")
Back to Journals » Journal of Blood Medicine » Volume 14
Pharmacologically Treated Anxiety and Depression in People Diagnosed with von Willebrand Disease: Matched Cohort Study
Authors Hagberg KW , Jick S , Özen G, Du P
Received 10 February 2023
Accepted for publication 19 June 2023
Published 11 July 2023 Volume 2023:14 Pages 413—425
DOI https://doi.org/10.2147/JBM.S407993
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Martin H Bluth
Katrina Wilcox Hagberg,1 Susan Jick,1,2 Gülden Özen,3 Ping Du3
1Boston Collaborative Drug Surveillance Program, Lexington, MA, 02421, USA; 2Boston University School of Public Health, Boston, MA, 02118, USA; 3Takeda Development Center Americas, Inc., Cambridge, MA, 02139, USA
Correspondence: Susan Jick, Boston Collaborative Drug Surveillance Program, 11 Muzzey Street, Lexington, MA, 02421, USA, Tel +1 781 862 6660, Fax +1 781 862 1680, Email [email protected]
Background: People diagnosed with von Willebrand disease (VWD) have reduced quality of life versus the general population, and there is limited evidence of increased rates of anxiety and/or depression among people diagnosed with VWD.
Aim: To understand the association between VWD and mental health outcomes.
Design and Setting: A retrospective cohort study was conducted using the UK Clinical Practice Research Datalink (CPRD) GOLD database (1988– 2016).
Methods: People diagnosed with VWD were matched 1:10 to randomly selected people in the database without VWD based on sex, birth year ± 2 years, CPRD record start year ± 2 years, and general practice attended. Individuals were followed from VWD diagnosis or match date to censoring (first event date, CPRD end date, or death). Treated anxiety and treated depression were identified by a diagnostic Read Code and a prescription for anxiety/depression medication recorded within 90 days of each other, after VWD diagnosis/match date.
Results: Treated anxiety was recorded in 89 of 1119 (8.0%) people diagnosed with VWD and 624 of 10,423 (6.0%) without VWD (age- and sex-adjusted incidence rate ratio [IRR], 1.37; 95% confidence interval [CI], 1.10– 1.71). Treated depression was recorded in 119 of 1083 (11.0%) people diagnosed with VWD and 846 of 9845 (8.6%) without VWD (adjusted IRR, 1.35; 95% CI, 1.11– 1.63). Females aged 20– 39 and 0– 19 years were at greatest risk for treated anxiety and treated depression, respectively.
Conclusion: Higher rates of treated anxiety and depression were observed among people diagnosed with versus without VWD, predominantly in young females.
Keywords: anxiety, depression, general practice, mental health, von Willebrand disease
Introduction
von Willebrand factor is a clotting protein that mediates platelet functions and stabilizes clotting factor VIII.1 Congenital von Willebrand disease (VWD) is characterized by impaired function or reduced levels of von Willebrand factor, and is the most common inherited bleeding disorder globally (prevalence of 600–1300 per 100,000 individuals).2 The prevalence of symptomatic disease requiring treatment is, however, much lower (10 per 100,000). VWD bleeding phenotypes vary depending on disease type, age, and sex.3 Common symptoms include bruising, epistaxis, bleeding from wounds or surgeries, joint and mucocutaneous bleeding, and menorrhagia.3–5 Rare and potentially life-threatening bleeding can occur in the central nervous system and gastrointestinal tract.3,5
People diagnosed with VWD have lower health-related quality of life, as measured by Short Form 36 mental component scores, than the general population,6,7 with some evidence suggesting that depression and anxiety are more common in people diagnosed with VWD.8 Bleeding disorders (hemophilia and VWD) have been reported to have a negative impact on psychological health, with unpredictable bleeding symptoms and fears for the future cited as causes of anxiety, and loss of or reduction in valued activities and loss of independence as causes of depression.9 For example, women diagnosed with VWD experience impaired quality of life and greater impact on daily activities as a result of menstruation than individuals without VWD.10 In addition, misdiagnosis and delayed diagnosis of VWD are common, particularly in women, and lead to worse outcomes,11–13 which may in turn contribute to impaired quality of life and mental health. Data on mental health disorders in people diagnosed with VWD are limited, however, and more information is needed to improve their overall health and wellbeing. This retrospective cohort study was conducted using UK clinical practice data to better understand the occurrence of treated anxiety and treated depression in people diagnosed with VWD.
Methods
Data Source
Data were extracted from the UK Clinical Practice Research Datalink (CPRD) GOLD database (January 1, 1988 to June 30, 2016), which is a large, prospectively collected, anonymized electronic medical record database that is broadly representative of the UK population, in terms of age, sex, and minority distribution. As UK health care is universal and free, selection bias resulting from differential health care access is minimized. CPRD GOLD comprises demographic information, prescription details, clinical events, and lifestyle details. Information relating to inpatient and outpatient medical encounters (specialists, hospital stays) is provided to individuals’ general practitioners (GPs) in consultant and discharge letters, and GPs may code these details in the patient’s electronic data. The study population was from the general practice setting and therefore is representative of individuals receiving general practice care.14
Study Population
Individuals with a Read Code indicating a diagnosis of VWD (D304.00), recorded at any time, were included. Individuals were excluded if they were suspected of having acquired von Willebrand syndrome due to a diagnosis of certain autoimmune disorders (ie, lymphoproliferative diseases, monoclonal gammopathies, systemic lupus erythematosus, hypothyroidism, essential thrombocythemia, polycythemia vera, myelofibrosis) or cancers (eg, myeloproliferative neoplasms).14 All other individuals were assumed to have congenital VWD, regardless of age at first recorded VWD diagnosis.
