")
Back to Journals » Patient Related Outcome Measures » Volume 15
Patient Satisfaction with Antiretroviral Therapy Services in Hadiya Zone, Central Ethiopia Using the Donebidean Model: A Time-Motion Study
Authors Halili A, Lubago BE , Agide FD
Received 18 December 2023
Accepted for publication 1 March 2024
Published 5 March 2024 Volume 2024:15 Pages 93—103
DOI https://doi.org/10.2147/PROM.S452389
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Robert Howland
Abayneh Halili, Belay Echafo Lubago, Feleke Doyore Agide
School of Public Health, College of Medicine and Health Sciences, Wachemo University, Hossana, Ethiopia
Correspondence: Feleke Doyore Agide, School of Public Health, College of Medicine and Health Sciences, Wachemo University, P.O. Box: 667, Hossana, Ethiopia, Tel +251916291489, Email [email protected]
Background: A time-motion study is a scientific method for recording time spent on various tasks in a narrow range of specialized work settings, beginning with initial enrollment in ART provision. Therefore, the study aimed to assess the time motion of patient satisfaction with antiretroviral therapy services in Central Ethiopia.
Methods: A facility-based cross-sectional study was conducted on a sample of 422 patients from June 14 to July 30, 2021. We used a simple random sampling technique to select the participants. Structural input-related qualitative data were collected using an in-depth interview and used for concurrent triangulation with quantitative. Quantitative data were collected using a standardized and pre-tested questionnaire and analyzed using SPSS version 24.0. Bivariate and multivariable logistic regressions were used to identify independent predictors of time motion and patient satisfaction. The degree of association between the outcome and independent variables was assessed by using an odds ratio with a 95% CI.
Results: The time motion of patient satisfaction study found that 53.1% (224/422) of the study participants were satisfied. As independent predictors, time spent (time motion) waiting to be seen by a health professional (AOR = 0.228, 95% CI = 0.079– 0.661), patient-provider interaction (AOR = 3.72, 95% CI = 2.111– 5.771), perceived privacy (AOR = 2.912, 95% CI = 1.76– 2.78), sex (AOR = 2.499, 95% CI = 1.556– 4.009), and income class (AOR = 0.228, 95% CI = 0.073– 0.707) were associated with outcome variable.
Conclusion: The study found low patient satisfaction with ART services, indicating the need for further improvement to enhance patient-centered services with the given time motion. Therefore, further research is needed to assess the intensity and reach of the information through an analysis of pre- and post-intervention that provides a complete picture of conceptualizations of time motion studies.
Keywords: ART, patient satisfaction, time motion, Central Ethiopia
Introduction
Advocating for the human immunodeficiency virus (HIV) is still a critical issue for the world, as HIV/AIDS has infected a total of 77.3 million people worldwide.1–4 According to the 2016 Ethiopian Demographic and Health Survey (EDHS) main findings on AIDS in Ethiopia, the national HIV prevalence rate among adults is expected to be 0.9%, with 2.9% in urban areas and 0.4% in rural areas.4,5 As a result, antiretroviral therapy (ART) has become an important aspect of HIV treatment4,6–8 and also significantly lowered the rate of HIV transmission from mother to child.9–12 According to a study conducted in one region of Ethiopia, low education and migratory status are factors in HIV infection.4 Furthermore, coverage of HIV services varies by demographic and region.5 HIV epidemics in specific areas may originate or re-emerge if these sub-regions and subpopulations are not addressed. Over the past ten years, Ethiopia has made impressive strides toward managing the HIV/AIDS epidemic. Nonetheless, compared to less than one percent nationwide, prevalence is still comparatively high in metropolitan regions, where estimates place the rate at three percent.4,5
Timely treatment of patients has made a significant difference in adherence to the developed and developing world.13–15 The world believes that increasing waiting time in outpatient departments (OPDs) has a negative impact on patient satisfaction; therefore, prompt patient care and adopting a compassionate and considerate approach to improving patient satisfaction will have a positive impact on service delivery. To this end, patient waiting times are increasingly important to a clinic’s ability to attract new clients in the competitive managed care environment. When patients are unhappy with the length of the waiting time, it is difficult to offer services.16–19 To solve this problem, many efforts have been made by the government of Ethiopia.3,4,20 The current state of the quality of ART services in health facilities is still seen to have different types of quality-related issues. Patient satisfaction to the level of best, which has gaps, is not definitely assessed.
Tested theories are prudent in describing the behavioural situations of individuals and groups, as well as organizations in one squad.21,22 Thus; this study uses the Donebidean model to assess the time motion of patient satisfaction with ART service utilization. The Donebidean model is a conceptual framework for investigating health services and assessing healthcare quality. The approach divides quality of care information into three categories: “structure”, “process”, and “outcomes”. The model represents the concept of input, process, and output elements that influence patient satisfaction. In the paradigm, input components are the health institution’s structural and physical setting, while process factors include patient-doctor contact and therapy. Whereas, output factors are the result of the input and process factors. The true application of the model links the input, process, and output in a connected manner.23–27 In other words, since patient satisfaction is the best predictor of the health service process of the patient, the input and process factors are still the question in Ethiopia since the knowledge we have at hand is inconclusive and abstract. That is why the Donebidean model was applied to look into the factors affecting patient satisfaction with ART services. Therefore, the study aimed to assess the time motion of patient satisfaction with antiretroviral therapy services in Hadiya Zone, Central Ethiopia, using the Donebidean Model (Figure 1).
