")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Preoperative Physical Dysfunction Characteristics and Influence Factors Among Elderly Patients with Early Lung Cancer: A Latent Class Analysis
Authors Zhang R , Yang Z, Shen X, Xia L, Cheng Y
Received 19 December 2023
Accepted for publication 9 April 2024
Published 23 April 2024 Volume 2024:17 Pages 1743—1754
DOI https://doi.org/10.2147/JMDH.S455669
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Rui Zhang,1,2 Zhengyao Yang,3 Xiaoyong Shen,3 Lu Xia,4 Yun Cheng5
1Department of Nursing, Huadong Hospital Affiliated to Fudan University, Shanghai, 200040, People’s Republic of China; 2School of Nursing, Fudan University, Shanghai, 200030, People’s Republic of China; 3Department of Chest Surgery, Huadong Hospital Affiliated to Fudan University, Shanghai, 200040, People’s Republic of China; 4Day Surgery Unit, Huadong Hospital Affiliated to Fudan University, Shanghai, 200040, People’s Republic of China; 5School of Medicine, The Chinese University of Hong Kong, Shenzhen, 518172, People’s Republic of China
Correspondence: Lu Xia, Day Surgery Unit, Huadong Hospital Affiliated to Fudan University, No. 221 of Yanan West Road, Jingan District, Shanghai, 200040, People’s Republic of China, Tel +86 21-62483180-530401, Email [email protected] Yun Cheng, School of Medicine, The Chinese University of Hong Kong, Shenzhen, 518172, People’s Republic of China, Tel +86 755-23519000, Email [email protected]
Objective: To identify latent classes of preoperative physical dysfunction in elderly patients with early lung cancer. To analyze the differences in demographic characteristics between different classes.
Methods: We invited elderly patients with early lung cancer who were scheduled for surgery at Shanghai Elderly Characteristic Hospital to participate in the study using a convenience sampling method. We took latent class analysis to divide elderly patients with early lung cancer into latent classes based on preoperative physical dysfunction features. Furthermore, we used single-factor analysis and multinomial logistic regression to investigate the influence variables of each latent class.
Results: The characteristics of preoperative physical dysfunction in elderly patients with early lung cancer can be divided into “Anxiety/depression emotion-poor sleep group” “Frailty of physical function group” “Pulmonary hypofunction-low activity tolerance group”. The distribution of age, chronic disease history, COPD history, smoking history and perceived social support level of elderly patients with early lung cancer in different potential categories were not the same, and the differences were statistically significant (P< 0.05). The elderly lung cancer patients with chronic disease history and age ≥ 75 years were more likely to be classified as “frailty of physical function group”. The elderly lung cancer patients with COPD and smoking history were more likely to be classified into “pulmonary hypofunction-low activity tolerance group”. Elderly lung cancer patients with moderate or low degree of perceived social support were more prone to be grouped into “anxiety/depression emotion-poor sleep group”.
Conclusion: The variety of preoperative physical dysfunction seen in elderly patients with early lung cancer can be categorized into three latent classes. Medical professionals should create strategies for intervention for multiple patient populations with the goal of further enhancing their general state of life.
Keywords: elderly, lung neoplasm, preoperative physical dysfunction, latent class analysis, influence factors
Introduction
Lung cancer is a major cause of morbidity and mortality in the elderly.1 Also, before being diagnosed with lung cancer, patients frequently experience a decline in physical function.2 Due to frailty, inadequate physiologic reserve, multimorbidity, and functional impairment, elderly patients are slower to return to physical function and quality of life after lung cancer surgery than younger patients.3 This further impacts the elderly patient’s quality of life and dyspnea.
According to the guidelines, prehabilitation can enhance a patient’s preoperative functional reserve, then improve their capacity to tolerate surgical stress and trauma. It is particularly beneficial for elderly patients who had limited function before surgery.4 Prehabilitation entails the evaluation of patients’ physical, psychological, and nutritional functions prior to surgery so as to determine the functional baseline. Then identify abnormal body functions, and provide targeted preoperative interventions. The aim of it is to improve the preoperative functional reserve of patients, surgical tolerance, perioperative morbidity, and postoperative complications.5
Current reported research confirms the efficacy of providing a set of prehabilitation measures on enhancing patients’ physical function and lowering postoperative complications.6,7 However, patient compliance will be greatly impacted by the short preoperative preparation duration and the objective resistance of interdisciplinary integration.8
Prehabilitation can be precisely applied if the heterogeneity of preoperative functional dysfunction in elderly individuals with early lung cancer can be characterized,9 thus will positively affect patient economic costs, optimize medical human resource allocation, increase patient compliance, and improve patient prognosis. Individuals and population heterogeneity can be classified using latent class analysis (LCA) based on their distinct response patterns to category salient variables.10 LCA can identify the characteristics of various patient categories and highlight particulars of each population group, making diagnosis and management easier.
As a result, this study investigates and analyzes the potential categories of preoperative physical dysfunction in elderly patients with early lung cancer in order to improve the identification of preoperative physical dysfunction and provide a foundation for the development of prehabilitation.
Methods
Study Participants
We employed convenience sampling to pick elderly patients at Shanghai Elderly Characteristic Hospital who had been treated for early lung cancer from January to June 2023. The inclusion criteria for patients were listed as follows: (1) age ≥60 years old, (2) admission diagnosis was “pulmonary space-occupying lesion”, (3) surgery for pulmonary was planned, (4) endorsed the informed consent document. Following was a list of the exclusion criteria for patients: (1) The intraoperative pathological results were non-early lung cancer, (2) with severe mental disorders or mental illness, (3) with severe complications of other organs.
Study Instruments
The required data had been collected using a ten-part questionnaire. Among them, Part 1 and Part 2 were combined as demographic characteristics.
Part 1: General Information Questionnaire
Based on the literature research, the investigator self-designed this section, which comprised patient clinical data and sociodemographic information. The patient clinical data were mainly intraoperative pathological results. The sociodemographic information included gender, age, education level, previous occupation, body mass index, chronic disease history, COPD history, smoking history, and alcohol consumption history.
