")
Back to Journals » Nursing: Research and Reviews » Volume 13
Postural Orthostatic Tachycardia Syndrome: Diagnosis and Management Guide for Nurses
Authors Seeley MC , Lau DH , Gallagher C
Received 10 April 2023
Accepted for publication 25 October 2023
Published 14 November 2023 Volume 2023:13 Pages 41—49
DOI https://doi.org/10.2147/NRR.S394822
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Pariya Fazeli
Marie-Claire Seeley,1,2 Dennis H Lau,1– 3 Celine Gallagher1,2
1Australian Dysautonomia and Arrhythmia Research Collaborative, University of Adelaide, Adelaide, South Australia, Australia; 2South Australian Health and Medical Research Institute, Adelaide, South Australia, Australia; 3Department of Cardiology, Royal Adelaide Hospital, Adelaide, South Australia, Australia
Correspondence: Celine Gallagher, Department of Cardiology, Royal Adelaide Hospital, Port Road, Adelaide, South Australia, 5000, Australia, Tel +61 8 8317 5300, Fax +61 8 8317 5190, Email [email protected]
Abstract: Postural Orthostatic Tachycardia Syndrome (POTS) is a heterogeneous condition where sufferers often present with a variety of orthostatic and non-orthostatic symptomatology. The condition can result in significant functional limitations and reduced quality of life. Diagnosis is based upon patient history in combination with a simple test such as an Active Stand Test. Treatment is both pharmacologically and non-pharmacologically based, with most interventions demonstrating only modest efficacy. There is an urgent need for further research to enhance understanding of aetiology, diagnosis and treatment of this condition. Nurses are well placed to care for patients presenting with symptoms consistent with POTS, to undertake or recommend testing to facilitate diagnosis and to provide education and support as part of a multidisciplinary team to improve patient outcomes.
Keywords: dysautonomia, treatment, quality of life, Post Acute Sequelae of Covid
Introduction
Postural Orthostatic Tachycardia Syndrome (POTS) is a complex and challenging condition, characterised by a sustained orthostatic heart rate elevation, resulting from underlying dysfunction of the autonomic nervous system. Whilst orthostatic symptoms are a prerequisite for diagnosis (eg dizziness, lightheadedness, pre-syncope, palpitations), there is frequently a plethora of non-orthostatic symptoms (eg fatigue, gastrointestinal symptoms, thermoregulatory disturbance, cognitive dysfunction) that accompany this condition. Health related quality of life is known to be poor in this population and many are unable to work due to functional disability arising from their symptoms.1,2 The condition primarily affects females from adolescence onwards, although it can affect both sexes of any age. Although the aetiology of POTS is not well understood, the condition can be triggered by several mechanisms, including post viral infections, and much of Long Covid, or Post Acute Sequelae of Covid-19 (PASC), is thought to be due to autonomic nervous system dysfunction.3–6 The long-term trajectory is largely unknown due to a distinct lack of research in this area. As with many other acute and chronic conditions, involvement of nurses at each stage of care delivery is likely to be associated with improved patient outcomes, enhanced cost effectiveness and patient satisfaction.7–11 As such, it is critical that nurses are upskilled in the diagnosis and management of those living with this condition. In this review, we will cover presenting symptoms, diagnosis and treatment options (non-pharmacological and pharmacological) and highlight the role of nurses in POTS diagnosis, treatment and management of this condition.
Background
Dysautonomia is an umbrella term for conditions arising from dysfunction of the autonomic nervous system. These conditions include orthostatic hypotension,12 neurocardiogenic syncope,13 POTS, multiple system atrophy14 and pure autonomic failure.15 POTS is the most common type of dysautonomia. The condition was first described in a 1993 publication, although there are earlier reports of similar clinical features and presentations, including reports from 1871 where the condition was reported as “irritable heart syndrome”.16 The exact prevalence of POTS is unknown, although it has been estimated to affect approximately 0.1–1% of the US population, with data from other countries currently lacking.17 Some of the challenges of determining prevalence arise from the lack of an International Classification of Disease (ICD) code for this condition, although this has recently been introduced in the USA with other countries expected to follow. However, the main diagnostic challenge relates to a lack of recognition or misdiagnosis of this condition by healthcare professionals.18 The condition has a clear female preponderance of approximately 4–5 females to 1 male.17 Common comorbidities seen in this population include joint hypermobility (Hypermobility Spectrum Disorder or hypermobile Ehlers Danlos Syndrome), mast cell activation syndrome (MCAS), migraine, autoimmune conditions, myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) and fibromyalgia.19 Much interest in the underlying pathophysiology linking POTS, joint hypermobility and MCAS has been demonstrated, given the frequent co-existence of such conditions, however this requires further research.20–22 Similarly a high preponderance of joint hypermobility, POTS and functional gastrointestinal disorders has also been demonstrated.23