Each person with VWD was matched to up to 10 people without VWD, selected randomly from all people in the database without a diagnosis of VWD. Matching criteria were sex, birth year (±2 years), CPRD record start year (±2 years), and general practice attended. As the case definitions for anxiety and depression required a diagnosis plus pharmaceutical treatment to be recorded in the electronic medical record, the study population was restricted to individuals whose first VWD diagnosis or match date was recorded after the start of the electronic CPRD record.
Outcomes of Interest
Treated anxiety or treated depression events were identified by a diagnostic Read Code for anxiety and/or depression plus receipt of a prescription for drugs used to treat anxiety or depression (Supplemental Table 1) within 90 days of each other, both recorded in the electronic record after the VWD diagnosis or match date. The index date was defined as the date of the qualifying diagnosis or medication prescription, whichever came first. To exclude pre-existing anxiety or depression, individuals with prior treated anxiety or treated depression events before the VWD diagnosis or match date were excluded from the relevant analyses.
Eligible individuals were followed from the VWD diagnosis or match date until the censoring date, defined as the index date, date of electronic record end, or death, whichever occurred first.
Covariates
In addition to the matching criteria, the presence of covariates related to general health at the VWD diagnosis/match date (including events present in the historical record) and at the case index date were described: hypertension, diabetes, hypercholesterolemia, chronic kidney disease, liver disease, alcohol abuse, and drug abuse. The presence of an anxiety or depression diagnosis before the VWD diagnosis/match date was also evaluated.
Statistical Analysis
Treated anxiety and treated depression were evaluated separately. Demographics were described at the VWD diagnosis/match date for the VWD and matched non-VWD cohorts, and at the index date for individuals with treated depression and/or anxiety. Person-years (PY) were accumulated separately for each outcome from the VWD diagnosis/match date to the censor date (ie, the index date for treated anxiety or depression, date of Clinical Practice Research Datalink record end, or death, whichever occurred first).
Incidence rates (IRs) with 95% confidence intervals (CIs) were calculated for each outcome for participants diagnosed with and without VWD overall and stratified by sex and age at treated anxiety or depression date using Byar’s method. Crude, sex- and age-adjusted incidence rate ratios (IRRs) with 95% CIs for each outcome for people diagnosed with VWD versus those without VWD were calculated using Poisson regression. The risk (cumulative incidence function) was also estimated for each outcome using the Kaplan–Meier method, overall and stratified by age at VWD diagnosis/match date. Kaplan–Meier curves were compared using a Log rank test. Descriptive and IR analyses were performed using SAS (version 9.4). All Kaplan–Meier and Cox model analyses were performed using R (version 4.0.2).
