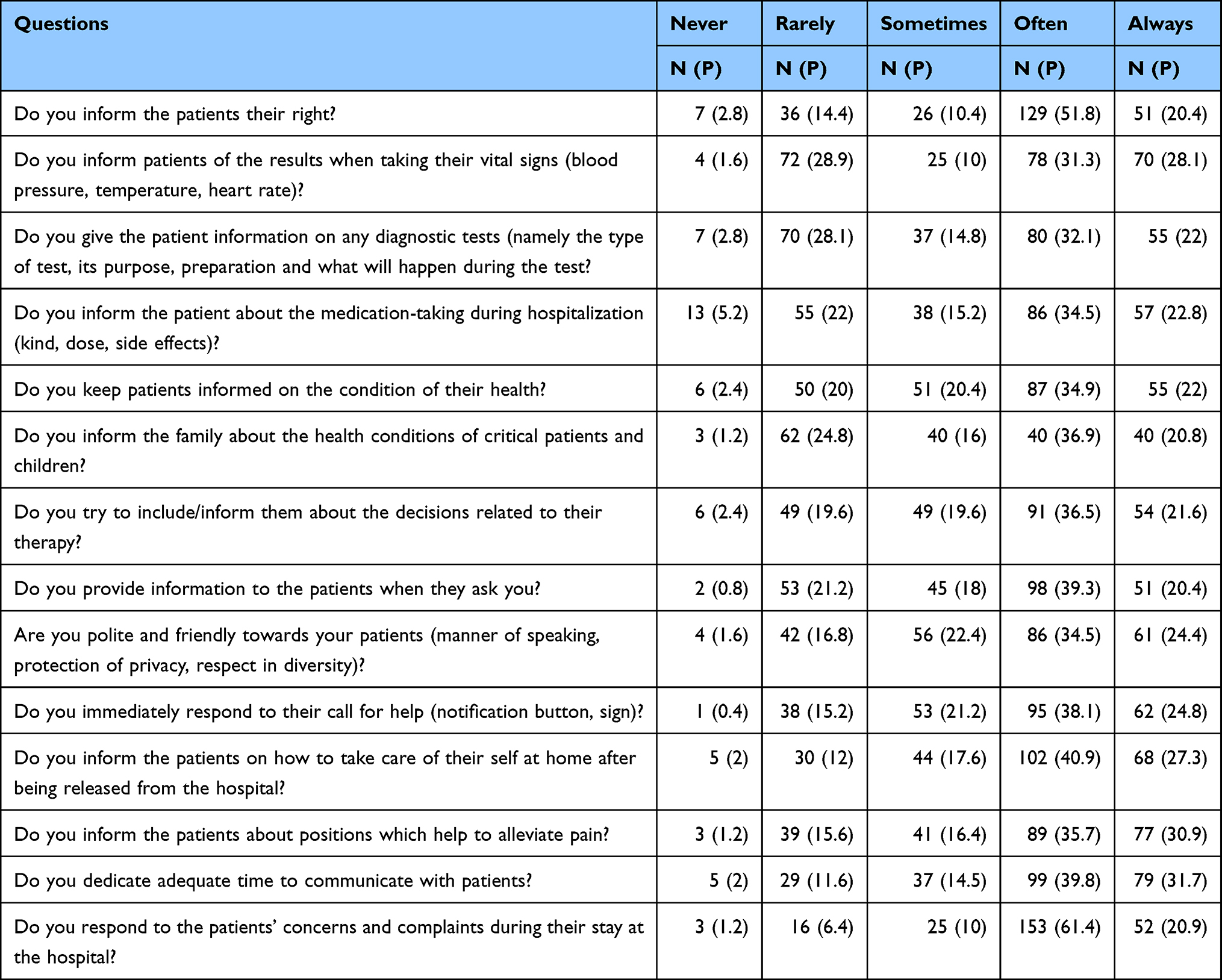 |
Table 5 Tertiary Hospitals’ Nurses’ Response to Each of the Nurses-to-Patient Communication Questions |
Palliative Care Practice
Among the study participants, 173 (69.5%) stated that palliative care discussions should be initiated during diagnosis. One hundred thirty-five (54%) nurses said that they inform terminally ill patients about their diagnosis. Similarly, 218 (62%) nurses considered family should be consulted on whether or not to tell patients about their diagnoses. To deal with the psychological problems of patients, 212 (85.1%) nurses provided emotional support. All study participants involved their own decision in decision-making processes related to the patient. Similarly, 201 respondents stated that they sought other health professionals’ opinions regarding their decisions. Regarding the use for pain management, 219 (88%) nurses used morphine. The aforementioned practice-related characteristics are presented in (Table 6). The overall palliative care practice level among nurses was 57%.
