")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Pandemic Responsiveness in an Acute Care Setting: A Community Hospital’s Utilization of Operational Resources During COVID-19
Authors McLean J, Clark C, McKee A, Legue S, Cocking J, Lamarche A, Heerschap C , Morris S, Fletcher T, McKee C, Kennedy K, Gross L, Broeren A, Forder M, Barner W, Tebbutt C, Kings S, DiDiodato G
Received 10 February 2022
Accepted for publication 2 June 2022
Published 14 June 2022 Volume 2022:15 Pages 1309—1321
DOI https://doi.org/10.2147/JMDH.S361896
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Jesse McLean,1 Cathy Clark,1 Aidan McKee,1,2 Suzanne Legue,1 Jane Cocking,1 Amanda Lamarche,1 Corey Heerschap,1 Sarah Morris,1 Tracey Fletcher,1 Corey McKee,1 Kristal Kennedy,1 Leigh Gross,1 Andrew Broeren,1 Matthew Forder,1 Wendy Barner,1 Chris Tebbutt,1 Suzanne Kings,1 Giulio DiDiodato1,3
1Royal Victoria Regional Health Centre, Barrie, ON, Canada; 2School of Medicine, Royal College of Surgeons in Ireland, Dublin, Ireland; 3Department of Health Research Methods, Evidence & Impact, McMaster University, Hamilton, ON, Canada
Correspondence: Giulio DiDiodato, Royal Victoria Regional Health Centre, 201 Georgian Drive, Barrie, ON, L4M 6M2, Canada, Email [email protected]
Background: To ensure continuity of services while mitigating patient surge and nosocomial infections during the coronavirus disease 2019 (COVID-19) pandemic, acute care hospitals have been required to make significant operational adjustments. Here, we identify and discuss key administrative priorities and strategies utilized by a large community hospital located in Ontario, Canada.
Methods: Guided by a qualitative descriptive approach, we performed a thematic analysis of all COVID-19-related documentation discussed by the hospital’s emergency operation centre (EOC) during the pandemic’s first wave. We then solicited operational strategies from a multidisciplinary group of hospital leaders to construct a narrative for each theme.
Results: Seven recurrent themes critical to the hospital’s pandemic response emerged: 1) Organizational structure: a modified EOC structure was adopted to increase departmental interoperability and situational awareness; 2) Capacity planning: Design Thinking guided rapid infrastructure decisions to meet surge requirements; 3) Occupational health and workplace safety: a multidisciplinary team provided respirator fit-testing, critical absence adjudication, and wellness needs; 4) Human resources/workforce planning: new workforce planning, recruitment, and redeployment strategies addressed staffing shortages; 5) Personal protective equipment (PPE): PPE conservation required proactive sourcing from traditional and non-traditional suppliers; 6) Community response: local partnerships were activated to divert patients through a non-referral-based assessment and treatment centre, support long-term care and retirement homes, and establish a 70-bed field hospital; and 7) Corporate communication: a robust communication strategy provided timely and transparent access to rapidly evolving information.
Conclusion: A community hospital’s operational preparedness for COVID-19 was supported by inter-operability, leveraging internal and external expertise and partnerships, creative problem solving, and developing novel tools to support occupational health and community initiatives.
Keywords: COVID-19, pandemic, infection, hospital, acute care, operational
Background
The emergence of the previously unknown severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) led to the rapid worldwide transmission of coronavirus disease 2019 (COVID-19).1 The relatively high infectiousness of SARS-CoV-2 and increased recognition that COVID-19 exhibits a diverse array of symptoms and complications1 have placed unprecedented strains on healthcare systems. With rates of hospitalization among COVID-19 patients ranging between 4% and 20% in different populations, and 25% of those cases requiring intensive care,2,3 hospitals and other acute care facilities have been impelled to shift operational priorities and strategies to maintain critical services while managing surges of acutely ill and infectious patients. Further adding to this burden, post-acute sequelae are experienced by the majority of hospitalized COVID-19 patients, which can lead to slow or incomplete recovery.4,5
As the ongoing pandemic monopolizes human and financial resources, operational transformation can be challenging for hospitals.6,7 Early in the pandemic, hospitals contended with a lack of empirical information regarding the pathophysiology, transmission, and treatment of COVID-19; however, rapidly evolving scientific literature, real-world data, and shared best practices helped inform on the clinical management of patients and efficient workflow strategies for various medical specialities.8–18 In contrast, only a few reports have discussed the non-clinical, operational strategies used by hospitals to manage their internal administrative resources during COVID-19. While previous respiratory outbreaks, such as the severe acute respiratory syndrome (SARS) emergency in 2003 and the H1N1 influenza pandemic in 2009, have underscored the importance of flexible, comprehensive emergency management planning,19–21 hospitals will often rely on generic plans that focus on localized, single-event disasters that are not designed for protracted outcomes22 and may not address various administrative barriers that are required for operationalizing a successful response.23,24
With a hospital’s capacity to respond to a pandemic often dependent on local expertise in infection prevention and control,21,25 this might place community hospitals at a particular disadvantage, as they often operate in geographic, administrative, and data silos, and are unable to access the same financial and human resources as their academic counterparts. This is of particular concern, considering that community hospitals serve as the primary healthcare site in most communities. For example, in Ontario, Canada’s most populous province, community hospitals operate as independent, not-for-profit organizations that are responsible for the majority of acute healthcare services provided to residents.26 As the experiences of community hospitals during the COVID-19 pandemic emerge, new operational tools will help these organizations better manage their resources during emergencies.
Here, we review and discuss key non-clinical, operational strategies and tools used by the Royal Victoria Regional Health Centre (RVH), a 408-bed acute care community hospital located in Barrie, Ontario. While RVH was the site of the first COVID-19-related death in Ontario, the hospital maximized efficient use of operational resources to mitigate nosocomial infections, create additional bed and staff capacity, accept patient transfers, and assist community partners in their own pandemic response. The objective of this work is to share this community hospital’s pandemic strategies and tools, such that peer organizations may benefit from this knowledge.