Results
Treated Anxiety
The baseline characteristics of 1119 people diagnosed with VWD and 10,423 matched individuals without VWD included in the anxiety analysis are shown in Table 1. The majority of people were female (62.8% with VWD; 62.4% without VWD), and most were aged ≤30 years at VWD diagnosis/match date (61.2% with VWD; 62.3% without VWD). A diagnosis of anxiety (without an associated prescription) was recorded before VWD diagnosis in 6.3% of people diagnosed with VWD and 3.9% of those without VWD.
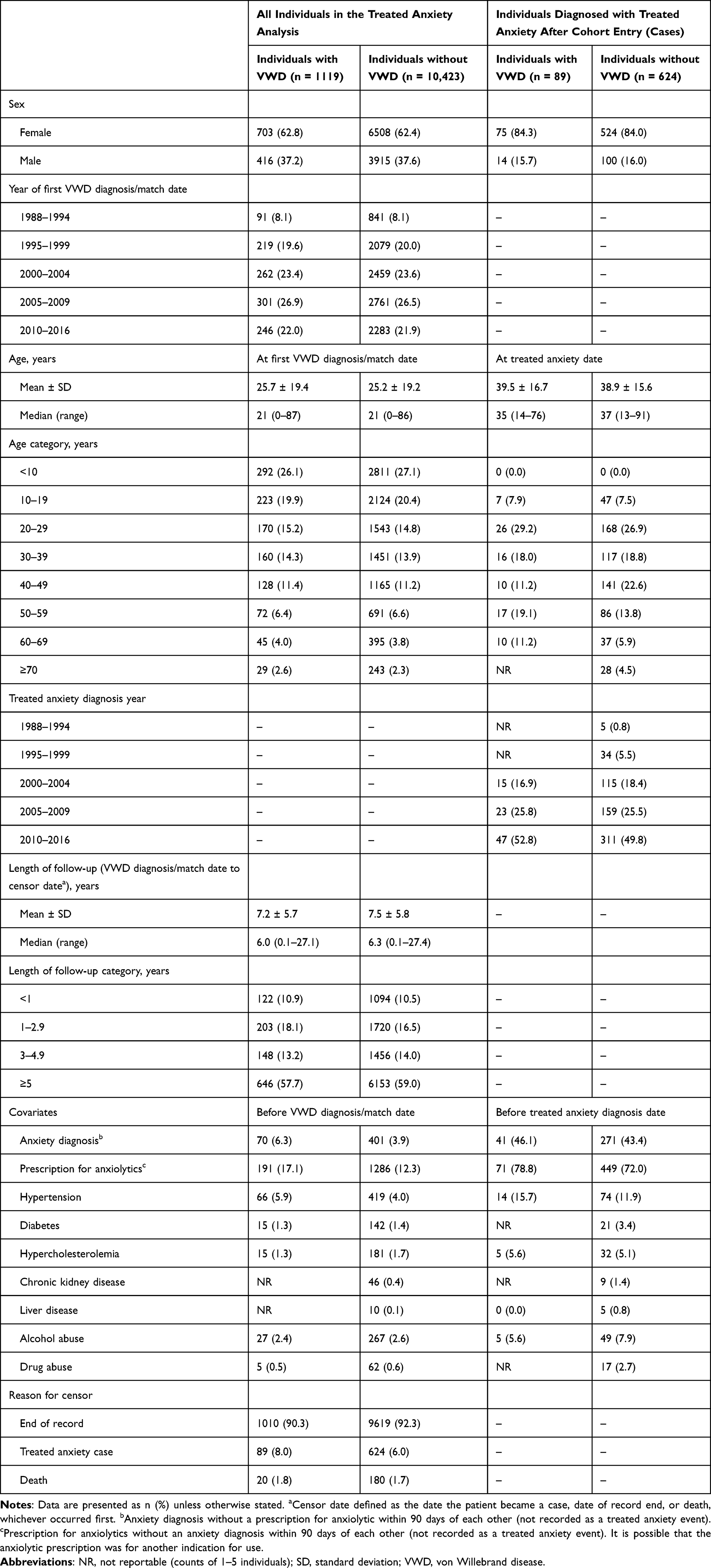 |
Table 1 Baseline Characteristics of Individuals Included in the Treated Anxiety Analysis and Characteristics of Treated Anxiety Cases |
Treated anxiety was recorded in 89 people with VWD (8.0%) and 624 without VWD (6.0%) (Table 1). People diagnosed with VWD and treated anxiety were slightly younger than those without VWD (median age of 35.0 versus 37.0 years, respectively). Similar numbers of individuals in the VWD and non-VWD cohorts had a record of an anxiety diagnosis without a prescription or a prescription without a diagnosis before they met the criteria for treated anxiety. The number of individuals with other medical conditions was low and relatively balanced between the two cohorts.
The cumulative incidence of treated anxiety was higher in people diagnosed with VWD versus those without VWD (P = 0.0038) (Figure 1). In stratified analyses, cumulative incidence was higher in females diagnosed with VWD versus those without VWD (P = 0.011), but not in males (P = 0.22) (Supplemental Figure 1), and was higher for people with versus without VWD for all age groups, but was only statistically significant for individuals aged <10 years (P = 0.042) or 20–29 years (P = 0.033) (Supplemental Figure 2). When stratified by sex and age, cumulative incidence was only statistically significant for females aged 20–29 years at VWD diagnosis or match date (P = 0.012) (Supplemental Figure 3).
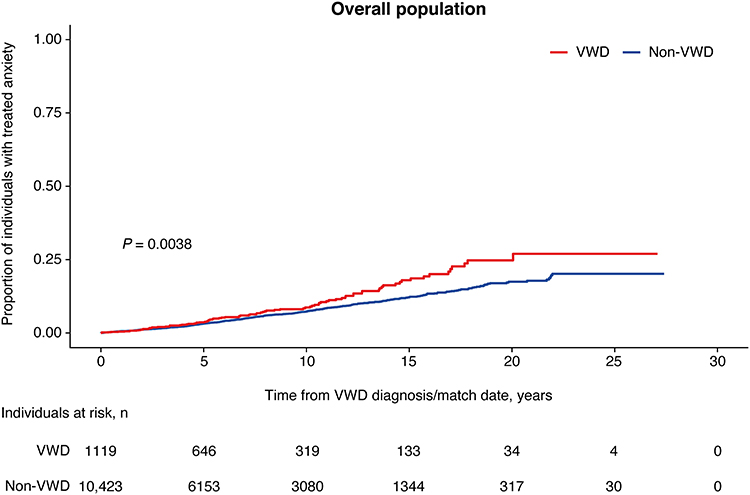 |
Figure 1 Cumulative incidence of treated anxiety after VWD diagnosis/match date among individuals with versus without VWD. Abbreviation: VWD, von Willebrand disease. |
The IR for treated anxiety was 11.0 (95% CI, 8.8–13.5) per 1000 PY for people diagnosed with VWD and 8.0 (95% CI, 7.3–8.6) per 1000 PY for people without VWD (Table 2). The IR for treated anxiety among females was 14.8 (95% CI, 11.6–18.5) per 1000 PY for those diagnosed with VWD and 10.9 (9.9–11.8) per 1000 PY for non-VWD matches, whereas the IRs for males were lower (4.6 [95% CI, 2.5–7.8] and 3.3 [95% CI, 2.7–4.0] per 1000 PY, respectively). IRs for treated anxiety varied by age and by age and sex (Table 2).
