")
Back to Journals » Journal of Blood Medicine » Volume 14
Predictors of Intensive Care Admission Among Adult Patients with Sickle Cell Disease in Eastern Province of Saudi Arabia
Authors Alsalman M , Alsalman Z , Alkhalifa HA , Alfaraj AN, Alkhalifah A , Almulihi Q
Received 17 August 2023
Accepted for publication 21 December 2023
Published 27 December 2023 Volume 2023:14 Pages 671—680
DOI https://doi.org/10.2147/JBM.S435861
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Martin H Bluth
Mortadah Alsalman,1 Zaenb Alsalman,2 Hussain Abduljaleel Alkhalifa,3 Aman N Alfaraj,3 Ali Alkhalifah,4 Qasem Almulihi5
1Department of Medicine, College of Medicine, King Faisal University, Alahsa, Saudi Arabia; 2Department of Family and Community Medicine, College of Medicine, King Faisal University, Alahsa, Saudi Arabia; 3Department of Medicine, King Fahad Specialist Hospital, Dammam, Saudi Arabia; 4Emergency Department, Eastern Health Cluster, Dammam, Saudi Arabia; 5Emergency Department, King Fahad University Hospital, Al Khobar, Saudi Arabia
Correspondence: Zaenb Alsalman, Departments of Family and Community Medicine, College of Medicine, King Faisal University, Po Box 3311, AlAhsa, 36346, Saudi Arabia, Tel +966545611633, Email [email protected]
Purpose: Sickle cell disease (SCD) comprises a complex group of hematologic disorders that are collectively the most common monogenic disorder and are associated with increased risk of intensive care unit admission (ICU). The purpose of this study is to investigate factors that predict admission of adult patients with SCD to the ICU.
Patients and Methods: This was a cross-sectional study that enrolled adult patients with SCD from Saudi Arabia.
Results: A total of 107 patients with SCD, with a median age 31.9± 12.1 years, were evaluated retrospectively. Regarding predictors of ICU admission, patients who indicated a history of blood transfusions were at 8.047-fold higher risk of ICU admission (OR=8.047; 95% CI=2.392– 27.07; p=0.001). Patients who started hydroxyurea were at least 3.071 times more likely to be admitted than those who did not (OR=3.071; 95% CI=1.164– 8.104; p=0.023). We also observed three or more hospitalizations per year to be associated with increased risk of ICU admission (OR=3.393; 95% CI=1.285– 8.960; p=0.014), with those making 3 to 5 visits annually having at least 10.4 times higher risk (OR=10.38; 95% CI=10.098– 98.19; p=0.041) and those with 6 to 10 ER admissions having 18 times higher risk (OR=18.00; 95% CI=2.149– 150.8; p=0.008). Finally, patients with high WBC were predicted to have at least 3.34 times higher risk of ICU admission (OR=3.337; 95% CI=1.131– 9.846; p=0.029).
Conclusion: SCD is a multi-systemic disease associated with increased morbidity and mortality. Recognition of high-risk features in patients helps to eliminate subjectivity in ICU referral decision. Frequent hospitalization and emergency visits, multiple blood transfusions, and elevated white blood cell count were significantly associated with a higher rate of ICU admission despite hydroxyurea usage.