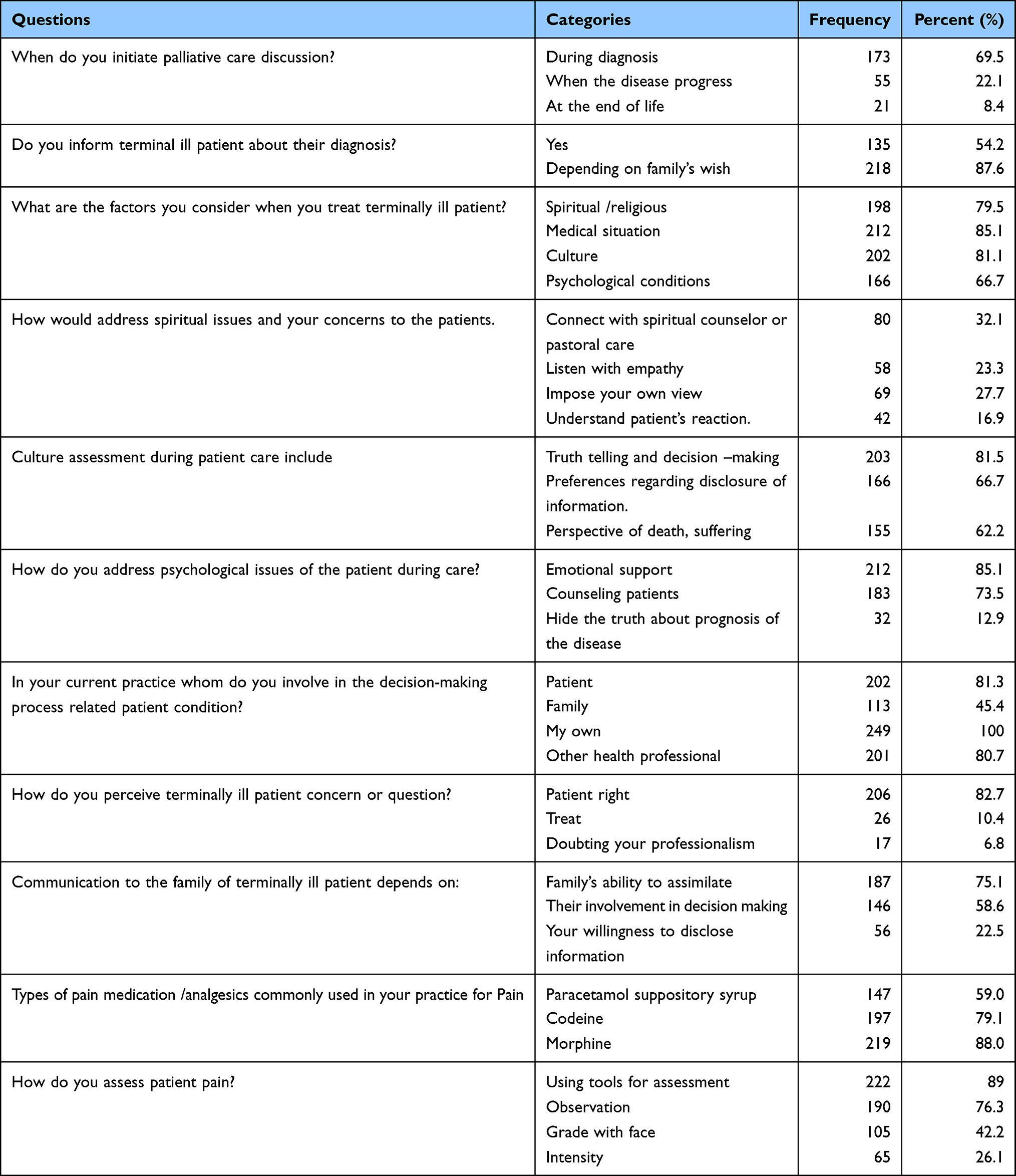 |
Table 6 Tertiary Hospitals’ Nurses’ Response to Each of the Palliative Care Practice-Related Questions |
Factors Associated with Nurses Practice Regarding Palliative Care
Bivariate logistic regression analysis was performed for all independent variables. Based on our bivariate logistic analysis, we noted that factors such as healthcare setting, nurses’ age, nurses’ educational level, nurses’ working department, nurses’ experience, palliative care training, palliative care national guideline utilization, nurses’ palliative care knowledge, and nurses’ attitudes towards palliative care were significantly associated with palliative care practice of nurses. We transferred variables with a p-value of less than 0.2 into a multivariable logistic regression to control for the effect of confounding factors. From multivariable logistic regression, we identified variables with a P-value less than or equal to 0.05, these variables were considered to be significantly associated with the dependent variable. In the multivariable regression analysis, the healthcare setting, educational level, knowledge, and attitude were significantly associated with nurses’ palliative care practices.