Presenting Symptoms
In a large online survey of a POTS population (n=4835), approximately half of all individuals surveyed reported symptom onset during adolescence and 94% were female. Light headedness, tachycardia and pre-syncope were the most commonly reported symptoms (99%, 97% and 94% of respondents respectively), however it is notable that headache and difficulty concentrating was reported in 94% of the population and it was common for participants to report the presence of all five symptoms (83%).24 Presenting symptoms of orthostatic intolerance may include dizziness, light-headedness, brain fog, pre-syncope, chest pain or discomfort, headache, nausea, visual disturbances, fatigue and tremulousness.25 POTS cannot be diagnosed without the presence of such symptoms. Dependent acrocyanosis, in which the feet or hands discolour or appear mottled with prolonged upright posture, may be self-reported or observed during an Active Stand Test or Head Up Tilt Table Test. A plethora of non-orthostatic symptoms frequently co-exist including cognitive26 and bladder issues,27 gastrointestinal symptoms,28 thermoregulatory and sleep disturbances29 (see Box 1). These are likely related to the underlying dysfunction of the autonomic nervous system and further research is required to better understand many of these associations and determine optimal treatment options. Although psychological symptoms are commonly reported in those with POTS, the heart rate response to orthostatic stress has been shown to not relate to anxiety but rather a pathophysiological process.30
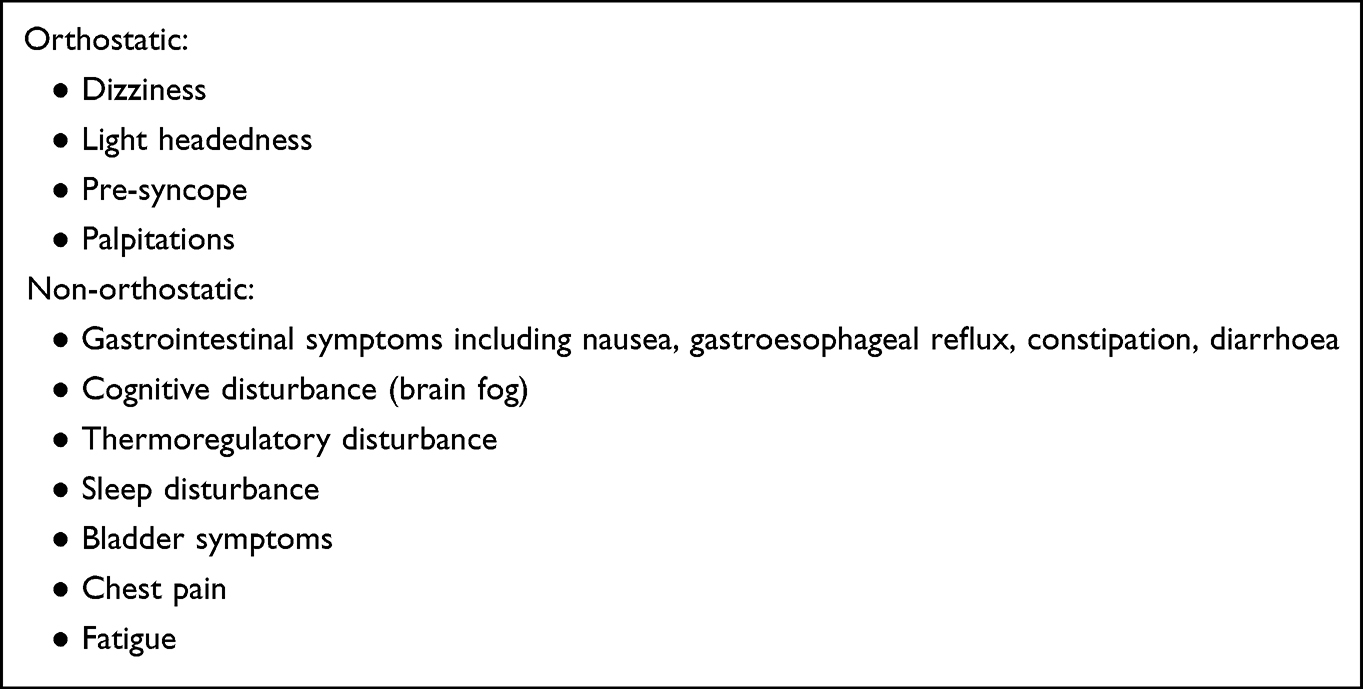 |
Box 1 Frequent Orthostatic and Non-Orthostatic Symptoms in POTS |
The economic impact of the condition is significant. In a large survey of 5556 adults with POTS, more than 70% had lost income as a direct result of their condition and 21% reported losing a job.1 Health related quality of life is poor compared to normative populations, with recently published data in an age and sex matched population (202 individuals in each cohort) demonstrating a higher burden of impairment across all domains of a commonly used health related quality of life measure (EQ-5D-5L) in those with POTS compared to a control population and an overall quality of life poorer than that of other common chronic conditions including chronic kidney disease, cardiovascular disease and diabetes.31 Importantly, the reduced quality of life was observed across all age groups. This was similarly demonstrated in a prior survey comparing several psychosocial factors in a POTS population (n=624) to a control population (n=139) demonstrating poorer physical health, greater activity limitations, increased fatigue and poor sleep, greater pain levels and a significantly greater suicide risk.2 Poor sleep is common in this population, and has been linked to increased suicidal ideation.32
Pathophysiology and Prognosis
The onset of POTS has a clear trigger in some individuals, often occurring post virally, at times of significant hormonal change (eg, menarche, pregnancy), post surgery or vaccination, or following a trauma or concussion. In others, onset is more insidious with a gradual increase in symptoms over time.17 Several underpinning pathogenic mechanisms have been proposed including autoimmunity.19 This has evolved following the observation that POTS is frequently triggered following immune system activation, in addition to an observed higher incidence of autoimmune conditions in POTS populations compared to controls.33 A retrospective chart review of 100 patients with confirmed POTS demonstrated that 20% had a confirmed autoimmune condition, with an expected prevalence of such conditions at 5–8% of the general population.34 Biopsy confirmed coeliac disease is higher in POTS populations compared to controls (4% vs 1%) in addition to self-reported gluten sensitivity via questionnaire (42% vs 19%).35 Whilst several autoimmune antibodies have been found in POTS, the relevance of this is, at this stage, unclear as commercially available assays may not be able to adequately discriminate activation of such autoantibodies.36
Although POTS has been categorised into various sub-types, eg, hypovolaemiac, neuropathic or hyperadrenergic, there is significant crossover and more than one subtype can exist in an individual.37 However, this sub-categorisation may be somewhat useful in relation to determining effective treatment modalities. Examples include the neuropathic subtype in which dependent acrocyanosis, or blood pooling, is frequently observed which may direct treatment towards amelioration of this. Several studies have demonstrated lower total blood volume in patients with POTS, with one well controlled study revealing an overall 13% deficit in blood volume consistent with a moderate to severe hypovolaemic state.38 Dysfunction of the renin angiotensin aldosterone system response to hypovolaemia may further exacerbate the situation.38 Finally, hyperadrenergic POTS is characterised by elevated plasma norepinephrine levels in upright positions.39 However, clinically it can be challenging to differentiate subtypes due to frequent overlap in clinical presentations, and difficulty in undertaking the clinical tests required for categorisation.