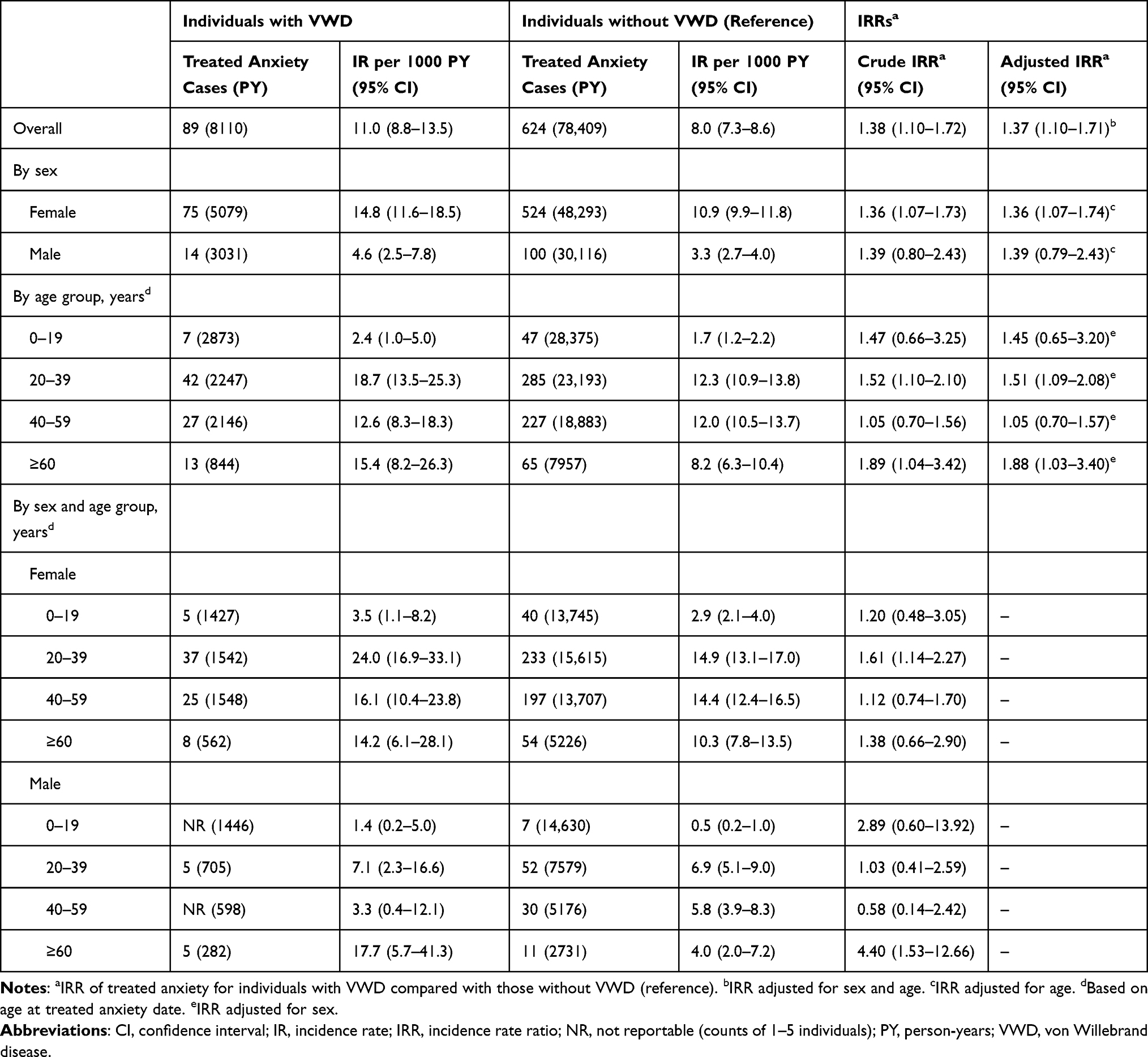 |
Table 2 IRs and IRRs of Treated Anxiety in Individuals with or without VWD |
Overall, the risk of treated anxiety was higher for people diagnosed with VWD than those without VWD (age- and sex-adjusted IRR, 1.37 [95% CI, 1.10–1.71]). Risk estimates were similar among females and males but varied by age, with a higher risk observed in individuals aged 20–39 years or ≥60 years (Table 2). When stratified by sex and age, the greatest risk of treated anxiety in females was observed among those aged 20–39 years, with these individuals having a 61% higher rate of treated anxiety than those without VWD. There were too few cases for risk estimates for males to be reliable when stratified by age group.
Treated Depression
Baseline characteristics for the 1083 people diagnosed with VWD and 9845 matched individuals without VWD included in the treated depression analysis are shown in Table 3. The majority of people were female (62.1% with VWD; 61.2% without VWD) and most (61.9% diagnosed with VWD; 63.8% without VWD) were aged ≤30 years at VWD diagnosis/match date. A diagnosis of prior non-treated depression was recorded in 7.2% of people with VWD and 4.9% of those without VWD.