Based on the results of the multiple logistic regression analysis, nurses working in the chronic care unit of St. Paul’s Hospital Millennium Medical College were 5.4 times more likely to practice good palliative care than nurses working in the Tikur Anbessa Specialized Hospital. Those nurses who had Bachelor of Science (BSC) qualification were 65% less likely to practice good palliative care as compared to nurses who had Master of Science (MSc) degree qualification. The odds of good palliative care practice were 78% lower among those who had poor knowledge than their counterparts. Furthermore, participants who had unfavorable attitudes were about 68% less likely to have good palliative care practices as compared to nurses who had favorable attitude. Table 7 shows both the crude and adjusted odds ratio for variables included in multivariable logistic regression.
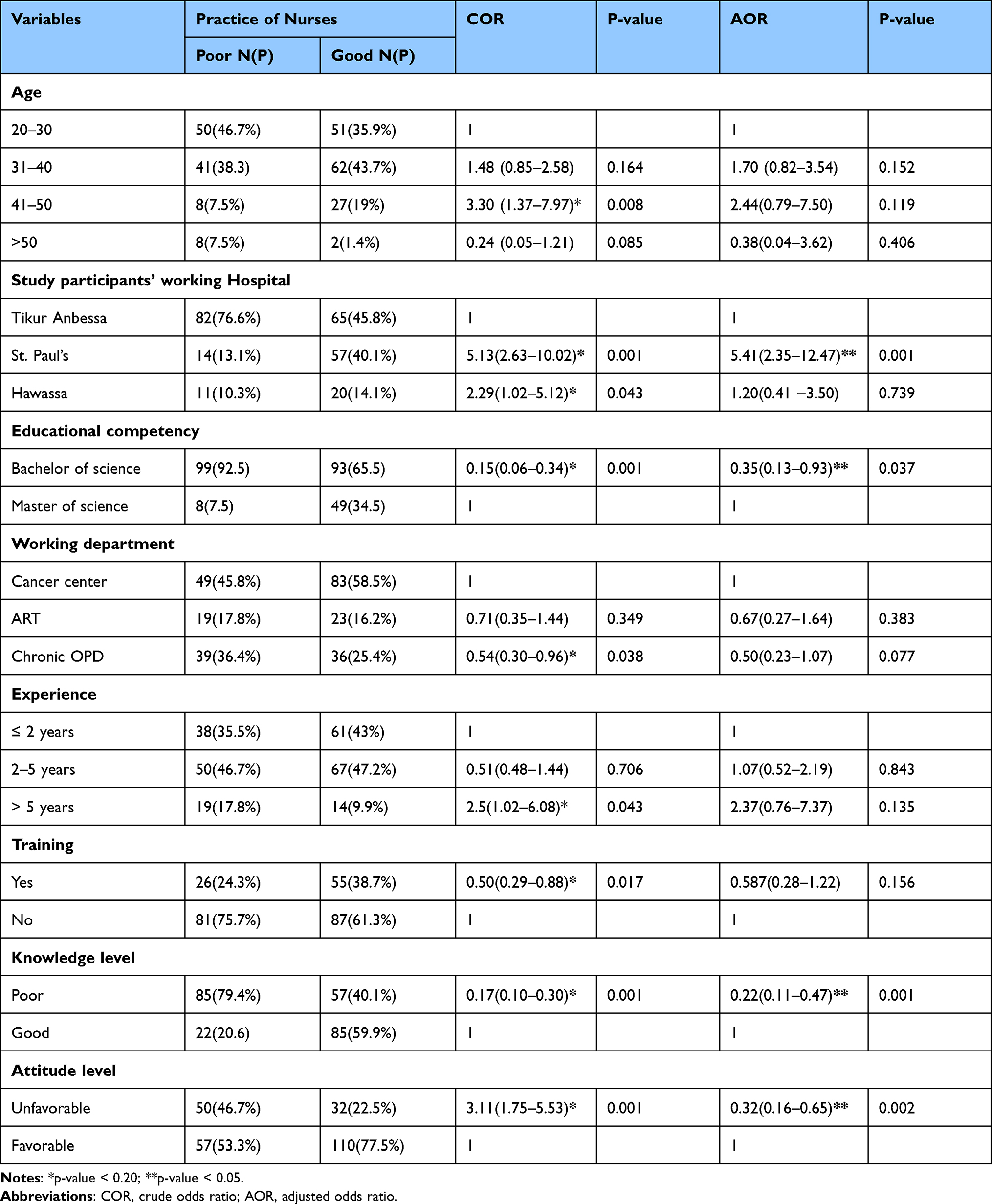 |
Table 7 Multivariable Logistic Regression Analysis of Tertiary Hospitals’ Nurses’ Practice of Palliative Care and Its Associated Factors |
Discussion
In this study, we included 255 nurses from three different tertiary-level hospitals found in Ethiopia, with a response rate of 98%. Of the total respondents, around 58% had good knowledge of palliative care. According to our study, a higher proportion of respondents had a favorable attitude towards palliative care. We attempted to determine the level of palliative care practice at the selected tertiary-level hospitals. Based on our findings, 57% of nurses had good palliative care practices. We also found that factors such as the type of healthcare facility, knowledge of palliative care, level of academic qualification, and nurses’ attitudes towards palliative care were associated with the level of palliative care practice.
Our findings regarding the practice of palliative care were higher than those of previous studies conducted in different parts of the world. For instance, studies conducted in the Philippines and Pakistan showed that the levels of palliative care practice among nurses working in hospitals found in these countries were relatively lower.24,25 This discrepancy could be explained by the fact that the palliative care knowledge of nurses working in hospitals in the Philippines and Pakistan was lower than the palliative care knowledge of nurses included in this study. According to the aforementioned studies, a relatively low level of nurses’ knowledge might affect the care of individuals with life-limiting diseases. Similarly, compared with the current study, the practice of palliative care was lower according to a study conducted in Eastern Nigeria.9 The numerical variation between these two studies might be attributed to the fact that the study conducted in Nigeria considered all types of healthcare facilities that were assumed to provide palliative care. In contrast, our study considered tertiary-level hospitals where the level of care and the hospital setup are considered to be improved.