Part 2: Perceived Social Support Scale (PSSS)
The scale was developed by Zimet’s team,11,12 which can be used to measure the perceived social support from within and outside the family, and the total score of the scale can be used to reflect the overall social support felt by the individual. PSSS of self-evaluation of a total of 12 items, each item all adopt 1~7 points scoring, which means strongly disagree to strongly agree. The scale dimensions were separated into three subscales: family support, friend support, and other support, with each component represented by the cumulative input points. Perceived social support scale scores for each item total score. The sum of total table and three subscales Cronbach’s α coefficients were 0.88, 0.91, 0.87, 0.85. The scale in Chinese hospital patients was investigated and studied for validity and reliability of evaluation. The whole table with three subscales had Cronbach’s α coefficients of 0.840, 0.818, 0.820, 0.813.13 In this study, the level of personal perceived social support was divided into medium-low support level (12~60 points) and high support level (61~84 points).
Part 3: Respiratory Function Related Indicators
The pulmonary function indexes of the patients were recorded by reviewing their pulmonary function test reports on admission. The evaluation index used in this study was the ratio of forced expiratory volume in one second to forced vital capacity (FEV1/FVC), forced expiratory volume in one second as a percentage of predicted value (ppo FEV1), the ratio of diffusion lung capacity for CO as a percentage of predicted value (ppo DLCO) and peak expiratory flow (PEF).14 The classification of lung function indices was made with reference to Clinical Pulmonary Function and in relation to the purpose of the study.15 The FEV1/FVC ratio can indicate the presence of an airflow restriction, and less than 70% was abnormal. The ppo FEV1 reflected pulmonary ventilation dysfunction, less than 80% was abnormal. The ppo DLCO reflected pulmonary gas exchange dysfunction, less than 80% was abnormal. PEF less than 3L/s revealed that the patients’ sputum ability is poor, that they are prone to discharge clogging, that they require particular strengthening deep breathing exercises and coughing, as well as additional interventions to promote postoperative airway and alveolar drainage.
Part 4: Nutritional Function Related Indicators
According the electronic medical records of patients on admission hemoglobin values (HB) and albumin values (ALB) fill in the questionnaire survey results. According to the normal adult male hemoglobin is 120~160 g/L, female adult normal is 110~150g/L standard combined with clinical significance. This study shows that the men’s hemoglobin is less than 120g/L, and the women’s hemoglobin is less than 110 g/L as abnormal. According to the normal adult normal albumin is 35~50g/L in combination with clinical significance, this study labeled albumin less than 35g/L for the abnormal value of the need to pay attention to.
Part 5: Motor Function Related Indicators
The motor function tests include 6-minute walk distance (6MWD), Usual gait speed (UGS), 5-times sit-to-stand test (FTSST), timed up and go test (TUGT). Calculating 6 minutes walking distance based on clinical practice,16,17 eventually to compare the results and the expected value. The value lower than the predicted value was abnormal. UGS and FTSST can be further assessment of elderly patients with physical function. UGS less than 1 m/s and FTSST greater than or equal to 12 seconds tipped physical function deterioration. TUGT more than 12 seconds indicates elderly patients had a high chance of a fall.4
Part 6: Frailty Phenotype Scale (FP)
Fried’s team designed the frailty phenotype scale, which is now widely utilized in the study of weak persons.18 The scale included five items: unintentional weight loss, self-reported exhaustion, decreased grip strength, slow walking speed, and low physical activity. Every indicator was calculated as 1 point, and the score range was 0~5 points. 0 points were considered as no frailty, 1~2 points were considered as pre-frailty, and 3 points and above were considered as frailty. The Cronbach’s α coefficient of the scale applied in the Chinese version was 0.93.19 In this study, physical frailty was defined as a score greater than or equal to 1.
Part 7: Nutritional Risk Screening (NRS-2002)
NRS2002 is recommended by Chinese Society of Enteral and Parenteral Nutrition as the preferred tool for nutritional status assessment in elderly inpatients.20 The scale included three dimensions: age, severity of disease and nutritional impairment.21 Above 70 years old was assigned 1 point, and age ≤70 years old was assigned 0 point. The severity of illness and nutritional impairment status were scored on a three-point scale (0~3 points), with a total score of 0~7 points, and a score ≥3 points indicates that the patient is at nutritional risk and should be initiated to develop a nutritional treatment plan.
Part 8: Miniature Cognitive Status Assessment Scale (Mini-cog)
The miniature cognitive status assessment scale was developed to test geriatric cognitive function. Two cognitive tests were included in the miniature cognitive state assessment scale: a three-word memory recall test and a sketch the clock exam. In the three words test, 1 point was awarded for each accurate word, 2 points for the clock drawing test, and 0 points for any or all faults. The score of Mini-cog equal to 5 was regarded to be in the normal group, while less than 5 was thought to be at risk of cognitive impairment.
Part 9: Hospital Anxiety and Depression Scale (HADS)
The hospital anxiety and depression measure created in 1983 by Zigmond et al which consisted of fourteen items total and can be divided into anxiety and depression dimensions.22 The scale score was as follows: 0~7 represented no symptoms; 8~10 indicated suspicious symptoms; and 11~21 represented certain symptoms. The final scale score in this study was split into 8~21 as potentially symptomatic and 0~7 as asymptomatic. According to a survey, the Chinese version of the scale had a Cronbach’s α coefficient of 0.879, 0.806, and 0.806 for the overall scale, depression, and anxiety aspects.23
Part 10: Pittsburgh Sleep Quality Index (PSQI)
The seven elements of the index were developed in 1989 by Dr. Buysse’s team and include subjective sleep quality, sleep latency, sleep duration, sleep efficiency, sleep disturbance, hypnotic medicine, and daytime dysfunction.24 The Likert scale is used to rate this scale. Total scores can range from 0~21, with a score of greater than 7 denoting poor quality of sleep. The English version of this scale has an overall reliability rating of 0.83, which suggests a high level of internal consistency. Additionally, the Chinese version’s consistency coefficient was 0.845.25
Data Collection
The data was gathered by graduate students studying clinical medicine and nursing. Patient clinical data were acquired by investigating electronic medical records, while sociodemographic information was obtained by engaging patients and their families. Both students were able to assist patients in cooperating with data collection in a very consistent manner after attending the corresponding training.