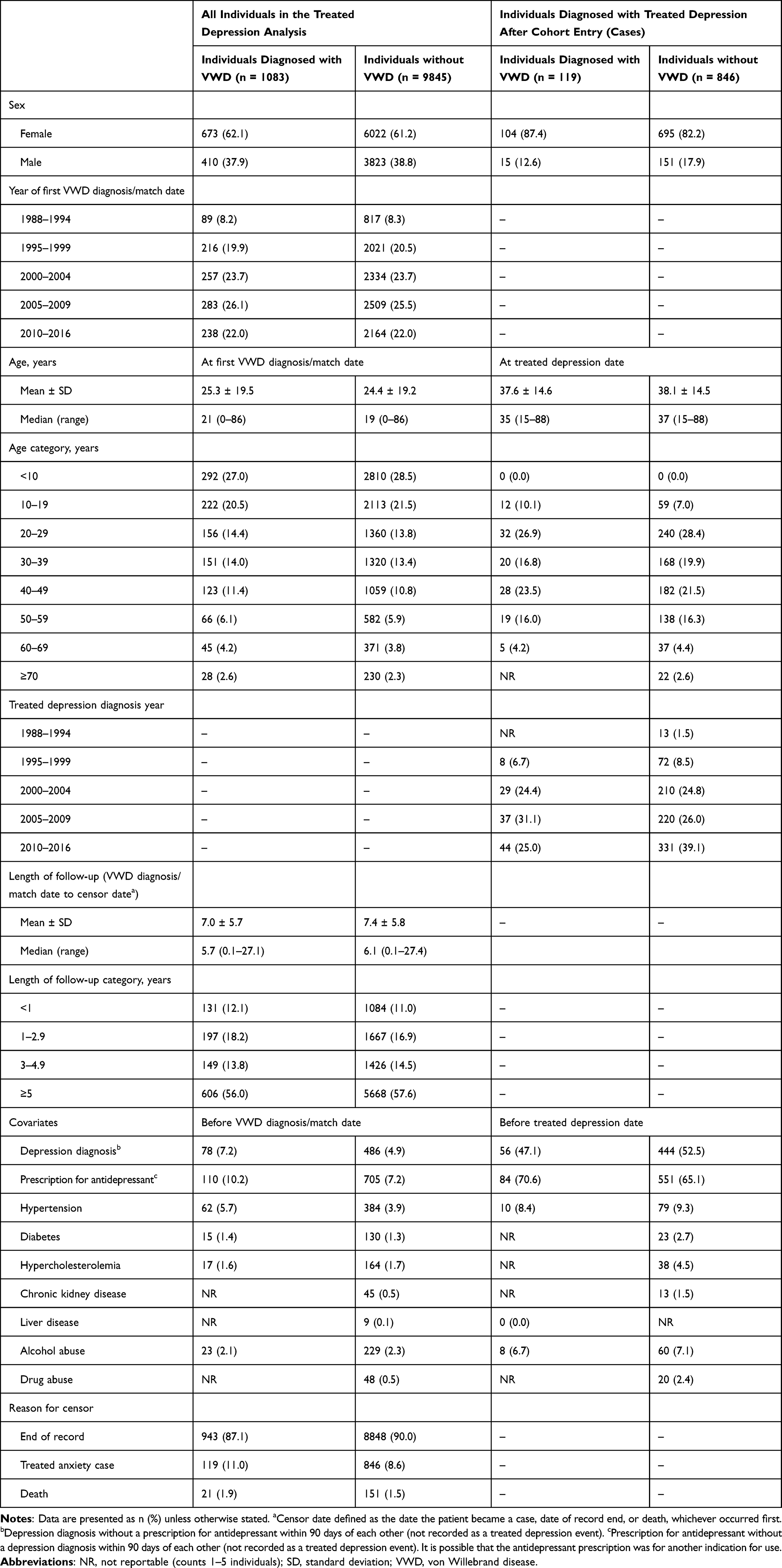 |
Table 3 Baseline Characteristics of Individuals Included in the Treated Depression Analysis and Characteristics of Treated Depression Cases |
Treated depression was recorded in 119 people (11.0%) diagnosed with VWD and 846 without VWD (8.6%) (Table 3). People diagnosed with VWD were slightly younger than those without VWD (median age of 35.0 versus 37.0 years, respectively). In the VWD and non-VWD cohorts, similar numbers of treated depression cases had a record of a depression diagnosis without a prescription or a prescription without a diagnosis before the individual met the criteria to be a treated depression case. The number of individuals with other conditions related to general health was low and similar between cohorts.
The cumulative incidence of treated depression was statistically significantly higher in people diagnosed with VWD than in those without VWD (P = 0.0024) (Figure 2). When stratified by sex and/or age at VWD diagnosis/match date, the cumulative incidence was statistically significantly higher in females with versus without VWD (P = 0.0012), individuals of both sexes aged 20–29 years (P = 0.0089), females aged <10 years (P = 0.047), or females aged 20–29 years (P = 0.0023) (Supplemental Figures 4–6).
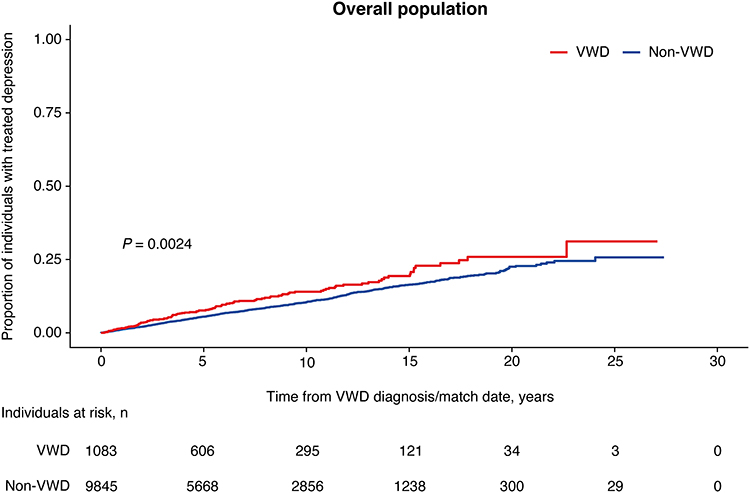 |
Figure 2 Cumulative incidence of treated depression after VWD diagnosis/match date among individuals with versus without VWD. Abbreviation: VWD, von Willebrand disease. |
The IR for treated depression was 15.6 (95% CI, 12.9–18.7) per 1000 PY for people diagnosed with VWD and 11.6 (95% CI, 10.8–12.4) per 1000 PY for those without VWD (Table 4). Among females, the IR for treated depression was 22.3 (95% CI, 18.2–27.0) per 1000 PY for the VWD and 15.9 (95% CI, 14.7–17.1) per 1000 PY for the non-VWD cohorts, whereas the IRs for males were lower (5.1 [95% CI, 2.8–8.3] and 5.2 [95% CI, 4.4–6.1]) per 1000 PY, respectively). IRs for treated depression were highest between the ages of 20 and 59 years, and varied when stratified by age and sex (Table 4).