In Ethiopia, several studies have been conducted in different settings;22,26,27 these studies were conducted to show the practice of palliative care in Addis Abeba, Jimma Zone, and Amhara Region, respectively. These studies revealed poor palliative care practices in each setting. As compared to our finding, a lower level of palliative care was noted among healthcare providers in these study facilities. One reason for these variations might be the type of healthcare facilities studied in previous studies, which is similar to the case in Eastern Nigeria,9 as discussed in the previous paragraph. Other factors like the time in which these studies were conducted and the level of staff competencies in these healthcare facilities could explain this difference.
Nurses working in the chronic units of St. Paul’s Hospital Millennium Medical College were about 4.5 times more likely to have good palliative care practice than nurses working in Tikur Anbessa Specialized Hospital. The likely explanation for the inconsistency in the level of practice between the hospitals could be the fact that St. Paul’s Hospital Millennium Medical College may have better organizational facilities, healthcare professionals might receive an updated guideline or different supportive learning materials, there might be better hospital policies towards palliative care, or there might also be equipment access that might contribute to better practice than the other hospitals.
Based on our findings, those nurses with a BSc degree were 65% less likely to have good palliative care practices as compared to those nurses with an MSc degree. In fact, as the level of education increases, the knowledge and the practice of nurses would improve in all areas of nursing care. Our finding is supported by the study conducted in the Philippines24 in which nurses who had an MSc degree qualification had better caring abilities than nurses who had a BSc degree qualification. Our finding is further strengthened by evidences from WHO5 and other similar studies;28,29 these studies suggested that attaining a higher level of education or having professional training experience would increase the quality of care.
Nurses with good knowledge were almost 4.3-fold more likely to practice good palliative care than their counterparts. This might be due to the fact that knowledge matters most for the provision of high-quality care, or palliative care, as mentioned on another study;30 this conclusion was also made by a study done in Jimma Medical Center, south-west Ethiopia.26 Nurses with good knowledge might spend most of their time engaging in searching and reading materials, which leads them to make more efficient decisions, intervene more independently, and control their work environment. In addition, because the present study area is chronic unit of tertiary hospitals, palliative care is more considerable. This would improve knowledge of nurses towards palliative care.