Statistical Analyses
The latent class model was established using Mplus8.3 in accordance with the model fitting assessment index.26 Log likelihood (LL), Akaike information criterion (AIC), Bayesian information criterion (BIC) and adjusted Bayesian information criterion (aBIC) are smaller values indicated better model fit. LoMendell-Rubin (LMR) and Bootstrapped likelihood ratio test (BLRT) were used to compare the model fitting differences. Its corresponding P values indicates that the k category model outperforms the k−1 category model. The accuracy with which the model could place individuals in the appropriate group was assessed using entropy. The values were on a range from 0 to 1, with 1 denoting greater classification accuracy. Entropy more than 0.80 was considered as high classification accuracy of the model.
For statistical analysis, SPSS 20.0 software was used. Count data were reported as frequency, percentage, or percentage, with the chi-square test used to compare groups. Multinomial logistic regression was used to investigate the influencing factors of potential categories of preoperative physical dysfunction characteristics in elderly patients with early lung cancer, using demographic characteristics as independent variables and LCA classification results as dependent variables. All tests were two-sided, with a P value of less than 0.05 considered statistically significant.
Results
Participants’ Demographic Characteristics
There were 248 participants in this study. Weed out unable to complete the questionnaire because preoperative examination of 9 cases, recycling questionnaire, total of 239 cases. According to the postoperative pathology evaluation, 12 individuals with non-early lung cancer were excluded, leaving 227 patients. Demographic Characteristics of elderly patients with early lung cancer are shown in Table 1. The occurrence of preoperative physical dysfunction is shown in Table 2.
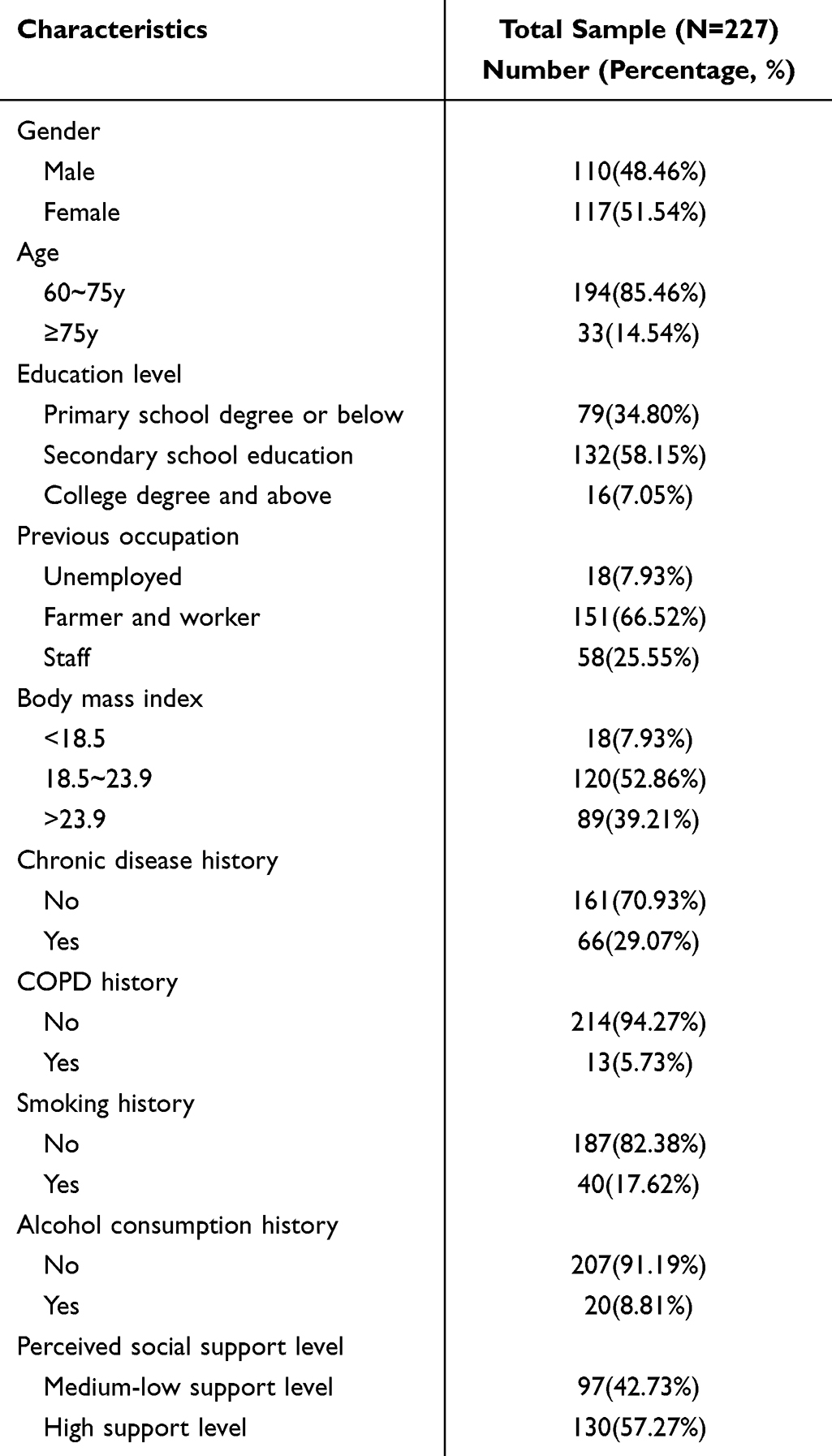 |
Table 1 Demographic Characteristics of Elderly Patients with Early Lung Cancer |
 |
Table 2 Occurrence of Preoperative Physical Dysfunction |
Identification of Preoperative Physical Dysfunction Characteristics Subgroups
Latent class analysis was performed on the abnormal values of preoperative physical dysfunction with incidence ≥40%.27 In this study, ppoFEV1, ppo DLCO, ALB, 6MWD, FTSST, TUGT, FP, HADS, and GSDS were included for latent class analysis. Starting from one class and increasing the number of classes in turn, a total of five latent classes were fitted. When three categories were retained, BIC reached the minimum, entropy was ideal, and LMR and BLRT both reached a significant level (P<0.05). Moreover, BIC began to increase when four classes were retained, and LMR did not reach a significant level (P>0.05). Therefore, three potential categories were selected for classification based on comprehensive consideration, as shown in Table 3. The average latent class probabilities for most likely latent class membership respectively was 0.925, 0.955, 0.968. The classification probabilities for the most likely latent class membership respectively were 0.954, 0.977, 0.934. It indicates that the classification results of the three latent class models are reliable.10
 |
Table 3 Fit Indices of Latent Profile Analysis of Preoperative Physical Dysfunction Characteristics in Elderly Patients with Early Lung Cancer |
There were 48 cases (21.14%) in Class 1, which was named as “pulmonary hypofunction-low activity tolerance group“ because of the high incidence of low ppo DLCO and low 6MWD, and the low incidence of other abnormal values. Class 2 contains 87 cases (38.33%), the category of depression/anxiety and sleep quality low incidence at a higher level, so named “anxiety/’ emotion - poor sleep group”. Class 3 contains 92 cases (40.52%), the category in pre-frailty or frailty and TUGT low rate at a higher level, so named “frailty of physical function group”. Preoperative Physical Dysfunction Characteristics in Elderly Patients with Early Lung Cancer for Each Latent Subgroup are shown in Figure 1.