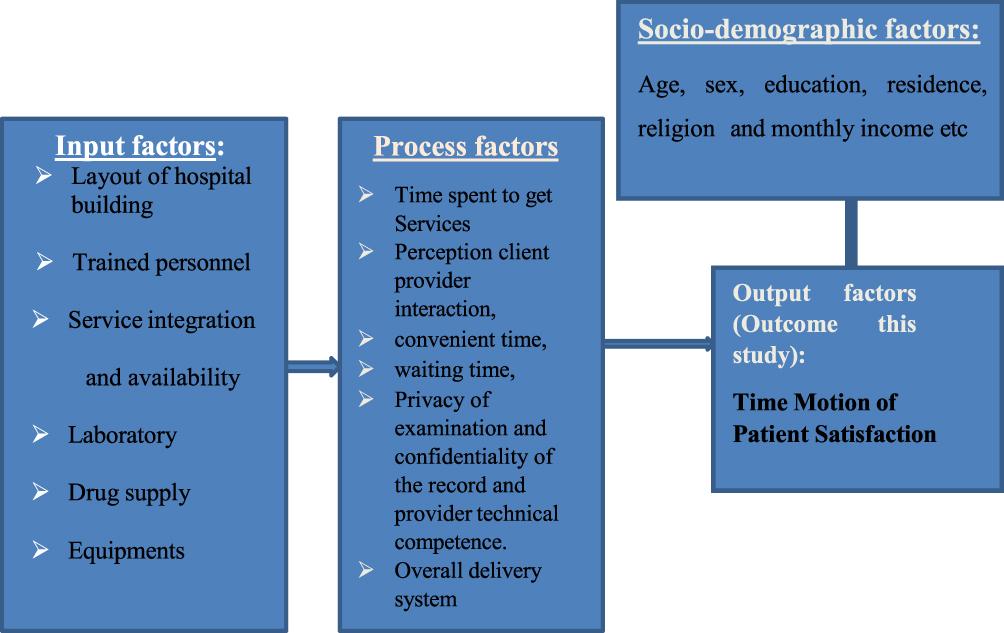 |
Figure 1 Conceptual framework of time-motion of patient satisfaction with antiretroviral therapy services in Hadiya Zone, Central Ethiopia using Donebidean model. |
Materials and Methods
Study Design, Participants and Study Setting
A facility-based cross-sectional study was conducted on a sample of 422 patients from June 14, to July 30, 2021. Source populations were all adult (age 18 years and above) people living with HIV/AIDS (PLWHA) who are receiving antiretroviral therapy services from governmental hospitals in the Hadiya zone. Sample populations were adult patients on ART whose ages were 18 and above. All adult patients who had been on ART for less than three months, were 18 years of age or older, had hearing difficulties, or had mental problems were excluded from the study. The study was conducted in the central part of Ethiopia, in Hadiya zone health facilities.
The Hadiya zone is one of the zones in Central Ethiopia. Its capital city is Hossana, and it is located at a distance of 230km from Addis Ababa. The zone has thirteen rural towns and eight administrative towns. There are three primary hospitals and one comprehensive specialized hospital. Those are Wachemo University Nigist Elleni Mohammed Memorial Comprehensive Hospital, Homecho, Shone, and Ginbichu primary hospitals. Then, all of them provide ART services to people living with HIV/AIDS (PLWHA). The number of ART service users at Wachemo University Nigist Elleni Mohammed Memorial Comprehensive hospital, Homecho, Shone and Ginbichu Hospitals is 1250, 36, 150 and 69 patients respectively.15 In the Zone, currently, the number of people living with HIV/AIDS (PLWHA) is 2350, many of whom were on ART. The chronology of ART client’s movement from entering to facility and exiting the facility varies from hospital to hospital depending on type and level of hospital. However, all hospitals use separate outpatient department and treatment set-up to increase patient privacy and confidentiality, and to reduce stigma and discrimination.
Sample Size Determination and Sampling Procedure
The sample size was calculated by using a single population proportion and considering the following assumptions: P = 50% (assuming a proportion of patients who are treated ART timely), marginal error (d) of 5%, confidence interval of 95%, and Z α/2 is the value of the standard normal distribution corresponding to a significant level of alpha (α) 0.05, which is 1.96. Finally, to account for contingencies such as non-response or recording error, the sample size was increased by 10%, resulting in 384 x 10/100 + 384 = 422. For sampling, the enumerated lists of Art patients’ were obtained from the record office all the four hospitals. Then, all four hospitals were included in the study, and from each hospital, sample households were chosen using a simple random sampling technique using a sampling frame. For qualitative, criterion related sampling technique was used to conduct six in-depth interviews with health workers and five with clients to collect information about the structural variables and some of the process data.