Nurses with favorable attitudes were approximately three times more likely to provide good palliative care than nurses with unfavorable attitudes. A possible explanation could be that having a good attitude has a positive impact on caring activities. Nurses working in these chronic case units may have had a good perception of palliative care or may have had experience that affected their attitude in a good way.27 These factors could impact nurses to develop a positive attitude towards palliative care and motivate them to work in collaboration with other staff for the effective management of patient complaints. In addition, since tertiary hospitals are at the top level of the healthcare system’s hierarchy, nurses’ positive attitudes may bring good quality healthcare services, which is not limited to palliative care.
Finally, this study was limited to assessing the self-reported practices of nurses due to the limited number of data collectors and time constraints. Thus, we recommend researchers, who will research on practice of palliative care, consider this study’s limitation and fill the gap by objectively assessing the practice of palliative care. Furthermore, researchers should also consider assessing the level of palliative care practice and the way to improve not only tertiary hospitals but also primary and secondary-level hospitals across the country.
Conclusion
This score of palliative care practice level should be improved. Since these nurses were working in chronic units at tertiary hospitals, where the necessary palliative care units were accessible, the palliative care practices of nurses should have been noteworthy. This result shows that hospital administrators should pay attention to palliative care. In addition, one can understand that the level of care at primary or secondary healthcare facilities would be much lower than the one we identified. Furthermore, this study identified that healthcare setting, nurses’ education level, nurses’ knowledge, and nurses’ attitudes towards palliative care were factors associated with palliative care practice. The Federal Ministry of Health, along with healthcare facilities in general and tertiary hospitals in particular, should strengthen good palliative care practice by providing up-to-date training for nurses. In addition, based on the evidence from this study, research has to be conducted, which shows the way to improve palliative care practices.
Acknowledgments
We would like to express our deepest gratitude to the School of Nursing, Institute of Health, Jimma University for offering us the opportunity to conduct this study. We also thank the three hospitals (Tikur Anbessa Specialized Hospital, St. Paul’s Hospital Millennium Medical College, and Hawassa University Comprehensive Specialized Hospital) administrations and staffs for their valuable cooperation during data collection.
Funding
We received no funds for this work.
Disclosure
The authors declare that they have no competing interests for this work.
References
1. World Health Organization. Palliative care-key facts; 2020. Available from: https://www.who.int/news-room/fact-sheets/detail/palliative-care.
2. World Health Organization. Palliative care for noncommunicable diseases: a global snapshot; 2019:1–4. Available from: https://www.who.int/publications-detail/ncd-ccs-2019.
3. Pease N, Dorman S. Palliative care. Medicine. 2007;35(5):292–295. doi:10.1016/j.mpmed.2007.03.011
4. African Palliative Care Association. Palliative care in Africa: the need; 2023. Available from: https://www.africanpalliativecare.org/awareness/palliative-care-in-africa-the-need/.
5. Giménez E, Muñoz-Cobo B, Solano C; Library WHO, Data C, Press WHO, Appia A, Press WHO. Planning and implementing palliative care services. Transpl Infect Dis. 2015;17(3):361–370. doi:10.1111/tid.12391
6. Worldwide hospice palliative care alliance. Universal health coverage and palliative care do not leave those suffering behind acknowledgements; 2014.
7. Care P. Palliative care: a special report. Afr Health. 2011;33(5):19–21.
8. Cross LL. Palliative care. Okla Nurse. 2002;47(3):15.
9. Anyanwu EC, Agbedia C. The practice of palliative care amongst nurses in selected hospitals in Eastern Nigeria. Open J Nurs. 2020;10(06):617–635. doi:10.4236/ojn.2020.106043
10. Dzierżanowski T. Definitions of palliative care – narrative review and new proposal. Palliat Med. 2021;13(4):187–200. doi:10.5114/pm.2021.114495
11. Sekse RJT, Hunskår I, Ellingsen S. The nurse’s role in palliative care: a qualitative meta-synthesis. J Clin Nurs. 2018;27(1–2):e21–38. doi:10.1111/jocn.13912
12. Westbrook JI, Duffield C, Li L, Creswick NJ. How much time do nurses have for patients? A longitudinal study quantifying hospital nurses’ patterns of task time distribution and interactions with health professionals. BMC Health Serv Res. 2011;11(1):319. doi:10.1186/1472-6963-11-319
13. Mamo Y, Habte A, W/Giorgis N, et al. The evolution of hospice and palliative care in Ethiopia: from historic milestones to future directions. Ethiop J Heal Dev. 2020;34(4):310–312.