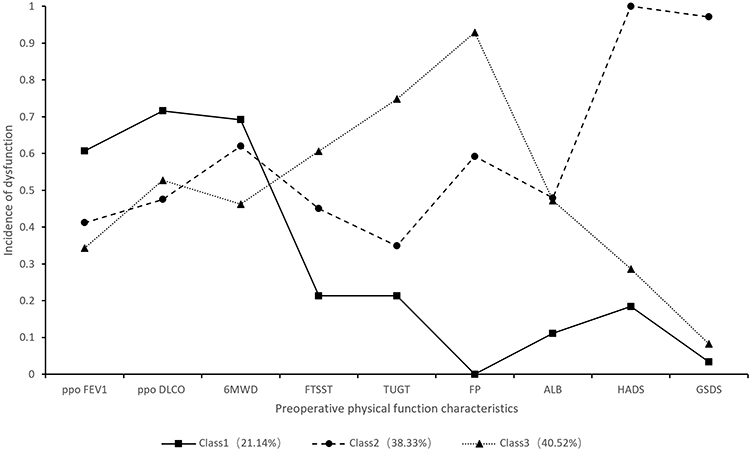 |
Figure 1 Preoperative Physical Dysfunction Characteristics in Elderly Patients with Early Lung Cancer for Each Latent Subgroup. |
Differences in Demographic Characteristics Among Preoperative Dysfunction Subgroups
Table 4 shows the differences in general characteristics between the “pulmonary hypofunction-low activity tolerance group”, “frailty of physical function group”, and “anxiety/depression emotion-poor sleep group” subgroups. Age, perceived social support level, chronic disease history, smoking history, and COPD history all exhibited significant differences in univariate analysis.
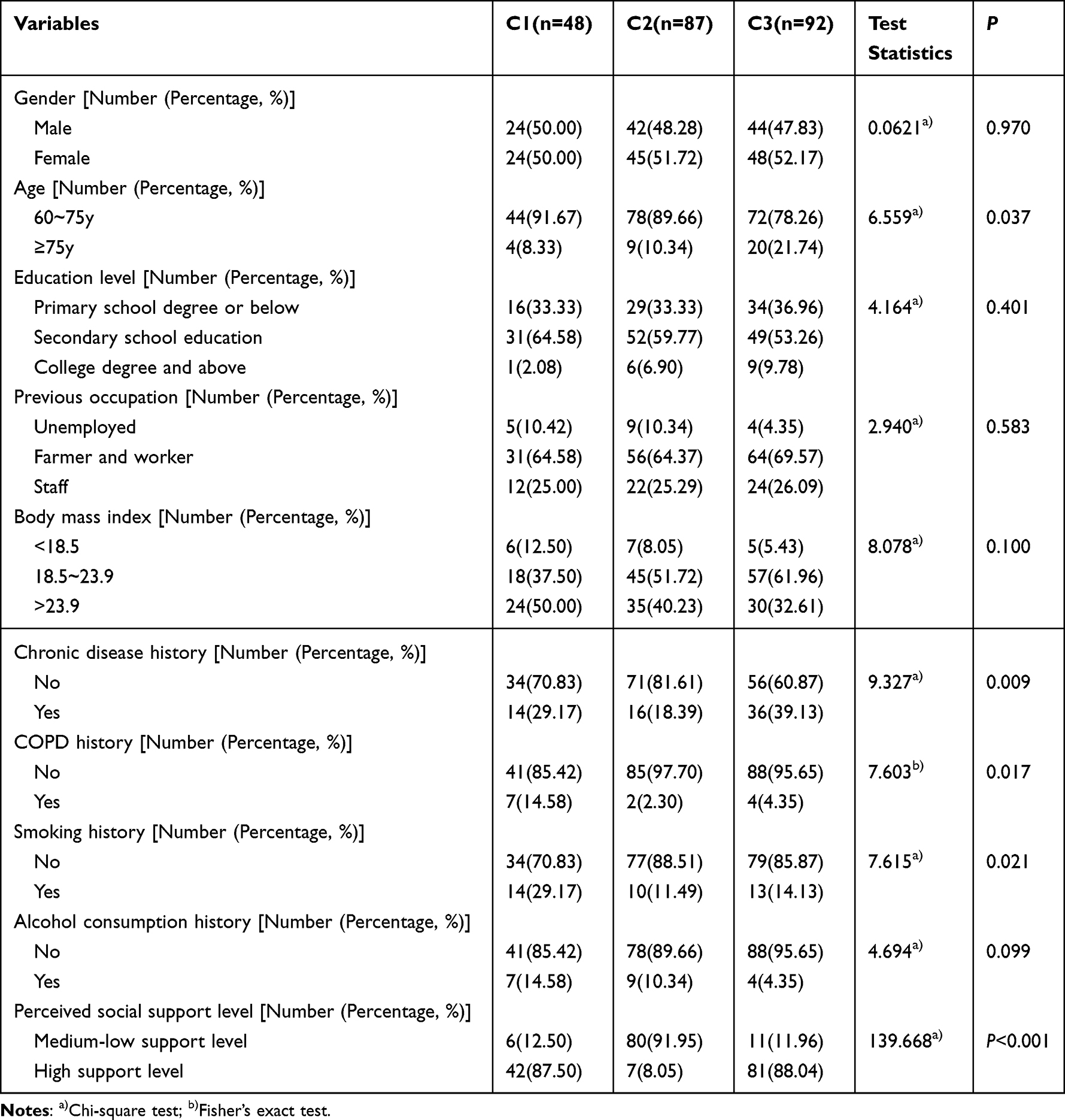 |
Table 4 Results of Demographic Characteristics Among Preoperative Dysfunction Subgroups |
The findings of multinomial logistic regression with factors for each subgroup, with the “frailty of physical function group” as the reference, are shown in Table 5. The elderly patients with early lung cancer who had no chronic disease history (odds ratio = 0.334, 95% CI[0.127, 0.878], P=0.026), who were younger than 75 years (odds ratio = 0.297, 95% CI[0.089, 0.989], P=0.048), who had COPD history (odds ratio = 7.035, 95% CI[1.481, 33.422], P=0.014), who had smoking history (odds ratio = 3.124, 95% CI[1.298, 7.518], P=0.011) had a greater chance to be noticed in the “pulmonary hypofunction-low activity tolerance group” than in the “frailty of physical function group”. The elderly patients with early lung cancer who had no chronic disease history (odds ratio = 0.165, 95% CI[0.052, 0.523], P=0.002), who were younger than 75 years (odds ratio = 0.199, 95% CI[0.054, 0.727], P=0.015), who in medium-low Perceived social support level (odds ratio = 135.641, 95% CI[42.477, 433.139], P<0.001) had a greater likelihood to be found in the “anxiety/depression emotion-poor sleep group” than in the “frailty of physical function group”.