Measurement of Variables
The outcome of this study is the time motion of patient satisfaction with ART services. Patient satisfaction is the patients’ care received from ART service delivery points and staff, which is computed by adding the satisfaction parameters captured through the five-point Likert scale. Respondents who fall within the mean score and above are considered satisfied. The existing situation of the health facility concerning input factors such as the minimum clinical package, the minimum pharmacy package, and the laboratory minimum package were assessed on 16 items. The exposure variables were socio-demographic factors such as age, religion, ethnicity, educational status, occupational status, and income, which were assessed with 10 items. Patient satisfaction with ART treatment services was assessed with 18 items. This questionnaire is graded by taking a percentage of the total score and categorizing it as either good or poor satisfaction. Participants in the study who scored mean were thought to have good satisfaction. Those who scored below the mean were considered to have poor satisfaction. To assess the level of satisfaction and perception of clients with each selected item, we used five Likert scales (strongly disagree, disagree, neutral, agree, and strongly agree). Finally, respondents who exclusively reported one of the three categories, namely neutral, disagree, or strongly disagree together, were considered to have not been satisfied, whereas respondents, who exclusively reported one of the two categories, namely agree or strongly agree together, were considered to have been satisfied. To gain information about structural input variables, the qualitative data collecting method was used, which involved an in-depth interview. The guideline inquires about the hospital’s pleasant layout, the availability of skilled personnel, the presence and availability of service integration, and the minimum standard for laboratory setup, drug supply, and equipment. Patients and health care providers received distinct interview on time-motion and delivery style, as well as some probing questions. Respective responses were recorded with a tape recorder and handwritten notes, then analyzed based on themes.
Data Collection, Processing, and Analysis
Data were collected using structured interviewer-administered questionnaires addressing socio-demographics, the quality of service provided, and the time motion of patient satisfaction. The questionnaire was adapted and developed based on the Donebidean Model framework through a review of various relevant literatures.21–27 Checklists were used for in-depth interviews. Questionnaires were translated into the local language and then back translated to English by another person to maintain internal consistency. A pre-test was carried out on 5% of the sample size before the actual data collection, and possible modifications of the tool were done based on the results of the pre-test. Two days of training were given for data collectors and supervisors, which focused on the aim of the study, procedures, data collection techniques, the art of interviewing, ways of collecting the data, and clarification on how to manage the data collection process. Supervisors and the principal investigator performed immediate supervision on a daily basis. Every day, the collected data was reviewed and cross-checked for completeness and relevance before data entry. The data were analyzed by SPSS Version 24.0. Prior to analysis, the data were checked for normality and homogeneity, then analyzed and interpreted by the research team. Inconsistencies and missing values were checked by running frequencies and other data explorations. Descriptive statistics like frequency distributions, mean, and standard deviation were computed. Bivariate analysis was done primarily to check which independent variables had an association with the dependent variable (time motion of patient satisfaction). Independent variables with marginal associations (P <0.25) in the bivariate analysis, which are plausible and those variables showed significant association in the previous studies, were entered into a multivariable logistic regression analysis in order to detect association with the outcome variable. We used the Hosmer-Lemeshow test to check the appropriateness of the model for analysis. Finally, adjusted odds ratios (AOR) with a 95% CI were estimated to assess the strength of associations; statistical significance was declared at a p-value < 0.05.
Ethical Clearance and Consent to Participate
This study was approved and conducted per the principles of the Helsinki Declaration. Ethical clearance was obtained from the Research Ethics Review and Approval Committee (REAC) of Wachemo University with reference number Ref.No.WCU/SGS/1173/12 and Date 10/09/12 (local date in Ethiopian calendar) with unique student registration number WCU003410. A formal letter from the college of medicine and health sciences was obtained and delivered to all appropriate offices in each kebele to request authorization. Informed verbal consent was obtained from each participant after thoroughly explaining the objectives and benefits of the study. We employed verbal consent since it is preferable for routine treatments such as prophylaxis, given that full records are already maintained in health institutions, because this study is being conducted on ART patients following their treatment in health institutions. In our scenario, we depend on verbal consent because the entire client’s written documents, including the name of the individual who gave the consent, are present. In our context, the ethics review committee gives a letter of permission with a reference number and date without disclosing the names of the institutional review committee, as mentioned above. The study participants were told that they have the right to withdraw at any time from the study. The participants were also informed that their responses would be kept confidential and that their names would not be mentioned. All participants’ rights to self-determination and autonomy were respected. The participants were also informed that the study had no loss of benefits and discontinuing answering the question also does not harm them and no punishments at all.