POTS is a fluctuating condition with individuals often reporting ‘flares’ interspersed with periods of relatively well controlled symptoms. Misdiagnosis frequently occurs, resulting in significant diagnostic delay, with an average time to diagnosis of almost 5 years.24 This reported delay is greater in females compared to males (5.0±7.2 years vs 3.0±4.4 years in females vs males respectively).24 The trajectory of the condition is unclear with lack of robust long-term follow-up data. However, in a cohort of adolescents diagnosed with the condition, most reported improvement, but not remission of symptoms over 5 years of follow up.40
POTS and Long Covid
Given the unprecedented nature of the coronavirus pandemic, there is increased attention on the entity of Long Covid or Post Acute Sequelae of Covid-19 (PASC) whereby a significant proportion of individuals with Long Covid has been found to have POTS. However, it should be noted that post viral syndromes, including POTS, other types of autonomic dysfunction and myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS) are not new and have been extensively described in the literature. Long Covid is a poorly discriminated post viral condition that is thought to affect at least 10% of individuals post Covid infection.41 An early Long Covid systematic review incorporating 47,910 patients demonstrated that 80% of those post infection developed persistant long term symptoms with fatigue and headache most commonly reported (58% and 44% respectively).42 The condition can result in significant disability, with a recent umbrella review demonstrating that at least 50% of individuals will suffer with extended periods of time away from work, altered workloads or loss of employment.43 Hence it is imperative from a public health and societal perspective to have greater understanding of this condition. Whilst our understanding of this condition is rapidly evolving, much of what is reported in the literature bears remarkable similarity to dysautonomia and specifically POTS. Several studies have confirmed a high prevalence of dysautonomia in PASC populations, yet it is often not routinely screened for in clinical practice. It has recently been demonstrated in a cohort of 99 individuals (n=33 with PASC, n=33 with POTS and n=33 control) that 79% of the PASC cohort, with unexplained symptoms that persist for longer than 3 months post their acute Covid infection, met criteria for POTS.5 A retrospective case review of 20 patients presenting with persistent neurological and cardiovascular symptoms post Covid infection demonstrated that 75% met criteria for POTS.4 Several case reports have also highlighted the development of POTS post Covid.44,45 Case series have subsequently published demonstrating the high prevalence of POTS in PASC.46,47 Another study demonstrated a high burden of autonomic dysfunction in patients referred to a Long Covid rehabilitation service. Whilst a high burden of symptoms of orthostatic intolerance was demonstrated this did not demonstrate strong correlation to heart rate changes observed on an Active Stand Test.48 This study highlights the limitation of over reliance on one test and stringent heart rate criteria for a POTS diagnosis, given that heart rate responses fluctuate and exhibit diurnal variations which is not accounted for in many studies.49 The plethora of published studies to date have resulted in a statement released from the American Autonomic Society on Long Covid, calling for greater research and clinical investment to rapidly identify ways in which this condition can be better diagnosed and treated to minimise the often debilitating functional disability in this population.50 Nurses are well placed in primary care or acute care settings to be vigilant to individuals presenting with symptoms of autonomic dysfunction in order to recommend appropriate autonomic diagnostic testing and management, following exclusion of other conditions known to be associated with post Covid complications.
Diagnosis
The diagnosis of POTS is based upon symptomatology, in addition to heart rate and blood pressure variations observed with standing. It is generally agreed that symptoms should be present for at least 3 months before POTS can be confirmed and in the absence of medications (sympathomimetics and anticholinergic agents) or conditions that could contribute to orthostatic tachycardia such as anaemia, dehydration, fever, pain, anorexia nervosa, hyperventilation, severe deconditioning, hyperthyroidism and phaeochromocytoma.25 A 10-minute Active Stand Test can be easily performed in most clinical settings. The participant should lay supine for 5–10 minutes before a 10 minute stand, in which the individual is requested to lean against a wall to minimise movement, to determine change in heart rate and blood pressure. A positive result, meeting criteria for POTS, is a sustained heart rate rise of ≥30 beats per minute in adults and ≥40 beats per minute in those aged 12–19 years and in the absence of orthostatic hypotension (drop in systolic blood pressure of >20 mmHg within 3 minutes of standing).25 An absolute heart rate of ≥120 beats per minute is also diagnostic.51 It should be noted that the heart rate criteria have been disputed, particularly in adolescents, when a high clinical suspicion exists.52 Diurnal variations in heart rate responses to orthostatic stress have been observed in this population and therefore testing is better performed in the morning.53 Questionnaires can also be useful in assisting with diagnosis and monitoring the effect of interventions. The newly developed Malmo POTS questionnaire quantifies the effect of commonly reported POTS symptoms with scores >42 demonstrating excellent sensitivity and specificity for a POTS diagnosis.54 A list of commonly reported symptoms are included in this questionnaire such as dizziness whilst standing, chest pain, palpitations, headache and fatigue, which are rated by respondents on a scale from 0–10. The Compass Autonomic Symptom Score (COMPASS-31) is a 31-item questionnaire providing information on broad symptoms of autonomic dysfunction, with scores >20 indicative of moderate autonomic symptom burden.55 The COMPASS-31 questionnaire quantifies autonomic symptom burden in six domains including orthostatic intolerance, vasomotor, secretomotor, gastrointestinal, bladder and pupillomotor function. Respondents are asked to quantify the extent to which symptoms are experienced under each domain, with higher scores representing worse autonomic symptom burden.