Keywords: sickle cell disease, intensive care unit, hydroxyurea
Introduction
Sickle cell disease (SCD) is a group of inherited red blood cell disorders caused by a mutation in the β-globin gene that results in the polymerization of hemoglobin S (HbS).1 There are different forms of SCD, however the most prevalent and severe form is homozygous HbSS (sickle cell anaemia).1 In Saudi Arabia, SCD affects 0.26% of the population, with another 4.2% having the sickle cell trait. The Eastern province has the highest prevalence, with 1.2% diseased and about 17% having the trait.2
Patients with SCD experience a wide range of clinical symptoms and consequences, such as vaso-occlusive crises, acute chest syndrome, chronic hemolytic anemia, and multiple organ failure. The majority of complications are manageable without need for critical care, but some have life-threatening effects and may require admission to the intensive care unit (ICU).2,3 Currently, a variety of therapeutic options are available including disease-modifying therapies like hydroxyurea and simple or exchange blood transfusions, which can improve quality of life, reduce the complication rate, and possibly prolong survival. However, the only curative option is stem cell transplantation, and its use is limited due to a lack of suitable donors.1,4 Despite these advances in management, the life expectancy of adult SCD patients is approximately twenty years shorter than the general population, with half of the mortality occurring in the ICU.5,6
Several studies have been conducted to determine predictors of ICU outcomes, with the need for renal replacement therapy, advanced age, fewer hospitalizations, and shorter stays in the ICU having all been linked to increased mortality rates in SCD patients.7 In addition, it has been reported that low hemoglobin levels, respiratory distress, and renal failure at the time of ICU admission are significant predictors of a complicated outcome.6 Ultimately, it is believed that reducing the need for ICU admission among SCD patients will lower mortality and unfavorable outcomes. Therefore, the purpose of the current study was to investigate factors that predict admission of adult patients with SCD to the ICU.
Materials and Methods
This was an observational retrospective cohort study conducted in Saudi Arabia’s eastern province, where SCD is more common than in other regions. All homozygous sickle cell patients between the age of 18 and 65, who attended hematology clinics or were admitted to King Fahad Hospital or Prince Saud Bin Jalawi Hospital between June and December 2022 were included in the study.
Participants initially underwent a survey through an interview conducted by a trained team member to collect demographic and clinical characteristics including age, education level, frequency of hospitalization, emergency visits, blood transfusion, previous ICU admission, frequency of ICU admission, cause of ICU admission, using and awareness about hydroxyurea. Hospital’s electronic database was used to collect baseline patient’s laboratory data from the most recent outpatient visit before ICU admission including complete blood count, hemoglobin electrophoresis, lactate dehydrogenase (LDH), and kidney function tests. Of note, using hydroxyurea was considered if patients have been on it for at least 2 months.
The study was approved by King Fahad Hospital’s Ethical Committee (KFHH RCA 33‐42‐2021). Also, the purpose of the study, the use of data, benefits of doing this research, the right to participate, and the confidentiality and anonymity of the data were explained to the participants and informed consent was taken.
Analyses were performed using the Statistical Package for Software Sciences (SPSS) version 26 (IBM Corporation, Armonk, New York). Descriptive statistics were computed and are reported as frequencies and proportions (%) for categorical variables or means and standard deviations for continuous variables. Univariate regression analysis was performed to determine predictors of ICU admission with corresponding odds ratio (OR) and 95% confidence interval (CI). Statistical significance was identified at p<0.05.
Results
A total of 107 patients with sickle cell disease were reviewed. As described in Table 1, more than half (52.3%) were aged 30 years or less, and the majority were female (60.7%). Patients with bachelor’s degrees constituted 40.2% of participants. The proportion with previous blood transfusions was 86.9%, with 30 (28%) who reported having more than 10 blood transfusions throughout their life. Around two-thirds (71%) were aware of hydroxyurea, but less than half (46.7%) had started using it. As regards hospitalizations, 11.2% had more than 10 hospitalizations per year, and 26.2% had that many emergency visits per year. A history of ICU admission was reported by 75.7%, and nearly one-third (31.8%) of participants had 2 to 5 times ICU admission per year. Among those with a previous ICU admission, 21% had received hydroxyurea. Moreover, the most common reason being acute chest syndrome (ACS) (49.4%) (Figure 1). The mean values of leukocyte count, hemoglobin level, and platelet were 10.4, 8.74, and 326, respectively. Other participants’ baseline laboratory parameters are shown in Table 2.