Methods
Design
A qualitative descriptive methodology was used for this study.27 This design was chosen as a result of limited information on the non-clinical, operational approaches taken by hospitals to manage their internal resources during a pandemic. This study sought to answer the question: what were the operational initiatives, strategies, and tools utilized by a large community hospital to respond to the COVID-19 pandemic? This study was conducted between June and August, 2020, near the tail end of the first pandemic wave in Ontario (March–August, 2020).
Setting
RVH is the largest acute care hospital within the Simcoe Muskoka region, an area located in the central portion of southern Ontario. The hospital provides basic birthing, medical, and surgical services, as well as a range of tertiary services, including advanced cardiac care, cancer treatment, renal care, child and youth mental health, and maternal and perinatal care, to a catchment population of 540,000 residents. In 2019–2020, RVH had an average of 1339 daily patient visits and was comprised of a team of 457 credentialed staff, 2959 employees, and 750 volunteers, with over 1000 student learners cycling through the hospital.
As of June 30, 2021, near the tail end of Ontario’s third COVID-19 wave (March–July, 2021), RVH had provided care for 535 COVID-19 inpatients and experienced 82 COVID-19 related deaths, including the provinces first laboratory-confirmed death on March 11, 2020. The hospital provided support to 30 long-term care (LTC) and retirement homes, assumed temporary, onsite management of an LTC home experiencing outbreak, accepted more than 220 patient transfers from other hospitals, performed 114,300 COVID-19 tests, and provided 87,400 COVID-19 immunizations. RVH did not experience any nosocomial infections among staff and patients until December, 2020.
Analysis
We performed a thematic review of all COVID-19-related documentation discussed at RVH’s Emergency Operation Centre (EOC) during the first wave of the pandemic (March–August, 2020). A qualitative content analysis according to Thomas (2006) was utilized in the development of themes.28 No pre-existing codes were applied to data; rather, codes, categories, and themes were inductively developed after lengthy review. Operational issues critical to RVH’s pandemic responsiveness emerged and could be binned into seven themes (Figure 1). We further solicited moderately structured, open-ended questions on operational initiatives and strategies to leaders involved in each theme to construct a narrative of events (Supplementary Box 1).
 |
Figure 1 A review of all COVID-19-related documentation discussed at RVH’s EOC committee between March-June, 2020, as well as COVID-19 documentation provided by external partners between February-June, 2020, identified recurrent themes critical to RVH’s pandemic response. |
Results
Organizational Structure
The emergency management program at RVH is a longstanding planning priority, with pre-existing emergency policies and standard operating procedures reviewed and updated every three years or earlier (eg, accreditation). In 2019, RVH undertook a review of its traditional EOC structure, aligning its emergency response and recovery processes with an Incident Management System (IMS) developed and updated by the Government of Ontario.29 Adoption of an IMS system permitted greater interoperability among clinical and external stakeholders by standardizing adherence to organizational structures, functions, processes, and terminology. The new IMS system was tested in an annual emergency exercise in November, 2019, which included the involvement of local public- and private-sector partners. RVH’s overall emergency response structure was further strengthened by a Pandemic Response Plan and Surge Capacity Plan, both reviewed and updated in 2019, as well as Business Continuity Plan, which was undergoing revisions in early 2020.
The hospital’s EOC was activated on March 13, 2020, one day after it received notification of its first lab-confirmed case of COVID-19 and two days after the World Health Organization declared COVID-19 a global pandemic. The EOC adopted a standard IMS organizational structure, consisting of an Incident Commander responsible for the overall coordination of Command Staff and General Staff. Over the first two weeks of operation, the EOC expanded its structure to address local needs, as new information about the natural history and transmissibility of COVID-19 emerged. To enable a more robust focus on clinical care, three interconnected pillars comprised the overall functional framework of the EOC structure: Clinical Care, Clinical Support, and Capacity Planning. Each pillar was divided into one or more traditional IMS functional sections, including Operations, Planning, Logistics, and Finance and Administration, which, in turn, were comprised of multiple clinical and/or administrative departments (Figure 2). During the most acute phase of first wave, which occurred from March-May, 2020, the EOC met once or twice daily.
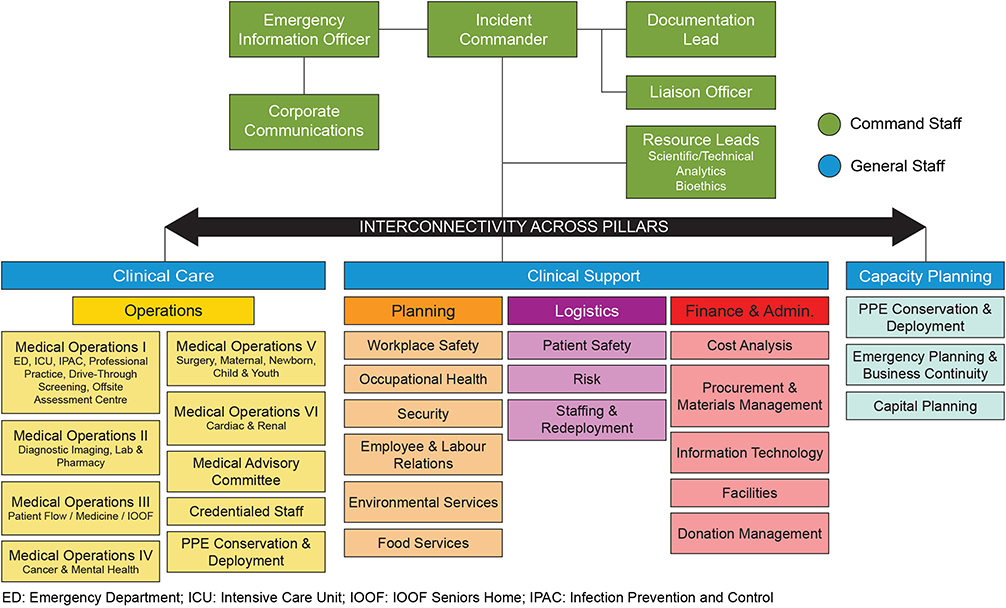 |
Figure 2 RVH’s modified EOC structure is based on a traditional IMS system, comprised of interconnected command staff (green) and general staff (blue), with clinical operations divided into clinical care, clinical support, and capacity planning. Non-traditional sections were added to fulfil local pandemic needs, including corporate communications and resource leads. |
Non-traditional IMS sections were also created, including a Corporate Communications section to synthesize and disseminate information, a Capacity Planning section to develop solutions for COVID-19 patient surge, and a Resource Leads section to provide evidence-based guidance on infection prevention and control, epidemiology, and bioethics (Figure 2). Resource Leads personnel included a Technical Specialist role, which was assigned to the hospital’s Infectious Disease Specialist, thus creating a direct link to the Infection Prevention and Control (IPAC) team, an Analytics Specialist role, comprised of research and decision support staff with knowledge of statistics, and a third-party bioethics consultant. The Safety Officer role, typically identified as Command Staff, was moved to the Planning section to better support the Occupational Health and Wellness and Human Resources departments.