Results
Socio-Demographic Characteristics
Four hundred twenty-two patients participated in the study, giving a response rate of 100%. Table 1 presents the socio-demographic and economic characteristics of respondents in Hadiya Zone, Central Ethiopia. Accordingly, the mean (±SD) age of the patients was 37.95±10.24 years. Of the total patients, 83.1% (325/422) were from Wachemo University Nigist Elleni Memorial Comprehensive Hospital, and the rest were from Shone Primary Hospital, Ginbichu Primary Hospital, and Homecho Primary Hospital. The majority, 64.5% (272/422), of the respondents were unmarried and Protestants by religion. More than three-fourths (335/422) learned for the first time from health providers about the availability of ART services (Table 1).
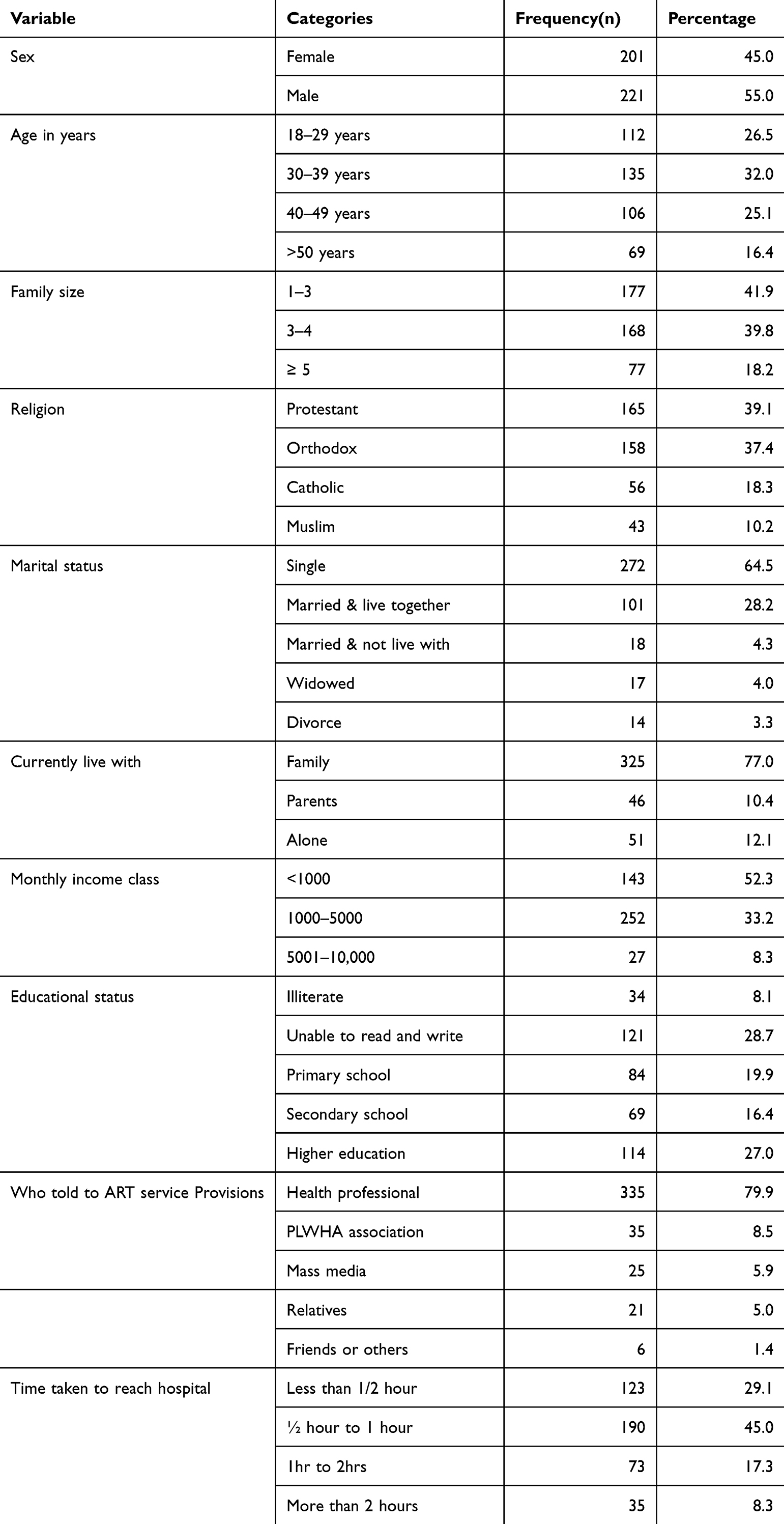 |
Table 1 Socio-Demographic Characteristics of ART Patients in the Four Hospitals in Hadiya Zone, Central Ethiopia, July 2021 (n=422) |
Time Motion and Process Variables for Patient Satisfaction on ART Services
Time motion and patient satisfaction level with ART services were measured using various items like time, information, and the interaction of the patient-provider service provision dimensions. Table 2 presents time motion and process variables for patient satisfaction on art services in four hospitals in the Hadiya zone. Accordingly, the overall level of satisfaction with time motion and patient satisfaction with ART service was 53.1%. Regarding the source of information, about 335 (79.4%) heard about ART services from health professionals, whereas 35 (8.3%) of the respondents heard from PLWHA. With respect to time to reach the health facility, about 190 (45.0%) of the patients took half an hour to 1 hour, and 73 (17.3%) took 61 minutes to 2 hours (Table 2).