Given the fluctuating nature of the condition, a negative Active Stand Test does not conclusively exclude a POTS diagnosis. For those who do not meet the heart rate criteria consistent with a POTS diagnosis, the Canadian Consensus Statement has labelled this population as Postural Symptoms without Tachycardia (PSWT), acknowledging that a high index of clinical suspicion exists and criteria for POTS may be met at a future time point.56 Indeed, the presence of extra-cardiac autonomic symptoms should prompt the clinician to maintain a high index of suspicion. Dependent acrocyanosis in which the feet or hands discolour or appear mottled with prolonged upright posture observed during an Active Stand Test is commonly observed in this population. Baseline blood tests such as full blood count, serum electrolytes, iron studies and thyroid function tests should be considered and prompt investigation into abnormalities that may contribute to symptomatology or warrant investigation for other conditions. A Head Up Tilt Table Test can be considered if it is deemed unsafe to perform the Active Stand Test or if the patient is unable to stand but is not required for diagnosis.25 Indeed, there have been active calls to abolish tilt table testing in favour of the active standing test wherever possible due to similar sensitivity but increased specificity, increased ability to detect other conditions including early or late orthostatic hypotension and enhanced reproducibility of presenting symptoms.57
Treatment
Management of POTS is largely directed at managing or alleviating symptoms in the absence of curative treatments. However, most interventions have demonstrated modest efficacy with further research urgently required to guide clinical management.58 Initial recommendations should focus on lifestyle modification to improve and support blood volume and include fluid loading, high salt diet, use of compression wear, a graded recumbent exercise programme in those in which this can be tolerated, and avoidance of triggers. Common triggers to avoid include hot, humid environments, hot showers, scenarios requiring prolonged standing still, excessive alcohol, tea, coffee or energy drinks. Fluid loading can be achieved by recommending consumption of 2–3 litres per day, with recommendations up to 4 litres prescribed.56 The majority of this should come from water, although electrolyte drinks are frequently utilised in this population. Oral rehydration solutions have demonstrated efficacy at both improving symptoms of orthostatic intolerance and improving cerebral blood flow in a paediatric population.59 However, care should be taken with use of such products on a regular basis due to their high sugar and/or artificial sweetener content and intake should be kept to as minimal as possible to improve symptoms. Fluid loading without the addition of extra salt loading is of little benefit and, in the absence of contradiction, a high salt diet should be recommended. The equivalent of 10 grams of salt per day should be consumed and can often be met by increasing intake of high salt foods and adding salt to meals.56 If this is unable to be tolerated, salt tablets may be used, although a worsening of gastrointestinal symptoms should be monitored for due to the acute increase in osmotic load.39 Compression garments may assist in supporting blood flow with upright posture, with one study demonstrating improved stroke volume on head up tilt table testing with both full (abdominal and full leg) and abdominal only compression.60 Cardiovascular exercise is helpful in managing this condition but often requires commencement of recumbent activity before more upright activity is tolerated.61 In a small before and after study, six months of unsupervised home exercise training was demonstrated to enhance quality of life, reduce supine and standing heart rates and reduce the frequency of syncope.62 However, this study is limited by a large dropout rate and inability to complete the prescribed regime raising uncertainty about exercise recommendations to the broader POTS population. Care should be taken to avoid post exertional malaise, where symptoms become acutely exacerbated within 24 hours of exercise and typically result in a “crash and burn” scenario. See Figure 1 for a schematic representation of lifestyle recommendations to manage POTS symptoms.
 |
Figure 1 Lifestyle interventions for POTS symptom management. |
Given the often-similar presentations between POTS and Myalgic Encephalomyelitis/Chronic Fatigue Syndrome (ME/CFS), this condition should be screened for in those whose symptoms have persisted beyond six months. In the ME/CFS population, specialist exercise physiology is recommended as symptoms are typically worsened by cardiovascular exercise. In the clinical setting a quick tool to assist with screening for this condition can be found in the Canadian Consensus Statement Criteria, although several such tools exist.63 Specialist exercise physiology is often recommended in the POTS population to monitor graduation from recumbent to upright exercise over time. Input from other members of the allied health team, including dieticians and occupational therapists, can also be extremely helpful. Pharmacotherapy is often warranted to manage symptom burden in this population, although it should be noted that many commonly used medications do not have established safety profiles for use in pregnancy and need to be managed under specialist care. Whilst a wide array of medications may be utilised, largely dependent on predominant symptoms, initial therapy is often targeted at blood pressure support through agents such as midodrine and fludrocortisone.25,56 Tachycardia may require management with agents including ivabradine and beta blockers such as propranolol, although caution needs to be taken to ensure this does not cause excessive hypotension.56 Hyperadrenergic responses may require use of clonidine or methyldopa.56 Use of medications will depend on local availability and patient preference. Often, withdrawal of these medications is necessary when planning pregnancy.