Capacity Planning
Given the highly transmissible nature of SARS-CoV-2, patient surge was identified as a critical operational priority. Early modelling predicted between 842 and 93,826 cumulative hospitalizations in the region over the first three months, depending on the extent to which non-pharmaceutical public health measures would be implemented (eg, social distancing, contact tracing, quarantine, lockdown). To prepare for this wide range of hospitalization possibilities, detailed capacity plans were developed for the Intensive Care Unit (ICU), Medicine Program, and Emergency Department. A phased approach permitting the rapid conversion of existing clinical infrastructure to level III critical care units, standard beds, and cots, on an “as needed” basis. This permitted safe reallocation of existing inpatients, while maintaining other critical services (eg, decompensating ward-based patients, urgent non-elective surgeries) during surge conditions. In general, the first COVID-19 inpatient admission to each unit triggered implementation of the next phase.
Adapting re-purposed facilities to meet the technical requirements of critical care units was required for surge expansion. A design methodology termed Design Thinking30 was used by the RVH Capacity Planning team to address surge demand for increased air exchange, negative air capacity, anterooms, filtration, and exhausting. Using non-linear, iterative concepts, Design Thinking is typically utilized for developing solutions for complex systems within the private sector, but is increasingly used by healthcare systems to address problems or practices that are ill-defined or unknown.31 The Design Thinking framework adopted by RVH encompassed methodological aspects of empathizing, defining, ideating, prototyping, and testing.32 This provided a practical framework for rapid problem solving, often with some failure that was learned from. The Design Thinking approach ultimately led to various mechanisms being tested to permit different departments to safely receive COVID-19 patients, including the use of air balancers, temporary hoarding, HEPA filtration units, leveraging headwall space and medical air availability, installing drivers on fan units, and leveraging vacant shelled space to expand internal capacity. The Design Thinking approach was further used to ideate and develop the 70-bed field hospital (see “Community Response” section below).
Through this planning, RVH provided an ICU Surge Capacity Plan that was capable of expanding its level 3 critical care capacity from 16 beds to 105 beds in 5–12 weeks, along with an additional 334 standard beds and 300 cots, as required (Figure 3).
 |
Figure 3 A robust capacity plan guided by the principles of design thinking permitted RVH to expand its level 3 critical care capacity from 16 beds to 105 beds in 5–12 weeks, along with an additional 334 standard beds and 300 cots (not shown), as required. |
Occupational Health and Workplace Safety
In 2019, RVH separated the services traditionally delivered by a single Occupational Health and Safety department into two distinct departments: Occupational Health and Wellness, and Workplace Safety. This separation resulted in an effective division of various roles and responsibilities addressing workplace safety during the COVID-19 pandemic. Notably, two major issues arose: respirator fit testing and COVID-19-related employee absences.
In January, 2020, anticipating that the novel coronavirus may be airborne, the Workplace Safety department, supported by staff from Occupational Health and Wellness, Emergency Management, and Security departments undertook a major campaign to conduct 700 qualitative respirator fit tests for staff, affiliated professional staff, and partnered community health agencies. Fit-testing clinics were held every day between 08:00 and 23:30 hr for a three-week period. The organization’s IPAC team further contributed by adapting their annual PPE training to a “just-in-time” training delivery model for frontline staff, including a newly established seven-day, 24-hour telephone support line.
In early March, 2020, the Workplace Safety team responded to ongoing concerns related to routes of SARS-CoV-2 exposure and transmission. A key concern was the diminishing supply of N95 respirators across the province, which was subsequently addressed by provincial guidance related to acceptable levels of respiratory protection and increases in organizational supply chains (see “Personal Protective Equipment” section below). The acquisition of several hundred half-face, filtered elastomeric respirators, which can be worn for many hours and then processed for reuse, was an important factor in RVH’s PPE conservation strategy. A dedicated location was established for the donning, doffing, and reprocessing of this new PPE and a decision made by the PPE Conservation Committee to deploy these respirators to clinical staff who were most likely to be involved in aerosol-generating medical procedures (AGMP). In order to facilitate the ongoing need for mask fit-testing and to operationalize the deployment of elastomeric respirators, the Workplace Safety team received assistance from redeployed staff, with dedicated stations established in multiple areas of the hospital. As elastomeric respirators require a 45-minute quantitative assessment of faceseal leakage per person, a partnership was developed with local fire and emergency services, who generously loaned their quantitative fit testing machines and participated in testing.
Distinct from the efforts of the Workplace Safety department, the Occupational Health and Wellness department engaged in early exposure assessments and contact tracing initiatives. In partnership with the local health unit’s Communicable Disease team, these efforts were based on existing protocols for the management of infectious disease outbreaks long established at the hospital. However, an unexpected corollary of the rapidly changing public health measures used to mitigate COVID-19 spread, was the development of a wide range of complex employee absence scenarios that impacted staffing availability and compensation. To provide safe, consistent, and standard guidance to staff and leaders, Occupational Health and Wellness proactively developed an Absence Scenarios document. The document began as a tool for leaders to address travel-related exposures and/or symptomatology in order to foster equitable pay treatment and to establish rigorous and consistent infection prevention and control practices for returning staff to work. Initially addressing six potential COVID-19-related absence scenarios, the document has grown to address up to 19 potential scenarios, including absences related to the unavailability of childcare (Supplementary Table 1).