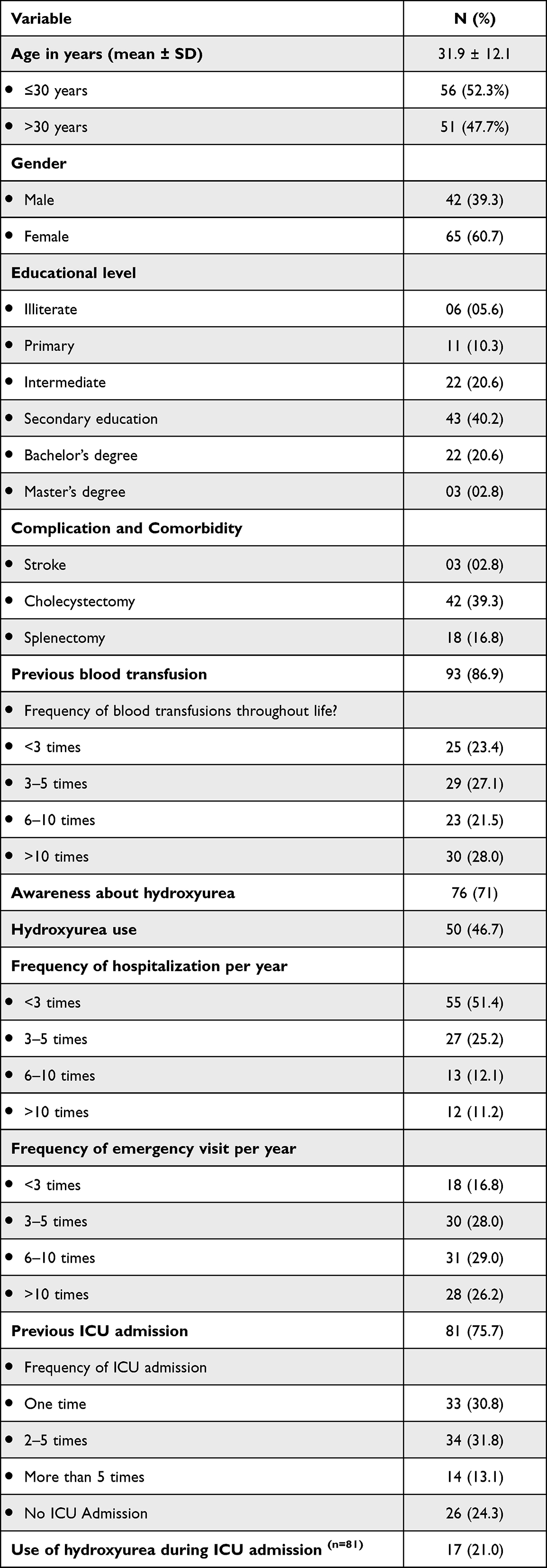 |
Table 1 Demographic and Clinical Characteristics of the Patients (n=107) |
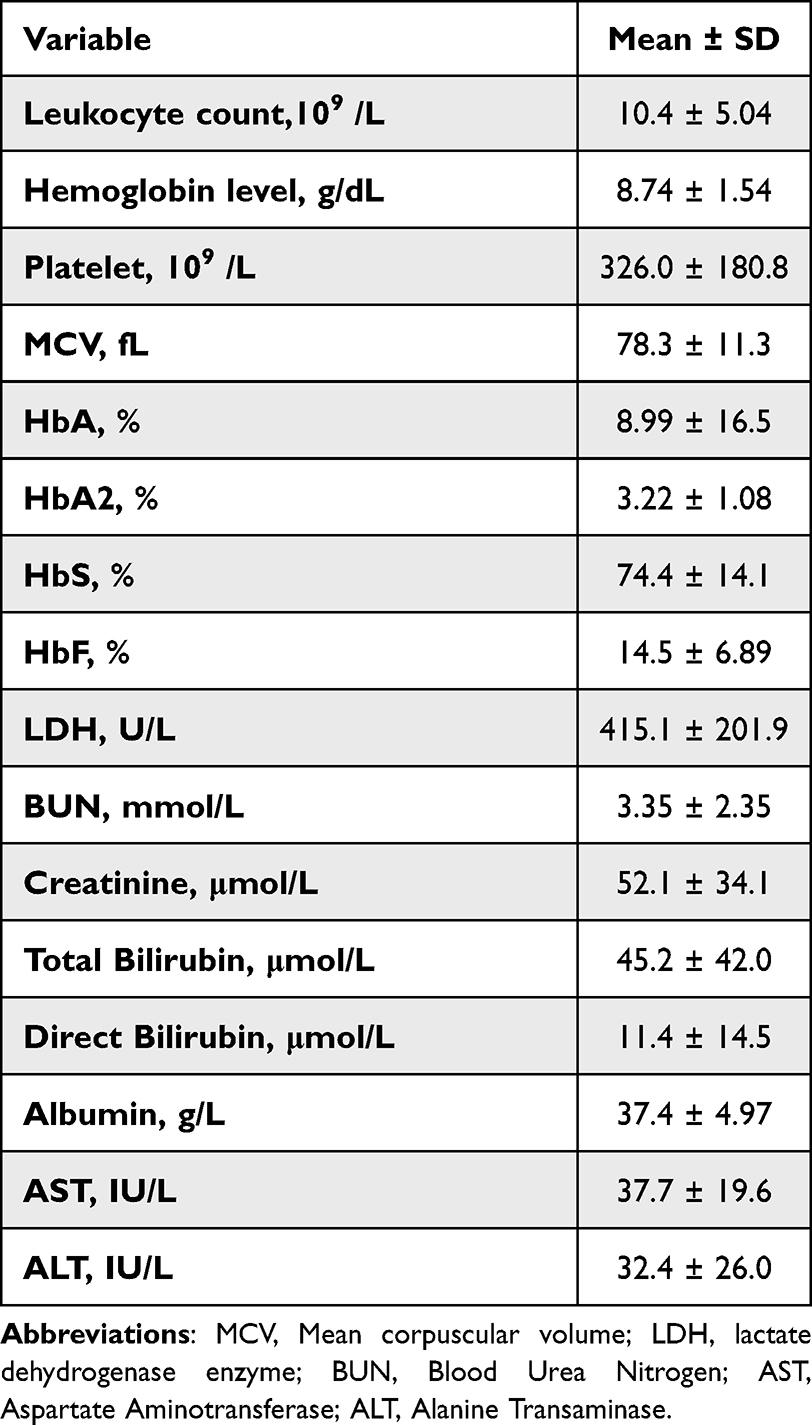 |
Table 2 Baseline Laboratory Data (n=107) |
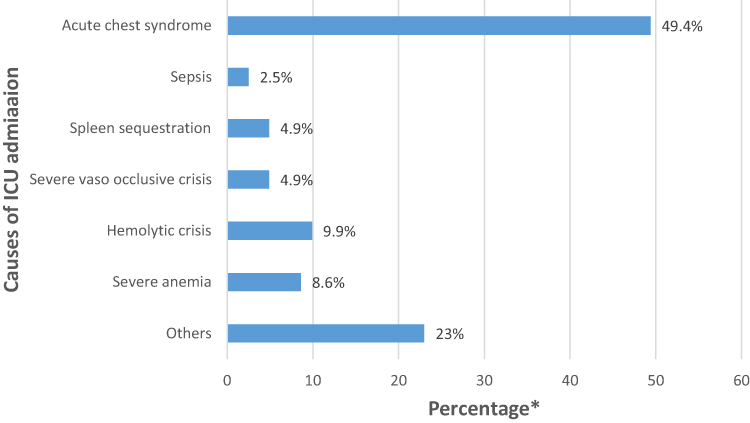 |
Figure 1 Causes of intensive care unit admission for sickle cell patients. Note: *Percentage ≠ 100. |
Regarding predictors of ICU admission, univariate analyses revealed previous blood transfusions, hydroxyurea initiation, frequency of hospitalizations per year, frequency of emergency visits per year, frequency of blood transfusions throughout life, and high WBC to be independent significant predictors of ICU admission. Specifically, compared to patients without a history of blood transfusion, those who indicated a history of blood transfusions were at 8.047-fold higher risk of ICU admission (OR=8.047; 95% CI=2.392–27.07; p=0.001). Patients who started hydroxyurea were predicted to have at least 3.071 times greater risk than those who did not (OR=3.071; 95% CI=1.164–8.104; p=0.023). Meanwhile, three or more hospitalizations per year was associated with 3.393-fold higher risk (OR=3.393; 95% CI=1.285–8.960; p=0.014), 3–5 blood transfusions with 8.862-fold higher risk (OR=8.862; 95% CI=2.643–29.71; p<0.001), and >5 transfusions with 4.320-fold higher risk (OR=4.320; 95% CI=1.287–14.51; p=0.018). Likewise, compared to patients with less than 3 ER visits per year, those who had 3 to 5 visits had at least 10.4 times higher risk of ICU admission (OR=10.38; 95% CI=10.098–98.19; p=0.041), those with 6 to 10 ER admissions had 18 times higher risk (OR=18.00; 95% CI=2.149–150.8; p=0.008), and those with more than 10 ER admissions had 9.39 times higher risk (OR=9.391; 95% CI=1.092–80.78; p=0.041). Finally, patients with high WBC were predicted to have at least 3.34 times higher risk of ICU admission than those with low WBC (OR=3.337; 95% CI=1.131–9.846; p=0.029). (Table 3).