The Role of Nurses
Nurses play a key role in the diagnosis, management and treatment of POTS. As in other chronic and complex conditions including heart failure, atrial fibrillation and diabetes, a multidisciplinary team approach has been shown to improve patient outcomes and enhance cost effectiveness.10,64–68 The patient presenting with POTS symptoms is often young, complex and comorbid. Consultations generally take longer periods of time due to this, making the use of sole physician management difficult due to time and cost inefficiencies. It is necessary for a broad spectrum of testing to be performed, including autonomic and assessing for common comorbidities including joint hypermobility. Due to high symptom burden, regular follow ups are often necessitated to provide re-enforcement and incorporate support of other allied healthcare professionals to assist with patient management. Nurses can also be alert to when a trial of pharmacotherapy may be warranted and can similarly assist in determining the response to such therapy. As care co-ordinators, nurses can deliver and co-ordinate the many different facets of care required including assessment, education, self-monitoring and management and psychosocial support (see Figure 2). In those who are functionally disabled by their condition, provision of advice and support on applying for local disability support for income and services can come under nurse jurisdiction, although this is currently difficult due to poor recognition of the condition. Although specialist autonomic centres are not widely available, nurses have capability in such centres to undertake patient assessment, autonomic testing, education and ongoing management. In some countries, specialist nurse practitioner roles would also facilitate prescription of pharmacotherapy to manage symptom burden and improve functionality.
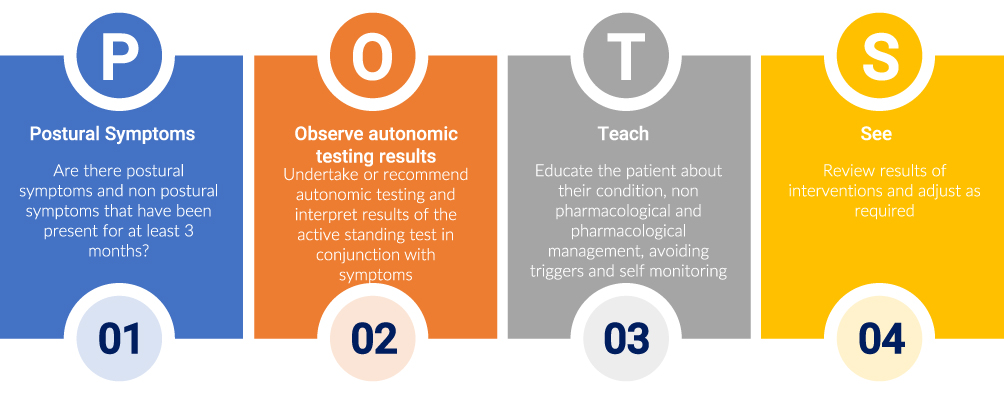 |
Figure 2 Suggested role for nurses in POTS diagnosis and management. |
Future Directions
Despite the integral role autonomic nurse specialists could have there has been a lack of research to evaluate the impact of multidisciplinary models of care on patient outcomes in this population and this remains an area of unmet need. There is a broad lack of awareness of dysautonomias, as this is frequently not taught in depth in undergraduate nursing, medical or allied health degrees. There are currently no specialist centres for nurses to train or upskill in the diagnosis and management of such conditions, further compounding the lack of specialists in this field. The coronavirus pandemic has raised awareness of dysautonomias and may assist in provision of nurse upskilling given that healthcare systems are struggling with the increase in patient loads arising from acute and Long Covid. Moving forward, specialised autonomic centres and recognition of autonomic dysfunction as a unique field will support development of specialist nurse’s role to provide comprehensive care delivery to the POTS and the broader dysautonomia population.
Conclusions
POTS is a complex clinical condition and nurses are integral to deliver comprehensive care to this population, from assessment to diagnosis and ongoing management. There is a current lack of evidence to base care delivery on and a broad lack of awareness of the condition which is frequently not taught in undergraduate health degrees. The development of specialist autonomic nursing roles, and specialised autonomic centres, should be undertaken as a matter of urgent priority to facilitate equitable access to diagnosis and treatment and ongoing chronic condition management to facilitate earlier diagnosis, reduce symptom burden, enhance self-management and improve functionality and quality of life in this population.
Disclosure
Ms Seeley is supported by an Australian Government Research Scholarship. Dr Lau reports that the University of Adelaide has received on his behalf lecture and/or consulting fees from Abbott Medical, Biotronik, Medtronic and MicroPort CRM. Dr Gallagher is supported by a postdoctoral research fellowship from the Australian POTS Foundation and an Emerging Leader grant from the University of Adelaide. The author reports no other conflicts of interest in this work.