Human Resources/Workforce Planning
Additional clinical personnel, cleaning staff, environmental services aides, and other staff essential to upholding safety and prevention protocols were required in preparation for and management of an acutely ill, infectious patient population. In addition, student and volunteer placements were indefinitely suspended to protect the broader community, thus requiring additional redeployment to help fulfil traditionally held volunteer roles. As such, a Professional Staff Human Resources COVID-19 Response Plan and Regional Health Human Resources Redeployment Plan were developed to address key issues related to human resources management, including 1) internal departmental plans to address surge, specifically in ICU and Medicine programs; 2) inter-departmental co-operation to support capacity management (eg, utilizing “extender” and “buddy” systems); 3) Emergency department surge; and 4) field hospital staffing.
As most acute care providers sought to expand their skilled workforce during the pandemic, an external labour market analysis was performed and talent acquisition strategy developed to help overcome barriers and shortages. A Workforce Planning Process was developed to provide information on existing workforce skills, desired workforce needs, and strategies and actions to address workforce gaps (Figure 4). Strategies for internal and external recruitment included 1) promoting internal opportunities; 2) establishing new leadership structures; 3) creating an internal “Reserve Unit”; 4) exploring opportunities to utilize non-practicing retired, graduate, or student healthcare professionals; 5) creating evergreen postings for clinical, allied health, environmental, and clerical roles; 6) conducting virtual job fairs; 7) establishing recruiting campaigns outside the region; and 8) creating a formal tactical acquisition plan.
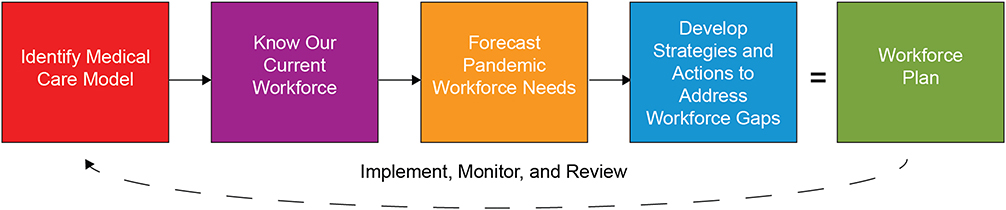 |
Figure 4 A structured, five-step workforce planning cycle was established to identify and fulfil clinical staffing requirements, as well as cleaning staff, environmental services aides, and other staff essential to meeting workforce demands and upholding patient safety. This framework was further supported by strategies and actions to source, recruit, onboard, train, and develop staff. |
Supporting staff employed at multiple sites or organizations presented additional human resources challenges, due to the prospect of suspected or declared COVID-19 outbreaks at other locations. Adopting the recommendations of Ontario Health, the government agency that oversees the administrative activities of the provincial health system, RVH chose not to restrict part-time staff from working at multiple organizations, but rather limit staff to a single location when working on a suspected or declared COVID-19 outbreak unit, a COVID-19 area within an organization, or an intensive care unit caring for probable or confirmed COVID cases until the outbreak had cleared. With professional staff increasingly redeployed to assist with COVID-19 efforts within the broader community (see “Community Response” section below), the Human Resources department developed a Mobility Between Work Locations/Sites Scenarios tool to assist leaders in balancing clinical resources to local conditions (Supplementary Table 2).
Personal Protective Equipment
Prior to COVID-19, RVH maintained a 3–4-week stockpile of essential PPE for emergency use, including gloves, masks, and gowns. Due to onsite space limitations, RVH typically stored stockpiles at an offsite location, in partnership with a third party who managed product expiration and refreshed supplies accordingly.
In January, 2020, in response to reports of an emerging novel coronavirus, RVH’s Procurement and Logistics team began increasing regular orders of essential PPE and cleaning supplies (eg, hard-surface disinfectants, hand sanitizer). During this time, the maximum permitted allotment from manufacturers and distributors to the organization was ordered, with the goal of increasing RVH’s onsite stockpile and with the intention of reintegrating excess PPE back into regular circulation if not required for pandemic use. As few hospitals are able to maintain a large onsite warehouse of supplies, identifying additional storage space was a challenge, so non-traditional spaces were secured and dedicated to storing PPE, such as converted administrative areas and vacant shelled space.
In March, 2020, a PPE subcommittee was formed to make decisions on PPE usage and preservation in response to constraints in global supply. A key aspect of the PPE subcommittee was that it was comprised of medical, financial, and legal professionals with delegated authority to make rapid decisions on behalf of the organization. With a greater emphasis on PPE conservation, the committee began tracking and forecasting daily PPE inventory. One early limitation of the tracking system was the relative lack of historical and published data on efficient PPE utilization and distribution during supply chain shortages. To combat shortages, non-traditional suppliers that met the required safety standards were engaged. The PPE subcommittee established a process of verification and evaluation to ensure that these supplies met all regulatory standards, including an American Society of Testing and Materials (ASTM) rating for all masks, Association for the Advancement of Medical Instrumentation (AAMI) rating for gowns, and ASTM or Acceptable Quality Level (AQL) requirements for gloves. An independent third party was contracted to test all PPE purchased from non-traditional sources. Finally, RVH supported local manufacturers and automation companies who retooled their operations to produce medical supplies, including providing assistance with navigating regulatory and licensing requirements.
Community Response
RVH provided critical support for three COVID-19 community initiatives: 1) establishing a local community assessment centre; 2) redeploying staff to long-term care and retirement homes experiencing COVID-19 outbreaks; and 3) creating a 70-bed field hospital, known locally as the Pandemic Response Unit (PRU).
In March, 2020, healthcare providers across Ontario were tasked with establishing local COVID-19 assessment centres dedicated to screening, clinical assessment, and testing. The objective of these centres was to divert patients with mild COVID-19 symptoms from emergency departments. Although the core function of each assessment centre was shared across Ontario, operationalization was left to the local providers, including infrastructure, workforce and staffing, hours of operation, and service modality (eg, in-home, virtual, in-centre, drive-through). This rapid response would have been a formidable task for local providers had it not been for the revitalization of the Barrie and Area Surge Planning Committee in 2019, which focused on preparedness activities in anticipation of an annual influenza-related surge across the full spectrum of regional healthcare services. Adopting a modified regional plan for an alternate treatment and assessment centre that had been implemented in 2009 during the H1N1 influenza pandemic, the committee was able to rapidly pivot from its focus on influenza to COVID-19. The plan was further edified by the commitment of local partners, including family health teams and paramedic services, to provide a clinically sound location and clinical staff for the centre. RVH provided nurse practitioners and nursing support staff, PPE for all clinic staff, coordinated laundry services, and served as the paymaster for environmental services. While the assessment centre was highly effective, conducting an average of 80 assessments per day during the first three months of operation, one drawback was that it was designed for relatively short-term surge resulting from seasonal influenza. Work demands on clinical staff were high, and it was determined that long-term operations would benefit from a location that did not negatively impact the operations of other clinics, with funding for dedicated clinical and administrative staff. By June, 2020, it was apparent that the assessment centre no longer required the support of RVH, becoming a stand-alone, community-run clinic.