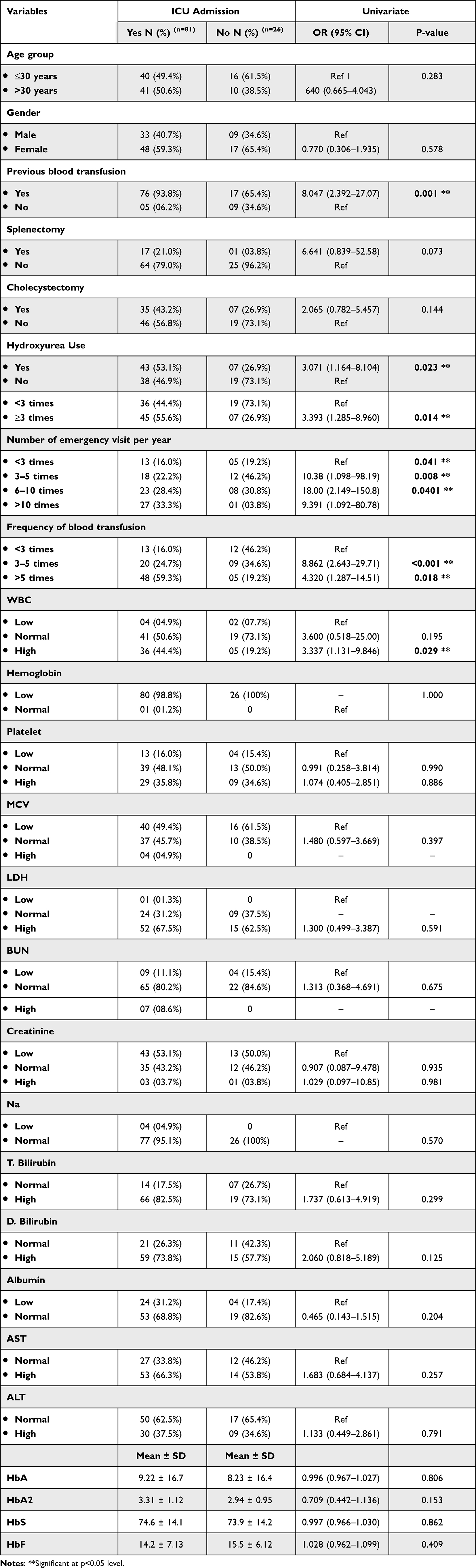 |
Table 3 Univariate Logistic Regression Analysis |
Discussion
Although considered the most common monogenic disorder, sickle cell disease comprises a complex group of hematologic disorders with multiple mechanisms involved in their pathophysiologies.8,9 The clinical heterogeneity and complexity of the disease are further modulated by fetal hemoglobin concentration and coincident alpha thalassemia. Thus, the SCD disease course spans a spectrum from very benign to very severe, with corresponding increases in morbidity and mortality.10,11 A previous study revealed that half of the mortality of individuals with SCD occurs in the ICU, with acute chest syndrome being the most common reason for admission.6 In our study, we found that around two-thirds of participants had required ICU admission at least once in their lifetime, with acute chest syndrome the most common reason for admission. Interestingly, participants taking hydroxyurea were more likely to be admitted compared to those who did not. This raises a concern that while hydroxyurea is an effective treatment, SCD is a complex disease and a multimodal approach likely remains needed.8,12 However, it is important to note that our study did not address whether patients were on the maximum tolerated dose of hydroxyurea or not and at which age hydroxyurea was offered.13,14
Several previous studies have reported concurring findings of increased risk of mortality among patients with SCD admitted to the ICU. In addition, five-year mortality is linked with a history of long ICU stay.15,16 Several predictors of increased mortality at ICU admission or during an ICU stay have been reported among patients with SCD; these include older age, renal replacement therapy, and frequent hospitalization use of inotropic support or mechanical ventilation.7,17 To our knowledge, the present work is the first study to address predictors of ICU admission among patients with SCD. Our result found that patients with three or more annual hospitalizations and emergency visits were at higher risk of ICU admission. Additionally, although red blood cell transfusion is an established treatment option for prevention of chronic organ damage, preoperative care, and acute complications of SCD, particularly acute chest syndrome, we found that history of previous blood transfusions of more than three was a significant predictor for ICU admission.16,18 These findings support a previous report of SCD patients having received exchange transfusions a few days prior to ICU admission; these patients may have an increased rate of alloimmunization and risk of delayed hemolytic transfusion reaction.19,20