 |
Table 2 Time Motion and Process Variables for Patient Satisfaction on ART Services in Four Hospitals in Hadiya Zone, July 2021 (n=422) |
Patients’ Perception on Time Motion of Patient Satisfaction
Table 3 presents the mean score for time motion and patients’ perceptions of the process of service provision. Accordingly, the average means scores perception of convenient hours and ideal time to get services were (mean ± standard deviation) (7.89 + 0.65) and (16.89 + 3.96), respectively. In similar terms, in this study, the average mean score of overall satisfaction was (mean ± standard deviation) (105.28 ± 36.88) (Table 3).
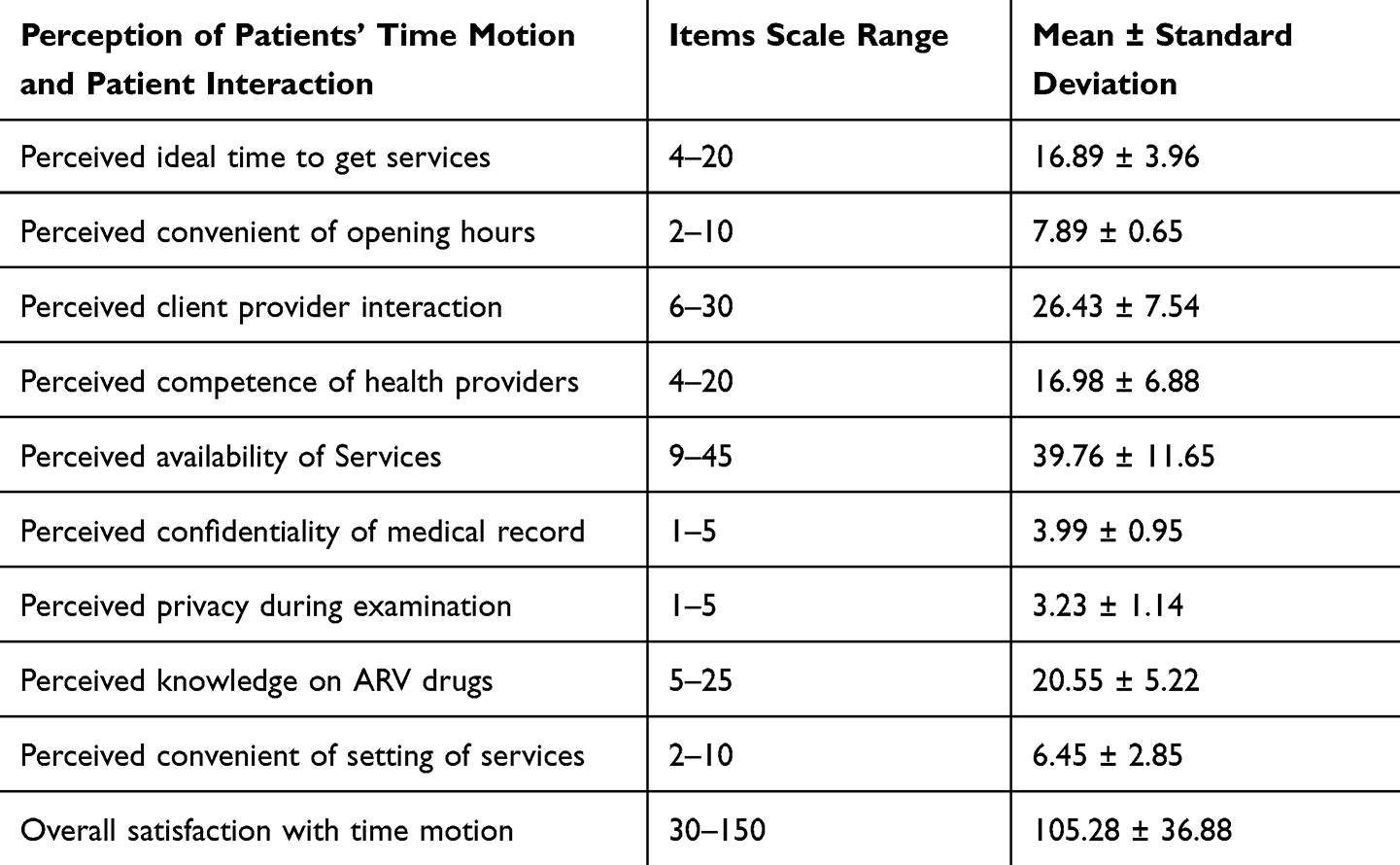 |
Table 3 Presents Average Mean Scores Patients’ Perception on Time Motion and Satisfaction in Hadiya Zone, Central Ethiopia, July 2021 (N=422) |
Factors Affecting Time Motion and Patient Satisfaction on ART Services
Sex, religion, income class, family size, service hour convenience, patient-provider interaction, perceived privacy, and time spent waiting to be seen by a health professional were selected as candidates for bivariate logistic regression. However, in a multivariable logistic regression analysis, sex, income class, time spent waiting to see a health professional, patient-provider interaction, and perceived privacy had a statistically significant association with time motion and patient satisfaction with ART services. This study showed that females were found to be 2.499 times more likely to be satisfied when compared with males (AOR = 2.499, 95% CI = [1.556, 4.009]). The findings of this study indicated that high-income participants were 77.2% less likely to be satisfied than those study participants who were from low-income classes (AOR =0.228, 95% CI (0.073–0.707)). The analysis of this study also revealed that study participants who had less than 30 minutes to see a doctor were 77.2% less likely to have satisfaction than those who had greater than 30 minutes (AOR =0.228, 95% CI [0.079–0.661]). Patient-provider interaction (AOR = 3.720, 95% CI = 2.111–5.771) and perceived privacy (AOR = 2.912, 95% CI = 1.76–2.78) also had higher odds of time motion and patient satisfaction as compared to those who were not (Table 4).