LTC and retirement homes became the epicentre of Canada’s first COVID-19 wave. With a 34% resident case fatality rate that accounted for more than 80% of all reported COVID-19 deaths in Canada during this time,33 residents experienced sustained and devastating outcomes that have been linked not only to the medical complexities and multi-morbidities of residents but to long-standing systemic issues, such as underfunding and business models.33–36 Moreover, infections among staff at residential care facilities represented more than 10% of the country’s total cases. On April 24, 2020, the Ontario Minister of Long-Term Care responded to the challenges faced by residential care facilities by issuing a Minister’s Directive requiring all long-term care homes in outbreak to provide entry to hospital staff to provide assistance with resident care, including IPAC assessments, clinical supervision, and nursing and personal support services. In response to the emergency order, RVH developed a Long-Term Care Management Plan in conjunction with the County of Simcoe, an “upper tier” municipal government composed of mayors and deputy mayors from towns and townships located within the region. A 90-day action plan was established that focused on three goals: 1) control the outbreak; 2) stabilize operations; and 3) transition operations. To meet these goals, twelve priority areas were identified through audits and risk assessments: 1) resident care; 2) environmental services; 3) general supplies and equipment; 4) IPAC; 5) PPE conservation and deployment; 6) quality, risk, and privacy; 7) financial management; 8) occupational health and workplace safety; 9) staff stabilization; 10) communication with licensee; 11) family engagement; and 12) joint corporate communications. Actions were performed by hospital staff to address gaps for each priority area to ensure residential care and infection prevention met or exceeded legislative standards of operation and best practices. For example, RVH’s Environmental Services department performed decluttering and terminal cleaning of the facility, including removing unnecessary furniture and equipment, as well as auditing existing environmental services practices and products, and implementing new policies and procedures that aligned with recommendations made by the Provincial Infectious Diseases Advisory Committee. RVH’s clinical experts, IPAC, Corporate Communications, Occupational Health, and Workplace Safety departments further developed and delivered education and training plans that helped establish more consistent infection prevention practices (eg, creating a PPE donning and doffing station) and resource management issues (eg, creating and tracking PPE inventory; ensuring daily staffing needs were met). RVH was also able to assist 30 LTC and retirement homes improve their IPAC processes to help overcome and prevent outbreaks.
The PRU was constructed in response to local surge forecasting and in alignment with similar structures constructed by two peer hospitals and with Ontario’s Emergency Order for Alternative Healthcare Facilities. The PRU is an 8250 square-foot, four-season, fully-functioning 70-bed field hospital located in RVH’s parking lot and connected to the health centre by an enclosed walkway (Figure 5). Mock codes with debriefings were frequently conducted to prepare for internal and external emergencies; this provided an appropriate level of response readiness, which was unexpectedly tested when an EF-2 tornado with 210 km/h winds touched down in south Barrie on July 15, 2021. The PRU opened in November, 2020, and was used for the transition of non-COVID-19 inpatients out of hospital, allowing RVH to continue providing core services and acting as a regional asset for other hospitals facing capacity challenges. Among the challenges of operating the PRU, the identification of an appropriate patient population was critical. Because of its structure (eg, stand-alone facility, exposed ductwork) and limited staffing, only independently mobile patients awaiting discharge were permitted. Additional patient inclusion criteria were required, as the PRU lacked geriatric and visitor chairs, overhead lifts, handrails and therapy poles, doors and ceilings on patient bays, and was limited in telemetry, space for assistive devices, and the ability to physically/visually redirect patients (Supplementary Table 3). As of June 30, 2021, the PRU has acted as an invaluable regional asset having treated over 795 patients, thereby enabling RVH to accept more patient transfers from local and distant partner hospitals than any other hospital in the province.
 |
Figure 5 The pandemic response unit (PRU) is a 70-bed, 8250 square-foot, four season, fully-functioning modular field hospital located in RVH’s parking lot and connected to the health centre by an enclosed walkway. The PRU is professionally staffed and fully equipped regional asset to assist RVH and partner hospitals facing capacity challenges during the COVID-19 pandemic. Of note, the PRU is not a unit for COVID patients, but for medically stable inpatients with an estimated stay of 3–5 days. |
Corporate Communication
The RVH Corporate Communications department had previously established a well-developed, robust crisis communication strategy. The greatest communication challenge, especially in the early days of the pandemic, was the volume of rapidly evolving information. Provincial directives were changing daily and Corporate Communications needed to utilize a diverse array of new and existing communication methods, such as virtual Town Halls, media releases, key messages for leaders, a strong social media plan and daily COVID-19 updates, as well as developing information products in preparation for surge conditions, such as a COVID-19-dedicated internal website and significant onsite signage.
Throughout the first wave, the primary source of information for staff and physicians was a daily COVID-19 update distributed by the CEO and Chief of Staff and featuring organizational, municipal, provincial, and federal public health updates, as well as information on the hospital’s COVID-19 status, news and events, and links to external COVID-19 resources. The daily update also included a mechanism for staff to ask COVID-related questions, which were subsequently answered by local experts. An initial concern that the volume of COVID-19 communication would result in audience fatigue were dispelled as staff, physicians, and volunteers relayed their appreciation for the depth and frequency of this accurate, comprehensive “one source of truth” during very uncertain and anxious times. Frequent meetings with regional and provincial communication leads provided an opportunity to share learnings and best practices. In fact, RVH shared its communication products with all hospitals in the region, recognizing that RVH does have significant in-house design capabilities while others are resource-limited. RVH also established frequent briefings, along with written updates, for elected representatives throughout the region.