14. Solomon S. A history of palliative care in Ethiopia; 2021. Available from: https://ehospice.com/international_posts/a-history-of-palliative-care-in-ethiopia-my-care-my-comfort/.
15. Wake AD. Knowledge and associated factors towards palliative care among nurses in Ethiopia: a systematic review and meta-analysis. SAGE Open Med. 2022;10:20503121221092336. doi:10.1177/20503121221092338
16. Abate AT, Amdie FZ, Bayu NH, Gebeyehu D, Gmariam T. Knowledge, attitude and associated factors towards end of life care among nurses’ working in Amhara Referral Hospitals, Northwest Ethiopia: a cross-sectional study. BMC Res Notes. 2019;12(1):1–8. doi:10.1186/s13104-019-4567-7
17. Getie A, Wondmieneh A, Mengesha A, Fitwi A, Gedefaw G, Demis A. Assessment of knowledge and attitude towards palliative care and associated factors among nurses working in North Wollo Hospitals. Ethiop J Health Sci. 2021;31(2):393–400. doi:10.4314/ejhs.v31i2.22
18. Zeru T, Gerensea H, Berihu H, Zeru M, Wubayehu T. Nurses practice towards palliative care in Shire endasilasie health facilities, northern Ethiopia: a cross-sectional study. Pan Afr Med J. 2020;35:1–7.
19. Tekalign T. Status of palliative care practice among health care providers working in health care setting of Jimma town, south west Ethiopia; 2016:86–88.
20. Ross MM, McDonald B, McGuinness J. The palliative care quiz for nursing (PCQN): the development of an instrument to measure nurses’ knowledge of palliative care. J Adv Nurs. 1996;23(1):126–137. doi:10.1111/j.1365-2648.1996.tb03106.x
21. Moges W, Solomon E, Worku A. Level of nurses to patients communication and perceived barriers in government hospitals of Bahir Dar City, Ethiopia, 2020. Clin J Nurs Care Pract. 2020;4(1):012–26. doi:10.29328/journal.cjncp.1001023
22. Kassa H, Murugan R, Zewdu F, Hailu M, Woldeyohannes D. Assessment of knowledge, attitude and practice and associated factors towards palliative care among nurses working in selected hospitals, Addis Ababa, Ethiopia. BMC Palliat Care. 2014;13(1):1–11. doi:10.1186/1472-684X-13-6
23. Access O, Tesfaye T, Anbessie Y, Gizaw BA. Palliative care practice and associated factors among nurses working in Jimma University Medical Center, Ethiopia. Palliative Med Care. 2018;2018:6–11.
24. Pasaol JC. Assessment of knowledge, attitude and practice and associated factors towards palliative care among health care providers to the pediatric oncology patients in southern Philippines.. J Clin Oncol. 2019;37(15_suppl):e21536–e21536. doi:10.1200/JCO.2019.37.15_suppl.e21536
25. Bibi F, Kausar S, Hussain HN, Kouser S, Khan S. Oncology nurses’ knowledge, attitude and practices towards palliative care in tertiary care hospitals of Lahore, Pakistan. Rawal Med J. 2020;45(1):66–70.
26. Tesfaye T, Anbessie Y, Belay A. palliative care practice and associated factors among nurses working in Jimma University Medical Center. Palliat Med Care. 2018;5(3):2374–8362.
27. Guadu T, Anteneh S, Kassa H, Demeke T. Assessment of nurses’ knowledge, attitude, practice and associated factors towards palliative care: in the case of Amhara Region Hospitals. Adv Biol Res. 2016;10(2):110–123.
28. Khoshnazar TAK, Rassouli M, Akbari ME, et al. Structural challenges of providing palliative care for patients with breast cancer. Indian J Palliat Care. 2016;22(4):459–466. doi:10.4103/0973-1075.191828
29. Rhee JY, Garralda E, Namisango E, et al. factors affecting palliative care development in Africa: in-country experts’ perceptions in seven countries. J Pain Symptom Manage. 2018;55(5):1313–1320.e2. doi:10.1016/j.jpainsymman.2018.01.009
30. Sorifa B, Mosphea K. Knowledge and practice of staff nurses on palliative care. Int J Heal Res Medico-Legal Pract. 2015;1(2):41–45.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.