 |
Table 4 Bivariate and Multivariable Analysis of Time Motion of Patient’s Satisfaction on ART Service in Four Hospitals in Hadiya Zone, Central Ethiopia, June 2012 (N=422) |
Discussion
The health status of the individuals was determined by timely getting the required services. The perceived time may be the same as the actual time. Though this study does not only focus on the time parameter, the time motion of patient satisfaction was studied using the Donebidean model, considering various factors that the hospital requires to fulfill and deliver. Thus, the current study found that overall patient satisfaction with ART service was 53.1% (296/422). This study is lower than the patient satisfaction studies conducted in several parts of Ethiopia, such as Tigray (89.6%),28 Addis Ababa (85.5%),29 and Jimma (82%).15 However, it is consistent the study conducted in Amara region.30 This might be because satisfaction is a psychological variable that varies from place to place owing to the structure of the hospital, the interaction of health professionals, and the time it takes to get the services. The other might be in the current study; time used as a variable and calculated with other process variables might cause the variation.
Previous studies documented that the average time to stay in an outpatient department varies from country to country; pointing out that the mean waiting time was approximately less than an hour.31–33 The present study also confirmed that time spent to see a doctor had a statistically significant association with time spent and patient satisfaction with ART services. The qualitative part also confirmed that all study hospitals fulfilled the minimum packages for the initiation of antiretroviral service. Participants also confirmed that service related organizational structure very pleasant to get services and treatment. This might be the expectation of the service obtained mostly depends on the patient’s perceived expectation of the service provided with his or her time.
In this study, female patients were found to be satisfied when compared with males. This is similar to the study conducted in various parts of Ethiopia and abroad.20,28–30 The qualitative findings also supported that females were good at following the treatment given and maintaining consistent follow-up. This might be a persistent follow-up treatment for the females that results in a decrease in viral load and pain.
In real science, the socio-economic status of a given society is the best predictor of the social determinants of health.34,35 The current study also found that participants who had a higher monthly income were more likely to be satisfied than those who did not have a monthly income. These findings are in line with the study done in Addis Ababa, Ethiopia and Midre-Genet Hospital in Northwest Tigray, where monthly incomes of 500–1000 Ethiopian Birr (ETB) and more than 1000 ETB were found to be 99.9% and 96.9% more likely to be satisfied than those who did not have a monthly income.28,29
The present study found that those who perceived patient-provider interaction had higher odds of time-motion of patient satisfaction than those who did not interact well. This is consistent with the studies conducted in Ethiopia and abroad.18,19,30–34 The main assumption of the Donebidean model in the process dimension also supports this idea.23–27 A qualitative interview also added that the current innovative training on compassionate and respectful care of patients improved the service delivery process.
In previous studies, the continuity of care was determined by keeping the patient’s privacy during the service delivery process.36,37 The present study found that those who perceived privacy during interaction had higher odds of time motion of patient satisfaction than those who did perceive their privacy was not kept. This might be because, as it has been demonstrated in the qualitative interview, all the physical facilities expected the ratio of patient to provider to be more than enough.
As strength, this study is an icebreaker for public health researchers to shift research dimensions to the most important component of service delivery: the time-motion study. Another strength is study used tested model as a conceptual framework ie Donebidean model. As limitations, the study was conducted using Donebidean model to assess the three dimensions of the service provision and however, process part of the model is limited to addressing the individual perception. Another limitation is since the study was conducted using a cross-sectional design, it is difficult to determine whether the behavior or the predicting variable occurred first. This study is also subjected to social desirability bias since satisfaction is too personal, which might increase the chance for underreporting or over-reporting of the behavior.