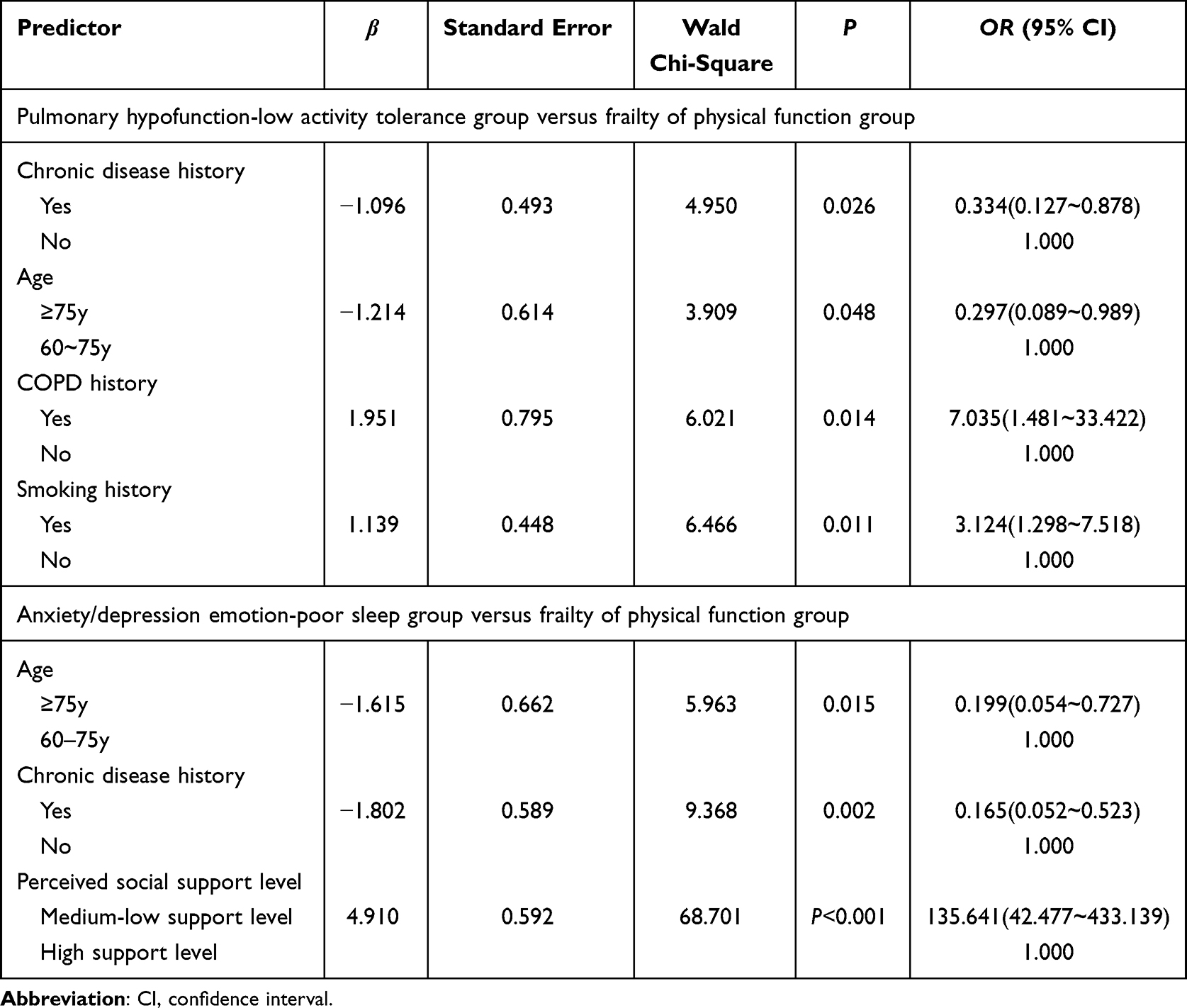 |
Table 5 Results of Multinomial Logistic Regression |
Discussion
Latent class analysis was used to divide the preoperative physical dysfunction characteristics of elderly patients with early lung cancer into three latent categories: “pulmonary hypofunction-low activity tolerance group” “anxiety/depression emotion-poor sleep group” “frailty of physical function group”. This shows that elderly patients with early lung cancer with preoperative physical dysfunction have individual variances. Voorn et al found that preoperative physical parameters in elderly lung cancer patients were associated with treatment tolerance and survival, and they recommended comprehensive physical and geriatric parameters before surgery, as well as active interventions to improve the physical status of elderly lung cancer patients prior to surgery, in order to better adapt to the surgery.28 The preoperative pulmonary functional status can have a substantial impact on the patient’s prognosis and postoperative quality of life.29 Preoperative pulmonary function training can enhance pulmonary ventilation and reduce pulmonary complications.30 Polański et al found that patients with anxiety and depression had a significantly lower quality of life. At the same time, they suggested early detection of anxiety and depression may aid in treatment options.31 According to research, debility has a considerable detrimental impact on the incidence of postoperative delirium, pneumonia, and death in elderly lung cancer patients.32,33 Therefore, medical staff need to do a comprehensive assessment of elderly patients with lung cancer before surgery combining a better prehabilitation plan to be able to help patients improve prognosis and quality of life.