With declining physical and mental health wellness a major concern among healthcare workers during the pandemic,37 Corporate Communications developed a resiliency strategy, which included a series of “Caring for You” videos that addressed common concerns and provided practical advice and coping skills. Key messages and Frequently Asked Questions were also regularly provided to department leaders, with the expectation that they huddle with their teams within 72 hours, ensuring staff have an opportunity to interact with their direct supervisor. In addition, a dedicated hashtag on social media, “#ShowRVHLove” was developed as a way for the community to express their gratitude for those working at the health centre. Through this hashtag, words of encouragement and appreciation, signs and artwork from the community were received and posted to the internal website.
Conclusion
Infectious disease outbreaks require hospitals to coordinate a multidisciplinary, multidepartmental response to mitigate nosocomial infections.19,21,38 While most implemented system-level changes irrespective of local case counts as an early response to COVID-19, substantial regional variability in the type and timing of these operational changes have been reported.39 While this variability may serve a pragmatic need as local situational issues arise, a better understanding of key operational priorities may better inform local and standardized preparedness strategies. To this end, the current study used a qualitative descriptive approach to identify key operational themes used by a large community hospital to prepare and respond to COVID-19. Our results are presented as a narrative exploring the details of the operational strategies and tools employed used for each theme by a multidisciplinary group of healthcare leaders.
In contrast to the clinical management of care pathways impacted by infectious disease outbreaks,8–18 non-clinical, operational strategies are seldom published. In 2019, a systematic review identified only 20 studies that focused on quantitative or qualitative dissemination of knowledge and tools related to hospital preparedness for biological disasters, including pandemics.40 The study identified eight categories of hospital preparedness for biological events, including planning, surge capacity, communications, training and education, medical management, surveillance, standard operation process, and safety and security. Similarly, barriers to successfully operationalizing and supporting clinical services during the COVID-19 pandemic are slowly emerging through shared experiences, reviews, commentaries, and research.41–46 In one report, Adelaja et al developed a comprehensive COVID-19 preparedness tool called CHAPs, to rapidly identify potential bottlenecks in hospital crisis management, focusing on six key operational themes commonly associated with resource strain, including workforce, infrastructure, supplies and equipment, service reconfiguration, data and information technology, and communications.23 Some of the themes identified in the current study are consistent with those aforementioned, particularly with respect to organizational structure, capacity planning, human resources, personal protective equipment, and communication, although it is challenging to compare specific details as other studies often lack detailed, site-specific strategies. For example, our experience with a modified IMS-based EOC structure permitted interoperability between clinical and administrative teams, as well as timely and accurate communication with all stakeholders, and are consistent with IMS frameworks developed by Daugherty after the 2009 H1N1 influenza outbreak19 and Zorn during the first six months of COVID-19.42 In addition, utilizing local expertise to inform on infectious disease management and epidemiology helped forecast surge capacity priorities, along with an associated increase in technical and staffing requirements, particularly for the ICU and PRU. Finally, design thinking permitted a multidisciplinary, adaptive approach to space planning in order to counter pandemic vulnerabilities attributed to hospital spatial layouts.43
To our knowledge, occupational health and wellness, workplace safety, and community response were unique themes, having critical roles in reviewing and revising COVID-19-related policies and procedures, conducting mock simulations, identifying staffing mobility issues, providing training and education, and developing local partnerships. Indeed, the novel tools described in this study were primarily developed to augment occupational health and local community issues identified by EOC, including the Absence Scenarios document, Mobility Between Work Locations/Sites Scenarios document, and Pandemic Response Unit eligibility criteria. Interestingly, despite being identified as an important operational factor during the SARS20,47 and H1N148 outbreaks, mental health support of healthcare workers is rarely identified as a significant COVID-19 preparedness strategy. This is likely because preparedness strategies focus on early responses to COVID-19, rather than protracted outcomes. As the psychological and psychosocial well-being of healthcare workers has been severely impacted by COVID-19,37 we recommend hospitals aggressively address mental health support as an operational preparedness strategy for future outbreaks.
Pandemic responsiveness is predicated on system-level and local-level responses being aligned and adaptive. In Ontario, most hospitals are private, non-profit organizations that are required to establish their own internal governance structure. After the 2003 SARS outbreak that devastated Toronto’s acute healthcare system, the Government of Ontario appointed an independent commission to investigate the introduction and spread of SARS.49 The SARS commission highlighted system failures in public health, infection prevention and control, workplace safety, laboratory testing, critical care, and information dissemination. The commission’s recommendations included the creation of centralized agencies, which proved indispensable during COVID-19, including Public Health Ontario, responsible for evidence synthesis, laboratory testing, and guideline synthesis and dissemination; Critical Care Services Ontario, responsible for monitoring and coordinating provincial critical care bed utilization; and Ontario Health, responsible for the coordination and management of acute healthcare services across the province. However, even with their expertise and resources, these agencies required the participation and partnership of hospital administrators to coordinate the local management of patients and healthcare workers. As COVID-19 spread unevenly and repeatedly across communities and regions, each hospital had to plan, coordinate, and implement unique solutions to their own prevailing issues. While working collaboratively with other hospitals located in their geographic and referral regions, the COVID-19 pandemic necessitated the mobilization of patients, healthcare providers, and resources both within and between healthcare organizations. Community hospitals played an especially important role in this process, as they normally provide care to over 65% of the province’s medical and surgical patients,26 despite having less financial and human resources than their academic counterparts. The current study demonstrates the importance of utilizing local resources and partnerships to overcome limited resources, particularly of leveraging local and external expertise to inform and act on infectious disease management, epidemiology, infrastructure, PPE availability, and community issues. Indeed, as much as academic hospital centres provided COVID-19 medical expertise to provincial agencies, community hospitals and their partners were able to provide much needed physical capacity to accommodate the interprovincial transfer of COVID-19 patients to offload overwhelmed academic hospitals. Given the capacity and competency of community hospitals and their partners to locally manage the COVID-19 pandemic, the province’s critical care and healthcare system avoided becoming overwhelmed.