In conclusion, 53.1% of ART patients in the research area reported being satisfied with the treatments they received, which were found to be substantially correlated with sex, income, perceived patient-provider interaction, perceived privacy, and the amount of time spent seeing medical personnel. To improve patient satisfaction, hospitals and the zone health department, as well as any organizations operating in the area of ART, should work on the service availability with time and accessibility to the nearest for the rich and poor on time. Hospitals should integrate and strengthen the system for timely service delivery. Furthermore, further study is required to analyze the strength and reach of the information through an examination of pre- and post-intervention, which offers a complete picture of conceptualizations of.
Data Sharing Statement
The data analyzed during the current study are available from the corresponding author on a reasonable request.
Acknowledgments
We would like to thank Wachemo University, College of Medicine and Health Sciences. We also thank all study participants, data collectors, and supervisors of data collection.
Author Contributions
All authors contributed to data analysis, drafting or revising the article, have agreed on the journal to which the article will be submitted, gave final approval of the version to be published, and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no conflicts of interests in this work.
References
1. Joint United Nations Programme on HIV/AIDS (UNAIDS). Ending AIDS: progress towards the 90-90-90 targets. Global AIDS update. 2017.
2. Babatunde AO, Akin‐Ajani OD, Abdullateef RO, Togunwa TO, Isah HO. Review of antiretroviral therapy coverage in 10 highest burden HIV countries in Africa: 2015–2020. J Med Virol. 2023;95(1):e28320. doi:10.1002/jmv.28320
3. Mirkuzie AH, Hu W. Implementation and outcomes of guideline revisions for the prevention of mother-to-child HIV transmission in Mother Support Programme, Addis Ababa, Ethiopia. PLoS One. 2018;13(6):e0198438. doi:10.1371/journal.pone.0198438
4. World Health Organization. The Use of Antiretroviral Drugs for Treating and Preventing Hiv Infection Preventing HIV Infection, 2016 Recommendations for a Public Health Approach, W.l.c.-I.-P. Data, Editor. Geneva, Switzerland: World Health Organization; 2016.
5. Addisu T, Tilahun M, Wedajo S, Sharew B. Trends Analysis of HIV Infection and Antiretroviral Treatment Outcome in Amhara Regional from 2015 to 2021, Northeast Ethiopia. HIV/AIDS-Res Palliative Care. 2023;31:399–410. doi:10.2147/HIV.S411235
6. World Health Organization. Guidelines: Updated Recommendations on HIV Prevention, Infant Diagnosis, Antiretroviral Initiation and Monitoring. World Health Organization; 2021.
7. World Health Organization. Consolidated Guidelines on HIV Testing Services, 2019: Web Annex L: Symptom and Risk-Based Screening to Optimize HIV Testing Services: A Scoping Review. World Health Organization; 2020.
8. Moyo F, Mazanderani AH, Barron P, et al. Introduction of routine HIV birth testing in the South African National Consolidated Guidelines. Pediatr Infect Dis J. 2018;37(6):559–563. doi:10.1097/INF.0000000000001840
9. Gutema G, Tola HH, Fikadu D, et al. Positivity rate, trend and associated risk factors of mother-to-child transmission of HIV among HIV-exposed infants. BMC Pediatric. 2023;23(1):283. doi:10.1186/s12887-023-04074-2
10. Okusanya B, Nweke C, Gerald LB, Pettygrove S, Taren D, Ehiri J. Are prevention of mother-to-child HIV transmission service providers acquainted with national guideline recommendations? A cross-sectional study of primary health care centers in Lagos, Nigeria. BMC Health Serv Res. 2022;22(1):1. doi:10.1186/s12913-022-08152-6
11. Wessels J, Sherman G, Bamford L, et al. The updated South African national guideline for the prevention of mother to child transmission of communicable infections (2019). Southern African Journal of HIV Medicine. 2020;21(1). doi:10.4102/sajhivmed.v21i1.1079
12. Zhylka N, Pedachenko N, Shcherbinska O, Gruzieva T, Pakharenko L Improvement of the health services for the prevention of HIV transmission from mother to child at the level of primary health care; 2022.
13. Leddy KM, Kaldenberg DO, Becker BW. Timeliness in ambulatory care treatment: an examination of patient satisfaction and wait times in medical practices and outpatient test and treatment facilities. J Ambul Care Manag. 2003;26(2):138–149. doi:10.1097/00004479-200304000-00006
14. Barsamian AM, Gregoire M, Sowa D, Lafferty L, Stone M. Timely resolution of patient concerns improves post-discharge satisfaction. J Am Diet Assoc. 2010;110(9):1346–1350. doi:10.1016/j.jada.2010.06.006
15. Gezahegn M, Wolde D, Ejigu Y, Tolessa F, Fufa D. Patient satisfaction with antiretroviral therapy service and associated factors at Jimma town public health facilities, southwest, Ethiopia. HIV/AIDS-Res Palliative Care. 2021;13:691–697. doi:10.2147/HIV.S300840
16. Manna N, Samsuzzaman M, Das S. A time motion study in the OPD clinic of a rural hospital of West Bengal. IOSR J Dent Med Sci. 2014;13(7):34–37. doi:10.9790/0853-13723437
17. Chopade RR, Sharma NK, Sundar SM. A time and motion study in outdoor patient department of rural health training centre of tertiary medical college in Konkan region, India. Int J Community Med Public Health. 2019;6(8):3242–3245. doi:10.18203/2394-6040.ijcmph20193434
18. Naaz F, Mohammed I. A time motion study to evaluate the average waiting time in OPD with reference to patient satisfaction in the setting of state-level AYUSH Hospital (India). Med J Islamic World Acad Sci. 2019;27(3):71–76. doi:10.5505/ias.2019.89410
19. Sengupta B, Kumar Mandal P, Kar A, Bhattacharyya N, Biswas S, Resident J. A time motion study of healthcare delivery system at general OPD of rural hospital of West Bengal. Int J Res Rev. 2020;7:254–260.