The “frailty of physical function group” had the largest proportion (40.52%). The higher incidence of FP and TUGT abnormalities in elderly patients with early lung cancer in this group could be attributed to increased risk of frailty and falls. Frailty and latent frailty are frequent in lung surgery patients.34 Preoperative frailty in elderly patients with early lung cancer should be addressed by medical professionals, and patients should be helped to safely finish the surgery preparation by prehabilitation. The “pulmonary hypofunction-low activity tolerance group” (21.14%), which has the lowest proportion of patients with ppoFEV1, an abnormal ppo DLCO, and 6MWD low at high levels. Namely, pulmonary gas exchange function and pulmonary ventilation function, and the low activity endurance is relatively high. The proportion of this part may be because the preoperative pulmonary function in patients with abnormal relatively obvious, there may be varying degrees of asthma, chest tightness and so on. Medical professionals should provide exercise coaching based on the results of lung function tests in patients with preoperative respiratory function. This is vital to enhancing lung function and activity endurance for patients.35 The “anxiety/depression emotion-poor sleep group” accounted for 38.33% of the total. The anxiety/depression and sleep index scores of elderly patients with early lung cancer in this group were greater, but the aberrant levels of other indicators were relatively modest. Perhaps since the patient would undoubtedly have mood changes and sleep pattern disturbances, but with reasonably decent physiological function, the abnormal psychological function is more noticeable. Medical professionals use psychological nursing and health education effectively for elderly patients with early lung cancer, which significantly improves the patient’s bad mood, quality of life, and prognosis, and has significant clinical value.36
Despite the limited sample size, this study found that only a small proportion of elderly patients with early lung cancer had reduced nutritional and cognitive function prior to surgery. As a result, we think that while the assessment of nutritional status cannot be skipped, quick and easy screening methods can be chosen to the greatest extent feasible. Besides, the cognitive function scale evaluation can be chosen based on the patient’s state. Therefore, the purpose of preoperative nutritional support can be appropriately adapted to the patient’s nutritional function. From correcting preoperative malnutrition turn to providing nutritional counseling and preoperative oral nutritional supplements to alleviate gastrointestinal discomfort during and after surgery. Besides, among the biochemical markers intimately associated with nutrition, the likelihood of anomalous ALB was comparatively elevated (40.09%). However, this did not impact the classification of latent categories.
According to the study’s findings, those who were 75 years of age or older and had a history of chronic illnesses were more likely to be placed in the “declining physical performance group”. This is consistent with expert consensus, which states that a history of chronic disease and age are the main risk factors for the development of impaired function, and that a significant increase in the incidence of incapacitation with age is particularly notable in people aged 75 years and older.37 Furthermore, in elderly patients with early lung cancer, preoperative physical function parameters are linked to treatment tolerance and survival rates, and low preoperative physical function scores are linked to a higher likelihood of unfavorable treatment outcomes.28 It is therefore recommended that older patients review their physical function before treatment, as well as chronic illnesses, and so on, in order to make a shared decision and option. Additionally, patients may benefit from preventive intervention during therapy. Prehabilitation may be beneficial for elderly patients with lung cancer whose body function is declining early, in order to enhance their therapy before the body’s condition of decline begins.
The study’s findings point to a higher likelihood of decreased exercise capacity or lung function in older smokers with early-stage lung cancer who also have a history of COPD. According to research, smoking is the primary risk factor for both COPD and lung cancer.38 Smoking also increases the risk of lung cancer on its own. The pathogenesis has a strong internal link and correlation. Reduced lung function is the most common clinical indication of COPD,39 and poor exercise endurance is another defining feature of the disease. Furthermore, an investigation has discovered that mice’s ability to tolerate exercise can be diminished by passive smoking.40 Appropriate correction of preoperative smoking can benefit patients in terms of exercise tolerance,41 and preoperative evaluation of COPD disease history can help in the early identification of patients with reduced lung function and exercise tolerance.
Social support is a significant and predictive factor that may have an impact on the clinical prognosis of elderly patients with early lung cancer.42 It is vital to assess elderly patients with early lung cancer who may exhibit signs of anxiety or depression prior to surgery, and to refer those who exhibit severe issues to psychologists. Professional nurses who have received training in psychological counseling can offer psychological counseling, guided relaxation techniques, music therapy, meditation, and other methods of reducing negative emotions to individuals who solely experience anxiety and/or depression. At the same time, with the assistance of the hospital’s social worker department, licensed social workers can be invited to assist elderly patients experiencing unpleasant feelings related to early lung cancer. A person’s ability to sense support from friends, family, and other social sources can be gauged by their understanding of social support.43,44 In order to address issues and provide assistance, social workers integrate their patients’ psychological, social, and physical concerns.45 Therefore, social work division can be more involved in helping elderly patients, including the patient’s family care, help contact care hospitals, health institutions, relevant communities or docking streets, looking for the matching of social resources.