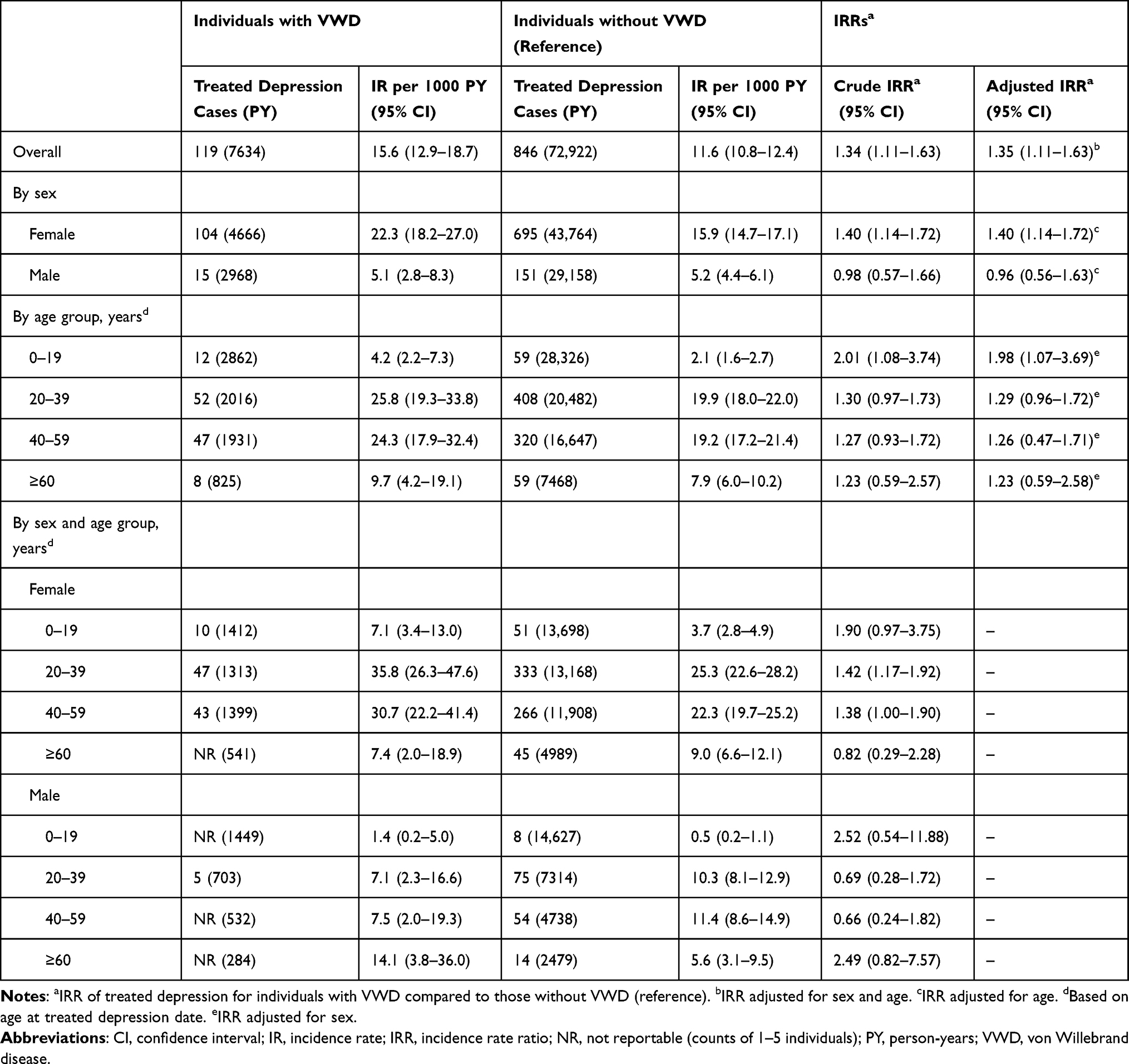 |
Table 4 IRs and IRRs of Treated Depression in Individuals with or without VWD |
The risk of treated depression was higher for people diagnosed with VWD than for those without VWD (age- and sex-adjusted IRR, 1.35 [95% CI, 1.11–1.63]) (Table 4). IRRs remained higher in females with versus without VWD when adjusted for age at treated depression date (IRR, 1.40 [95% CI, 1.14–1.72]). For males, however, the age-adjusted risk of treated depression was not higher in individuals with VWD than in those without VWD (IRR, 0.96 [95% CI, 0.56–1.63]). The IRR was highest for people (of both sexes) diagnosed with VWD aged 0–19 years compared with those without VWD when stratified by age group (Table 4). When stratified by age and sex, the greatest risk was observed in females aged 0–19 years at treated depression date and was also elevated for females aged 20–39 and 40–59, compared to similarly aged females without VWD. IRs and IRRs for males were based on too few cases to be informative.