20. Assefa Y, Jerene D, Lulseged S, Ooms G, Van Damme W. Rapid scale-up of antiretroviral treatment in Ethiopia: successes and system-wide effects. PLoS Med. 2009;6(4):e1000056. doi:10.1371/journal.pmed.1000056
21. Lalazaryan A, Zare-Farashbandi F. A review of models and theories of health information seeking behavior. Int J Health Sys Disaster Manage. 2014;2(4):193. doi:10.4103/2347-9019.144371
22. Bergeron K, Abdi S, DeCorby K, Mensah G, Rempel B, Manson H. Theories, models and frameworks used in capacity building interventions relevant to public health: a systematic review. BMC Public Health. 2017;17(1):1–2. doi:10.1186/s12889-017-4919-y
23. Ibn El Haj H, Lamrini M, Rais N. Quality of care between Donabedian model and ISO9001V2008. Int J Qual Res. 2013;7:1.
24. Sharew Y, Mullu G, Abebe N, Mehare T. Quality of health care service assessment using Donabedian model in East Gojjam Zone, Northwest Ethiopia, 2018. African J Med Health Sci. 2020;19(9):157–165.
25. Tossaint-Schoenmakers R, Versluis A, Chavannes N, Talboom-Kamp E, Kasteleyn M. The challenge of integrating eHealth into health care: systematic literature review of the Donabedian model of structure, process, and outcome. J Med Int Res. 2021;23(5):e27180. doi:10.2196/27180
26. Doyore F, Moges B. Client satisfaction to antiretroviral treatment services and associated factors among clients attending ART clinics in Hossana town, southern Ethiopia. Clin Res. 2016;2(6):6.
27. LoPorto J. Application of the Donabedian quality-of-care model to New York State direct support professional core competencies: how structure, process, and outcomes impacts disability services. J Sustain Soc Change. 2020;12(1):5.
28. Atsebeha KG, Chercos DH. High antiretroviral therapy service delivery satisfaction and its’ associated factors at Midre-genet hospital; Northwest Tigray, Ethiopia. BMC Health Serv Res. 2018;18(1):1–9. doi:10.1186/s12913-018-3055-4
29. Mindaye T, Taye B. Patients satisfaction with laboratory services at antiretroviral therapy clinics in public hospitals, Addis Ababa, Ethiopia. BMC Res Notes. 2012;5(1):1–7. doi:10.1186/1756-0500-5-184
30. Tebeje M, Worku W, Getachew F, Temesgen SA. Patients’ satisfaction with laboratory services at Anti-Retroviral Therapy clinic of Felegehiwot Hospital, Bahirdar, North West Ethiopia. Ethiopian J Public Health Nutri. 2020;4:1.
31. Chebolu-Subramanian V, Sule N, Sharma R, Mistry N. A time motion study of community mental health workers in rural India. BMC Health Serv Res. 2019;19(1):1–7. doi:10.1186/s12913-019-4732-7
32. Kalne PS, Mehendale AM. The purpose of time-motion studies (TMSs) in healthcare: a literature review. Cureus. 2022;14:10.
33. Singh S, Dwivedi N, Dongre A, et al. Functioning and time utilisation by female multi-purpose health workers in South India: a time and motion study. Human Res Health. 2018;16(1):1. doi:10.1186/s12960-018-0327-3
34. Raphael D. Social determinants of health: Canadian perspectives. Can Scholars Press. 2016;10:12.
35. Hicks LJ, Mushquash CJ, Toombs E. A national-level examination of First Nations peoples’ mental health data: predicting mental well-being from social determinants of health using the 2017 Aboriginal Peoples Survey. Front Public Health. 2023;11:1073817. doi:10.3389/fpubh.2023.1073817
36. Crooks VA, Agarwal G. What are the roles involved in establishing and maintaining informational continuity of care within family practice? A systematic review. BMC Fam Pract. 2008;9(1):1–9. doi:10.1186/1471-2296-9-65
37. Perwej Y, Akhtar N, Kulshrestha N, Mishra P. A Methodical Analysis of Medical Internet of Things (MIoT) security and privacy in current and future trends. J Emerg Technol Innova Res. 2022;9(1):d346–71.
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.