Conclusion
In this study, we used the latent class analysis to categorize the preoperative physical dysfunction characteristics of elderly patients with early lung cancer into three categories, including “Anxiety/depression emotion-poor sleep group” “Frailty of physical function group” “Pulmonary hypofunction-low activity tolerance group”. It suggested that clinical professions should be aware of it. Patients who require less time for preoperative preparation or who exhibit low adherence may benefit from using the “key intervention and comprehensive education” approach, which is focused on implementing preoperative rehabilitation. This approach not only helps to save medical resources but also enhances patient compliance and the effectiveness of short-term rehabilitation. The following factors will influence atypical characteristics: age, perceived social support level, chronic disease history, smoking history, and COPD history. Medical professionals should provide appropriate interventions for these topics, and appropriate health education can be provided based on the patients’ aberrant traits.
Ethics Statement
This study complied with the Declaration of Helsinki and obtained ethical approval from the institution review boards of the Huadong Hospital Affiliated to Fudan University (No.20230021).
Funding
This study was supported by Key Research and Development Program of the Ministry of Science and Technology of China (2019YFE105600), Shanghai Municipal Science and Technology Commission program (16411951200), Shanghai Hospital Development Center Clinical science and technology innovation project (SHDC22021218).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Chen J, Che WG, Sun DQ, et al. Consensus of Chinese experts on surgical treatment of lung cancer in the elderly (2022 Edition). Chin J Lung Cancer. 2023;26(2):83–92. doi:10.3779/j.issn.1009-3419.2023.102.09
2. Kowalski L. Functional decline as an indicator of ill-health: a retrospective case study of the process leading to lung cancer. J Multidiscip Healthc. 2021;14:919–927. doi:10.2147/jmdh.S295498
3. Raz DJ, Kim JY, Erhunwmunesee L, et al. The value of perioperative physical activity in older patients undergoing surgery for lung cancer. Expert Rev Respir Med. 2023;17(8):691–700. doi:10.1080/17476348.2023.2255133
4. Liu ZJ, Zhang L, Liu HS, et al. Expert consensus on prehabilitation management for enhanced recovery in patients undergoing thoracic surgery (2022). J Med Peking Union Med Coll Hosp. 2022;13(3):387–401.
5. Carli F, Ferreira V. Prehabilitation: a new area of integration between geriatricians, anesthesiologists, and exercise therapists. Aging Clin Exp Res. 2018;30(3):241–244. doi:10.1007/s40520-017-0875-8
6. Geng CR, Mao M, Chen L. Effects of preoperative rehabilitation on pulmonary function and exercise capacity of lung cancer patients over 60 years old. Chin J Rehabil Med. 2019;34(9):1034–1037.
7. Li Y, Yan C, Li J, et al. A nurse-driven enhanced recovery after surgery (ERAS) nursing program for geriatric patients following lung surgery. Thorac Cancer. 2020;11(4):1105–1113. doi:10.1111/1759-7714.13372
8. Voorn MJJ, Bastiaansen EMW, Schröder CD, et al. A qualitative stakeholder analysis of beliefs, facilitators, and barriers for a feasible prehabilitation program before lung cancer surgery. J Cancer Res Clin Oncol. 2023;149(17):15713–15726. doi:10.1007/s00432-023-05298-6
9. Ordak M. Precision medicine in oncology - machine learning recommendations. Am J Cancer Res. 2023;13(4):1617–1619.
10. Wen ZL, Xie JY, W HH. The principle, steps and procedures of latent class models. J East Chin Normal University. 2023;41(01):1–15. doi:10.16382/j.cnki.1000-5560.2023.01.001
11. Zimet GD, Dahlem NW, Zimet SG, et al. The multidimensional scale of perceived social support. J Pers Assess. 1988;52(1):30–41. doi:10.1207/s15327752jpa5201_2
12. Zimet GD, Powell SS, Farley GK, et al. Psychometric characteristics of the multidimensional scale of perceived social support. J Pers Assess. 1990;55(3–4):610–617. doi:10.1080/00223891.1990.9674095
13. Zhang F, Zhu SZ, D PJ. Evaluation of perceived social support scale used in study of social support among hospitalized patients in China. Chin Nurs Res. 2018;32(13):2048–2052.
14. Mao X, Zhang W, Ni YQ, et al. A prediction model for postoperative pulmonary complication in pulmonary function-impaired patients following lung resection. J Multidiscip Healthc. 2021;14:3187–3194. doi:10.2147/jmdh.S327285
15. Zhu L. Clinical Pulmonary Function.
16. Chinese Society of Cardiology of Chinese Medical Association, Professional Committee of Cardiopulmonary Prevention Rehabilitation of Chinese Rehabilitation Medical Association, Editorial Board of Chinese Journal of Cardiology. Chinese expert consensus on standardized clinical application of 6-minute walk test. Chin J Cardiol. 2022;50(5):432–442. doi:10.3760/cma.j.cn112148-20211206-01054
17. Enright PL, Sherrill DL. Reference equations for the six-minute walk in healthy adults. Am J Respir Crit Care Med. 1998;158(5 Pt 1):1384–1387. doi:10.1164/ajrccm.158.5.9710086
18. Fried LP, Tangen CM, Walston J, et al. Frailty in older adults: evidence for a phenotype. J Gerontol a Biol Sci Med Sci. 2001;56(3):M146–M156. doi:10.1093/gerona/56.3.m146
19. Han J, Wang JQ, Xie BQ, et al. Comparison of consistency and validity of fried frailty phenotype, FRAIL scale and Edmonton frailty scale for frailty screening among community-dwelling older adults. Chin Gen Pract. 2021;24(21):2669–2675.