References
1. Bourne KM, Chew DS, Stiles LE, et al. Postural orthostatic tachycardia syndrome is associated with significant employment and economic loss. J Intern Med. 2021;290(1):203–212. doi:10.1111/joim.13245
2. Pederson CL, Brook JB. Health-related quality of life and suicide risk in postural tachycardia syndrome. Clin Auton Res. 2017;27(2):75–81. doi:10.1007/s10286-017-0399-5
3. Ormiston CK, Świątkiewicz I, Taub PR. Postural orthostatic tachycardia syndrome as a sequela of COVID-19. Heart Rhythm. 2022;19(11):1880–1889. doi:10.1016/j.hrthm.2022.07.014
4. Blitshteyn S, Whitelaw S. Postural orthostatic tachycardia syndrome (POTS) and other autonomic disorders after COVID-19 infection: a case series of 20 patients. Immunol Res. 2021;69(2):205–211. doi:10.1007/s12026-021-09185-5
5. Seeley MC, Gallagher C, Ong E, et al. High incidence of autonomic dysfunction and postural orthostatic tachycardia syndrome in patients with long COVID: implications for management and health care planning. Am J Med. 2023. doi:10.1016/j.amjmed.2023.06.010
6. Larsen NW, Stiles LE, Shaik R, et al. Characterization of autonomic symptom burden in long COVID: a global survey of 2314 adults. Front Neurol. 2022;13:1012668. doi:10.3389/fneur.2022.1012668
7. Woo BFY, Lee JXY, Tam WWS. The impact of the advanced practice nursing role on quality of care, clinical outcomes, patient satisfaction, and cost in the emergency and critical care settings: a systematic review. Hum Resour Health. 2017;15(1):63. doi:10.1186/s12960-017-0237-9
8. Ordóñez-Piedra J, Ponce-Blandón JA, Robles-Romero JM, Gómez-Salgado J, Jiménez-Picón N, Romero-Martín M. Effectiveness of the advanced practice nursing interventions in the patient with heart failure: a systematic review. Nurs Open. 2021;8(4):1879–1891. doi:10.1002/nop2.847
9. Hendriks JM, de Wit R, Crijns HJ, et al. Nurse-led care vs. usual care for patients with atrial fibrillation: results of a randomized trial of integrated chronic care vs. routine clinical care in ambulatory patients with atrial fibrillation. Eur Heart J. 2012;33(21):2692–2699. doi:10.1093/eurheartj/ehs071
10. Azami G, Soh KL, Sazlina SG, et al. Effect of a nurse-led diabetes self-management education program on glycosylated hemoglobin among adults with type 2 diabetes. J Diabetes Res. 2018;2018:4930157. doi:10.1155/2018/4930157
11. Laurant M, van der Biezen M, Wijers N, et al. Nurses as substitutes for doctors in primary care. Cochrane Database Syst Rev. 2018;7(7):Cd001271.
12. Freeman R, Wieling W, Axelrod FB, et al. Consensus statement on the definition of orthostatic hypotension, neurally mediated syncope and the postural tachycardia syndrome. Clin Auton Res. 2011;21(2):69–72. doi:10.1007/s10286-011-0119-5
13. Hawkins NM, Krahn AD. Does any therapy really work for neurocardiogenic syncope? Cardiol J. 2014;21(6):616–624. doi:10.5603/CJ.2014.0094
14. Fanciulli A, Wenning GK, Longo DL. Multiple-system atrophy. N Engl J Med. 2015;372(3):249–263. doi:10.1056/NEJMra1311488
15. Coon EA, Singer W, Low PA. Pure Autonomic Failure. Mayo Clin Proc. 2019;94(10):2087–2098. doi:10.1016/j.mayocp.2019.03.009
16. Schondorf R, Low PA. Idiopathic postural orthostatic tachycardia syndrome. Neurology. 1993;43(1 Part 1):132. doi:10.1212/WNL.43.1_Part_1.132
17. Arnold AC, Ng J, Raj SR. Postural tachycardia syndrome - Diagnosis, physiology, and prognosis. Auton Neurosci. 2018;215:3–11. doi:10.1016/j.autneu.2018.02.005
18. Sebastian SA, Co EL, Panthangi V, et al. Postural Orthostatic Tachycardia Syndrome (POTS): an update for clinical practice. Curr Probl Cardiol. 2022;47(12):101384. doi:10.1016/j.cpcardiol.2022.101384
19. Vernino S, Bourne KM, Stiles LE, et al. Postural orthostatic tachycardia syndrome (POTS): state of the science and clinical care from a 2019 national institutes of health expert consensus meeting - part 1. Auton Neurosci. 2021;235:102828. doi:10.1016/j.autneu.2021.102828
20. Bonamichi-Santos R, Yoshimi-Kanamori K, Giavina-Bianchi P, Aun MV. Association of postural tachycardia syndrome and Ehlers-Danlos syndrome with mast cell activation disorders. Immunol Allergy Clin North Am. 2018;38(3):497–504. doi:10.1016/j.iac.2018.04.004
21. Wang E, Ganti T, Vaou E, Hohler A. The relationship between mast cell activation syndrome, postural tachycardia syndrome, and Ehlers-Danlos syndrome. Allergy Asthma Proc. 2021;42(3):243–246. doi:10.2500/aap.2021.42.210022
22. Miller AJ, Stiles LE, Sheehan T, et al. Prevalence of hypermobile Ehlers-Danlos syndrome in postural orthostatic tachycardia syndrome. Auton Neurosci. 2020;224:102637. doi:10.1016/j.autneu.2020.102637
23. Tai FWD, Palsson OS, Lam CY, et al. Functional gastrointestinal disorders are increased in joint hypermobility-related disorders with concomitant postural orthostatic tachycardia syndrome. Neurogastroenterol Motil. 2020;32(12):e13975. doi:10.1111/nmo.13975
24. Shaw BH, Stiles LE, Bourne K, et al. The face of postural tachycardia syndrome - insights from a large cross-sectional online community-based survey. J Intern Med. 2019;286(4):438–448. doi:10.1111/joim.12895
25. Sheldon RS, Grubb BP, Olshansky B, et al. 2015 heart rhythm society expert consensus statement on the diagnosis and treatment of postural tachycardia syndrome, inappropriate sinus tachycardia, and vasovagal syncope. Heart Rhythm. 2015;12(6):e41–63. doi:10.1016/j.hrthm.2015.03.029