Discussion
This retrospective cohort study describes mental health–related outcomes in people diagnosed with VWD in UK general practice. Overall, treated anxiety and treated depression were more common in individuals with VWD than in matched individuals without VWD. Females aged 20–39 and 0–19 years were at greatest risk for treated anxiety and treated depression, respectively.
Anxiety and depression rates in our study were substantially less than those in a prospective study in individuals attending hemophilia treatment centers in the USA.8 Overall rates of anxiety and depression in the US study were 58% and 64%, respectively, versus 8% and 11% among people diagnosed with VWD managed by GPs in this UK-based study. VWD complications associated with depression in the US study included self-reported chronic pain and joint problems, while joint problems were also associated with anxiety.8 In addition, findings revealed that joint problems and not being in a relationship (ie, single, widowed, or divorced) were important predictors of depression and anxiety, while anxiety was also more common in adolescents (12–18 years of age) and individuals whose general health had deteriorated in the prior 3 months.8 Although the study populations differed between the two studies, higher rates of anxiety and depression were observed in females diagnosed with VWD compared with males in both studies. The definitions of anxiety and depression in our study were more restrictive than those in the US study, in which diagnosis was based on patient-reported outcomes at the last follow-up visit (7-item Generalized Anxiety Disorder questionnaire and 8-item Patient Health Questionnaire).8 The case definition in our study required a formal diagnosis plus a prescription for anxiety or depression treatment within 90 days. This definition was intended to capture clinically relevant anxiety or depression requiring GP treatment, which should have been reliably recorded in the UK CPRD database.15–17 Thus, the incidence of anxiety and treated depression may have been underestimated in our study because only clinically treated individuals were identified. Also, individuals in whom diagnosis and treatment were recorded >90 days apart, or in whom diagnosis and treatment took place outside of primary care, would not appear in the analysis. However, this misclassification should not differ between the VWD and non-VWD populations, as individuals were matched on general practice, leading to similar GP recording habits.
This was a population-based study using data from the UK, where universal health care results in few barriers to care. All people diagnosed with VWD covered in CPRD GOLD who had a VWD diagnosis at any time were, therefore, captured. This is an important strength of our analysis, as the study cohort is likely to include individuals with a wider range of VWD severity than those being cared for by specialty centers and is likely to be representative of individuals seeking general practice care. This is in contrast to previous studies of quality of life and mental health in people diagnosed with VWD, which usually focus on those in specialist care.6–8 Another strength of this study is that individuals without VWD were matched to people diagnosed with VWD based on sex, age, calendar year, and GP attended, to control for differences in risk and data availability by these matching factors. A limitation of the study is that electronic medical records are not available for care provided in secondary/specialist care settings. Although GPs receive and have access to letters from specialists detailing care provided in secondary care settings, the GP may not have recorded these in a way that is accessible to researchers. In addition, detailed information about VWD type and severity is not available in the CPRD database. The small number of males diagnosed with VWD in the analysis meant that reliable estimates could not be calculated for this population. Finally, cardiac valvular disease, which is an underlying disease for acquired von Willebrand syndrome typically in elderly populations,18 was not included as an exclusion criteria. However, only 2.6% of individuals with VWD and 2.3% of those without VWD in the study population were aged ≥70 years at the VWD diagnosis/match date. Therefore, the potential inclusion of elderly patients with acquired von Willebrand syndrome due to cardiac valvular disease is likely to have minimal impact on the results of this study.
Conclusions
In this retrospective cohort study, treated anxiety and treated depression were more common in people diagnosed with VWD than in those without VWD, predominantly in females. These findings highlight mental health–related conditions as a potential unmet need in people diagnosed with VWD, and suggest that mental health screening could be a valuable addition to the care of people diagnosed with VWD.
Abbreviations
CI, confidence interval; CPRD, Clinical Practice Research Datalink; GP, general practitioner; IR, incidence rate; IRR, incidence rate ratio; PY, patient-years; VWD, von Willebrand disease.
Ethical Review and Data Sharing Statement
This study is based on data from the CPRD obtained under license from the UK Medicines and Healthcare products Regulatory Agency. The data are provided by patients and collected by the UK National Health Service (NHS) as part of their care and support. The interpretation and conclusions contained in this study are those of the authors alone. This study was approved by the Independent Scientific Advisory Committee (ISAC) for Medicines and Healthcare products Regulatory Agency database research, and the protocol was made available to the journal reviewers upon request (protocol No: 17_242R2A, Hospital Episode Statistics (HES) Copyright© [2018], reused with permission of The Health & Social Care Information Centre. All rights reserved). Researchers can apply for a limited license to access CPRD data for public health research, subject to individual research protocols meeting CPRD data governance requirements. More details, including data specifications, license fees, and the application process, are available on the CPRD website (https://www.cprd.com).
Acknowledgments
Statistical analysis support was provided by Rebecca Persson, MPH, epidemiologist at Boston Collaborative Drug Surveillance Program (Lexington, MA, USA). The authors would like to thank Françoise Truong Berthoz from Takeda Pharmaceuticals International AG, Zurich, Switzerland, and Spiros Tzivelekis from Takeda Development Center Americas, Inc., Cambridge, MA, USA, for their contributions to the study design. Under the direction of the authors, medical writing support was provided by Joanne Vaughan, BSc, employee of Excel Medical Affairs (Fairfield, CT, USA) and was funded by Takeda Development Center Americas, Inc., Lexington, MA, USA.
Data contained within this article were presented in part at the World Federation of Hemophilia Congress; May 8–11, 2022.19
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by Baxalta US Inc., a Takeda company, Lexington, MA, USA. The sponsor was involved with the study design, interpretation of findings, report development, and in the decision to submit the article for publication.