While the themes and narrative presented in this study may assist peer hospitals in their own pandemic strategies, limitations to this study exist. As a qualitative descriptive study, the results are representative of a single hospital’s experience with COVID-19. Understanding causal relationships between an organization’s pandemic response to any perceived or real benefits is limited without an appropriate outcome assessment and, in this study, any successful outcomes we describe are experiential. As the study employed an open-ended questionnaire, self-selection bias among participants may exist, although this was mitigated by directed questions about specific themes. Regardless of these limitations, we share RVH’s pandemic preparedness strategies and tools, such that peer organizations may benefit from this knowledge.
Data Sharing Statement
The authors confirm that the data supporting the findings of this study are available within the figures and tables of this article and its (supplementary materials).
Ethics Approval and Informed Consent
The Chair of the RVH Research Ethics Board ruled that the current study did not require ethics review as the study does not involve research on humans (individuals, samples, or data) or animals.
Consent for Publication
The authors confirm that the contents of the manuscript can be published.
Acknowledgments
The authors thank Jane Lamoth, Jamie Boreland, Pamela Oertel, and Rosalyn Rowe (RVH) for helpful discussions.
Author Contributions
All authors made significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was supported by the RVH Foundation.
Disclosure
The authors declare no conflicts of interest in relation to this work.
References
1. Wiersinga WJ, Rhodes A, Cheng AC, Peacock SJ, Prescott HC. Pathophysiology, transmission, diagnosis, and treatment of Coronavirus Disease 2019 (COVID-19): a review. JAMA. 2020;324(8):782–793. doi:10.1001/jama.2020.12839
2. Salzberger B, Buder F, Lampl B, et al. Epidemiology of SARS-CoV-2. Infection. 2021;49(2):233–239. doi:10.1007/s15010-020-01531-3
3. Uddin M, Mustafa F, Rizvi TA, et al. SARS-CoV-2/COVID-19: viral genomics, epidemiology, vaccines, and therapeutic interventions. Viruses. 2020;12(5):526. doi:10.3390/v12050526
4. Nalbandian A, Sehgal K, Gupta A, et al. Post-acute COVID-19 syndrome. Nat Med. 2021;27(4):601–615. doi:10.1038/s41591-021-01283-z
5. Pavli A, Theodoridou M, Maltezou HC. Post-COVID syndrome: incidence, clinical spectrum, and challenges for primary healthcare professionals. Arch Med Res. 2021;52(6):575–581. doi:10.1016/j.arcmed.2021.03.010
6. Emanuel EJ, Persad G, Upshur R, et al. Fair allocation of scarce medical resources in the time of Covid-19. N Engl J Med. 2020;382(21):2049–2055. doi:10.1056/NEJMsb2005114
7. Legido-Quigley H, Asgari N, Teo YY, et al. Are high-performing health systems resilient against the COVID-19 epidemic? Lancet. 2020;395(10227):848–850. doi:10.1016/S0140-6736(20)30551-1
8. Brethauer SA, Poulose BK, Needleman BJ, et al. Redesigning a department of surgery during the COVID-19 pandemic. J Gastrointest Surg. 2020;24(8):1852–1859. doi:10.1007/s11605-020-04608-4
9. Coccolini F, Perrone G, Chiarugi M, et al. Surgery in COVID-19 patients: operational directives. World J Emerg Surg. 2020;15(1):25. doi:10.1186/s13017-020-00307-2
10. Freer PE. The Impact of the COVID-19 pandemic on breast imaging. Radiol Clin North Am. 2021;59(1):1–11. doi:10.1016/j.rcl.2020.09.008
11. Griffin KM, Karas MG, Ivascu NS, Lief L. Hospital preparedness for COVID-19: a practical guide from a critical care perspective. Am J Respir Crit Care Med. 2020;201(11):1337–1344. doi:10.1164/rccm.202004-1037CP
12. Ierardi AM, Wood BJ, Gaudino C, et al. How to handle a COVID-19 patient in the angiographic suite. Cardiovasc Intervent Radiol. 2020;43(6):820–826. doi:10.1007/s00270-020-02476-8
13. Lim WH, Wong WM. COVID-19: notes from the front line, Singapore’s primary health care perspective. Ann Fam Med. 2020;18(3):259–261. doi:10.1370/afm.2539
14. Merchan C, Soliman J, Ahuja T, et al. COVID-19 pandemic preparedness: a practical guide from an operational pharmacy perspective. Am J Health Syst Pharm. 2020;77(19):1598–1605. doi:10.1093/ajhp/zxaa212
15. Naljayan M, Yazdi F, Struthers S, Sharshir M, Williamson A, Simon EE. COVID-19 in New Orleans: a nephrology clinical and education perspective and lessons learned. Kidney Med. 2020;3(1):99–104. doi:10.1016/j.xkme.2020.09.012
16. Phua J, Weng L, Ling L, et al. Intensive care management of coronavirus disease 2019 (COVID-19): challenges and recommendations. Lancet Respir Med. 2020;8(5):506–517. doi:10.1016/S2213-2600(20)30161-2
17. Rao G, Singh A, Gandhotra P, et al. Paradigm shifts in cardiac care: lessons learned from COVID-19 at a large New York health system. Curr Probl Cardiol. 2021;46(3):100675. doi:10.1016/j.cpcardiol.2020.100675
18. Yackzan S, Shah M. Ambulatory oncology: infrastructure development in response to the COVID-19 pandemic. Clin J Oncol Nurs. 2021;25(1):41–47. doi:10.1188/21.CJON.41-47
19. Daugherty EL, Carlson AL, Perl TM. Planning for the inevitable: preparing for epidemic and pandemic respiratory illness in the shadow of H1N1 influenza. Clin Infect Dis. 2010;50(8):1145–1154. doi:10.1086/651272
20. Loutfy MR, Wallington T, Rutledge T, et al. Hospital preparedness and SARS. Emerg Infect Dis. 2004;10(5):771–776. doi:10.3201/eid1005.030717
21. Rebmann T. Assessing hospital emergency management plans: a guide for infection preventionists. Am J Infect Control. 2009;37(9):708–14.e4. doi:10.1016/j.ajic.2009.04.286
22. Zoutman DE, Ford BD, Melinyshyn M, Schwartz B. The pandemic influenza planning process in Ontario acute care hospitals. Am J Infect Control. 2010;38(1):3–8. doi:10.1016/j.ajic.2009.10.002
23. Adelaja I, Sayma M, Walton H, et al. A comprehensive hospital agile preparedness (CHAPs) tool for pandemic preparedness, based on the COVID-19 experience. Future Healthc J. 2020;7(2):165–168. doi:10.7861/fhj.2020-0030
24. Burgansky A, Coletta-Lucas J, Garcia MS. COVID-19 in a community hospital. Semin Perinatol. 2020;44(6):151292. doi:10.1016/j.semperi.2020.151292
25. Popescu S. Roadblocks to infection prevention efforts in health care: SARS-CoV-2/COVID-19 response. Disaster Med Public Health Prep. 2020;14(4):538–540. doi:10.1017/dmp.2020.55
26. DiDiodato G, DiDiodato JA, McKee AS. The research activities of Ontario’s large community acute care hospitals: a scoping review. BMC Health Serv Res. 2017;17(1):566. doi:10.1186/s12913-017-2517-4
27. Sandelowski M. Whatever happened to qualitative description? Res Nurs Health. 2000;23(4):334–340. doi:10.1002/1098-240x(200008)23:4<334::aid-nur9>3.0.co;2-g
28. Thomas DR. A general inductive approach for analyzing qualitative evaluation data. Am J Eval. 2006;27(2):237–246. doi:10.1177/1098214005283748
29. Province of Ontario. The Incident Management System (IMS) for Ontario; 2009. Available from: https://www2.emergencymanagementontario.ca/sites/default/files/content/emo/docs/IMS%20Doctrine%20for%20Ontario_EN_PDFUA.pdf.