26. Wells R, Malik V, Brooks AG, et al. Cerebral blood flow and cognitive performance in postural tachycardia syndrome: insights from sustained cognitive stress test. J Am Heart Assoc. 2020;9(24):e017861. doi:10.1161/JAHA.120.017861
27. Kaufman MR, Chang-Kit L, Raj SR, et al. Overactive bladder and autonomic dysfunction: lower urinary tract symptoms in females with postural tachycardia syndrome. Neurourol Urodyn. 2017;36(3):610–613. doi:10.1002/nau.22971
28. Tu Y, Abell TL, Raj SR, Mar PL. Mechanisms and management of gastrointestinal symptoms in postural orthostatic tachycardia syndrome. Neurogastroenterol Motil. 2020;32(12):e14031. doi:10.1111/nmo.14031
29. Miglis MG, Muppidi S, Feakins C, Fong L, Prieto T, Jaradeh S. Sleep disorders in patients with postural tachycardia syndrome. Clin Auton Res. 2016;26(1):67–73. doi:10.1007/s10286-015-0331-9
30. Masuki S, Eisenach JH, Johnson CP, et al. Excessive heart rate response to orthostatic stress in postural tachycardia syndrome is not caused by anxiety. J Appl Physiol. 2007;102(3):896–903. doi:10.1152/japplphysiol.00927.2006
31. Seeley MC, Gallagher C, Ong E, et al. Poor health-related quality of life in postural orthostatic tachycardia syndrome in comparison with a sex- and age-matched normative population. Clin Auton Res. 2023;33(4):469–477. doi:10.1007/s10286-023-00955-9
32. Pederson CL, Blettner Brook J. Sleep disturbance linked to suicidal ideation in postural orthostatic tachycardia syndrome. Nat Sci Sleep. 2017;9:109–115. doi:10.2147/NSS.S128513
33. Vernino S, Stiles LE. Autoimmunity in postural orthostatic tachycardia syndrome: current understanding. Auton Neurosci. 2018;215:78–82. doi:10.1016/j.autneu.2018.04.005
34. Blitshteyn S. Autoimmune markers and autoimmune disorders in patients with postural tachycardia syndrome (POTS). Lupus. 2015;24(13):1364–1369. doi:10.1177/0961203315587566
35. Penny HA, Aziz I, Ferrar M, et al. Is there a relationship between gluten sensitivity and postural tachycardia syndrome? Eur J Gastroenterol Hepatol. 2016;28(12):1383–1387. doi:10.1097/MEG.0000000000000740
36. Hall J, Bourne KM, Vernino S, et al. Detection of G protein-coupled receptor autoantibodies in postural orthostatic tachycardia syndrome using standard methodology. Circulation. 2022;146(8):613–622. doi:10.1161/CIRCULATIONAHA.122.059971
37. Kichloo A, Aljadah M, Grubb B, Kanjwal K. Management of postural orthostatic tachycardia syndrome in the absence of randomized controlled trials. J Innov Card Rhythm Manag. 2021;12(7):4607–4612. doi:10.19102/icrm.2021.120705
38. Raj SR, Biaggioni I, Yamhure PC, et al. Renin-aldosterone paradox and perturbed blood volume regulation underlying postural tachycardia syndrome. Circulation. 2005;111(13):1574–1582. doi:10.1161/01.CIR.0000160356.97313.5D
39. Mar PL, Raj SR. Postural orthostatic tachycardia syndrome: mechanisms and new therapies. Annu Rev Med. 2020;71(1):235–248. doi:10.1146/annurev-med-041818-011630
40. Bhatia R, Kizilbash SJ, Ahrens SP, et al. Outcomes of adolescent-onset postural orthostatic tachycardia syndrome. J Pediatr. 2016;173:149–153. doi:10.1016/j.jpeds.2016.02.035
41. Davis HE, McCorkell L, Vogel JM, Topol EJ. Long COVID: major findings, mechanisms and recommendations. Nat Rev Microbiol. 2023;21(3):133–146. doi:10.1038/s41579-022-00846-2
42. Lopez-Leon S, Wegman-Ostrosky T, Perelman C, et al. More than 50 long-term effects of COVID-19: a systematic review and meta-analysis. Sci Rep. 2021;11(1):16144. doi:10.1038/s41598-021-95565-8
43. Nittas V, Gao M, West EA, et al. Long COVID through a public health lens: an umbrella review. Public Health Rev. 2022;43:1604501. doi:10.3389/phrs.2022.1604501
44. Kanjwal K, Jamal S, Kichloo A, Grubb BP. New-onset postural orthostatic tachycardia syndrome following coronavirus disease 2019 infection. J Innov Card Rhythm Manag. 2020;11(11):4302–4304. doi:10.19102/icrm.2020.111102
45. Miglis MG, Prieto T, Shaik R, Muppidi S, Sinn DI, Jaradeh S. A case report of postural tachycardia syndrome after COVID-19. Clin Auton Res. 2020;30(5):449–451. doi:10.1007/s10286-020-00727-9
46. Goodman BP, Khoury JA, Blair JE, Grill MF. COVID-19 Dysautonomia. Front Neurol. 2021;12:624968. doi:10.3389/fneur.2021.624968
47. Johansson M, Ståhlberg M, Runold M, et al. Long-Haul Post-COVID-19 symptoms presenting as a variant of postural orthostatic tachycardia syndrome: the Swedish experience. JACC Case Rep. 2021;3(4):573–580. doi:10.1016/j.jaccas.2021.01.009
48. Isaac RO, Corrado J, Sivan M. Detecting orthostatic intolerance in long COVID in a clinic setting. Int J Environ Res Public Health. 2023;20(10):5804. doi:10.3390/ijerph20105804
49. Cai H, Wang S, Zou R, et al. Diagnostic value of diurnal variability of orthostatic heart rate increment in children and adolescents with POTS. Front Pediatr. 2021;9:644461. doi:10.3389/fped.2021.644461
50. Raj SR, Arnold AC, Barboi A, et al. Long-COVID postural tachycardia syndrome: an American Autonomic Society statement. Clin Auton Res. 2021;31(3):365–368. doi:10.1007/s10286-021-00798-2
51. Stewart JM, Boris JR, Chelimsky G, et al. Pediatric Disorders of Orthostatic Intolerance. Pediatrics. 2018;141(1). doi:10.1542/peds.2017-1673
52. Boris JR, Moak JP. Pediatric postural orthostatic tachycardia syndrome: where we stand. Pediatrics. 2022;150(1). doi:10.1542/peds.2021-054945
53. Raj SR. The Postural Tachycardia Syndrome (POTS): pathophysiology, diagnosis & management. Indian Pacing Electrophysiol J. 2006;6(2):84–99.