Disclosure
KWH and SJ have received grant/research support from Baxalta US Inc., a Takeda company, Lexington, MA, USA. GÖ is an employee of Takeda Development Center Americas, Inc., Cambridge, MA, USA, and is a Takeda stockholder. PD was an employee of Takeda Development Center Americas, Inc., Cambridge, MA, USA, at time of study. The authors report no other conflicts of interest in this work.
References
1. Lillicrap D, James P. Von Willebrand disease: an introduction for the primary care physician. Treatment of hemophilia # 47; 2009. Available from: https://www1.wfh.org/publication/files/pdf-1204.pdf.
2. Orphanet. Von Willebrand disease; 2020. Available from: https://www.orpha.net/consor/cgi-bin/OC_Exp.php?Lng=EN&Expert=903.
3. Leebeek FW, Eikenboom JC, Longo DL. Von Willebrand’s disease. N Engl J Med. 2016;375(21):2067–2080. doi:10.1056/NEJMra1601561
4. Connell NT, Flood VH, Brignardello-Petersen R, et al. ASH ISTH NHF WFH 2021 guidelines on the management of von Willebrand disease. Blood Adv. 2021;5(1):301–325. doi:10.1182/bloodadvances.2020003264
5. Nichols WL, Hultin MB, James AH, et al. von Willebrand Disease (VWD): Evidence-based Diagnosis and Management Guidelines, the National Heart, Lung, and Blood Institute (NHLBI) Expert Panel Report (USA). Haemophilia. 2008;14(2):171–232. doi:10.1111/j.1365-2516.2007.01643.x
6. Rae C, Furlong W, Horsman J, et al. Bleeding Disorders, Menorrhagia and Iron Deficiency: Impacts on Health-related Quality of Life. Haemophilia. 2013;19(3):385–391. doi:10.1111/hae.12014
7. Xu Y, Deforest M, Grabell J, Hopman W, James P. Relative contributions of bleeding scores and iron status on health-related quality of life in von Willebrand disease: a cross-sectional study. Haemophilia. 2017;23(1):115–121. doi:10.1111/hae.13062
8. Roberts JC, Kulkarni R, Kouides PA, et al. Depression and anxiety in persons with von Willebrand disease. Haemophilia. 2023;29(2):545–554. doi:10.1111/hae.14725
9. Barlow JH, Stapley J, Ellard DR, Gilchrist M. Information and self-management needs of people living with bleeding disorders: a survey. Haemophilia. 2007;13(3):264–270. doi:10.1111/j.1365-2516.2007.01444.x
10. Kirtava A, Drews C, Lally C, Dilley A, Evatt B. Medical, reproductive and psychosocial experiences of women diagnosed with von Willebrand’s disease receiving care in haemophilia treatment centres: a case-control study. Haemophilia. 2003;9(3):292–297. doi:10.1046/j.1365-2516.2003.00756.x
11. Sidonio RF, Haley KM, Fallaize D. Impact of diagnosis of von Willebrand disease on patient outcomes: analysis of medical insurance claims data. Haemophilia. 2017;23(5):743–749. doi:10.1111/hae.13292
12. VanderMeulen H, Arya S, Nersesian S, Philbert N, Sholzberg M. What have we learned about the patient’s experience of von Willebrand disease? A focus on women. Hematology Am Soc Hematol Educ Program. 2022;2022(1):631–636. doi:10.1182/hematology.2022000391
13. Atiq F, Saes JL, Punt MC, et al. Major differences in clinical presentation, diagnosis and management of men and women with autosomal inherited bleeding disorders. EClinicalMedicine. 2021;32:100726. doi:10.1016/j.eclinm.2021.100726
14. Hagberg KW, Jick S, Du P, Truong Berthoz F, Özen G, Tzivelekis S. Impact of von Willebrand disease on women’s health outcomes: a matched cohort database study. J Womens Health. 2022;31(9):1262–1270. doi:10.1089/jwh.2022.0082
15. Hagberg KW, Divan HA, Nickel JC, Jick SS. Risk of incident antidepressant-treated depression associated with use of 5α-reductase inhibitors compared with use of α-blockers in men with benign prostatic hyperplasia: a population-based study using the Clinical Practice Research Datalink. Pharmacotherapy. 2017;37(5):517–527. doi:10.1002/phar.1925
16. Hagberg KW, Li L, Peng M, Shah K, Paris M, Jick S. Incidence rates of suicidal behaviors and treated depression in patients with and without psoriatic arthritis using the Clinical Practice Research Datalink. Mod Rheumatol. 2016;26(5):774–779. doi:10.3109/14397595.2015.1136726
17. Persson R, Lee S, Yood MU, et al. Incident depression in patients diagnosed with multiple sclerosis: a multi-database study. Eur J Neurol. 2020;27(8):1556–1560. doi:10.1111/ene.14314
18. Federici AB, Rand JH, Bucciarelli P, et al. Acquired von Willebrand syndrome: data from an international registry. Thromb Haemost. 2000;84(2):345–349. doi:10.1055/s-0037-1614018
19. Du P, Hagberg KW, Tzivelekis S, Truong Berthoz F, Özen G, Jick S. Impact of von Willebrand disease on mental health outcomes: a matched cohort database study. Haemophilia. 2022;28(Suppl 3):90. doi:10.1111/hae.14537
 © 2023 Takeda. This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 Takeda. This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.