20. Elderly Nutrition Support Group of Society of Parenteral and Enteral Nutrition of the Chinese Medical Association. Chinese expert consensus on elderly parenteral and enteral nutrition support. Chin J Geriatr. 2013;32(9):913–929. doi:10.3760/cma.j.issn.0254-9026.2013.09.001
21. Kondrup J, Allison SP, Elia M, et al. ESPEN guidelines for nutrition screening 2002. Clin Nutr. 2003;22(4):415–421. doi:10.1016/s0261-5614(03)00098-0
22. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
23. Sun ZX, Liu HX, Jiao LY, et al. Reliability and validity of Hospital Anxiety and Depression Scale. Chin J Clinicians. 2017;11(02):198–201.
24. Buysse DJ, Reynolds CF, Monk TH, et al. The Pittsburgh sleep quality index: a new instrument for psychiatric practice and research. Psychiatry Res. 1989;28(2):193–213. doi:10.1016/0165-1781(89)90047-4
25. Lu TY, Li Y, Xia P, et al. Analysis on reliability and validity of the Pittsburgh Sleep Quality Index. Chongqing Med. 2014;43(03):260–263.
26. Chen F. Medical Methods of Multivariate Statistical Analysis.
27. Miaskowski C, Dunn L, Ritchie C, et al. Latent class analysis reveals distinct subgroups of patients based on symptom occurrence and demographic and clinical characteristics. J Pain Symptom Manage. 2015;50(1):28–37. doi:10.1016/j.jpainsymman.2014.12.011
28. Voorn MJJ, Bootsma MFR, Bootsma GP, et al. Association of pretreatment physical and geriatric parameters with treatment tolerance and survival in elderly patients with stage I-II non-small cell lung cancer: an evaluation of usual care data. Cancers. 2022;14(23):5994. doi:10.3390/cancers14235994
29. Fuzhi Y, Dongfang T, Wentao F, et al. Rapid recovery of postoperative pulmonary function in patients with lung cancer and influencing factors. Front Oncol. 2022;12:927108. doi:10.3389/fonc.2022.927108
30. Laurent H, Aubreton S, Galvaing G, et al. Preoperative respiratory muscle endurance training improves ventilatory capacity and prevents pulmonary postoperative complications after lung surgery. Eur J Phys Rehabil Med. 2020;56(1):73–81. doi:10.23736/s1973-9087.19.05781-2
31. Polański J, Chabowski M, Chudiak A, et al. Intensity of anxiety and depression in patients with lung cancer in relation to quality of life. Adv Exp Med Biol. 2018;1023:29–36. doi:10.1007/5584_2017_50
32. Komici K, Bencivenga L, Navani N, et al. Frailty in patients with lung cancer: a systematic review and meta-analysis. Chest. 2022;162(2):485–497. doi:10.1016/j.chest.2022.02.027
33. Tian JY, Hao XY, Cao FY, et al. Preoperative frailty assessment predicts postoperative mortality, delirium and pneumonia in elderly lung cancer patients: a retrospective cohort study. Ann Surg Oncol. 2023;30(12):7442–7451. doi:10.1245/s10434-023-13696-w
34. Cooper L, Gong Y, Dezube AR, et al. Thoracic surgery with geriatric assessment and collaboration can prepare frail older adults for lung cancer surgery. J Surg Oncol. 2022;126(2):372–382. doi:10.1002/jso.26866
35. Pu CY, Batarseh H, Zafron ML, et al. Effects of preoperative breathing exercise on postoperative outcomes for patients with lung cancer undergoing curative intent lung resection: a meta-analysis. Arch Phys Med Rehabil. 2021;102(12):2416–2427.e4. doi:10.1016/j.apmr.2021.03.028
36. Sun Y, Wang X, Li N, et al. Influence of psychological nursing and health education on depression, anxiety and life quality of elderly patients with lung cancer. Psychogeriatrics. 2021;21(4):521–527. doi:10.1111/psyg.12700
37. Wu JQ, Chen B, Mao YJ, et al. Chinese expert consensus on prevention and control intervention for elderly with physical function impairment (2022). Chin J Geriatrics. 2022;41(10):1137–1145. doi:10.3760/cma.j.issn.0254-9026.2022.10.002
38. Bugge A, Lund MB, Brunborg C, et al. Survival after surgical resection for lung cancer in patients with chronic obstructive pulmonary disease. Ann Thorac Surg. 2016;101(6):2125–2131. doi:10.1016/j.athoracsur.2015.12.057
39. Ye LJ, Zhou JM, Cui YY, et al. Study on pulmonary function, psychological status and coping methods of lung cancer patients combined with moderate and severe COPD treat by surgery. Chin J Health Psycholo. 2019;27(10):1517–1521. doi:10.13342/j.cnki.cjhp.2019.10.020
40. Liu GL, Yang XZ. Experimental Study of passive smoking on healthy mice’s endurance. Chin Healthc Frontiers. 2009;4:22.
41. Ni HJ, Pudasaini B, Yuan XT, et al. Exercise training for patients pre- and postsurgically treated for non-small cell lung cancer: a systematic review and meta-analysis. Integr Cancer Ther. 2017;16(1):63–73. doi:10.1177/1534735416645180
42. Chambers A, Damone E, Chen YT, et al. Social support and outcomes in older adults with lung cancer. J Geriatr Oncol. 2022;13(2):214–219. doi:10.1016/j.jgo.2021.09.009
43. Ma FY, Ren N, Tian MB, et al. Correlation between surgery control preference and perceived social support of lung cancer patients. Chin J Thoracic Cardiovasc Surg. 2023;12:1–6.
44. Fang XH, Wu Q, Tao SS, et al. Social support and depression among pulmonary tuberculosis patients in Anhui, China. J Multidiscip Healthc. 2022;15:595–603. doi:10.2147/jmdh.S356160
45. Zhang AJ, Wang ZG, Luo CC, et al. To explore the professional integration of medical social workers in the discharge preparation service for elderly patients led by case nurses. Beijing Med J. 2021;43(12):1212–1214. doi:10.15932/j.0253-9713.2021.12.015
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.