Sickle cell disease is characterized by heightened inflammation involving leukocytes, platelets, and endothelial cells, and also by inflammation resolution failure. We observed that patients with high white blood cell count were at higher risk to be admitted compared to those with low counts. Meanwhile, baseline thrombocytosis or thrombocytopenia were poorly correlated with ICU admission in our study, which is contrary to prior findings that thrombocytopenia is a poor prognostic indicator among ICU-admitted SCD patients.21,22
This study illuminated characteristics that are predictors of ICU admission among patients with SCD. These include frequent hospitalization and emergency visits, multiple blood transfusions and elevated white blood cell count; moreover, admission increased despite hydroxyurea usage. The constellation of these factors could be translated into a scoring system that could be utilized to identify a high-risk group for early initiation of disease-modifying agents and to make early referrals to the ICU in order to achieve better outcomes. However, our study is limited by its retrospective nature and by physician-to-physician variability in making the decision for ICU admission. On this basis, prospective future studies are required, with the consideration of hydroxyurea usage duration and being on the maximum tolerated dose are crucial.
Conclusion
In conclusion, SCD is a multi-systemic disease associated with increased morbidity and mortality, and has a complex pathophysiology that mandates a multimodal treatment approach. Frequent hospitalization and emergency visits, multiple blood transfusions, and elevated white blood cell count were significantly associated with higher rate of ICU admission despite hydroxyurea usage. Recognition of these high-risk features in patients and establishment of severity scoring system can prompt initiation of a disease-modifying agent at a younger age and help to eliminate subjectivity in the timing of an ICU referral.
Data Sharing Statement
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethical
The study was conducted in accordance with the Declaration of Helsinki and approved by King Fahad Hospital’s Ethical Committee (KFHH RCA 33‐42‐2021). All participants provided informed consent before participation.
Acknowledgments
We would like to thank all participants for their collaboration.
Funding
This research did not receive any specific grant from funding agencies in the public, commercial, or not for fit sectors.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Ware RE, de Montalembert M, Tshilolo L, Abboud MR. Sickle cell disease. In: The Lancet. Vol. 390. Lancet Publishing Group; 2017:311–323.
2. Jastaniah W. Epidemiology of sickle cell disease in Saudi Arabia. Annals of Saudi Medicine. 2011;31(3):289–293. doi:10.4103/0256-4947.81540
3. Houwing ME, de Pagter PJ, van Beers EJ, et al. Sickle cell disease: Clinical presentation and management of a global health challenge. In: Blood Reviews. Vol 37. Churchill Livingstone; 2019.