30. Brown T. Design thinking. Harv Bus Rev. 2008;86(6):84–92.
31. Roberts JP, Fisher TR, Trowbridge MJ, Bent C. A design thinking framework for healthcare management and innovation. Healthc. 2016;4(1):11–14. doi:10.1016/j.hjdsi.2015.12.002
32. Seidel VP, Fixson SK. Adopting design thinking in novice multidisciplinary teams: the application and limits of design methods and reflexive practices. J Prod Innov Manag. 2013;30:19–33. doi:10.1111/jpim.12061
33. Canadian Institute for Health Information. The impact of COVID-19 on long-term care in Canada: focus on the first 6 months; 2021. Available from: https://www2.emergencymanagementontario.ca/sites/default/files/content/emo/docs/IMS%20Doctrine%20for%20Ontario_EN_PDFUA.pdf.
34. Clarke J. Impacts of the COVID-19 pandemic in nursing and residential care facilities in Canada; 2021. Available from: https://www150.statcan.gc.ca/n1/pub/45-28-0001/2021001/article/00025-eng.htm.
35. Liu M, Maxwell CJ, Armstrong P, et al. COVID-19 in long-term care homes in Ontario and British Columbia. CMAJ. 2020;192(47):E1540–E1546. doi:10.1503/cmaj.201860
36. Stall NM, Jones A, Brown KA, Rochon PA, Costa AP. For-profit long-term care homes and the risk of COVID-19 outbreaks and resident deaths. CMAJ. 2020;192(33):E946–E955. doi:10.1503/cmaj.201197
37. Shaukat N, Ali DM, Razzak J. Physical and mental health impacts of COVID-19 on healthcare workers: a scoping review. Int J Emerg Med. 2020;13(1):40. doi:10.1186/s12245-020-00299-5
38. Peiffer-Smadja N, Lucet JC, Bendjelloul G, et al. Challenges and issues about organizing a hospital to respond to the COVID-19 outbreak: experience from a French reference centre. Clin Microbiol Infect. 2020;26(6):669–672. doi:10.1016/j.cmi.2020.04.002
39. Mathews KS, Seitz KP, Vranas KC, et al. Variation in Initial U.S. hospital responses to the Coronavirus disease 2019 pandemic. Crit Care Med. 2021;49(7):1038–1048. doi:10.1097/CCM.0000000000005013
40. Aminizadeh M, Farrokhi M, Ebadi A, Masoumi GR, Kolivand P, Khankeh HR. Hospital management preparedness tools in biological events: a scoping review. J Educ Health Promot. 2019;8:234. doi:10.4103/jehp.jehp_473_19
41. Wurmb T, Scholtes K, Kolibay F, et al. Hospital preparedness for mass critical care during SARS-CoV-2 pandemic. Crit Care. 2020;24(1):386. doi:10.1186/s13054-020-03104-0
42. Zorn CK, Pascual JM, Bosch W, et al. Addressing the challenge of COVID-19: one health care site’s leadership response to the pandemic. Mayo Clin Proc Innov Qual Outcomes. 2021;5(1):151–160. doi:10.1016/j.mayocpiqo.2020.11.001
43. Łukasik M, Porębska A. Responsiveness and adaptability of healthcare facilities in emergency scenarios: COVID-19 experience. Int J Environ Res Public Health. 2022;19(2):675. doi:10.3390/ijerph19020675
44. Brown J, Guru S, Williams K, Florentino R, Miner J, Cagir B. Rural healthcare center preparation and readiness response to threat of COVID-19. J Am Coll Surg. 2020;230(6):1105–1110. doi:10.1016/j.jamcollsurg.2020.04.006
45. Asmaningrum N, Ferguson C, Ridla AZ, Kurniawati D. Indonesian hospital’s preparedness for handling COVID-19 in the early onset of an outbreak: a qualitative study of nurse managers. Australas Emerg Care. 2022. doi:10.1016/j.auec.2022.02.002
46. Shen Y, Cui Y, Li N, et al. Emergency responses to Covid-19 outbreak: experiences and lessons from a general hospital in Nanjing, China. Cardiovasc Intervent Radiol. 2020;43(6):810–819. doi:10.1007/s00270-020-02474-w
47. Hawryluck L, Lapinsky SE, Stewart TE. Clinical review: SARS - lessons in disaster management. Crit Care. 2005;9(4):384–389. doi:10.1186/cc3041
48. Aiello A, Khayeri MYE, Raja S, et al. Resilience training for hospital workers in anticipation of an influenza pandemic. J Contin Educ Health Prof. 2011;31(1):15–20. doi:10.1002/chp.20096
49. Campbell AG. Spring of fear: the SARS commission final report; 2006.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.