54. Spahic JM, Hamrefors V, Johansson M, et al. Malmö POTS symptom score: assessing symptom burden in postural orthostatic tachycardia syndrome. J Intern Med. 2023;293(1):91–99. doi:10.1111/joim.13566
55. Sletten DM, Suarez GA, Low PA, Mandrekar J, Singer W. COMPASS 31: a refined and abbreviated composite autonomic symptom score. Mayo Clin Proc. 2012;87(12):1196–1201. doi:10.1016/j.mayocp.2012.10.013
56. Raj SR, Guzman JC, Harvey P, et al. Canadian cardiovascular society position statement on Postural Orthostatic Tachycardia Syndrome (POTS) and related disorders of chronic orthostatic intolerance. Can J Cardiol. 2020;36(3):357–372. doi:10.1016/j.cjca.2019.12.024
57. Kulkarni N, Mody P, Levine BD. Abolish the tilt table test for the workup of syncope! Circulation. 2020;141(5):335–337. doi:10.1161/CIRCULATIONAHA.119.043259
58. Wells R, Elliott AD, Mahajan R, et al. Efficacy of therapies for postural tachycardia syndrome: a systematic review and meta-analysis. Mayo Clin Proc. 2018;93(8):1043–1053. doi:10.1016/j.mayocp.2018.01.025
59. Medow MS, Guber K, Chokshi S, Terilli C, Visintainer P, Stewart JM. The benefits of oral rehydration on orthostatic intolerance in children with postural tachycardia syndrome. J Pediatr. 2019;214:96–102. doi:10.1016/j.jpeds.2019.07.041
60. Bourne KM, Sheldon RS, Hall J, et al. Compression garment reduces orthostatic tachycardia and symptoms in patients with postural orthostatic tachycardia syndrome. J Am Coll Cardiol. 2021;77(3):285–296. doi:10.1016/j.jacc.2020.11.040
61. Fu Q, Levine BD. Exercise and non-pharmacological treatment of POTS. Auton Neurosci. 2018;215:20–27. doi:10.1016/j.autneu.2018.07.001
62. Gibbons CH, Silva G, Freeman R. Cardiovascular exercise as a treatment of postural orthostatic tachycardia syndrome: a pragmatic treatment trial. Heart Rhythm. 2021;18(8):1361–1368. doi:10.1016/j.hrthm.2021.01.017
63. Conroy KE, Islam MF, Jason LA. Evaluating case diagnostic criteria for myalgic encephalomyelitis/chronic fatigue syndrome (ME/CFS): toward an empirical case definition. Disabil Rehabil. 2023;45(5):840–847. doi:10.1080/09638288.2022.2043462
64. Gallagher C, Elliott AD, Wong CX, et al. Integrated care in atrial fibrillation: a systematic review and meta-analysis. Heart. 2017;103(24):1947–1953. doi:10.1136/heartjnl-2016-310952
65. Hendriks J, Tomini F, van Asselt T, Crijns H, Vrijhoef H. Cost-effectiveness of a specialized atrial fibrillation clinic vs. usual care in patients with atrial fibrillation. Europace. 2013;15(8):1128–1135. doi:10.1093/europace/eut055
66. Son YJ, Choi J, Lee HJ. Effectiveness of nurse-led heart failure self-care education on health outcomes of heart failure patients: a systematic review and meta-analysis. Int J Environ Res Public Health. 2020;17(18):1.
67. Huang Z, Liu T, Chair SY. Effectiveness of nurse-led self-care interventions on self-care behaviors, self-efficacy, depression and illness perceptions in people with heart failure: a systematic review and meta-analysis. Int J Nurs Stud. 2022;132:104255. doi:10.1016/j.ijnurstu.2022.104255
68. Cho MK, Kim MY. Self-management nursing intervention for controlling glucose among diabetes: a systematic review and meta-analysis. Int J Environ Res Public Health. 2021;18(23):12750. doi:10.3390/ijerph182312750
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.