4. Ribeil JA, Hacein-Bey-Abina S, Payen E, et al. Gene therapy in a patient with sickle cell disease. New England Journal of Medicine. 2017;376(9):848–855. doi:10.1056/NEJMoa1609677
5. Lubeck D, Agodoa I, Bhakta N, et al. estimated life expectancy and income of patients with sickle cell disease compared with those without sickle cell disease. JAMA Netw Open. 2019;2(11):e1915374. doi:10.1001/jamanetworkopen.2019.15374
6. Cecchini J, Lionnet F, Djibré M, et al. Outcomes of adult patients with sickle cell disease admitted to the ICU: a case series. Crit Care Med. 2014;42(7):1629–1639. doi:10.1097/CCM.0000000000000316
7. Al Khawaja SA, Ateya ZM, Al Hammam RA. Predictors of mortality in adults with Sickle cell disease admitted to intensive care unit in Bahrain. J Crit Care. 2017;42:238–242. doi:10.1016/j.jcrc.2017.07.032
8. McGann PT, Ware RE. Hydroxyurea for sickle cell anemia: what have we learned and what questions still remain? Curr Opin Hematol. 2011;18(3):158–165. doi:10.1097/MOH.0b013e32834521dd
9. Carden MA, Little J. Emerging disease-modifying therapies for sickle cell disease. In: Haematologica. Vol. 104. Ferrata Storti Foundation; 2019:1710–1719.
10. Shah N, Beenhouwer D, Broder MS, et al. Development of a severity classification system for sickle cell disease. ClinicoEconomics and Outcomes Research. 2020;12:625–633. doi:10.2147/CEOR.S276121
11. Steinberg MH, Sebastiani P. Genetic modifiers of sickle cell disease. American Journal of Hematology. 2012;87(8):795–803. doi:10.1002/ajh.23232
12. Jagadeeswaran R, Rivers A. Evolving treatment paradigms in sickle cell disease. Hematology. 2017;2017(1):440–446. doi:10.1182/asheducation-2017.1.440
13. Mak V, Davies SC. The pulmonary physician in critical care • Illustrative case 6: acute chest syndrome of sickle cell anaemia. Thorax. 2003;58(58):726–728. doi:10.1136/thorax.58.8.726
14. John CC, Opoka RO, Latham TS, et al. Hydroxyurea dose escalation for sickle cell anemia in sub-saharan Africa. New England Journal of Medicine. 2020;382(26):2524–2533. doi:10.1056/NEJMoa2000146
15. Hermans G, Van Aerde N, Meersseman P, et al. Five-year mortality and morbidity impact of prolonged versus brief ICU stay: a propensity score matched cohort study. Thorax. 2019;74(11):1037–1045. doi:10.1136/thoraxjnl-2018-213020
16. Mekontso Dessap A, Fartoukh M, Machado RF. Ten tips for managing critically ill patients with sickle cell disease. Intensive Care Med. 2017;43(1):80–82. doi:10.1007/s00134-016-4472-7
17. Tawfic QA, Kausalya R, Al-Sajee D, Burad J, Mohammed AK, Narayanan A. Adult sickle cell disease: a five-year experience of intensive care management in a university hospital in Oman. Sultan Qaboos Univ Med J. 2012;12(2):177–183. doi:10.12816/0003110
18. Howard J, Hart N, Roberts-Harewood M, Cummins M, Awogbade M, Davis B. Guideline on the management of acute chest syndrome in sickle cell disease. Br J Haematol. 2015;169(4):492–505. doi:10.1111/bjh.13348
19. Linder GE, Chou ST. Red cell transfusion and alloimmunization in sickle cell disease. In: Haematologica. Vol. 106. Ferrata Storti Foundation; 2021:1805–1815.
20. Agbakou M, Mekontso-Dessap A, Pere M, et al. Nationwide retrospective study of critically ill adults with sickle cell disease in France. Sci Rep. 2021;11(1). doi:10.1038/s41598-021-02437-2
21. Shome D, Jaradat A, Mahozi A, et al. The platelet count and its implications in sickle cell disease patients admitted for intensive care. Indian J Crit Care Med. 2018;22(8):585–590. doi:10.4103/ijccm.IJCCM_49_18
22. Hogg PJ. TMX1: a new vascular thiol isomerase. Blood. 2019;133(3):188–190. doi:10.1182/blood-2018-11-887679
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.